Catalyzing Innovative Health System Transformation: An Opportunity Agenda for the Center for Medicare & Medicaid Innovation (2025)
Chapter: Appendix D: Case Studies Developed for September 28, 2021, Meeting on Multi-Payer Alignment on Value-Based Care
APPENDIX D
CASE STUDIES DEVELOPED FOR SEPTEMBER 28, 2021, MEETING ON MULTI-PAYER ALIGNMENT ON VALUE-BASED CARE: ARKANSAS’S IMPLEMENTATION OF THE CPC+ MODEL CASE STUDY
PURPOSE OF THE CASE STUDIES
As part of the National Academy of Medicine’s (NAM’s)project on Catalyzing Innovative Health System Transformation, NAM staff developed two case studies to inform the discussion of actionable approaches to Multi-Payer Alignment on Value-Based Care. These cases were selected to provide context on the strategies and tactics presented by two critical stakeholders: states and private payers. The learnings from the state effort, Arkansas’s Implementation of the Coordinated Primary Care Plus (CPC+) Model and from private payer Anthem’s Enhanced Personal Health Care offer insights on the potential for synergistic innovative payment approaches and incentives to drive care delivery transformations.
BACKGROUND
Leveraging CPC to Build a Patient-Centered Care Delivery System
In 2012, two years after the establishment of the Center for Medicare & Medicaid Innovation (CMMI), Arkansas was selected as one of seven regions to participate in the four-year Centers for Medicare & Medicaid Services (CMS) Comprehensive Primary Care (CPC) Initiative (AHCPII, 2019). The Arkansas Health Care
Payment Improvement Initiative (AHCPII) was established to facilitate the triple aim of improving population health; enhancing patient experiences through quality, access, and reliability; and reducing, or at least controlling, the total cost of care (AHCPII, 2019). AHCPII’s implementation mandate was bolstered by a 2013 CMS State Innovation Model Testing grant, which awarded Arkansas $42 million in federal funds. The funds were used to foster collaboration between private and public payers and the state to operationalize the development and expansion of patient-centered medical homes (PCMHs) as the main delivery mechanism of primary care (AHCPII, 2019).
Considering the widespread adoption of CPC by payers such as Blue Cross Blue Shield, and employers, including Walmart and Arkansas public schools, the Arkansas Insurance Department released rules in 2015 mandating PCMH participation as a condition for participation in the insurance marketplace (Chernew et al., 2015). Notable impacts on CPC practice outcomes were a 15.7% reduction in hospitalizations in 2015 and net savings of $12.5 million, or $20.95 per beneficiary per month in 2016 (CMS, 2016).
Transition to CPC+
In 2016, Arkansas was selected by CMS as one of 14 regions to participate in CPC+, an updated program that provided additional enhancements in care delivery and quality measurements (ACHI, 2017). Arkansas began implementing CPC+ in 2017 and extended Medicare participation in PCMH to 182 primary care practices, compared to only 58 practices in CPC (CMS, 2016). While practices are not required to be PCMH certified to participate in CPC+, CPC+’s requirements of 24/7 access to care, its triaging of patients into dedicated patient care teams, and the provision of care delivery options outside of traditional office visits may align with PCMH certification criteria (ACP, 2017). The five-year pilot program involved major payers such as AR Blue Cross Blue Shield, AR Health and Wellness Solutions, AR Medicaid, AR Superior Select, HealthSCOPE Benefits, and QualChoice (ACHI, 2017).
APPROACH TO IMPLEMENTING MULTI-PAYER ALIGNMENT
Flexible Eligibility
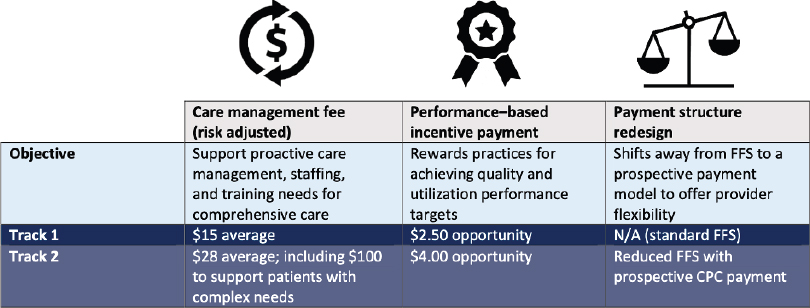
Two CPC+ practice eligibility criteria, Track 1 and Track 2, were established at the program’s inception (ACHI, 2017). Track 1 practices meet substantially fewer requirements than Track 2: they “must have at least 150 Medicare beneficiaries, use a certified electronic health record, assign patients to a provider panel, support quality improvement activities, and provide 24/7 access for patients” (ACHI, 2017). Track 2 practices must meet all Track 1 requirements along with the additional requirements of “developing and recording care plans, following up with patients after emergency department (ED) or hospital discharge, linking patients to community-based resources, and providing letters of support from health IT vendors outlining vendor commitments to care optimization” (ACHI, 2017).
Innovations in Care Quality, Safety, and Standards
To leverage the infrastructure implemented as part of the PCMH program, Arkansas set minimum standards for care coordination and practice transformation for all practices participating in CPC+ to receive a per-beneficiary per-month (PBPM) medical home support payment. To receive PBPM payments, practices and providers must demonstrate:
- Access and Continuity: For Track 1 CPC+ practices, “provide patients with 24/7 access to care and assign patient care teams”; Track 2 should “provide care delivery options outside of traditional office visits.”
- Care Management: For both Track 1 and Track 2 practices, identify high-need patients through risk stratification to provide targeted case management, including ED and hospital visit follow-up care.
- Comprehensiveness and Coordination: Track 1 practices should “manage primary care, behavioral health, and any
- health-related social or specialty care across the system,” including identifying specialists for referrals. Data points that were collected include patient admission, discharge, and transfers from EDs and hospitals. Track 2 practices should perform all of the above, as well as psychosocial needs assessments.
- Patient and Caregiver Engagement: Track 1 practices should “conduct annual Patient and Family Advisory Council (PFAC) meetings,” while Track 2 practices should “conduct PFAC meetings twice a year and provide patients with self-management support.”
- Planned Care and Population Health: Track 1 practices must “review quality and utilization reports from payers quarterly to assess and inform population health management,” while Track 2 should meet weekly to review population-level data.
- Reporting and Health IT Requirements: Providers should “use practice-level health IT to support population health and team-based structure and focus,” including the use of certified electronic health records and electronic clinical quality measures reporting. Track 2 practices should “work with vendors to develop and optimize a set of health IT functions” (ACHI, 2017).
Payment Innovations
Medicare and partner payers in Arkansas pay up-front PBPM care management fees in addition to a PBPM performance-based incentive payment for both Track 1 and Track 2 practices. As part of a payment restructuring away from fee-for-service reimbursements, Arkansas CPC+ provides a prospective payment to support care delivery to patients with complex needs (ACHI, 2017).
Statewide Health Information Exchange
In partnership with Arkansas’s Office of Health Information Technology, AHCPII connected 171 CPC+ clinics to the State Health Alliance for Records Exchange (SHARE) (AHCPII, 2017). The health information exchange (HIE) integrates with electronic
SOURCE: ACHI, 2017.
medical records, virtual health records, and secure messaging access. SHARE also supports sending immunization records to the immunizations registries and connecting to Arkansas’s public reporting registries (AHCPII, 2017).
RESULTS
Participation in Arkansas’s PCMH program and CPC+ is now occurring throughout the state. By 2018, 182 practices, 77 Track 1 and 105 Track 2 clinics, and 689 primary care clinicians were participating in CPC+ across Arkansas, of which 50 practices were enrolled in both PCMH and CPC+, possibly reflecting the alignment of both programs on some quality measures and care delivery eligibility requirements (ACP, 2017; AHCPII, 2017). Combined, these practices serve almost 750,000 patients (AHCPII, 2017).
The model disbursed a substantial amount of funding for Arkansas providers and advanced the adoption of health information technology statewide. For 2017-2018, $90 million in CPC+ payments were made to Arkansas providers, including care management fees, prospective performance-based incentive payments, and comprehensive primary care payments (AHCPII, 2017). Due to the creation of the SHARE health information exchange facilitated by CPC and CPC+ funding, 171 CPC+ clinics are connected to SHARE (AHCPII, 2017). The model also drove engagement and feedback between patients, providers, regional payers, and poli-
cymakers. Finally, the adoption of the model drove collaboration and the sharing of best practices between Arkansas, Oklahoma, and Greater Kansas City CPC+ payers.
Despite these strides, an initial analysis of Arkansas Blue Cross beneficiary claims conducted in 2020 returned inconclusive results for CPC+’s ability to reduce costs and health care expenditures. No significant reductions in per-member per-quarter (PMPQ) savings were recorded for Arkansas CPC+ participants, while an increase of $17.93 PMPQ relative to practices that did not participate was observed. However, a reduction of $7.54 PMPQ for acute care spending and $3.67 PMPQ for ED spending was observed (Milbank Memorial Fund, 2020).
CONCLUSION
The CPC+ model concluded on December 31, 2021, with Arkansas practices then required to join an Accountable Care Organization or the state’s Primary Care First programs in 2022 (AAFP, 2021). Meanwhile, CMS and Mathematica are evaluating the program’s overall impacts in their final 5th year evaluation, to be released in 2023 (Mathematica, 2022).
REFERENCES
American Academy of Family Physicians (AAFP). 2021. CMS Innovation Center to End CPC+ Alternative Payment Model for All Participants This Year. Available at: https://www.aafp.org/journals/fpm/blogs/gettingpaid/entry/cpc_early_end.html (accessed September 9, 2021).
American College of Physicians (ACP). 2017. Eligibility Assessment for Comprehensive Primary Care Plus(CPC+). Available at: https://www.acponline.org/system/files/documents/practice-resources/business-resources/payment/models/other-care/acp_cpc_plus_eligibility_assessment_revised_v3.pdf (accessed September 9, 2021).
Arkansas Center for Health Care Improvement (ACHI). 2017. Comprehensive Primary Care Plus (CPC+). Available at: https://
achi.net/library/cpc-plus-fact-sheet/ (accessed September 9, 2021).
Arkansas Health Care Payment Improvement Initiative (AHCPII). 2019. 4th Annual Statewide Tracking Report. Available at: https://achi.net/wp-content/uploads/2019/09/ACHI_Statewide_Tracking_Report_2019_4th_Annual.pdf (accessed September 9, 2021).
Centers for Medicare & Medicaid Services (CMS). 2016. Comprehensive Primary Care (CPC) Initiative 2016 Shared Savings & Quality Results. Available at: https://innovation.cms.gov/files/x/cpci-2016sharedsavings-qualitydata.pdf (accessed September 9, 2021).
Chernew, M. E., W. E. Golden, C. H. Mathis, A. M. Fendrick, M. W. Motley, and J. W. Thompson. 2015. The Arkansas Payment Improvement Initiative: Early Perceptions of Multi-Payer Reform in a Fragmented Provider Landscape. The American Journal of Accountable Care 3(2). Available at: https://www.ajmc.com/view/the-arkansas-payment-improvement-initiative-early-perceptions-of-multi--payer-reform-in-a-fragmented-provider-landscape (accessed September 9, 2021).
Mathematica. 2022. Independent Evaluation of Comprehensive Primary Care Plus (CPC+): Fourth Annual Report. https://www.mathematica.org/publications/independent-evaluation-of-the-comprehensive-primary-care-plus-cpc-fourth-annual-report (accessed July 15, 2022)
Milbank Memorial Fund. 2020. Value-Based Primary Care: Insights from a Commercial Insurer in Arkansas. Available at: https://www.milbank.org/publications/value-based-primary-care-insights-from-a-commercial-insurer-in-arkansas/ (accessed September 15, 2021).
MULTI-PAYER ALIGNMENT ON VALUE-BASED CARE: ANTHEM’S ENHANCED PERSONAL HEALTH CARE PROGRAM CASE STUDY
BACKGROUND
Anthem’s Enhanced Personal Health Care (EPHC) program launched in 2013, based on lessons learned and results from the Accountable Care Organization (ACO) and Patient-Centered Medical Homes (PCMHs) pilots. The EPHC program is Anthem’s leading value-based payment program, created to transform primary care practices through collaboration between health plans and providers. EPHC has four types of contract agreements, including the Enhanced Personal Health Care for Primary Care, Freestanding Patient-Centered Care, Enhanced Personal Health Care Essentials, and Comprehensive Primary Care Plus. These agreements include value-based compensation (Anthem, 2020). The EPHC program supports providers by giving them access to incentives, data, tools, and guidance they need to transform the way they deliver health care (Empire, 2018). The EPHC program is designed to accomplish three goals:
- “Support the transformation of care delivery through collaboration with providers with varying experience levels with risk-based contracting;
- Improve patients’ quality and experience of care and their health status and outcomes; and
- Slow the growth of total cost of care to ensure the affordability of high-value coverage” (PCC, 2018).
The program covers primarily commercial lines of business and applies to any provider organization with a foundation in primary care, including ACOs, PCMHs, Independent Physician Associations, Integrated Delivery Networks, small and independent Primary Care Providers (PCPs), and hospitals (PCC, 2018).
Within the first year of EPHC’s launch, 11% of payments made by Anthem to providers were value-based. A year later, the value-based payments jumped from 11% to 40% (Anthem Public Policy Institute, 2016). Anthem health plans have connected 50%
of commercial plans to quality using a variety of compensation methodologies. Furthermore, after three years of operation, the EPHC program grew to 54,000 providers caring for 4.6 million members. The EPHC program is currently in 14 states, including California, Colorado, New Hampshire, New York, Ohio, Virginia, Connecticut, Georgia, Maine, Missouri, Nevada, Wisconsin, Indiana, and Kentucky (Anthem Public Policy Institute, 2016).
PAYMENT MODEL
The EPHC program has the following payments models in place:
- Shared Savings. This model is built on standards from organizations such as the National Committee for Quality Assurance, the Healthcare Effectiveness Data and Information Set, the American Diabetes Association, and the American Academy of Pediatrics. Additionally, the model includes preventive care, acute and chronic care, and health care utilization measures. The shared savings are earned based on the provider’s performance. Anthem also monitors the engagement rates of its members.
- Care Coordinated Payments. Anthem reimburses its providers for several clinical interventions that do not have a current procedural terminology code and occur outside transitional offices. These interventions include “care planning, maintaining health registries, improving access, and following up with patients by phone or email.”
- Shared Risk. Providers such as ACOs are generally willing to take on more risk and accountability for quality and cost of care. They are also accountable for transitioning from aligned care management to collaborative care management. Under the collaborative model, they are responsible for care planning and management with Anthem’s help. They also participate in data sharing, which allows for the creation of a single patient record (PCC, 2018).
IMPLEMENTATION
The EPHC provides a framework and a set of principles that guide Anthem’s engagement with all provider organizations.
Anthem’s strategy to move away from fee-for-service to value-based payment models is realized by concentrating on a patient-centered model that strives to be proactive, holistic, efficient, and focused on a patient’s health and well-being. The core principles of the EPHC include:
- “Risk-stratified care management,
- Coordination of care across the continuum,
- Shared decision-making and accountability between physicians and their patients/caregivers,
- Ensured access,
- Promotion of wellness and prevention, and
- Measuring and monitoring compliance with evidence-based guidelines” (PCC, 2018).
Providers participating in the EPHC program receive meaningful and actionable clinical data through a web-based application. This application allows providers to identify patients that need additional attention or interventions. Data such as inpatient census information, predictions on readmissions, and emergency department visits are updated daily. Data such as care gaps that identify missing recommended preventive care services or risk stratification are updated monthly. EPHC providers also share savings if attributed members have a lower cost of care than projected and maintain the quality of care for 12 months (Anthem Public Policy Institute, 2016). Quality of care is determined through measures endorsed by the National Quality Forum and the Centers for Medicare & Medicaid Services, and metrics adopted from renowned specialty societies. Over time, the number of required quality measures have decreased. The quality metrics included in the EPHC program are:
- “Preventive care, including cancer screening, childhood immunization, and well child visits, and
- Acute and chronic care, including diabetes-related measures such as hemoglobin A1C (Hba1c) and lipid profile testing, and monitoring persistent medication” (PCC, 2018).
As a condition of participating in the program, EPHC providers also agree to:
- “Provide 24/7 access to members through extended hours or after-hours call coverage.
- Have a dedicated position within their practices that support participation in the EPHC and practice transformation.
- Participate regularly in collaborative learning sessions and use support tools, such as hot-spotting reports to identify gaps in care.
- Use a disease registry to manage care for patients with certain chronic conditions and engage in care planning for the high-risk population.
- Use generic prescription drugs when clinically appropriate.
- Engage in quality and performance measurement and meet appropriate performance standards on nationally endorsed quality measures” (Anthem Public Policy Institute, 2016).
RESULTS
An analysis from the first year of the program included “744,000 members in Anthem plans attributed to 7,974 providers from 422 participating EPHC practices” (Anthem Public Policy Institute, 2016). The analysis found:
- “Gross medical savings of $9.51 per attributed member per month for members who saw EPHC providers compared to members who did not, representing a 3.3% reduction in medical costs.
- 7.8% fewer acute inpatient admissions compared to the control group.
- 3.5% decrease in ER costs and a 1.6% decrease in ER utilization.
- 5.1% per attributed member per month decrease in outpatient surgery costs.
- 7.4% decrease in acute admissions for high-risk patients with chronic conditions.
- An increase of 22.9 per 1000 PCP visits for high-risk patients, implying increased utilization of proactive health management” (Anthem Public Policy Institute, 2016).
Of note, most of the savings were derived from the ACOs. In a separate analysis, EPHC providers outperformed their non-
participating peers in multiple quality categories, indicating a consistent provision of evidence-based care and preventive care. Also, surveys taken by patients seeing an EPHC provider showed improved consumer satisfaction with access to care and enhanced consumer experience (Anthem Public Policy Institute, 2016).
CONCLUSION
While there is an increasing trend in moving away from fee-for-service to value-based payment model development and implementation, there are still gaps in understanding or defining the best value-based payment model and a successful program. Programs such as the EPHC help fill the research and evaluation gaps and help to highlight design and program features essential for successful value-based payment programs (Anthem Public Policy Institute, 2016).
Additionally, an initial analysis of the EPHC showed that collaborations with payers and providers are crucial to success. Value-based payment must be successfully implemented with a range of providers, ensuring improved patient experience and quality. Finally, ongoing testing of payment and delivery reforms will need to consider the complexity of evaluations. As policymakers move toward value-based payment programs, EPHC should be examined for lessons learned to inform the development and implementation of future models (Anthem Public Policy Institute, 2016). Anthem’s recommendations for CMS as the entity that designs and revises models include:
- Concentrate not only on increasing participation but also on retention in value-based payments. Ensuring contracting options are flexible and have a wide range of providers will be critical to success.
- Investigate and evaluate successful private sector value-based payment programs to define alternative payment model parameters in Medicare and other programs. Encourage providers to develop partnerships with health plans to facilitate their participation in value-based payments (Anthem Public Policy Institute, 2016).
REFERENCES
Anthem Blue Cross Blue Shield (Anthem). 2020. Enhanced Personal Health Care. Available at: https://www.unicare.com/wps/portal/ahpprovider?content_path=provider/va/f1/s0/t0/pw_e185959.htm&state=va&rootLevel=3&label=Enhanced%20Personal%20Health%20Care (accessed September 15, 2021).
Anthem Public Policy Institute. 2016. Early Results from the Enhanced Personal Health Care Program: Learnings from the Movement Towards Value-Based Payments. Available at: https://www.anthempublicpolicyinstitute.com/userFiles/uploads/02/2_Report_Early-Results-from-the-Enhanced-Personal-Health-Care-Program.pdf (accessed September 9, 2021).
Empire Blue Cross Blue Shield (Empire). 2018. Driving Better Outcomes Through Proactive Care Coordination: Tidewater Physicians Multispecialty Group. Available at: https://www.empireblue.com/docs/public/inline/NY_EPHC_0001.pdf (accessed September 15, 2021).
Primary Care Collaborative (PCC). 2018. Anthem – Enhanced Personal Health Care. Available at: https://www.pcpcc.org/initiative/anthem-enhanced-personal-health-care (accessed September 9, 2021).
This page intentionally left blank.













