Effects of Health Programs on Child Mortality in Sub-Saharan Africa (1993)
Chapter: 4 Other Interventions Targeted at Single Diseases
4
Other Interventions Targeted at Single Diseases
In addition to the diseases that can be prevented through immunization, there are other diseases that are responsible for large proportions of mortality in Africa. In this chapter, we examine diarrheal diseases, malaria, and acute respiratory infections.
Currently, programs aimed at controlling diarrheal diseases focus on a case-management strategy that promotes the use of oral rehydration therapy, which includes oral rehydration solutions, recommended home fluids such as rice water or gruels, and feeding with extra fluid. In addition, diarrheal disease control programs promote breastfeeding and safe weaning practices, use of potable water, and personal and domestic hygiene. Programs that combine these different strategies are in operation in almost all sub-Saharan African countries.
Malaria is a major cause of morbidity among children and adults, but is particularly serious among infants and children. Strategies for controlling malaria include eliminating breeding places for mosquitoes that transmit the disease, direct killing of mosquitoes with insecticide, preventing mosquito bites by means of barriers such as bed nets, drug prevention, and treating fevers that may be due to malaria.
Acute respiratory infections (ARIs) are also discussed in this chapter. Pneumonia is the principal cause of death among these diseases, although bronchitis, asthma, and influenza are also responsible for some infant and child deaths. The strategy promoted by the World Health Organization emphasizes early detection of these infections and appropriate antibiotic
treatment made available through primary health care programs. Although these diseases are a major cause of infant and child deaths in the region, relatively few sub-Saharan African countries yet have national ARI control programs.
DIARRHEAL DISEASE CONTROL PROGRAMS
The term diarrheal diseases refers to a heterogeneous group of illnesses characterized by frequent loose or liquid stools and caused by a wide variety of viral and bacterial pathogens, as well as a few parasites. These conditions can also be classified as acute watery, dysenteric, or persistent diarrhea, according to their clinical presentation. Acute watery diarrhea can be associated with substantial losses of water and electrolytes, resulting in life-threatening dehydration. Although not the most important cause of acute dehydrating diarrhea in African children, cholera can also lead to high mortality in some settings. Cholera epidemics in the 1970s and 1980s had high case-fatality rates in many countries in sub-Saharan Africa (Glass and Black, 1992). Dysentery (generally defined as loose or liquid stools with blood) does not commonly result in dehydration and therefore is less often life threatening. It may require specific antimicrobial therapy. Persistent diarrhea, usually defined as any diarrheal episode that continues for 14 days or more, is often found in children who have malnutrition and a high incidence of prior diarrhea. Therapy is focused predominantly on nutritional management during and after the illness.
There is limited information on the frequency of occurrence of the various clinical syndromes of diarrhea or the frequency of dehydration. In The Gambia, it was found that 17 percent of children had at least one episode of clinically dehydrating diarrhea in the first two years of life (Goh-Rowland et al., 1985).
EPIDEMIOLOGY
Diarrheal diseases are recognized as an important public health problem in the countries of sub-Saharan Africa. A recent review by Kirkwood (1991) of more than 100 surveys or longitudinal studies of diarrheal disease in 33 sub-Saharan African countries found that the overall median incidence of diarrhea was 4.9 episodes per year for a child less than 5 years old, and that the median prevalence was nearly 10 percent. Where information was available by age, the peak rates of incidence and prevalence appeared to occur in children 6-18 months old, as in other developing countries. In sub-Saharan Africa, diarrhea is generally the most common cause of death during the postneonatal period and the second most common among children aged 1-4 years.
Globally, diarrheal diseases are considered to be one of the two leading causes of death among children. Again, as summarized by Kirkwood (1991), a large number of studies using various methodologies to ascertain the causes of death indicated that a median of 38 percent of all deaths in children aged 0-4 years were associated with diarrhea, but within a wide range from 4 to 70 percent. Studies of the diarrheal mortality rate among children under age 5 are infrequent, and many of the studies that exist are of questionable validity. It is very difficult to obtain reliable estimates of incidence rates even with frequent surveillance. For example, reliability tests in Kenya suggest that mothers were overreporting diarrhea among children by 15 to 40 percent (Leeuwenburg et al., 1978). Among the studies using better methodologies, estimates ranging from 3.4 to 18.0 diarrheal deaths annually per 1,000 children under 5 years old were found for small areas of Kenya, Malawi, Senegal, and Tanzania.
It has generally been believed that many if not most of the childhood deaths associated with diarrhea in developing countries are the result of acute dehydration. Undoubtedly acute dehydrating diarrhea represents a substantial proportion of the diarrheal deaths, but it may be less a predominant cause than initially believed. Recent information from four countries (India, Bangladesh, Brazil, and Senegal) indicates that acute watery diarrhea accounted for about 35 percent (25-46 percent) of all diarrhea-associated deaths (Programme for Control of Diarrhoeal Diseases, 1991a). In Bangladesh, 40 percent of diarrhea-associated deaths in the age group 1-11 months and only 9 percent in the age group 1-4 years had acute watery diarrhea (Fauveau et al., 1991). The remainder of the diarrhea-associated deaths in these settings were associated with either acute or persistent dysentery or persistent nondysenteric diarrhea. In 30 villages in Senegal, 46 percent of the diarrhea-associated deaths in children under 5 years of age were with acute diarrhea, 47 percent with persistent diarrhea, and 8 percent with dysentery. In addition to the role of diarrhea as a primary cause of death, it may also contribute indirectly to high mortality through malnutrition and micronutrient deficiency, which are important underlying factors for a high proportion of child mortality in sub-Saharan Africa.
Information on the epidemiology of diarrhea in Africa indicates great similarity with other impoverished populations in developing countries that have crowded conditions, inadequate sanitation, limited quantity and quality of water, and poor personal and domestic hygiene (Kirkwood, 1991). One major source of infection is weaning foods, which are often stored and fed to the child throughout the day (Rowland et al., 1978; van Steenbergen et al., 1983). As in the other settings, malnutrition is common, and some infectious diseases such as measles and malaria may also increase the incidence or adverse consequences of diarrhea.
TREATMENT
Diarrheal disease control programs in developing countries, including those in sub-Saharan Africa, have focused primarily on the management of acute dehydrating diarrhea (Claeson and Merson, 1990). Studies begun in the 1970s demonstrated that diarrheal dehydration could be treated with oral as opposed to intravenous fluid and electrolyte replacement, potentially making this therapy much more widely accessible (Parker et al., 1985). Subsequent studies have borne out the applicability of oral rehydration therapy (ORT), along with continued feeding in the management of diarrhea. This approach, with the selective use of intravenous fluids for severely dehydrated cases, has formed the mainstay of diarrheal disease control programs. Unfortunately, not much attention has been paid to date to protocols for the correct use of antibiotics for the treatment of dysentery or to the dietary management of persistent diarrhea, and these two problems may account for a majority of the diarrhea-associated deaths.
The efficacy of ORT in comparison with intravenous therapy has been amply demonstrated in controlled research settings throughout the last two decades. Furthermore, the effectiveness of ORT in hospitals (based on inpatients) has also been proven. Studies of children under age 5 in hospitals in Angola, Malawi, and Nigeria have documented declines of 39 to 95 percent in case-fatality rates among all diarrheal patients (World Health Organization, 1988). Studies in Angola, Nigeria, and Zaire further documented reductions in under-5 inpatient diarrheal case-fatality rates ranging from 7 to 46 percent (World Health Organization, 1988). In only one study in Malawi did the inpatient case-fatality rate increase; this result was linked to an increase in the severity of cases that were admitted to the hospital, with more patients being managed as outpatients. In addition to reducing case-fatality rates, ORT programs in these major hospitals reduced inpatient admissions by 10-95 percent, and in several cases, the average number of days children were kept in the hospital declined by more than a day.
Although there has not been a population-based study that demonstrates a reduction in mortality from the introduction of ORT in hospitals in Africa, there has been one in a rural area of Bangladesh. This study indicated that in an area with high access to a diarrheal treatment center, facility-based care may have reduced infant mortality by 1-8 percent and 1- to 4-year-old mortality by 4-14 percent (Oberle et al., 1990). Another study in the same area of rural Bangladesh also suggested that the diarrheal treatment center resulted in an 8 percent reduction in infant mortality and a 12 percent reduction in 1- to 4-year-old mortality (Chen et al., 1983).
It has been hypothesized that the use of oral rehydration therapy begun early in an episode of diarrhea could prevent the development of dehydration and reduce related mortality. A number of community-based research
studies were conducted to evaluate the effect of home management of diarrhea on total and diarrhea-associated mortality. These studies are reviewed here briefly because they provide the only available evidence of the efficacy or effectiveness of diarrheal disease control programs in relation to mortality at a population level.
A study conducted between 1977 and 1979 in a remote area of Bangladesh compared mortality in a village in which oral rehydration solution was provided for episodes of diarrhea, with mortality in another village where persons had no home provision of treatment but were closer to a diarrheal treatment center than the treatment group (Rahaman et al., 1979). The study reported that the village with home ORT (78 percent of diarrheal episodes being treated) had a diarrheal mortality rate among infants of 1.6 per 1,000 compared to 17.4 per 1,000 population in the comparison area. The diarrheal mortality rate in children 1-4 years was 1.9 per 1,000 in the intervention area and 5.7 per 1,000 in the comparison area. Rahaman et al. (1982) compared the comparison group and other nonintervention areas and reported that the attendance rate at the diarrheal treatment center for persons living further away was lower. Also children living more than 2 miles away from the treatment center had higher diarrhea-associated mortality than those living closer to the center.
A number of studies have been conducted in Egypt, first as large-scale community-based intervention trials and later as evaluations of an extensive National Control of Diarrheal Diseases Program. A study begun in 1980 in the Nile Delta (Dakahlaia governorate) to compare various delivery strategies for oral rehydration therapy (Kielmann et al., 1985) described a decrease of 40 percent in total childhood mortality after the introduction of ORT through home visiting. A different intervention, also in the Nile Delta (Menoufia governorate), in the same time period did not succeed in substantially altering the diarrheal treatment practices in ''treatment villages" compared with "control villages," and reported no change in childhood mortality rates (Tekçe, 1982).
The National Control of Diarrheal Diseases Program (NCDDP) in Egypt later achieved wide use of ORT for diarrhea of 50 percent and higher. After the program had been in operation for four years, the intervention and control areas involved in the previous Dakahlaia governorate study were evaluated for trends in mortality (National Control of Diarrheal Diseases Project, 1988). In 1986 the use of ORT was equivalent in what had previously been intervention and control areas as a result of national program efforts. By this time, there was no longer a difference in mortality rates, which in both instances were about half of those at the onset of the intervention study in 1980. Most of the mortality reduction was reported to be related to a drop in diarrhea-associated mortality. Further evaluation of the NCDDP has indicated substantial declines in infant mortality of approximately
8 per 1,000 and diarrhea-associated infant mortality of approximately 7 per 1,000 on a national basis (Rashad, 1989, 1992; El-Rafie et al., 1990). The temporal concordance of the sharp drops in mortality with the increasing rates of treatment with ORT, along with the apparent decrease in diarrhea-associated but not other mortality in this period, has led to the conclusion that the program efforts resulted in the mortality reduction. However, because there were other changes during this time period, such as improvement in immunization coverage, changes in nutritional status, and enhancement of other health services, the direct contribution of the diarrheal disease control program or of other health programs cannot be quantified with certainty.
Unfortunately, few studies of the mortality impact of ORT programs have been done in other areas, and none have been done in sub-Saharan Africa. A study in India provided oral rehydration solution at a community level for episodes of diarrhea and reached levels of usage of up to 68 percent in study areas (Kumar et al., 1987). This study reported a substantial decrease in case-fatality rates and about a 60 percent reduction in diarrhea-associated deaths. However, the total childhood mortality rate in the areas differed by less than 10 percent from the rate in control areas.
The available studies suggest that childhood mortality can be reduced by diarrheal case-management programs that achieve a level of coverage of approximately 50-60 percent and effective use of oral rehydration therapy for diarrheal episodes. However, national diarrheal disease control programs have been variable in their success in achieving high coverage and effective use of ORT. Globally, it is estimated that 36 percent of diarrheal episodes are treated with ORT and the rate of use in sub-Saharan Africa is estimated by WHO to be similar (Programme for Control of Diarrhoeal Diseases, 1991b). However, it is recognized that ORT is not always utilized correctly (Touchette et al., 1990). Figure 4-1 illustrates the use of ORT during recent episodes of diarrhea, based on data from eight Demographic and Health Surveys (DHS) conducted in sub-Saharan Africa. A wide range of 3 to 72 percent is observed. In some countries, such as Botswana, Burundi, and Ghana, commercially prepared oral rehydration salts (ORS) are used more frequently. In Kenya and Nigeria, home-prepared solutions are used more often. (Zimbabwe did not report data on ORS.) Although approximately 70 percent of recent childhood diarrheal episodes received ORT according to the DHS in Botswana and Kenya, only 19 and 29 percent, respectively, of these cases were said to have received more fluids, as they should have (Boerma et al., 1991). Furthermore, although the recommendation is to continue the use of solid foods as before the illness, approximately half of the children in both of these settings were said to have been given less solid food during their illness. Also, the use of drugs, most of them unnecessary and some hazardous, remains quite high.
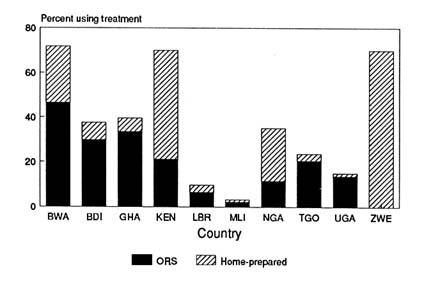
FIGURE 4-1 Use of oral rehydration therapy among children under 5 years of age, selected countries of sub-Saharan Africa. NOTE: Cases of diarrhea reported in the two weeks prior to survey. BWA—Botswana, BDI—Burundi, GHA—Ghana, KEN-Kenya, LBR—Liberia, MLI—Mali, NGA—Nigeria, TGO—Togo, UGA—Uganda, ZWE—Zimbabwe. SOURCE: Demographic and Health Survey reports (see Appendix B).
In eight DHS that collected information on the use of drugs during recent episodes of diarrhea, the median value was approximately 30 percent of episodes having received drugs, with a range of 10 to 44 percent (Boerma et al., 1990).
Demographic and Health Surveys can also be used to examine differentials in the use of ORT for treatment of diarrhea. Although children in the first six months of life may have a high risk of dehydration and subsequent mortality when they have diarrhea, eight DHS in sub-Saharan Africa (Botswana, Burundi, Ghana, Kenya, Liberia, Mali, Togo, and Uganda) consistently found that this age group had the lowest rate of use of ORT for diarrhea. In these surveys, there is evidence that use of ORS packets was higher in urban than in rural areas, with the exception of Kenya. In all countries except Uganda, there were higher rates of use of ORS among mothers with more education. ORS use was also higher in all countries in households with a radio. Thus, appropriate case management of diarrhea may still be inadequate in reaching the socially and economically disadvantaged populations of these countries, populations that are likely to have higher rates of childhood mortality.
With the severe limitations of data from sub-Saharan Africa, it is almost impossible to make calculations of current or future reductions in
child mortality because of diarrheal disease control program efforts. However, even simplistic calculations can provide a perspective on the relative magnitude of the mortality impact that might be expected. For illustrative purposes, we assume that (1) 50 percent of diarrhea-associated mortality can be prevented by ORT if it is used optimally, and (2) currently 35 percent of diarrheal episodes are treated in the countries of sub-Saharan Africa, but (3) only 50 percent of these are treated effectively. Given these assumptions, we can calculate the maximum effect on diarrhea-associated mortality by multiplying these fractions together. Thus, these calculations would suggest that present levels of diarrheal disease control program efforts in sub-Saharan Africa may be reducing diarrhea-associated mortality in children under 5 years of age by approximately 9 percent. If 40 percent of deaths under age 5 are associated with diarrhea, then these programs might be reducing mortality under age 5 by about 3 or 4 percent. Additional reduction of diarrhea-associated child mortality could be achieved by increasing the number of episodes treated with ORT, improving the quality of diarrheal management, and widening program focus to address more fully the problems of dysentery and persistent diarrhea.
SUMMARY
Diarrheal diseases are a major contributing cause of infant and child mortality worldwide. The median number of episodes among children under 5 in studies in sub-Saharan Africa was 4.9 per year, with peak rates occurring between ages 6 and 18 months. Estimates of mortality due to diarrhea vary widely across studies and across populations. However, diarrheal diseases are often among the top three causes of death.
Most interventions directed at diarrheal disease focus on the management of acute dehydrating diarrhea by using oral rehydration therapy and continued feeding. Little emphasis has been placed on antibiotic therapy for treating dysentery or on dietary management for persistent diarrhea. Oral rehydration therapy is commonly used, and both hospital-based and community-based studies show that it is efficacious in reducing mortality from dehydrating acute watery diarrhea, but may be of limited use for treating dysentery and persistent diarrhea. No evaluations of the mortality effect of ORT have been conducted in sub-Saharan Africa, and virtually all research conducted in the region has been hospital based. Although it is an effective treatment, it is often used incorrectly or not given to infants under 6 months of age.
There is a need for more research on how to improve the coverage and the quality of home-based treatment and on the mortality impact of programs that encourage the use of ORT. Research on educational and other programs could contribute to a reduced incidence of the infections that
cause diarrhea. Because the effect might be a reduction in mortality under age 5 of less than 5 percent, it would be very difficult to design studies that could document the effect of the programs on mortality rates.
MALARIA CONTROL PROGRAMS
Malaria is one of the major causes of death in Africa, and it is almost certainly responsible for the largest number of healthy days of life lost to disease in the entire population of certain countries (Ghana Health Assessment Team, 1981). It accounts for 20 to 60 percent of all illness seen in health facilities in the region, even though a large proportion of cases are treated only at home (Campbell, 1991). The World Health Organization has estimated that there are 1 to 2 million deaths worldwide from malaria each year (World Health Organization Scientific Group on the Chemotherapy of Malaria, 1990); most of these are in sub-Saharan Africa. Malaria mortality and morbidity may actually be increasing (Greenberg et al., 1989; Brinkmann and Brinkmann, 1991) as malaria moves into areas where it was previously absent or under control (e.g., Trape, 1987; Gascon et al., 1988, quoted by Brinkmann and Brinkmann, 1991).
The treatment of malaria is increasingly complicated by resistance to chloroquine. Brinkmann and Brinkmann (1991) concluded that in most countries of Africa, chloroquine resistance is found in from 25 to more than 60 percent of children. Recent studies have documented chloroquine resistance in all areas of the continent including most recently Senegal (Trape et al., 1989), Liberia (Björkman et al., 1991), and other parts of West Africa (Moran and Bernard, 1989), Somalia (Warsame et al., 1991), and South Africa (Freese et al., 1991). However, treatment with chloroquine remains effective in the majority of cases.
EPIDEMIOLOGY
Malaria is a parasitic disease that is spread by mosquitoes. Various stages of the parasite's life cycle must take place inside mosquitoes, so direct transmission between individuals is not possible except through blood transfusion. Therefore, the study of malaria transmission and of potential control measures includes studies of the biology of the parasite, the life cycle of mosquitoes, and the natural history of the disease in man.
There are several species of malaria. The most dangerous species is Plasmodium falciparum, which is very common in Africa. Other types include P. vivax, P. ovale, and P. malariae. The clinical manifestations of malaria often include a cycle of shaking chills, intense fevers, and drenching sweats. However, the symptoms vary greatly, especially among individuals
who have acquired some immunity to the disease. Severe cases, generally from P. falciparum, can lead rapidly to death, often from cerebral malaria—a type of malaria in which the parasites clog capillaries in the brain. Other severe complications include renal failure, hypoglycemia, severe anemia, pulmonary edema, and shock. The wide range of symptoms can make diagnosis difficult. A definitive diagnosis of malaria infection is based on microscopic verification of the presence of parasites in the blood.
The epidemiology of malaria depends on the environment and its effect on the mosquito population. Malarious areas have been characterized by the level and seasonality of transmission as holoendemic (if transmission is year-round), hyperendemic (seasonal transmission), mesoendemic (a low level of transmission with occasional severe epidemics), or hypoendemic (limited transmission).
Individuals who have had repeated cases of malaria can develop partial immunity to it. However, repeated exposure is required to maintain this immunity. Thus, adults in holoendemic areas often have high levels of immunity. In mesoendemic regions, transmission is not frequent enough to maintain high levels of immunity. Thus, the severity of malarial infections is related to the level of transmission. Because children must have malaria before they can develop effective levels of immunity, malaria mortality is especially high in children in holoendemic and hyperendemic areas.
The Institute of Medicine Committee on Malaria Prevention and Control (Oakes et al., 1991) recently completed a report that covered a wide range of issues, including the current state of knowledge about the disease, the efficacy of current drugs, the economics of malaria, and priorities for research on new drugs and vaccines. The report presented eight paradigms that describe the range of ecologies in which malaria persists. These paradigms are not a complete classification system; they merely suggest the variety of circumstances in which malaria presents a serious health problem.
The paradigm that characterizes most of the areas in Africa where malaria is a serious health problem is the African savanna. The report (Oakes et al., 1991:217-218) states that
eighty percent of the world's malaria and 90 percent of mortality due to the disease occur in Africa south of the Sahara, mostly in the savannah regions .… Malaria transmission is seasonal and correlates with relatively predictable patterns of rainfall, although transmission may continue at lower levels during the dry season. Because of the extremely high inoculation rates, virtually all of those living in these areas become infected early in life. For children, treatment … may prevent death long enough for acquired immunity to establish itself, which can provide protection from malaria-related death or illness later in life. Young children who do not
acquire this protective immunity, and whose infections are not treated adequately or promptly, are at particular risk of dying from the disease.
Six of the other seven paradigms are also represented in parts of Africa:
forest malaria, which describes parts of equatorial and central Africa;
malaria associated with irrigated agriculture, including the commercial cotton farms of the Gezira in the Sudan;
highland fringe malaria, in parts of Ethiopia and the mountain slopes of Kenya;
desert fringe and oasis malaria, found in areas such as the Sahel, on the fringes of the Kalahari desert, and in parts of Ethiopia;
urban malaria; and
seashore malaria.1
In some areas, the features of the environment and the disease suggest a combination of these paradigms, such as riverine malaria, which "is usually an intensification of either plains malaria or African savannah malaria, and associated with greater potential for vector breeding" (Oakes et al., 1991:221).
The diversity of malaria in sub-Saharan Africa is so great that there is no consensus on the best ways to approach the disease. There is agreement that no single approach makes sense for all types of areas (Oakes et al., 1991). However, national health programs have very limited resources for evaluating the situation in each local area.
MALARIA MORTALITY IN SUB-SAHARAN AFRICA
Estimates of mortality and morbidity from malaria are uncertain even in the best of circumstances. For example, in an excellent study of malaria mortality in The Gambia, 23 of 25 children who died of malaria died at home, 2 died in a dispensary, and none died in the hospital. Only six had received any treatment for the final illness other than traditional medicine or treatment at home (Greenwood et al., 1987). Therefore, few of these cases were ever seen by modern health workers and most of the deaths were ascribed to malaria using verbal autopsies.
In many studies, diagnosis of cause of death is based on information collected in verbal autopsies, although diagnosis is uncertain even in a clinical setting (Bassett et al., 1991). Simple microscopic tests can improve diagnosis. However, even when performed correctly this approach is problematic.
In nonimmune patients, symptoms can arise from very low rates of parasitemia (i.e., parasites in the blood), which may become apparent only after repeated blood films. Moreover, when parasites are detected, there is no way to establish that the malaria infection is responsible for the observed symptoms. This lack of clarity is especially common for individuals with partial immunity to the disease who may be asymptomatic when infected (Oakes et al., 1991).
Good estimates of the contribution of malaria to child mortality rates in Africa are currently not available. The studies of causes of death reviewed in Chapter 2 suggest that malaria is often the third or fourth leading cause of mortality under age 5. However, the sensitivities and specificities of the usual criteria for diagnosing malaria by verbal autopsies are not very high. Therefore, estimates from verbal autopsies are probably useful only in age groups or seasons where malaria is responsible for 10 to 25 percent of deaths.
Greenwood et al. (1987) estimated that in a rural area of The Gambia, the malaria mortality rate was 6.3 per 1,000 among infants and 10.7 among children aged 1-4 years. These rates amounted to 4 percent of infant deaths and 25 percent of child deaths. However, it is likely that malaria mortality rates in this area vary substantially from year to year. A study of children less than 3 years of age in a coastal area of Benin estimated that the death rate due to malaria was probably about 8 deaths per 1,000 children (95 percent confidence interval (C.I.) 3.7-14.2 deaths per 1,000 children) (Velema et al., 1991). The rate was highest in the second year of life (14.9 per 1,000 children, 95 percent C.I. 11.2-18.6 per 1,000 children). A hospital-based study in Kinshasa, Zaire, estimated that the mortality rate to malaria was at least 4 per 1,000 in infants and 1.6 per 1,000 at ages 1-4 years (Greenberg et al., 1989).
PROGRAM OPTIONS
In 1959, the Eighth World Health Assembly adopted the goal of eradicating malaria. However, sub-Saharan Africa was excluded from immediate plans for eradication because of the perceived magnitude of the malaria problem and the lack of technical and organizational capability in the region. There were success stories during the 1950s and 1960s, especially in cities and at higher altitudes (e.g., Taylor and Mutambu, 1986). However, the goal of eradication proved to be elusive. In 1960, the World Health Assembly revised its global malaria strategy to emphasize control of malaria in areas where eradication was not possible.
The complex epidemiology of malaria provides several stages at which interventions can reduce the transmission or severity of cases. Spraying with insecticides and eliminating mosquito breeding grounds reduce the
population of mosquitoes. If the number of mosquitoes is reduced enough, malaria incidence rates will fall. Bed nets and mosquito coils can reduce the incidence of mosquito bites and thereby reduce transmission from mosquitoes to humans. Chemoprophylaxis is the use of antimalarial drugs (often chloroquine or mefloquine) to protect against malarial infections. Treatment of cases (or presumed cases) of malaria reduces the severity and duration of the disease.
During the 1950s, most antimalarial programs were based on spraying with insecticides. This approach requires regular coverage to all areas for extended periods of time. It also requires careful monitoring of the levels of insecticide resistance among mosquitoes or the introduction of progressively more expensive insecticides. In most parts of Africa, these malarial control programs have not been sustainable because of the high degree of organization required and the increasing costs associated with insecticide resistance. However, some of the best evidence on the potential effects of malaria control on mortality comes from research on the effect of spraying programs.
The following sections review the evidence of the effect of malaria eradication on mortality and the effectiveness of three types of antimalarial programs. The first is presumptive treatment of suspected cases with antimalarial drugs, which includes both a review of the effect of programs designed to increase the proportion of cases treated with chloroquine and a review of studies of the importance of self-treatment. The second is chemoprophylaxis for pregnant women, which is designed to reduce the incidence of complications of pregnancy, low birthweight, and anemia among children. Finally, we briefly examine the potential of bed nets treated with insecticide.
Today the outlook for global eradication of malaria is very dim. The spread of drug-resistant malaria and insecticide-resistant mosquitoes has made control even more difficult than it was 20 years ago. One promising change is the development of malaria vaccines. There is evidence that immunization with various antigens can both reduce the consequences of malaria infections and help to disrupt transmission of the disease. However, efficacious vaccines will not be available for large-scale use for several years (Oakes et al., 1991).
STUDIES OF THE EFFECT OF MALARIA ERADICATION ON MORTALITY
There have been three studies attempting to eradicate malaria from small areas of Africa. These studies suggest the importance of malaria, but do not offer practical solutions for reducing its effect.
Pare-Taveta Malaria Scheme (1954-1959)
Conducted in northeastern Tanzania, the Pare-Taveta project reduced malaria transmission to very low levels through residual spraying of houses with dieldrin. The crude death rate dropped from about 24 per 1,000 to between 12 and 16 per 1,000 of all ages following spraying, and the infant mortality rate dropped from a range of 165-260 per 1,000 live births to between 78 and 132 deaths per 1,000 live births (Draper, 1962; Bradley, 1991a).
A second study, the Pare-Taveta Vital Statistics Survey (Pringle and Matola, 1967), covered the period 1962 to 1966 after the spraying program ended. It was designed to determine whether mortality returned to previous high levels. Although mortality at ages 1-4 returned to the earlier levels, mortality at other ages remained at the new lower levels. There were extensive investigations into the entomological and parasite biology and ecology to try to explain this result. The researchers concluded that the lower mortality rates were sustained in most age groups by a substantial, though undocumented, increase in the use of antimalarial drugs for presumptive treatment of fevers (Draper et al., 1972; Bradley, 1991a).
Kisumu Project
The Kisumu project tested the effect of residual spraying with fenitrothion on mortality in a district of Kenya (Payne et al., 1976). The daily malaria incidence rate dropped by about 96 percent in the program area. The crude death rate in the treated area declined from 24 deaths per 1,000 in the year preceding the spraying to 16 and 13.5 during the two subsequent years. The death rate in the control area actually increased slightly from 23 to 26 and 24, respectively, in the two subsequent years. The infant mortality rate dropped from 157 deaths per 1,000 in unprotected infants to 93—a 41 percent reduction. The drop in infant mortality affected only infants over 3 months of age.
Garki Project
The Garki project tested the effects of house spraying and prophylactic drug use on malaria in the northern part of Nigeria (Molineaux and Gramiccia, 1980). This area is part of the Sudan savanna that runs across Africa from Senegal to the Sudan. In the Garki area, transmission of malaria was more intense and more seasonal than in Kisumu (Molineaux, 1985). The project tested residual spraying with propoxur, both with and without periodic mass drug administration. In one area there was distribution of sulfalene-pyrimethamine every 10 weeks; in a second area, the frequency of distribution was increased
to every 2 weeks during the wet seasons when malaria was most prevalent.
Before the start of the program, about 47 percent of the population tested positive for Plasmodium falciparum during the dry season and about 60 percent during the wet season (Molineaux and Gramiccia, 1980). Spraying alone brought about little change in the prevalence of infection. During the first wet season, prevalence in the spraying area was only 15 percent below the rate in the control area. During the second dry season, it was 26 percent below the rate in the control area. House spraying was not as successful in Garki as it was in Kisumu because a large proportion of the mosquitoes in Garki remained outside the houses and were not affected by spraying. During the dry season, the addition of mass drug administration every 10 weeks dropped the prevalence to 98 percent below the rate in the control area, but did not interrupt transmission. In the second wet season, the prevalence was only 72 percent below the rate in the control area. More frequent drug distribution reduced the prevalence by at least 95 percent, but still did not interrupt transmission.
The demographic data collected by the Garki project were extensive. However, the analysis of the data was weak and the sample size was small, leaving a number of questions unanswered. The mortality data for the baseline year suggested that it was not typical. The infant mortality rate (IMR) during the baseline was 246 deaths per 1,000 live births. During the following two years the IMR in the control area was only 155.2 This difference is significant at the 5 percent level.3 During the first intervention year, the IMR was 135 in the control area and only 55 in the treatment area (all treatments combined). For the whole intervention period the rates were 155 and 73, which are significantly different at the 5 percent level. However, we do not know how much of this difference between the control area and the intervention areas might be due to differences that existed before the start of the program. Although Molineaux and Gramiccia (1980) reported that the IMRs in the intervention and control areas were not significantly different at the baseline, they do not report the actual values. They also did not present the IMRs separately for the spraying area and the area that received both spraying and mass drug administration. The data in the figures showing seasonal fluctuations suggest that the decline in the IMR was larger in both types of intervention areas than in the control area (Molineaux
and Gramiccia, 1980:237-239, Figures 68-70). However, without baseline data for the various areas, we do not know if the differences between the declines were statistically significant.
The link between malaria control and differences in the IMR in the intervention and control areas was strengthened by the relationship between the infant death rates and the infant parasitological conversions rate (ICR), which measured the rate at which infants became infected. During the baseline year and in the control area data, there was a close relationship between the seasonal patterns of the IMR and the ICR. With the start of the program, the seasonal pattern disappeared and the IMR dropped in the intervention areas.
The mortality rate at 1-4 years also appears to have dropped in both the control and the intervention areas during the first year of intervention. However, the decrease in the areas that received both insecticide and mass drug administration (70 percent) was much larger than the drop in the control area and the area that received only insecticide (both about 25-30 percent). There was also a sharp change in the seasonal pattern of mortality in the intervention area. Molineaux and Gramiccia (1980) did not present an analysis of changes in mortality over age 5.
The Garki project demonstrated that in some environments in Africa it is not feasible to interrupt transmission of malaria. Even with extensive spraying and frequent distribution of prophylactic drugs, the Garki project never interrupted transmission even during the dry seasons. The high cost of this intensive approach and the complications introduced by insecticide and drug resistance reinforce this conclusion.
PRESUMPTIVE TREATMENT OF FEVERS WITH ANTIMALARIAL DRUGS
Each of the three projects reviewed above demonstrated that mortality under age 5 would decline if we could greatly reduce or eliminate malaria. However, there is currently no feasible method for accomplishing these tasks in most of Africa. The high costs and the heavy logistical requirements of control programs are among the reasons for this conclusion. Also supporting this conclusion are the exceedingly high transmission rates of malaria in much of Africa. In some areas, rates are so high that a program would have to reduce transmission by a factor of as much as a thousand to bring malaria under control (Bradley, 1991b). Therefore, as Campbell (1991:1,208) has noted "the challenge for control of malaria in African children is to develop operational strategies that will minimize the risks of illness without eliminating the continued exposure to infection necessary for maintaining clinical immunity."
Aggressive programs to provide chemotherapy are often advocated to
achieve this balance. In most cases these programs take the form of presumptive treatment with chloroquine of all childhood fevers in malarious areas during malaria seasons. The practical reason for presumptive treatment of all fevers is that in areas where malaria is a serious problem, it is not feasible to identify those fevers that are due to malaria, even when microscopy is available and performed correctly (Bradley, 1991b; Oakes et al., 1991). Moreover, in most of Africa, microscopic verification is not available.
The potential efficacy of presumptive treatment depends in part on the proportion of fever cases that are attributable to malaria. Greenwood et al. (1987) estimated that in a rural area of The Gambia, only 40 percent of cases of fever in children under age 7 were attributable to malaria. In a monthly household survey in Benin, only about 33 percent of fever cases in children under 3 years of age were attributed to malaria (Velema et al., 1991).
Even if the fever is not caused by malaria, treating a preexisting case of malaria may reduce the overall infectious load enough to increase the child's chance of surviving. For example, Greenwood et al. (1987) found that 64 percent of fever cases had malaria parasites in their blood. The proportion of fever attributable to malaria, and therefore the potential of presumptive treatment, vary across areas and often by season. At a health clinic in Niamey, Niger, 54 percent of children with fever in the rainy season had malaria. However, in the dry season, only 3.6 percent had malaria (Olivar et al., 1991). Thus, these proportions may understate the potential for presumptive treatment.
There are many questions about the long-term efficacy of presumptive therapy in reducing mortality in Africa. In some cases, presumptive treatment may simply delay the onset of a massive attack. For example, such a delay has been suggested as an explanation for the appearance of cerebral malaria in teenagers in Banjul, The Gambia (Bradley, 1991b).
Chloroquine is still the most commonly used drug for presumptive treatment because of its safety and low cost. However, the efficacy of chloroquine is reduced in much of the continent by chloroquine resistance. As chloroquine resistance increases, many cases still show clinical improvement immediately following treatment (e.g., reduced fever). However, fever and other symptoms can return very quickly because of a failure to completely clear all parasites. When treatment fails within a few weeks, the child may not be able to recover fully from the attack. A study in Malawi (Centers for Disease Control, 1991) demonstrated that anemic children with malaria did not recover from the anemia after treatment with chloroquine. However, those treated with Fansidar showed increased hemoglobin levels within three weeks. Chloroquine resistance may be the cause of the reported increasing severity of pediatric anemia (Greenberg et al., 1989).
Studies of the Effect of Programs Designed to Increase Presumptive Treatment of Fevers with Chloroquine
Three basic strategies can be used to increase the proportion of fever cases treated with antimalarial drugs. The first is to encourage parents to take children to a health center whenever they have fever. A second is to train village health workers to treat fevers with antimalarials and to refer serious cases to a health center. The third strategy is to encourage home use of antimalarials for treatment of simple cases of fever. There are two studies conducted in Kenya and The Gambia that examine the efficacy of programs that rely on village health workers to treat cases of fever with chloroquine, as well as one study of an education program to increase home use.
Saradidi Health Development Project
The Saradidi Health Development Project was a community health program in western Kenya based on village-level organizations and "village health helpers" (VHHs) (Kaseje and Sempebwa, 1989). The program raised funds to build buildings for clinics, maternity services, and other facilities necessary for providing community health services. The VHHs provided health education on topics including environmental health, promotion of maternal and child health services and immunizations, family planning, and nutrition education. In selected areas, they provided antimalarial chemoprophylaxis (i.e., use of drugs to prevent infection) for pregnant women and treatment for malaria. A comparison of mortality rates before and during the community-based malaria control intervention showed a significant decline in child mortality (ages 1-4 years) in the intervention areas (from 25.5 to 18.2 per 1,000). However, this decline was apparently due to lower measles mortality and not to the antimalarial activities (Spencer et al., 1987). The research team concluded that "the most likely reason for the lack of any detectable effect is that there was already a high level of chloroquine use for illness presumed to be due to malaria before the program" (Spencer et al., 1987:14). The main change in treatment patterns was a change in the source of chloroquine from shops and health clinics to the village health helpers (Mburu et al., 1987).
Village Health Workers in The Gambia
A study in The Gambia (Greenwood et al., 1988; Menon et al., 1990) compared mortality and malaria morbidity rates in three areas. Two areas were included in the government's primary health care (PHC) program. In both areas, village health workers (VHWs) learned to treat malaria with
chloroquine. In one of the areas the VHWs also distributed, every two weeks, malaria chemoprophylaxis or a placebo to all children aged 3-59 months of age. Children were allocated to the chemoprophylaxis or placebo group randomly by compound. The third area was not covered by the PHC program, but treatment of malaria was available from a dispensary.
The authors (Greenwood et al., 1988:1,125) summarized their results for 9 to 21 months after the start of the program as follows:
Treatment of presumptive clinical malaria by VHWs with chloroquine had no significant effect on mortality and morbidity from malaria in young Gambian children whilst treatment combined with malaria chemoprophylaxis given by VHWs reduced mortality and morbidity in children aged 1-4 years. … [Chemoprophylaxis did not reduce mortality in infants aged 3-11 months, for … malaria accounts for only about 4% of deaths in infants.
The results remained the same in a second study 33 to 45 months after the start of the program (Menon et al., 1990).
For whatever reasons, the program apparently did not lead to a large increase in presumptive treatment of fevers with chloroquine. Because the VHWs were only voluntary workers, they may not have been able to provide sufficient coverage for acute episodes. In the villages with primary health care, children received an average of 0.52 regimens of chloroquine per year, which included an average of 0.34 regimens distributed by the VHWs and 0.18 regimens from a dispensary. In the non-PHC villages, children received an average of 0.42 regimens from a dispensary. Both averages are probably too low in a community where children have an average of 0.5 to 1.0 clinical episode of malaria per year. Therefore, the VHWs failed to achieve a meaningful increase in the proportion of cases treated with chloroquine. However, the study did not provide information on whether the use of VHWs changed the promptness of treatment, amount of drug taken, or duration of treatment.
Conclusions About the Effectiveness of Programs to Increase Presumptive Treatment
Because the village workers in both of these programs failed to increase treatment levels significantly, the studies do not provide tests of the efficacy of presumptive treatment. Instead they test the use of village health workers to increase presumptive treatment. Therefore, we still do not know what would happen if we could achieve presumptive treatment of all fevers with chloroquine.
It may not be possible to conduct a trial of presumptive treatment with chloroquine because in most places where malaria is a significant problem, presumptive treatment of fevers is already common. Case-control studies
would be hindered by problems of retrospective reporting of general treatment practices as well as specification errors resulting from use of other modern treatments for other diseases. It may be that studies could be based on prospective surveys comparing families that report relying on use of chloroquine with other families. However, even this approach is not likely to provide a reliable estimate of the efficacy of presumptive treatment because of the likelihood of other differences between these two groups of families.
Studies of Self-Treatment
Self-treatment of fevers with antimalarials (generally chloroquine) is very common in many parts of sub-Saharan Africa. The term self-treatment refers to treatment that was not given during or after a visit to a health center. It can include, but is not limited to, use that was recommended by a pharmacy, commercial shop, or traditional healer. In general, self-treatment is based on drugs acquired at a shop or from a health clinic during a visit for a previous disease episode. Table 4-1 summarizes the importance of self-treatment found in studies in eight areas of Africa. Between 8 and 98 percent of children received self-treatment for fevers.
Data from the Demographic and Health Surveys suggest that self-treatment is very common. Most of the DHS in Africa inquired about recent cases of fever among children 1-59 months of age. They generally asked whether the child was taken to a medical facility and what treatments were received. Table 4-2 shows that antimalarial use was reported for 20 to 74 percent of recent cases of fever among children and that in most of the surveys, about half of the recent cases of fever were treated at a medical facility (Burundi, Ghana, Kenya, Senegal, and Uganda all reported values between 48 and 58 percent). In Botswana, 90 percent reported going to a medical facility, whereas 3 percent did in Mali and 31 percent in Togo.
The DHS did not ask where the drugs were acquired or whether they were prescribed by a doctor. Therefore, we do not know how many children received antimalarials before going to a clinic. However, we can derive a minimum estimate by looking at the proportion of children who reportedly received antimalarials but did not attend a health facility. Table 4-2 shows that in the five countries where the DHS provides the relevant information, 9 to 35 percent of recent cases of fever among children were reportedly treated by antimalarials but not at a health facility. It is likely that many children who did attend a clinic received antimalarials before going to the clinic. This is especially true for Ghana, Senegal, and Uganda, where about half of all children with fever were taken to a health clinic.
The most detailed study of self-treatment of fever was carried out by Deming et al. (1989) in the Plateaux Region of Togo. They found that 83
TABLE 4-1 Home-Based Presumptive Treatment of Fevers in Children with Antimalarial Drugs, Eight Areas of Sub-Saharan Africa
Area | Cases of Fever Receiving Antimalarials at Home (%) |
Urban |
|
Ghana (Accra) | 56 |
Guinea (Conakry) | 51 |
Rural |
|
Ghana (Berekuso) | 98 |
Guinea (Dinguiraye) | 13 |
Guinea (Dabola) | 21 |
Rwanda (national) | 8 |
Togo (Plateaux) | 83 |
Zaire (Kingandu and Pai-Kongila) | 28 |
NOTE: Estimates for Ghana assume that the distribution of drugs used for treating fever is the same for home treatment (which accounted for 87 and 94 percent, respectively, of treatments) as for all treatment. SOURCE: Deming (1989), except for data from Ghana, which is from Gardiner et al. (1984). | |
percent of children with a recent case of suspected fever were treated with antimalarial drugs (almost always chloroquine) at home before attending or instead of attending a clinic. Mothers stated that virtually all (97 percent) children treated at home with antimalarials began treatment on the first day of their fever. In contrast, only 17 percent of children who were taken to a clinic were taken on the first day of fever. This difference is of consequence, given the importance of early treatment (World Health Organization, 1990).
Deming et al. also compared the dose reported by mothers to that required for the child's weight. This comparison led to an estimated mean dosage of 8.9 milligrams of chloroquine per kilogram of body weight during the first 24 hours of therapy. At the time of the survey, the recommended treatment with chloroquine was a single dose of 10 milligrams per kilogram during the first 24 hours. The mean dosage did not differ significantly for children 0-1 and 2-4 years. Only 1 percent of reported dosages during the first 24 hours were 20 milligrams per kilogram or higher, a value taken to represent potentially serious toxicity. The mean total dose per episode of malaria was 16.6 milligrams per kilogram.
It appears, therefore, that in at least one area of Africa, self-treatment of presumed fever was very prompt and the reported dosages were very
TABLE 4-2 Treatment Patterns (percent) Among Children Aged 1-59 Months Who Had a Fever, Nine Countries of Sub-Saharan Africa
Country | Treated with Antimalarials | Taken to Health Center or Doctor | Treated with Antimalarials but did not Attend Health Center |
Botswana | n.a. | 90.2 | n.a. |
Burundi | 19.8 | 49.9 | 8.8 |
Ghana | 24.9 | 56.4 | 12.3 |
Kenya | n.a. | 55.5 | n.a. |
Liberia | 73.5 | n.a. | n.a. |
Mali | 35.5 | 2.9 | 34.6 |
Senegal | 26.7 | 57.6 | 17.9 |
Togo | 56.5 | 30.8 | n.a. |
Uganda | 57.1 | 48.3 | 28.0 |
NOTE: n.a. = not available. SOURCE: Demographic and Health Survey reports (see Appendix B). | |||
close to the recommended levels.4 This result was obtained despite the fact that self-treatment was not promoted as a national policy or encouraged as an alternative to treatment at health centers, although it was recommended in local health education projects.
A study in The Gambia (Menon et al., 1988) tested an education program designed to improve self-treatment of malaria. In this area, they found that women knew little about the causes of malaria, and few (2 percent) reported that they would use chloroquine first if they thought their child had malaria. After an education campaign, 91 percent knew the correct treatment for various hypothetically ill children. In a prospective survey, about 70 percent of women gave chloroquine as instructed for treatment of fever. However, many also gave chloroquine for upper respiratory, gastrointestinal, and dermatological symptoms presumably not related to malaria.
This study suggests the potential for education programs aimed at proper treatment of fevers. However, it demonstrates that these education programs must be designed to help mothers identify malaria and to recognize serious cases that require immediate medical attention. This type of education program might be combined with a program that uses village health workers who could periodically reinforce the education messages.
As noted earlier, self-treatment is not inconsistent with attendance at a health clinic. In a pilot study in Accra, Ghana (Orofi-Adjei et al., 1984), nine children presenting with fever and anemia were tested for serum chloroquine levels. Although only two cases admitted to using chloroquine prior to admission, seven of the children had chloroquine in their serum. Prior medication can complicate treatment at the clinic since prescription of additional chloroquine can lead to overdosing (World Health Organization, 1990). Also, continued treatment with chloroquine may unnecessarily delay treatment with other drugs in cases of chloroquine resistance.
PROGRAMS BASED ON CHEMOPROPHYLAXIS AMONG PREGNANT WOMEN
Chemoprophylaxis is the use of antimalarial drugs to prevent cases of malaria. The World Health Organization Scientific Group on the Chemotherapy of Malaria (1990) concluded that "chemoprophylaxis is only recommended at present for special risk groups, notably pregnant women, nonimmune travellers, and nonimmune persons living in closed communities in endemic areas for fixed predetermined periods (e.g., labor forces and police and army units)." For this reason, chemoprophylaxis is rarely a component of health programs in Africa. Therefore, we have not reviewed the extensive literature on the efficacy of chemoprophylaxis for young children. We have reviewed studies about use of chemoprophylaxis among pregnant women, which is a part of many health programs.
The recommendation of chemoprophylaxis during pregnancy rests on the following chain of reasoning:
Proposition 1: Malaria during pregnancy has been associated with anemia, miscarriage, fetal death, intrauterine growth retardation, low birthweight, and preterm delivery. Most studies find that these effects are concentrated in first pregnancies (i.e., primigravidae). See, for example, studies of low birthweight and malaria (Gilles, 1969; McGregor, 1984).
Proposition 2: Chemoprophylaxis during pregnancy can prevent or effectively treat malaria and reduce the incidence of low birthweight and anemia during pregnancy. Figure 4-2 presents the estimates of the effect of prophylaxis on birthweight in first births from six randomized trials in Africa (Burkina Faso—Cot et al., 1992; Uganda—Hamilton et al., 1972; The Gambia—Greenwood et al., 1989; Imesi, Nigeria—Morley et al., 1964; Ibadan, Nigeria—Gilles et al., 1969; and Zaria, Nigeria—Fleming et al., 1986). The studies differ substantially in sample size, so the width of the bars in the figure is roughly proportional to the inverse of the variance of the estimate of effect. The two largest studies (Hamilton et al., 1972; Cot et al., 1992) found difference in birthweights among first births of about 80 grams
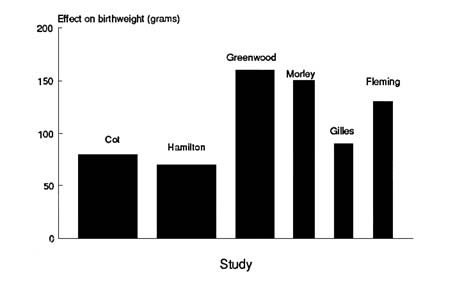
FIGURE 4-2 Effect of malaria prophylaxis on birthweight, first births in six randomized trials in Africa. NOTE: Width of bars proportional to the inverse of the variance of estimate. Sources: Morley et al. (1964); Gilles et al. (1969); Hamilton et al. (1972); Fleming et al. (1986); Greenwood et al. (1989); Cot et al. (1992).
associated with prophylaxis, although this difference was not significant in either study.5 In the third largest trial (Greenwood et al., 1989), the estimated effect on first births was much greater and was significant at the 5 percent level. The overall average effect of prophylaxis in all of the studies was about 100 grams.6 The similarity of the results is impressive, given the differences in study designs, treatment regimens, ecological settings, and levels of treatment provided to the control group. For example, the proportion of pediatric deaths in Togo ascribed to malaria or anemia increased steadily between 1986 and 1989 (Centers for Disease Control, 1991) and the number of cases of malaria reported in Burundi almost tripled between 1987 and 1992 (Republique du Burundi, 1993). In addition, case-fatality rates of malaria have increased in Zaire and the Central African Republic (Centers for Disease Control, 1991).
Four of the studies (Cot et al., 1992; Hamilton et al., 1972; Greenwood et al., 1989; Morley et al., 1964) give estimates for the effects in later pregnancies. These estimates are more difficult to compare because the studies grouped the parities differently and the largest study (Cot et al., 1992) did not provide a separate estimate for higher parity women.7 It appears that prophylaxis has little or no effect on births of order 2 through 4, but may be beneficial among higher parity women.
Several of these studies also examined the effect of chemoprophylaxis on the incidence of anemia during pregnancy. Greenwood et al. (1989) found that prophylaxis affected hemoglobin levels only in the primigravidae. Gilles et al. (1969) and Fleming et al. (1986) also demonstrated this effect in primigravidae.
Proposition 3: Low birthweight is associated with increased risk of infant death. The literature on this topic is reviewed in Chapter 5.
Although the research supports each of these propositions, only two studies have been uncovered that present data on the effect of chemoprophylaxis on child survival. Greenwood et al. (1989) show that the stillbirth and neonatal mortality rates were lower among first pregnancies for women who received Maloprim than for women who received a placebo. However, the rates were not significantly different. When neonatal mortality and stillbirths are combined, first pregnancies led to a bad outcome 8.1 percent of the time for those on prophylaxis and 15.4 percent of the time for those on placebo (relative risk of 0.53 times; 95 percent C.I. 0.20-1.37 times). Among later pregnancies there was virtually no difference associated with prophylaxis (4.4 percent compared to 6.0 percent for the control group). Morley et al. (1964) found no difference in the combined stillbirth and neonatal mortality rate associated with prophylaxis for women of all parities.
There are several ways the logic that links these three propositions could prove misleading. First, if the effect of chemoprophylaxis on birthweight is very small, it might not lead to any noticeable difference in child survival. Second, most of the studies present data on mean birthweights. However, the proportion with low birthweight is probably a better measure of the potential effect on child survival. Cot et al. (1992) reported that the relative risk of low birthweight among primigravidae was 0.88 for those on prophylaxis, compared to the controls, although this difference was not significant. Greenwood et al. (1989) reported that prophylaxis was associated
with a drop in the proportion with low birthweight among primigravidae from 22 to 5 percent (probability less than .05).
Third, some studies show that the rate of malaria parasitemia may decrease during the last trimester even without treatment (McGregor, 1984). If the growth retardation associated with malaria occurs at a different stage of pregnancy than retardation caused by other factors, the relationship between low birthweight and child survival may differ as well. Similarly, it is not clear whether malarial infections lead to short gestation or to growth retardation (i.e., low weight for gestational age).
Fourth, the use of chemoprophylaxis in pregnant women is complicated by the increasing prevalence of chloroquine resistance. Chloroquine is inexpensive, relatively safe, and well-tolerated, and the general policy on chemoprophylaxis during pregnancy relies heavily on these features of the drug. Although chloroquine may be more effective in adults who have partial immunity than in children, several studies have indicated high failure rates (i.e., breakthrough with a clinical attack of malaria during pregnancy) of chloroquine prophylaxis among pregnant women (McDermott et al., 1988; Mutabingwa et al., 1991). The alternatives to chloroquine for chemotherapy are quite limited. The Institute of Medicine (Oakes et al., 1991:67) concluded that ''the safety and efficacy of alternative prophylactic regimens in pregnancy is an open question."
A study in Tanzania suggested that chloroquine is still a useful drug for pregnant women in areas where chloroquine resistance is common. However, chemoprophylaxis with a weekly dose of chloroquine was more apt to lead to failure than daily doses of proguanil (Mutabingwa et al., 1991).
McDermott et al. (1988) studied the efficacy of chloroquine in Malawi, which ad had documented chloroquine resistance for several years. They found that chloroquine was successful in clearing malaria parasitemia in 9 of 19 pregnant women and may have reduced placental infection rates.8 However, 25 percent of women (18 of 73) experienced breakthrough parasitemia during pregnancy while they were taking either chloroquine or amodiaquin, with no significant difference between the two drugs.
Finally, programs designed to deliver prophylaxis to pregnant women would have to address the issue of coverage rates and compliance. For example, a study in Saradidi, Kenya, showed that only 29 percent of pregnant women attending maternal and child clinics were taking chemoprophylaxis, despite a program that used village health helpers to encourage its use. Only 25 percent of pregnant women aged 15-29 were taking chemoprophylaxis
(Spencer et al., 1987). The World Health Organization Scientific Group on the Chemotherapy of Malaria (1990:80) has noted that in "well supervised studies … compliance [in children or adults] rarely exceeds 90% and generally ranges from 30% to 60%."
Heymann et al. (1990) addressed the issues of chloroquine efficacy and compliance in a study in Malawi. The program provided women at a prenatal clinic with a one-month supply of chloroquine. They estimated that chloroquine reduced the incidence of Plasmodium falciparum infection by only 23 percent among the 36 percent of pregnant women who complied. Therefore, the program prevented only about 8 percent of cases of infection among pregnant women.
It may be difficult to design studies that measure the effect of chemoprophylaxis on child survival. Because it has been determined that chemoprophylaxis increases birthweight, it may not be possible to withhold it for research purposes. Therefore, it might be necessary to rely on naturally occurring control areas or on evidence of changes in the level or seasonal pattern of infant mortality associated with increased prophylaxis. On the other hand, studies that directly address the question of child survival would have to overcome the problems of recording birthweights and gestational ages, both of which are very difficult to collect in Africa.
PROGRAMS BASED ON VECTOR CONTROL
Before the harmful effects of DDT and other residual insecticides were fully appreciated, considerable progress was achieved in the reduction of malaria mortality and morbidity through spraying. In some areas, mostly in cities and towns, these programs continue and are still effective in controlling the population of mosquitoes and malaria. More recently, greater stress has been laid on the use of personal protection against mosquito bites, including wearing long clothes, using mosquito coils, using ointments containing insecticide, and sleeping in mosquito nets (Rozendaal, 1989). None of these protective measures are part of a national strategy to control malaria, but more recently, the introduction of bed nets and curtains dipped in insecticide (permethrin is the most common) has been adopted as a community-based intervention against malaria in both adults and children. The experimental work on which these strategies are based took place in 1988-1990 in central Gambia, where Alonso and Greenwood showed that mortality in the test villages among children ages 1-4 was 37 percent below the rate in the control villages (Alonso et al., 1991). The trial also demonstrated that much of the decrease in mortality was due to the reduction of deaths identifiable as due to malaria by the verbal autopsy process (see Alonso et al., 1991; Greenwood and Pickering, 1993, for details).
The large reductions in malaria morbidity and mortality reported from
the Gambian trial are unlikely to be repeated in national programs for various reasons associated with the capricious nature of the disease in relation to climatic and other ecological conditions, and to the difference between the effects anticipated in an experiment compared with those expected from a national program. Nonetheless, the use of treated bed nets seems worthy of further studies in other environments. One feature of the trial of impregnated bed nets is the larger than expected reduction in overall mortality. There are enormous problems in identifying a death due to malaria, but those aside, there seems to be some evidence in the changing cause-of-death distributions that other causes of death have also declined as a result of the reduction of malaria morbidity and mortality (see Alonso et al., 1991; Greenwood and Pickering, 1993, for a fuller discussion).
Several large trials of the effects of treated bed nets on malaria, childhood mortality and morbidity, and the birthweights of firstborn are in progress under the supervision of the World Health Organization (WHO). Apart from the problem of introducing bed nets into areas where they are uncommon, the principal obstacle to further use of the treated bed nets is the high recurring cost of the insecticide. Nonetheless, the evidence from the first year of the Gambian national intervention is very encouraging. There are measurable effects on the mosquito population, on the incidence of malaria illness, on childhood mortality, and on the birthweights of firstborn children (Cham and D'Alessandro, personal communication, 1992). Results from other national studies will soon be forthcoming.
SUMMARY
Malaria is a major cause of death and morbidity in Africa. There is substantial variation in the importance of malaria among various regions of sub-Saharan Africa, but in many populations it is the third or fourth most common cause of death. Studies in several areas have demonstrated that infant and child mortality could be reduced substantially if malaria were eliminated or greatly reduced. However, the design of antimalarial programs is complicated by the diversity of ecologies, the spread of chloroquine-resistant strains, and the high costs and managerial complexity of many of the available technologies.
Given the careful examination of strategies for malaria control by the World Health Organization (1984, 1990), the Institute of Medicine (Oakes et al., 1991), and the American Association for the Advancement of Science (1991), this report has not attempted a complete review of the evidence of the effectiveness of all approaches to reducing mortality to malaria. Rather, it has focused principally on three topics: use of village health workers to increase presumptive treatment of fevers, home-based presumptive treatment of fevers, and chemoprophylaxis during pregnancy.
Neither of the two major studies of the use of village health workers to increase presumptive treatment documented a reduction in child mortality. In both cases the programs failed to achieve an adequate increase in the proportion of cases treated. Therefore, we cannot conclude that an increase in presumptive treatment would not reduce child mortality.
These studies raise serious questions about the use of village health workers to increase presumptive treatment of fevers. We have not attempted a complete review of studies of coverage rates and compliance in programs of this sort. However, given the existing high rates of home-based use in many areas, the problems of managing and supplying large numbers of village health workers, the increasing prevalence of chloroquine resistance, and the lack of evidence of mortality reduction, it is not certain that programs based on village health workers can reduce child mortality by encouraging presumptive treatment.
It is still important for health clinics to provide presumptive treatment of fevers in areas and seasons during which malaria is a major cause of illness. The Institute of Medicine (IOM) identified this task as its first priority for malaria control (Oakes et al., 1991:16). In some areas where village health workers provide other services, adding presumptive treatment to their portfolios may be useful. The choice of appropriate drugs and treatment strategies must be worked out in each area, based on the prevalence of chloroquine resistance, the availability and affordability of alternatives, and the likelihood that patients will return to health clinics for further treatment if chloroquine fails.
It is well known that home-based treatment of fevers with chloroquine is very common in sub-Saharan Africa. However, there has been little research on self-treatment. Given the high frequency of this practice documented in numerous areas, there is a need for more studies of the drugs and dosages used, the promptness of self-treatment, and the ability of mothers to determine when it is important to take their children to a health center.
The paucity of data on self-treatment and the frequent emphasis on prevention rather than treatment have led most researchers to understate the potential importance of health education programs designed to encourage, discourage, or improve self-treatment. Efforts to increase the proper treatment of presumed cases of fever usually have been limited to treatment at health centers or by village health workers.
If self-treatment is found to be common and reasonably effective, then health education programs might focus on improving methods of recognizing symptoms of fevers, increasing knowledge of symptoms that require prompt modern treatment, and increasing awareness of the need for prompt treatment with appropriate dosages. If self-treatment is found to involve improper doses, to be used in inappropriate cases, or to delay or prevent seeking modern medical care in severe cases, then health education might
discourage self-treatment and encourage prompt treatment at modern medical facilities. In either case, self-treatment is so prevalent that it cannot be ignored either as a potential opportunity to improve prompt presumptive treatment or as a hindrance to coverage of superior sources of treatment. In many populations, education programs designed to improve home-based presumptive treatment may be more cost-effective than programs based on village health workers. The potential effectiveness of self-treatment will also depend on the efficacy of chloroquine and the costs and perceived safety of alternative drugs that might be used for self-treatment.
Research on the effect of malaria control activities must involve monitoring of self-treatment and treatment at dispensaries. It is not adequate to consider an area as a pure "control" without consideration of existing treatment practices. For example, the Saradidi project in Kenya found that the main effect of the use of village health workers for treating presumptive cases of malaria was a change in the source of chloroquine. Similarly, the use of village health workers in The Gambia led to 57 percent less use of drugs from the dispensaries in the program area compared to the control, and only a 24 percent higher overall rate of treatment. Few of the large-scale studies of methods for preventing or treating malaria provide sufficient information about the baseline or control levels of prophylaxis or treatment.
The World Health Organization Scientific Group on the Chemotherapy of Malaria (1990) recommends chemoprophylaxis for pregnant women. However, the IOM committee and WHO Scientific Group on the Chemotherapy of Malaria both concluded that there is little evidence that prevention or reduction of malaria in pregnant women improves the prognosis for infants (World Health Organization Scientific Group on the Chemotherapy of Malaria 1990:85; Oakes et al., 1991:64-54, 234). There is strong evidence that chemoprophylaxis can increase mean birthweights among first births, but it is not clear to what extent this increase translates into higher child survival rates. No studies have examined the effect of chemoprophylaxis during pregnancy on the infant mortality rate, and there is little information about the effect on perinatal or neonatal mortality. In addition, there is little evidence from large-scale health programs. In these programs the effect of chemoprophylaxis is probably quite small, given that compliance is often low, not all women seek prenatal care early in their pregnancy, and the efficacy of chloroquine (the most commonly used drug) is declining in many areas.
ACUTE RESPIRATORY INFECTIONS
Acute respiratory infections (ARIs) are a group of upper and lower respiratory tract illnesses caused by bacterial, viral, or fungal infections. Of these infections, acute lower respiratory infections (ALRI), predominantly pneumonia, are the most serious and are major causes of mortality in developing countries among children under 5 years of age.
Studies in a number of developing countries, including The Gambia, Zaire, Nigeria, and Kenya, have indicated that serious and potentially fatal cases of pneumonia are predominantly due to two bacterial organisms Streptococcus pneumoniae and Hemophilus influenzae. This recognition and the success in individual cases of treatment with antibiotics have led to the predominance of a case management strategy for ARI control. This strategy is based on an algorithm that uses primarily respiratory rate and recognition of chest indrawing as a basis for diagnosis of pneumonia in children with cough, and on the appropriate treatment of such an illness with antibiotics (Programme for Control of Acute Respiratory Infections, 1990).
EPIDEMIOLOGY
The magnitude of the problem of acute respiratory infections in sub-Saharan Africa was reviewed recently by Kirkwood (1991), who summarized 42 studies from 21 countries (approximately half of the countries in this subregion). Whereas a number of studies reported on the high rates of all respiratory infections, few studies provided information on acute lower respiratory infections or pneumonia. A study in Kenya using both home and clinic surveillance found an incidence rate for ALRIs of 21 per 100 child-years (Selwyn, 1990). This rate is consistent with those found in other developing country settings, where the peak incidences appear to occur in the youngest children (Kirkwood, 1991).
In developing countries, pneumonia is thought to be one of the two most common causes of death in childhood. As summarized by Kirkwood (1991), studies that used an appropriate methodology to determine the cause-of-death structure among children under age 5 found that approximately 7.5 percent of these were due to pneumonia. Angola and Guinea-Bissau had age-specific mortality information available (Kirkwood, 1991). In these countries, the proportionate mortality from pneumonia was highest in children 1-4 years of age (15.2 percent in Angola and 8.9 percent in Guinea-Bissau). However, a larger number of deaths due to ARI occurred among infants because the infant mortality rates were substantially higher than the rates of children aged 1-4 years. The estimated mortality rates due to ARI globally are 10 to 30 deaths per 1,000 live births in infancy and 1.6 to 4.0 deaths per 1,000 children 1-4 years old (Foster, 1985).
There are a number of host and environmental risk factors for pneumonia in children. These include low birthweight, protein-energy malnutrition, lack of breastfeeding in young children, and possibly vitamin A deficiency. They also include exposure to air pollution, especially that caused by biomass fuel combustion in households. All of these factors would appear to be present in much of the sub-Saharan African population. Although it is not known to be a risk factor for pneumonia per se, malaria may complicate the diagnosis of pneumonia and the management of sick children.
A review of the sub-Saharan African DHS indicates that the incidence of ARI symptoms is greater among children living in rural areas than among those children living in urban areas. Little difference was observed in the incidence of ARI based on the mother's educational status.
INTERVENTIONS
A number of intervention trials have been initiated to test the effectiveness and feasibility of reducing pneumonia mortality through population-based case-management programs, which previously had not been attempted on a large scale. To date, results from seven intervention studies from around the world have been published and provide evidence for mortality reduction (Mtango and Neuvians, 1986; Datta et al., 1987; Pandey et al., 1989, 1991; Bang et al., 1990; Khan et al., 1990; Fauveau et al., 1992). A recent meta-analysis of the published case-management intervention trials provides a conservative estimate of an overall reduction of infant mortality by 15.9 deaths per 1,000 births and a cumulative under-5 mortality rate reduction of 36 deaths per 1,000 children (Sazawal and Black, 1992). These estimates would be consistent with a 20 percent reduction in infant mortality and a 25 percent reduction in all under-5 mortality for the studies analyzed.
The only one of these intervention trials in sub-Saharan Africa was in the Bagamoyo District of Tanzania (Mtango and Neuvians, 1986). In this study, episodes of pneumonia were sought by household visiting every six to eight weeks. In addition, women were taught about the need for seeking care if the child had certain signs and symptoms. All detected cases of pneumonia were treated with oral co-trimoxazole, and severe cases were referred to higher-level care. The difference in the mortality rate under age 5, 5m0, was 7.7 deaths per 1,000 children (32.5 deaths per 1,000 children in the intervention area compared to 40.1 in the control area; 95 percent C.I. for difference was 2.0-13.5 deaths per 1,000 children). Thus, the probability of dying by age 5, 5q0, was lower by 38.5 per 1,000 births, consistent with the meta-analysis of the other studies. The pneumonia-specific mortality rates declined by 30 percent over the two-year intervention period.
National efforts to implement the ARI case-management strategy have begun only in the last several years. As an indicator of performance, these programs use the proportion of pneumonia episodes needing antibiotics that actually receive them. In surveys, this indicator may be approximated by the proportion of recent cases of cough with rapid or difficult breathing that received antibiotics. Data from a few surveys conducted in sub-Saharan Africa are available on the current status of programs.
The data suggest a fairly consistent level of respiratory difficulties. In the Zimbabwe DHS, 7.6 percent of children 1-59 months of age had an episode of cough with rapid or difficult breathing in the four weeks preceding the survey (Boerma et al., 1991). In the Nigeria DHS, 6.7 percent reported to have had these symptoms sometime during the previous two weeks (Nigerian Federal Office of Statistics and Institute for Resource Development, 1992). In Mali and Togo, a question was asked about breathing problems of the children in the preceding two weeks (Boerma et al., 1991). The percentages of children with such a problem were 6.5 and 9.3, respectively.
In spite of these high levels, only a relatively small proportion receive medical attention in many countries. Of the children with respiratory difficulties in Mali, only 5.9 percent were taken to a medical facility, whereas in Togo, 33.2 percent were. On the other hand, in Kenya, 65 percent of children with respiratory complaints were taken to a medical facility. The proportion of children in these three countries treated appropriately with antibiotics could not be determined reliably from these surveys.
In Nigeria, mothers reported that 35 percent of these children with cough and rapid breathing were taken to a health facility or provider, 23 percent were given an antibiotic pill or syrup, and 23 percent received an unidentified injection (Nigerian Federal Office of Statistics and Institute for Resource Development, 1992). However, certain groups, such as children in rural areas and in families with lower levels of maternal education, were less likely to be taken to a medical facility. Thus, it is likely that the reduction in mortality will be proportionately lower in these groups than in other groups.
Even without an intensive ARI control program, existing medical services may be having some effect on reducing mortality from pneumonia in children. Because the proportion of cases of ARI receiving medical attention varies so widely among sub-Saharan African countries (6 to 65 percent of such episodes in the four countries mentioned above), it is impossible to estimate the mortality effect of such care-seeking. It is also likely that the diagnosis and treatment of pneumonia by health providers is suboptimal because of limitations in the availability of trained personnel and antibiotics. Given the successful demonstration of the ARI case-management strategy, which emphasizes early detection of pneumonia cases and appropriate
antibiotic treatment, it is likely that such programs could have a much greater effect on child mortality than they do now. However, most sub-Saharan African countries have not yet developed ARI control programs, and those countries with programs have just begun their implementation.
SUMMARY
Acute respiratory infections, especially pneumonia, are among the leading causes of death of children in sub-Saharan Africa. The incidence rate in Africa is about 21 per 100 child-years, with the highest incidence observed among the youngest children in households. Most cases of ARI are attributable to two bacteria and the recommended case management is based on antibiotic therapy. Many countries have begun national strategies for combating ARI in recent years. However, there have been few large-scale studies of this approach. A meta-analysis of case-management intervention trials estimated a reduction of infant mortality rate of 15.9 per 1,000 and an under-5 mortality rate reduction of 36 per 1,000. The proportion of children displaying symptoms of ARI who receive medical attention varies by country (from 6 to 65 percent in four DHS in sub-Saharan Africa), and we have little information on current levels of treatment with antibiotics even among those treated at a health clinic. However, given what is known about current levels of antibiotic treatment for ARI, health programs in sub-Saharan Africa probably are not having much effect on overall mortality rates.