Evidence Review of the Adverse Effects of COVID-19 Vaccination and Intramuscular Vaccine Administration (2024)
Chapter: 10 Shoulder Injuries and Vaccines
10
Shoulder Injuries and Vaccines
INTRODUCTION
The deltoid muscle is the preferred location for vaccination because of an apparent lower risk of subcutaneous injection, and the immunogenicity is higher compared to gluteal injections (Shaw et al., 1989). The committee was tasked with reviewing the evidence regarding vaccination and specific injuries to the shoulder (see Chapter 1). Before doing so, for completeness, the committee provides background information on nonspecific shoulder injuries associated with vaccination but does not make conclusions. Unlike the previous chapters in this report, this chapter is not restricted to COVID-19 vaccines. Therefore, the literature search spans from 2011 to 2023, ensuring inclusion of material released subsequent to the last report by the Institute of Medicine (IOM) in 2012 (IOM, 2012).
The first report of a relationship between vaccination and shoulder injury profiled two patients who developed shoulder pain and dysfunction after injection into the deltoid (Bodor and Montalvo, 2007). Atanasoff et al. (2010) offered a case series of 13 patients who developed prolonged shoulder pain after vaccination and offered the term “SIRVA,” for “shoulder injury related to vaccine administration,” characterized by shoulder pain with limited motion that develops within a few minutes to <24 hours of vaccine administration and lasts more than 6 months, which distinguishes it from the typical transient soreness after vaccination administration (Atanasoff et al., 2010; Cagle, 2021).
SIRVA represents a clinical syndrome, is not a specific diagnosis, and may have a number of causes. There are no specific objective tests to diagnose the condition and no specific International Classification of Diseases (ICD)-10 codes exist for “SIRVA” (Zheng et al., 2022). In fact, “SIRVA represents a constellation of different pain-causing diagnoses” (Atanasoff et al., 2010; Cagle, 2021; MacMahon et al., 2022; Slette et al., 2022; Wood and Ilyas, 2022; Wright et al., 2023). As a result, “SIRVA” is considered confusing (Petrakis et al., 2023), is controversial (MacMahon et al., 2022), leads to conflicting reports in the literature (Leopold, 2022), and may be best described as a medico-legal term instead of a diagnosis (Mackenzie et al., 2022). The American Academy of Orthopaedic Surgeons offered a position statement (AAOS, 2017) that does not use the term “SIRVA” and states, “The members of the American Academy of Orthopaedic Surgeons (AAOS) take the position that vaccination administered to the shoulder cannot cause or contribute to common shoulder pathologies such as rotator cuff tendinopathy, glenohumeral arthritis, and adhesive capsulitis.”
In the absence of epidemiological studies, the committee chose to focus on case reports as the primary source of analysis, especially in this chapter. Despite being regarded as the lowest level of evidence, well-defined case reports can provide compelling evidence, which is what the committee aims to present in this context.
The committee has reviewed evidence on the etiology of shoulder injuries following vaccination, considering three possible mechanisms of injury. The first encompasses direct trauma from improper placement within the arm, potentially due to deviations from the optimal injection technique. The second mechanism involves injury following the needle or fluid injection, even when the vaccination is correctly placed, suggesting a reaction independent of the technique. The third potential mechanism is the constituents of the vaccine, such as antigens or adjuvants, which might induce harms without any error in the administration process. The committee will discern the most likely causative factors for shoulder injuries or related structural damage when possible.
The committee avoids “SIRVA” and, in response to the Statement of Task, instead focuses on the specific shoulder-related diagnoses that have been associated with vaccine administration. See Box 10-1 for all conclusions in this chapter.
BOX 10-1
Conclusions for Shoulder Injuries
Conclusion 10-1: The evidence establishes a causal relationship between vaccine administration and subacromial/subdeltoid bursitis caused by direct injection into the bursa.
Conclusion 10-2: The evidence establishes a causal relationship between vaccine administration and acute rotator cuff or acute biceps tendinopathy caused by direct injection into or adjacent to the tendon.
Conclusion 10-3: The evidence favors rejection of a causal relationship between vaccine administration and chronic rotator cuff disease.
Conclusion 10-4: The evidence is inadequate to accept or reject a causal relationship between vaccine administration and adhesive capsulitis.
Conclusion 10-5: The evidence is inadequate to accept or reject a causal relationship between vaccine administration and septic arthritis.
Conclusion 10-6: The evidence establishes a causal relationship between vaccine administration and bone injury caused by direct injection into or adjacent to the bone.
Conclusion 10-7: The evidence establishes a causal relationship between vaccine administration and axillary or radial nerve injury caused by direct injection into or adjacent to the nerve.
Conclusion 10-8: The evidence is inadequate to accept or reject a causal relationship between vaccine administration and Parsonage-Turner syndrome.
Conclusion 10-9: The evidence is inadequate to accept or reject a causal relationship between vaccine administration and complex regional pain syndrome.
SUBACROMIAL/SUBDELTOID BURSITIS
Subacromial/subdeltoid bursitis is characterized by inflammation of the subacromial and subdeltoid bursae located in the shoulder. Bursae are small, fluid-filled sacs that serve as cushions and lubricating structures between bones (see Figure 10-1), tendons, and muscles to reduce friction and enable smooth movement. Bursitis typically results from factors such as overuse, trauma, or underlying issues, such as rotator cuff injuries, tendonitis, or arthritis.
Common symptoms of subacromial/subdeltoid bursitis include shoulder pain, especially when performing overhead movements or lifting the arm, along with swelling, tenderness, reduced range of motion, radiating pain into the upper arm, and weakness (due to pain or disuse) in the affected shoulder. Diagnosis involves a physical examination by a health care provider and may include imaging studies, such as X-rays, ultrasonography, or magnetic resonance imaging (MRI) scans, to confirm the presence of bursitis and rule out other shoulder conditions.
The prevalence of subacromial/subdeltoid bursitis varies by age group. Although it can affect individuals of all ages, it is more commonly observed in adults, particularly those over the age of 30. This is largely due to age-related changes in the shoulder, such as degeneration of tendons and bursa, which can increase the risk of developing bursitis. The prevalence is not strongly biased toward one gender. Some studies have suggested that it may be slightly more common in men, but the gender difference is not significant.
The underlying causes often involve factors such as repetitive overhead activities, trauma, and pre-existing shoulder problems, including rotator cuff injuries and tendonitis. Individuals engaged in activities that place increased stress on the shoulder, such as athletes or manual laborers, may be at higher risk.
Evidence from Epidemiological Studies and Case Reports
In recent years, multiple case reports have documented patients developing acute subacromial bursitis shortly after receiving vaccines. Additionally, Hesse et al. (2020) used the Vaccine Safety Datalink to assess the risk of subdeltoid bursitis after influenza vaccination. They found that an attributable risk of 7.78 (95% confidence interval [CI]: 2.19–13.38) additional cases of bursitis occur per 1 million persons vaccinated. Post-vaccine subdeltoid bursitis has been observed in adults spanning an age range of 23–82 years. A common issue identified was the incorrect injection technique, particularly the placement of injections too high on the arm (see Figure 10-1), underscoring the importance of adherence to proper vaccination procedures to minimize risk of harm.
The evidence most significant to the committee consisted of numerous well-documented case reports in adults (see Table 10-1). No cases of imaging-documented bursitis after vaccine administration were found for the pediatric population.
The prognosis is generally positive, with most experiencing a complete resolution of symptoms. However, the recovery time can vary considerably, from as little as 1 week to as long as over 6 months, underscoring the importance of individualized care and management.
Patients with postvaccine subdeltoid bursitis have commonly reported that the vaccine was administered at a higher site than anticipated, as documented in studies by Atanasoff et al. (2010), Bodor and Montalvo (2007), and Hesse et al. (2020). This inadvertent high placement of the vaccine injection may be a contributing factor due to the proximity of the subacromial and subdeltoid bursae to the injection site.
To mitigate the risk of improper vaccine placement and reduce the likelihood of bursitis, numerous techniques and guidelines have been proposed and discussed in the medical literature. Researchers and health care providers have recognized the importance of ensuring correct vaccine administration to minimize the risk of complications. The literature is replete with reports and recommendations, including studies authored by Bancsi et al. (2018), Cook (2011), Cross et al. (2016), Doppen et al. (2023), Kowatari et al. (2023), Mardourian et al. (2023), Marshall et al. (2022), Nakajima et al. (2017), and Pettyjohn et al. (2022).
These reports and studies highlight the significance of proper injection and emphasize the need to avoid vaccine placement in the proximity of the subacromial and subdeltoid bursae.1 Inadvertently injecting the vaccine into or too close to these structures can lead to irritation, inflammation, and ultimately bursitis, resulting in pain and difficulty in shoulder motion technique (see Figure 10-1).
___________________
1 An IOM committee concluded that “the evidence convincingly supports a causal relationship between the injection of a vaccine and deltoid bursitis” (IOM, 2012).
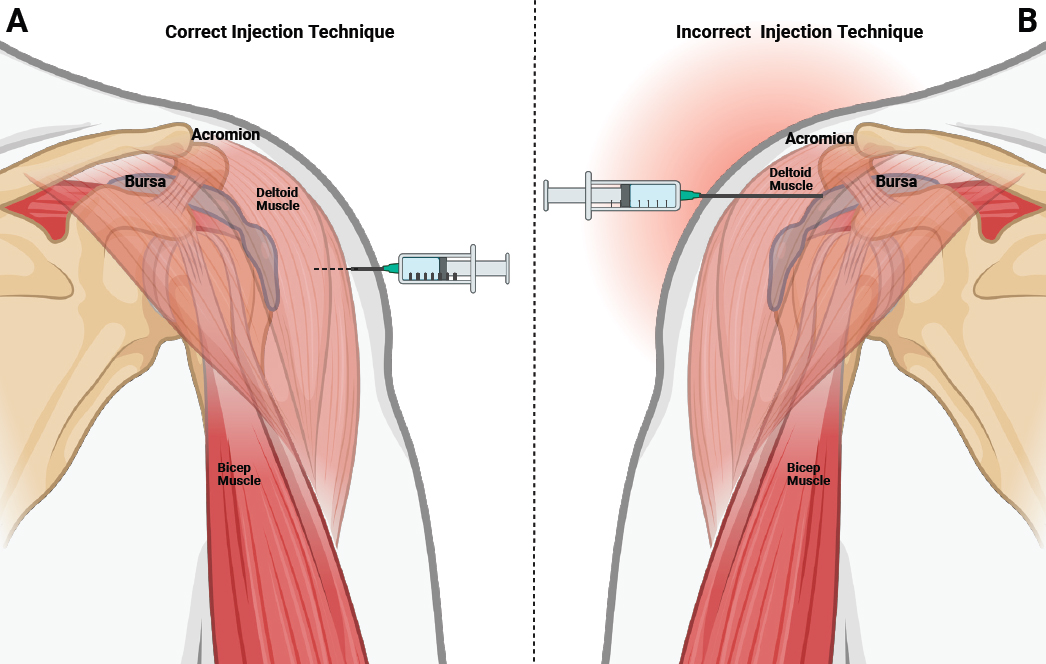
NOTES: A. Correct injection technique: Demonstrates proper administration of an intramuscular vaccine into the deltoid muscle, utilizing an appropriate anatomical approach for effective delivery. Dotted line indicates needle inside the deltoid muscle. B. Incorrect injection technique: Depicts an erroneous injection leading to inadvertent administration into the subdeltoid bursa, potentially inducing deltoid or subdeltoid bursitis. Solid needle line indicated breach into the bursa. Created with BioRender.com.
From Evidence to Conclusion
The committee conclusion is derived from a body of evidence, as demonstrated in the 15 case reports described in Table 10-1, that consistently features ultrasound or MRI imaging and symptom onset in the ipsilateral shoulder occurring within a biologically significant time window (typically 0–48 hours after vaccination). Studies that lacked pertinent imaging data or extend beyond this critical time frame present a less compelling connection to vaccination. Many patients report that the injection was “too high” or “too deep,” which would put the vaccine material in the subdeltoid bursa. The mechanism behind subacromial/subdeltoid bursitis following vaccine administration is closely tied to the incorrect placement of the needle, particularly when it is higher than expected.
Conclusion 10-1: The evidence establishes a causal relationship between vaccine administration and subacromial/subdeltoid bursitis caused by direct injection into the bursa.
TABLE 10-1 Case Reports Regarding Subacromial/Subdeltoid Bursitis After Vaccination
| Author | Age | Sex | Vaccine(s) | Onset of Symptoms | Symptom Duration Before Evaluation | Imaging |
|---|---|---|---|---|---|---|
| Cantarelli Rodrigues et al. (2021) | 61 | F | ChAdOx1-S | 30 min | 8 weeks | MRI |
| Chow et al. (2022) | 62 | F | ChAdOx1-S | Immediate | 2 weeks | Ultrasound and MRI |
| Chuaychoosakoon et al. (2021) | 52 | M | Sinovac (COVID-19) | 3 days | NR | Ultrasound |
| Chuaychoosakoon and Boonsri (2023) | 52 | F | mRNA COVID-19 | 2 weeks | 17 days | MRI |
| Cook (2014) | 76 | M | Influenza | Immediate | 3 days | Ultrasound |
| Cross et al. (2016) | 82 | F | Pneumococcal (PPSV23) | 2 hours | NR | Ultrasound |
| Cross et al. (2016) | 23 | F | DTaP | 24 hours | 2–3 days | Ultrasound |
| Honarmand et al. (2021) | 42 | M | mRNA-1273 | 2 days | NR | MRI |
| Honarmand et al. (2021) | 38 | M | BNT162b2 | 2 weeks | NR | Ultrasound |
| Jenkins et al. (2020) | 61 | F | Influenza | NR | 3 months | MRI |
| Maliwankul et al. (2022) | 52 | M | Sinovac (COVID-19) | 2 days | 6 days | MRI |
| Maliwankul et al. (2022) | 51 | F | ChAdOx1-S | 3 hours | 4 days | MRI |
| Maliwankul et al. (2022) | 71 | M | ChAdOx1-S | 1 day | 6 weeks | MRI |
| Maliwankul et al. (2022) | 68 | M | ChAdOx1-S | 1 day | 2 weeks | Ultrasound |
| Moya et al. (2022) | 69 | F | Sputnik V (COVID-19) | Immediate | 5 days | MRI |
| Okur et al. (2014) | 66 | F | Influenza | Immediate | NR | MRI |
| Okur et al. (2014) | 39 | M | Influenza | NR | 2 months | MRI |
| Okur et al. (2014) | 36 | M | Influenza | NR | NR | MRI |
| Pearson and Bent (2022) | 74 | M | COVID-19 (unspecified) | 3 days | 3–4 weeks | MRI |
| Salmon et al. (2015) | 26 | F | DTaP | NR | 48 hours | MRI |
| Uchida et al. (2012) | 45 | F | HPV (Cervarix) | 3 hours | 3 days | MRI |
| Wharton et al. (2022) | 31 | M | mRNA-1273 | 1 day | 2.5 weeks | MRI |
| Wong et al. (2021) | 51 | F | Influenza | 48 hours | 3 months | MRI |
| Wright et al. (2019) | 72 | F | Influenza | NR | 2 weeks | MRI |
| Yuen et al. (2022) | 84 | F | mRNA COVID-19 | 3 days | 1 week | MRI |
NOTES: BNT162b2 refers to the COVID-19 vaccine manufactured by Pfizer-BioNTech under the name Comirnaty®. mRNA-1273 refers to the COVID-19 vaccine manufactured by Moderna under the name Spikevax®. ChAdOx1-S refers to the COVID-19 vaccine manufactured by Oxford-AstraZeneca. DTaP: diphtheria, tetanus, and acellular pertussis; F: female; HPV: human papillomavirus; M: male; MRI: magnetic resonance imaging; NR: not reported.
SOURCES: Cantarelli Rodrigues et al., 2021; Chow et al., 2022; Chuaychoosakoon and Boonsri, 2023; Chuaychoosakoon et al., 2021; Cook, 2014; Cross et al., 2016; Honarmand et al., 2021; Jenkins et al., 2020; Maliwankul et al., 2022; Moya et al., 2022; Okur et al., 2014; Pearson and Bent, 2022; Salmon et al., 2015; Uchida et al., 2012; Wharton et al., 2022; Wong et al., 2021; Wright et al., 2019; Yuen et al., 2022.
ACUTE ROTATOR CUFF OR ACUTE BICEPS TENDINOPATHY
Acute rotator cuff or biceps tendinopathy caused by direct injection into the tendon or tendon sheath is characterized by onset of pain within 24 hours and evidence of acute pathology (such as marked edema in the tendon) on imaging. Imaging of a partial- or full-thickness rotator cuff tear or chronic tendinosis alone is insufficient to demonstrate a direct injury to the tendon.
Acute rotator cuff tendinopathy refers to acute inflammation or irritation of the tendons comprising the rotator cuff, a group of four tendons that surround the shoulder joint: the supraspinatus (SSP), infraspinatus, teres minor, and subscapularis tendons. Acute tendinopathy typically arises from trauma, overuse, or sudden strain on these tendons. Common clinical presentations include shoulder pain, limited range of motion, and localized tenderness. Imaging modalities, such as ultrasound or MRI, are often employed to aid in diagnosis, revealing signs of inflammation and tendon damage. Treatment strategies are rest, anti-inflammatory medication, physical therapy, and sometimes corticosteroid injections to alleviate pain and promote healing.
Acute biceps tendinopathy involves inflammation or injury to the long head of the biceps tendon, which runs through the bicipital groove in the upper arm and attaches to the superior labrum of the glenoid in the shoulder joint. This condition can arise from sudden overexertion, repetitive strain, or direct trauma to the biceps tendon. Clinical manifestations include localized anterior shoulder pain, which may be aggravated by certain movements, such as overhead lifting or reaching. Patients may experience weakness and discomfort during activities that involve the affected tendon. Diagnosis often relies on clinical evaluation, imaging studies (such as ultrasound or MRI), and occasionally, arthroscopy to assess the extent of damage. A consistent hallmark is the conspicuous enlargement of the affected tendon or muscle in diagnostic imaging with a significant increase in signal intensity, indicating pronounced edema. These findings are instrumental in identifying and characterizing the condition.
The clinical outcomes of individuals afflicted with this tendinopathy can be quite diverse. Although some improve in a week or two, others may endure discomfort and functional limitations for an extended period, sometimes beyond 6 months.
Mechanisms of Injury
In assessing the strength of mechanistic evidence related to this condition, it is important to consider the combination of clinical factors, including the specific demographic characteristics, imaging findings, and observed outcomes. These elements collectively contribute to the overall understanding of the cause of rotator cuff or biceps acute tendinopathy caused by vaccine injection, aiding in evaluation and management.
Evidence from Case Reports
Rotator cuff or acute biceps tendinopathy induced by inadvertent injection into the rotator cuff tendon or muscle has been notably reported in adults spanning a relatively wide age range, 26–83 years (see Table 10-2). Among these 14 cases, the onset of pain is a particularly salient feature, with the majority of individuals experiencing immediate discomfort. No cases of imaging-documented acute rotator cuff injury have been reported in the pediatric population.
TABLE 10-2 Case Reports of Acute Rotator Cuff or Acute Biceps Tendinopathy After Vaccination
| Author | Age | Sex | Vaccine | Onset of Symptoms | Symptom Duration Before Evaluation | Imaging | Findings |
|---|---|---|---|---|---|---|---|
| Bansal and DiLorenzo (2020) | 59 | F | DTaP | <24 hours | 6 weeks | MRI | High-grade partial teres minor tear |
| Barnes et al. (2017) | 22 | F | Influenza | 2 hours | 2 months | MRI and ultrasound | Partial supraspinatus tear |
| Bathia and Stitik (2009) | 34 | F | Influenza | Immediate | 3 weeks | MRI | Tendinosis of infraspinatus |
| Chuaychoosakoon and Boonsri (2023) | 52 | F | mRNA COVID-19 | NR | 3 days | MRI | Fluid supraspinatus tendinosis |
| Klabklay et al. (2022) | 50 | M | ChAdOx1-S | 3 hours | 3 days | Ultrasound | Swelling of supraspinatus, calcific tendonitis in subscapularis |
| Maliwankul et al. (2022) | 64 | M | ChAdOx1-S | 2 days | 1 month | Ultrasound | Biceps tenosynovitis |
| Nakajima et al. (2023) | 83 | F | BNT162b2 | Immediate | 8 days | X-ray and MRI | Calcium in supraspinatus inflammatory subdeltoid bursitis |
| Natanzi et al. (2020) | 42 | F | Influenza | Immediate | 7 weeks | MRI | Edema at teres minor insertion |
| Natanzi et al. (2020) | 38 | F | Influenza | Immediate | 2 months | MRI | Edema in humerus and teres minor insertion |
| Sahu and Shetty (2022) | 33 | M | Covaxin (COVID-19) | Immediate | 2 days | X-ray | Calcific tendonitis supraspinatus |
| Shabhaz et al. (2019) | 35 | F | Influenza | Immediate | 1 hour | MRI | Biceps tenosynovitis |
| Sukhija et al. (2022) | 26 | F | Covaxin (COVID-19) | 15 days | 15 days | MRI and ultrasound | Edema in myotendinous junction of teres minor* |
| Szari et al. (2019) | 31 | M | Influenza | Immediate | 4 months | MRI | Partial cuff tear diffuse cuff tendinosis |
| Zeldin et al. (2023) | 53 | F | Influenza | Immediate | 2 months | MRI | Fluid collection lateral to biceps groove with hyperechoic focus, possibly a needle tip |
NOTES: *The committee identified edema in the myotendinous junction of Teres Minor on the MRI images, which was not specifically indicated in the case study. BNT162b2 refers to the COVID-19 vaccine manufactured by Pfizer-BioNTech under the name Comirnaty®. ChAdOx1-S refers to the COVID-19 vaccine manufactured by Oxford-AstraZeneca. DTaP: diphtheria, tetanus, and acellular pertussis; F: female; M: male; MRI: magnetic resonance imaging; NR: not reported.
SOURCES: Bansal and DiLorenzo, 2020; Barnes et al., 2017; Bathia and Stitik, 2009; Chuaychoosakoon and Boonsri, 2023; Klabklay et al., 2022; Maliwankul et al., 2022; Nakajima et al., 2023; Natanzi et al., 2020; Sahu and Shetty, 2022; Shahbaz et al., 2019; Sukhija et al., 2022; Szari et al., 2019; Zeldin et al., 2023.
From Evidence to Conclusion
The committee’s decision is derived from a body of evidence, as demonstrated in the case reports provided (see Table 10-2). Injection of a vaccine into the biceps or rotator cuff tendon can produce an acute tendinosis characterized by edema and increased signal on ultrasound or MRI imaging.
Conclusion 10-2: The evidence establishes a causal relationship between vaccine administration and acute rotator cuff or acute biceps tendinopathy caused by direct administration of vaccine into or adjacent to the tendon.
CHRONIC ROTATOR CUFF DISEASE
Chronic rotator cuff disease comprises a diverse range of injuries and pathological conditions, with its prevalence escalating in correlation with age. This encompassing term encapsulates chronic tendinosis as well as partial- and full-thickness tears of the rotator cuff, collectively delineating the multifaceted nature of the condition. Approximately 22 percent of individuals over 40 are affected by full-thickness rotator cuff tears (Kuhn, 2023). The prevalence increases with advancing age: approximately 13 percent of people in their fifth decade, 20 percent in their sixth decade, 30 percent in their seventh decade, and a striking 50 percent in their eighth decade of life have full-thickness rotator cuff tears (Kuhn, 2023; Minagawa et al., 2013; Tempelhof et al., 1999; Teunis et al., 2014; Yamamoto et al., 2011). It is essential to note that the overwhelming majority of these cases are asymptomatic, meaning that individuals may not experience noticeable symptoms despite the presence of these tears (Jeong et al., 2017; Kuhn, 2023; Minagawa et al., 2013; Reilly et al., 2006; Tempelhof et al., 1999). As most patients with rotator cuff tears are asymptomatic it is not surprising that surgical intervention is performed in fewer than 5 percent of all individuals with rotator cuff tears (Kuhn, 2023).
In cases where individuals develop shoulder pain, particularly after vaccination, diagnostic imaging is frequently employed to evaluate the shoulder joint. An investigation of patients who applied for compensation through vaccine injury programs revealed that 80.3 percent of these individuals underwent MRI imaging. Interestingly, partial and complete rotator cuff tears were observed in 44.3 percent of these cases (Hesse et al., 2020). The median age was approximately 51, which aligns with the prevalence data in the general population. Given the high prevalence, especially in older individuals, it has been suggested that the observed rotator cuff pathology after vaccination is not directly related to the vaccine itself (AAOS, 2017; Slette et al., 2022).
Mechanism of Injury
Chronic tendinosis and partial- and full-thickness tears of the rotator cuff collectively represent common degenerative shoulder conditions (Jeong et al., 2017; Minagawa et al., 2013; Reilly et al., 2006; Tempelhof et al., 1999; Teunis et al., 2014). No plausible mechanism exists whereby vaccine administration would be responsible for chronic rotator cuff disease.
From Evidence to Conclusion
Chronic rotator cuff disease is typically a degenerative age-related condition and ubiquitous in the adult population. An injection into tendon material may produce increased signal on MRI imaging and an acute tendinosis (see section on acute tendinopathy) but not acute rotator cuff tears or corresponding rotator cuff muscle atrophy. Although it is common for patients with shoulder pain to undergo imaging and identify degeneration in the rotator cuff, these findings are more likely pre-existing and not related to a vaccine. The committee found the lack of a mechanistic explanation for chronic rotator cuff disease compelling.
Conclusion 10-3: The evidence favors rejection of a causal relationship between vaccine administration and chronic rotator cuff disease.
ADHESIVE CAPSULITIS
Frozen shoulder, also known as “adhesive capsulitis,” is a debilitating condition that affects 1–5 percent of the population (Kingston et al., 2018). Certain demographic factors may increase the risk, with higher prevalence rates in females between 40 and 60, who have obesity, or who have diabetes (Huang et al., 2013; Kingston et al., 2018). Despite the higher prevalence in those under 50, reports in pediatric patients are rare (Levin et al., 2021). Furthermore, frozen shoulder can sometimes manifest as a complication after surgical procedures or injuries that require immobilization, such as a proximal humerus fracture. The multifaceted demographic associations highlight the need for careful assessment and tailored management.
Diagnosing frozen shoulder can be a complex process. In the early stages, when the condition may be inflammatory, it is often a clinical diagnosis of exclusion, as it shares symptoms with other shoulder conditions. However, in later stages, where it may be fibrotic, a marked loss of motion becomes a defining feature. Diagnostic imaging, such as MRI, may reveal characteristic signs, including rotator interval thickening and axillary capsule thickening (Choi and Kim, 2020). Early diagnosis is critical for a favorable prognosis, but health care providers often face challenges in accurately diagnosing frozen shoulder in its early stages due to its shared symptoms.
Although frozen shoulder was considered a self-limited issue with a typical duration of 1-year, longer-term studies have revealed that some individuals continue to experience unresolved pain and limited motion beyond this time frame (Hand et al., 2008; Kim et al., 2020). These findings emphasize the importance of ongoing monitoring and management to optimize long-term outcomes. The multifaceted nature of this condition, including its demographic associations, diagnostic challenges, and evolving treatment approaches, underscores the complexity of addressing it effectively.
Evidence from Case Reports
Data reviewed by the committee regarding frozen shoulder after vaccination are limited (see Table 10-3): four case series ranging in sample size from 3 to 16 cases (Chu, 2022; Ghosh et al., 2023; Sahu and Shetty, 2022; Saleh et al., 2015). Three of the four reported on frozen shoulder with symptom onset within days after either BNT162b22 or ChAdOx1-S3 and diagnosis months to years later (Chu, 2022; Ghosh et al., 2023; Sahu and Shetty, 2022). In addition, three case studies reported frozen shoulder in three patients diagnosed months to a year after BNT162b2, mRNA-1273,4 or ChAdOx1-S. The fourth case series reported on frozen shoulder 1.5 months to 2 years after unidentified flu (n = 2) and pneumonia (n = 1) vaccination (Saleh et al., 2015). An additional two case studies reported on frozen shoulder after an unidentified flu vaccine (Thompson and Ensrud, 2020) and a human papillomavirus (HPV) vaccine (Smith et al., 2020); the child who had the HPV vaccine had diagnoses of Parsonage-Turner syndrome (PTS) and osteomyelitis.
From Evidence to Conclusion
The cause of frozen shoulder is still unclear, and diagnosis often comes at later stages, when a fibrotic process greatly limits motion and function. The clinical diagnosis is least clear early on, and a diagnosis months to years later makes establishing a cause and effect unlikely, given the many confounding factors over time. Thus, attribution to vaccination is difficult if not impossible.
Conclusion 10-4: The evidence is inadequate to accept or reject a causal relationship between vaccine administration and adhesive capsulitis.
___________________
2 The COVID-19 vaccine manufactured by Pfizer-BioNTech under the name Comirnaty®.
3 The COVID-19 vaccine manufactured by Oxford-AstraZeneca.
4 The COVID-19 vaccine manufactured by Moderna under the name Spikevax®.
TABLE 10-3 Case Reports of Adhesive Capsulitis After Vaccination
| Author | Age | Sex | Vaccine(s) | Onset of Symptoms | Symptom Duration Before Evaluation | Imaging | Findings |
|---|---|---|---|---|---|---|---|
| Aldosary (2022) | 52 | F | ChAdOx1-S | 24 hours | 8 months | MRI | Frozen shoulder 8 months after injection |
| Biglia et al. (2023) | 50 | F | BNT162b2 | 48 hours | 1 month | Ultrasound | Frozen shoulder |
| Chu (2022) | 18+ | 4 M 12 F |
BNT162b2 (12/16 patients) | 3.5 ± 2.5 days | >3 months | MRI | Frozen shoulder in 10/16 patients |
| Ghosh et al. (2023) | 48.7 ± 12.7 years | 5 M 4 F |
ChAdOx1-S | 12.3 ± 3.1 days | 9.4 ± 2.4 weeks | NR | Frozen shoulder |
| Quinodoz et al. (2023) | “In his 40s” | M | mRNA-1273 | 4 months | 1 year | MRI | Frozen shoulder |
| Sahu and Shetty (2022) | 10 cases, mean 53.8 | 9 F 1 M 4 diabetic or prediabetic and 4 hypothyroid |
ChAdOx1-S (9 cases) Covaxin (COVID-19) (1 case) |
24–48 hours | 14+ months | X-rays, MRI in 3 | Frozen shoulder |
| Saleh et al. (2015) | 30 67 69 |
2 M F |
Influenza (2) Pneumonia (1) |
Following day; soon after; same day | 3 months; 2 years; 6 weeks |
Lab work, X-ray, MRI | Frozen shoulder |
| Smith et al. (2020) | 15 | F | HPV (Gardisil) | 11 days | NR | X-ray, MRI | Frozen shoulder, Parsonage-Turner, and osteomyelitis |
| Thompson and Ensrud (2020) | 64 | M | Influenza | 3 days | >9 months | MRI | Frozen shoulder 6 months after injection |
NOTES: BNT162b2 refers to the COVID-19 vaccine manufactured by Pfizer-BioNTech under the name Comirnaty®. mRNA-1273 refers to the COVID-19 vaccine manufactured by Moderna under the name Spikevax®.ChAdOx1-S refers to the COVID-19 vaccine manufactured by Oxford-AstraZeneca. F: female; HPV: human papillomavirus; M: male; MRI: magnetic resonance imaging; NR: not reported.
SOURCES: Aldosary, 2022; Biglia et al., 2023; Chu, 2022; Ghosh et al., 2023; Quinodoz et al., 2023; Sahu and Shetty, 2022; Saleh et al., 2015; Smith et al., 2020; Thompson and Ensrud, 2020.
SEPTIC ARTHRITIS
Septic arthritis of the shoulder, also referred to as “infectious arthritis,” is a rare but serious condition characterized by the invasion of the shoulder joint by infectious microorganisms, typically bacteria. A cross-sectional study involving 97 patients indicated that the primary source of infection is often hematogenous, meaning that the bacteria spread through the bloodstream and access the joint (Sweet et al., 2019). However, other contiguous infections (e.g., soft tissue abscess, osteomyelitis) can be a cause. Septic arthritis can also arise from direct inoculation of bacteria into the joint via major trauma or, very rarely, by injection of bacterially contaminated material directly into the joint. The most commonly identified infectious organism in these cases is Staphylococcus aureus. Septic arthritis leads to inflammation and damage within the joint, resulting in significant pain, reduced range of motion, and potential joint destruction if not promptly and effectively managed.
TABLE 10-4 Case Reports of Septic Arthritis After Vaccination
| Author | Age | Sex | Vaccine | Onset of Symptoms | Symptom Duration Before Evaluation | Imaging | Findings |
|---|---|---|---|---|---|---|---|
| Darnley et al. (2019) | 32 | F | Influenza | 2 weeks | NR | Negative X-rays, positive MRI |
Septic arthritis |
| Floyd et al. (2012) | 59 | F | Pneumococcal (PPSV23) | 2 hours | 3 days | MRI and surgical cultures negative | Aseptic inflammatory arthritis |
NOTE: F: female; MRI: magnetic resonance imaging; NR: not reported.
SOURCES: Darnley et al., 2019; Floyd et al., 2012.
Epidemiological data on septic arthritis of the shoulder are limited, but estimates suggest an annual U.S. incidence of approximately 3,200 cases (Jiang et al., 2017). Certain risk factors have been associated with an increased likelihood, including older age, pre-existing joint diseases, lower socioeconomic status, diabetes, and underlying skin infections (Brennan and Hsu, 2012; Favero et al., 2008; Kunutsor et al., 2016).
Diagnosis typically involves a combination of clinical evaluation, laboratory testing, and imaging studies. One key criterion is the presence of a positive synovial fluid culture, which confirms the presence of infectious microorganisms within the joint. Laboratory tests, such as complete blood counts and inflammatory markers, can support the diagnosis.
Evidence from Case Reports
The evidence reviewed by the committee, two case studies, is meager (see Table 10-4). In the first case (Darnley et al., 2019), the diagnosis was made via surgical pathology 3.5 months after influenza vaccination. Given the long interval between vaccination and diagnosis, it is impossible to rule out other sources of the infection. Furthermore, the initial MRI finding of an SSP tear could have explained the shoulder pain. In the second case, the diagnosis was septic arthritis, but a surgical culture was negative (Floyd et al., 2012). Neither case report was of a child.
From Evidence to Conclusion
Evidence linking septic arthritis of the shoulder with vaccination is limited to two case studies.
Conclusion 10-5: The evidence is inadequate to accept or reject a causal relationship between vaccine administration and septic arthritis.
BONE INJURY
Bone injuries following vaccinations have been highlighted through numerous case reports, indicating a wide array of bone-related issues in adults. There are diverse symptoms that typically manifest within a few days after vaccination. Advanced diagnostic tools such as MRI have been used in uncovering a range of bone pathologies post-vaccination, including marrow edema, cortical bone erosions, avascular necrosis, and cystic lesions particularly noted in the humeral head (see Table 10-5).
Mechanism of Injury
The mechanism underlying bone injury after vaccination is supported by one small case series where 12 of 16 adults diagnosed with an influenza vaccine–mediated shoulder injury had ultrasound, immunophenotypic analyses, human leukocyte antigen (HLA) typing, and antigen-specific immunoassays. Vaccine-related bone toxicity and T cell/osteoclast interactions were assessed in vitro. Of these 12 adults, imaging demonstrated inflammatory tissue
TABLE 10-5 Case Reports of Bone Injury After Vaccination
| Author | Age | Sex | Vaccine | Onset of Symptoms | Symptom Duration Before Evaluation | Imaging | Findings |
|---|---|---|---|---|---|---|---|
| Erickson et al. (2019) | 51 | F | Influenza | 1 day | 10 months | MRI at 2 months and 10 months | 10-month MRI showed humeral head osseous erosion |
| Flores et al. (2022) | 49 | M | Influenza | 1 day | 2 months | MRI | Bone marrow edema |
| Kashkosh et al. (2023) | 40 | M | COVID-19 | 2 days | 12 weeks | MRI, normal CT 3 months prior | Focal avascular necrosis |
| Kuether et al. (2011) | 48 | F | Influenza | 2.5 hours | 10 weeks | MRI | Localized avascular necrosis humeral head |
| Littrell et al. (2020) | 51 | M | Influenza | 2 hours | 6 weeks | MRI 6 weeks | 6 weeks: cortical irregularity, bone edema 9 months : progressive erosive changes of humeral head bone marrow edema |
| Messerschmitt et al. (2012) | 46 | M | Influenza | 3 days | 3 weeks | Bone scan, MRI, X-ray | Humeral head lytic lesion chondrolysis from intraosseous injection |
| Okur et al. (2014) | 39 | M | Influenza | NR | 2 months | MRI | Edema in greater tuberosity |
| Okur et al. (2014) | 36 | M | Influenza | NR | NR | MRI | Edema in greater tuberosity |
| Salmon et al. (2015) | 26 | F | Diptheria, tetanus, polio | NR | 48 hours | MRI | Edema in humeral head |
| Shabhaz et al. (2019) | 35 | F | Influenza | Immediate | 1 hour | MRI 1 week, 6 weeks, 8 months |
1 week effusion 4 weeks biceps tendonitis 8 months reactive bone edema |
| Szari et al. (2019) | 31 | M | Influenza | Immediate | 4 months | MRI | Edema in humeral head |
| Taylor and Hinke (2014) | 55 | F | Influenza | <1 day | 3 months | MRI | Humeral head edema, repeat at 3 months, cortical erosion |
NOTES: CT: computed tomography scan; F: female; M: male; MRI: magnetic resonance imaging; NR: not reported.
SOURCES: Erickson et al., 2019; Flores et al., 2022; Kashkosh et al., 2023; Kuether et al., 2011; Littrell et al., 2021; Messerschmitt et al., 2012; Okur et al., 2014; Salmon et al., 2015; Shabhaz et al., 2019; Szari et al., 2019; Taylor and Hinke, 2014.
damage, including bone erosions, in six. Tissue damage was associated with a strong peripheral blood T and B cell activation and extracellular matrix-reactive autoantibodies (autoantigen microarray). Subjects with erosions were HLA-DRB1*04 positive and showed extracellular matrix-reactive HLA-DRB1*04 restricted T cell responses targeting heparan sulfate proteoglycan. Antigen-specific T cells potently activated osteoclasts via receptor activator of nuclear factor kappa-B (RANK) interaction with its ligand (RANK/RANK-L), and the osteoclast activation marker Trap5b was high in sera of patients with an erosive shoulder injury. In vitro, the vaccine adjuvant alphatocopheryl succinate recapitulated bone toxicity (Hirsiger et al., 2021).
Evidence from Case Reports
Vaccine-related bone injury has appeared in a number of case reports for adults aged 22–55. No pediatric cases of imaging-documented vaccine-related bone injury have been reported (see Table 10-5). Symptoms typically
develop within 3 days. MRI demonstrated a variety of bone pathologies, including marrow edema near the site of the injection, cortical bone erosions (Salmon et al., 2015), avascular necrosis (Kashkosh et al., 2023; Kuether et al., 2011), and humeral head cystic lesions (Erickson et al., 2019). Treatment included nonsteroidal anti-inflammatory drugs, corticosteroid injections, physical therapy, and rarely surgery. The course for recovery of bone changes is variable but typically lasts many months.
From Evidence to Conclusion
The conclusion is derived from a body of evidence, as demonstrated in the case reports (see Table 10-5), which consistently feature imaging and symptom onset within a biologically significant time window (typically 0–72 hours after vaccination). Studies that lack pertinent imaging data or extend beyond this critical time frame are likely to present a less compelling connection to vaccination. Patients who develop shoulder pain after vaccination will rarely demonstrate bone erosions, new-onset avascular necrosis, or bone marrow edema. These changes occur at the site of the injection and appear acute on imaging. Although the mechanistic data are limited, they do suggest that bone erosions in patients with shoulder pain may have T cell activation of osteoclasts, which would produce these erosions.
Conclusion 10-6: The evidence establishes a causal relationship between vaccine administration and bone injury caused by direct injection into or adjacent to the bone.
AXILLARY OR RADIAL NERVE INJURY
The axillary nerve is a branch of the brachial plexus, a network of nerves in the shoulder and upper arm. It controls the deltoid, a major muscle involved in shoulder movement and stability. Axillary nerve injury can occur due to various causes, including trauma, compression, or surgical procedures in the shoulder area. Common symptoms include weakness or paralysis of the deltoid muscle, leading to difficulty in raising the arm and performing overhead movements.
The radial nerve is another major nerve of the arm, originating from the brachial plexus, connecting to the muscles that control wrist and finger extension, and playing a vital role in hand and forearm function. Radial nerve injuries can result from a variety of factors, including trauma, fractures of the arm bones, compression of the nerve, or complications from medical procedures. Symptoms typically include weakness or loss of function in wrist and finger extension, which can lead to difficulties in gripping objects and performing fine motor tasks.
Nerve injuries, including to the axillary and radial nerves, can vary in severity, from mild and temporary to more severe and long lasting, depending on the cause and extent. Treatment may involve physical therapy, medication, and sometimes surgical intervention to repair the damaged nerve or address underlying issues. Nerve injuries can significantly impact motor function, and management is often focused on restoring as much functionality as possible.
Axillary and radial nerve injuries can also be associated with vaccination, particularly when the vaccine is injected directly into or very close to the nerve. This unusual occurrence is characterized by progressive weakness that typically develops within 24 hours. To support the diagnosis of such injuries related to vaccination, medical professionals often rely on diagnostic tests, such as electromyogram and nerve conduction studies (EMG/NCS), and imaging techniques, such as ultrasound or MRI. These tests can help confirm the presence of nerve damage and its specific location, aiding in the identification and evaluation of the injury.
In these cases, the proximity of the vaccine injection site to the nerves in question can potentially lead to localized trauma or inflammation, resulting in nerve injury and its associated symptoms. Vaccine-related nerve injuries are extremely rare and represent only a small fraction of vaccine-related adverse events. Nonetheless, health care professionals carefully monitor and investigate such cases to ensure vaccine safety and provide appropriate care.
Mechanism of Injury
The mechanism related to vaccination appears to stem from a direct injury to the nerve or inflammation in the vicinity of the nerve. This typically occurs when the needle placement is in close proximity to the nerve, which may inadvertently traumatize or irritate it, leading to damage. The proximity of the injection to the nerve can result in localized trauma or inflammation, which may trigger nerve injury or lead to nerve compression, irritation, or damage, ultimately resulting in weakness and related symptoms. This mechanism highlights the importance of precise and careful injection techniques to minimize the risk.
Evidence from Case Reports
Direct nerve injuries related to vaccination have been documented in four case reports (Beredjiklian et al., 2012; Blumstein and Kreithen, 1966; Imran and Hayley, 2013; Meirelles and Motta Filho, 2004) (see Table 10-6). A comprehensive review of these data appears in a systematic review (Wright et al., 2023).
These cases reveal certain demographic patterns: direct nerve injuries have been exclusively reported in adults, spanning a wide age range, 23–73 years. The vaccines included two solitary influenza, one combined influenza and tetanus/diphtheria, and one tetanus. Of the documented cases, two involved injuries to the axillary nerve; the other two affected the radial nerve. All four patients consistently reported developing symptoms within 24 hours after vaccination. These symptoms typically manifested as progressive weakness in the affected limbs. No cases of nerve injury related to vaccination have been reported in children.
Physicians employed a variety of diagnostic techniques. EMG and NCS were used to identify the nerve injuries in two patients, and imaging techniques such as ultrasound or MRI were employed for one patient each.
The treatment approach in all four cases was nonsurgical, emphasizing noninvasive methods to manage the nerve injuries. Ultimately, all four patients experienced a degree of recovery, regaining function, although recuperation time varied significantly. The recovery period ranged from as short as 1 month to as long as 31 months. One patient reported some residual weakness even after recovery, underlining the diversity in outcomes among cases of direct nerve injury associated with vaccination.
TABLE 10-6 Case Reports of Axillary or Radial Nerve Injury After Vaccination
| Author | Cases | Age | Sex | Vaccine | Onset of Symptoms | Symptom Duration Before Evaluation | Imaging |
|---|---|---|---|---|---|---|---|
| Beredjiklian et al. (2012) | 1 | 26 | M | Influenza | 16 hours | 1 day | MRI edema along radial nerve EMG neuropathy |
| Blumstein and Kreithen (1966) | 1 | 23 | M | Tetanus | <1 day | 7 hours | NR |
| Imran and Hayley (2013) | 1 | 73 | M | Influenza | Immediate | 8 weeks | None |
| Meirelles and Motta Filho (2004) | 1 | 67 | M | Influenza, diphtheria, tetanus | <1 day | 6 months | NCS axillary nerve with reinnervation |
NOTES: EMG: electromyogram; M: male; MRI: magnetic resonance imaging; NCS: nerve conduction study; NR: not reported.
SOURCES: Beredjiklian et al., 2012; Blumstein and Kreithen, 1966; Imran and Hayley, 2013; Meirelles and Motta Filho, 2004.
From Evidence to Conclusion
The committee conclusion is derived from a body of evidence, as demonstrated in the case reports provided (see Table 10-6), which consistently feature imaging or EMG/NCS and symptom onset occurring within a biologically significant time (typically 0–24 hours after vaccination). Studies that lack pertinent imaging data or extend beyond this critical time frame are likely to present a less compelling connection to vaccine administration.
The axillary and radial nerves are potentially at risk for deltoid vaccine injections. A direct injection of vaccine material into or near a nerve could damage it, producing pain and weakness for its sensory and motor portions. Damage can be confirmed by diagnostic studies.
Conclusion 10-7: The evidence establishes a causal relationship between vaccine administration and axillary or radial nerve injury caused by direct injection into or adjacent to the nerve.
PARSONAGE-TURNER SYNDROME
PTS is a clinical syndrome classically typified by new onset of pain in the upper quarter followed by, within hours to days, paresis. Also known as “neuralgic amyotrophy” or “idiopathic brachial plexus neuropathy,” it presents as a distinctive clinical syndrome characterized by abrupt, intense pain, typically within the shoulder and upper arm regions (Van Eijk et al., 2016). This pain is often described as sharp, burning, or neuralgic. Within a relatively short time frame, typically hours to days, individuals can develop muscle weakness or paralysis that is often localized along the innervation pathway of specific nerves within the brachial plexus, resulting in particular functional impairments (Van Eijk et al., 2016).
Commonly affected nerves include the long thoracic, suprascapular, and anterior interosseous nerves (Van Eijk et al., 2016). Damage to the long thoracic nerve can lead to scapular winging, characterized by the abnormal protrusion of the shoulder blade, which can cause both visible and functional changes in the shoulder region. Injury to the suprascapular nerve often makes it challenging to lift the arm and rotate it outward. Damage to the anterior interosseous nerve may lead to decreased grip strength, impacting the ability to hold and grasp objects effectively. In addition to pain and muscle weakness, individuals may experience tingling sensations and sensory disturbances in the upper extremity. This multifaceted clinical presentation underscores the complexity of PTS.
The diagnosis typically involves a thorough clinical assessment and EMG/NCS. Occasionally, an MRI will show inflammation around the brachial plexus. These diagnostic tests help confirm the presence of nerve damage and assess the extent of neural involvement.
The prevalence of PTS is not well defined and has generated variable estimates. The epidemiology remains uncertain, and incidence rates reported in the literature vary significantly, from 1–3 cases per 1,000 to 1–3 cases per 100,000 (van Alfen et al., 2015; Van Eijk et al., 2016). This disparity highlights the challenges in precisely establishing prevalence.
PTS may be more frequent in certain populations. Some studies have suggested that it may be more common in men than women (Ameer et al., 2023; van Alfen and van Engelen, 2006), but the underlying factors contributing to this difference are not fully explained. Children can be diagnosed with PTS, albeit rarely and more often after immunization or viral infection (van Alfen et al., 2000).
Mechanism of Injury
The pathophysiology also remains unclear. The evidence does not support a genetic susceptibility or autoimmunity as primary causes. Limited low-level evidence has indicated potential associations between PTS and recent infections, but the causative relationship remains uncertain (van Alfen and van Engelen, 2006). Additionally, there have been reports of PTS after vaccination for various diseases, including COVID-19 (Ameer et al., 2023), influenza (Shaikh et al., 2012), and typhoid (Kim et al., 2021). These associations are still a subject of ongoing investigation and require further research to establish the nature of these links definitively.
TABLE 10-7 Case Reports of Parsonage-Turner Syndrome After Vaccination
| Author | Age | Sex | Vaccine | Onset of Symptoms | Symptom Duration Before Evaluation | Imaging | Findings |
|---|---|---|---|---|---|---|---|
| Bernheimer and Gasbarro (2022) | 42 | F | mRNA-1273 | 3 weeks | 3 weeks + 1 day | MRI unremarkable | Parsonage-Turner syndrome |
| Chua et al. (2022) | 64 | M | mRNA-1273 | 12–24 hours | 3 weeks | EMG, nerve conduction study, MRI | Brachial neuritis |
| Coffman et al. (2021) | 66 | F | BNT162b2 | 1 month | NR | EMG | Parsonage-Turner syndrome |
| Flikkema and Brossy (2021) | 43 | M | mRNA-1273 | 2 days | NR | MRI of brachial plexus | Parsonage-Turner syndrome |
| Fransz et al. (2014) | 25 | M | Hepatitis B | 1 month | NR | EMG | Parsonage-Turner syndrome |
| Holmes et al. (2019) | 12 | M | Influenza | More than a year | NR | None | Brachial neuritis |
| Kang and Cho (2022) | 63 | M | ChAdOx1-S | Within a week | 1 month | EMG | Brachial neuritis |
| Kawegere and Goldberg (2022)> | 62 | F | Influenza | Within hours | NR | X-ray, MRI | Brachial neuritis |
| Kim et al. (2021) | 20 | M | Typhoid | 6 days | 3 days | EMG, MRI | Parsonage-Turner syndrome |
| Koh et al. (2021) | Mean 50.66 with range 44–58 | 3 M | 2 BNT162b2 and 1 mRNA-1273 | 25 days, 4 days, 7 days | NR | MRI, EMG | Parsonage-Turner syndrome |
| Lindgren et al. (2019) | 54 | M | Shingles | A few days | 9+ months | EMG, MRI | Parsonage-Turner syndrome |
| Öncel and Coşkun (2022) | 56 | M | BNT162b2 (second dose) | 24 hours | NR | EMG, MRI | Parsonage-Turner syndrome |
| Shields et al. (2022) | 6 patients aged 36–84 | 3 M 3 F |
mRNA-1273 and BNT162b2 | Not stated | NR | EMG | Parsonage-Turner syndrome |
| Sinha and Gupta (2017) | 85 | M | Influenza | 1 week | NR | MRI, EMG | Parsonage-Turner syndrome |
| VanLancker and Sheth (2022) | 29 | M | mRNA COVID-19, Influenza | A few hours | NR | EMG | Brachial neuritis |
| Vitturi et al. (2021) | 51 | M | ChAdOx1-S | Onset of symptoms not reported | A few days | EMG | Brachial neuritis |
NOTES: BNT162b2 refers to the COVID-19 vaccine manufactured by Pfizer-BioNTech under the name Comirnaty®. mRNA-1273 refers to the COVID-19 vaccine manufactured by Moderna under the name Spikevax®. ChAdOx1-S refers to the COVID-19 vaccine manufactured by Oxford-AstraZeneca. EMG: electromyogram; F: female; M: male; MRI: magnetic resonance imaging; NR: not reported.
SOURCES: Bernheimer and Gasbarro, 2022; Chua et al., 2022; Coffman et al., 2021; Flikkema and Brossy, 2021; Fransz et al., 2014; Holmes et al., 2019; Kang and Cho, 2022; Kawegere and Goldberg, 2022; Kim et al., 2021; Koh et al., 2021; Lindgren et al., 2019; Öncel and Coşkun, 2022; Shields et al., 2022; Sinha and Gupta, 2017; VanLancker and Sheth, 2022; Vitturi et al., 2021.
Evidence from Case Reports
A syndrome is defined by a collection of clinical signs and symptoms where the pathophysiology and cause of a disease are poorly understood. PTS is no exception. The evidence reviewed by the committee is confined to two case series, totaling nine patients, and 14 case studies (see Table 10-7). In the case series of six patients, all of them reported symptoms after COVID-19 messenger ribonucleic acid (mRNA) injection (BNT162b2, mRNA-1273), but when symptoms appeared was not reported in individual patients, making the timeline unknown (mean duration of 17 days, with 5 days–8-week range) (Shields et al., 2022). In the case series of three patients, symptoms appeared 4–25 days after mRNA injection (two BNT162b2 and one mRNA-1273) (Koh et al., 2021). In addition, in nine case studies, symptoms appeared days to months after COVID-19 vaccination, the majority after mRNA vaccines. In five case studies, symptoms appeared after vaccinations for influenza (n = 3), hepatitis B (n = 1), and typhoid (n = 1).5
From Evidence to Conclusion
The committee identified descriptions of PTS after vaccination in 23 people. In several cases, the onset of symptoms was either not reported or months after several different kinds of vaccination. In addition, PTS appears to be rare with a poorly understood pathophysiology; because of these issues, the evidence is limited to case studies, and establishing cause and effect is difficult.
Conclusion 10-8: The evidence is inadequate to accept or reject a causal relationship between vaccine administration and Parsonage-Turner syndrome.
COMPLEX REGIONAL PAIN SYNDROME
Complex regional pain syndrome (CRPS), previously known as “reflex sympathetic dystrophy,” is a multifaceted and often debilitating chronic condition that typically affects a limb, although it can spread to other parts of the body. CRPS is characterized by persistent, intense pain, and a range of sensory, motor, and autonomic symptoms.
CRPS exhibits a diverse demographic profile. Its incidence varies widely across studies, estimated at 5–26 individuals per 100,000 per year (de Mos et al., 2007; Elsharydah et al., 2017; Ott and Maihofner, 2018; Sandroni et al., 2003). Certain demographic variables have been associated with a higher risk, including being female and of Caucasian ethnicity and having a higher socioeconomic status, a history of depression, headaches, or drug abuse (Elsharydah et al., 2017). Conversely, diabetes, obesity, and hypothyroidism have been linked to lower rates of CRPS Type 1 (Elsharydah et al., 2017; Harden et al., 2010). Evidence is quite limited in children. A scoping review on CRPS in pediatric athletes (Moretti et al., 2021) identified twelve case studies and three case series implying that sport-related injury may be a causal factor.
Diagnosis can be challenging, given no universally accepted standard. To enhance diagnostic accuracy, the Budapest criteria, developed by Harden and colleagues in 2007 (see Table 10-8), have been used (Harden et al., 2007; Kessler et al., 2020). They include a combination of clinical effects, including sensory, vasomotor, sudomotor/edema, and motor/trophic symptoms, and provide a standardized framework to aid health care providers, promoting more consistent and accurate identification. The fourth criterion seems to indicate that CRPS is a diagnosis of exclusion.
Mechanism of Injury
The pathological etiology remains complex and multifactorial. Although a definitive cause has not been established, inflammation is considered a potential contributor. Research has indicated elevated levels of proinflammatory
___________________
5 An IOM committee concluded that “the evidence favors acceptance of a causal relation between tetanus toxoid and brachial neuritis” (IOM, 1994).
TABLE 10-8 Budapest Criteria to Diagnose Complex Regional Pain Syndrome
| 1. Continuing pain that is disproportionate to inciting event | |
| 2. At least one sign in three of four categories by history | Sensory: Hyperesthesia or allodynia Vasomotor: Temperature abnormalities/asymmetry, skin color changes/asymmetry Sudomotor: Edema, sweating changes/asymmetry Motor/trophic: Decreased range of motion; weakness; dystonia; hair, nail, or skin changes |
| 3. At least one sign in two of four categories by exam | Sensory: Evidence of hyperalgesia (to pinprick) and/or allodynia (to light touch and/or temperature sensation and/or deep somatic pressure and/or joint movement) Vasomotor: Evidence of temperature asymmetry > 1 degree C, skin color changes/asymmetry Sudomotor: Evidence of edema, sweating changes, asymmetry Motor/trophic: Evidence of decreased range of motion; weakness; tremor; dystonia; hair, nail, skin changes |
| 4. There is no other diagnosis that better explains the symptoms | |
SOURCES: Harden et al., 2007; Kessler et al., 2020.
cytokines and decreased levels of the anti-inflammatory protein interleukin (IL)-1RA, suggesting an inflammatory component (Lenz et al., 2013). Trauma has also been implicated as a cause (Beerthuizen et al., 2012).
Evidence from Case Reports
Evidence reviewed by the committee on the association of CRPS with vaccination is confined to one database study of 120 female vaccinees after HPV (Ozawa et al., 2017) and one after anthrax (Phillips et al., 2017) (see Table 10-9). Unfortunately, the database study (Ozawa et al., 2017) had no report of treatment or outcome, and patients reported onset of symptoms an average of 319 days after vaccination. Over such an extended period, many confounding factors are likely. Another study (Naleway et al., 2023) assessed the incidence of CRPS involving the upper extremity in individuals aged 9-30 years in a single integrated health system during three time periods: 2002–2006, before HPV vaccine licensure; 2007–2012, after licensure but before published case reports; and 2013–2017, after published case reports. Cases were identified using ICD-9/ICD-10 codes and text-based diagnoses
TABLE 10-9 Case Reports of Complex Regional Pain Syndrome After Vaccination
| Author | Age | Sex | Vaccine | Onset of Symptoms | Symptom Duration Before Evaluation | Imaging | Findings |
|---|---|---|---|---|---|---|---|
| Naleway et al. (2023) | 14 | F | HPV | Same day as vaccination | 49 days | NR | CRPS |
| Ozawa et al. (2017) | Mean 13.6 ±1.6 years; range 11–19 | 120 F | HPV | 1 to 1,532 days (average 319.7 ± 349.3 days) | >8 months | NR | CRPS |
| Phillips et al. (2017) | 21 | F | Anthrax | 2 weeks | >7 months | EMG, MRI | CRPS |
NOTES: CRPS: complex regional pain syndrome; EMG: electromyogram; F: female; HPV: human papillomavirus; MRI: magnetic resonance imaging; NR: not reported.
SOURCES: Naleway et al., 2023; Ozawa et al., 2017; Phillips et al., 2017.
in the electronic health record. There was no difference in the incidence between these three time periods, and out of the total of 113 verified cases identified, only one case was attributed by a practitioner to HPV vaccination.6
From Evidence to Conclusion
A syndrome is defined by a collection of clinical signs and symptoms where the pathophysiology and cause of a disease are poorly understood. CRPS is no exception. The case descriptions in Table 10-9 include sufficiently long times between vaccination and onset of symptoms to cloud interpretation of the role vaccination might have played.
Conclusion 10-9: The evidence is inadequate to accept or reject a causal relationship between vaccine administration and complex regional pain syndrome.
REFERENCES
AAOS (American Academy of Orthopaedic Surgeons). 2017. Position statement 1190: Rotator cuff tendinopathy and glenohumeral arthritis are unlikely to be caused by vaccine administration. American Academy of Orthopaedic Surgeons.
Aldosary, A. H. 2022. Prolonged shoulder dysfunction after coronavirus disease vaccination: A case of shoulder injury related to vaccine administration. SAGE Open Medical Case Reports 10:2050313X221089494. https://doi.org/10.1177/2050313x221089494.
Ameer, M. Z., A. U. Haiy, M. H. Bajwa, H. Abeer, B. Mustafa, F. Ameer, Z. Amjad, and A. U. Rehman. 2023. Association of Parsonage-Turner syndrome with COVID-19 infection and vaccination: A systematic review. Journal of International Medical Research 51(7):3000605231187939. https://doi.org/10.1177/03000605231187939.
Atanasoff, S., T. Ryan, R. Lightfoot, and R. Johann-Liang. 2010. Shoulder injury related to vaccine administration (SIRVA). Vaccine 28(51):8049–8052. https://doi.org/10.1016/j.vaccine.2010.10.005.
Bancsi, A., S. K. D. Houle, and K. A. Grindrod. 2018. Getting it in the right spot: Shoulder injury related to vaccine administration (SIRVA) and other injection site events. Canadian Pharmacists Journal 151(5):295–299. https://doi.org/10.1177/1715163518790771.
Bansal, D., and D. R. DiLorenzo. 2020. Shoulder injury related to vaccine administration: Isolated teres minor tear. Applied Radiology 49(1):50–52.
Barnes, L. A. F., H. M. Kim, J. M. Caldwell, J. Buza, C. S. Ahmad, L. U. Bigliani, and W. N. Levine. 2017. Satisfaction, function and repair integrity after arthroscopic versus mini-open rotator cuff repair. The Bone & Joint Journal 99-B(2):245–249. https://doi.org/10.1302/0301-620X.99B2.BJJ-2016-0055.R1.
Bathia, N. A., and T. Stitik. 2009. Poster 35: “Influenza vaccine shoulder”—vaccination-related traumatic injury to the infraspinatus: A case report. PM&R 9(1):S118.
Beerthuizen, A., D. L. Stronks, A. Van’t Spijker, A. Yaksh, B. M. Hanraets, J. Klein, and F. J. P. M. Huygen. 2012. Demographic and medical parameters in the development of complex regional pain syndrome type 1 (CRPS1): Prospective study on 596 patients with a fracture. Pain 153(6):1187–1192. https://doi.org/10.1016/j.pain.2012.01.026.
Beredjiklian, P. K., L. N. Nazarian, M. J Bercik, M. Gorski, and S. Mandel. 2012. Isolated radial nerve palsy secondary to influenza vaccination: A case report with imaging correlation. Practical Neurology 14–16.
Bernheimer, J. H., and G. Gasbarro. 2022. Parsonage-Turner syndrome following vaccination with mRNA-1273 SARS-CoV-2 vaccine. Journal of Clinical Neuromuscular Disease 23(4):229–230. https://doi.org/10.1097/cnd.0000000000000411.
Biglia, A., V. Morandi, G. Zanframundo, D. Donati, F. Maggiore, F. Vita, L. Sammarchi, C. Pagani, L. Cavagna, S. Galletti, and C. Montecucco. 2023. Adhesive capsulitis after COVID-19 vaccine injection: A peculiar case treated with combined bursa distention and glenohumeral capsular hydrodilatation. Journal of Ultrasound 26(4):909–911. https://doi.org/10.1007/s40477-022-00739-3.
Blumstein, G. I., and H. Kreithen. 1966. Peripheral neuropathy following tetanus toxoid administration. JAMA 198(9):1030–1031. Bodor, M., and E. Montalvo. 2007. Vaccination-related shoulder dysfunction. Vaccine 25(4):585–587. https://doi.org/10.1016/j.vaccine.2006.08.034.
Brennan, M. B., and J. L. Hsu. 2012. Septic arthritis in the native joint. Current Infectious Disease Reports 14(5):558–565. https://doi.org/10.1007/s11908-012-0285-1.
___________________
6 An IOM committee concluded that “the evidence is inadequate to accept or reject a causal relationship between the injection of a vaccine and CRPS” (IOM, 2012).
Cagle, P. J., Jr. 2021. Shoulder injury after vaccination: A systematic review. Brazilian Journal of Orthopedics 56(3):299–306. https://doi.org/10.1055/s-0040-1719086.
Cantarelli Rodrigues, T., P. F. Hidalgo, A. Y. Skaf, and A. Serfaty. 2021. Subacromial-subdeltoid bursitis following COVID-19 vaccination: A case of shoulder injury related to vaccine administration (SIRVA). Skeletal Radiology 50(11):2293–2297. https://doi.org/10.1007/s00256-021-03803-x.
Choi, Y.-H., and D. H. Kim. 2020. Correlations between clinical features and MRI findings in early adhesive capsulitis of the shoulder: A retrospective observational study. BMC Musculoskeletal Disorders 21:1–9.
Chow, J.C.K., S. L. Koles, and A. J. Bois. 2022. Shoulder injury related to SARS-CoV-2 vaccine administration. Canadian Medical Association Journal 194(2):E46–E49. https://doi.org/10.1503/cmaj.211162.
Chu, E. C.-P. 2022. Shoulder injury related to vaccine administration (SIRVA) in 16 patients following COVID-19 vaccination who presented to chiropractic, orthopedic, and physiotherapy clinics in Hong Kong during 2021. Medical Science Monitor 28:e937430. https://doi.org/10.12659/msm.937430.
Chua, M. M. J., M. T. Hayes, and R. Cosgrove. 2022. Parsonage-Turner syndrome following COVID-19 vaccination and review of the literature. Surgical Neurology International 13:152. https://doi.org/10.25259/sni_4_2022.
Chuaychoosakoon, C., and P. Boonsri. 2023. Partial infraspinatus tear with bursitis following an mRNA vaccination: A case report. Annals of Medicine and Surgery 85(5):2159–2161. https://doi.org/10.1097/ms9.0000000000000655.
Chuaychoosakoon, C., W. Parinyakhup, P. Tanutit, K. Maliwankul, and P. Klabklay. 2021. Shoulder injury related to Sinovac COVID-19 vaccine: A case report. Annals of Medicine and Surgery 68:102622. https://doi.org/10.1016/j.amsu.2021.102622.
Coffman, J. R., A. C. Randolph, and J. S. Somerson. 2021. Parsonage-Turner syndrome after SARS-CoV-2 BNT162b2 vaccine: A case report. JBJS Case Connector 11(3). https://doi.org/e21.0037010.2106/jbjs.Cc.21.00370.
Cook, I. F. 2011. An evidence based protocol for the prevention of upper arm injury related to vaccine administration (UAIRVA). Human Vaccines & Immunotherapeutics 7(8):845–848. https://doi.org/10.4161/hv.7.8.16271.
Cook, I. F. 2014. Subdeltoid/subacromial bursitis associated with influenza vaccination. Human Vaccines & Immunotherapeutics 10(3):605–606. https://doi.org/10.4161/hv.27232.
Cross, G. B., J. Moghaddas, J. Buttery, S. Ayoub, and T. M. Korman. 2016. Don’t aim too high: Avoiding shoulder injury related to vaccine administration. Australian Family Physician 45(5):303–306.
Darnley, J. E., J. A. Rosenbaum, G. L. Jones, and J. Y. Bishop. 2019. Septic arthritis of the glenohumeral joint following influenza vaccination: Case report and review of the literature. Current Orthopaedic Practice 30(5):495–497.
de Mos, M., A. G. de Bruijn, F. J. Huygen, J. P. Dieleman, B. H. Stricker, and M. C. Sturkenboom. 2007. The incidence of complex regional pain syndrome: A population-based study. Pain 129(1–2):12–20. https://doi.org/10.1016/j.pain.2006.09.008.
Doppen, M., M. Black, I. Braithwaite, J. Bong, A. Eathorne, L. Kirton, S. Kung, M. Walton, T. Hills, M. Weatherall, R. Beasley, and C. Kearns. 2023. Skin-to-deltoid-muscle distance at three recommended sites for intramuscular vaccination in a population with obesity: An observational study. New Zealand Medical Journal 136(1573):67–76.
Elsharydah, A., N. H. Loo, A. Minhajuddin, and E. S. Kandil. 2017. Complex regional pain syndrome type 1 predictors—epidemiological perspective from a national database analysis. Journal of Clinical Anesthesia 39:34–37. https://doi.org/10.1016/j.jclinane.2017.03.027.
Erickson, B. J., E. F. DiCarlo, B. Brause, L. Callahan, and J. Hannafin. 2019. Lytic lesion in the proximal humerus after a flu shot: A case report. JBJS Case Connector 9(3):e0248.
Favero, M., F. Schiavon, L. Riato, V. Carraro, and L. Punzi. 2008. Rheumatoid arthritis is the major risk factor for septic arthritis in rheumatological settings. Autoimmunity Reviews 8(1):59–61. https://doi.org/10.1016/j.autrev.2008.07.018.
Flikkema, K., and K. Brossy. 2021. Parsonage-Turner syndrome after COVID-19 vaccination: A case report. JBJS Case Connector 11(4). https://doi.org/e21.0057710.2106/jbjs.Cc.21.00577.
Flores, C., W.S. Choate, and R. Tupler. 2022. Shoulder injury related to vaccine administration. Ochsner Journal 22(3). https://doi.org/doi.org/10.31486/toj.21.0114.
Floyd, M. W., B. M. Boyce, R. M. Castellan, and E. B. McDonough. 2012. Pseudoseptic arthritis of the shoulder following pneumococcal vaccination. Orthopedics 35(1):e101–e103.
Fransz, D. P., C. P. Schönhuth, T. J. Postma, and B. J. van Royen. 2014. Parsonage-Turner syndrome following post-exposure prophylaxis. BMC Musculoskeletal Disorders 15(1):265. https://doi.org/10.1186/1471-2474-15-265.
Ghosh, S., S. K. Pandey, A. Biswas, and J. Pandey. 2023. Adhesive capsulitis after COVID-19 vaccination: A case series. American Journal of Physical Medicine and Rehabilitation 102(6):e79–e82. https://doi.org/10.1097/phm.0000000000002194.
Hand, C., K. Clipsham, J. L. Rees, and A. J. Carr. 2008. Long-term outcome of frozen shoulder. Journal of Shoulder and Elbow Surgery 17(2):231–236. https://doi.org/10.1016/j.jse.2007.05.009.
Harden, N. R., S. Bruehl, R. Perez, F. Birklein, J. Marinus, C. Maihofner, T. Lubenow, A. Buvanendran, S. Mackey, J. Graciosa, M. Mogilevski, C. Ramsden, M. Chont, and J.-J. Vatine. 2010. Validation of proposed diagnostic criteria (the “Budapest criteria”) for complex regional pain syndrome. Pain 150(2):268–274. https://doi.org/10.1016/j.pain.2010.04.030.
Harden, R. N., S. Bruehl, M. Stanton-Hicks, and P. R. Wilson. 2007. Proposed new diagnostic criteria for complex regional pain syndrome. Pain Medicine 8(4):326–331. https://doi.org/10.1111/j.1526-4637.2006.00169.x.
Hesse, E. M., S. Atanasoff, B. F. Hibbs, O. J. Adegoke, C. Ng, P. Marquez, M. Osborn, J. R. Su, P. L. Moro, T. Shimabukuro, and N. Nair. 2020. Shoulder injury related to vaccine administration (SIRVA): Petitioner claims to the National Vaccine Injury Compensation Program, 2010–2016. Vaccine 38(5):1076–1083. https://doi.org/10.1016/j.vaccine.2019.11.032.
Hirsiger, J. R., G. Tamborrini, D. Harder, G. R. Bantug, G. Hoenger, M. Recher, C. Marx, Q.-Z. Li, I. Martin, C. Hess, A. Scherberich, T. Daikeler, and C. T. Berger. 2021. Chronic inflammation and extracellular matrix-specific autoimmunity following inadvertent periarticular influenza vaccination. Journal of Autoimmunity 124:102714. https://doi.org/10.1016/j.jaut.2021.102714.
Holmes, R., K. Armon, and P. Bale. 2019. P39 physiotherapy management of long thoracic nerve injury (LTNI) post-flu vaccine in an immunocompromised patient with vasculitis: What is the best strategy? Rheumatology 58(Suppl 4):kez416.006.
Honarmand, A. R., J. Mackey, and R. Hayeri. 2021. Shoulder injury related to vaccine administration (SIRVA) following mRNA COVID-19 vaccination: Report of 2 cases of subacromial-subdeltoid bursitis. Radiology Case Reports 16(12):3631–3634. https://doi.org/https://doi.org/10.1016/j.radcr.2021.08.019.
HRSA (Health Resources and Services Administration). 2023. Vaccine injury table. Health Resources and Services Administration. Huang, Y.-P., C.-Y. Fann, Y.-H. Chiu, M.-F. Yen, L.-S. Chen, H.-H. Chen, and S.-L. Pan. 2013. Association of diabetes mellitus with the risk of developing adhesive capsulitis of the shoulder: A longitudinal population-based followup study. Arthritis Care & Research 65(7):1197–1202. https://doi.org/10.1002/acr.21938.
Imran, M., and D. Hayley. 2013. Injection-induced axillary nerve injury after a drive-through flu shot. Clinical Geriatrics 21(12).
IOM (Institute of Medicine). 1994. Adverse events associated with childhood vaccines: Evidence bearing on causality. Edited by K. R. Stratton, C. J. Howe, and R. B. Johnston, Jr. Washington, DC: National Academy Press.
IOM. 2012. Adverse effects of vaccines: Evidence and causality. Edited by K. Stratton, A. Ford, E. Rusch, and E. W. Clayton. Washington, DC: The National Academies Press.
Jenkins, M., D. Rupp, and L. J. Goebel. 2020. Post-influenza vaccine subdeltoid bursitis. Cureus 12(10).
Jeong, J., D.-C. Shin, T.-H. Kim, and K. Kim. 2017. Prevalence of asymptomatic rotator cuff tear and their related factors in the Korean population. Journal of Shoulder and Elbow Surgery 26(1):30–35. https://doi.org/10.1016/j.jse.2016.05.003.
Jiang, J. J., H. I. Piponov, D. P. Mass, J. G. Angeles, and L. L. Shi. 2017. Septic arthritis of the shoulder: A comparison of treatment methods. Journal of the American Academy of Orthopaedic Surgeons 25(8):e175–e184. https://doi.org/10.5435/JAAOS-D-16-00103.
Kang, J., and J.-Y. Cho. 2022. Diaphragmatic dysfunction due to neuralgic amyotrophy after SARS-CoV-2 vaccination: A case report. Journal of Korean Medical Science 37(38):e283. https://doi.org/10.3346/jkms.2022.37.e283.
Kashkosh, A., C. M. Peake, A. A. Narvani, and M. Imam. 2023. Spontaneous avascular necrosis of the humeral head following COVID-19 vaccination. Archives of Bone and Joint Surgery 11(2):140.
Kawagere, E., and T. Goldberg. 2022. Shoulder injury related to vaccine administration (SIRVA). Journal of General Internal Medicine 37. https://doi.org/covidwho-1995707.
Kessler, A., M. Yoo, and R. Calisoff. 2020. Complex regional pain syndrome: An updated comprehensive review. NeuroRehabilitation 47(3):253–264.
Kim, D. H., Y. S. Kim, B.-S. Kim, D. H. Sung, K.-S. Song, and C.-H. Cho. 2020. Is frozen shoulder completely resolved at 2 years after the onset of disease? Journal of Orthopaedic Science 25(2):224–228.
Kim, J. G., S. Y. Kim, H. S. Oh, and D. H. Jo. 2021. Parsonage-Turner syndrome following typhoid vaccination. Yonsei Medical Journal 62(9):868–871. https://doi.org/10.3349/ymj.2021.62.9.868.
Kingston, K., E. J. Curry, J. W. Galvin, and X. Li. 2018. Shoulder adhesive capsulitis: Epidemiology and predictors of surgery. Journal of Shoulder and Elbow Surgery 27(8):1437–1443.
Klabklay, P., P. Boonsri, P. Kanyakool, and C. Chuaychoosakoon. 2022. A COVID-19 vaccination precipitating symptomatic calcific tendinitis: A case report. Annals of Medicine and Surgery 74:103347. https://doi.org/https://doi.org/10.1016/j.amsu.2022.103347.
Koh, J. S., Y. Goh, B. Y.-Q. Tan, A. C.-F. Hui, R. H. M. Hoe, A. Makmur, P. L. Kei, J. Vijayan, K. W. P. Ng, A. M. L. Quek, and U. Thirugnanm. 2021. Neuralgic amyotrophy following COVID-19 mRNA vaccination. QJM: An International Journal of Medicine 114(7):503–505. https://doi.org/10.1093/qjmed/hcab216.
Kowatari, R., H. Sasaki, K. Murata, K. Sato, K. Sagawa, M. Kudo, and M. Minakawa. 2023. Establishment of prediction equations for subcutaneous tissue thickness in two representative intramuscular deltoid injections. Vaccine X 14:100316. https://doi.org/10.1016/j.jvacx.2023.100316.
Kuether, G., B. Dietrich, T. Smith, C. Peter, and S. Gruessner. 2011. Atraumatic osteonecrosis of the humeral head after influenza A-(H1N1) V-2009 vaccination. Vaccine 29(40):6830–6833.
Kuhn, J. E. 2023. Prevalence, natural history, and nonoperative treatment of rotator cuff disease. Operative Techniques in Sports Medicine 31(1). https://doi.org/ARTN15097810.1016/j.otsm.2023.150978.
Kunutsor, S. K., M. R. Whitehouse, A. W. Blom, A. D. Beswick, and INFORM Team. 2016. Patient-related risk factors for periprosthetic joint infection after total joint arthroplasty: A systematic review and meta-analysis. PLoS One 11(3):e0150866. https://doi.org/10.1371/journal.pone.0150866.
Lenz, M., N. Üçeyler, J. Frettlöh, O. Höffken, E. K. Krumova, S. Lissek, A. Reinersmann, C. Sommer, P. Stude, A. M. WaagaGasser, M. Tegenthoff, and C. Maier. 2013. Local cytokine changes in complex regional pain syndrome type I (CRPS I) resolve after 6 months. Pain 154(10):2142–2149. https://doi.org/10.1016/j.pain.2013.06.039.
Leopold, S. S. 2022. Editor’s spotlight/take 5: Discussing two systematic reviews with opposing conclusions on shoulder pain after vaccine administration. Clinical Orthopaedics and Related Research 480(7):1234–1240. https://doi.org/10.1097/CORR.0000000000002259.
Levin, J., A. R. Siddiqi, and H. Kim. 2021. Capsular distention for adhesive capsulitis in a pediatric patient with acute flaccid myelitis: A case report. Journal of Pediatric Rehabilitation Medicine 14(1):37–40. https://doi.org/10.3233/prm-190640.
Lindgren, B., D. Rivers, and J. Clark. 2019. Bilateral Parsonage-Turner syndrome after initial unilateral presentation: A case report. Cureus 11(12):e6422. https://doi.org/10.7759/cureus.6422.
Littrell, L. A., D. F. Leslie, D. M. Bierle, and D. E. Wenger. 2020. Progressive monoarticular inflammatory arthritis following influenza vaccination. Mayo Clinic Proceedings: Innovations, Quality & Outcomes 5(1):204–209.
Mackenzie, L. J., M. A. Bushell, P. Newman, and J. A. Bousie. 2022. Shoulder injury related to vaccine administration (SIRVA): What do we know about its incidence and impact? Exploratory Research in Clinical and Social Pharmacy 8:100183. https://doi.org/10.1016/j.rcsop.2022.100183.
MacMahon, A., S. K. Nayar, and U. Srikumaran. 2022. What do we know about shoulder injury related to vaccine administration? An updated systematic review. Clinical Orthopaedics and Related Research 480(7):1241–1250. https://doi.org/10.1097/Corr.0000000000002181.
Maliwankul, K., P. Boonsri, P. Klabklay, and C. Chuaychoosakoon. 2022. Shoulder injury related to COVID-19 vaccine administration: A case series. Vaccines 10(4):588.
Mardourian, M., K. A. Hao, W. Wiggins, J. Arias, J. J. King, T. W. Wright, and J. O. Wright. 2023. Optimizing needle length and site choice for adult immunization. Vaccine 41(33):4836–4843. https://doi.org/10.1016/j.vaccine.2023.06.031.
Marshall, T., M. Addison, N. W. Crawford, J. P. Buttery, and D. R. Cheng. 2022. Aiming too high: Shoulder injury related to vaccine administration (SIRVA): A case series. Vaccine 40(52):7505–7509. https://doi.org/10.1016/j.vaccine.2022.10.086.
Meirelles, H., and G. R. Motta Filho. 2004. Axillary nerve injury caused by intramuscular injection into the deltoid: Case report. Brazilian Review of Orthopedics 39(10).
Messerschmitt, P. J., F. W. Abdul-Karim, J. P. Iannotti, and R. G. Gobezie. 2012. Progressive osteolysis and surface chondrolysis of the proximal humerus following influenza vaccination. Orthopedics 35(2):e283–e286.
Minagawa, H., N. Yamamoto, H. Abe, M. Fukuda, N. Seki, K. Kikuchi, H. Kijima, and E. Itoi. 2013. Prevalence of symptomatic and asymptomatic rotator cuff tears in the general population: From mass-screening in one village. Journal of Orthopaedics 10(1):8–12. https://doi.org/10.1016/j.jor.2013.01.008.
Moretti, A., A. Palomba, M. Paoletta, S. Liguori, G. Toro, and G. Iolascon. 2021. Complex regional pain syndrome in athletes: Scoping review. Medicina 57(11). https://doi.org/10.3390/medicina57111262.
Moya, D., D. Gómez, P. Patiño, N. N. Altamirano, M. Balzarini, and K. Freitag. 2022. Shoulder injury related to vaccine administration following misplaced SARS-CoV-2 vaccination: A case report and review of literature. Journal of Orthopaedic Case Reports 12(3):100.
Nakajima, K., A. Miyata, S. Kato, Y. Oshima, and S. Tanaka. 2023. Calcific tendinitis of the shoulder induced by an mRNA vaccine for COVID-19: A case report. Modern Rheumatology Case Reports 7(1):211–214. https://doi.org/10.1093/mrcr/rxac006.
Nakajima, Y., K. Mukai, K. Takaoka, T. Hirose, K. Morishita, T. Yamamoto, Y. Yoshida, T. Urai, and T. Nakatani. 2017. Establishing a new appropriate intramuscular injection site in the deltoid muscle. Human Vaccines & Immunotherapeutics 13(9):2123–2129. https://doi.org/10.1080/21645515.2017.1334747.
Naleway, A. L., M. L. Henninger, S. A. Irving, S. Bianca Salas, T. L. Kauffman, B. Crane, K. F. Mittendorf, S. Harsh, C. Elder, and J. Gee. 2023. Epidemiology of upper limb complex regional pain syndrome in a retrospective cohort of persons aged 9–30 years, 2002–2017. Permanente Journal 27(2):75–86. https://doi.org/10.7812/tpp/22.170.
Natanzi, N., F. Hebroni, and M. Bodor. 2020. Teres minor injury related to vaccine administration. Radiology Case Reports 15(5):552–555. https://doi.org/10.1016/j.radcr.2020.02.009.
Okur, G., K. A. Chaney, and L. M. Lomasney. 2014. Magnetic resonance imaging of abnormal shoulder pain following influenza vaccination. Skeletal Radiology 43:1325–1331.
Öncel, A., and E. Coşkun. 2022. Parsonage-Turner syndrome after SARS-CoV-2 vaccination: A case report. Turkish Journal of Physical Medicine and Rehabilitation 68(3):418–421. https://doi.org/10.5606/tftrd.2022.10456.
Ott, S., and C. Maihöfner. 2018. Signs and symptoms in 1,043 patients with complex regional pain syndrome. Pain 19(6):599–611.
Ozawa, K., A. Hineno, T. Kinoshita, S. Ishihara, and S.-I. Ikeda. 2017. Suspected adverse effects after human papillomavirus vaccination: A temporal relationship between vaccine administration and the appearance of symptoms in Japan. Drug Safety 40:1219–1229.
Pearson, M., and S. Bent. 2022. Postvaccination subacromial bursitis. Journal of General Internal Medicine 37(2):467.
Petrakis, N., M. Addison, B. Penak, S. Schrader, J. Mallard, H. J. Clothier, J. P. Buttery, N. W. Crawford, and D. R. Cheng. 2023. Shoulder injury following COVID-19 vaccine administration: A case series and proposed diagnostic algorithm. Expert Review of Vaccines 22(1):299–306. https://doi.org/10.1080/14760584.2023.2189463.
Pettyjohn, E. W., J. R. Clugston, and J. L. Zaremski. 2022. Shoulder injury related to vaccine administration and a growing challenge: A focused review. Current Sports Medicine Reports 21(3):78–83. https://doi.org/10.1249/jsr.0000000000000939.
Phillips, C., A. Constanzo, and I. Fowler, 2017. Complex regional pain syndrome following anthrax vaccine. Pain Medicine 18(3):52. https://doi.org/10.1093.
Quinodoz, A., F. Luthi, S. Revaz, and M. Konzelmann. 2023. Acute myopericarditis and left shoulder capsulitis following second dose of mRNA SARS-CoV-2 Moderna vaccination. BMJ Case Reports 16(6):e254110. https://doi.org/10.1136/bcr-2022-254110.
Reilly, P., I. Macleod, R. Macfarlane, J. Windley, and R. J. Emery. 2006. Dead men and radiologists don’t lie: A review of cadaveric and radiological studies of rotator cuff tear prevalence. Annals of the Royal College of Surgeons of England 88(2):116–121. https://doi.org/10.1308/003588406X94968.
Sahu, D., and G. Shetty. 2022. Frozen shoulder after COVID-19 vaccination. JSES International 6(4):682–685. https://doi.org/10.1016/j.jseint.2022.02.013.
Saleh, Z. M., S. Faruqui, and A. Foad. 2015. Onset of frozen shoulder following pneumococcal and influenza vaccinations. Journal of Chiropractic Medicine 14(4):285–289. https://doi.org/10.1016/j.jcm.2015.05.005.
Salmon, J., M. Geoffroy, J. Eschard, and X. Ohl. 2015. Bone erosion and subacromial bursitis caused by diphtheria-tetanus-poliomyelitis vaccine. Vaccine 33(46):6152–6155.
Sandroni, P., L. M. Benrud-Larson, R. L. McClelland, and P. A. Low. 2003. Complex regional pain syndrome type I: Incidence and prevalence in Olmsted County, a population-based study. Pain 103(1–2):199–207. https://doi.org/10.1016/s0304-3959(03)00065-4.
Shahbaz, M., P. D. Blanc, S. J. Domeracki, and S. Guntur. 2019. Shoulder injury related to vaccine administration (SIRVA): An occupational case report. Workplace Health & Safety 67(10):501–505. https://doi.org/10.1177/2165079919875161.
Shaikh, M. F., T. J. Baqai, and H. Tahir. 2012. Acute brachial neuritis following influenza vaccination. BMJ Case Reports 2012. https://doi.org/10.1136/bcr-2012-007673.
Shaw, F. E., Jr., H. A. Guess, J. M. Roets, F. E. Mohr, P. J. Coleman, E. J. Mandel, R. R. Roehm, Jr., W. S. Talley, and S. C. Hadler. 1989. Effect of anatomic injection site, age and smoking on the immune response to hepatitis B vaccination. Vaccine 7(5):425–430. https://doi.org/10.1016/0264-410x(89)90157-6.
Shields, L. B. E., V. G. Iyer, Y. P. Zhang, J. T. Burger, and C. B. Shields. 2022. Parsonage-Turner syndrome following COVID-19 vaccination: Clinical and electromyographic findings in 6 patients. Case Reports in Neurology 14(1):58–67. https://doi.org/10.1159/000521462.
Sinha, A., and S. Gupta. 2017. Poster 266: Parsonage-Turner syndrome following influenza vaccination: A case report. PM&R 9:S216.
Slette, E., M. Rohrback, and D. V. Ring. 2022. Persistent shoulder pain after vaccine administration is associated with common incidental pathology: A systematic review. Clinical Orthopaedics and Related Research 480(7):1251–1258. https://doi.org/10.1097/Corr.0000000000002191.
Smith, S. S., Y. Lee, and L. Wang. 2020. Adolescent with osteomyelitis after intramuscular administration of a vaccine: A case report. Journal of the American Pharmacists Association 60(6):e357–e360. https://doi.org/https://doi.org/10.1016/j.japh.2020.03.015.
Sukhija, S., S. Singh, S. Saxena, S. Ambwani, and P. S. Khera. 2022. Shoulder injury related to vaccine administration (SIRVA) with COVID-19 vaccination—a case report. Journal of Family Medicine and Primary Care 11(12):7937–7940. https://doi.org/10.4103/jfmpc.jfmpc_798_22.
Sweet, M. C., G. J. Sheena, S. Liu, F. E. Fisk, J. R. Lynch, and S. J. Muh. 2019. Clinical characteristics and long-term outcomes after septic arthritis of the native glenohumeral joint: A 20-year retrospective review. Orthopedics 42(1):e118–e123.
Szari, S., A. Belgard, K. Adams, and J. Freiler. 2019. Shoulder injury related to vaccine administration: A rare reaction. Federal Practitioner 36(8):380–384.
Taylor, B. C., and D. Hinke. 2014. Shoulder injury related to vaccine administration (SIRVA). Applied Radiology 43(12):30–32.
Tempelhof, S., S. Rupp, and R. Seil. 1999. Age-related prevalence of rotator cuff tears in asymptomatic shoulders. Journal of Shoulder and Elbow Surgery 8(4):296–299. https://doi.org/10.1016/s1058-2746(99)90148-9.
Teunis, T., B. Lubberts, B. T. Reilly, and D. Ring. 2014. A systematic review and pooled analysis of the prevalence of rotator cuff disease with increasing age. Journal of Shoulder and Elbow Surgery 23(12):1913–1921. https://doi.org/10.1016/j.jse.2014.08.001.
Thompson, A. R., and E. R. Ensrud. 2020. Bilateral adhesive capsulitis following influenza vaccination: A case report. Clinical Case Reports 8(11):2155–2157. https://doi.org/10.1002/ccr3.3072.
Uchida, S., A. Sakai, and T. Nakamura. 2012. Subacromial bursitis following human papilloma virus vaccine misinjection. Vaccine 31(1):27–30.
van Alfen, N., and B. G. M. van Engelen. 2006. The clinical spectrum of neuralgic amyotrophy in 246 cases. Brain 129(Pt 2):438–450. https://doi.org/10.1093/brain/awh722.
van Alfen, N., J. Schuuring, B. G. van Engelen, J. J. Rotteveel, and F. J. Gabreëls. 2000. Idiopathic neuralgic amyotrophy in children. A distinct phenotype compared to the adult form. Neuropediatrics 31(6):328–332. https://doi.org/10.1055/s-2000-12954.
van Alfen, N., J. J. van Eijk, T. Ennik, S. O. Flynn, I. E. G. Nobacht, J. T. Groothuis, S. Pillen, and F. A. van de Laar. 2015. Incidence of neuralgic amyotrophy (Parsonage-Turner syndrome) in a primary care setting—a prospective cohort study. PLoS One 10(5):e0128361. https://doi.org/10.1371/journal.pone.0128361.
Van Eijk, J.J., J. T. Groothuis, and N. Van Alfen. 2016. Neuralgic amyotrophy: An update on diagnosis, pathophysiology, and treatment. Muscle and Nerve 53(3):337–350. https://doi.org/10.1002/mus.25008.
VanLancker, J., and D. Sheth. 2022. Brachial neuritis from the mRNA SARS-COV-2 and influenza vaccines. Annals of Allergy, Asthma & Immunology 129(5 Suppl):S96–S97. https://doi.org/10.1016/j.anai.2022.08.773.
Vitturi, B. K., M. Grandis, S. Beltramini, A. Orsi, A. Schenone, G. Icardi, and P. Durando. 2021. Parsonage-Turner syndrome following coronavirus disease 2019 immunization with ChAdOx1-S vaccine: A case report and review of the literature. Journal of Medical Case Reports 15(1):589. https://doi.org/10.1186/s13256-021-03176-8.
Wharton, B. R., K. C. Doan, and M. L. Wolcott. 2022. Shoulder injury related to COVID-19 vaccine administration: A case report. JSES Reviews, Reports & Techniques 2(2):178–181.
Wong, W., C. Okafor, E. Belay, C. S. Klifto, and O. Anakwenze. 2021. Arthroscopic surgical management of shoulder secondary to shoulder injury related to vaccine administration (SIRVA): A case report. Journal of Shoulder and Elbow Surgery 30(6):e334–e337.
Wood, C. T., and A. M. Ilyas. 2022. Shoulder injury related to vaccine administration: Diagnosis and management. Journal of Hand Surgery Global Online 4(2):111–117. https://doi.org/10.1016/j.jhsg.2021.12.009.
Wright, A., R. Patel, and D. Motamedi. 2019. Influenza vaccine-related subacromial/subdeltoid bursitis: A case report. Journal of Radiology Case Reports 13(6):24.
Wright, J. O., W. Wiggins, M. S. Smith, J. J. King, and T. W. Wright. 2023. Shoulder pain and dysfunction after vaccination: A systematic review. JBJS Reviews 11(1). https://doi.org/e22.0013410.2106/JBJS.RVW.22.00134.
Yamamoto, A., K. Takagishi, T. Kobayashi, H. Shitara, and T. Osawa. 2011. Factors involved in the presence of symptoms associated with rotator cuff tears: A comparison of asymptomatic and symptomatic rotator cuff tears in the general population. Journal of Shoulder and Elbow Surgery 20(7):1133–1137.
Yuen, W. L. P., Y. J. Loh, and D. B. Wang. 2022. SIRVA (shoulder injury related to vaccine administration) following mRNA COVID-19 vaccination: Case discussion and literature review. Vaccine 40(18):2546–2550.
Zeldin, E. R., D. M. Boyette, and J. W. Norbury. 2023. Shoulder pain after influenza vaccine administration: A clinical vignette. American Journal of Physical Medicine and Rehabilitation 102(10):e141–e143. https://doi.org/10.1097/PHM.0000000000002242.
Zheng, C., J. Duffy, I. A. Liu, L. S. Sy, R. A. Navarro, S. S. Kim, D. S. Ryan, W. Chen, L. Qian, C. Mercado, and S. J. Jacobsen. 2022. Identifying cases of shoulder injury related to vaccine administration (SIRVA) in the United States: Development and validation of a natural language processing method. JMIR Public Health Surveillance 8(5):e30426. https://doi.org/10.2196/30426.























