Developing an Agenda for Population Aging and Social Research in Low- and Middle-Income Countries (LMICs): Proceedings of a Workshop (2024)
Chapter: 5 The Role of Family
5
The Role of Family
The fourth session of the workshop was moderated by Emily Agree (Johns Hopkins University, workshop planning committee member) and focused on how family changes might affect the health and well-being of older populations in low- and middle-income countries (LMICs). Specifically, presenters had been asked to consider how changes in household composition, family size, and time to marriage affect the health of older populations.
CARE OF OLDER ADULTS IN LATIN AMERICA
There are three trends in the care environment in Latin American countries, said Pablo Ibarrarán (Inter-American Development Bank [IDB]). First, there is a strong reliance on family care. This is in part because of cultural reasons and in part out of necessity because of a lack of formal care systems. A huge majority of care—around 90%—is done within families, and mostly by women in the family. The second trend, he said, is that the number of older people is increasing because of birth patterns and longer life expectancy. In addition, a higher proportion of older adults are needing care because of the prevalence of chronic diseases that are associated with functional dependency. Third, changes in family size and composition mean that the supply of traditional caregivers is decreasing. A trend toward smaller families and women working in the formal labor market mean that there are fewer available caregivers at the same time that there is an increase in the demand for care.
Professional care is very uncommon in Latin American countries. Only about 0.5% of older people in the region live in long-term institutions, and around 80% of older people being cared for at home are cared for by family members. While data on care are lacking in many countries, said Ibarrarán, data from Argentina show that only 3% of people receiving care at home receive care from someone who is professionally trained. Between two-thirds and three-quarters of care in the home is provided by women. Many women are combining paid work and care work, which has both economic and health consequences. For example, if a woman reduces her paid work in order to care for a family member, she is reducing her potential social security or pension. This has “long-lasting impacts,” said Ibarrarán.
Care needs are increasing in Latin America, with about 14.4% of people over 65 being care dependent. With expected demographic changes, the number of people who need care is projected to triple by 2050: see Figure 5-1. This is a conservative estimate, Ibarrarán said, because it assumes the same rate of dependency as today. While care needs are increasing, he reiterated, the supply of caregivers is shrinking. Lower fertility rates, coupled with national and international migration patterns, mean that families are smaller and older people are more likely to live alone. These trends put the traditional care model, which the region has relied on for years, under stress.
These patterns—an increase in care needs and a decrease in the supply of caregivers—have resulted in conversations about how policies might be able to address the situation, said Ibarrarán. Many people are currently not receiving the care they need; around 20% of older people report that they need help to perform basic activities of daily living but are not receiving care. The situation is not a “viable equilibrium,” he said. These challenges
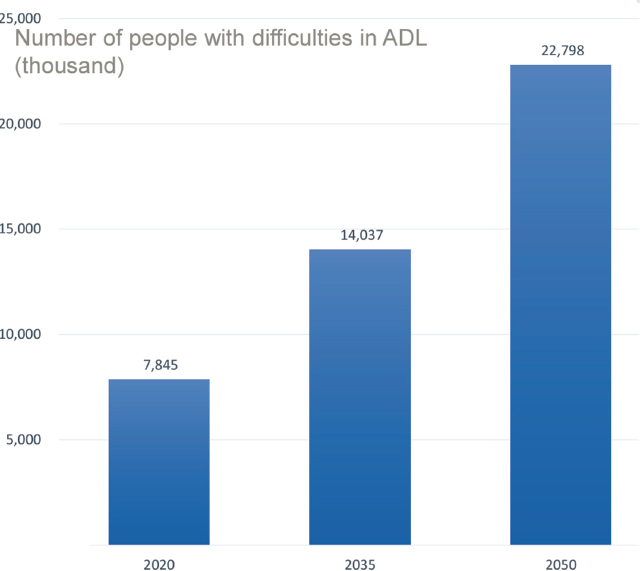
SOURCE: Workshop presentation by Pablo Ibarrarán. Adapted from data in Aranco et al. (2022).
can only be overcome if the data needed to understand the specific needs and characteristics of countries and regions are available to design policies based on these needs. There is huge variation both within and across countries in terms of the supply and demand for care.
Unfortunately, current data sources are “very scarce and very heterogeneous,” said Ibarrarán. There are two main data sources in the region that are relevant to aging and caregiving: surveys on health and aging and time-use surveys. Health and aging surveys include information about level of dependence, care arrangements, and basic caregiver characteristics. However, the data about caregivers are sparse, with no information about training or experience. The time-use surveys provide information about time spent by individuals in paid and unpaid work, time spent caring for others, and caregiver characteristics. Other data sources in the region include disability surveys, household surveys, and a recent Generations and Gender Survey in Uruguay1 that looks at cultural changes regarding family and gender representations.
___________________
1 https://ggp.colectica.org/item/int.ggp/e173d029-c667-43cc-8f51-83f8d3897c59/
While these surveys and studies are an excellent source of some data, policy making requires “much more precise information,” said Ibarrarán. One challenge is a lack of consistency to enable comparison across countries. Data on labor force participation and poverty tend to be fairly consistent, but there is a lot of variation on measures of functional dependency. There are differences in the populations considered, the number and type of activities considered, the type and range of possible answers, and the wording used. There is a need to standardize and harmonize these tools so that the data can be compared within and across countries. Moreover, there are few countries that conduct multiple rounds of data collection. Mexico is an exception to this rule; the Estudio Nacional de Salud y Envejecimiento en México—National Survey of Health and Nutrition, in English—is an excellent source of quality data. Ibarrarán said that while surveys like this require a “considerable investment,” it is a sound investment given their potential to inform policy making.
Ibarrarán described the efforts of IDB to increase knowledge about paid and unpaid caregivers in Latin America. Currently, little is known about paid caregivers because many care arrangements tend to be informal, with untrained caregivers. There are some countries, such as Costa Rica, with more developed formal caregiving markets. However, most caregiving in the region is provided by women in their mid-40s or 50s with low levels of education; only about one-third pay social security contributions. Labor force surveys provide some information in this area, but there are issues of capturing different types of care work and categorization (e.g., caregivers may be mixed in with those who do household work). IDB is trying to fill these gaps by carrying out a regional survey on around 330 unpaid caregivers and 550 paid caregivers who work in both homes and institutions. Six countries are participating. There are plans to extend to other countries and to conduct a longitudinal survey of paid care workers in the home setting.
Ibarrarán closed by stating that “We need to understand more so we can promote better policies.” He offered several questions that are priority areas for future research:
- How has the gender division of care responsibilities evolved?
- How do care strategies affect the quality of life of dependent persons?
- How do care strategies affect the quality of life of family caregivers?
- What are the working conditions of paid care workers and how do they affect their quality of life and the care provided?
“I am convinced that the region can have a much better future for older persons,” said Ibarrarán. There is an increasing awareness in governments of the importance of a society in which older people and their families have
a good quality of life, with access to strong social protection networks that include long-term care services for all of those who need it. To reach this goal, one of the first steps is to gain a better understanding of the current conditions and to invest in data in order to evaluate and demonstrate the most efficient and most advantageous policies that can be implemented.
INTERGENERATIONAL TIES IN CHINA
China is similar to the rest of the world in that the population is aging, said Feinian Chen (Johns Hopkins University). However, the rate at which the population of older adults is rising is quite high in comparison with other nations: see Figure 5-2. China has a huge population, second only to India, so the 30% of the population that will be over 65 by the year 2050 translates to 360 million people. This rapid acceleration of the older population is “no surprise,” said Chen, given the combination of the decrease in fertility and the increase in life expectancy in recent decades in the country.
Another major trend in China is a decline in family size and changes in family structure, said Chen. In 2020, the average family household was 2.61 individuals, compared with a high of 4.43 in 1964: see Figure 5-3. The decrease of household size coincides with a significant rise in one-generation households, although two- and multiple-generation households remain the most prevalent living arrangement among Chinese older adults as of 2018: see Figure 5-4. There has been massive internal migration in China over the last several decades, resulting in an increasing number of “skipped-generation households”: households in which working-age adults leave their parents and children behind.
In China, “filial piety is considered the cornerstone of the old-age family support system,” said Chen. The question, she said, is whether these recent trends in longevity, family size, and family structure will have a negative impact on family support and older adults’ health and well-being. Chen shared her own research journey on the topic of living arrangements and intergenerational ties, which spanned from 2001 to 2023. The data for her research have come from four main sources: the China Health and Nutrition Survey, the Chinese Longitudinal Healthy Longevity Study, the China Health and Retirement Longitudinal Survey, and the China Longitudinal Aging Social Survey.
Evidence from these sources on the impact of living arrangements on health is mixed, said Chen. For example, a 2008 study found that living in a traditional extended household promotes subjective well-being. Results actually demonstrated that living with a daughter instead of a son improved well-being, in contradiction of the culturally preferred arrangement. In contrast, however, a 2018 study found that living in a multigenerational household offered limited health benefits to rural older adults, as measured
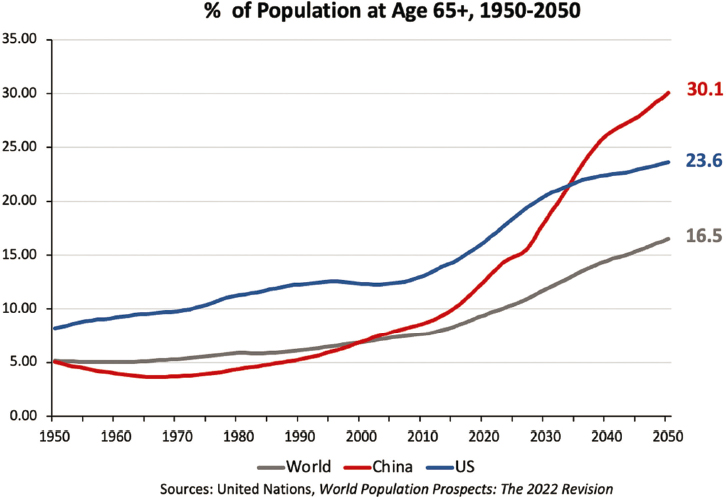
SOURCE: Workshop presentation by Feinian Chen.
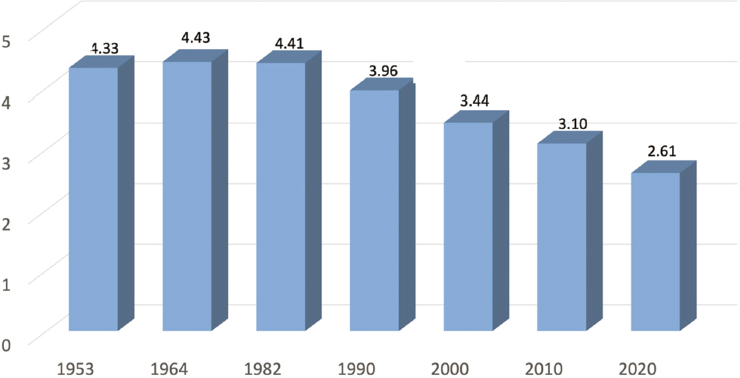
SOURCE: Workshop presentation by Feinian Chen based on data from Chinese census.
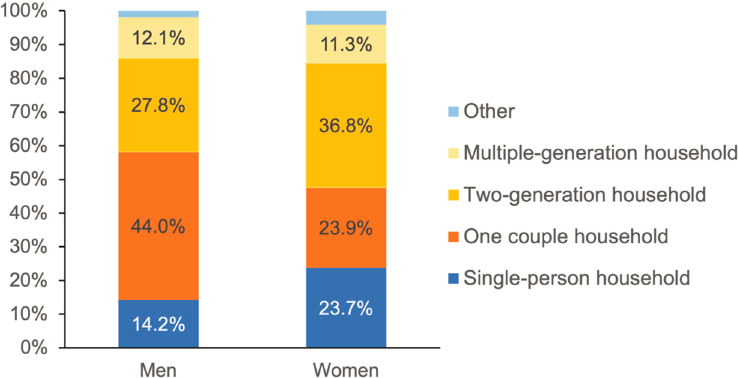
SOURCE: Workshop presentation by Feinian Chen based on data from China Health and Retirement Longitudinal Study, 2018.
by biomarkers. Chen said that these inconsistent findings demonstrated two challenges of studying living arrangements. First, a person’s living arrangement is not random: a family’s choice of living arrangement depends on societal norms, expectations, needs, and temperament. Second, it is important to look beyond living arrangements to consider the household composition of all of a person’s living children. In addition, there are important family and friendship ties that go beyond the household. For example, a 2022 study found that friendship ties were associated with reduced depressive symptoms in older adults who lived alone (but not in older adults in other living arrangements), and nonhousehold family ties had the most positive effects on older adults living with children.
Chen and her colleagues have also examined living alone, loneliness, and social isolation as three forms of social disconnectedness. They found that just living alone is not a risk factor for poor life satisfaction. However, when living alone is combined with loneliness, it is clearly detrimental. Older adults who experience all three forms of social disconnectedness—living alone, loneliness, and social isolation—have the lowest life satisfaction of any group.
While living arrangements are clearly an important factor in older adults’ health and well-being, there are other variables at play that should be studied. For example, for people who do not live with their children, proximity to children may matter, and the quality of the relationship with their children may matter. Chen and her colleagues found that life satisfaction was similar among adults who lived with children and had a high-quality relationship to those whose children lived close by and had a high-quality relationship. While older adults are often thought of as those who need care, they also provide care, said Chen. In China, in particular, grandparents play an important role in caregiving. Examining this role and its impact on health is another critical piece of the picture.
Chen shared a few lessons learned from China that may have implications for other LMICs. First, intergenerational ties have become ever more important in the 21st century. The extended household is still very important in China and many other countries, although some of the dynamics have shifted over time. Second, families are becoming more diverse and complicated globally. Demographers tend to look at families as units or households, but it is increasingly important to look at families as sets of relationships. Third, family obligations continue to exist, but the caring capacity of the family cannot be assumed, given trends in family size and the labor force. Finally, Chen emphasized the importance of “social embeddedness,” which encompasses friendship ties, family ties, and social environment. Policies need to consider these ties beyond the household in order to maintain a strong support system for a rapidly aging society. In closing, Chen offered her “wish list” for new directions for research:
- grandparent–grandchild relationship as an important source of older-age support;
- parent–child dyadic analysis to further explore the linked lives;
- time-use diary data to capture detailed activities of older adults;
- data collection that starts before mid- and later-life; and
- leveraging existing longitudinal data other than aging surveys.
FAMILY TRENDS IN MEXICO
Family structure and the concept of family have changed dramatically recently, said Carmen García Peña (Instituto Nacional de Geriatria, Mexico). Family households are more fluid, with frequent changes in size and composition, and the fertility rate has dropped worldwide, particularly in Latin America. The average household size has declined, and there has been a sharp increase in the proportion of women in the labor force. Interestingly, the proportion of multigeneration households has increased in many Latin American countries since 2000; García-Peña suggested this is related to the problems faced during times of economic downturns. People are living longer, she said, but these extra years are not necessarily healthy. The difference between life expectancy and healthy life expectancy is around 8 to 10 years in most Latin American countries.
Aging in Mexico has been “accelerated and heterogeneous,” said García-Peña. The proportion of older adults has risen rapidly, but the percentage of older adults in different regions of the country varies quite a bit. As in other Latin American countries, longevity has risen but there is still a difference of around 10 years between health-adjusted life expectancy at the age of 60 and life expectancy. This 10 years, she said, represents people living with functional dependency and the consequences of diseases, such as diabetes. Around 12% of adults over 60 live alone in Mexico, but around 70% of older people with severe functional dependency live alone. García-Peña said this is an “important challenge” to address. Another major challenge is the link between loneliness, social isolation, and mortality. A study in Mexico found results similar to those that Chen presented on China: social isolation increased the probability of dying after a fall by 1.3 times. Researchers concluded that a decrease in social interaction can affect the search for appropriate medical treatment, contribute to nonadherence to medications, and lead to unhealthy behaviors.
For better or worse, said García-Peña, the family is a crucial social determinant of health. Extended households can be a strategy for survival and interchange of supplies, but living with family can also be related to distress and abuse. Changes in family structure—from smaller family sizes to more flexible family structures—may have positive or negative effects on the well-being of older persons. There is a need for more research on how
family relationships intersect with socioeconomic status and other factors to affect health and well-being, said García-Peña.
DISCUSSION
Minki Chatterji (National Institute on Aging) asked panelists about the status of social protection policies in Latin America, suggesting that it could be beneficial to prioritize research toward a country that is starting to do work in this area. Ibarrarán replied that there is a very wide range in terms of countries’ social protection and care policies. Many countries have services for older people, but the services are not necessarily part of a broader policy implementation. Researchers are looking to evaluate small, specific interventions in order to build evidence about what works.
Will Dow (University of California, Berkeley) said that there is a need for more harmonized, longitudinal data in the Latin America region. It has been challenging, he said, to get regional budgetary buy-in for survey work. It could be useful to partner with others, such as the IDB and Pan American Health Organization, in order to advance this work. Ibarrarán said that partner organizations are beneficial for getting the process started and making recommendations, but that it is ideal if countries assume the ongoing costs of survey work. Emily Agree (John Hopkins University; workshop planning committee member) concurred and said it is easier for NIA to support harmonization than to fully fund a study; she encouraged participants to think about how partnerships could be initiated in high-value contexts. She added that there are existing data that are underutilized, for example, data on family structure in the MHAS. There could be an opportunity, she said, for NIA to incentivize the use of this rich source of data.
Chen noted that LMICs in all parts of the world are going through “very dramatic changes” in terms of demographics, family trends, policies, and socioeconomics. It is important to conduct research in order to tease apart the various changes and outcomes by taking many factors into consideration, including birth cohort and patterns across the life course.









