Developing an Agenda for Population Aging and Social Research in Low- and Middle-Income Countries (LMICs): Proceedings of a Workshop (2024)
Chapter: 7 Role of Environmental Exposures
Mary Ganguli (University of Pittsburgh; planning committee member), who chaired the session, noted that low- and middle-income countries (LMICs) are the most vulnerable to the effects of climate change and other environmental exposures. Given this, the sixth session of the workshop focused on how environmental exposures affect the health and well-being of older populations in LMICs. Several questions guided the presentations and discussion:
- What are the mechanisms through which exposures operate?
- What adaptation and mitigation strategies have been or need to be developed to reduce the harmful effects of environmental exposure?
- To what extent are the impacts of exposure on health outcomes specific to LMICs, given their country-specific contexts?
HOUSEHOLD AIR POLLUTION AND HEALTH IN LMICS
Humans have almost always used fire as a way to cook their food, and for heating, light, and protection, said Sara Adar (University of Michigan). In high-income settings, most people use fairly clean fuel for cooking and heating. In low-income settings, however, 3 billion people are burning solid fuels for cooking and heating, such as wood, animal waste, and coal. Burning these substances is inefficient and releases numerous pollutants into the air, including carbon monoxide, fine particulate matter (PM2.5), polycyclic aromatic hydrocarbons (PAHs), formaldehyde, benzene, volatile organic carbons, nitrogen dioxide, and sulfur dioxide.
A wood-fired three-stone stove, said Adar, produces the same amount of smoke in 1 hour as 400 cigarettes and, in 1 year, the same amount as 20 diesel trucks each driving 30,000 miles. People cooking over a fire are generally very close to the fire, and they are exposed to 10–100 times a healthy level of smoke. In addition to irritating a person’s eyes and throat, smoke exposures have long-term health implications, including inflammation of the lungs and systemic inflammation that can affect the rest of the body. The smallest particles can get into the bloodstream and may even travel into the brain through the nose. Adar presented data on the relative risk of various outcomes that are associated with the use of burning fuels, including lung cancer, cardiovascular diseases, adverse pregnancy outcomes, and asthma: see Figure 7-1. Burning of polluting fuels has also been associated with a higher risk of mortality, including under-5 mortality, cardiovascular mortality, respiratory mortality, and all-cause mortality.
Researchers have estimated that the global burden of disease due to the household burning of polluting fuels is approximately 1.8 million premature deaths and 60.9 million disability-adjusted life years lost (Lee et al., 2020). These burdens are almost entirely carried by LMICs, said Adar.
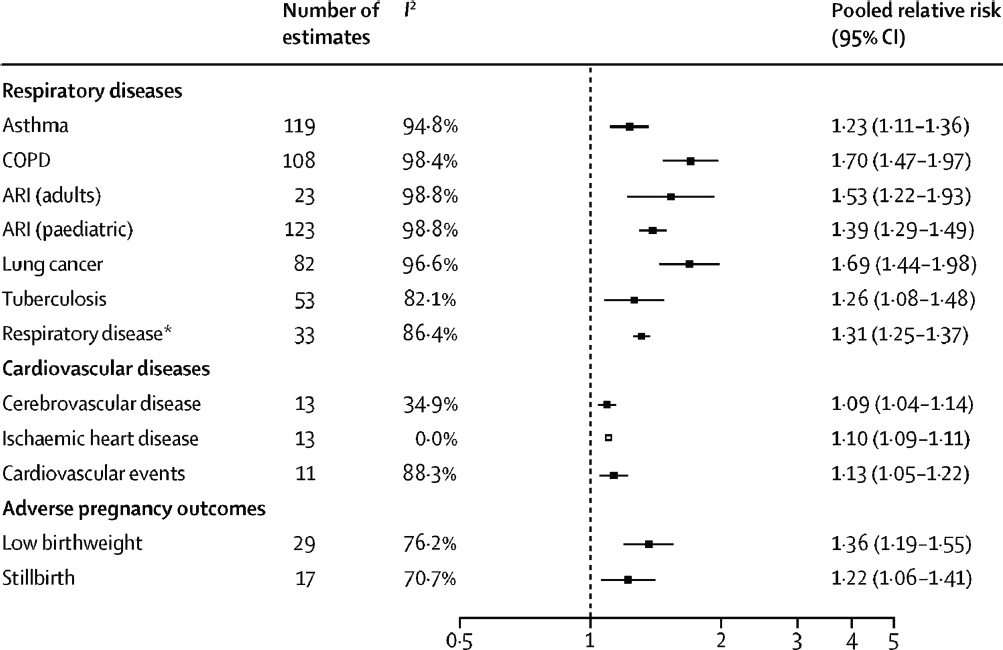
NOTE: ARI, acute respiratory infection; COPD, chronic obstructive pulmonary disease.
SOURCE: Lee et al. (2020, Figure 1). Reprinted under Creative Commons 4.0 license: https://creativecommons.org/licenses/by/4.0/
The largest burden is in Southeast Asia, Africa, and the western Pacific. Highly polluting household fuels are also associated with lower cognitive function. Using harmonized datasets, Adar said that she and her colleagues found that higher exposures to highly polluting fuels for household heating and cooking were associated with more cognitive deficits. The impact was significant, she said, with deficits equivalent to about 3–6 years (Saenz et al., 2021).
There have been many efforts by both governments and individual groups to try to reduce exposures by providing better cookstoves or cleaner sources of fuel. Better cookstoves burn cleaner or use chimneys to vent smoke outside of the home. The benefits of this type of intervention, said Adar, is that it reduces exposure while allowing people to use the fuel that they are accustomed to. The drawbacks are the costs of the equipment and the upkeep that it might require. The benefits of a chimney system are not as large as one might expect, since the smoke goes outside but can come back into the home through doors and windows. Another option for reducing exposure is providing cleaner fuel, such as liquified petroleum gas or ethanol. These substances are not “perfectly clean,” but they are much better than the current fuels being used. The challenge with this type of intervention is the practical aspects of continued access, including refilling cylinders and ensuring a steady supply to remote communities. There can also be cultural challenges, said Adar, such as fears of cylinders exploding in their home. Adar noted that when given new sources of fuel, some people will actually use both the new fuel and the old fuel (e.g., wood). A third type of intervention is called “leapfrogging”: moving people all the way to the cleanest types of cooking, such as induction or solar energy. The major drawbacks of this intervention are high cost and lack of available resources (e.g., constant supply of electricity).
Research has found that these interventions are effective in reducing exposures, both in personal exposure and the concentration of pollution in the kitchen. However, Adar noted that none of the interventions have succeeded in getting levels down to goals by the World Health Organization for “low concentrations” of pollution. Furthermore, the reductions in exposure have not always led to measurable improvements in health. Adar said that there are two potential reasons for this disconnect. First, while exposures are lower, they are still high enough to cause damage to the body. Second, interventions on individual homes may not be effective if other homes in the community continue to burn highly polluting fuel since this smoke can pass from home to home as it contaminates the outdoor air. It may be necessary, she said, to intervene in entire communities in order to have the significant effects on people’s health.
The impact of interventions aimed at reducing the use of polluting fuels reach far beyond the targeted individuals and communities, said Adar. The
burning of these fuels is causing deforestation, generating greenhouse gases, and generating short-lived pollutants in the air that absorb heat and keep it in the atmosphere. Helping people replace their cookstoves or fuel sources can improve their health and also affect people across the globe. In addition, she noted, climate change is increasing the number and intensity of wildfires; wildfire smoke is contributing greater portions of people’s yearly exposures to air pollution, even in the United States. Adar said that there is also research from her research group to show that wildfire smoke may be one of the more toxic sources of particulate pollution for the brain (Zhang et al., 2023).
There are many future opportunities in this area for further research, said Adar, including:
- further examination of the effects of household air pollution;
- understanding “how low is low enough?”;
- better exposure assessment;
- better consideration of the outcomes for aging and aging populations;
- implementation research;
- the impacts of and resilience to climate change;
- understand the heterogeneity of people’s experiences; and
- capacity building and models that promote LMIC investigators.
HEALTH IMPACTS OF CLIMATE CHANGE IN LMICS
There are multiple components of climate change and climate shocks, said Elizabeth Frankenberg (University of North Carolina). The physical dimensions of climate change include exposure to wind, rainfall, and drought; humidity; temperature; sea level and tides; and ground saturation. Climate events vary across different parameters, including speed of onset, predictability, duration, scale, and chronic or acute. The impact of these events can be far-reaching and wide-ranging, and can include property damage, exposure to physical threats, changes in work opportunities, disruption of daily activities, disruption to social networks, reduced access to health care, and rising prices.
The degree to which people and communities are affected by climate change and climate shocks, said Frankenberg, varies depending on demographic, economic, and social factors. There is an increasing frequency and intensity of extreme events, she said, and these are occurring against a backdrop of changing baseline conditions. Biologists see this as a “pulse and press” framework, in which the “new normal” of more devastating fires, storms, and hurricanes occurs more often and lasts longer, and there
is less recovery time between events. Social scientists need to consider such questions as:
- To what extent does an event affect health, increase mortality, or both?
- What are the impacts on livelihoods, assets, and socioeconomic well-being?
- What resources are available to support a postevent recovery phase?
- Does the biology of aging or the evolution of socioeconomic status that accompanies aging diminish people’s ability to respond and adapt?
As people age, Frankenberg said, they may experience reduced physical mobility, greater frailty, cognitive decline, and diminished thermal regulation. They may also have fewer ways of coping with and mitigating the effects of climate change, including limited economic resources, shrinking social and family networks, anxiety about change, and a deep attachment to place.
Measurements and methods that are important in the context of assessing the impact of climate change include constructing accurate measurements of climate-related physical forces, collecting evidence from populations both before and after a climate event, and establishing dose–response relationships using a natural experiment framework.
To illustrate her points, Frankenberg talked about the 2004 Sumatra Andaman earthquake and tsunami that affected 26 countries, focusing specifically on Aceh, Indonesia. The earthquake occurred about 150 kilometers off the coast and involved a 1,200 kilometer “unzipping” of the sea floor. A series of tsunami waves were set off and hit Aceh about 15 minutes after the earthquake. The tsunami was unexpected (the last to hit Aceh was over 600 years ago), and there was local variation in impact that was driven by offshore topography. People had little to no time to move before the waves hit. About 200,000 people were killed—about 5% of the province’s population—and about 750,000 were displaced. The “beautiful, idyllic coastal landscape” with fields, roads, and settlement was replaced by bare earth. There was a strong effort to raise money for recovery; assistance funds raised totaled $7 billion. Within 5 years after the tsunami, the area had made substantial strides toward recovery, with beaches, roads, homes, and fields beginning to return.
Frankenberg and her colleagues conducted the Study of the Tsunami Aftermath and Recovery (STAR),1 which used as a baseline pre-tsunami
___________________
data from a government survey that had collected information on 26,000 individuals. Researchers followed up with 96% of survivors and followed people who had moved all over Indonesia. They conducted 5 years of annual surveys immediately after the tsunami, then moved to surveys every 5 years; these were interspersed with collections of more extensive biomarkers and cognitive data on a subsample of participants. Survey domains included household composition, economic resources, education, migration, work, fertility, psychosocial health, tsunami shocks, loneliness, sleep, frailty, memory, social support, and networks.
Frankenberg presented information on mortality among the residents of Aceh. Clearly, initial mortality rates were highest in the communities that were hardest hit by the tsunami. However, in the 10 years following the tsunami, the hardest-hit communities actually experienced lower mortality. She suggested that this reflected a positive selection effect: namely, that those who survived were selected on factors that promote longevity. There were particular “scarring” experiences related to the tsunami that affected the prospects of survival for adults 50 and older. For females, losing a spouse reduced survival. For males, losing a spouse increased survival, while living in temporary housing or experiencing high levels of post-traumatic stress reactivity decreased survival. There was no evidence of such “scarring” for younger adults, she said.
Exposure to the tsunami was found to affect cognitive and biological functioning, said Frankenberg. Males who lived in communities that were badly damaged had worse cognitive scores, as did females who saw or heard the water as a personal exposure. Two markers that are associated with stroke and cardiovascular disease (C-reactive protein and adiposity) were increased in both females and males who lived in communities that were heavily damaged; this effect was found 12 years after the tsunami (Frankenberg et al., 2018).
The economic impact of the tsunami was long lasting, said Frankenberg. For example, 10 years after the tsunami, the earnings of men who were aged 40 to 60 when they were directly exposed to the tsunami were 30% lower than before the tsunami, and 30% lower than the earnings of men who were not directly exposed. For directly exposed younger men, earnings recovered over time, but they remained 12% lower than those who were not directly exposed. There are a number of mechanisms driving these differences, said Frankenberg. A lot of earnings recovery was driven by reconstruction; these opportunities are more available to younger men. In response to the tsunami and its impact, women entered the labor market, households started businesses and took on financial risks, and families sold assets. Assistance was critical to survivors: 21% of survey respondents received an assistance home, and receipt was more likely among those with fewer resources before the disaster. Those who received a home showed a
decline in post-traumatic stress reactivity levels, and this effect was concentrated among those whose homes were destroyed. Frankenberg said that this study demonstrated a critical nexus between housing and psychosocial health (Frankenberg et al., 2023).
In summary, Frankenberg said that exposure to the effects of climate change creates stressors that affect physical, psychosocial, and cognitive health over the short and longer term. The financial, social, and human resources with which people enter midlife are likely critical for how old age unfolds with respect to the effects of climate change for health and economics. She noted that “institutions matter” by reducing exposures and the consequences of exposure, and institutions vary hugely across LMICs. Frankenberg identified some key questions that remain for future research:
- What are cost-effective strategies for preventing or facilitating recovery from large negative climate shocks or less severe but more frequent events?
- What are the general equilibrium effects on economic and social systems?
- How do these dynamics intersect with the aging process to generate differential vulnerability?
Regarding research infrastructure, Frankenberg emphasized several lessons learned from the STAR study. First, tracking people both before and after an event is key; this may mean following people long term to other locations. Second, there is a need to conceptualize and measure exposure, to assess its exogeneity, and to capture variation in exposure. The dose–exposure relationship is important and can reveal interesting patterns. Third, national representation is not always the highest priority for studies of environmental exposures. Heterogeneity in exposure is important, as is having a large enough sample size to be able to drill down into finer-grained questions. Fourth, there are scientific opportunities in building networks of studies using a natural experiment “dose of exposure” framework. Comparisons across studies of different events and populations will be fruitful. Finally, adding and evaluating the impact of interventions is key to reducing consequences for the health and well-being of affected populations.
ENVIRONMENTAL RISKS AND ADAPTATIONS IN LMICS
Jennifer Ailshire (University of Southern California) provided a broad view of the topic of environmental risks and how they may affect the health of older populations in LMICs. She began by sharing a framework for environmental impacts on health in LMICs: see Figure 7-2. Risk is formed through the interaction of hazards, exposure, and vulnerability. Hazards
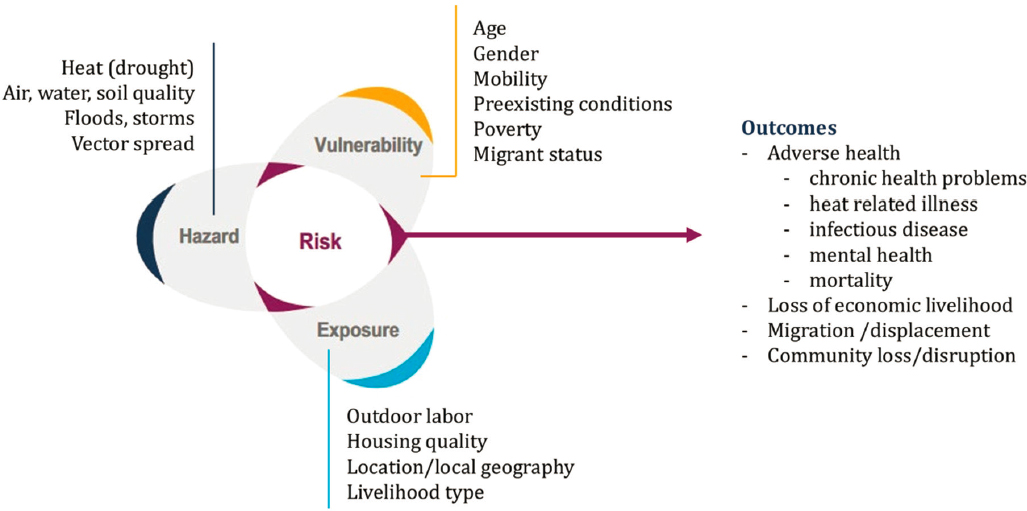
SOURCE: Adapted from Cissé et al. (2022, Figure 7.4).
can include heat, air and water quality, floods, storms, and the spread of vector-borne diseases. The potential for exposure is related to the context in which people live, and it can include such factors as housing quality, work environment, location, and type of work. Ailshire noted that people in LMICs are often more likely to be exposed to hazards due to their location and lifestyle. For example, people working outdoors are exposed to poor air quality, people living in substandard housing are less protected from storms, and people who work in agriculture may lose work opportunities because of drought or land damage. Hazard and exposure interact with an individual’s vulnerability factors, which include age, gender, mobility, preexisting conditions, poverty, and migrant status.
There are a wide variety of ways that these factors can make a person more environmentally vulnerable, she said. For example, a lack of mobility can make it harder to move away from a fast-moving event (e.g., flood), women may be exposed to indoor air pollution from cooking, men may be exposed to poor air quality outdoors, poor people lack resources to mitigate or cope with climate events, and people with preexisting conditions may have exacerbated outcomes. Migrants may be particularly vulnerable, said Ailshire, because of such factors as informal work arrangements, poor-quality housing, and lack of eligibility for social support and health care services that might be provided to the rest of the population after an environmental event.
Taken together, hazards, exposure, and vulnerability create risks, which can translate into outcomes. Outcomes can be health related, such as chronic health problems, infectious disease, mortality, and mental health issues. Outcomes can also include loss of economic livelihood, forced migration or displacement, and the loss or disruption of community. Ailshire noted that people in LMICs who live, work, and socialize in the same small community may be more affected by a localized event than people in higher-income areas. For example, she noted that in high-income countries a fire that threatens a person’s home is unlikely to also threaten their place of work since they tend to be located in different places; this is less so in low-income countries.
Ailshire shared three maps that show the predicted future impact of air pollution, extreme heat, and mosquito-borne illness across the globe. In each map, the biggest impacts are in countries in Latin America, Africa, and Asia. Compounding these projected risks, said Ailshire, is that many of these countries have rapidly growing older populations, developing economies that are shifting to more industrialization and more pollution, a lack of urban planning or standards for building, and inadequate health care systems. Furthermore, she said, these countries often lack the wealth at both the individual and macro levels to invest in technology to mitigate these risks (e.g., to buy air conditioners for rising heat). Older adults in
these countries have specific challenges that make them more vulnerable, including:
- greater health burdens that exacerbate adverse environmental events;
- lack of access to health care;
- limited social protection programs targeted to them;
- changes in urbanization, economic development, and family configurations; and
- inadequate economic resources for recovery in event of environmental adversity.
The extent to which the hazard–exposure–vulnerability nexus translates into risk depends on a population’s ability to be resilient or to develop adaptation strategies, said Ailshire. The Intergovernmental Panel on Climate Change offers a clear definition of resilience and adaptation: “Human vulnerability is influenced by the adaptive capacity of physical (built) structures, social processes (economic, well-being and health) and institutional structures (organisations, laws, cultural and political systems/norms)” (Dodman et al., 2022, p. 929). Ailshire said that she likes this definition because it does not put the onus of resilience on individuals or families, but instead acknowledges that it will take macro-level changes and macro-level actors to facilitate resilience in communities. There are a number of ways that LMIC communities can become more resilient or adapt to changes, including:
- early warning systems,
- urban development,
- rural investment,
- resilient transportation infrastructure,
- increased capacity of health care systems,
- insurance schemes,
- uptake of innovative technologies, and
- better family and community supports.
While LMICs do not have the resources or infrastructure of higher-income countries, they do have some advantages in resiliency and adaptation, said Ailshire. Some of the most innovative adaptations come from LMICs because “they have to innovate.” For example, countries without ready access to fossil fuels are investing in solar, wind, and other technologies. In addition, LMICs have the opportunity to rely on strong family and community supports, which are less common in higher-income countries.
However, she said, these supports could be weakening as family size and structure are changing over time.
Ailshire shared an example of a macro-level adaptation effort undertaken by the World Bank. Unpaved roads can become difficult or impossible to navigate after heavy rain; it may be even more difficult for people with mobility issues or women carrying children. To address this issue, the World Bank has begun improving roads in India, building a road system that is resilient to weather conditions and improves access to education, health care, and economic opportunities.2
There are a number of research challenges and opportunities in the area of environmental hazards and their impact on LMICs, said Ailshire. In terms of collecting data on the environment, environmental data may be sparse in LMIC settings, and administrative data typically do not have adequate coverage. However, there are opportunities for surveys to innovate—for example, by using personal air pollution monitors or having interviewers capture observations of environmental conditions. In her own work in India, she said, they are using satellite data and other systems like Google Street View to get a sense of environmental conditions and physical environments. Even with data, however, Ailshire warned that there is an additional challenge around the conceptualization of environmental effects. Risks for poor outcomes will differ across settings, and there is a need for content and context experts to think about how to measure environments and model the effects. Modeling is a challenge, particularly because environmental events can vary substantially in timing, duration, and impact, and there are synergistic effects between multiple physical and social environmental hazards and stressors. For example, air pollution may exacerbate a heat wave, and the effects on individuals may vary considerably depending on length of exposure, mobility and preexisting conditions, and ability to mitigate or adapt to an event.
DISCUSSION
Minki Chatterji (National Institute on Aging) began a wide-ranging discussion after noting that it was helpful to have pre-event data when studying the effects of the tsunami in Indonesia. Of course, “we don’t know where these things are going to happen,” so how do we prioritize data collection? In addition, Chatterji said that the Indonesia study is important because it demonstrated how different policies that were put into place mitigated some of the negative effects of the event. With climate change, there will be more events like this one, so there is a need to consider how to best collect data on both the event itself and policies implemented.
___________________
2 https://www.worldbank.org/en/country/india/brief/connecting-villages-through-rural-roads-in-india
Emily Agree (Johns Hopkins University; workshop planning committee member) said that one important takeaway from the session was about the role of infrastructure. “Even in the best of times,” lack of infrastructure affects health and well-being, and natural disasters and events can exacerbate these challenges. It is important to do the work to understand the environment and infrastructure of areas in order to assess a community’s vulnerability to disasters or access to health care.
Anthony Ngugi (The Aga Khan University) asked Frankenberg whether there is a way to tap into local knowledge when studying communities. He noted that when people have lived in a place for a long time, they often have accumulated knowledge about drivers that cause health outcomes or about changes that have occurred over time. He recounted that he and his colleague encountered a group of Maasai men when scouting for research sites; the men could tell Ngugi and his colleague about how cattle grazing had changed over the last 50 years due to climate change and government actions. He asked: “How can we tap into this kind of knowledge in order to not look at these populations only as study subjects, but as people who also have knowledge that can be useful?” Frankenberg agreed with the importance of local knowledge and said that the STAR study conducted detailed community and facility interviews to talk to multiple informants at the community level. She added that the knowledge of the community is often not about “big dramatic changes” but about smaller changes over time that the local inhabitants have observed. For example, in coastal North Carolina communities, people who are often hesitant to talk about climate change are very much aware of the changes over the last 20 years in the type of shrimp that can be caught in the area.
This page intentionally left blank.













