Effects of Health Programs on Child Mortality in Sub-Saharan Africa (1993)
Chapter: 3 Immunization Programs
3
Immunization Programs
The Expanded Programme on Immunization (EPI), with recommended guidelines established by the World Health Organization, is a major international effort to increase the proportion of children covered by basic immunizations against childhood diseases. Because of Africa's unusually high rates of child mortality from measles, the prevalence of tuberculosis, and in many places, substantial mortality due to neonatal tetanus, EPI plays a central role in the health strategy for Africa. In addition, the low levels of funding for health programs in Africa have forced many countries to focus their scarce resources on what are perceived as the most cost-effective interventions, which include EPI (Walsh and Warren, 1979).
In general, the vaccines that form the core of EPI programs are measles, diphtheria-pertussis-tetanus, poliomyelitis, bacille Calmette-Guérin (BCG) for tuberculosis, and tetanus for pregnant women or women of childbearing age. Each of these vaccines has been proven efficacious to varying degrees. However, vaccine efficacy does not necessarily imply that a program based on vaccinations is effective in reducing mortality. There are two reasons that programs might be less effective than suggested by the efficacy of the vaccines. First, as pointed out in Chapter 2, child mortality in Africa often results from the interaction of several diseases, frequently including malnutrition (although malnutrition, in many cases, may be a consequence of infectious and parasitic diseases). The interactions among different childhood diseases are so complex that it is difficult to estimate the effect of reducing the incidence of a single disease by using mathematical simulations.
The EPI programs in most African countries have achieved large increases in the proportion of children who receive all of the standard vaccinations. Figure 3-1 shows the proportions of children aged 12-23 months that had received all the standard vaccinations, based on data from the Demographic and Health Surveys conducted in the mid- to late 1980s. Given the relatively high levels in some countries, it is possible that these programs have had a substantial effect on infant and childhood mortality. Because most of the increase in vaccination coverage occurred after 1985, many of the children born shortly before the survey have a higher likelihood of being vaccinated than their older siblings. However, the effect of these programs on child mortality may be too recent to be evident in the available demographic data for most countries. Moreover, although the trends in immunization coverage are upward, coverage can vary greatly on
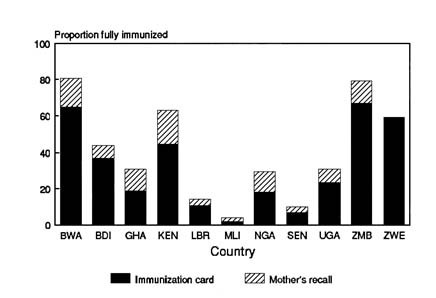
FIGURE 3-1 Proportion of fully immunized children 12-23 months of age, selected sub-Saharan African countries. NOTE: Based on immunization cards and mothers' recall. BWA—Botswana, BDI—Burundi, GHA—Ghana, KEN-Kenya, LBR—Liberia, MLI—Mali, NGA—Nigeria, SEN—Senegal, UGA—Uganda, ZMB—Zambia, ZWE —Zimbabwe. SOURCE: Demographic and Health Survey reports (see Appendix B).
a year-to-year basis, especially among programs depending on special vaccination programs.
Generally, statistics gathered for the EPI program at the national level focus on specific immunizations rather than the proportion of fully immunized children. The goal of the African Region EPI program for 1990 was to make immunizations available for all infants and to achieve coverage of at least 75 percent for all six EPI vaccines. As of August 1991, the immunization coverage for children 12 to 23 months of age in Africa was estimated to have reached 79 percent for BCG, 57 percent for the third dose of the diphtheria-pertussis-tetanus (DPT) vaccine, 56 percent for the third dose of the oral poliomyelitis vaccine, and 54 percent for the measles vaccine. Although the goals have not yet been achieved, comparison with coverage in 1982 of approximately 28 percent for BCG, 21 percent for poliomyelitis, and 18 percent for measles suggests that vaccination coverage has increased greatly as the EPI program became activated (Expanded Programme on Immunization, 1992).
The following sections examine the evidence that vaccination programs against measles, pertussis, tuberculosis, and tetanus have reduced child mortality. Most of the research on EPI programs has focused on measles. The reasons for this emphasis include the high mortality rates from measles, its relative ease of diagnosis, and the potential of program failure because of improper vaccine handling. Much less research exists on pertussis, tuberculosis in children, and tetanus. However, there are several indications of the potential effects of these programs.
We have not reviewed the literature on two of the EPI diseases: poliomyelitis and diphtheria. We have not included polio because of the low number of deaths from this disease. However, several African studies suggest that poliomyelitis vaccination campaigns can reduce the incidence of disease and paralysis (Rodrigues, 1991; Deming et al., 1992), despite the vaccine's lower efficacy in Africa than in developed countries (Oduntan, 1978; Böttinger et al., 1981; Expanded Programme on Immunization, 1990; de Swardt et al., 1990).
Diphtheria has a low incidence rate in sub-Saharan Africa because of high levels of acquired immunity, but can have a high case-fatality rate (Rodrigues, 1991). This immunity may be due to widespread, relatively mild, subclinical cases. Among children diagnosed with diphtheria, the case-fatality rate is high. Relative to other diseases, diphtheria is apparently not a major cause of death among African children. One study suggests that DPT vaccination in Sudan has reduced the incidence of diphtheria (Loevinsohn, 1990). We know very little about the role of diphtheria in African mortality because no reliable sources of community-based data exist, nor is there information about the contribution of diphtheria vaccine to the effect of vaccination programs in Africa (Rodrigues, 1991).
Several vaccines that are included in immunization programs in some parts of the African continent are not reviewed here. In particular, yellow fever and meningitis vaccines are used to control epidemics in parts of West Africa.
MEASLES
As discussed in the introduction to this chapter, measles is one of the leading causes of infant and child mortality in sub-Saharan Africa. Here, we review the state of knowledge on measles. We begin with a discussion of the epidemiology and vaccine efficacy. A discussion on why Africa may be different from other parts of the world with respect to measles follows. Measles immunization programs are then examined, with a focus on their effects, the relationship between immunization coverage and measles mortality, and program history and coverage. Finally, treatment strategies are discussed.
EPIDEMIOLOGY
Measles is caused by a paramyxovirus called morbilli. It is highly infectious and transmitted from person to person via droplet spread (sneezes or coughs) or through direct contact with nasal or throat secretions of infected persons. The incubation period of approximately 10 to 12 days is followed by cough, nasal congestion, and conjunctivitis. The characteristic rash appears about two to four days after the onset of other symptoms. The total illness generally lasts 7 to 10 days (Orenstein et al., 1986). A case of measles provides lifetime protection, and repeat cases are rare. The symptoms of the disease are well known in Africa, and there are local names for it in many languages. Common complications include otitis media (inner ear infections), laryngitis, pneumonia, diarrhea, and encephalitis.
Measles is one of the major causes of death among children in Africa. It is a contributing factor in 8 to 10 percent of deaths among African children (Ofosu-Amaah, 1983; Rodrigues, 1991). The proportion is even higher in many parts of the continent. For example, a study in Senegal in 1963-1965 found that measles deaths accounted for 26 percent of deaths among children ages 1 to 4 and 19 percent of all deaths under age 5 (Cantrelle, 1968). During epidemic years, measles can be responsible for 50 percent of all deaths at ages 1 to 4 years (Garenne and Cantrelle, 1986).
Because measles often leads to severe diarrhea or respiratory infections, it is probably an underlying cause of many more child deaths. For example, a study in Bangladesh (Clemens et al., 1988) found that measles vaccination reduced the odds of dying from diarrhea by 59 percent, the odds
from respiratory illness by 22 percent, and the odds from malnutrition (i.e., ''swelling or edema") by 47 percent. Feachem and Koblinsky (1983) listed measles immunization as one strategy for reducing child mortality from diarrheal diseases. They calculated that measles immunization at the age of 9-11 months, with coverage of 45 to 90 percent might avert 6-26 percent of diarrhea deaths among children less than 5 years of age.
Although respiratory and gastrointestinal infections often occur during or in the month after measles cases, excess mortality can continue for many months. Hull et al. (1983) followed children who had measles and compared their overall mortality with that of children who did not have measles. Half of the extra deaths among children who had measles occurred three to nine months after the case. Therefore, studies that ascribe death in the one to three months following a case as measles deaths may be understating the true effect of measles on mortality rates. One possible explanation for the long-term effect of measles is the growth retardation that often follows. The Kasongo Project Team (1986) documented that three months after the onset of measles, growth retardation was still apparent based on both weight-for-age and weight-for-height relative to local standards, as discussed in Chapter 5. Another possible explanation is an alternation of physical defense mechanisms or a decrease in immunocompetence because of the measles virus.
VACCINE EFFICACY
There are several measles vaccines in use today. The most common in Africa is the Schwarz vaccine, an attenuated live vaccine introduced in 1966. During the 1980s, this and other measles vaccines were modified to increase their stability and, thereby, their effectiveness. A second vaccine, the Edmonston-Zagreb, has recently been tested in high doses as a way of lowering the standard age at which the vaccination can be given.
Several studies, most of them prospective studies based in communities, have estimated the efficacy of measles vaccine, which is its ability to prevent measles when used in carefully controlled trials. In a recent clinical trial conducted in Senegal, the efficacy of the Schwarz measles vaccine given at 10 months of age was 98 percent (the 95 percent confidence interval (C.I.) was 86-100 percent; Garenne et al., 1992). A study by Hull et al. (1983) estimated that measles vaccine efficacy in The Gambia was 89 percent in children more than 9 months of age (95 percent C.I. 77-94 percent). Lamb (1988) estimated an efficacy of 90 percent for The Gambia. These estimates are close to those from Europe and North America (e.g., Miller, 1987; Rebiere et al., 1990).
However, a study by Aaby et al. (1990b) estimated a lower vaccine efficacy of only 46 percent (95 percent C.I. 7-69 percent) in Bandim district
in Guinea-Bissau, among children born in 1984-1985. Even after assuming that the vaccine was not effective until 35 days after the injection, they still estimated that its efficacy was only 68 percent (95 percent C.I. 39-84 percent). This low efficacy was not due to vaccine failure since antibody tests of vaccinated children showed rates of seropositivity greater than 95 percent. It is also unlikely that this low estimate is a result of either misclassification of vaccination status or inappropriate age at vaccination.
The effectiveness of measles vaccines may be lower in field conditions than in carefully conducted studies because of inappropriate storage of the vaccine (cold chain failures), inappropriate age at vaccination, or other incorrect vaccination procedures (e.g., Cutts et al., 1990a).
A recent study of children vaccinated at the Institute of Child Health at University College Hospital in Ibadan, Nigeria (Adu et al., 1992) suggests that vaccine effectiveness might be a serious problem. Only 55 percent of children seroconverted after vaccination, and 87 percent of these had low antibody levels. The vaccines came from four different manufacturers and nine batches. The authors suggested that this low efficacy may have been a result of cold chain failures.
Attempts to measure effectiveness of large immunization programs are complicated by problems in verifying both vaccination status and measles cases. For example, a study in Mozambique found that adjustments for the estimated accuracy of mother's reports of measles cases raised the estimated vaccine efficacy from 37 to 66 percent (Cutts et al., 1990a). A similar study in Tanzania found an efficacy of 54 percent based on mother's recall of vaccination status compared to an estimate of 96 percent based on clinic cards (Killewo et al., 1991).
Garenne et al. (1992) used health cards, as well as clinical and serological records, to estimate the efficacy of vaccines delivered by the national vaccination campaigns in the study area of Niakhar, Senegal, in 1986-1987. They estimated the vaccine efficacy for those children immunized at 86 percent (95 percent C.I. 77-92 percent). This estimate represents a failure rate five times greater than that found in clinical trials using the same vaccine in the same area. Porter et al. (1990) examined vaccine efficacy in five refugee camps in Malawi. They based their calculations on the vaccination status of children who had a health card (which indicates immunizations definitely received) and estimated efficacy to be greater than 90 percent.
These studies suggest that vaccine efficacy is very high in Africa in carefully controlled studies. However, in programs, vaccine failure can be a serious problem. Therefore, we cannot simply assume that high coverage rates necessarily imply that large proportions of children are protected against measles.
There are some studies in other continents that demonstrate the effectiveness
of measles vaccination in reducing mortality. For example, a study in Bangladesh (Koenig et al., 1990) found that mortality among vaccinated children ages 9 to 60 months was about 40 percent lower than among a matched group of unvaccinated children. This difference remained after controlling for differences in socioeconomic status and after several tests for selectivity in the acceptance of vaccination.1
WHY AFRICA MIGHT BE DIFFERENT
Measles is a more significant factor in child mortality in Africa than in other areas of the world. One reason for this higher significance is that the high fertility rates in Africa quickly replenish the population of children who have not had measles. In cities, this replenishment leads to frequent epidemics and a younger mean age of cases than was true in Europe before the availability of measles vaccine. Differences in residence patterns between Africa and other areas of the world, with extended families living in enclosed areas in some parts of Africa, can lead to higher case-fatality rates (see below).
Estimates of the case-fatality rate for measles suggest that it is unusually severe in some parts of West Africa (Aaby, 1988). The high case-fatality rate is probably not due solely to the young age distribution of cases because the epidemic in southwestern Ethiopia also exhibited very high case-fatality rates, despite 22.6 percent of cases having occurred among children aged 5 to 10 years and 5.9 percent in children 11 years or older (Lindtjorn, 1990). Although the high prevalence of malnutrition is often mentioned as a reason for high case-fatality rates, the evidence is inconclusive (see discussion of nutrition and measles in Chapter 5). It is likely that the high case-fatality rates are related to the low level of health services available in many areas and the high proportion of secondary cases in households (discussed in detail below).
Another feature of measles in Africa is that measles vaccination is effective at earlier ages than is true in developed countries because maternal antibodies wane earlier in African children. This reduction in immunity is
apparently due to lower levels of maternal antibodies and less efficient transport of antibodies to the fetus (Black et al., 1986). There is some evidence that children born to mothers who are positive for human immunodeficiency virus (HIV) may have even poorer transport of measles antibodies and a higher risk of measles infection before age 9 months than other children (Embree et al., 1992).
The recommended age for vaccination is 9-11 months for tropical Africa, compared to 12-15 months for Europe and the United States (Kenya Ministry of Health and World Health Organization, 1977; Expanded Programme on Immunization, 1982). In some areas, programs have lowered the age for measles vaccination to 6 months. In a study in The Gambia, the efficacy dropped to 37 percent when administered at 6-8 months of age (Hull et al., 1983). Therefore, regular vaccination before 9 months of age is generally not recommended unless it is possible to provide a second does after age 9 months. Studies of the use of high-titer vaccines (i.e., vaccines with high levels of the attenuated virus) on younger children (4-6 months) show reasonable levels of seroconversion and efficacy in preventing measles cases (Whittle et al., 1984, 1988; Aaby et al., 1988b), but low efficacy in reducing mortality (Garenne et al., 1991).
EVIDENCE OF MORTALITY AND MORBIDITY EFFECTS FROM AFRICA
There are quite a few studies of the effect of measles vaccination on both mortality and the incidence of disease in Africa. The following sections first review the evidence that vaccination against measles can reduce mortality in Africa, then the evidence that programs have reduced the incidence of measles cases.
There are several studies that examine the effect of measles vaccination on child mortality rates in sub-Saharan Africa. These studies can be divided into two groups: (1) studies that measure the effect of regular measles immunization programs on mortality, and (2) studies of effects in model programs limited to special research areas. The former evaluations are closer to our main interest because they examine the effect of large-scale programs. The second group of studies demonstrates what can be accomplished in carefully managed programs. These studies provide evidence of the relationship between changes in the incidence of measles and reductions in overall child mortality.
Effects of General Measles Immunization Programs
Garenne et al. (1985) studied the effect of the national vaccination program in Senegal. The program increased coverage with measles vaccine
nationally from a few percent in the early 1960s to 74 percent for 1967 and 1968. After 1968, coverage dropped for several years. Garenne et al. (1985) provided data showing that the annual number of measles cases reported nationally dropped by 35 percent in 1967-1971 compared to 1963-1966, corresponding to the national vaccination campaign in 1967-1969. They also show that the proportion of deaths ascribed to measles decreased substantially in the two rural study areas of Ngayokhème and Ndemène (among deaths at ages 0-14 years) and in Dakar (deaths at all ages).
After a brief drop, vaccination coverage in Senegal remained greater than about 75 percent nationally for 1974-1979 (Garenne et al., 1985). Even so, the number of children seeking medical attention for measles returned to high levels. In addition, the proportion of child deaths due to measles returned to high levels for 1972-1978 in Ngayokhème and Ndemène, areas covered by continuous registration of deaths.
Two studies in Guinea-Bissau, one in an urban area (Bandim; Aaby et al., 1984b) and one in a rural area (Quinhamel; Aaby et al., 1984a), were natural experiments brought about by the introduction of measles vaccination in preexisting research areas. In Bandim, the mortality rate among children aged 6-35 months was 127 deaths per 1,000 in 1979. After a measles vaccination campaign, the rate dropped to 47 in 1980 and 48 in 1981. During 1980 and 1981, the mortality rates for vaccinated children were much lower than the rates among unvaccinated children (Aaby et al., 1984b). Mortality was also lower among vaccinated children than among children who had previously had measles. In Quinhamel, the rates were 107 per 1,000 in 1979 and 98 per 1,000 in 1980. After a measles vaccination campaign in early 1981, the rate was 44 among the vaccinated and 72 among the unvaccinated (Aaby et al., 1984a). Quinhamel was the only one of five rural areas studied where measles was a problem during the study period (Aaby, 1988).
Effects of Measles Vaccinationin Field Trials and Model Programs
There have been several field trials in defined study populations that were specifically designed to measure the effects of vaccination on mortality. In addition, several model programs have demonstrated the potential of programs. These studies offer more information than vaccine trials because they provide estimates of both the direct and the indirect effects of vaccination. In particular, the measured effects from these studies include the reduction of mortality from diarrhea, respiratory infections, and malnutrition. In vaccine trials, some of these deaths would not be recognized as resulting from measles. If continued for a sufficiently long time, these studies also can show changes in the frequency of epidemics and the resulting
change in the age distribution of cases. Similarly, these studies are often superior to evaluations of general health programs since they are often based on more scientific study designs. For example, they can include control areas, randomization, or estimation of the effect of the program on those who actually received services.
However, these special studies can present a misleading picture of the likely effect of real programs. One reason is that large-scale programs rarely match the high level of supervision and training achieved in smaller programs. It is possible, therefore, that large-scale programs might have more cold chain failures and be less likely to reach the most vulnerable parts of the population. A second reason is that it is easier to carry out field trials in populations where measles is a frequent health problem. In particular, it is not feasible to test the effect of a measles program in an area that experiences measles epidemics only every three to five years. It is also more difficult to carry out these studies in urban areas because of high rates of population mobility. Finally, areas used in research studies often have better access to general health services than other rural areas.
Vaccine Field Trial in Khombole, Senegal
Garenne and Cantrelle (1986) estimated the efficacy of the Schwarz vaccine using data from field trials in Khombole, Senegal, in 1965-1968. They found that the proportion dying between ages 6 months and 10 years was 26 percent lower among children in the area receiving vaccinations than among children in the control area. It is possible that these results might be affected by other factors related to the selection of the children who were vaccinated. Vaccinations were offered to all children in the vaccination zone. Sixty percent of eligible children were vaccinated in 1965 and 86 percent were vaccinated in 1967. However, because of the nature of the program and the lack of large socioeconomic differentials within the study population, it is unlikely that the results are an artifact of selectivity.
Kasongo Project in Zaire
The Kasongo Project Team (1981) compared mortality in two areas of rural Zaire. In one area, a measles vaccination program achieved a coverage rate of 83 percent among the cohort born between September 1974 and October 1975.2 In the test area, the mortality rate between 7 and 35 months
of age was 95 deaths per 1,000 for the unvaccinated cohort born between June 1973 and August 1974. The rate dropped to 48 per 1,000 for the cohort covered by the vaccination program. In the control area, the rate fell from 80 to 69 over the same period. Therefore, mortality was reduced by 36 deaths per 1,000 more in the vaccination area than in the control area, a difference that was not statistically significant. The Kasongo Project Team suggested that the gains from vaccination appeared to have been reversed at later ages. This conclusion is not warranted by the data they present. Mortality at ages 22-35 months of age increased by 7 per 1,000 in the control area but by only 1 per 1,000 in the vaccination area. These estimates were not significantly different. Data for children beyond age 36 months are not presented.
Pahou Primary Health Care Project, Benin
The Pahou project measured the effect of primary health care services established in 16 villages 30 kilometers from Cotonou, Benin. Velema et al. (1991) matched each child who died between 4 and 35 months of age with up to four controls of the same age and sex from the same village. A comparison of the vaccination status of cases and controls showed that children vaccinated before 12 months of age experienced a relative risk of death between 4 and 35 months of 0.36, compared to nonvaccinated children (95 percent C.I. 0.16-0.81 times). 3 However, vaccination after 12 months of age was not associated with reduced mortality (relative risk: 1.02 times, 95 percent C.I. 0.43-2.41 times). These results remained after the addition of controls for socioeconomic status, nutritional status, and other measures of the effect of primary health care. These data cannot be used to estimate the change in mortality associated with vaccination because the study did not provide mortality rates for the population.4
Estimates of Effect from Cases of Vaccine Failure
A study in Guinea-Bissau by Aaby et al. (1989) compared children who seroconverted after measles vaccination with a group for whom the vaccination
failed. The proportion dying between ages 6 and 35 months from all causes was less than one-third the rate among those who seroconverted (4.5 per 1,000 compared to 15.1 per 1,000). The advantage of this study is that the unprotected children were selected by the random timing of vaccine failure. Therefore, there is no reason to believe that the unvaccinated children in the study differed from the vaccinated children in socioeconomic status, maternal beliefs, or any other potentially confounding characteristic.
Effect of Programs on Incidence in Africa
Studies of the mortality effect of measles immunization demonstrate the effectiveness of programs based on the standard vaccination regimen. If these programs based on the standard vaccines and standard age schedule for vaccination are having an effect, we should be able to determine their effectiveness through changes in the incidence of measles or the incidence of cases treated at health facilities. If a large enough number of children at risk of measles receive a potent vaccine to reduce the incidence of disease, it should be possible to document the effect on disease incidence.
Changes in the observed incidence of measles can be compared with the predictions of mathematical models. These models predict two changes that may occur when vaccination coverage increases. First, there might be a change in the frequency of measles epidemics. It is not easy to predict the change that will result from a given level of coverage because populations differ substantially in the degrees of contact between children. However, if vaccination coverage increases sufficiently, epidemics will be less frequent during the years immediately after the start of the vaccination program (Cutts et al., 1991). Second, there might be a substantial change in the age distribution of cases, which is discussed later in the chapter.
Several studies have documented dramatic changes in the incidence of measles following large increases in vaccination coverage. One of the earliest demonstrations of the potential effect of measles vaccination in Africa is based on data from 10 countries in West Africa that were included in a regional program to eradicate smallpox and control measles that began in 1967. By aggregating the data from about 150 geographical units in these countries according to the start of the vaccination program, Foege (1971) showed that the number of measles cases dropped by 54 percent in the year following, compared to the 12 months preceding, the start of the program.
Foege (1971) also presented more detailed data from The Gambia that provide a dramatic demonstration of the reduction of measles cases after the first national measles vaccination campaign. Figure 3-2 shows the number of measles cases in five regions of The Gambia during each four-week period of 1967 and 1968. Each region had a measles campaign during
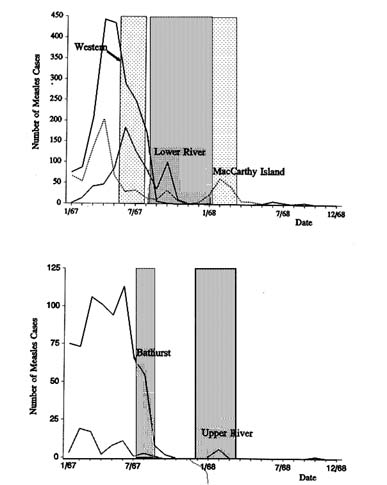
FIGURE 3-2 Effect of measles vaccination coverage on measles cases (by four-week period), five areas of The Gambia. NOTE: Shaded areas indicate periods of initial vaccination campaign in each area. SOURCE: Foege (1971).
different months of 1967 and early 1968. The campaign targeted all children aged 6 months to 4 years and achieved a coverage rate of 96 percent. Although the numbers of measles cases had begun to drop in several of the regions, they dropped dramatically, to zero in many cases, following the campaign in each region. By June 1968, measles transmission had been interrupted. There were only 16 cases during 1969 and 1970, and most of them were imported.
The campaigns begun in the late 1960s did not lead to a large-scale program of continuous vaccination with high coverage rates. However,
data are available for several countries that increased their vaccination coverage rates during the 1980s. For example, vaccination coverage in Malawi increased from 10 percent in 1976-1978 to about 60 percent in 1985-1987. Surveillance data show that the number of cases in the later period was only about half of the number reported a decade earlier (Expanded Programme on Immunization, 1989). Similarly, Cutts et al. (1991) found that the reported number of cases of measles in Burundi decreased by more than 50 percent between 1981 and 1988. Vaccination coverage in 1986-1988 averaged more than 60 percent, compared to about 20 percent in 1980. They also found that in Rwanda, the reported incidence in 1988, when coverage was greater than 80 percent, was only 3 percent of the rate reported before the start of immunization program. Similarly, data for Lesotho show a large drop in reported incidence rates as vaccination coverage increased.
Dabis et al. (1988) examined the decline in reported measles cases in Pointe-Noire, Congo, during implementation of the Expanded Programme on Immunization, which began there in January 1982. The estimated coverage rate increased to 31 and 37 percent, respectively, in 1982 and 1983, and to 47 percent in 1984 and 1985. A community survey in 1985 estimated that 54 percent of the children 12-23 months of age had documented evidence of vaccination against measles. Measles had been endemic in Pointe-Noire since at least 1979, with annual epidemics. Data on hospital admissions for measles showed that the monthly number of measles cases dropped to very low figures during late 1983 and early 1984, instead of rising for the annual epidemic. In addition, between 1983 and 1985 (both epidemic years), the hospitalization rate for measles among children 9 to 23 months of age dropped by 49 percent. This decline was associated with an increase in the proportion of hospitalized cases less than 9 months of age from 13 to 17 percent.
A study in Yaoundé, Cameroon, in 1974-1979 showed that the number of recorded measles cases dropped by 44 percent when the cold chain was improved and the minimum age at vaccination was increased from 6 to 9 months (Heymann et al., 1983). Despite the increase in the minimum age at vaccination, the number of cases dropped in all age groups, including less than 9 months.
NONLINEARITIES IN RELATIONSHIP BETWEEN COVERAGE AND EFFECT
The potential effect of measles vaccination on mortality can vary substantially across populations and programs. First, the potential effect of programs will differ according to the epidemiology of measles in various populations, including features such as the frequency of epidemics and the intensity of infections. Second, the relationship between vaccination coverage
and mortality is not simple. For example, a 40 percent coverage rate might be sufficient to disrupt a pattern of annual epidemics in a small town with low fertility rates. A large city with high fertility would require a much higher coverage rate to achieve the same result. The studies reviewed above demonstrate that a vaccination program in Africa that reduces the incidence of the disease will reduce mortality as well. However, it is difficult to estimate how much mortality will decline in any given situation.
The following sections describe the factors that determine the relationship between vaccine coverage and mortality reduction.
Vaccination and Frequency of Epidemics
An increase in the proportion of the population protected by vaccination can change the whole epidemiology of the disease. For example, an effective vaccination campaign can virtually stop transmission of the disease for two to three years. The level of coverage required to achieve this result depends on the density of the population, the fertility rate, and local practices that affect transmission rates (e.g., migration patterns).
Effect of Vaccination on Age Distribution of Cases
The age distribution of cases is important for two reasons. First, because case-fatality rates are highest among cases under 12 months of age, a change in the age distribution of cases can change the case-fatality rate. Second, in some populations, the best evidence of the effect of the program comes from a change in the number and age distribution of cases seen at hospitals and health centers.
Programs designed to increase the coverage of measles vaccination generally reduce incidence rates at all ages. However, because the biggest declines are often concentrated at ages 12-35 months, there is often a change in the age distribution of cases observed in hospitals and clinics. A sudden increase in program effort often leads to a temporary drop in the proportion of cases at 12-35 months of age and an increase in the proportion of cases among children more than 5 years of age. The proportion over age 5 increases in some populations because without vaccination, most children get measles before this age. If vaccination coverage increases the interval between epidemics or leads to smaller isolated epidemics, some children escape measles until later ages. For example, Aaby et al. (1988a) reported that in Guinea-Bissau, greater vaccination coverage increased the proportion of cases over age 5 from 22 to 29 percent. Change in the age distribution of cases is a useful indicator of program effectiveness. These changes can often be documented through surveillance systems when complete population surveys are not available. For example, in the city of Maputo, Mozambique,
TABLE 3-1 Proportion of Measles Cases Among Children Over Age 5 Years in Areas Where Vaccination Coverage Has Remained High
Country | Vaccine Coverage (%) | Reported Cases >5 years (%) |
Burundi | 57 | 35 |
Lesotho | 78 | 62 |
Rwanda | 86 | 31 |
Swaziland | 74 | 41 |
The Gambia | 90 | 50 |
SOURCES: National data from Cutts et al. (1991), except for The Gambia, for which data are from Keneba, reported by Lamb (1988). | ||
vaccination coverage increased from 42 percent in 1982 to 86 percent in 1986. Data on cases reported by health centers showed a shift in the proportion of cases over 5 years of age from about 10 percent in 1982-1983 to 28 percent in 1986 and 40 percent in 1987 (Cutts et al., 1990b).
After a program has maintained high coverage levels for several years, the proportion of children over age 5 protected by vaccination will increase. However, that proportion can still remain high. Table 3-1 presents the proportion of cases over age 5 in five areas in which vaccination coverage had remained greater than 50 percent for several years. After vaccination levels have remained high for many years, it may be useful to consider providing a second dose to older children. This strategy will protect those who were missed initially and those who were not protected adequately by the first dose, although the mortality effect will be lower with the second dose than with the first.
Increases in vaccination coverage may result in an increase in the proportion of cases less than 12 months of age. Because the case-fatality rate is highest among infants, increasing the proportion of cases in this age group is likely to raise the overall case-fatality rate. During the years when coverage is high, there are fewer cases among children age 1-3 because of the vaccination, and still fewer cases over age 5 because these children have either been vaccinated or had measles. Therefore, the proportion of cases under 1 year of age is likely to increase, at least in the short run. For example, in Pointe-Noire, Congo, the proportion of hospitalized cases at 0-8 months of age increased from 13 to 17 percent when vaccination coverage increased from about 30-35 percent to 45 percent (Dabis et al., 1988). Similarly, Taylor et al. (1988) reported on the trends in measles in Kinshasa, Zaire. Between 1977 and 1983, coverage with measles vaccine increased from 37 to 62 percent among children age 12-23 months. Between 1983 and 1985 it
remained between about 50 and 60 percent. Despite this high rate of coverage, measles epidemics continued in alternate years between 1980 and 1985. Surveillance data from hospitals and health centers and a community survey showed that the proportion of cases among children less than 1 year of age increased with increasing vaccination coverage.
The new equilibrium age distribution of cases depends on the pattern of measles in the population and the nature of the vaccination program. For example, in Maputo, Mozambique, the proportion of reported cases less than 9 months of age increased slightly from 19 percent in 1982 to 22 percent in 1985. The proportion then dropped to 15 percent in 1987 (Cutts et al., 1990b). On the other hand, Aaby et al. (1988a) report almost no change in Guinea-Bissau in the proportion of cases under age 12 months—rising only from 17 to 18 percent.
Data from health facilities can exaggerate the increase in the proportion of cases among infants. Since younger children often have more severe cases (in part because they are more likely to be secondary cases), infants are overrepresented at health facilities. Because vaccination reduces the number of cases at 12-18 months of age (which also have higher severity), the proportion of hospitalized patients under 1 year is apt to increase substantially. In Machakos, Kenya, the percentage of cases among infants was twice as large for hospitalized cases as for all cases (Muller et al., 1977). In Kinshasa, 45 percent of cases reported in hospitals and clinics between 1980 and 1985 were less than 1 year of age, while in a community study, only 37 percent were infants (Taylor et al., 1988). Similarly, in an outbreak in Kampala, Uganda, in 1990, 28 percent of measles patients in hospitals were less than 9 months of age. However, a community survey about three months later reported that only 11 percent of cases were children under 12 months of age (Expanded Programme on Immunization, 1991).
It is important to stress that these changes in the age distribution of cases do not reflect changes in the incidence rate among infants. Vaccination programs reduce the incidence of measles among children under age 12 months. However, the case rates at older ages often decline more than those at the youngest ages, and therefore the proportion of cases at each age will change.
As coverage increases, the proportion of cases associated with vaccine failure will increase. This shift does not imply an increase in the proportion of vaccinations that fail. Instead, it reflects the increasing number who are vaccinated and consequently at risk of vaccine failure. Therefore, it is not possible to monitor changes in program effectiveness merely by documenting the number of vaccine failures or the proportion of cases associated with vaccine failure.
Changes in the Proportion of Secondary Cases
One reason case-fatality rates decrease with age is that younger children are more likely to become infected through contact with an older household member. Numerous studies have demonstrated that secondary cases of measles in a household (i.e., those who are infected by another household member) have a higher case-fatality rate than isolated cases (Aaby et al., 1984a,c; Hull, 1988; Koster, 1988; Lamb, 1988; Pison and Bonneuil, 1988; Aaby and Leeuwenberg, 1990; Garenne and Aaby, 1990). The higher case fatality may be a result of higher doses of virus associated with closer continuous contact between children in the same household.
If a vaccination program reduces the proportion of secondary cases, the case-fatality rate can drop substantially. For example, Aaby et al. (1988a) reported that the proportion of isolated cases increased from 16 percent before the vaccination program to 33 percent over the next three years. This change was largely responsible for a drop in the case-fatality rate of children under age 12 months from 28 to 17 percent—although this latter figure is still very high.
The change in the proportion of secondary cases will depend on the way in which vaccinations are distributed in the population. For example, if vaccination coverage remains low in a segment of the population with large families (e.g., polygamous households), then the proportion of secondary cases could increase. On the other hand, as the interval between epidemics increases, a larger proportion of cases will be children over age 5 who are apt to have one or more younger siblings. During an outbreak in a primary school in Burundi, 25 of the 28 cases were primary cases in their household. These led to 31 secondary cases, 90 percent of which were younger siblings (Cutts et al., 1991).
When vaccination coverage increases enough to delay measles epidemics for several years, small epidemics can arise from cases that originate at a health facility (e.g., Expanded Programme on Immunization, 1986; Chahnazarian et al., 1993). Such outbreaks occur because the health facilities bring together a number of children at risk of measles. A case-control study in a child health clinic on the outskirts of Abidjan, Côte d'Ivoire, during a measles epidemic showed that attending the clinic was associated with a 30 percent additional risk (95 percent C.I. 9-102 percent) of contracting measles (Expanded Programme on Immunization, 1986). In this population, where coverage of measles vaccination was 64 percent, about 67 percent of cases were attributable to attendance at the clinic during the epidemic.
A study of measles cases in Mbeya, Tanzania (Burgess et al., 1986), suggested that these ''nosocomial" cases may have a higher case-fatality rate. These data provide a strong argument for vaccinating all unvaccinated children who attend any child health clinic, including those with fever and
rashes that are often incorrectly assumed to be contraindications for vaccination.
Other Factors
Other factors can influence the effect of programs. First, there is a report that cases of measles among vaccinated children (e.g., vaccine failures) have a lower case-fatality rate than those among unvaccinated children (Aaby et al., 1986). However, another study failed to demonstrate this difference (Lamb, 1988). Second, Aaby and his colleagues have demonstrated that in Guinea-Bissau, children exposed to measles before 6 months of age have higher mortality than other children (Aaby et al., 1990a, 1993), even though about 75 percent of both the exposed and the unexposed were later vaccinated against measles. This difference does not appear to be due to selectivity factors determining who gets vaccinated or to socioeconomic differentials. The effect of exposure to measles appears to last for 2 to 3 years following exposure. Therefore, it is possible that vaccination programs might reduce mortality by reducing exposure to measles before age 6 months in addition to the direct effect of vaccination at a later age.
PROGRAM HISTORY, COVERAGE, AND QUALITY
In 1966, mass vaccination campaigns were begun in West and Central Africa through a 20-country program for smallpox eradication and measles control (Ofosu-Amaah, 1983). Consequently, vaccine coverage increased significantly in the late 1960s and early 1970s. Although these programs were successful in vaccinating large numbers of children, there were also many technical and managerial problems. Coverage rates dropped as these problems became apparent and program efforts slackened. After the World Health Assembly in 1974, the World Health Organization launched the Expanded Programme on Immunization. In 1978, the World Conference on Primary Health Care held in Alma-Ata identified immunization as an essential element of primary care. These renewed efforts were based on the newer, more heat-stable measles vaccines and a major programmatic emphasis on technical training of local personnel.
The most current estimates (early 1990s) for sub-Saharan African countries suggest a measles vaccination coverage rate of about 52 percent. These figures compare favorably with 1981 estimates of about 30 to 33 percent (International Science and Technology Institute, 1990; United Nations Children's Fund, 1991; Expanded Programme on Immunization, 1992; Nigerian Federal Office of Statistics and Institute for Resource Development, 1992). Figure 3-3 illustrates the changes in coverage rates at the national level between the early 1980s and early 1990s. These estimates are very rough;
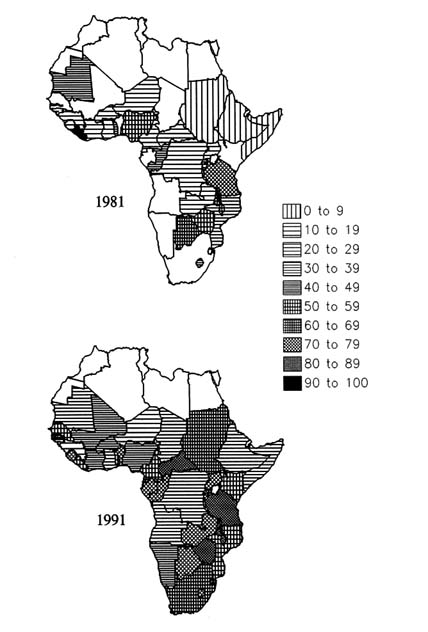
FIGURE 3-3 Proportions of children aged 12-23 months who have received measles vaccination, countries of sub-Saharan Africa, 1981 and 1991. SOURCES: 1981 data from United Nations Children's Fund (1991); 1991 data from International Science and Technology Institute (1990) and Expanded Programme on Immunization (1992).
many are based on administrative records rather than population surveys. Even the data based on surveys generally have a 95 percent confidence interval of at least ±10 percent. Surveys generally accept only vaccination cards, which provide information on when specific vaccinations were given—rather than relying on mothers' recall—as proof of vaccination. Estimated coverage may be biased downward if women lose or do not have vaccination cards to show to the interviewer or if programs run short of cards. On the other hand, accepting a mother's recall of past vaccinations might bias the estimate upward.
Gareaballah and Loevinsohn (1989) tested the accuracy of mother's recall of measles vaccinations in the Sudan. They interviewed illiterate mothers who had vaccination cards. They found that 87 percent of mothers whose child had been vaccinated reported correctly (the sensitivity) as did 79 percent of mothers whose child had not been vaccinated (the specificity). Therefore, they conclude that in the Sudan, limiting estimates of vaccination coverage to card-verified cases would lead to an underestimation of coverage. The coverage rate based on cards was only 43 percent compared to 66 percent based on cards and mothers' reports.
Moreover, coverage can vary substantially from year to year, especially in countries that rely on periodic national campaign days and those plagued by political problems. If coverage surveys are often carried out to demonstrate program success, these surveys may give more emphasis to high-coverage years. Because the estimates for 1981 are more likely to be based on administrative records, and coverage rates were changing rapidly at that time, estimates for 1981 are probably less reliable than those for 1991.
Despite the data problems, we can safely conclude that many more African children are currently protected by measles vaccination than were 10 years ago. The countries that have the lowest coverage rates are often those that have been affected by other economic and political problems (e.g., Ethiopia, Somalia, and Angola). Other countries may have experienced declines in coverage because of political problems since these estimates were made (e.g., Liberia and Zaire).
In places with relatively high coverage, it is possible that a small additional percentage in vaccination coverage can have an important effect on mortality. First, vaccination coverage is generally higher among children living in urban areas (where health facilities are often concentrated) and among children whose mothers are educated (Boerma et al., 1990). Mothers' education is not just a reflection of urban status. For example, a study in two periurban towns in The Gambia demonstrated significant differences between the educational status of both the mothers and the fathers of vaccinated and unvaccinated children within a single urban area (Hanlon et al., 1988). Expanding vaccination coverage in rural areas and among children with uneducated parents might have a greater effect than providing vaccinations
to the more advantaged parts of the population. Second, at higher levels of coverage, changes in the frequency of epidemics might provide the best protection for children under the recommended age for vaccination.
TREATMENT OF MEASLES (INCLUDING VITAMIN A)
The thrust of current programs is to reduce measles through vaccination, but there are still a large number of measles cases each year. The case-fatality rate among hospitalized cases of measles is often 10 to 15 percent (Kimati and Lyaruu, 1976; Dabis et al., 1988; Fischer, 1988). One strategy for combating measles cases is through improved treatment of complications, such as diarrhea and acute respiratory infections. Reduction in these illnesses can reduce measles-related mortality. (See Chapter 4 for discussions of case management of diarrheal diseases and ARI.) Moreover, recent research has suggested that treatment with vitamin A may reduce case fatality in hospitalized patients, as discussed in more detail in Chapter 5. Because in much of Africa, many children with severe cases of measles receive treatment in a hospital or health center, vitamin A treatment has the potential to have a substantial effect on case fatality.
A study of children hospitalized with measles in Kinshasa showed that among children less than 2 years of age, low serum vitamin A levels are associated with increased risk of dying (Markowitz et al., 1989). After controlling for muscle wasting, low white blood cell levels, and pneumonia at admission, those with vitamin A stores of less than 5 micrograms per deciliter had a case-fatality rate 2.9 times (95 percent C.I. 1.3-6.8) greater than those with higher serum levels. Among children 24-60 months of age, serum vitamin A was not significantly associated with increased risk of death (relative risk 1.2; 95 percent C.I. 0.2-7.8). This study demonstrated a relationship between measles and serum vitamin A levels, but it did not prove that depletion of vitamin A levels is part of the causal chain leading to death. However, reduced vitamin A levels probably increase the risk of pneumonia and diarrhea.
The first trial of the efficacy of vitamin A in the treatment of measles was carried out by Barclay et al. (1987) in Tanzania. This study showed lower mortality among measles cases under age 2 who received vitamin A (probability less than .05), but no difference among cases over age 2. For all ages, the difference between the treatment and comparison groups was not significant (probability of .13). A trial in Cape Town, South Africa (Hussey and Klein, 1990) also showed significantly lower mortality among measles cases treated with vitamin A (relative risk 0.21 times; 95 percent C.I. 0.05-0.94).
Coutsoudis et al. (1991) ran a randomized trial in Durban, South Africa, limited to cases of measles in African children under 2 years of age who
presented with both pneumonia and diarrhea complications. Only one death occurred—to a child receiving the placebo. However, there was a significant difference over a seven-day follow-up in the duration of pneumonia, with the vitamin A group having a mean duration of 3.8 days compared to 5.7 for the controls (probability less than .05). There were similar differences between the durations of diarrhea and fever, although these were not statistically significant. Of the vitamin A-treated children, 96 percent recovered fully within seven days, compared to only 65 percent among controls (probability less than .0002). Although the supplemented children showed better recovery in the seven-day follow-up, measles mortality can continue for many months after the infection because of its debilitating consequences.
SUMMARY
Several studies demonstrate that measles vaccination programs can greatly increase child survival in Africa. This conclusion is strengthened by the wide variety of research designs employed in these studies. These range from case control (Velema et al., 1991), to comparisons of vaccine failures with other children (Aaby et al., 1989), to comparison of program and nonprogram areas (Kasongo Project Team, 1981). The variety of research designs makes it difficult to compare the exact magnitude of the effect of programs in different settings. However, this variety increases our confidence in the overall conclusion.
Although measles vaccination is estimated to have a large effect on child mortality, we must note that these studies cover only a small part of the continent. The studies in Senegal, The Gambia, and guinea-Bissau were all carried out in coastal zones in areas very close to each other. The study in Benin was also carried out in a coastal area of West Africa. Only the Kasongo project in Zaire was in a noncoastal area outside West Africa. Therefore, it is risky to extrapolate from these studies to estimate the number of deaths prevented by measles vaccination in other parts of the region.
In addition, in some of the areas where the effectiveness of measles vaccination has been demonstrated, there is evidence that the efficacy may have been quite low at other times. For example, the studies by Aaby and his colleagues demonstrated that the measles vaccination program in Bandim, Guinea-Bissau, reduced child mortality during 1979-1981 (Aaby et al., 1984b). However, a later study showed that vaccine efficacy was no more than 68 percent in Bandim among children born in 1984-1985 (Aaby et al., 1990b).
Similarly, Garenne et al. (1985) showed that in Senegal the number of reported measles cases and the proportion of mortality attributed to measles dropped in several areas after the national vaccination campaign in 1966-1968. However, both reported cases and measles mortality returned to high
levels during 1972-1978. Garenne et al. (1992) also examined vaccine efficacy during the national vaccination campaign in one rural area in 1986-1987. Vaccine efficacy was reasonable (86 percent), but below the levels achieved in clinical trials in the same area.
These studies suggest that even in areas where measles vaccination has been demonstrated to be very effective in reducing mortality, the health programs did not always maintain high levels of effectiveness. This lack of effectiveness is supported by occasional reports of high failure rates in other programs (e.g., Cutts et al., 1990a; Adu et al., 1992). The evidence from some areas suggests that large-scale programs can succeed in reducing the incidence of measles (e.g., Foege, 1971; Dabis et al., 1988; Expanded Programme on Immunization, 1989; Cutts et al., 1991; Kambarami et al., 1991). However, program vigilance in necessary to ensure a reasonable level of vaccine efficacy in routine programs.
Measles vaccination programs are not likely to eliminate measles from Africa in the near future. Therefore, there will continue to be cases of measles that require treatment, especially among children who are too young to be vaccinated according to the standard vaccination schedule. These younger children have higher risks of measles mortality in addition to elevated risks from the diarrhea, pneumonia, and malnutrition that frequently accompany measles.
Studies suggest that vitamin A supplementation may reduce measles mortality. However, evaluation of treatment strategies for measles cases continues to be a pressing need. Studies need to be conducted that include longer follow-up of cases and controls to ensure that increases in survival to hospital discharge represent long-term gains and not just short-term abatement of the underlying risks.
PERTUSSIS (WHOOPING COUGH)
Although a commonly occurring and often debilitating disease, whooping cough has been a neglected subject of research throughout the world and in developing countries in particular. Mortimer (1988) notes that in preindustrial Britain, the lack of earlier recorded history of pertussis may have been due to the preoccupation of physicians with other severe infections, such as plague, typhus, and smallpox, leaving the care of pertussis to mothers and other caregivers. The case would appear to be the same in contemporary Africa. A recent editorial in the South African Medical Journal (1989) noted a visible lack of interest in this important disease by researchers and physicians alike.
One possible explanation for this persistent lack of attention is that pertussis is a less visible infectious disease than others. It is characterized
primarily by a cough, a symptom that can be caused by many other organisms. Although a frequent cause of death, whooping cough rarely kills in a quick dramatic way, as measles, smallpox, and cholera do. Pertussis is also more difficult to document both bacteriologically and serologically than many other diseases.
PERTUSSIS IN DEVELOPED COUNTRIES
Epidemiology
Whooping cough is a bacterial respiratory infection caused by Bordetella pertussis. Bordetella parapertussis, a closely related organism, can produce a similar disease, although its incidence seems to be 20 times lower than B. pertussis (Muller and Leeuwenburg, 1985). Cases of pertussis-like diseases have also been attributed to B. bronchiseptica and to different viruses. The incubation period is generally considered to be 9 or 10 days. During the first week, the symptoms are mild (cough, fever). The cough later becomes spasmodic and is often followed by a characteristic whoop, bluish coloring of the skin, and vomiting. This phase can last several weeks. Recovery is slow and gradual, and the cough may persist for many weeks (Mortimer, 1988).
The classical clinical picture of severe cases among older children is usually easily recognized by medical personnel and even by parents themselves. However, infants often have atypical symptoms, and mild forms of the disease are seen at all ages, especially in isolated cases outside major epidemics, and among vaccinated children. Culture of B. pertussis in the laboratory is also difficult. Even with laboratory confirmation, the algorithms for diagnosis have relatively low sensitivities and specificities (Mortimer, 1988; Patriarca et al., 1988). For example, Patriarca et al. (1988) studied four different serologic tests for diagnosing cases of pertussis. By combining the presence of cough for at least two weeks with each of these tests individually, they achieved specificities ranging from 75 to 90 percent with sensitivities ranging from 82 to 91 percent. Without the serology, they could only achieve a specificity of 80 percent with a sensitivity of 50 percent or less.
Whopping cough is a relatively frequent cause of death in developing countries. Sudden death from asphyxia due to obstruction of the airway may occur in the most severe cases. Furthermore, B. pertussis infection may induce pulmonary, encephalitic, and nutritional complications. Pulmonary changes may be caused by B. pertussis itself or, more frequently, by secondary invasion of other microorganisms such as streptococci or pneumococci. These changes may be sufficiently severe to compromise respiratory function and cause death. Acute encephalopathy may cause convulsions,
altered consciousness, permanent brain damage, or death. The persistent vomiting after the cough can also induce severe malnutrition, dehydration, and later death (Morley, 1966; Mata, 1978). In addition, pertussis may aggravate other infectious diseases such as measles and tuberculosis.
Whooping cough is transmitted from person to person by droplet spread (e.g., during coughing or sneezing) and usually occurs in epidemics. Virtually all children are susceptible to whooping cough from birth. Most children are infected before age 15 years, and in unvaccinated populations, the incidence, periodicity, and dynamics of whooping cough epidemics are similar to measles epidemics. A case generally confers lifetime immunity.
Pertussis is highly contagious after infection and the onset of cold-like symptoms, which occur one to two weeks before the typical whooping cough begins. Mortality from pertussis can be controlled by proper case management based on antibiotic therapy. The cough may last for one to two months in cases not treated with antibiotics (typically erythromycin, which is an expensive drug in Africa). In the untreated case, the person may remain communicable for 4-5 weeks. Among those receiving treatment, the period of infectiousness usually lasts only 5-7 days after beginning therapy (Benenson, 1985).
Vaccine Efficacy
The main strategy for reducing pertussis mortality is immunization programs. A first generation of killed whole-cell vaccines was developed before World War II, but gave poor results. A second generation of whole-cell vaccines combined with other antigens was marketed around 1950. The diphtheria-pertussis-tetanus vaccine is a major component of national immunization programs. However, the pertussis vaccine has not only a relatively low efficacy but also infrequent side effects, such as convulsions, high fevers, and brain dysfunction, and has been the object of major controversies (Miller et al., 1982; Ferry, 1984; Hinman, 1984; Hinman and Koplan, 1984). It is still not recommended in some European countries. A third generation of vaccines, the so-called a cellular vaccines, has been developed and used in Japan for many years. Several other formulas are under study.
The protective efficacy of the vaccine depends very much on the definition of a case. The vaccine seems to have virtually no capacity to protect against the infection, defined as the presence of the pathogen and at least one day of cough. However, it seems to protect against the severe forms of disease, and probably against death. Studies in the United States and in the United Kingdom have shown that vaccination reduces the severity of the disease, measured by duration of symptoms, mean number of coughing spasms, number of complications, and admission to hospital (Cherry, 1984; Pollock et al., 1984).
One dose of the vaccine provides little protection, and three to four injections are needed to provide maximum protection. In an outbreak investigation in Atlanta (Broome et al., 1981), the efficacy of three injections of whole-cell pertussis vaccine was estimated at 94 percent (95 percent C.I. 75-99 percent). Another smaller study in Maryland reported by Cherry (1984) found an efficacy of 89 percent among children aged 0-9 years. In England and Wales, protective efficacy was estimated in 10 different studies; results varied from 31 to 87 percent, with a mean of 57 percent (Cherry, 1984). The largest and most comprehensive study conducted in England and Wales (Fine and Clarkson, 1984) estimated the efficacy at 56 percent (95 percent C.I. 50-61 percent).
The World Health Organization currently recommends that children in developing countries receive three injections of DPT at intervals of at least four weeks. The first injection should be given as soon as possible after 6 weeks of age. In many countries, children are rarely fully vaccinated before age 6 months, creating a high-risk period for pertussis during the first six months of life.
PERTUSSIS IN AFRICA
Epidemiology
Prior to large-scale vaccination in the 1970s, whopping cough may have been among the top 10 causes of death among infants and children in sub-Saharan Africa. However, because of the difficulty in diagnosing pertussis by using verbal autopsies, we cannot be sure of its true importance. Even in the United States, pertussis cases are widely unrecognized (Hinman et al., 1986). In Africa, as in other developing countries, pertussis mortality rates are highest in the first six months of life and decline rapidly with age. The age pattern of deaths differs from that of measles, from which death rarely occurs before 4 months of age.
Much of what is known about pertussis in Africa is based on two longitudinal studies conducted in rural areas—Machakos, Kenya, and Niakhar, Senegal. In Machakos, two epidemics of pertussis occurred between 1974 and 1981. The average annual incidence for the period 1974-1981 was estimated at 1.6 percent among children under age 15 and 2.7 percent among children under age 5. Vaccination coverage was relatively low during this period. The case-fatality rate was 10 per 1,000 for all ages combined and 26 per 1,000 under age 1 (Muller et al., 1984b). These case-fatality rates (like the rates for measles in Machakos) are much lower than those recorded elsewhere (World Health Organization, 1975).
The pertussis incidence rate in Niakhar between 1983 and 1986 was 107 per 1,000 among children under age 5. The median age of cases was
4.5 years, and vaccination coverage was very low during this period (4 percent). However, as vaccination coverage increased between 1987 and 1989, the incidence rate was reduced by 79 percent (M. Garenne, personal communication, 1992). The case-fatality rates between 1983 and 1986 were 23 per 1,000 for all ages combined and 59 per 1,000 for infants. During 1987-1989, when vaccination coverage was higher and children were treated whenever possible, the case-fatality rate among children under 5 dropped to 13 per 1,000, a reduction of 43 percent. There were no pertussis deaths in the study area between 1988 and 1990 (Garenne et al., 1991). Cases of malnutrition were observed twice as often among children under age 5 after pertussis as after measles (Garenne and Cantrelle, 1986).
Vaccine Efficacy
In Machakos, the incidence of pertussis among vaccinated children was 54 percent lower than among nonrandomized controls of the same birth cohorts (Muller et al., 1984a,b). This finding suggests a vaccine efficacy similar to that observed in developed countries. Similar values were also found in South Africa. Investigation of an epidemic in Cape Town, South Africa, in 1988-1989 (Strebel et al., 1991) estimated an incidence rate of 66.7 percent among pre-primary school children with less than two doses of the DPT vaccine and 32.1 percent among those with three or four doses of the vaccine. This incidence suggests an efficacy of the pertussis vaccine of 52 percent (95 percent C.I. 12-74 percent). Preliminary results of a study conducted in Senegal showed a similar efficacy of 65 percent (M. Garenne, personal communication, 1992). Much of the variation in the vaccine efficacy arises from a range of case definitions. If a case definition of three weeks of cough is used, then the vaccine will have a high efficacy; but if a case definition of the presence of bacteria and one day of cough is used, the vaccine efficacy will be lower.
PROGRAM EFFORT
Figure 3-4 shows the proportion of children aged 12-23 months who had received three DPT injections as recorded in surveys taken around 1981 and 1991. In 1981, about 21-24 percent of African children had received three DPT injections (United Nations Children's Fund, 1991). By 1991 the proportion had increased to about 50 percent (International Science and Technology Institute, 1990; Expanded Programme on Immunization, 1992; Nigerian Federal Office of Statistics and Institute for Resource Development, 1992). This increase shows substantial progress, but leaves many children unprotected. The average for the continent is heavily influenced by low coverage rates in the three largest countries in the region. For 1991,
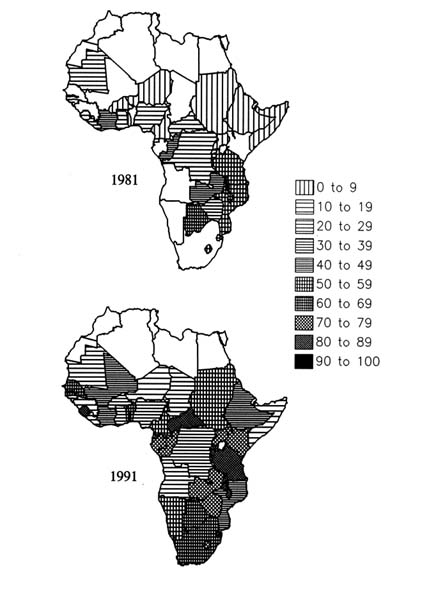
FIGURE 3-4 Proportions of children aged 12-23 months who have received three injections of DPT vaccine, countries of sub-Saharan Africa, 1981 and 1991. SOURCES: 1981 data from United Nations Children's Fund (1991); 1991 data from International Science and Technology Institute (1990) and Expanded Programme on Immunization (1992).
Nigeria had a rate of 33 percent, Ethiopia 44 percent, and Zaire 32 percent. In the rest of the region, coverage averaged 60 percent. However, the coverage rates in any one country can change drastically from year to year in response to major vaccination campaigns and political disturbances.
Unlike measles, there are very few studies of trends in the incidence of reported cases of pertussis. Data on outpatient cases of pertussis and coverage with three injections of DPT are available for Malawi between 1976 and 1987, as shown in Figure 3-5 (Expanded Programme on Immunization, 1989). During most of the period, vaccination coverage was increasing and the number of cases tended to decline. However, there were relatively large numbers of cases reported in the last three years of the series, which may have been due to the number of unvaccinated older children. The correlation between coverage and incidence is only .28, not statistically significant. However, in Cape Town, South Africa, pertussis death rates among nonwhites declined dramatically after introduction of the DPT vaccine in January 1950 (Strebel et al., 1991).
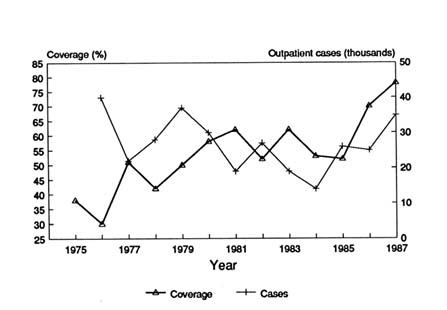
FIGURE 3-5 Trends in pertussis vaccination coverage and reported cases of pertussis in Malawi, 1976-1987. NOTE: Pertussis vaccination coverage is defined as children having three doses of vaccination against diphtheria, pertussis, and tetanus. SOURCE: Expanded Programme on Immunization (1989).
SUMMARY
Pertussis receives relatively little attention because it is less visible than other diseases and its symptoms are less distinguishable from those of other diseases. The pertussis vaccine, requiring at least three doses to be effective, is an essential component of child survival programs. The exact effect of the pertussis component of EPI vaccination on child mortality has not yet been determined, although studies suggest a wide range of efficacy. As with measles, a major benefit of the pertussis vaccine is that it lowers the severity of infection. As a consequence, it is also likely to lower the incidence of malnutrition, which is often caused by severe whooping cough. Immunization coverage has improved in recent years and is currently estimated at approximately 50 percent.
Case management currently includes treatment with antibiotics, although the disease is seldom detected when therapy can be most effective. Strategies for the most appropriate case management of whooping cough in the population require further research.
TUBERCULOSIS AND LEPROSY
Tuberculosis may be responsible for more deaths worldwide than any other disease caused by a single pathogen (Sudre et al., 1992). Approximately 171 million Africans are infected with tuberculosis; the prevalence rate is about 34 percent (Sudre et al., 1992). The annual incidence rate of 2.65 per 1,000 population is the highest of all regions. About one-sixth of these new cases are in individuals who are infected with the human immunodeficiency virus, which causes AIDS. The annual mortality rate due to tuberculosis is about 0.9 to 1.0 per 1,000 population—also higher than in any other region of the world. Only about 15 percent of tuberculosis cases occur in the population under age 15. The largest proportion of cases is found among adults aged 25 to 44 years (Murray, 1991).
Because the vaccination for tuberculosis also prevents leprosy, we consider that disease here as well. Its incidence and epidemiology are discussed later.
EPIDEMIOLOGY OF TUBERCULOSIS
In children, infection with the Mycobacterium tuberculosis is usually relatively benign and self-limiting. However, serious complications (particularly miliary disease—the presence of small nodules in the affected organ or body part—and tuberculous meningitis) are often fatal if left undiagnosed and untreated. Most diagnosed cases are in adults (Rodrigues,
1991), although many of these are the result of resurgence of infections acquired at earlier ages.
Data on causes of death among children rarely include tuberculosis, probably because of the difficulty of diagnosis. Verbal autopsies rarely provide a definitive diagnosis of tuberculosis, although cough lasting more than three months and weight loss are usually good indicators of respiratory tuberculosis. It is difficult to diagnosis pediatric tuberculosis even in clinics because of the difficulty in obtaining sputum samples from children and the unavailability of x-ray facilities. Moreover, the clinical symptoms of pediatric tuberculosis are often atypical, and tuberculin tests are difficult to interpret (Migliori et al., 1992). In addition, the mortality rate due to tuberculosis probably understates the likely effect of tuberculosis on child mortality because cases of tuberculosis may lead to severe weight loss and indirectly increase child mortality in other ways.
The tuberculosis situation in Africa is likely to worsen significantly during the next decade because of the link between AIDS and tuberculosis. The decline of an HIV patient's immunity often leads to the development of an overt infectious case of tuberculosis. Thus, the number of tuberculosis cases is increased through resurgence of old cases among HIV-positive individuals and through their spread of the disease to HIV-negative individuals. The incidence of tuberculosis among children will therefore increase in areas where HIV prevalence is high because even HIV-negative children will be subjected to an additional risk of infection. Schulzer et al. (1992) have projected that the annual risk of tuberculosis infection in HIV-negative individuals could increase by 13 to 141 percent in African countries, depending on the prevalence of tuberculosis and AIDS. In southern Uganda, the annual risk of smear-positive tuberculosis (i.e., infective cases capable of being transmitted) among HIV-negative adults could reach 0.4 percent by the year 2000. For the total population, Schulzer et al. estimate that the annual risk of infection could approach 2 percent per year. An increase in tuberculosis is already apparent in Tanzania, where the reported number of smear-positive cases increased from 8,000 in 1984 to 10,000 in 1989. In Uganda the annual number of confirmed cases doubled between 1984 and 1987 (Schulzer et al., 1992).
PREVENTION AND TREATMENT OF TUBERCULOSIS
There are two basic public health approaches to tuberculosis. The first is vaccination with bacille Calmette-Guérin. BCG was derived from a strain of Mycobacterium bovis and has been used as a vaccine against M. tuberculosis since the 1920s. In Africa, tuberculosis is also caused by M. africanum. BCG also provides some protection against M. Leprae, which causes leprosy. It is now a central part of the Expanded Programme on Immunization.
In Africa, most pediatric tuberculosis cases result from transmission from an infectious case in an adult. Most active cases among adults result from reactivation of infections that may have been dormant for many years. Thus, the BCG immunization is not an effective means of reducing the incidence of tuberculosis because it does not protect against primary infection. The immunization merely reduces the risk of progression from latent infection to clinically active disease (Rieder, 1992). Therefore, the best approach to reducing incidence is treatment of cases to reduce the period of transmission. Drug therapy can cure tuberculosis and thereby prevent death from tuberculosis as well as reduce the spread of the disease. About 75 percent of cases requiring treatment are among those aged 15-59 (Murray et al., 1991), and these are the source of infection for most new cases.
The main problem in treatment programs is compliance because treatment lasts between 6 and 18 months. Patients often feel well long before they are cured, which leads to a high default rate. For example, in a program in northern Ghana, 52 percent of male and 40 percent of female patients did not complete their treatment (van der Werf et al., 1990). The default rates for the standard therapy were 24 percent and 16 percent, respectively, for programs in Mozambique and Tanzania (Murray et al., 1991). Default rates are lower in programs that utilize the more expensive ''short-course" treatments. In Mozambique, Tanzania, and Malawi, default rates for short-course regimens were 11, 10, and 2 percent, respectively (Murray et al., 1991). When patients discontinue treatment before they are cured, they are at risk of a resurgence of the infection and are infectious for a longer period.
Murray et al. (1991) estimate the effective cure rates5 of standard therapy in the national programs of Mozambique and Tanzania to be 66 and 60 percent, respectively. They estimate that the effectiveness of short-course therapy is about 90 percent in Malawi and Mozambique, and 86 percent in Tanzania.
High default rates encourage the development of drug-resistant strains. A study in northern Ghana (van der Werf et al., 1989) found that initial resistance (i.e., resistance among patients who reported that they had not received previous treatment) was 27 percent to the drug isoniazid, 23 percent to streptomycin, and 29 percent to thiacetazone. Only 45 percent of samples were sensitive to all three drugs. A study of trends in initial drug resistance in black adult patients in South Africa (Weyer and Kleeberg, 1992) showed that resistance to isoniazid declined from 29 percent in 1965-1970 to 14 percent in 1980-1988. Similarly, resistance to streptomycin dropped from 34 to 12 percent. These declines are probably a result of
improved treatment practices. However, drug resistance is still a problem in South Africa among some ethnic groups. For example, among the Xhosa, 23 percent of infections were resistant to isoniazid.
The studies of tuberculosis treatment programs have focused on the effectiveness of treatment among identified cases. Because there are probably large differences in the success of programs in identifying cases, it is difficult to estimate the effect of treatment programs on populations. In addition, most of the patients in treatment programs are adults. For these reasons, we limit our review to studies of the effectiveness of vaccination programs that provide BCG.
EFFICACY OF BACILLE CALMETTE-GUÉRIN (BCG) VACCINATION
Estimates of the efficacy of BCG in preventing tuberculosis vary from zero to 80 percent in numerous studies (Fine, 1988). During the past 30 years there has been extensive debate over the reasons for this variation. However, there is still no consensus on what factors lead to high efficacy. As a result, there is a need for studies to determine whether BCG is effective in numerous different populations. Although the efficacy of BCG in preventing tuberculosis is variable, the consensus is that it is efficacious—as high as 95 percent—in reducing the incidence of serious forms of tuberculosis, including miliary tuberculosis and tuberculous meningitis (Tuberculosis Control Programme and Expanded Programme on Immunization, 1986; Schwoebel et al., 1993). These complications, which are frequent in children, are usually fatal if left untreated. Uncomplicated cases among children are relatively benign but may be important underlying causes of mortality, working particularly through malnutrition.
BCG Efficacy Against Tuberculosis in Africa
There are three studies of the efficacy of BCG in preventing tuberculosis in Africa. All three are case-control studies that compare the vaccination history of tuberculosis cases with the history of nontubercular controls. There are numerous problems that can bias case-control studies (e.g., ascertainment of vaccination status and diagnosis of tuberculosis in children). However, the costs of randomized control trials are so high that it is not possible to carry out such studies in all regions (Smith, 1988).
Blin et al. (1986) carried out a case-control study of the efficacy of BCG in preventing tuberculosis. The cases were adults aged 17-26 who were newly diagnosed with sputum-positive pulmonary tuberculosis in 1983-1984 in the only tuberculosis dispensary in Yaoundé, Cameroon. Many of these cases were probably infected as children. The controls were from an
antivenereal dispensary in Yaoundé and general dispensaries in two towns in the region. Vaccination status was determined by the presence or absence of a BCG residual scar. The subjects were between 0 and 18 years of age during the BCG mass vaccination campaign.6 The estimated protective effect of BCG against pulmonary tuberculosis in young adults was 66 percent (95 percent C.I. 53-75 percent). This estimate controls for potential confounding by sex, age, socioeconomic group, and geographic region of origin. However, none of these variables was significantly related to differences in efficacy.
Tidjani et al. (1986) reported on a trial conducted in Togo of BCG among children age 6 years or less who were in contact with newly diagnosed cases of tuberculosis. These children were at increased risk of infection and therefore provided an efficient sample for measuring vaccine efficacy. The estimate of efficacy of BCG from this study is 66 percent (95 percent C.I. 54-74 percent). The data suggest that the efficacy is higher for more severe forms of the disease. Statistical controls for the closeness of contact with a case of tuberculosis (parents or others) and for age and sex reduce the estimated efficacy to close to 60 percent. However, the efficacy of BCG might be lower in this sample than in the general population because the subjects were exposed to higher doses of the bacteria, which could overwhelm the resistance they acquired from BCG.
The population of a case-control study initially conducted in Malawi between 1980 and 1984 by Fine et al. (1986) remained under observation through 1989 (Pönnighaus et al., 1992). (The original study is discussed in the following section with other studies of the efficacy of BCG vaccine against leprosy.) By the end of the 1989 follow-up, 180 new incident cases of tuberculosis had been diagnosed in the population of 83,445. Confirmation of tuberculosis was based on sputum specimens of self-reported cases collected at health centers and the district hospital. The infection rates among BCG scar-positive and BCG scar-negative individuals were very similar. The differences between the age-corrected estimates, based on a number of age groups, case definitions, and estimation techniques, were not significant. This finding suggests that BCG vaccination is not protective against tuberculosis in the population.
EPIDEMIOLOGY OF LEPROSY
Leprosy is an infectious disease caused by Mycobacterium leprae; it is rarely fatal. The individual's response to the infection depends on the
cellular immune mechanism. A person with a good cellular immune response is more likely to have a milder tuberculoid type, and a person with weak or no cellular immunity is likely to develop the lepromatous type (Bloom and Godol, 1983). The clinical symptoms vary from a single hypopigmented skin patch that heals spontaneously to damage to the nervous system, bones, eyes, muscles, and extremities. The average incubation period is estimated to be 2 to 4 years, though it may vary from 9 months to 12 years (World Health Organization, 1985). The World Health Organization (1982) recommends that treatment last between six months and two years, depending on the type of case. It is estimated that approximately 11.5 million cases of leprosy exist worldwide—5.3 million of which are registered for treatment (Irgens and Skjaerven, 1985). In Africa, it is thought that 3.5 million cases of leprosy exist. Only about 1 percent of the cases are estimated to be among children under age 5 (World Health Organization, 1982).
BCG also provides protection against leprosy, and this protection is an important element in the evaluation of its effect in Africa (Rieder, 1992). BCG provides some protection against leprosy through cross protection between Mycobacterium bovis and M. leprae. Studies of the efficacy of BCG against leprosy in Asia show it to be 20 percent efficacious in Myanmar, 30 percent in South India, and 44 percent in New Guinea (Fine and Pönnighaus, 1988).
There have been two studies of the efficacy of BCG in preventing leprosy in Africa. The first, conducted by Stanley et al. (1981), was a cohort study of children who were contacts or relatives of known leprosy patients in Uganda. In the first stage of the study in 1960-1962, 16,150 tuberculin-negative or weakly tuberculin-positive children were allocated at random to BCG-vaccinated and unvaccinated groups. The researchers examined these children at intervals of approximately two years for the next eight years. Eighty percent of these children were under age 10 at the start of the study. At the first follow-up visit in 1963, 1,976 children born into the trial families were added to the cohort to increase the number of young children in the study. Between 1970 and 1975, new cases at leprosy clinics were checked to see if they were included in the cohort study.
Stanley et al. estimated that the efficacy of BCG against leprosy was 80 percent (95 percent C.I. 72-86 percent) based on the experience of the original cohort recruited in 1960-1962 through 1970. The data from 1970 to 1975 suggest that the vaccine continued to be effective 12 to 13 years after vaccination. Data on the children who had lesions of doubtful etiology at intake suggested that BCG may not have had a large effect on preexisting leprosy lesions. However, the numbers of such cases were too small to produce reliable estimates of efficacy in slowing progression of the disease. Similarly, there was no evidence that BCG slowed the progression or
severity of the disease in children who had no sign of lesions at intake (i.e., among apparent cases of vaccine failures).
Fine et al. (1986) ran a study of BCG efficacy against leprosy in northern Malawi. This study began with a survey of 112,000 households between 1980 and 1984. Each case of leprosy was matched with all individuals living in the same square kilometer who were of the same sex, five-year age group, and schooling status. The study was limited to those under age 35 because BCG coverage beyond that age was very low. Persons whose BCG scar status was doubtful or unknown (10.3 percent) were excluded from the analysis. Analysis of the matched case-control data led to an estimate of BCG efficacy against leprosy of 41 percent (95 percent C.I. 11-61 percent), showing very little difference across age groups. Data on cases of leprosy identified after the initial survey (i.e., through prospective data collection) led to an estimate of efficacy of 57 percent (95 percent C.I. 24-75 percent). The estimate of efficacy based on the case-control design (41 percent) was probably biased downward because it included some cases in which infection occurred before vaccination. Because of this bias and because errors in BCG scar ascertainment and in diagnosis of leprosy might reduce the efficacy estimate, the authors concluded that the efficacy was at least 50 percent. In a follow-up study between 1985 and 1989 among the same population, an efficacy of 50 percent or greater was observed (Pönnighaus et al., 1992).
These studies suggest that BCG is more effective against leprosy in Africa than in South India and Myanmar (Fine, 1988; Fine and Pönnighaus, 1988). There is no generally accepted explanation for this difference. However, it does appear that BCG is effective against leprosy in eastern and southern Africa. Because there are a large number of cases of leprosy in Nigeria, it would be useful to estimate the efficacy of the vaccine in that country.
PROGRAM COVERAGE
Figure 3-6 presents the estimates of coverage of BCG by country in 1981 and 1991 (Boerma et al., 1990; International Science and Technology Institute, 1990; United Nations Children's Fund, 1991; Expanded Programme on Immunization, 1992; Nigerian Federal Office of Statistics and Institute for Resource Development, 1992). For all of sub-Saharan Africa, BCG coverage increased from about 31-34 percent in 1981 to 72 percent in 1991. These estimates are very rough. Many of the estimates come from administrative records rather than population surveys. Even the data based on surveys usually have a 95 percent confidence interval of about ±10 percentage points. However, it is clear that BCG coverage has increased drastically during the past decade.
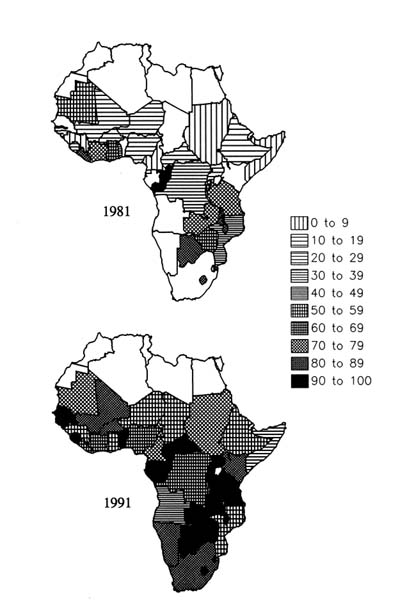
FIGURE 3-6 Proportions of children aged 12-23 months who have received BCG vaccination, countries of sub-Saharan Africa, 1981 and 1991. SOURCES: 1981 data from United Nations Children's Fund (1991); 1991 data from International Science and Technology Institute (1990) and Expanded Programme on Immunization (1992).
SUMMARY
The prevalence of tuberculosis in Africa is estimated to be 34 percent. Given the link between AIDS and tuberculosis, it is likely that the prevalence of tuberculosis will continue to increase. The BCG vaccination, although of varying and questionable efficacy, has been shown to be effective against both tuberculosis and leprosy in Africa. However, given the great variation in efficacy across continents, it would be useful to have more studies in different African settings.
Programs that provide BCG have probably saved many lives and reduced morbidity. However, no precise estimates of the effect of BCG on mortality exist. Childhood deaths that have tuberculosis as an underlying cause may actually outnumber the deaths directly attributed to the disease. Therefore, it is not possible to produce an accurate estimate of the likely effect of the increase in BCG coverage on child mortality in Africa.
TETANUS
Tetanus is a major cause of neonatal death in much of Africa, as well as among other age groups. Because of the small proportion of the population protected by immunization at all but childhood ages, and the large proportion of births that occur under poor hygienic conditions related especially to home deliveries, tetanus mortality rates in Africa are probably among the highest in the world. The tetanus mortality rate is best documented for neonates—the population in which the problem predominates. Tetanus of the umbilicus is responsible for a substantial proportion of neonatal and infant mortality in many regions where most deliveries are performed by untrained traditional birth attendants or relatives.
EPIDEMIOLOGY
The few available studies suggest that rates of 10 to 20 neonatal tetanus deaths per 1,000 live births are not unusual. Studies in rural parts of Sierra Leone have led to estimates as high as 70 per 1,000 (Kandeh, 1986). Tetanus may be less of a problem in southern and eastern Africa than in western Africa. The Machakos project in Kenya recorded a rate of only 1.2 per 1,000 (van Ginneken and Muller, 1984).
Some studies of tetanus are apparently biased by underreporting of neonatal deaths. This bias is particularly important for estimates based on retrospective reporting of deaths. In several studies, underreporting is apparent in the trends of tetanus mortality rates. In particular, several surveys show higher rates for the months closer to the survey date (e.g., Stanfield
and Galazka (1984) and Sokal et al. (1988) in Côte d'Ivoire; Expanded Programme on Immunization (1983) in Malawi; however, Melgaard et al. (1988) report no trend in Kenya). On the other hand, estimates of tetanus mortality may be biased upward by errors in diagnosis. For example, Snow et al. (1992) compared verbal autopsies with records of hospital deaths. They found that verbal autopsies performed rather well for neonatal tetanus deaths (sensitivity of 90 percent and specificity of 79 percent). These led to an exaggeration of the neonatal tetanus mortality rate of about 30 percent.
More sophisticated treatment of tetanus cases is not currently a viable policy option because such treatment is expensive and difficult. The case-fatality rate of hospitalized cases of neonatal tetanus is usually 60-80 percent (Bwibo, 1971; Kenya Ministry of Health, 1978; Merhai and Kumar, 1986; Maru et al., 1988; Babaniyi and Parakoyi, 1989; Einterz and Bates, 1991). There are fewer data on tetanus after the first month of life. In Kenya in 1978, the case-fatality rate among inpatient cases was 33 percent for children 1-14 and 47 percent for adults over age 15 (Kenya Ministry of Health, 1978).
A study in Tanzania reported a lower case-fatality rate among neonates treated with antitetanus equine serum (Mongi et al., 1987). However, a recent meta-analysis (which included the study by Mongi et al.) did not find convincing evidence that this approach improved survival among neonates with tetanus (Abrutyn and Berlin, 1991). Yet, the effect of serum depends on when it is given. During the first two days of life, it has a beneficial effect; thereafter, it does not (M. Garenne, personal communication, 1992).
Although improvements in case fatality are possible, only a small proportion of neonatal cases ever receive hospital treatment (Expanded Programme on Immunization, 1983; Babaniyi and Parakoyi, 1989). For example, in a rural area of Côte d'Ivoire, only 2 percent of neonatal tetanus cases came to the attention of medical authorities (Sokal et al., 1988). During 1979 in Kenya, there were 2,258 outpatient cases and 767 inpatient cases of tetanus at all ages in the 33 districts for which data were available (Kenya Ministry of Health, 1978). Extrapolating to the whole population, the Ministry of Health estimated that there were about 3,300 cases at all ages nationally. In comparison, Melgaard et al. (1988) used data on three districts to estimate that there were about 8,000 to 12,000 neonatal deaths due to tetanus annually in the mid-1980s. It is likely therefore that only a fraction of cases of tetanus ever receive even minimal care.
PROGRAMS TO REDUCE THE INCIDENCE OF NEONATAL TETANUS
In 1989 the World Health Assembly called for the worldwide elimination of neonatal tetanus by 1995 (World Health Organization, 1990). The
two policy options are improving delivery practices and providing immunizations. One way to improve deliveries is to increase the proportion of deliveries that occur in hospitals or dispensaries where it is easier to maintain appropriate antiseptic practices. In hospitals and dispensaries, it is also possible to administer tetanus antitoxin to newborns shortly after delivery—a practice common in francophone areas (Sokal et al., 1988). Alihonou (1970) attributes the rapid decline or reported deaths from neonatal tetanus in Dakar to this practice. An alternative approach is to train traditional birth attendants or midwives to improve home deliveries by using sterile instruments for cutting the umbilicus and to treat the stump appropriately.
The other option is immunization of pregnant women, which provides temporary immunity to the fetus and protects the newborn for several months. The World Health Organization recommendation is that women receive two injections of tetanus toxoid at least one month apart as early as possible during pregnancy. One study (Owa and Makinde, 1990) suggests that children who do contract neonatal tetanus have a greater chance of survival if their mother has had a single prenatal tetanus injection. A single booster injection is recommended for subsequent pregnancies. Four or five tetanus toxoid vaccinations are likely to provide lifetime protection for the mother and for each of her children during the neonatal period (Wassilak and Berlin, 1986). In areas where neonatal tetanus is a serious problem, vaccination programs should target all women of childbearing age.
In practice, most programs include efforts both to improve deliveries and to provide tetanus immunization to women. Although the combination is probably more efficacious than either approach alone, it is difficult to evaluate the independent efficacy of each approach. Only one study has attempted to compare these strategies. Orenstein et al. (1985, quoted in Babaniyi and Parakoyi, 1989), estimated that in Nigeria the efficacy of two doses of tetanus toxoid was higher than that of either hospital delivery or home delivery by a trained midwife.
Incidence of Neonatal Tetanus Among Hospital Deliveries
Several studies have shown that the incidence of neonatal tetanus is much lower among hospital deliveries than among other births (Dan et al., 1971; Stanfield and Galazka, 1984; Kofoed and Simonsen, 1988; Sokal et al., 1988). Melgaard et al. (1987) reported that in three districts of Kenya the neonatal tetanus mortality rates were 14.1 for home deliveries and 4.3 for deliveries in health institutions. These estimates yield a relative risk of 3.3 associated with home deliveries compared to hospital deliveries. Other studies have found that all recorded cases of neonatal tetanus were among children born at home (e.g., Sokal et al., 1988).
Women who deliver in hospitals may be different from other women in many ways (e.g., they are more likely to live in urban areas and may be
better educated). However, the lower incidence of neonatal tetanus among hospital births also probably reflects better care of the umbilical stump. Even so, hospital delivery is not a guarantee of protection. Even the most careful delivery will not protect the child against treatment of the stump or circumcision practices after the child leaves the hospital.
Evidence of the Effect of Training of Traditional Birth Attendants
Because of the high cost and unavailability of hospital deliveries for most African women in rural areas, many authorities have recommended training traditional birth attendants (TBAs) in aseptic procedures for cutting the umbilical cord and caring for the umbilical stump. A study by Leroy and Garenne (1991) in rural Senegal suggests that the most important risk factor for neonatal tetanus is whether or not the person who delivered the baby washed her hands with soap prior to cutting the cord. However, most training programs have concentrated on improving the instrument used for cutting the cord.
There are very few studies anywhere in the world that provide evidence of the effect of training TBAs on tetanus mortality in populations in which tetanus toxoid coverage did not also increase (Ross, 1986). Studies in the Philippines and Bangladesh have shown that midwife training reduces overall neonatal mortality more than maternal immunization, but maternal immunization alone causes a larger reduction in the incidence of neonatal tetanus than midwife training (Stanfield and Galazka, 1984).
There has been one such study in Africa in the Thies region of Senegal. In the first part of the study, birth attendants in six villages learned to care for the cord properly. After this training, the neonatal mortality rate in the program villages was 38 per 1,000 live births, compared to 101 in the control villages (Dan et al., 1971). The recorded postneonatal rates in the two areas were identical (147 and 146 per 1,000).
In the years following this study, the program reached an increasing number of villages. Sanokho and Senghor (1975, quoted by Ross, 1986) examined the place of residence of neonatal tetanus cases recorded at the Khombole hospital. The proportion of these cases that were from villages selected for the midwife training program dropped substantially after the start of the program. These studies suggest that the training of traditional birth attendants can reduce the incidence of neonatal tetanus, at least in populations with high rates.
Evidence of the Effect of Programs that Provide Tetanus Toxoid Immunization to Women
Studies of antenatal immunization against tetanus in other parts of the world have shown that two injections of tetanus toxoid early in pregnancy
are 95 percent effective in preventing neonatal tetanus in the child born of that pregnancy. The effect of two injections declines over time. Some studies show that the injections are still 40 percent effective in reducing neonatal tetanus four to five years later, and Koenig (1992) reports that two doses of tetanus toxoid may provide protection against neonatal tetanus for 15 years or more. A single booster shot restores the full effectiveness. A single injection during pregnancy provides partial protection for that pregnancy (see summary in Stanfield and Galazka, 1984).
Susceptibility to tetanus and case-fatality rates are not affected by the presence of other common diseases (e.g., malaria, malnutrition). Therefore, there is no reason to expect that at a given level of neonatal tetanus mortality and a given level of program coverage, the effect of an immunization program would differ across populations. What is uncertain is the success rate of various types of programs in achieving high levels of effective coverage. In particular, there is little information on the proportion of women who deliver at home after receiving at least two injections of tetanus toxoid. We also do not have studies that suggest what proportion of births are partially protected by tetanus toxoid injections during a previous pregnancy.
A few studies in Africa have demonstrated the efficacy of immunization with or without midwife training programs. Ross (1986) reported the results of a program that formed village health teams in 11 villages near Serabu Hospital, Sierra Leone. The program trained TBAs in improved perinatal care and encouraged them to refer pregnant women for antenatal care, which included tetanus toxoid injections. Within a year of the start of the program, the neonatal tetanus mortality rate declined from 72 to 11 per 1,000 live births (this difference is significant at the 0.001 level). In the next few years, the mortality from neonatal tetanus continued to decline to ''virtually zero" (Ross, 1986). The program near Serabu Hospital must be considered a field trial because it is not clear whether that program could be successfully replicated in larger populations.
Two studies of large-scale programs that participated in the Combattings Childhood Communicable Diseases (CCCD) project, funded by the U.S. Agency for International Development and carried out by the Centers for Disease Control of the U.S. Department of Health and Human Services, provide some evidence of the efficacy of tetanus immunization on neonatal mortality. In one area of Zaire and two counties in Liberia, the CCCD programs were evaluated by using retrospective maternity histories before and after the start of the program. In Liberia, data on cause of death based on verbal autopsies suggested that there was a reduction of approximately 50 percent in neonatal tetanus mortality (probability less than .05; Becker et al., 1993). This decrease was probably the result of an increase in the proportion of mothers who had received two tetanus toxoid injections from very low levels to more than 30 percent (Vernon et al., 1993). The CCCD
surveys in Zaire did not include verbal autopsies. However, there was no evidence of a decline in infant mortality. This apparent lack of effect is consistent with the absence of neonatal tetanus cases reported by the local hospital and health centers before the program (Vernon et al., 1993).
Because case-fatality rates are so high and few cases receive modern medical care, we can safely use data on disease incidence to monitor programs. A study of neonatal tetanus in Maputo, Mozambique, suggests that a vaccination program alone can have a significant effect in urban areas. Cutts et al. (1990b) reported that from 1976 to 1978, there were between 173 and 254 cases of neonatal tetanus reported annually in Maputo. After the start of the vaccination campaign, the proportion of mothers reporting at least two injections of tetanus toxoid increased to 42 percent in 1982, 91 percent in 1983, and 87 percent in 1986. This increase in vaccination coverage coincided with a rapid decline in the number of reported cases to a range of only 3 to 13 cases per year between 1982 and 1987. Although it is not possible to calculate the mortality effect of this program based on these surveillance data, the program must have been associated with a dramatic drop in neonatal tetanus mortality.
In Malawi, immunization of pregnant women with tetanus toxoid began in 1984. Coverage increased from about 27 percent in 1985 to more than 60 percent in 19887 (Expanded Programme on Immunization, 1989). Although the number of neonatal tetanus cases reported in hospitals dropped in 1986 and 1987, the change was not significant.
Finally, Sokal et al. (1988) quoted a study by Yada et al. (1981) from Burkina Faso. In one area of the country, coverage with two injections of tetanus toxoid reached 50 percent and hospital admissions for tetanus decreased by two-thirds.
PROGRAM COVERAGE
Figure 3-7 presents national estimates for 1981 and 1991 of the proportion of recent deliveries in which the woman had at least two injections of tetanus toxoid during pregnancy (International Science and Technology Institute, 1990; United Nations Children's Fund, 1991; Expanded Programme on Immunization, 1992; Nigerian Federal Office of Statistics and Institute for Resource Development, 1992). In 1991, about 41 percent of deliveries were protected by recent tetanus toxoid injections. This coverage is much larger than the value for 1981, which was less than 15 percent. Estimates for West Africa, where neonatal tetanus may be more common, indicate that
coverage increased from about 12 to 44 percent. These estimates are subject to numerous types of sampling and reporting error because they are often based on women's retrospective reporting and on sample surveys. In addition, children born to women who received several tetanus toxoid injections during previous pregnancies are partially protected against tetanus. Despite these weaknesses, the data suggest substantial improvements in coverage, although most pregnancies are still not protected.
PROGRAMS TO REDUCE NONNEONATAL TETANUS MORTALITY
The standard EPI program in most African countries includes tetanus immunization of young children as part of the DPT series. With the high coverage rates achieved in many areas, there have likely been reductions in nonneonatal and pediatric tetanus. However, to our knowledge there have not been any studies of the effect of this aspect of EPI programs. Similarly, antenatal immunization may have reduced tetanus mortality among adult women, but we are not aware of any studies of the effect of these programs on adult mortality.
SUMMARY
Tetanus is a leading cause of neonatal death in sub-Saharan Africa, with a range of 10 to 20 deaths per 1,000 live births in much of the region prior to control efforts. Lower rates in southern and eastern Africa suggest that regional differentials exist in neonatal mortality, but this result could be due to biases arising from underreporting of neonatal deaths. Programs designed to reduce mortality from neonatal tetanus generally focus on improving delivery conditions (such as training TBAs to incorporate sanitary practices) and immunizations of pregnant women or women of reproductive age.
A number of studies conducted in Liberia, Mozambique, and Burkina Faso indicate that as the proportion of pregnant women who are immunized increases, mortality from neonatal tetanus decreases. For a woman to be covered adequately against tetanus, she needs to have received at least two injections of tetanus toxoid at least one month apart as early as possible during the pregnancy (the first time she receives the immunization), with a single booster injection (up to three) given during subsequent pregnancies for the mother and for the child during the neonatal period. Results from the Demographic and Health Survey indicate that a relatively large proportion of mothers of children born during the five years prior to the survey in most countries were adequately immunized against tetanus. Similarly, an association is observed between women being immunized against tetanus
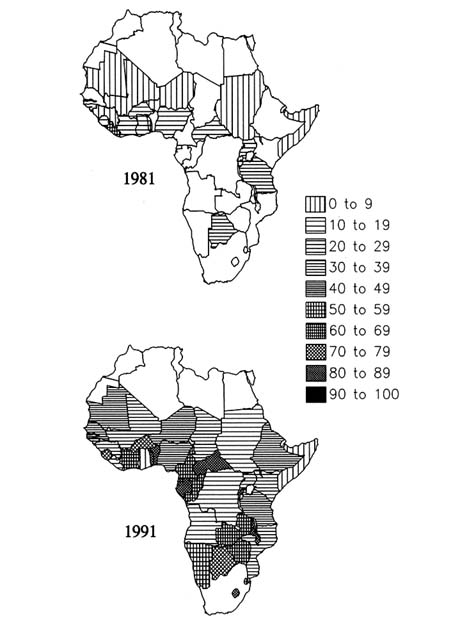
FIGURE 3-7 Proportions of births preceded by at least two prenatal injections of tetanus toxoid, countries of sub-Saharan Africa, 1981 and 1991. SOURCES: 1981 data from United Nations Children's Fund (1991); 1991 data from International Science and Technology Institute (1990) and Expanded Programme on Immunization (1992).
and those having hospital-based deliveries. Thus, the women with the greatest likelihood of having unsanitary conditions at delivery are also those who have not received adequate immunization against neonatal tetanus.
CONCLUSION
The Expanded Programme on Immunization has had a large impact on increasing vaccination coverage. As noted earlier, vaccination coverage for the preventable diseases included in the EPI increased substantially between the 1980s and 1990s, as illustrated by the increase in BCG coverage from 28 to 79 percent and measles vaccination coverage from 18 to 54 percent. Despite the increase in coverage, the quantity and quality of research on the effects of various components of standard EPI immunization programs on child mortality are uneven.
Measles has been studied widely in Africa from epidemiological and programmatic perspectives. Programs using the standard age schedule for vaccination with the standard vaccine can be effective in preventing measles and reducing child mortality in Africa by large proportions. Although the vaccine is highly efficacious, studies indicate that in some large-scale programs, cold chain failures have greatly reduced program effectiveness. In some study areas, program effectiveness has varied substantially over time. Although vaccination coverage is increasing, measles is not likely to be eliminated from Africa in the near future. Thus, in addition to the need for continued research on the disease's epidemiology, we need to know more about treatment strategies for children who contract the disease.
The vaccination coverage for pertussis has not achieved the EPI program goal of 75 percent; currently, it is estimated to be about 57 percent. Pertussis is difficult to diagnose because it has no uniquely distinguishing symptoms in its early stages. A wide range of estimates of the efficacy of the pertussis component of the DPT series has been reported. The vaccine, however, has reduced the incidence of the disease and may lower the severity of infection among those who are vaccinated and become ill. We do not have any estimates of the effect of DPT on mortality.
Tuberculosis is an important cause of mortality and morbidity among both children and adults in Africa, with an estimated prevalence of 34 percent. Its effect among children may be underestimated because it is often a contributing cause, rather than the primary cause of death. The BCG vaccination is of questionable efficacy in preventing cases of tuberculosis—estimates range from 0 to 80 percent—but may be more effective in preventing the more serious forms of the disease. It has also been shown to be effective in preventing leprosy.
Tetanus is a leading cause of neonatal mortality in some areas of sub-Saharan
Africa. It is preventable if the mother has been adequately vaccinated. Other options for reducing the disease are the training of traditional birth attendants in hygienic delivery practices and the administration of tetanus antitoxin to the child shortly after delivery.
Before the initiation of the Expanded Programme on Immunization, as recently as the early 1980s, vaccination coverage in Africa was the lowest in the world (Rodrigues, 1991). To augment national programs, acceleration strategies based on outreach components such as mobile units and improved cold chains were implemented in the mid-1980s. Greater attention to these preventable diseases through increased immunization has probably had a large effect on reducing mortality, but the full potential of these programs has not been achieved. Increased coverage with the standard EPI immunizations and maintenance of high coverage should continue to be top priorities for reducing child mortality.