Identifying and Managing Veteran Suicide Risk: Proceedings of a Workshop (2023)
Chapter: 5 Best Practices, Gaps, and Challenges for Identifying and Managing Suicide Risk Across Veteran Populations
5
Best Practices, Gaps, and Challenges for Identifying and Managing Suicide Risk Across Veteran Populations
INTRODUCTION
Eric Caine observed that the VHA is the largest integrated health care system in the United States, yet it only serves a subset of the veteran population. Further complicating this issue, he continued, is that the highest count of veteran suicides is among those not in VHA care.
Caine elaborated that the highest veteran suicide rate is among younger veterans, ages 18–34. In 2020, he continued, 317 of these deaths were among veterans in VHA care, and 526 were among veterans not in VHA care. However, the highest suicide count is among veterans ages 55 and older. Caine emphasized that this dichotomy in rate and count presents a significant health system challenge—effective interventions for a 28-year-old and a 68-year-old, for a New York city resident and an Alaska resident, or for a Black veteran and a White veteran might all be very different.
Caine pointed out that suicide is more than simply a “disease with symptoms;” it involves multifactorial patterns among individuals. To address such patterns effectively, he asserted that the “medical model” that focuses only on what happens in the brain is insufficient. That model should be expanded to a model that prioritizes various community interactions and influences. Furthermore, he underscored the need for increased efforts to better engage veterans in health care systems beyond VHA. However, questions remain as to whether other health care settings can achieve the highest standards of evidence-based care.
Caine described three public health approaches to preventing suicide, attempted suicide, and adverse health behaviors: universal prevention (for
the whole population), selective prevention (for high-risk populations), or indicated preventive (for symptomatic populations) interventions. As an example of a selective prevention intervention, he indicated that all-cause mortality (i.e., death due to any cause), opioid overdose deaths, and suicides all decreased with medication-assisted treatment for opioid use disorder. This evidence demonstrates that the systematic use of medication-assisted treatment is a suicide prevention initiative with the potential to change individuals’ trajectories.
Turning to a discussion of opportunities to better connect veterans to health care systems, Caine explained that every setting, such as a particular university, a particular workplace, or a particular health care site, has a “social geography,” meaning there are populations likely to be engaged in the setting, and others who are not likely to be engaged in the setting. The social geography of VHA, for example, includes people who visit medical settings; veterans who do not visit medical settings will be missed at the VHA. An understanding of social geography could help to identify people who are engaged in a setting who might be in need of care. For example, a young adult veteran with a full-time factory job would not be engaged on a college campus unless enrolled in classes, while a homeless veteran could be engaged via a local government agency. Identified veterans could then be brought to a health system, instead of waiting for them to visit a health system. Social ecology also plays an important role, with the focus being on first identifying higher-risk veterans and then determining likely sites where they might be reached (e.g., identifying veterans with alcohol and substance use disorders in the court system). He stressed that social geography and social ecology enable a systematic process to determine where to find veterans in need of care, which veterans need care, and which interventions are appropriate; a question remains as to whether a medical, disease-oriented health system can shift to this type of public health system that prioritizes helping people from the community.
INDIVIDUALS RECEIVING HEALTH CARE OUTSIDE OF VHA
Lessons Learned from the Governor’s Challenge to Prevent Suicide Among Service Members, Veterans, and Their Families
Cicely Burrows-McElwain (VA Office of Mental Health and Suicide Prevention) and Stacey Owens (Center for Mental Health Services, Substance Abuse and Mental Health Services Administration [SAMHSA]) provided an overview of the Governor’s Challenge to Prevent Suicide Among Service Members, Veterans, and Their Families (SMVF).1
___________________
1 https://www.samhsa.gov/smvf-ta-center/mayors-governors-challenges
Burrows-McElwain explained that the Governor’s Challenge commenced in 2018 after questions arose about how to identify veterans, how to determine where veterans were seeking care, and how to capture the corresponding data. The Governor’s Challenge is a cross-agency collaboration between VA and SAMHSA, in which state policy makers partner with local leaders to implement suicide prevention policies and practices for SMVF. The initiative also focuses on veteran-to-veteran coalition-building and veteran leadership development as well as community engagement and partnerships for suicide prevention (Figure 5-1). To create and implement a strategic action plan, teams are formed within each participating state/territory with interagency military and civilian collaboration. She indicated that these teams are guided by SAMHSA’s Strategic Prevention Framework (Substance Abuse and Mental Health Services Administration, 2019), VA’s
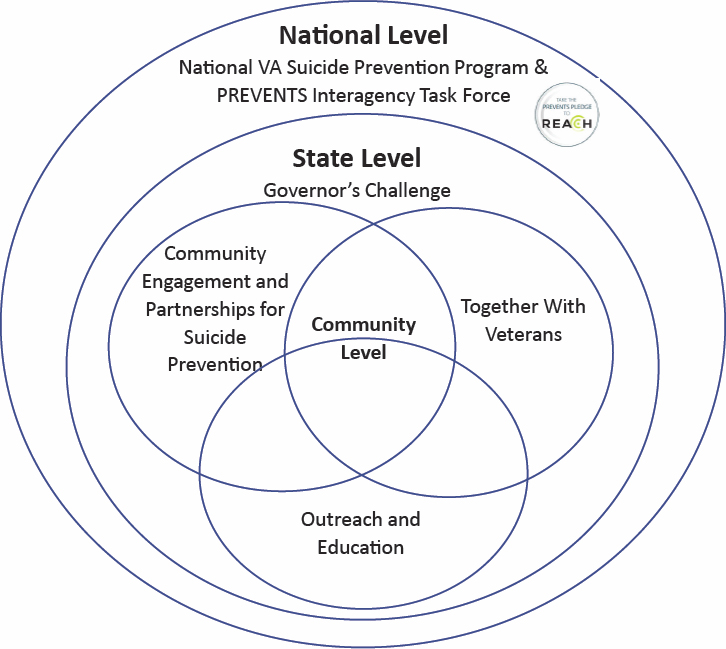
SOURCE: Department of Veterans Affairs, n.d.
National Strategy for Preventing Veteran Suicide 2018–2028 (Department of Veterans Affairs, 2018), and RAND’s Getting To Outcomes® models;2 and the teams participate in technical assistance events facilitated by VA and SAMHSA.
Owens described the Governor’s Challenge process. Year 1 is a planning year, with time to assemble the state/territory’s community team, conduct analysis and determine strategies, align outcomes for strategies, and submit a strategic action plan to reduce suicide among SMVF in the specific jurisdiction. Year 2 focuses on implementation, by initiating strategies and beginning pilot efforts through a strategic partnership. In following years, effective pilots turn into permanent interventions and new pilots are identified, with a focus on tracking results, collecting data, and analyzing the effectiveness of the strategies. The overall goals of the initiative are policy change and state/territory-wide implementation of best practices to improve suicide prevention efforts. She underscored that broad engagement helps to create synergy around suicide prevention efforts—as of May 2023, 54 states and territories are participating.
Owens noted that the Governor’s Challenge has three priority areas for suicide prevention:
- Identify SMVF and screen for suicide risk: several teams are implementing “Ask the Question” (about veteran status) campaigns as a trained/mandated practice and/or are integrating a universal screening instrument (e.g., the Columbia Suicide Severity Rating Scale).
- Promote connectedness and improve care transitions: several teams are promoting Caring Contacts as a standard practice for post-crisis hospitalization, the Expiration Term of Service Sponsorship Program for service members transitioning to civilian life, and telehealth and telepsychiatry services.
- Increase lethal-means safety and safety planning: several jurisdictions are implementing Counseling on Access to Lethal Means and VHA Lethal Means Safety Training, effective media campaigns to promote lethal-means safety, and Crisis Response Planning training.
Owens shared two examples of state-level best practices to identify SMVF. New Hampshire’s “Ask the Question” toolkit,3 much of which is customizable, is available for all states and can be used not only by health care providers but also by children’s services and school systems, faith-based groups, employment and vocational services, aging and senior services, and
___________________
2 https://www.rand.org/health-care/projects/getting-to-outcomes.html
law enforcement and first responders. Missouri took a “legislation-first” approach to “Ask the Question” via Senate Bill 120;4 a question about veteran status (self or family member) has been added to all state agency forms and will trigger notification about available services and benefits. She added that the Missouri Governor’s Challenge Team is developing a toolkit to assist state agencies with this implementation.
Burrows-McElwain provided two examples of state-level best practices to improve screening and care transition. The Virginia Identify, Screen, and Refer Pilot,5 which continues to be expanded, connects community organizations to state agencies to help eliminate gaps in access to care for SMVF. She remarked that the approach has been particularly effective owing to its “two-lead” structure—comprised of the state-level VA and state department of behavioral health. Another successful initiative comes from the Harris Center in Houston, which worked with the DeBakey VA Medical Center to create a memorandum of understanding on crisis care coordination in 2019.6 She emphasized that all of this work is leveraged through open-source sharing of best practices, barriers, and solutions. Additionally, she noted that a new collaboration is under way with subject matter experts in tribal communities to develop a more culturally appropriate approach to address suicide prevention in native veteran populations.
Approaches to Policies, Practices, and Training for Suicide Prevention at Cohen Veterans Network
Stephanie Renno (Cohen Veterans Network and workshop planning committee member) described Cohen Veterans Network as a “not-for-profit organization with a mission to improve the quality of life for post-9/11 veterans, service members, and their families by providing low to no cost, high-quality, accessible, and integrated mental health care.” She noted that almost 50 percent of Cohen Veterans Network clients are military and veteran family members and 50 percent are veterans or active-duty service members; 59.5 percent of the veterans report enrollment in or receipt of VA care.
Renno explained that suicide prevention policies and procedures at Cohen Veterans Network are guided by the VA/DOD Clinical Practice Guideline for the Assessment and Management of Patients at Risk for Suicide, a scientific advisory board, and consultation with other experts. The first step is screening: within 24 hours of reaching out to a clinic, a
___________________
4 https://www.senate.mo.gov/21info/pdf-bill/intro/SB120.pdf
5 https://www.governor.virginia.gov/newsroom/all-releases/2019/december/headline-850263-en.html
6 https://www.houston.va.gov/features/Mayors_Challenge_Prevent_Veteran_Suicide.asp
person has an opportunity for screening with non-clinical staff. If the person endorses suicidal ideation, a licensed clinician is engaged to complete a standardized screening questionnaire, and immediate care or crisis services are initiated if needed. If the person is determined to be high risk, that person enters an “elevated risk pathway,” she continued, which includes a monthly review and update of a safety plan; lethal-means counseling; weekly screening; targeted treatment goals around suicidality; and increased follow-up and monitoring around no-show appointments, which are tracked through electronic health records.
Renno highlighted other approaches to enhance patient safety at Cohen Veterans Network. The Cohen Clinical Quality Institute collects and analyzes patient safety data reported by health care providers, improves patient safety and health care quality, and creates a “learning health system” with legal protections for collected information. Quality assurance managers review clinic data, meet monthly, and identify areas for possible risk improvement. The quality assurance team oversees a peer review process in an effort to better support individual clinics and spread best practices. She explained that the sentinel event review process, which occurs after a client dies by suicide, also supports the clinics. Clinics are offered assistance to work through the postvention process and engage in review for compliance with elevated risk protocols and given additional training and remediation if necessary. She emphasized that all of these policies are intended to enhance care for the clients, helping them to discover lives worth living. Cohen’s approach of comprehensive support includes individual intervention (i.e., evidence-based treatment, medication management, and telehealth options), case management (i.e., resources to address barriers to care and to support Social Determinants of Health), and engagement with the family and community (i.e., groups, couples and family therapy, family support, and community activities).
Renno asserted that the cornerstone of suicide prevention at Cohen Veterans Network is training for clinicians. The training includes monthly suicide prevention consultation calls with national experts as well as instruction in the following: suicide prevention foundations (e.g., how to ask a veteran about suicide), lethal-means counseling for veterans, cognitive behavioral therapy for suicide prevention, and Collaborative Assessment and Management of Suicidality.7 She championed Cohen’s use of the “train the trainers” approach, in which trainers are staff members in Cohen clinics.
Renno pointed out that mitigating clinician burnout and trauma is a key aspect of training. She asserted that clinicians should understand that they cannot control client suicide—they can only influence it—and recognizing clinician limitations is important for conducting suicide assessment.
___________________
Like clients, she continued, clinicians are doing the best they can, given their history and current resources. She urged the health care community to continue to “strengthen its resources, learn more, and do even better.”
In closing, Renno highlighted five remaining challenges in the work to prevent suicide among veterans:
- Quality care is expensive; quality assurance, clinician training, and access to expert consultation have both direct and indirect costs.
- Issues remain with billing and payment; many key tasks are “non-reimbursable activities,” and sometimes the financial burden falls on the veteran.
- Clinicians and systems can sometimes focus on personal liability instead of on what is best for the individual patient, which requires flexible and creative approaches.
- Current technology presents barriers to the integration of electronic health records.
- Established best practices are still missing the mark.
Evidence and Opportunities in Health Systems for Veteran Suicide Prevention
Brian K. Ahmedani described suicide as a significant public health concern in the United States. U.S. suicide rates have risen 25 percent since 2000, and nearly 50,000 people die by suicide each year. He noted the importance of focusing not only on suicide deaths but also on suicide attempts, of which close to two million occur per year, and on suicidal thoughts, which are acknowledged by nearly 10 million people per year. He explained that veterans have an elevated risk for suicide, as approximately 6,000 veterans die by suicide each year. He emphasized that because only approximately 62 percent of veterans receive some VHA care, health care systems across the United States have a critical responsibility to work together to care for veterans and prevent veteran suicide.
Ahmedani pointed out that because the notion of health care system responsibility for suicide prevention strategies only emerged about two decades ago, related treatments and interventions have not yet become embedded in the culture. He provided a brief overview of the 2012 National Strategy for Suicide Prevention,8 which included new goals for health care systems to “integrate and coordinate suicide prevention across multiple sectors and settings;” “promote suicide prevention as a core component of health care services;” and “promote and implement effective clinical and professional practices for assessing and treating those at risk for suicidal
___________________
8 An updated strategy is scheduled to be released in 2024.
behaviors.” He underscored that achieving these goals is especially important in enhancing suicide prevention for veterans who receive some or all care in community health systems.
Ahmedani revealed that 83 percent of a cohort of nearly 6,000 people who died by suicide from 2000 to 2010 had a health care visit sometime in the year leading up to their death (mostly primary care visits, where suicide risk identification has not always been emphasized). Less than 50 percent of this cohort had a mental health diagnosis before dying by suicide, and only approximately 33 percent of this cohort had a behavioral health visit—the setting in which many of the formal suicide prevention strategies are implemented—prior to dying by suicide (Ahmedani et al., 2014, 2019). Therefore, he asserted that if suicide prevention is only targeted during behavioral health visits, two-thirds of those at risk of dying by suicide could be overlooked. In addition to expanding the reach of suicide prevention across health care settings, he suggested developing different intervention strategies that vary by intensity for particular populations. Furthermore, he indicated that in the past, mental health interventions have received greater attention than suicide prevention; however, those interventions alone will not reduce suicide risk. For example, depression and alcoholism are not the same as suicidal ideation. Thus, treating depression and alcoholism alone might not affect suicidal ideation. He stressed that effective interventions are those that treat suicidal ideation as a unique disease and target it directly and concurrently with any other conditions.
Ahmedani described an effective suicide prevention initiative that Henry Ford Health launched in 2001. The Zero Suicide Model consists of a series of evidence-based processes that serve as a suicide prevention care pathway (see Figure 5-2). The pathway starts with suicide risk screening using the PHQ-9, followed by suicide risk assessment using the C-SSRS or other identification strategies. If the assessment reveals the presence of suicidal ideation, a brief intervention is delivered to support care and care transitions between settings and providers, and then the patient is referred for suicide specific treatment (Richards et al., 2021).
Ahmedani remarked that the model successfully reduced the Henry Ford Health behavioral health population’s suicide death rate by 80 percent (see Coffey et al., 2015; Hampton, 2010). As new evidence has emerged over the past two decades, interventions and processes have been updated, and the model has been implemented in more than 20 countries and in hundreds of U.S. health systems, including VHA. He emphasized that the Zero Suicide Model is one of the few documented programs in the world that has reduced suicide deaths and suicide attempts in health care systems. The model continues to be implemented broadly across health systems and has been expanded, for example, to offer care pathways specific to emergency departments.
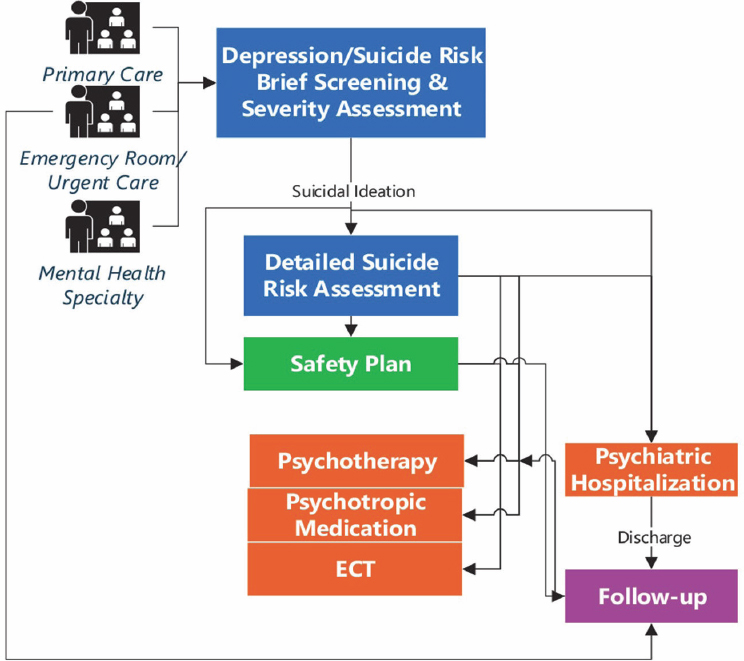
SOURCE: Richards et al., 2021.
Looking to the future, Ahmedani explained that because the nature of suicidal ideation prevents people from getting the care they need to be healthy, health care systems should provide support for those individuals and their families. He described the value of developing a systematic care pathway to best leverage clinical values and skills as well as increasing connections with the community. Most importantly, he continued, clinical interventions should be tailored for veterans, but health care systems often do not know which patients are veterans. He proposed asking for veteran status automatically, just as race/ethnicity and date of birth are always requested, so that health systems could provide enhanced care coordination services. Furthermore, because veterans might be more likely to use firearms as a means of suicide, an emphasis on lethal-means safety would be beneficial. Other opportunities to improve care for veterans include creative care models such as systematic outreach, peer support, community
health support, tele-mental health services, and mobile health services. He encouraged enhanced partnerships between VHA and health systems, with informatics to connect patient records and care relationships between entities, as well as enhanced partnerships between health systems and other community sectors such as employers and recreation organizations.
Discussion
Caine moderated a discussion among the session’s speakers. He described the challenges of identifying risk during a suicide screening because the person might not be suicidal at that particular moment in time, and wondered whether intervention programs are engaging people who are experiencing personal turmoil and might be at risk at a later date, or whether they only target people with active suicidal ideation. Burrows-McElwain explained that the goal of the Governor’s Challenge is to create a comprehensive, community-wide approach to suicide prevention, which includes risk screening and safety planning. She said that safety planning is especially important for those not in immediate risk, as it serves as a “safety net” when their level of risk increases. The community also plays a key role in safety planning—for example, by offering training and changing policy to better connect systems to provide support. Although the goal for comprehensive care has not been fully realized, she continued, much progress has been made. Ahmedani noted that during suicide risk screening, a person’s responses are not absolute. He compared screening practices for suicide risk to those used to assess heart attack risk. Although high cholesterol scores and high Framingham Risk Scores indicate an increased risk for heart attack, clinicians do not know when or if a patient might have a heart attack. However, because the risk is elevated, medication is given to reduce cholesterol levels. Similarly, Ahmedani continued, if someone screens positive for suicidal ideation, this indicates an increased risk of suicide sometime in the future, and action should be taken. Furthermore, he continued, some people who screen negative are still at risk of suicide, and providers should identify warning signs, understand risk factors, complete a suicide risk assessment, deliver a safety plan, and begin care coordination in an effort to prevent suicide.
Rajeev Ramchand presented a concern that if suicide prevention is the central focus during a primary care visit, the clinician might not be able to address the reason for the visit, which could frustrate the veteran. Renno replied that clinician training emphasizes how to have honest conversations with the client and be prepared to talk about the exact “why” suicide is being discussed—because the person’s safety is important and something the person said raised concern, not because it is a VA requirement.
An online workshop participant asked about interactions between faith-based communities and academic settings. Renno responded that
protective factors to reduce suicide risk and to promote general well-being include faith, religion, and community support. For instance, Cohen Veterans Network offers a community room for faith-based organizations to host meetings for veterans. It also promotes partnerships with and referrals to community-based counseling. Caine described the relationship between faith-based communities and academia as complicated, in part owing to cultural differences. For example, after a long history of discrimination by the University of Rochester Medical Center against members of the Black community, trust-building between a Black faith-based community and the university took many years before new programs could be discussed. He encouraged collaboration, humility, respect, time, patience, and mutual curiosity to develop and sustain effective community partnerships.
Carl A. Castro noted that because chaplains oversee suicide prevention programs in the military, veterans might gravitate toward faith leaders instead of mental health professionals for support; thus, faith-based collaboration is critical to provide continuity. Ahmedani agreed that because some people trust only their faith leader, building relationships with faith-based groups to facilitate care is essential—faith is often a powerful aspect of recovery and healing. He reiterated the value of building suicide prevention efforts across the community instead of within silos. Burrows-McElwain explained that during Year 1 of the Governor’s Challenge, the VA Center for Faith-Based and Neighborhood Partnerships and state-level leaders with enhanced faith-based community partnerships are invited to speak to the teams, who are then encouraged to include faith-based partners in their work. Furthermore, VA stood up Community Engagement and Partnership Coordinators across the nation to apply the public health model of the Governor’s Challenge at the local level. She added that more than 1,000 coalitions have been created with faith-based community partners from different sectors.
Shawn Moore observed that a veteran’s primary community is the family, but not enough tools are provided to family members on how to recognize signs of suicide risk and, more importantly, what to do next. She noted that when “Ask the Question” also identifies loved ones of those who have served, these resources can be provided more readily to family members (e.g., in hospital settings, schools). An online workshop participant highlighted VA S.A.V.E. (Department of Veterans Affairs, 2022), a program offered by the VA suicide prevention team that provides training about signs and next steps to care for veterans in crisis. Castro pointed out that veterans who die by suicide often have been to mental health visits because a friend took them, which demonstrates the effectiveness of raising awareness about the signs and symptoms of suicidal ideation. However, he remarked that while veterans might recognize the warning signs, many of them just want to be left alone, and they have the right to refuse care. He underscored that this further complicates the challenges of identifying and managing suicide risk.
Workshop participant Trista Maccini posed a question about the potential for having “veteran champions” in community hospitals who are employees of those particular medical systems and are either veterans themselves or are related to veterans. These “champions” would have a direct contact in VA and be able to provide information about available programs and services to assist with transition of care after hospitalization, for example. Caine supported this idea but emphasized the need for medical center leadership to promote such an initiative, which would require cultural and behavioral change.
Allen Levi Simmons asserted that although communication seems to be a key theme to preventing veteran suicide, a critical link between DOD and VA is missing. Instead, he continued, information should be passed securely between the two, as well as to other subgroups that are assisting VA with mental health care, to better identify and manage suicide risk.
INDIVIDUALS RECEIVING HEALTH CARE IN VA-PURCHASED COMMUNITY CARE SETTINGS
Suicide Prevention Opportunities and Challenges
Megan E. Vanneman (Department of Internal Medicine, Division of Epidemiology, and Department of Population Health Sciences, Division of Health System Innovation and Research, University of Utah School of Medicine; Informatics, Decision-Enhancement and Analytic Sciences Center, VA Salt Lake City Health Care System) explained that, of the 16.5 million veterans who live in the United States, nearly nine million are enrolled in the VA health care system, and approximately 6.3 million are VA health care patients in any given year. VHA is a large integrated health care system, with 171 medical centers; 1,113 outpatient clinics; and an annual budget of $69 billion (Veterans Health Administration, 2022). On average, she continued, patients relied on VA for 50 percent of their care in 2014 (Giroir & Wilensky, 2015).
Vanneman highlighted two legislative actions to expand access to care for veterans. The Veterans Access, Choice, and Accountability Act of 2014 (Choice Act) provided access to care for VA enrollees regardless of where they live. It also expanded eligibility for VA-purchased community care9 based on drive distance to a VA facility, wait time for VA care, and hardship in accessing VA care. The VA Maintaining Internal Systems and Strengthening Integrated Outside Networks Act of 2018 (MISSION Act) consolidated community care programs, established the Community Care Network with additional providers, and further expanded VA enrollees’ access to
___________________
9 VA-purchased community care is care that is purchased by VA in the private sector.
community care by replacing the criteria of long drive distance with long drive time to a VA facility and updating the wait time metrics. Those eligible through Choice were grandfathered in. She pointed out that in 2022, out of the approximately 6.3 million VA health care users, approximately 3.5 million used VA-direct care exclusively; 2.6 million used a combination of VA-direct care and community care; and 180,000 used community care exclusively. This heterogeneity has significant implications for care coordination, which is a legislative requirement for VA.
Vanneman presented research on primary care and mental health care for veterans that has emerged since the era of the Choice Act and MISSION Act. In a study on the expansion of primary care via VA-purchased community care, Gordon and colleagues (2021) found that the proportion of primary care received in the community (vs. in VHA facilities) is growing, and VA-purchased primary care might be serving an access need in rural counties, counties without a VA facility, and counties with a lower supply of providers. In another study, Vanneman and colleagues (2020) considered veterans’ experiences with outpatient care by comparing access, coordination, communication, and provider rating between VA and community care for both primary care and mental health care. VA scored better than community care in communication, coordination, and provider rating, but no statistically significant differences existed in access to primary or mental health care. In a more recent study, Vanneman and colleagues (2023) explored the differences between VHA-delivered and VHA-purchased behavioral health care—treatment for psychiatric and substance use disorders—in service characteristics and in patient and provider characteristics. Based on the percentage of veterans using any community care for behavioral health in 2016–2019, approximately 20 percent of the behavioral health inpatient care was provided via community care as opposed to by VHA, and three percent of all behavioral health outpatient care was provided via community care. When comparing the types of providers veterans saw for behavioral health outpatient visits, Vanneman and colleagues (2023) found that the proportion of visits with psychiatry and behavioral neurology providers was approximately 22 percent in VHA (vs. 10% in community care) in 2016–2019. She emphasized that although these findings do not indicate the quality of care received, understanding what services veterans are receiving, determining what providers they are seeing in the community as compared to in VHA, and providing the appropriate services with the appropriate individuals to deliver them are all important next steps.
Lastly, Vanneman highlighted new, unpublished research on behavioral health admissions, which reviewed hospital discharge data from 10 states to determine what portion of behavioral health inpatient stays among veterans occurred across different settings. Preliminary findings indicated that 58 percent of the behavioral health inpatient stays occurred in VA
facilities and seven percent occurred in VA-purchased community care, but veterans were less likely to go to VA and more likely to seek community care for behavioral health inpatient care over time. Adjusted predictions demonstrated that behavioral health inpatient stays at VA (8.5 days) tended to be longer than in community care (5.5 days); costs at VA ($14,743) were considerably higher than those in community care ($5,442); and the readmission rate for VA (16%) was lower than that for community care (20%).
Vanneman described the implications of these research findings on both suicide prevention challenges and opportunities as VA-purchased community care continues to expand:
- Many unknowns remain—for example, whether community care versus VA-only care increases, decreases, or has no effect on suicidal crisis or suicide attempts.
- A delicate balance exists between expanding the Community Care Network and meeting provider requirements—for instance, VA is required to offer relevant training to community care providers, but community care providers are not required to complete this training.
- Information sharing is limited between VA and community care providers—in other words, community care providers might not receive all relevant patient information from VA, and VA providers do not have easy access to all relevant information from community care providers.
- Integrating VA and non-VA data for risk prediction and real-time impact is difficult.
- Enrollment in VA and connection to VA and non-VA services have been strengthened by recent policy changes. For example,
- the Sergeant First Class Heath Robinson Honoring Our Promise to Address Comprehensive Toxics (PACT) Act of 2022 will likely increase enrollment in VA;
- the Commander John Scott Hannon Veterans Mental Health Care Improvement Act (Hannon Act) focuses on mental health care during the transition from service member to veteran; and
- the Veterans Comprehensive Prevention, Access to Care, and Treatment (COMPACT) Act of 2020 focuses on emergent suicide care and treatment at VA and non-VA locations.
- Research and quality improvement efforts are under way to engage veterans in care and address upstream predictors of risk.
- A new contract with Community Care Network providers is forthcoming.
DISCUSSION
Timothy Strauman moderated a discussion between the workshop participants and Vanneman.
Workshop participant Benjamin Paul remarked that some service members and veterans feel mistreated and/or misunderstood during inpatient stays in civilian hospitals and have no desire to return to those facilities for care—VA facilities may allow for longer stays and offer care to meet patients’ unique needs. If a civilian hospital is the only option for care, he pointed out that a veteran might not seek care or might not stay as long as needed to receive treatment. Strauman commented that understanding the psychology of how people make these choices, whether they feel empowered, and how such choices affect future behavior is important as efforts to improve mental health care for veterans expand.
Caine posed a question about whether the nature of admission status (i.e., voluntary vs. involuntary) is considered when measuring patient satisfaction. Vanneman said that data on the nature of admission status are often difficult to obtain. She stressed that to truly understand differences in quality of care, more data—beyond claims data—would be beneficial.
An online workshop participant asked how reliance on VA and community care changed after the passage of the Choice Act and the MISSION Act, respectively. Vanneman described slight decreases in the reliance on VA (vs. community) care for primary care and mental health care among post-9/11 veterans following the Choice Act, even though veterans remain highly reliant on VA for primary care and mental health care. She also noted that analyses are being conducted on the Referral Coordination Initiative, which was implemented to engage veterans in decisions about where they receive their care—such work is critical to determine which activities influence veterans’ decision making.
Ahmedani agreed with Paul that veterans might be more comfortable interacting with people at VA health facilities. Furthermore, he noted that because private insurance companies often do not pay for additional days of hospitalization, civilian hospitals are notorious for discharging people as quickly as possible; veterans who say they feel fine just to get out of the hospital might be more likely to be readmitted. He highlighted the value of additional research on the dynamics of how private hospitals and VA pay for care. Vanneman explained that VA pays for community care at the Medicare rate, adjusted for locality. VA uses standardized episodes of care, which are bundled services but not bundled payments. She commented that research is under way in this important area.
Referencing Vanneman’s preliminary findings that VA costs are higher than those in community care for a patient’s behavioral health inpatient stay, Ahmedani pointed out that reducing readmissions could reduce the
total cost of care for a patient. Vanneman indicated that considering both initial costs and downstream costs is important, as is understanding the effects of these costs. Furthermore, different factors influence these costs—for example, certain criteria (e.g., related to length of stay) apply in the private sector but not in VA. She referenced another study that found that VA costs were lower than those in the private sector when calculating the costs associated with 28 days of services following an emergency department visit.
REFERENCES
Ahmedani, B. K., Simon, G. E., Stewart, C., Beck, A., Waitzfelder, B. E., Rossom, R., Lynch, F., Owen-Smith, A., Hunkeler, E. M., Whiteside, U., Operskalski, B. H., Coffey, M. J., & Solberg, L. I. (2014). Health care contacts in the year before suicide death. Journal of General Internal Medicine, 29(6), 870–877. https://doi.org/10.1007/s11606-014-2767-3
Ahmedani, B. K., Westphal, J., Autio, K., Elsiss, F., Peterson, E. L., Beck, A., Waitzfelder, B. E., Rossom, R. C., Owen-Smith, A. A., Lynch, F., Lu, C. Y., Frank, C., Prabhakar, D., Braciszewski, J. M., Miller-Matero, L. R., Yeh, H.-H., Hu, Y., Doshi, R., Waring, S. C., & Simon, G. E. (2019). Variation in patterns of health care before suicide: A population case-control study. Preventive Medicine, 127, 105796. https://doi.org/10.1016/j.ypmed.2019.105796
Coffey, M. J., Coffey, C. E., & Ahmedani, B. K. (2015). Suicide in a health maintenance organization population. JAMA Psychiatry, 72(3), 294–296. https://doi.org/10.1001/jamapsychiatry.2014.2440
Department of Veterans Affairs. (n.d.). Community-based interventions for suicide prevention overview. https://www.prainc.com/wp-content/uploads/2022/09/CBI-SP-Overview-508.pdf
___. (2018). National strategy for preventing veteran suicide 2018–2028. https://www.mental-health.va.gov/suicide_prevention/docs/Office-of-Mental-Health-and-Suicide-Prevention-National-Strategy-for-Preventing-Veterans-Suicide.pdf
___. (2022). VA S.A.V.E. training: Supporting our veterans. https://www.mentalhealth.va.gov/suicide_prevention/docs/VA_SAVE_Training.pdf
Giroir, B. P., & Wilensky, G. R. (2015). Reforming the Veterans Health Administration. New England Journal of Medicine, 373(18), 1693–1695.
Gordon, S. H., Beilstein-Wedel, E., Rosen, A. K., Zheng, T., Kelley, A. T., Cook, J., Zahakos, S. S., Wagner, T. H., & Vanneman, M. E. (2021). County-level predictors of growth in community-based primary care use among veterans. Medical Care, 59(Suppl 3), S301–S306. https://doi.org/10.1097/MLR.0000000000001555
Hampton, T. (2010). Depression care effort brings dramatic drop in large HMO population’s suicide rate. JAMA, 303(19), 1903–1905.
Richards, J. E., Simon, G. E., Boggs, J. M., Beidas, R., Yarborough, B. J. H., Coleman, K. J., Sterling, S. A., Beck, A., Flores, J. P., Bruschke, C., Goldstein Grumet, J., Stewart, C. C., Schoenbaum, M., Westphal, J, & Ahmedani, B. K. (2021). An implementation evaluation of “Zero Suicide” using normalization process theory to support high-quality care for patients at risk of suicide. Implementation Research and Practice, 2, 1–14. https://doi.org/10.1177/26334895211011769
Substance Abuse and Mental Health Services Administration. (2019). A guide to SAMHSA’s Strategic Prevention Framework. https://www.samhsa.gov/sites/default/files/20190620-samhsa-strategic-prevention-framework-guide.pdf
Vanneman, M. E., Wagner, T. H., Shwartz, M., Meterko, M., Francis, J., Greenstone, C. L., & Rosen, A. K. (2020). Veterans’ experiences with outpatient care: Comparing the Veterans Affairs system with community-based care. Health Affairs, 39(8). https://doi.org/10.1377/hlthaff.2019.01375
Vanneman, M. E., Rosen, A. K., Wagner, T. H., Shwartz, M., Gordon, S. H., Greenberg, G., Zheng, T., Cook, J., Beilstein-Wedel, E., Greene, T., & Kelley, A. T. (2023). Differences between VHA-delivered and VHA-purchased behavioral health care in service and patient characteristics. Psychiatric Services, 74(2), 148–157. https://doi.org/10.1176/appi.ps.202100730
Veterans Health Administration. (2022). About VHA. va.gov/health/aboutvha.asp
This page intentionally left blank.

















