Assessment of the SBIR and STTR Programs at the National Institutes of Health (2022)
Chapter: 5 Impact of the NIH SBIR/STTR Programs
5
Impact of the NIH SBIR/STTR Programs
This chapter examines the observable impact of the National Institutes of Health (NIH) Small Business Innovation Research (SBIR)/Small Business Technology Transfer (STTR) programs based on key metrics of innovation and commercialization, including publications, patents, clinical trials, drugs, medical devices, and follow-on funding from venture capitalists. NIH SBIR/STTR–funded firms have produced a number of clinically significant drugs and devices. Although it is difficult to prove that SBIR/STTR funding affected the ability of these firms to develop and produce these important drugs and devices, the awardee firms have had better commercialization outcomes relative to firms that did not receive this funding.
The analyses in this chapter rely on a variety of sources: data on Food and Drug Administration (FDA)–approved drugs, data on devices from the FDA’s Applications for Premarket Approval (PMAs) for Class III devices, data on devices that are equivalent to currently marketed devices from the FDA’s premarket application clearance (510[k]’s), data on clinical studies from ClinicalTrials.gov, data on granted patents from the U.S. Patent and Trademark Office’s (USPTO’s) PatentsView database, data on trademarks from USPTO’s trademark case files, data on venture funding from Crunchbase, data on publications from the National Library of Medicine’s PubMed database, and data from the Startup Cartography Project (SCP) Entrepreneurial Quality Index. In addition, the committee relied on information provided by NIH on all SBIR/STTR applicants from 1995 to 2019 and used publicly available data in the NIH RePORTER database. For more information on these data sources, see Annex 5-1 at the end of this chapter.
This chapter first describes various commercialization outcomes associated with NIH SBIR/STTR awardee firms. It then describes the committee’s attempt to assess whether the firms’ outcomes can be causally linked to the SBIR/STTR funding they received. Next, because NIH institutes and centers (ICs) may be selecting a portfolio of projects with an eye to diversifying risks, increasing the breadth of investments, or achieving other program-level goals, the
chapter turns to an analysis of the impact of SBIR/STTR funding on outcomes from SBIR/STTR funding at the IC level. Finally, the chapter considers what information can be gleaned from these analyses concerning broader public health care impacts.
INNOVATION AND COMMERCIALIZATION OUTCOMES
One of the challenges of assessing commercialization, not just with regard to the SBIR/STTR programs at NIH or elsewhere, is the difficulty of systematically observing links between federally funded research and development (R&D) and any commercialization outcomes. There are occasionally cases in which a technical breakthrough can be traced to a specific product sold on commercial markets; for example, Alexza is an NIH SBIR awardee whose award outcome included the development of Adasuve, an inhaled medication for rapid treatment of agitation associated with schizophrenia or bipolar disorder.1 However, being able to trace an innovation from grant to marketed product is very difficult. For most innovations, the receipt of an SBIR/STTR award is likely to be but one element of a broader innovation and commercialization process that involves the need for additional private-sector capital and takes a long time to be reflected in firm sales and growth. Even in the Adasuve example, the SBIR grants were awarded in 2002–2006, while the drug did not receive FDA approval until 2012.
As discussed in Chapter 2, measuring the impact of federal investments, especially those for R&D, is difficult for a number of reasons: there are long lags between research and ultimate impact; benefits are widely diffused across firms and industries, not just those that received the funding; and other spillovers are difficult to measure. For example, knowledge gained from an SBIR or STTR project can be applied to other work carried out by the firm, or a principal investigator (PI) may leave the firm and carry knowledge gained to a new firm or industry. Also take, for example, the development of a new drug or vaccine. Revenue from the sales of the drug demonstrate only the benefits to the firm, not the societal benefit of lowering the incidence of the disease in the general population or even the quality-of-life improvements realized by the people who take the drug or vaccine.
Measuring Outcomes: Marketed Drugs, Devices, and Trademarks
Despite the above difficulties, the committee attempted to measure the impact of SBIR and STTR awards on biotech and medtech innovations in the marketplace and found that a number of clinically valuable drugs and devices have been introduced by SBIR/STTR-funded firms. The committee matched SBIR and STTR grantee names with new molecular entities (NMEs) to track
___________________
1 Alexza cited its NIH SBIR Phase II award from the National Institute of Neurological Disorders and Stroke in the government-interest section of one of the patent applications for Adasuve.
small-molecule drugs, biologics license applications (BLAs) for biologic drugs, PMAs for Class III medical devices, premarket notifications for devices that do not require premarket approval (510[k]’s), and trademarks granted by USPTO. This list does not represent a comprehensive picture of biomedical innovations, nor does this approach fully capture the impacts of NIH SBIR/STTR awards. For instance, it excludes digital health products not requiring FDA approval unless they were trademarked.
A list of all drugs approved from 1996 to 2020 that are associated with NIH SBIR or STTR awardees is included in Annex Table 5-2.1.2 The data show that a number of NIH SBIR/STTR awardees have introduced medicines that have had a profound impact on health and associated sales in the hundreds of millions of dollars. Annex Table 5-2.1 includes 99 drugs (NMEs and BLAs), representing more than 12 percent of the total number of such drugs approved in the same 1996–2020 time period (11 percent of NMEs and 15 percent of BLAs).3 About 16 percent of “priority review” drugs approved over this period—those representing significant health advances over available treatments—emanated from SBIR/STTR grantees.4 It is difficult to establish the role played by the SBIR/STTR grant in supporting these firms or enabling market introduction of the drugs. The list of drugs associated with SBIR/STTR awardees may, on the one hand, overestimate the impact of the awards on marketed drugs (since a drug may have been developed anyhow or be unrelated to the grant). However, this table includes important drugs that appear to be topically connected to an NIH SBIR or STTR grant. At the same time, the list underestimates the award’s impact on grantees whose name later changed, as well as impacts due to knowledge spillovers to other firms.5
The SBIR/STTR awardees that have introduced medical devices into the marketplace show a similar pattern. Matching of medical devices with SBIR/STTR grantees through the FDA PMA and 510(k) lists revealed 34 linked PMAs and 2,475 linked 510(k)’s. Annex Tables 5-2.2 and 5-2.3, respectively, contain a random sample of companies associated with SBIR/STTR awards that, based on these two lists, introduced medical devices into the marketplace. As with drug approvals, although it is difficult to tie SBIR/STTR grantees to the specific devices included in these tables, there are a number of cases in which there appears to be a direct relationship between the grant and the final product. For example, Abiomed received NIH Phase I and II awards for an implantable partial left ventricular assist device (LVAD) and its Impella heart pumps support more
___________________
2 Annex Tables 5-2.1 to 5-2.4 are included in Annex 5-2 at the end of this chapter.
3 Drugs@FDA: FDA-Approved Drugs, available at https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=reportsSearch.process.
4 These SBIR/STTR-associated drugs also account for 18 percent of orphan drugs. Drugs@FDA: FDA-Approved Drugs.
5 Additionally, Annex Table 5-2.1 does not include non-NME new drug approvals; thus, it does not include new dosage forms and other line extensions associated with SBIR/STTR-funded firms, such as Adasuve and Vivitrol.
than 170,000 patients today.6 And Candela Corporation’s GentleLase laser, with more than $100 million in annual revenue, is related to its SBIR Phase I and II awards for pulsed laser treatment of pigmented lesions.7
In addition to drugs and devices, 8,974 trademarks are registered to SBIR/STTR-awardee firms. Trademarks are associated with specific products and represent one form of intellectual property protection. Some trademarked companies are highlighted as SBIR/STTR success stories. A notable example, 23andMe, which received six SBIR Phase I awards and two SBIR Phase II awards between 2010 and 2017, provides genetic health assessment and ancestry information and was valued at approximately $3.5 billion in 2021 (Brown, 2021).8 A random sample of SBIR/STTR-awardee firms with trademarks is shown in Annex Table 5-2.4. This sampling of trademarks shows a wide variety of trademarked products, from digital health products, to medical supplies and instrument parts, to nutritional supplements
Award-Level Outcomes
Although the tables in Annex 5-2 show a large number of commercial products produced by NIH SBIR/STTR awardees, they underestimate the value contributed by SBIR/STTR-awardee firms to the biotech innovation ecosystem. First, the vast majority of drug and vaccine candidates fail to reach FDA approval, although some of these candidates may receive a trademark (Wong et al., 2019). Moreover, looking only at outcomes in the commercial marketplace ignores the broader role of SBIR/STTR-awardee firms on the life sciences innovation system. These firms contribute to the overall knowledge stock; advance the careers of life sciences researchers, who may find new opportunities to commercialize their research; and enable innovations in other firms through knowledge spillovers.
To provide a more complete picture of the impact of NIH SBIR/STTR-awardee firms on early-state biotech and medtech innovation, the committee reviewed three outcomes tracked by NIH in its RePORTER database: publications, patents, and clinical studies citing support from projects.9 Note that the NIH-tracked outcomes are reported at the award level, not the firm level.
The ways in which these data are collected by NIH vary depending on the type of outcome involved. Projects are linked to publications through an NIH tool called the Scientific Publication Information Retrieval and Evaluation System, or SPIRES. This tool integrates information from PubMed, which records information on grants acknowledged in published articles, and biographical information from the National Center for Biotechnology Information, in which
___________________
6https://www.abiomed.com/; https://www.sbir.gov/sbirsearch/detail/803.
7https://www.sbir.gov/sbirsearch/detail/116896.
8https://www.sbir.gov/node/1308525; https://www.sbir.gov/sbc/23andme-inc.
9https://exporter.nih.gov/about.aspx; https://exporter.nih.gov/faq.aspx.
investigators compliant with the NIH open access policy deposit their publications.
Linking of clinical studies to grants relies on data from ClinicalTrials.gov, which includes a field for grant numbers. While the coverage of the ClinicalTrials.gov database and the rules on reporting to it have changed over time,10 trials data, as is the case with publications, rely on an external database rather than on self-reporting by awardees.
In contrast, patent data available in RePORTER are from iEdison, which grantees use to report inventions and patents to agencies so as to comply with the Bayh-Dole Act. NIH is unique among federal agencies in that it makes the patent data from iEdison publicly available. Analyses by the Government Accountability Office (GAO) (1999, 2002) and academics (Rai and Sampat, 2012) have found incomplete compliance by grantees in reporting to iEdison, but most of these analyses have focused on reporting overall, not on SBIR/STTR reporting per se (see also NRC, 2011). Appearing to reflect this gap, the RePORTER database cautions that “not all recipients of NIH funding are compliant with the iEdison reporting requirements, particularly after their NIH support has ended.”11
The committee analyzed the reported publications, patents, and clinical trials of NIH Phase II awardees who received their first Phase II award between 2010 and 2015 and found that 6.5 percent of those awardees reported a patent, 42 percent reported a publication, and 7.4 percent reported a clinical study. To gain perspective on the relative efficacy of SBIR/STTR awards, the committee compared these results with reported outcomes for Research Protect Grant (R01) awards and found that 5 percent of those grants in the same period reported a patent, 97 percent reported a publication, and 8 percent reported a clinical study.12 After controlling for differential effects across science areas and time, the committee found no statistical difference in the number of patents or clinical studies per dollar spent on SBIR/STTR versus R01 grants, but did find a substantial difference in publication records between the two programs. Not surprisingly, R01s generate many more publications overall, and nearly all of these awards result in at least one publication.
Given the commercial focus of the SBIR/STTR programs, it is surprising to see no statistical difference in patent or clinical study outcomes between R01 and SBIR/STTR grants. But there is reason to believe that these data do not reflect the full extent of these outcomes for the latter grants. As discussed in Chapter 4, SBIR/STTR awardee firms are much less likely to report patents back to NIH compared with R01 grantees. As noted in Chapter 4, all patents with government-interest statements in the USPTO database acknowledging NIH funding should also appear in the RePORTER database under that project, but only 30 percent of
___________________
10 See https://grants.nih.gov/policy/clinical-trials/reporting/index.htm; see also Ross and colleagues (2012).
11https://exporter.nih.gov/faq.aspx.
12 The committee also analyzes these outcomes on a firm-level basis later in this chapter.
SBIR/STTR awards reported in the USPTO database are reported back to NIH, compared with 64 percent of other NIH grants (mostly R01s). Thus, looking only at the patents identified in RePORTER grossly underestimates the number of patents produced by SBIR/STTR awardees.13 In fact, only one SBIR-funded patent listed in the RePORTER database—Genzyme’s CERDELGA (eliglustat), which was approved in 2014 for the treatment of Gaucher disease—can be linked to a marketed drug listed in the FDA’s Orange Book. Additionally, as discussed below, the apparent lack of clinical studies among SBIR/STTR-supported firms in some ICs may be due to the fact that not all ICs allow SBIR/STTR funding for clinical trials.
Even without correcting for the underreporting of patents for SBIR/STTR awardees, just the similarity of early-stage innovations in the biotech and medtech innovation product cycle between R01 and SBIR/STTR grants provides compelling evidence of the value of the SBIR/STTR programs in this innovation ecosystem. A body of evidence developed over the past two decades documents the significant financial and public health impact of NIH funding, the bulk of which is associated with R01 grants (Azoulay et al., 2019; Blume-Kohout, 2012; Cutler and Kadiyala, 2003; Manton et al., 2009; Toole, 2007). In an influential study, Azoulay and colleagues (2019) show that a $10 million increase in NIH funding (the vast bulk of which consists of R01 grants) spurs the development of 2.7 private-sector patents with an associated present discounted value of $23–187 million.
Differences across ICs
While the award-level analyses in the previous section suggest that publications are a more common reported outcome of SBIR/STTR awards relative to patents or clinical trials overall, breaking these data down by IC reveals interesting variation, reflecting the different foci of the ICs and the types of outputs produced by their SBIR/STTR awardees. Figure 5-1 shows a breakdown of the share of all NIH SBIR/STTR grants associated with reported patents and clinical trials for each of the 20 ICs with the largest SBIR/STTR programs.
Some IC-funded SBIR/STTR projects, including those funded by the National Institute on Minority Health and Health Disparities (NIMHD), the National Institute on Drug Abuse (NIDA), the National Institute on Alcohol Abuse and Alcoholism (NIAAA), and the National Institute of Mental Health (NIMH), are more likely to produce trials than patents. The opposite is true, however, at most ICs, and some, such as the National Institute of Biomedical Imaging and Bioengineering (NIBIB), are much more likely to be linked to patents than to trials. This variation can be explained in part by the fact, noted above, that some ICs do not allow use of SBIR/STTR funds for clinical trials and in part by the nature of the technologies being advanced by the ICs. Although not
___________________
13 See the section on “missing patent data” in Chapter 4 of this report.
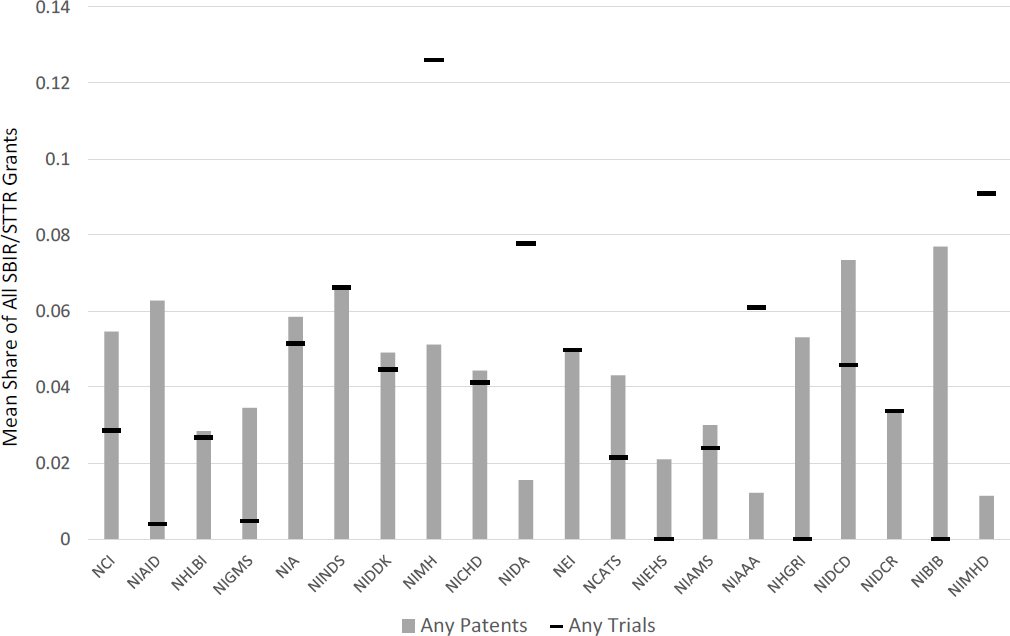
SOURCE: Committee calculations based on data in NIH RePORTER.
presented in Figure 5-1, there is also a disparity in SBIR/STTR awardees’ propensity to publish, ranging from 18 percent of grants for NIMHD to 44 percent of grants for the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), with most ICs being in the 30–40 percent range. These differences have implications for evaluation going forward: the most appropriate outcome metrics may vary by IC and take account of differing IC objectives.
This heterogeneity can also be seen in the technical focus of patents, based on patent classes from the World Intellectual Property Organization (WIPO). Table 5-1 shows the top two patent classes for each IC with 20 or more patents reported in the NIH database. While these patenting data show some IC focus on pharmaceuticals, other ICs patent in other fields. Only five ICs (National Cancer Institute [NCI], National Institute of Allergy and Infectious Diseases [NIAID], National Institute on Aging [NIA], NIMH, and National Institute of Dental and Craniofacial Research [NIDCR]) have pharmaceuticals as the main technology field in patents reported by SBIR/STTR-awardees. For other ICs (National Heart, Lung, and Blood Institute [NHLBI]; National Institute of Neurological Disorders and Stroke [NINDS]; National Institute of Diabetes and Digestive and Kidney Diseases [NIDDK]; National Institute of Child Health and Human Development [NICHD]; NIDA; National Eye Institute [NEI]; NIAMS; and National Institute on Deafness and Other Communication Disorders [NIDCD]), the largest shares of patents among their awardees are in the patent class of medical technology, while for other ICs (National Institute of General Medical Sciences [NIGMS], National Human Genome Research Institute [NHGRI]) the largest shares are in the patent class of biotechnology. For NIBIB, patents are equally likely to be in electrical machinery, apparatus, energy, or medical technology. More than half of the environmental science patents are measurement related.
Similar heterogeneity can be seen in trademark data, which show that SBIR/STTR-funded firms have registered trademarks in a wide variety of classes, although electrical and scientific apparatus represents the largest share (23 percent), and chemicals and pharmaceuticals combined account for another 43 percent of trademarks. Services—computer, medical, and advertising and business—are also trademarked by these firms, along with environmental control apparatus, cosmetics, and education. Much of the previous work on NIH has focused on links to pharmaceuticals (Azoulay et al., 2019; Sampat and Lichtenberg, 2011; Toole, 2007), but at least for SBIR/STTR funding, a focus on drugs, especially small-molecule pharmaceuticals, will miss a considerable portion of the outcome activity. Accordingly, a broader suite of outcome measures is needed when looking at health care products linked to SBIR/STTR-funded firms.
Measuring the Causal Impact of SBIR/STTR Awards
The firm-level and award-level data presented in the previous sections provide information only about outcomes linked to SBIR/STTR awards or to the
TABLE 5-1 Patent Data for NIH SBIR/STTR Awards, by Awarding Institute/Center (IC)
| NIH IC | Acronym | Top Two WIPO Patent Classes (share of patents) | Total Number of Patents |
|---|---|---|---|
| National Cancer Institute | NCI |
Pharmaceuticals (.35) Biotechnology (.21) |
332 |
| National Institute of Allergy and Infectious Diseases | NIAID |
Pharmaceuticals (.58) Organic fine chemistry (.14) |
228 |
| National Heart, Lung, and Blood Institute | NHLBI |
Medical technology (.37) Pharmaceuticals (.26) |
148 |
| National Institute of General Medical Sciences | NIGMS |
Biotechnology (.31) Measurement (.16) |
208 |
| National Institute on Aging | NIA |
Pharmaceuticals (.36) Medical technology (.27) |
56 |
| National Institute of Neurological Disorders and Stroke | NINDS |
Medical technology (.47) Pharmaceuticals (.16) |
98 |
| National Institute of Diabetes and Digestive and Kidney Diseases | NIDDK |
Medical technology (.31) Pharmaceuticals (.27) |
124 |
| National Institute of Mental Health | NIMH |
Pharmaceuticals (.39) Computer technology (.14) |
29 |
| National Institute of Child Health and Human Development | NICHD |
Medical technology (.36) Pharmaceuticals (.26) |
69 |
| National Institute on Drug Abuse | NIDA |
Medical technology (.5) Pharmaceuticals (.3) |
20 |
| NIH IC | Acronym | Top Two WIPO Patent Classes (share of patents) | Total Number of Patents |
|---|---|---|---|
| National Eye Institute | NEI | Medical technology (.3) Pharmaceuticals (.26) | 46 |
| National Institute of Environmental Health Sciences | NIEHS | Measurement (.53) Analysis of biological materials (.18) | 20 |
| National Institute of Arthritis and Musculoskeletal and Skin Diseases | NIAMS | Medical technology (.45) Pharmaceuticals (.34) | 62 |
| National Human Genome Research Institute | NHGRI | Biotechnology (.71) Basic materials chemistry (.12) | 23 |
| National Institute on Deafness and Other Communication Disorders | NIDCD | Medical technology (.44) Audio-visual technology (.15) | 28 |
| National Institute of Dental and Craniofacial Research | NIDCR | Pharmaceuticals (.48) Medical technology (.26) | 31 |
| National Institute of Biomedical Imaging and Bioengineering | NIBIB | Electrical machinery, apparatus, energy (.29) Medical technology (.29) | 23 |
NOTES: The table includes ICs with 20 or more SBIR/STTR-related patents. WIPO = World Intellectual Property Organization.
SOURCE: Committee calculations based on NIH RePORTER using all years available; WIPO patent classes.
awardee firms, not about whether the grants caused the outcomes—that is, whether absent the grants, the linked patents, publications, trials, and drugs would not exist. Assessing causal impacts is notoriously difficult because it requires a careful characterization of counterfactuals: What would have happened if the programs had not been implemented?
The gold standard for causal estimation is the randomized controlled trial, in which otherwise identical participants are randomized between treatment and control groups and outcomes are compared across the two groups. When such an approach is infeasible, as is the case when studying the SBIR/STTR programs, quasi-experimental approaches are used to create comparisons that simulate randomization. In the present case, the committee compared applicants who look observationally similar but differ in their SBIR/STTR funding success.
Absent active randomization, the most informative study design would rely on the priority scores of each application. As part of the standard NIH review protocol, each proposal submitted to the program is evaluated by an expert review panel and assigned a priority score that reflects project quality (see Chapter 3). For some ICs, proposals are then ranked and generally funded in order of priority scores until financial resources have been exhausted. Because proposals just above and just below the payline threshold (the cutoff point for scores below which applications generally are not funded) are very similar, one can compare the outcomes of these two groups to enable credible causal estimates. Previous analyses of NIH programs (Azoulay et al., 2019; Jacob and Lefgren, 2011; Li and Agha, 2015) and the SBIR/STTR program of other agencies (Howell, 2017) have used priority score–type information in regression discontinuity designs to compare “just funded” to “just not funded” applicants, and provide estimates of the program effects. In addition, a previous National Academies report assessing the Advanced Research Projects Agency-Energy (ARPA-E) program used individual reviewer scores to evaluate that program’s funding selection processes (NASEM, 2017).
Although the committee requested priority score information from NIH, this information was not provided because of confidentiality concerns. If future analyses are to be more robust and enable stronger statements on program impact, NIH will need to find a way to provide this information to researchers, as it (Ginther et al, 2011; Jacob and Lefgren 2011; Li and Agha, 2015) and other agencies (Howell, 2017; NASEM, 2017) have done in the past. The scores can be useful for program evaluation even if, as described in Chapter 3, they are not used uniformly by ICs or there are deviations from score-based funding.
Because the committee did not have access to priority scores, the analysis that follows takes an alternative approach by exploiting another feature of the peer review process at NIH. NIH provided data on which applications were discussed and of these, which were funded, for all applications between 1995 and 2019. In the review process, all of the submitted proposals are given a preliminary score, and review panels limit their discussions to the most promising proposals. Proposals that were discussed but ultimately not funded are presumed to be closer in quality to funded proposals than unfunded projects that were not discussed.
Accordingly, the causal impacts of funding in this framework can be viewed as a comparison of outcomes for funded proposals/applicants and discussed but not funded proposals/applicants. For the sake of completeness, the committee’s analysis also includes data on those proposals that were neither funded nor discussed.
This analysis is focused at the individual project level, and the committee notes that this approach may miss some important portfolio aspects of the SBIR/STTR programs. ICs may invest in a collection of projects to diversify risks, increase the breadth of investments, and achieve other program-level goals. These types of returns can be properly captured only by an IC-level analysis that exploits variation in funding across years to assess impacts.
Unfortunately, this IC-level approach is not without its own causal inference challenges and fundamentally relies on assumptions about what is driving the funding-level variation. If, for example, NIH increases funding to the SBIR/STTR program of a particular IC because there are more promising opportunities in that IC’s disease area, the additional funding may appear to lead to more discoveries when, in fact, causality runs in the other direction. Fortunately, the funding allocation rules for the SBIR/STTR programs help alleviate this concern. Each IC allocates a fixed percentage of its overall budget to these programs that is determined by Congress, and because that percentage hovers around 4 percent, it appears quite likely that any opportunity-driven changes in the programs’ budgets will be driven by the larger extramural programs that account for the other roughly 96 percent of an IC’s resource consumption. That said, if the scientific opportunities that drive the larger allocation are correlated with opportunities at the SBIR/STTR level, inference challenges may remain. Nonetheless, the committee contends that a straightforward analysis examining the impacts of variation in SBIR/STTR funding at the IC level on a range of innovation outcomes can be regarded as a credible approach to estimating the causal impacts of the two programs. In addition to the outcomes described previously, the analysis here includes receipt of venture capital funding as a metric.
Ex ante Quality of Firms Participating in NIH’s SBIR/STTR Programs
In the context of the constraints described above, the committee began its analysis by first examining the “quality” of NIH SBIR/STTR participants. To measure a firm’s propensity for high growth, the committee drew on data from the Startup Cartography Project (SCP) (Andrews et al., 2020; Guzman and Stern, 2015), which combines comprehensive business registration data with a predictive analytics approach to produce an estimate of the underlying growth potential (or entrepreneurial “quality”) of firms. Specifically, building on Guzman and Stern (2015), Andrews and colleagues (2020) forecast quality for firms by estimating the probability of “growth” (i.e., either an initial public offering [IPO] or a significant acquisition of greater than $10 million) for a firm within 6 years of its founding based on a number of factors observable at or around the time of
founding. The factors found to be predictors of high growth include startup characteristics based on business registration (such as whether the firm is registered in Delaware and whether it is registered as a corporation rather than an LLC or partnership) and other startup characteristics (e.g., firms with longer names and those named after their founder are less likely to be high-growth), as well as intellectual property measures (e.g., whether the firm applies for a patent or trademark within 1 year of its founding.14
Applying these data, the committee found that small businesses that participate in the NIH SBIR/STTR programs are of significantly higher ex ante quality relative to average firms. After controlling for the broad sector in which the startup is likely operating, firms that ever apply to the NIH SBIR/STTR programs are roughly 140 percent more likely to be forecast to achieve a meaningful growth event compared with an average startup in the biotech sector (see column 3 in Table 5-2).15 The results of the committee’s analysis indicate that small businesses that participate in the NIH SBIR/STTR programs, regardless of whether they are ultimately funded, have a higher potential for growth relative to the average small business in the United States, even after accounting for the fact that these firms are concentrated in high-tech sectors.
TABLE 5-2 Mean Differences between NIH SBIR/STTR Applicants and Startup Firms: Overall and in Biotech
| Quality Index | Log(quality index) | ||
|---|---|---|---|
| (1) | (2) | (3) | |
| Ever applies to NIH | 0.00445a | 0.00409a | 1.356a |
| SBIR/STTR | (0.000108) | (0.000106) | (0.0107) |
| Constant | 0.000615a (0.000000638) | 0.000716 a (0.00000109) | −8.058a (0.000371) |
| Sector controls | Sector controls applied | Sector controls applied | |
| Number of observations | 22,946,207 | 22,946,207 | 22,946,207 |
SOURCE: Committee analysis using NIH-provided application information for 2000–2018.
NOTES: Quality index is from the Startup Cartography Project Entrepreneurial Quality Index. Observations are firm-level. Robust standard errors in parentheses.
a p <0.01.
___________________
14 For more detail on the Startup Cartography Project (SCP) Entrepreneurial Quality Index, see Guzman and Stern (2015) and Andrews and colleagues (2020).
15 Firms in the biotechnology cluster in the SCP index were found by searching for words in the firms’ names that are most commonly used in the biotech cluster, as identified in the U.S. Cluster Mapping Project from the U.S. Economic Development Administration.
As shown in Figure 5-2, the SCP quality index indicates that the growth potential (i.e., quality) of first-time applicants16 to NIH’s SBIR or STTR programs has improved over time. In other words, the potential for growth among first-time applicants to these programs has been increasing over time, and the program has increasingly been attracting firms with high growth potential. Moving from 0.01 to 0.1 on the x-axis of Figure 5-2 represents a 10-fold increase in the probability of a major growth event.
In addition to the fact that the NIH SBIR/STTR programs attract applicants with high growth potential, NIH’s review and selection processes tend to favor applicants with such potential. Figure 5-3 shows that first-time funded applicants are of higher quality than applicants whose first proposals are not funded, regardless of whether they are discussed.
Table 5-3 reports summary statistics for eight unique outcomes for firms that received SBIR/STTR awards during fiscal years (FY) 2000–2018. Most outcomes are rare, making it difficult to draw meaningful comparisons, but funded firms tend to have more of these outcomes compared with unfunded firms. For
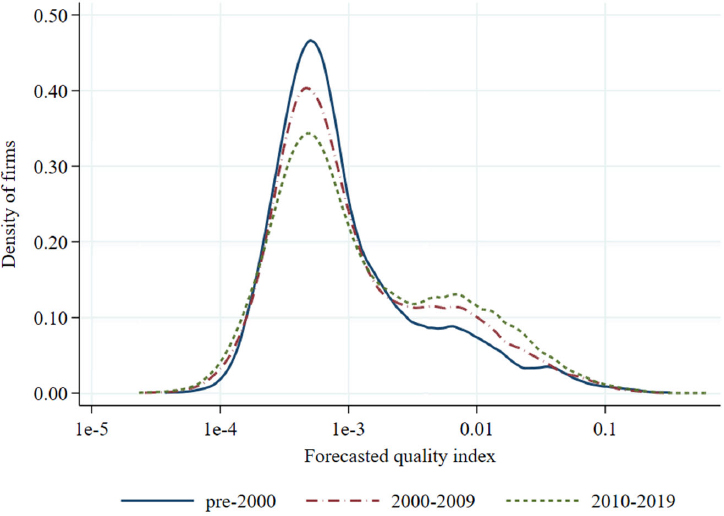
SOURCE: Committee analysis using NIH-provided application information and the Startup Cartography Project Entrepreneurial Quality Index.
___________________
16 First-time applicants are firms that apply to the SBIR/STTR program the first time as identified by their NIH firm ID. This paragraph and related text in Chapter 5 were edited to clarify the definition of first-time applicants after providing a prepublication version of the report to NIH.
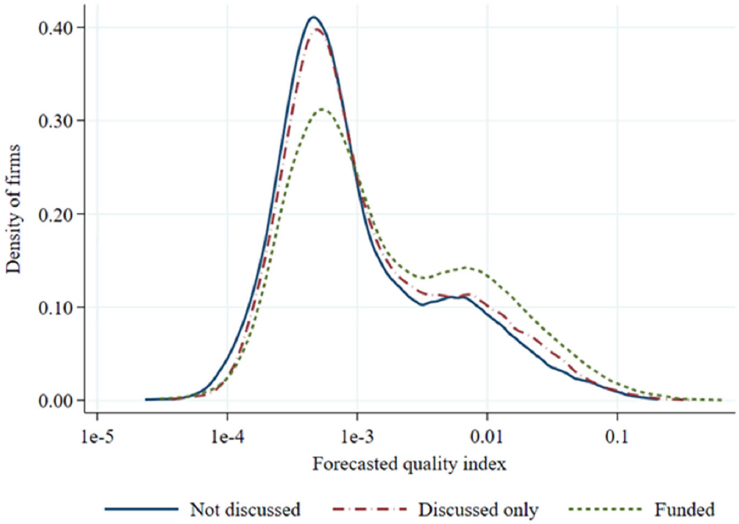
SOURCE: Committee analysis using NIH-provided application information and the Startup Cartography Project Entrepreneurial Quality Index, for applications in fiscal years 2000–2018.
Note: The analysis is restricted to the outcomes of first applications to NIH SBIR/STTR programs.
example, 11 percent of unfunded firms have publications in a given year, compared with 26 percent of funded firms, and the number of annual publications for those firms that produce publications is larger for funded than for unfunded firms. Similarly, 4 percent of unfunded SBIR/STTR applicants have a patent in a given year, compared with 9 percent of funded firms. Funded firms are also more likely to attract venture capital funding (4 percent compared with 2 percent of unfunded firms), and the amount of money raised by funded firms is much higher. These statistics are based on firm-year observations for the 10 years after the firms’ first SBIR/STTR application and are split by whether or not the firms’ first application was funded. Additionally, patents and publications are weighted by the number of authors, meaning that if there are three authors on a given publication or patent and only one author is from the SBIR/STTR-funded small business, the firm is credited with one-third of the publication or patent.
As with the results reported in Annex Tables 5-2.1 to 5-2.4, the analysis in this section relies only on a match between a firm’s name in the SBIR/STTR application list and patents in the USPTO database, in contrast to some of the prior
TABLE 5-3 Firm-year Outcome Summary Statistics for Fiscal Years 2000–2018, NIH SBIR/STTR Applicants, Following First Application Decision
| Outcome | Decision on Firm’s First Application | Number of Observations | Percent with Positive Nonzero Outcomes | Summary Statistics for Nonzero Outcomes | ||
|---|---|---|---|---|---|---|
| Median | Mean | Standard Deviation | ||||
| VC Funding | Unfunded | 136,737 | 2 | $3,500,000 | $11,290,008 | $28,981,228 |
| Funded | 24,811 | 4 | $5,000,000 | $13,679,346 | $22,453,088 | |
| Publication | Unfunded | 136,737 | 11 | 0.58 | 1.55 | 4.95 |
| Funded | 24,811 | 26 | 0.75 | 1.39 | 2.4 | |
| Trademark | Unfunded | 136,737 | 4 | 1 | 2.11 | 2 |
| Funded | 24,811 | 6 | 1 | 2.02 | 1.77 | |
| Patent | Unfunded | 136,737 | 4 | 1 | 2.31 | 4.3 |
| Funded | 24,811 | 9 | 1 | 2.35 | 3.25 | |
| Clinical Trial | Unfunded | 136,737 | 2 | 1 | 1.67 | 1.52 |
| Funded | 24,811 | 3 | 1 | 1.52 | 1.1 | |
| 510(k) | Unfunded | 136,737 | 1 | 1 | 1.52 | 1.37 |
| Funded | 24,811 | 1 | 1 | 1.45 | 0.99 | |
| Device PMA | Unfunded | 136,737 | <1 | 1 | 1 | 0 |
| Funded | 24,811 | <1 | 1 | 1 | 0 | |
| Drug Approval | Unfunded | 136,737 | <1 | 1 | 1 | 0 |
| Funded | 24,811 | <1 | 1 | 1 | 0 | |
NOTES: Based on approximately 3,000 firms with funded first applications and 17,600 firms with unfunded first applications. Observations are at the firm-year level and are based on the 10 years after the first application decision in the data (conditional on data availability and time censoring). “Unfunded” includes discussed but not funded applications. The outcomes are based on the firms’ first application to NIH so do not include resubmissions of the original proposals or subsequent proposals by these firms. The rightmost three columns report statistics for the nonzero distribution. Publication and patent outcomes are share-weighted by authors or assignees, which is why fractional outcomes are possible. Based on applications for fiscal years 2000–2018. PMA = Premarket Approval Application; VC = venture capital.
SOURCES: Committee calculations based on fiscal year 2000–2018 NIH SBIR/STTR application data, Crunchbase, PubMed, U.S. Patent and Trademark Office (USPTO) data on trademarks, Food and Drug Administration (FDA) data on devices and drug approvals.
analyses in this chapter that look at outcomes at a per-SBIR/STTR-award level based on reporting in NIH’s RePORTER database. Additionally, for all the outcome variables, the outcomes are on an annual rather than a cumulative basis. In other words, to take an example from Table 5-3, each year is likely to see 26 percent of funded firms produce a publication.
Importantly, at this point the evidence does not differentiate whether better outcomes for funded firms are due to (1) the funds having a causal effect on the production of outcomes or (2) the fact that the review and funding processes likely select better applicants to fund (as illustrated in Figure 5-3). In most cases, the probability of any outcome is significantly more likely for firms whose first application is funded compared with those whose first application is not. Because the device PMA and drug approval outcomes are so rare, those outcomes are converted in all of the following analyses into binary indicators of whether the firm had any of those outcomes or not.17
In an attempt to determine the extent to which the differences in outcomes in Table 5-3 are due to the causal effect of firms receiving SBIR/STTR funding rather than a tendency for the outreach and selection processes to select high-potential firms, the committee first ran a series of regressions to estimate whether receiving funding had a significant impact on outcomes. After controlling for the SCP estimate of entrepreneurial quality, the committee found that the award of a grant or contract did not yield a statistically significant difference in outcomes. Put another way, focusing only on firms applying for the first time to the NIH SBIR/STTR programs, and after including a measure to control for the growth potential of firms (measured using data from before the application to the SBIR/STTR program), there was no statistically significant difference in outcomes between those firms that received an SBIR/STTR award on their first application and those that applied to the programs but were rejected during that application cycle. As a result, the committee was unable to determine how much of the increase in outcomes in Table 5-3 was due to selection by the NIH SBIR/STTR programs (i.e., funding of higher-quality firms) versus causal effects of the programs (i.e., providing funds that led to outcomes that would not have occurred in the absence of those funds).18
To be clear, these regression findings do not mean that SBIR/STTR awardees did not produce significant innovation outputs. Indeed, as highlighted in Table 5-3, SBIR/STTR awardees did produce significant innovation outputs along a number of dimensions compared with the overall population of SBIR/STTR applicants. One potential explanation for this result is that, given the high selectivity for an award within the NIH SBIR/STTR programs, firms that were of similar quality (but did not receive an award on their first application) were able to attract or obtain resources (e.g., from future NIH SBIR/STTR
___________________
17 For now, the analysis focuses on outcomes before and after a firm’s first NIH SBIR/STTR application because this approach facilitates more direct statistical tests.
18 For more detail on this causal analysis, see Appendix C.
awards, other federal agencies, venture capital, or state-level grant programs) that also allowed them to produce meaningful innovation outputs.
To explore differences among cohorts of applicants, the next group of figures (Figures 5-4 through 5-8) looks at outcomes from Table 5-3 before and after the time of first application to the NIH SBIR/STTR programs. Specifically, this series of figures shows venture capital funding, publications, trademarks, patents, and clinical trials, comparing firms with first applications that were not discussed, firms with first applications that were discussed but not funded, firms with funded applications falling in the bottom 90 percent of support from the programs from 1995 to 2019, and firms with funded applications falling in the top 10 percent of support from the programs during those same years. These are annual rates of outcomes, where the years on the x-axes refer to years relative to a firm’s first SBIR/STTR application.
Several important patterns are illustrated in Figures 5-4 to 5-8. First, there is a clear, monotonic increase in the rate of outcomes depending on how successful the firms’ first applications were. This increase may indicate a causal effect of the SBIR/STTR grants. It is notable that firms whose first application was funded and ultimately received a substantial amount of SBIR/STTR funding (i.e., are in the top 10 percent of lifetime funding from the programs) have significantly higher scores on outcomes as indicated in Figures 5-5 through 5-8. While previous research on the SBIR/STTR programs has suggested that agencies should consider limiting the number of Phase II awards to firms (Rozansky, 2019), the evidence for NIH suggests that more outcomes are associated with multiple awards.
However, a second pattern emerges, showing a difference in outcomes even before the first SBIR/STTR application/award. These differential trends in outcomes prior to the first application indicate that these postapplication outcome differences may be due in part to the SBIR/STTR programs selecting applications to fund based on features of firms and their applications that, in the absence of funding of their first application, would still generate positive outcomes after the application decision.
IC-level Production Functions
Given the significant challenges involved in determining the causal impact of the SBIR/STTR programs on innovation outcomes at the level of individual grants, the committee considered a final analysis focused on the overall output associated with the grants allocated to each IC on a yearly basis. Specifically, the committee examined how changes over time in the budget appropriated to each IC for extramural R&D for each fiscal year (which then translates on a percentage basis to the SBIR and STTR budget for that IC for that fiscal year) corresponded to changes in the future level of innovation and commercialization outcomes for the firms funded by that IC within that fiscal year. The committee believes that this approach offers insight since there is good
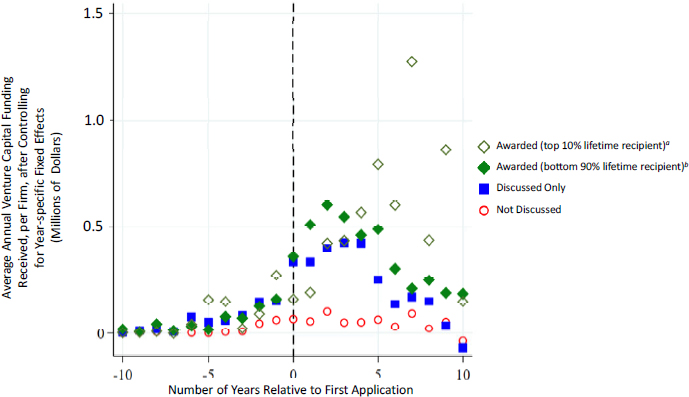
SOURCE: Committee calculations based on fiscal year 2000–2018 NIH SBIR/STTR application data and Crunchbase data.
a Firms that fall in the top 10 percent of support from the programs from 1995 to 2019.
b Firms that fall in the bottom 90 percent of support from the programs from 1995 to 2019.
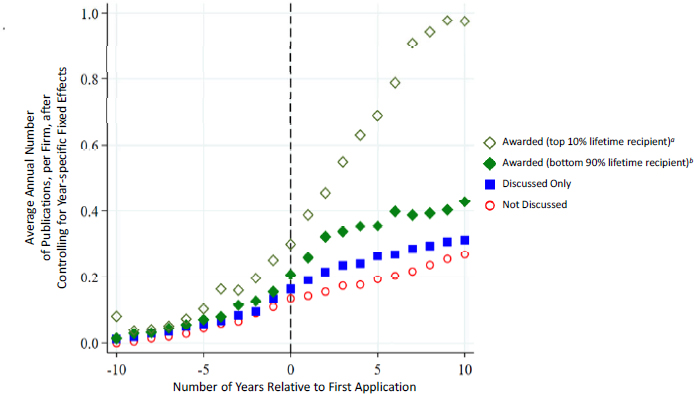
SOURCE: Committee calculations based on fiscal year 2000–2018 NIH SBIR/STTR application data and PubMed data.
a Firms that fall in the top 10 percent of support from the programs from 1995 to 2019.
b Firms that fall in the bottom 90 percent of support from the programs from 1995 to 2019.
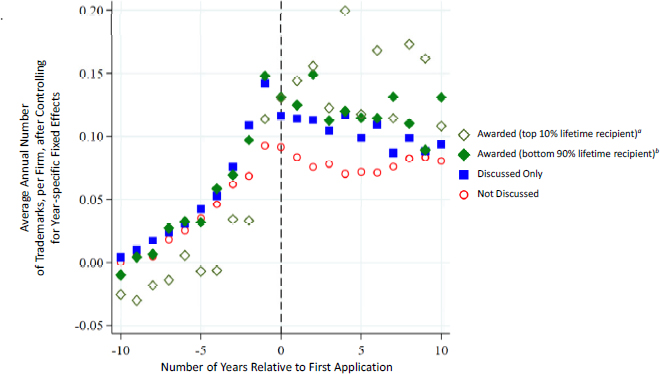
SOURCE: Committee calculations based on fiscal year 2000–2018 NIH SBIR/STTR application data and U.S. Patent and Trademark Office registered trademark data.
a Firms that fall in the top 10 percent of support from the programs from 1995 to 2019.
b Firms that fall in the bottom 90 percent of support from the programs from 1995 to 2019.
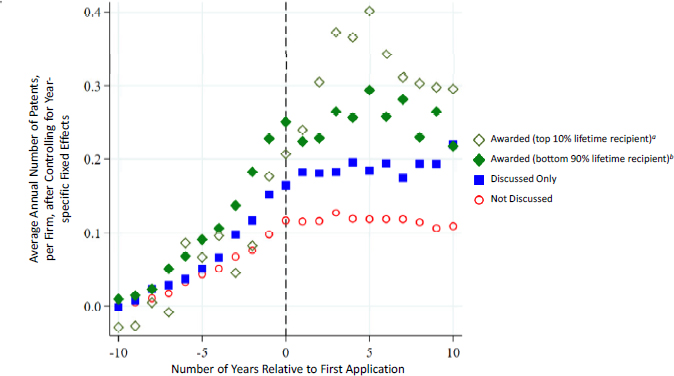
SOURCE: Committee calculations based on fiscal year 2000–2018 NIH SBIR/STTR application data and U.S. Patent and Trademark Office PatentsView database.
a Firms that fall in the top 10 percent of support from the programs from 1995 to 2019.
b Firms that fall in the bottom 90 percent of support from the programs from 1995 to 2019.
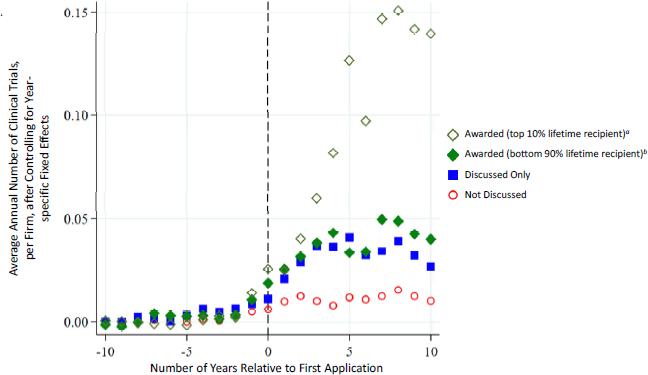
SOURCE: Committee calculations based on fiscal year 2000–2018 NIH SBIR/STTR application data and data on clinical studies from ClinicalTrials.gov.
a Firms that fall in the top 10 percent of support from the programs from 1995 to 2019.
b Firms that fall in the bottom 90 percent of support from the programs from 1995 to 2019.
reason to believe that aggregate fluctuations at the IC level are unrelated to unobservable shocks in the supply of or demand for the specific research performed by these firms (compared with the firm-level variation in funding), especially because the SBIR/STTR programs account for fixed percentage of each IC’s funding amount.
For this analysis the committee first converted firm-level data into IC-level data by allocating all firms’ outcomes to the ICs in a proportional manner based on which ICs funded each firm. These funding choices were then related to outcomes, focusing on IC-year-level variation. Specifically, outcomes and funding flows at the IC-year level are summed over funded and unfunded firms separately, generating two observations for each IC-year unit: one for the outcomes and funding levels (up to that year) for all firms that were ever funded by that IC, and one for the outcomes for all firms that were never funded but applied to that same IC (where funding was always zero). The committee then considered the impact of changes in the overall funding flow for a given IC in a given year on each of the innovation and commercialization outcomes. The specification controlled for both the IC and the year, and so the source of variation is defined as the degree of variation within a given IC over time (compared with other ICs and with firms that applied for but did not receive funding).
The committee used this approach to develop an estimate of the implied “cost” of producing various innovation and commercialization outcomes. Specifically, by estimating how much a particular outcome measure changed with a change in the overall IC spending on the SBIR/STTR programs, the committee was able to estimate the rate at which additional funding translated into additional levels of that outcome measure. The committee used a stock-and-flow regression to estimate how the flow of outcomes relates to the stock of SBIR/STTR funding; the results are shown in Table 5-4.
Table 5-4 reports estimates for each of the eight outcomes, which were used to estimate eight separate regressions, along with the implied marginal costs based on those estimates. This table shows that increased funding allocated to an IC’s SBIR/STTR programs would generate more future outcomes in the form of publications, patents, trademarks, clinical trials, and drug approvals. The marginal costs indicate how much funding is necessary to spur one more outcome (recognizing that the SBIR/STTR money is only part of the financing that gets these firms to these outcomes). There is no statistically significant effect for venture capital funding, 510(k)’s, and device PMAs. While the estimate of the impact of SBIR/STTR funding on follow-on venture capital funding is large, it is not statistically significant; moreover, the large standard error indicates that a great deal of variation in venture capital funding across firms is not captured by this model.
The implied marginal cost per patent—about $1.5 million—is roughly in line with prior estimates of the marginal cost per patent in the Department of Energy’s SBIR/STTR programs (Howell, 2017; Myers and Lanahan, 2021; NASEM, 2020). According to recent estimates, a U.S. patent generates about
TABLE 5-4 NIH SBIR/STTR: Institute/Center (IC)–Level Production Function Estimates
| Venture Capital Funding (1) | Publications (2) | Patents (3) | Trademarks (4) | Clinical Trials (5) | 510(k)’s (6) | Any Device PMA (7) | Any Drug Approval (8) | |
|---|---|---|---|---|---|---|---|---|
| Stock of SBIR Funding (millions of dollars) | 22,035.1 (20,649.7) | 0.140a (0.00672) | 0.0652a (0.0147) | -0.0137a (0.00340) | 0.0396a (0.00305) | 0.000380 (0.000756) | 0.0000449 (0.0000536) | 0.000271a (0.0000565) |
| Dollars/outcome | 4.54 | 0.715 million | 1.53 million | -7.32 million | 2.53 million | 263.4 million | 2,228 million | 368.9 million |
| Number of observations | 760 | 760 | 760 | 760 | 760 | 760 | 760 | 760 |
| Adjusted R2 | 0.62 | 0.92 | 0.69 | 0.83 | 0.80 | 0.72 | 0.19 | 0.19 |
SOURCE: Committee calculations based on fiscal year 2000–2018 NIH SBIR/STTR application data.
NOTES: Observations are at the IC-year-group level, where the two groups are aggregations of all firms that either ever receive funding or never receive funding. Robust standard errors are in parentheses.
a p <0.01.
$7–8 million in private value to a company (Kogan et al., 2017); this estimate suggests that NIH’s SBIR/STTR programs are stimulating technology in a cost-efficient manner at a rate comparable to that realized by other agencies.
Although there is no perfect benchmark estimate for the marginal cost of publication resulting from a program such as the SBIR/STTR programs, the marginal cost per publication implied by this table—about $715,000—is slightly larger than existing estimates of the R01 program’s marginal cost per publication, which has been estimated to be in the range of $300,000–600,000 (Myers, 2020). Intuitively, the R01 program would be expected to be more cost-effective in generating publications (of any sort) because those grants are awarded almost entirely to academic scientists whose primary objective is publishing papers.
The negative effect of funding on the rate of trademarks obtained by SBIR/STTR-funded firms could be due to patents substituting for trademarks for funded firms, as trademarks may serve as cheaper strategic substitutes for patents (Llerena and Millot, 2013). The estimates for clinical trials and drug approval outcomes are positive and statistically significant, suggesting that NIH’s SBIR/STTR programs provide funding that helps firms make important strides in the testing and commercialization of medical therapies.
The reported marginal costs (for all outcome metrics) do not necessarily reflect the implied total marginal costs (e.g., borne by the firm, the SBIR/STTR programs, and outside investors), but the marginal effect of funding from the SBIR/STTR programs and all of the resources this funding attracts. At the same time, the societal benefit of new therapeutics can be a multiple of their sales revenue, suggesting that the social value of these investments may be well worth their cost (Goldman et al., 2010; Lakdawalla et al., 2010; Philipson and Jena, 2005).
IMPACT ON HEALTH CARE
Numerous previous studies have attempted to link overall NIH funding to aggregate health outcomes. Manton and colleagues (2009) examine associations between mortality rates for four major diseases and previous NIH funding for the ICs most likely to fund them, finding a decline in mortality for two of the diseases correlated with NIH funding. More microlevel case study approaches look at linkages between progress in cardiovascular outcomes (Cutler and Kadiyala, 2003) and heart attack treatment (Heidenreich and McClellan, 2003) and specific NIH investments. Still other approaches use patent linkages and other measures to look at how specific small-molecule drugs link to public-sector funding (Sampat and Lichtenberg, 2011; Stevens et al., 2011), including work on the most “transformative’’ drugs for patient care (Kesselheim et al., 2015). Finally, econometric approaches (Azoulay et al. 2019; Blume-Kohout et al., 2009; Toole, 2012) relate variation in NIH funding to outcomes, including approved drugs and clinical trials.
None of these approaches works perfectly for the SBIR/STTR programs. Relating overall variation in SBIR/STTR funding to health aggregates (e.g.,
mortality, drug approvals in a disease area), while feasible, would not make sense since SBIR/STTR funding correlates with the much larger stock and flow of overall NIH funding. Moreover, the exercise would face some of the perennial measurement and conceptual issues encountered by broader exercises to assess health returns (including those cited above), such as the following:
- The lags between NIH funding and outcomes are long and heterogeneous.
- The impact of the funding may not be in the same disease area, and indeed some funding does not map neatly to specific diseases.
- Variation in funding may be associated with other factors affecting health outcomes.
- Public funding may “crowd out’’ private funding.
Twenty-five years ago, Cockburn and Henderson (1996) noted that “it has proven very difficult to estimate the rate of return to publicly funded research with any precision.” This statement remains true today.
Another issue with previous studies of NIH in general is that not all, or even most, of the effects of NIH funding will influence health through specific products. Instead, the knowledge generated may change health behaviors or clinical practices (Cutler and Kadiyala, 2003; Heidenreich and McClellan, 2003). Still, given the mandate and focus of the SBIR/STTR programs, looking at products linked to the programs’ funding is a useful first step for understanding their health care impact.
As discussed above, firms associated with the SBIR/STTR programs developed 99 drugs, 34 devices, 2,475 510(k)’s, and more than 8,974 trademarks (many of which are products) after receiving their first SBIR/STTR funding over the 1996 to 2020 time period. A proper assessment of the health impact of the programs would require clinical evidence on each of these outputs, along with some evidence that they would not have been developed absent the programs. Nonetheless, the lists of these outputs provide an overview of the product space for funded firms. Monitoring and tracking of trademarks could inform NIH’s own collection of “success stories’’ by linking the SBIR/STTR programs to products.19
The committee’s analysis provides evidence that increases in SBIR/STTR funding allocations at the IC level led to statistically significant increases in publications, patents, clinical trials, and drug approvals.20 With the exception of the last of these measures, none has been directly validated as a “surrogate endpoint” or proxy for improved health outcomes. For pharmaceuticals, numerous papers (Lichtenberg, 2018, 2019, 2020, 2021) report associations between new drugs and reduced morbidity, mortality, hospitalization, costs, and other measures of disease burden.
___________________
19https://sbir.nih.gov/stories.
20 Note, however, that the new drug measure used in the committee’s analysis includes not just NMEs (the focus of most previous research) but also line extensions and biologic drugs.
ADDITIONAL DATA NEEDED FOR FUTURE ANALYSES
As described earlier in this chapter, the committee benefited from public information on SBIR and STTR awardees available in NIH’s RePORTER database and from information on applicants from 1995 to 2019 provided by NIH through a data request to the NIH Small Business Education and Entrepreneurial Development (SEED) Office. The applicant data provided by NIH included the names of the small businesses and principal investigators for all applications. In addition, NIH provided information about whether each application was discussed by the Center for Scientific Review’s review panel.21 The information provided by NIH was extremely valuable for the committee’s program evaluations reported in this chapter, and the committee recognizes the considerable time and effort spent by NIH in collecting this information.
While the RePORTER database is quite comprehensive in many ways, there are opportunities for NIH to augment and verify the data therein. In particular, as pointed out in Chapter 4, the patent data in RePORTER do not include all of the patents attributed to NIH’s SBIR and STTR awards as reported in the government-interest statements filed with USPTO. Updating these data in RePORTER, as well as augmenting such innovation and commercialization metrics as trademarks, 510(k)’s, and PMAs for SBIR and STTR awards, would help NIH understand the impact of its SBIR and STTR programs. Additionally, although NIH is required to make the review panel rosters public, the agency maintains electronic copies of these rosters only for the current fiscal year cycle. After that, paper copies are sent to the Library of Congress, but the committee found that many of those review panel rosters were not available in the Library of Congress. In particular, the Library of Congress had no record of the 2015–2019 review panel rosters. To determine whether changes in the demographics of reviewers affect the set of awardees, it is important for evaluators to have access to all review panel rosters, preferably in a machine-readable format, to aid in evaluation.
Congress assigned responsibility for developing and maintaining a public electronic database of SBIR/STTR awards to the administrator of the Small Business Administration (SBA). While this database contains information on the demographics of small business owners, it does not contain some of the other information required by the SBIR/STTR Reauthorization Act of 2011, such as the demographics of the PIs. Additionally, comparisons between the RePORTER database and the SBA awards database revealed that many of the awards in the SBA database that were included in RePORTER were missing (or missing most of) the information that is available in RePORTER. Thus the SBA database needs to be matched against public information, such as that in RePORTER. In addition, missing demographic information could be verified and augmented through the SAM.gov database. Finally, information on research partners is available only for STTR awards. However, SBIR awards are likely to have a research partners, even
___________________
21 See Chapter 3 for a detailed description of the application review process.
though this is not required. A full understanding of how partnerships between research institutions and small businesses occur will require information on partnerships between SBIR awardees and their research partners.
In addition to SBA’s public database, the SBA administrator was assigned responsibility for developing and maintaining a government database of all SBIR/STTR applicants to be used exclusively for SBIR and STTR program evaluation. As discussed in this chapter, information on how SBIR and STTR applicants scored on peer review is an important component of evaluating the programs and therefore warrants inclusion in the government database.
FINDINGS AND RECOMMENDATIONS
Finding 5-1: NIH SBIR/STTR awards result in numbers of patents (reported through iEdison) and clinical studies per award and per dollar similar to those resulting from NIH’s Research Project Grant (R01) program. The actual number of patents is likely much larger for NIH SBIR/STTR awards because of underreporting.
Finding 5-2: NIH SBIR/STTR-funded firms have introduced many clinically important drugs, both small-molecule and biologics; devices; and products. About one-third of SBIR/STTR awardees have received a trademark and/or Food and Drug Administration clearance to market a drug or device (PMA or 510[k]) after receiving their award.
Finding 5-3: The NIH SBIR/STTR programs are attracting applicants that are more likely to be high-growth companies relative to the general biotech startup population, and the quality of awardees has been increasing over time.
Finding 5-4: NIH SBIR/STTR-funded firms do better than unfunded applicants on various commercialization metrics and outcomes. However, these firms were already doing well on these measures before receiving SBIR/STTR funding.
Finding 5-5: Higher levels of funding at the IC level would result in higher levels of publications, patents, clinical trials, and drug approvals.
Recommendation 5-1: The NIH Small Business Education and Entrepreneurial Development Office should systematically monitor commercialization outcomes for SBIR/STTR recipients in Food and Drug Administration databases for commercialized drugs and devices and U.S. Patent and Trademark Office databases for patented and trademarked products. Doing so would inform NIH’s own collection of “success stories,” as well as analyses of the health and economic impacts of specific linked products.
Recommendation 5-2: To facilitate evaluation of the impact of SBIR and STTR grants, Congress should consider requiring amendments to the data collection requirements for the SBIR/STTR public and government databases mandated in the Small Business Act.
- Congress should consider requiring that the administrator of the Small Business Administration use data in other government databases, as collected from the respective agencies, to verify and supplement all data in the SBIR/STTR public and government databases to ensure the accuracy and completeness of the SBIR/STTR data. For example, demographic information on small business owners and principal investigators could be verified using SAM.gov, and the set of awardees could be verified with NIH’s RePORTER database.
- Congress should also consider requiring that the government SBIR/STTR database include data on the scoring or ranking of all applicants. For NIH, that would include the Center for Scientific Review’s priority scores for applicants.
- Additionally, Congress should consider requiring that the SBIR/STTR public database contain information on research partnerships for SBIR awards, complementing its current requirement to report this information for STTR awards.
ANNEX 5-1:
DATA SOURCES FOR NAME-MATCHED OUTCOMES
Food and Drug Administration (FDA) Drugs
The committee collected information on FDA-approved drugs from the Compilation of CDER NME and New Biologic Approvals database: https://www.fda.gov/drugs/drug-approvals-and-databases/compilation-cder-newmolecular-entity-nme-drug-and-new-biologic-approvals. The committee focused on all new molecular entities (NMEs) and biological license applications (BLAs) in the dataset approved between 1995 and 2020. The committee used the applicant field in the file to determine the firm linked to marketing approval for each product.
FDA Devices: Applications for Premarket Approval (PMAs)
PMA is the regulatory pathway for novel devices that pose substantial levels of risk to patients. The PMA pathway is used for Class III devices—those that “support or sustain human life, are of substantial importance in preventing impairment of human health, or which present a potential, unreasonable risk of illness or injury.” The committee collected information on PMAs for Class III medical devices from the FDA: https://www.fda.gov/medical-devices/device
approvals-denials-and-clearances/pma-approvals. As with drugs, the committee focused on all approvals between 1995 and 2020. The committee focused on the first approval for each PMA (removing supplements), and determined the firm associated with each such approval. The device database includes information on the city and state for each applicant, which the committee also used in the match below.
FDA Devices: 510(k)’s
510(k) is the regulatory pathway for devices to be legally marketed if they can be deemed substantially equivalent to currently marketed devices that have already been cleared by the FDA. The vast majority of medical devices sold in the United States have been cleared for sale via the 510(k) pathway. The committee collected data on 510(k) clearances directly from the OPEN FDA website, using the endpoint application programming interface (API) for 510(k): https://open.fda.gov/apis/device/510k. The committee downloaded all 510(k)’s from the years 1995–2020. Like the PMA data, the 510(k) dataset includes information on the city and state for each applicant, which the committee used in the match below.
Clinical Trials
The committee collected data on clinical trials from the Aggregate Analysis of ClinicalTrials.gov (AACT) database, which includes all studies registered in ClinicalTrials.gov. The committee used the firm name information in the file sponsors.txt to link to a clinical trials identifier (NCTID).
Granted Patents
The committee collected data on granted patents from the U.S. Patent and Trademark Office’s (USPTO’s) PatentsView database: https://patentsview.org/download/data-download-tables. For each patent, the committee determined the filing date, issue data, assignee(s), and assignee(s)’ location, using information from the application, patent, and assignee files. The committee focused on all granted patents filed after 1995.
Granted Trademarks
The committee used information from the raw USPTO trademark case files to link firms to trademarks: https://developer.uspto.gov/product/trademarkcase-file-economics-data-stata-dta-and-ms-excel-csv. The committee used collected information from the case file to compile all granted trademarks filed after 1995, and used information from the owner file to determine city and state for the initial owners. In some analyses, the committee also used information from the intl_class file to describe distributions of trademarks by field.
Venture Capital Funding
To gather data on funding from private investors obtained by startup firms, the committee used data from Crunchbase, which aggregates data on startups: https://www.crunchbase.com/home. The committee pulled data on all rounds of venture capital and angel funding for U.S.-based firms in the biotech and health care industries between January 1, 2000, and December 31, 2020.
Startup Cartography Project Entrepreneurial Quality Index
To create a proxy for firms’ underlying quality, the committee relied on the Startup Cartography Project (SCP) Entrepreneurial Quality Index (Andrews et al., 2020). The authors use data on new business registrations to predict the probability of a firm’s “growth,” defined as a successful initial public offering (IPO) or acquisition within 6 years of founding. With a relatively small number of observables, they can predict growth with relative accuracy (e.g., the R2’s on their models are typically around 0.15, which is meaningful given the rarity of growth among all small firms). See Andrews et al. (2020) for further details on their data sources and methodology. Because of the difficulties of matching data using firms’ names (see below), the committee was able to match only 68 percent of NIH applicants to their SCP forecasts. Thus, any analyses relying on these forecasts are based on this subset of the data.
PubMed Indexed Publications
Firms’ research journal publications were collected from an index of the National Library of Medicine’s PubMed database. Firm names were identified via the “affiliation” field for any authors on publications.
Name-Matching Algorithm
The committee used the firm name information from each of the above data sources to merge to the NIH applicant data. Specifically, the committee relied on name standardization codes from the National Bureau of Economic Research (NBER) Patent Project22 to standardize firms’ reported names in the NIH data and all outcome datasets. The committee relied on NIH’s official firm identification number for a firm’s unique identifier. Roughly 2 percent of NIH applicants had firm names that were not unique after the name standardization code had been applied. For these few firms, the committee used the firm-year-level average of any outcomes as its prediction of the firms’ actual outcome rates.
___________________
ANNEX 5-2:
ADDITIONAL TABLES
TABLE 5-2.1 NIH SBIR/STTR-funded Firms: Firm-linked NMEs and BLAs, for drugs receiving FDA approval from 1996 to 2020
| Firm | First Year Funded/Last Year Funded (fiscal year) | Approval Year | Proprietary Name | Active Ingredient | NDA/BLA | Description | Publicly Traded (calendar year) |
|---|---|---|---|---|---|---|---|
| Acadia Pharmaceuticals San Diego, CA | 2000 2014 | 2016 | Nuplazid | pimavanserin | NDA | Indicated for the treatment of hallucinations and delusions associated with Parkinson’s disease psychosis. | ACAD |
| Acorda Therapeutics Hawthorne, NY | 1996 2005 | 2010 | Ampyra | dalfampridine | NDA | Indicated as a treatment to improve walking in patients with multiple sclerosis (MS). This was demonstrated by an increase in walking speed. | ACOR |
| Adolor Malvern, PA | 1997 2001 | 2008 | Entereg | alvimopan | NDA | Indicated to accelerate the time to upper and lower gastrointestinal recovery following partial large or small bowel resection surgery with primary anastomosis. | Acq. by Cubist Pharmaceuticals, 2011 |
| Alexion Pharmaceuticals Cheshire, CT | 1994 2006 | 2007 | Soliris | eculizumab | BLA | Indicated for the treatment of paroxysmal nocturnal hemoglobinuria to reduce hemolysis. | Acq. by AstraZeneca, 2021 |
| Alexion Pharmaceuticals Cheshire, CT | 1994 2006 | 2015 | Kanuma | sebelipase alfa | BLA | Indicated for the treatment of patients with a diagnosis of lysosomal acid lipase (LAL) deficiency. | Acq. by AstraZeneca, 2021 |
| Alexion Pharmaceuticals Cheshire, CT | 1994 2006 | 2015 | Strensiq | asfotase alfa | BLA | Indicated for the treatment of patients with perinatal/infantile- and juvenile-onset hypophosphatasia (HPP). | Acq. by AstraZeneca, 2021 |
| Alexion Pharmaceuticals Cheshire, CT | 1994 2006 | 2018 | Ultomiris | ravulizumabcwvz | BLA | Indicated for the treatment of adult patients with paroxysmal nocturnal hemoglobinuria (PNH). | Acq. by AstraZeneca, 2021 |
| Alkermes Cambridge, MA | 1990 2001 | 2015 | Aristada | aripiprazole lauroxil | NDA | Indicated for treatment of schizophrenia. | n/a |
| Allos Therapeutics Denver, CO | 1995 2000 | 2009 | Folotyn | pralatrexate | NDA | Indicated for the treatment of patients with relapsed or refractory peripheral T-cell lymphoma (PTCL). | Acq. by Spectrum Pharamceuticals, 2012 |
| Alnylam Pharmaceuticals Cambridge, MA | 2006 | 2018 | Onpattro | patisiran | NDA | Indicated for the treatment of the polyneuropathy of hereditary transthyretin-mediated amyloidosis in adults. | ALNY |
| Alnylam Pharmaceuticals Cambridge, MA | 2006 | 2019 | Givlaari | givosiran | NDA | Indicated for the treatment of adults with acute hepatic porphyria (AHP). | ALNY |
| Alnylam Pharmaceuticals Cambridge, MA | 2006 | 2020 | Oxlumo | lumasiran | NDA | Indicated for the treatment of primary hyperoxaluria type 1 (PH1) to lower urinary oxalate levels in pediatric and adult patients. | ALNY |
| Ariad Pharmaceuticals | 1993 1997 | 2012 | Iclusig | ponatinib | NDA | Indicated for the treatment of adult patients with chronic phase, accelerated phase, or blast phase chronic myeloid leukemia (CML) that is resistant to prior tyrosine kinase inhibitor therapy or Philadelphia chromosome positive | Acq. by Takeda, 2017 |
| Firm | First Year Funded/Last Year Funded (fiscal year) | Approval Year | Proprietary Name | Active Ingredient | NDA/BLA | Description | Publicly Traded (calendar year) |
|---|---|---|---|---|---|---|---|
| acute lymphoblastic leukemia (Ph+ALL) that is resistant or intolerant to prior tyrosine kinase inhibitor therapy. | Acq. by Takeda, 2017 | ||||||
| Ariad Pharmaceuticals | 1993 1997 | 2017 | Alunbrig | brigatinib | NDA | Indicated for the treatment of patients with anaplastic lymphoma kinase (ALK)-positive metastatic non-small cell lung cancer (NSCLC) who have progressed on or are intolerant to crizotinib. | Acq. by Takeda, 2017 |
| Avanir Pharmaceuticals San Diego, CA | 1990 2005 | 2000 | Abreva | docosanol | NDA | Indicated for the treatment of cold sores and fever blisters. | Acq. by Otsuka Pharmaceuticals, 2014 |
| Avid Radiopharmaceuticals, Inc. Philadelphia, PA | 2005 2009 | 2012 | Amyvid | florbetapir F 18 | NDA | Indicated for positron emission tomography (PET) imaging of the brain to estimate beta-amyloid neuritic plaque density in adult patients with cognitive impairment who are being evaluated for Alzheimer’s disease (AD) and other causes of cognitive decline. | Acq. by Lilly, 2010 |
| Avid Radiopharmaceuticals, Inc. Philadelphia, PA | 2005 2009 | 2020 | Tauvid | flortaucipir F 18 | NDA | Indicated for positron emission tomography (PET) imaging of the brain to estimate the density and distribution of aggregated tau neurofibrillary tangles (NFTs) in | Acq. by Lilly, 2010 |
| adult patients with cognitive impairment who are being evaluated for Alzheimer’s disease (AD). | |||||||
| BioCryst Pharmaceuticals Birmingham, AL | 1991 2004 | 2014 | Rapivab | peramivir | NDA | Indicated for the treatment of acute uncomplicated influenza in patients 18 years and older who have been symptomatic for no more than 2 days. | BCRX |
| BioCryst Pharmaceuticals Birmingham, AL | 1991 2004 | 2020 | Orladeyo | berotralstat | NDA | Indicated as prophylaxis to prevent attacks of hereditary angioedema (HAE) in adults and pediatric patients 12 years and older. | BCRX |
| BioMarin Pharmaceutical Novato, CA | 1998 2002 | 2014 | Vimizim | elosulfase alfa | BLA | Indicated for patients with Mucopolysaccharidosis type IVA (MPS IVA; Morquio A syndrome). | BMRN |
| BioMarin Pharmaceutical Novato, CA | 1998 2002 | 2017 | Brineura | cerliponase alfa | BLA | Indicated to slow the loss of ambulation in symptomatic pediatric patients 3 years of age and older with late infantile neuronal ceroid lipofuscinosis type 2 (CLN2), also known as tripeptidyl peptidase 1 (TPP1) deficiency. | BMRN |
| BioMarin Pharmaceutical Novato, CA | 1998 2002 | 2018 | Palynziq | pegvaliase-pqpz | BLA | Indicated to reduce blood phenylalanine concentrations in adult patients with phenylketonuria (PKU) who have uncontrolled blood phenylalanine concentrations greater than 600 micromol/L on existing management. | BMRN |
| Firm | First Year Funded/Last Year Funded (fiscal year) | Approval Year | Proprietary Name | Active Ingredient | NDA/BLA | Description | Publicly Traded (calendar year) |
|---|---|---|---|---|---|---|---|
| BioMarin Pharmaceutical Novato, CA | 1998 2002 | 2003 | Aldurazyme | laronidase | BLA | Indicated for patients with Hurler and Hurler-Scheie forms of Mucopolysaccharidosis I (MPS I) and for patients with the Scheie form who have moderate to severe symptoms. | BMRN |
| BioMarin Pharmaceutical Novato, CA | 1998 2002 | 2005 | Naglazyme | galsulfase | BLA | Indicated for treatment of patients with Mucopolysaccharidosis VI (MPS VI). | BMRN |
| BioMarin Pharmaceutical Novato, CA | 1998 2002 | 2007 | Kuvan | sapropterin dihydrochloride | NDA | Indicated to reduce blood phenylalanine levels in patients with hyperphenylalaninemia (HPA) due to tetrahydrobiopterin (BH4)-responsive Phenylketonuria (PKU). | BMRN |
| Cell Therapeutics Seattle, WA | 1999 | 2000 | Trisenox | arsenic trioxide | NDA | Indicated for induction of remission and consolidation in patients with acute promyelocytic leukemia (APL) who are refractory to, or have relapsed from, retinoid and anthracycline chemotherapy, and whose APL is characterized by the presence of the t(15;17) translocation or PML/RAR-alpha gene expression. | CTIC |
| COR Therapeutics South San Francisco, CA | 1989 2002 | 1998 | Integrilin | eptifibatide | NDA | Indicated for treatment of patients with acute coronary syndrome (UA/NQMI), including patients who are to be managed medically and those undergoing percutaneous coronary intervention (PCI). | Acq. by Millennium Pharmaceuticals, 2001 |
| Corixa Seattle, WA | 1994 2004 | 2003 | Bexxar | tositumomab, iodine I 131 tositumomab | BLA | Indicated for the treatment of patients with CD20 positive, follicular, non-Hodgkin’s lymphoma, with and without transformation, whose disease is refractory to Rituximab and has relapsed following chemotherapy. | Acq. by GSK, 2017 |
| Cubist Pharmaceuticals Lexington, MA | 1995 2004 | 2003 | Cubicin | daptomycin | NDA | Indicated for treatment of complicated skin and skin structure infections caused by susceptible strains of Gram-positive microorganisms. | Acq. by Merck & Co., 2014 |
| Cubist Pharmaceuticals Lexington, MA | 1995 2004 | 2014 | Sivextro | tedizolid phosphate | NDA | An oxazolidinone-class antibacterial indicated for the treatment of acute bacterial skin and skin structure infections (ABSSSI) caused by susceptible isolates of several Gram-positive microorganisms. | Acq. by Merck & Co., 2014 |
| Cubist Pharmaceuticals Lexington, MA | 1995 2004 | 2014 | Zerbaxa | ceftolozane, tazobactam | NDA | Indicated for the treatment of patients 18 years or older with infections caused by several designated susceptible Gram-negative and Gram-positive microorganisms. | Acq. by Merck & Co., 2014 |
| Firm | First Year Funded/Last Year Funded (fiscal year) | Approval Year | Proprietary Name | Active Ingredient | NDA/BLA | Description | Publicly Traded (calendar year) |
|---|---|---|---|---|---|---|---|
| CV Therapeutics Palo Alto, CA | 2000 | 2006 | Ranexa | ranolazine | NDA | Indicated for the treatment of chronic angina. | Acq. by Gilead Sciences, 2009 |
| Cypress Bioscience San Francisco, CA | 1985 1997 | 2009 | Savella | milnacipran hydrochloride | NDA | Indicated for the management of fibromyalgia. Savella is not approved for use in pediatric patients. | Acq. by Ramius, 2010 |
| Diatide Londonderry, NH | 1993 1998 | 1998 | AcuTect | technetium Tc-99m apcitide | NDA | Indicated for scintigraphic imaging of acute venous thrombosis in the lower extremities of patients who have signs and symptoms of acute venous thrombosis. | Acq. by Schering Berlin, 1999 |
| Diatide Londonderry, NH | 1993 1998 | 1999 | NeoTect | technetium Tc 99m depreotide | NDA | Indicated as a scintigraphic imaging agent that identifies somatostatin receptor-bearing pulmonary masses in patients presenting with pulmonary lesions on computed tomography and/or chest x-ray who have known malignancy or who are highly suspect for malignancy. | Acq. by Schering Berlin, 1999 |
| Discovery Laboratories Warrington, PA | 2000 2016 | 2012 | Surfaxin | lucinactant | NDA | Indicated for the prevention of respiratory distress syndrome (RDS) in premature infants at high risk for RDS. | WINT |
| Dow Pharmaceutical Sciences Petaluma, CA | 2004 2006 | 2014 | Jublia | efinaconazole | NDA | An azole antifungal indicated for the topical treatment of onychomycosis of the toenail(s) due to Trichophyton rubrum and Trichophyton mentagrophytes. | Acq. by Valeant, 2008 |
| Dyax Corporation Cambridge, MA | 1996 2000 | 2009 | Kalbitor | ecallantide | BLA | Indicated for treatment of acute attacks of hereditary angioedema (HAE) in patients 16 years of age and older. | Acq. by Shire, 2015 |
| Dyax Corporation Cambridge, MA | 1996 2000 | 2018 | Takhzyro | lanadelumab-flyo | BLA | Indicated for prophylaxis to prevent attacks of hereditary angioedema (HAE) in patients 12 years and older. | Acq. by Shire, 2015 |
| Genzyme Corp. Boston, MA | 1986 1990 | 1998 | Thyrogen | thyrotropin alfa | BLA | Indicated for use as an adjunctive diagnostic tool for serum thyroglobulin (Tg) testing with or without radioiodine imaging in the follow-up of patients with well-differentiated thyroid cancer. | Acq. by Sanofi, 2011 |
| Genzyme Corp. Boston, MA | 1986 1990 | 2003 | Fabrazyme | agalsidase beta | BLA | Indicated for use in patients with Fabry disease to reduce globotriaosylceramide (GL-3) deposition in capillary endothelium of the kidney and certain other cell types. | Acq. by Sanofi, 2011 |
| Genzyme Corp. Boston, MA | 1986 1990 | 2004 | Clolar | clofarbine | NDA | Indicated for treatment of pediatric patients 1–21 years old with relapsed or refractory acute lymphoblastic leukemia after at least two prior regimens. | Acq. by Sanofi, 2011 |
| Genzyme Corp. Boston, MA | 1986 1990 | 2006 | Myozyme | alglucosidase alfa | BLA | Indicated for treatment of Pompe disease (GAA deficiency). | Acq. by Sanofi, 2011 |
| Firm | First Year Funded/Last Year Funded (fiscal year) | Approval Year | Proprietary Name | Active Ingredient | NDA/BLA | Description | Publicly Traded (calendar year) |
|---|---|---|---|---|---|---|---|
| Genzyme Corp. Boston, MA | 1986 1990 | 2008 | Mozobil | plerixafor | NDA | Indicated in combination with granulocyte-colony stimulating factor (G-CSF) to mobilize hematopoietic stem cells to the peripheral blood for collection and subsequent autologous transplantation in patients with non-Hodgkin’s lymphoma (NHL) and multiple myeloma (MM). | Acq. by Sanofi, 2011 |
| Genzyme Corp. Boston, MA | 1986 1990 | 2010 | Lumizyme | alglucosidase alfa | BLA | Lysosomal glycogen-specific enzyme indicated for patients 8 years and older with late (noninfantile) onset Pompe disease (acid alpha-glucosidase [GAA] deficiency) who do not have evidence of cardiac hypertrophy. | Acq. by Sanofi, 2011 |
| Genzyme Corp. Boston, MA | 1986 1990 | 2013 | Kynamro | mipomersen sodium | NDA | Indicated as an adjunct to lipid-lowering medications and diet to reduce low density lipoprotein-cholesterol (LDL-C), apolipoprotein B (apo B), total cholesterol (TC), and non-high-density lipoprotein-cholesterol (non-HDL-C) in patients with homozygous familial hypercholesterolemia (HoFH). | Acq. by Sanofi, 2011 |
| Genzyme Corp. Boston, MA | 1986 1990 | 2014 | Cerdelga | eliglustat | NDA | Indicated for the long-term treatment of adult patients with Gaucher disease type 1 (GD1) who are CYP2D6 extensive metabolizers (EMs), intermediate metabolizers (IMs), or poor metabolizers (PMs) as detected by an FDA-cleared test. | Acq. by Sanofi, 2011 |
| Gilead Sciences Foster City, CA | 2000 2004 | 2001 | Viread | tenofovir disoproxil fumarate | NDA | Indicated for the treatment of HIV-1 infection in adults in combination with other antiretroviral agents. | GILD |
| Gilead Sciences Foster City, CA | 2000 2004 | 2002 | Hepsera | adefovir dipivoxil | NDA | Indicated for treatment of chronic hepatitis B in adults with evidence of active viral replication and either evidence of persistent elevations in serum alanine aminotransferase (ALT)/aspartate aminotransferase (AST) or histologically active disease. | GILD |
| Gilead Sciences Foster City, CA | 2000 2004 | 2003 | Emtriva | emtricitabine | NDA | Indicated for the treatment of HIV infection in adults. | GILD |
| Gilead Sciences Foster City, CA | 1989 1994 | 2007 | Letairis | ambrisentan | NDA | Indicated for treatment of pulmonary arterial hypertension (WHO Group I) in patients with WHO class II or III symptoms to improve exercise capacity and delay clinical worsening. | GILD |
| Gilead Sciences Foster City, CA | 2000 2004 | 2012 | Stribild | elvitegravir, cobicistat, emtricitabine, tenofovir disoproxil fumarate | NDA | Indicated as a complete regimen for the treatment of HIV-1 infection in adults who are antiretroviral treatment-naïve. | GILD |
| Firm | First Year Funded/Last Year Funded (fiscal year) | Approval Year | Proprietary Name | Active Ingredient | NDA/BLA | Description | Publicly Traded (calendar year) |
|---|---|---|---|---|---|---|---|
| Gilead Sciences Foster City, CA | 2000 2004 | 2013 | Sovaldi | sofosbuvir | NDA | A hepatitis C virus (HCV) nucleotide analog NS5B polymerase inhibitor indicated for the treatment of chronic hepatitis C (CHC) infection as a component of a combination antiviral treatment regimen. | GILD |
| Gilead Sciences Foster City, CA | 2000 2004 | 2014 | Zydelig | idelalisib | NDA | Indicated, in combination with rituximab, for the treatment of patients with relapsed chronic lymphocytic leukemia (CLL) for whom rituximab alone would be considered appropriate therapy due to other co-morbidities. Also indicated for the treatment of patients with relapsed follicular B-cell non-Hodgkin’s lymphoma (FL) who have received at least two prior systemic therapies. | GILD |
| Gilead Sciences Foster City, CA | 2000 2004 | 2014 | Harvoni | ledipasvir, sofosbuvir | NDA | Indicated for the treatment of chronic hepatitis C (CHC) genotype 1 infection in adults. | GILD |
| Gilead Sciences Foster City, CA | 2000 2004 | 2015 | Genvoya | elvitegravir, cobicistat, emtricitabine, | NDA | Indicated as a complete regimen for the treatment of HIV-1 infection in adults and pediatric patients 12 years of age and older | GILD |
| tenofovir alafenamide | who have no antiretroviral treatment history or to replace the current antiretroviral regimen in those who are virologically-suppressed (HIV-1 RNA less than 50 copies per mL) on a stable antiretroviral regimen for at least 6 months with no history of treatment failure and no known substitutions associated with resistance to the individual components of GENVOYA. | ||||||
| Gilead Sciences Foster City, CA | 2000 2004 | 2016 | Epclusa | sofosbuvir and velpatasvir | NDA | Indicated for the treatment of adult patients with chronic hepatitis C virus (HCV) genotype 1, 2, 3, 4, 5, or 6 infection—without cirrhosis or with compensated cirrhosis—with decompensated cirrhosis, for use in combination with ribavirin. | GILD |
| Gilead Sciences Foster City, CA | 2000 2004 | 2017 | Vosevi | sofosbuvir, velpatasvir, voxilaprevir | NDA | Indicated for the treatment of adult patients with chronic hepatitis C virus (HCV) infection without cirrhosis or with compensated cirrhosis (Child-Pugh A) who have genotype 1, 2, 3, 4, 5, or 6 infection and have previously been treated with an HCV regimen containing an NS5A inhibitor. | GILD |
| Gilead Sciences Foster City, CA | 2000 2004 | 2018 | Biktarvy | bictegravir, emtricitabine, tenofovir alafenamide | NDA | Indicated as a complete regimen for the treatment of human immunodeficiency virus type 1 (HIV-1) infection in adults who | GILD |
| Firm | First Year Funded/Last Year Funded (fiscal year) | Approval Year | Proprietary Name | Active Ingredient | NDA/BLA | Description | Publicly Traded (calendar year) |
|---|---|---|---|---|---|---|---|
| have no antiretroviral treatment history or to replace the current antiretroviral regimen in those who are virologically suppressed (HIV-1 RNA less than 50 copies per mL) on a stable antiretroviral regimen for at least 3 months with no history of treatment failure and no known substitutions associated with resistance to the individual components of BIKTARVY. | |||||||
| Gilead Sciences Foster City, CA | 2000 2004 | 2020 | Veklury | remdesivir | NDA | Indicated for the treatment of coronavirus disease 2019 (COVID-19) requiring hospitalization in adults and pediatric patients (12 years of age and older and weighing at least 40 kg). | GILD |
| Idec Pharmaceuticals San Diego, CA | 1988 1999 | 2002 | Zevalin | ibritumomab tiuxetan | BLA | As part of a specific therapeutic regimen including Rituximab, Indium-111, Ibritumomab Tiuxetan, and Yttrium-90 Ibritumomab Tiuxetan, indicated for the treatment of patients with relapsed or refractory low-grade, follicular, or transformed B-cell non-Hodgkin’s lymphoma, including patients with Rituximab (Rituxan) refractory follicular non-Hodgkin’s lymphoma. | BIIB |
| (Rituxan) refractory follicular non-Hodgkin’s lymphoma. | |||||||
| Idenix Pharmaceuticals Cambridge, MA | 2000 2002 | 2006 | Tyzeka | telbivudine | NDA | Indicated for treatment of chronic hepatitis B (CHB) in patients with evidence of viral replication and active liver inflammation. | Acq. by Merck & Co., 2017 |
| ImClone Systems New York, NY | 1987 2000 | 2004 | Erbitux | cetuximab | BLA | In combination with irinotecan, indicated for treatment of EGFRexpressing, metastatic colorectal carcinoma in patients who are refractory to irinotecan-based chemotherapy; as a single agent for treatment of EGFRexpressing, metastatic colorectal carcinoma in patients who are intolerant to irinotecan-based chemotherapy. | Acq. by Lilly, 2008 |
| Immunomedics, Inc. Morris Plains, NJ | 1985 2013 | 1996 | CEA-Scan | arcitumomab | BLA | Indicated for use in conjunction with computerized tomography scans to detect recurrent or metastatic colorectal cancer. | Acq. by Gilead Sciences, 2020 |
| Immunomedics, Inc. Morris Plains, NJ | 1985 2013 | 2020 | Trodelvy | sacituzumab govitecan-hziy | BLA | Indicated for the treatment of adult patients with metastatic triple-negative breast cancer (mTNBC) who have received at least two prior therapies for metastatic disease. | Acq. by Gilead Sciences, 2020 |
| Insmed | 1994 2000 | 2005 | Iplex | mecasermin rinfabate (rDNA origin) | BLA | Indicated for treatment of growth failure in children with severe primary IGF-1 deficiency (Primary IGFD) or with growth hormone (GH) gene deletion who have developed neutralizing antibodies to growth hormone. | INSM |
| Firm | First Year Funded/Last Year Funded (fiscal year) | Approval Year | Proprietary Name | Active Ingredient | NDA/BLA | Description | Publicly Traded (calendar year) |
|---|---|---|---|---|---|---|---|
| Intra-Cellular Therapies New York, NY | 2003 2016 | 2019 | Caplyta | lumateperone | NDA | Indicated for the treatment of schizophrenia in adults. | ITCI |
| Ionis Pharmaceuticals Carlsbad, CA | 2008 2009 | 2018 | Tegsedi | inotersen | NDA | Indicated for the treatment of the polyneuropathy of hereditary transthyretin-mediated amyloidosis in adults. | IONS |
| Karyopharm Therapeutics Newton, MA | 2016 2018 | 2019 | Xpovio | selinexor | NDA | Indicated in combination with dexamethasone for the treatment of adult patients with relapsed or refractory multiple myeloma (RRMM) who have received at least four prior therapies and whose disease is refractory to at least two proteasome inhibitors, at least two immunomodulatory agents, and an anti-CD38 monoclonal antibody. | KPTI |
| Lexicon Genetics The Woodlands, TX | 1996 | 2017 | Xermelo | telotristat ethyl | NDA | Indicated for the treatment of carcinoid syndrome diarrhea in combination with somatostatin analog (SSA) therapy in adults inadequately controlled by SSA therapy. | LXRX |
| MacroGenics, Inc. Rockville, MD | 2002 2004 | 2020 | Margenza | margetuximabcmkb | BLA | Margenza is indicated in combination with chemotherapy, for the treatment of adult patients | MGNX |
| with metastatic HER2-positive breast cancer who have received two or more prior anti-HER2 regimens, at least one of which was for metastatic disease. | |||||||
| MedImmune Gaithersburg, MD | 1989 1998 | 1998 | Synagis | palivizumab | BLA | Indicated for prophylaxis of serious lower respiratory tract disease, caused by respiratory syncytial virus (RSV), in pediatric patients at high risk of RSV disease. | Acq. by AstraZeneca, 2007 |
| Millennium Pharmaceuticals Cambridge, MA | 1995 1999 | 2003 | Velcade | bortezomib | NDA | Indicated for treatment of multiple myeloma patients who have received at least two prior therapies and have demonstrated disease progression on the last therapy. | Acq. by Takeda, 2008 |
| NPS Pharmaceuticals Salt Lake City, UT | 1990 1998 | 2012 | Gattex | teduglutide (rDNA origin) | NDA | Indicated for the treatment of adult patients with short bowel syndrome (SBS) who are dependent on parenteral support. | Acq. by Shire, 2015 |
| NPS Pharmaceuticals Salt Lake City, UT | 1990 1998 | 2015 | Natpara | parathyroid hormone | BLA | Indicated as an adjunct to calcium and vitamin D to control hypocalcemia in patients with hypoparathyroidism. | Acq. by Shire, 2015 |
| Navidea Biopharmaceuticals Dublin, OH | 2012 2019 | 2013 | Lymphoseek | technetium Tc 99m tilmanocept | NDA | Indicated for lymphatic mapping with a handheld gamma counter to assist in the localization of lymph nodes draining a primary tumor site in patients with breast cancer or melanoma. | NAVB |
| Neurex Menlo Park, CA | 1986 1996 | 1997 | Corlopam | fenoldopam mesylate | NDA | Indicated for the in-hospital, short-term (up to 48 hours) use in | Acq. by Elan, 1998 |
| Firm | First Year Funded/Last Year Funded (fiscal year) | Approval Year | Proprietary Name | Active Ingredient | NDA/BLA | Description | Publicly Traded (calendar year) |
|---|---|---|---|---|---|---|---|
| the management of severe hypertension when rapid, but quickly reversible, emergency reduction of blood pressure is clinically indicated, including malignant hypertension with deteriorating end-organ function. | |||||||
| Neurocrine Biosciences, Inc. San Diego, CA | 1994 2005 | 2017 | Ingrezza | valbenazine | NDA | Indicated for the treatment of adults with tardive dyskinesia. | NBIX |
| Neurocrine Biosciences, Inc. San Diego, CA | 1994 2005 | 2020 | Ongentys | opicapone | NDA | Indicated for the adjunctive treatment to levodopa/carbidopa in patients with Parkinson’s disease (PD) experiencing “off” episodes. | NBIX |
| Onyx Pharmaceuticals Richmond, CA | 1996 2000 | 2012 | Kyprolis | carfilzomib | NDA | Indicated for the treatment of patients with multiple myeloma who have received at least two prior therapies including bortezomib and an immunomodulatory agent and have demonstrated disease progression on or within 60 days of completion of the last therapy. | Acq. by Amgen, 2013 |
| Optimer Pharmaceuticals San Diego, CA | 2003 2009 | 2011 | Dificid | fidaxomicin | NDA | Indicated for treatment of of Clostridium difficile-associated diarrhea (CDAD), only for infections that are proven or | Acq. by Cubist Pharmaceuticals, 2013 |
| strongly suspected to be caused by Clostridium difficile. | |||||||
| Orphan Medical Minnetonka, MN | 1996 | 1996 | Cystadane | betaine anhydrous | NDA | Indicated for treatment of homocystinuria to decrease elevated homocysteine blood levels. | Acq. by Jazz Pharma, 2005 |
| Orphan Medical Minnetonka, MN | 1996 | 1997 | Antizol | fomepizole | NDA | Indicated as an antidote to ethylene glycol (antifreeze) poisoning in patients who have ingested, or are suspected of having ingested ethylene glycol. | Acq. by Jazz Pharma, 2005 |
| Orphan Medical Minnetonka, MN | 1996 | 1998 | Sucraid | sacrosidase | BLA | Indicated for treatment of the genetically determined sucrase deficiency, which is part of congenital sucrase-isomaltase deficiency (CSID). | Acq. by Jazz Pharma, 2005 |
| Orphan Medical Minnetonka, MN | 1996 | 2002 | Xyrem | sodium oxybate | NDA | Indicated for treatment of cataplexy associated with narcolepsy. | Acq. by Jazz Pharma, 2005 |
| OSI Pharmaceuticals Uniondale, NY | 1985 2001 | 2004 | Tarceva | erlotinib hydrochloride | NDA | Indicated for treatment of locally advanced or metastatic non-small cell lung cancer (NSCLC) after failure of at least one prior chemotherapy regimen. | Acq. by Astellas Pharma, 2010 |
| Palatin Technologies Princeton, NJ | 1986 2002 | 2004 | NeutroSpec | technetium Tc 99m fanolesomab | BLA | Indicated for scintigraphic imaging of patients with equivocal signs and symptoms of appendicitis who are 5 years of age or older. | PTN |
| Pharmacyclics Sunnyvale, CA | 1995 | 2013 | Imbruvica | ibrutinib | NDA | Indicated for treatment of patients with mantel cell lymphoma (MCL) who have received at least one prior therapy. | Acq. by AbbVie, 2015 |
| Firm | First Year Funded/Last Year Funded (fiscal year) | Approval Year | Proprietary Name | Active Ingredient | NDA/BLA | Description | Publicly Traded (calendar year) |
|---|---|---|---|---|---|---|---|
| Portola Pharmaceuticals South San Francisco, CA | 2005 2012 | 2017 | Bevyxxa | betrixaban | NDA | Indicated for the prophylaxis of venous thromboembolism (VTE) in adult patients hospitalized for an acute medical illness who are at risk for thromboembolic complications due to moderate or severe restricted mobility and other risk factors for VTE. | Acq. by Alexion Pharmaceuticals, 2020 |
| Progenics Pharmaceuticals Tarrytown, NY | 1990 2008 | 2008 | Relistor | methylnaltrexone bromide | NDA | Indicated for treatment of opioid-induced constipation in patients with advanced illness who are receiving palliative care, when response to laxative therapy has not been sufficient. | Acq. by Lantheus Holdings, 2020 |
| RadioMedix, Inc. Houston, TX | 2014 2021 | 2020 | Detectnet | copper Cu 64 dotatate | NDA | Indicated for positron emission tomography (PET) for localization of somatostatin receptor–positive neuroendocrine tumors (NETs) in adults. | n/a |
| Scios Sunnyville, CA | 1992 2000 | 2001 | Natrecor | nesiritide | NDA | Indicated for treatment of patients with acutely decompensated congestive heart failure who have dyspnea at rest or with minimal activity. | Acq. by Johnson & Johnson, 2003 |
| Seattle Genetics, Inc. Bothell, WA | 2000 2005 | 2011 | Adcetris | brentuximab vedotin | BLA | Indicated for treatment of patients with Hodgkin’s lymphoma (HL) | SGEN |
| Firm | First Year Funded/Last Year Funded (fiscal year) | Approval Year | Proprietary Name | Active Ingredient | NDA/BLA | Description | Publicly Traded (calendar year) |
|---|---|---|---|---|---|---|---|
| after failure of autologous stem cell transplant (ASCT) or after failure of at least two prior multiagent chemotherapy regimens in patients who are not ASCT candidates. Also indicated for the treatment of patients with systemic anaplastic large-cell lymphoma (sALCL) after failure of at least one prior multiagent chemotherapy regimen. | SGEN | ||||||
| Seattle Genetics, Inc. Bothell, WA | 2000 2005 | 2020 | Tukysa | tucatinib | NDA | Indicated in combination with trastuzumab and capecitabine for treatment of adult patients with advanced unresectable or metastatic HER2-positive breast cancer, including patients with brain metastases, who have received one or more prior antiHER2-based regimens in the metastatic setting. | SGEN |
| Sepracor Marlborough, MA | 1986 1998 | 2004 | Lunesta | eszopiclone | NDA | Indicated for treatment of insomnia. | Acq. by Sumitomo Dainippon Pharma, 2009 |
| SIGA Technologies Corvallis, OR | 1999 2009 | 2018 | Tpoxx | tecovirimat | NDA | Indicated for the treatment of human smallpox disease caused by variola virus in adults and pediatric patients weighing at least 13 kg. | SIGA |
| Firm | First Year Funded/Last Year Funded (fiscal year) | Approval Year | Proprietary Name | Active Ingredient | NDA/BLA | Description | Publicly Traded (calendar year) |
|---|---|---|---|---|---|---|---|
| Stemline Therapeutics New York, NY | 2006 | 2018 | Elzonris | tagraxofusp-erzs | BLA | CD123-directed cytotoxin indicated for the treatment of blastic plasmacytoid dendritic cell neoplasm (BPDCN) in adults and in pediatric patients 2 years and older. | Acq. by Menarini Group, 2020 |
NOTE: BLA = biologics license application; FDA = Food and Drug Administration; NDA = new drug application; NME = new molecular entity.
SOURCE: NIH RePORTER, Small Business Administration Awards Database, and FDA data.
TABLE 5-2.2 Premarket Approval Applications (PMAs) Linked to NIH SBIR/STTR-Funded Firms from 1996 to 2020
| Company Name | Year Founded | SBIR/STTR Awards: First funded year and Last funded year (fiscal year) | Trademark | Description | Trademark Filing Year | Publicly Traded |
|---|---|---|---|---|---|---|
| Abiomed, Inc. Danvers, MA | 1981 | 1983 2011 | IMPELLA 2.5 System | Equipment for providing cardiac pumping or support | 2014 | ABMD |
| Abiomed, Inc. Danvers, MA | 1981 | 1983 2011 | Impella RP System | Implantable cardiac assist device, mainly for blood pumping | 2017 | ABMD |
| Advanced Breath Diagnostics Brentwood, TN | 2001 | 2003 2005 | Gastric Emptying Breath Test (GEBT) | Breath test to aid in diagnosis of gastroparesis | 2011 | N/A |
| Advanced Circulatory Systems, Inc. Rockville, MN | 1997 | 2000 2013 | ResQCPR SYSTEM | Medical device for cardiopulmonary resuscitation and treatment of humans in medical emergency | 2011 | Acq. by ZOLL Medical Corp, 2014 |
| Almen Laboratories, Inc. Vista, CA | 1995 | 2004 2008 | Breast Companion Software System | Software for processing digital images of the anatomy for diagnosis and treatment | 2010 | N/A |
| Angel Medical Systems, Inc. Eatontown, NJ | 2001 | 2009 2015 | AngelMed Guardian System | Implantable medical devices to detect heart anomalies | 2015 | N/A |
| Cardiofocus, Inc. Marlborough, MA | 1990 | 1994 1999 | HeartLight Endoscopic Ablation System | Endoscopically guided and multispectra or light emitting cardiac catheters | 2015 | N/A |
| Company Name | Year Founded | SBIR/STTR Awards: First funded year and Last funded year (fiscal year) | Trademark | Description | Trademark Filing Year | Publicly Traded |
|---|---|---|---|---|---|---|
| Carl Zeiss Meditec, Inc. Jena, Germany | 2002 | 2004 2005 | MEL 80 Excimer Laser System | Lasers for ophthalmological surgical use | 2006 | OCTMKTS: CZMWY |
| Carl Zeiss Meditec, Inc. Jena, Germany | 2002 | 2004 2005 | VisuMax Femtosecond Laser | Surgical lasers and lenses | 2015 | OCTMKTS: CZMWY |
| Cohera Medical, Inc Pittsburgh, PA | 2006 | 2007 2014 | TissuGlu | Surgical glue | 2013 | N/A |
| Cryolife, Inc. Kennesaw, GA | 1984 | 1987 2001 | BioGlue Surgical Adhesive | Biological adhesive for use in the implantation of biological tissue for surgical and clinical use | 2001 | CRY |
| Cryolife, Inc. Kennesaw, GA | 1984 | 1987 2001 | TMR Holmium Laser System | Low-powered laser targeted at heart muscle in order to promote growth of new blood vessels | 1997 | CRY |
| Dexcom, Inc. San Diego, CA | 1999 | 2001 | Dexcom G4 Platinum Contiuous Glucose Monitoring System | Medical sensors to measure glucose content in human body | 2012 | DXCM |
| Dexcom, Inc. San Diego, CA | 1999 | 2001 | Dexcom STS Continous Monitors | Medical sensors to measure glucose content in human body | 2005 | DXCM |
| Genzyme Corporation Boston, MA | 1981 | 1988 1997 | FocalSeal-L Synthetic Absorbable Sealant | Polymerizable material for sealing air leaks following pulmonary surgery | 1999 | Acq. by Sanofi, 2011 |
| Genzyme Corporation Boston, MA | 1981 | 1989 1997 | LEGOO | Medical instruments for use in surgery for occlusion of blood vessels | 2011 | Acq. by Sanofi, 2011 |
| Glaukos Corporation San Clemente, CA | 1998 | 2002 2005 | iStent inject Trabecular Micro-Bypass System (Model G2-M-IS) | Ocular implants and devices for screening and treating glaucoma | 2017 | GKOS |
| Glaukos, Corporation San Clemente, CA | 1998 | 2002 2005 | Glaukos iStent Trabecular Bypass Stent Model GTS100R/L | Ocular implants and devices for screening and treating glaucoma | 2008 | GKOS |
| Hyperbranch Medical Technology, Inc. Durham, NC | 2003 | 2005 2006 | Adherus Autospray Dural Sealant | Synthetic liquid hydrogel-based sealant to create watertight seal for surgical and trauma cases for medical use | 2013 | Acq. by Stryker, 2018 |
| Illumina, Inc. San Diego, CA | 1998 | 1999 2006 | Praxis Extended RAS Panel | Reagants and nucleotides for scientific or medical research use | 2016 | ILMN |
| Integra Lifesciences Corporation Billerica, MA | 1969 | 1995 1999 | DuraSeal Dural Sealant System | Synthetic sealant to insure against dural leakage after head surgery | 2004 | IART |
| Integra Lifesciences Corporation Billerica, MA | 1970 | 1995 1999 | DuraSeal Exact Spine Sealant System | Synthetic sealant to facilitate watertight repair of dural defects after spinal surgery | 2008 | IART |
| Invitrogen Corporation Waltham, MA | 1987 | 1994 2000 | SPOT-Light HER2 CISH Kit | Kits consisting of reagants for scientific or medical research for detection of nucleic acids | 2005 | Acq. By Thermo Fisher Scientific, 2008 |
| Company Name | Year Founded | SBIR/STTR Awards: First funded year and Last funded year (fiscal year) | Trademark | Description | Trademark Filing Year | Publicly Traded |
|---|---|---|---|---|---|---|
| Koning Corporation Norcross, GA | 2002 | 2003 2011 | Koning Breast CT (Model CBCT1000) | Breast imaging scanner for diagnostic imaging of breast cancer | 2013 | N/A |
| Natus Medical Incorporated Pleasanton, CA | 1989 | 1995 | Olympic Cool-Cap | Instruments for measuring, monitoring, recording, reproducing, transmitting data and images regarding electrical activity of the brain | 2004 | NTUS |
| Orasure Technologies, Inc. Bethlehem, PA | 1987 | 2000 2012 | OraQuick HCV Rapid Antibody Test | Rapid-test kits primarily consisting of oral fluid collection pads and vitals | 2008 | OSUR |
| Therox, Inc. Irvine, CA | 1994 | 1996 1998 | TherOx Downstream System | Medical instruments, namely, catheters, pump systems, and tubing to treat conditions such as tissue ischemia and postischemic tissues | 2017 | Acq. by ZOLL Medical Corp, 2019 |
| Thoratec Corporation Pleasanton, CA | 1976 | 1985 1998 | HeartMate II Left Ventricular Assist System | Heart assist devices, namely, blood pumps either pneumatically or electrically actuated | 2006 | Acq. by St. Jude Medical, 2015 |
| Thoratec Corporation Pleasanton, CA | 1976 | 1985 1998 | HeartMate 3 Left Ventricular Assist System | Heart assist devices, namely, blood pumps either pneumatically or electrically actuated | 2016 | Acq. by St. Jude Medical, 2015 |
| W. L. Gore & Associates, Inc. Newark, DE | 1958 | 1986 2005 | GORE Carotid Stent | Stent for aortoilic occlusive disease | 2018 | N/A |
| W. L. Gore & Associates, Inc. Newark, DE | 1958 | 1986 2005 | GORE TAG Thoracic Endoprosthesis | Conformable stent for endovascular treatment for the thoracic aorta | 2004 | N/A |
| W. L. Gore & Associates, Inc. Newark, DE | 1958 | 1986 2005 | GORE TIGRIS Vascular Stent | Synthetic stent grafts | 2016 | N/A |
| W. L. Gore & Associates, Inc. Newark, DE | 1958 | 1986 2005 | GORE Viabahn VBX Balloon Expandable Endoprosthesis | Implantable medical stent graft for endoprosthesis | 2016 | N/A |
| W. L. Gore & Associates, Inc. Newark, DE | 1958 | 1986 2005 | GORE VIATORR TIPS | Endovacular prosthesis | 2004 | N/A |
SOURCE: NIH RePORTER and Food and Drug Administration data.
TABLE 5-2.3 Random Sample of NIH SBIR/STTR-Awarded Firms Linked to 510(k) Medical Devices
| Company Name | Year Founded | SBIR/STTR Awards (First funded year–Last funded year) | Device and Name | Approval Year | Description | Publicly Traded |
|---|---|---|---|---|---|---|
| Surmodics, Inc. Eden Prairie, MN | 1979 | 1983–2003 | Guide Sheath | 2019 | Product for radial artery access | SRDX |
| Photonicare, Inc. Champaign, IL | 2013 | 2015–2020 | Tomi Scope | 2019 | OtoSight Middle Ear Scope | N/A |
| C4 Imaging, LLC Doylestown, PA | 2009 | 2010–2015 | Mri Marker | 2013 | Determines position of high dose rate (HDR) brachytherapy treatment catheters for precise delivery of radiation for cancer treatment | N/A |
| Implant Sciences Corporation Wakefield, MA | 1984 | 1988–2008 | Implant Sciences Corp, Model Hdr-4140 | 2005 | Treatment of cancer through temporary interstitial, intracavitary, intraluminal, intraoperative, or surface irradiation | Acquiring in 2007 by L3 Technologies [LLL] Now Known as Secure Point Technologies Inc. |
| Vista Scientific, LLC Andover, MA | 1997 | 1999–2008 | Vista Scientific Barium Sulfate, Model 3001-1 | 2003 | An additive to Codman CranioplasticTM (Type l-Slow set) to provide radiopacity for imaging purposes | N/A |
| Integra Lifesciences Corp. Plainsboro, NJ | 1989 | 1995–1999 | Avagen Wound Dressing | 2002 | Management of a variety of wounds | IART |
| Omniguide Inc. Cambridge, MA | 2000 | 2002–2005 | Omniguide Beampath Laser Beam Delivery System | 2006 | Product for precise otologic (ear) surgery | N/A |
| Cardiovascular Imaging Technologies Kansas City, MO | 2001 | 2003–2008 | Imagenspect | 2016 | Windows-based software solution providing multiple reconstruction algorithms to increase SPECT image resolution | N/A |
| Rochal Industries, LLC San Antonio, TX | 1986 | 2008–2020 | Atteris Antimicrobial Skin Protectant | 2016 | Protects minor wounds and damaged skin | N/A Sanara MedTech Inc. [SMTI] acquired certain assets of Rochal Industries in 2021 |
| Vidacare Corporation San Antonio, TX | 1999 | 2004–2006 | Humeral Head, Manual Driver | 2006 | For emergency vascular access when standard venous access is not possible | N/A Acquiring Co: Teleflex [TFX] Year of Acquisition: 2013 |
| Spectros Corporation Portola Valley, CA | 1995 | 1996–2011 | T-Stat 303 Ischemia Monitoring System | 2008 | Measures the oxygen content of hemoglobin at a microvascular level | N/A Acquiring Co: Jawbone Year of Acquisition: 2015 |
| DexCom, Inc. Madison, WI | 1999 | 2001 | Studio On The Cloud Data Management Software | 2014 | Data analysis and storage platform for diabetics | DXCM |
| Scantibodies Laboratory, Inc. Santee, CA | 1976 | 2000 | Total Pth Immunoradiometric Assay(Irma) Diagnostic Kit, Model 3kg600 | 2001 | Determines total immunoreactive intact PTH (Total Intact PTH) in blood samples | N/A |
| Company Name | Year Founded | SBIR/STTR Awards (First funded year–Last funded year) | Device and Name | Approval Year | Description | Publicly Traded |
|---|---|---|---|---|---|---|
| HemoSonics, LLC Charlottesville, VA | 2004 | 2010–2017 | Quantra Qplus System | 2020 | Product for in vitro diagnostic use | N/A Acquiring Co: Stago Year of Acquisition: 2017 |
| Cynosure, Inc. Bedford, MA | 1991 | 1992–2000 | Picosure Workstation | 2018 | Product for treating pigmentary conditions, tattoo removal, and skin revitalization | CYNO Acquiring Co: Hologic Year of Acquisition: 2017 Hologic sold Cynosure in 2019 |
| InBios International, Inc. Seattle, WA | 1996 | 2000–2020 | Cl Detect Rapid Test | 2014 | Product for rapid detection of Leishmania species antigen in ulcerative skin lesions | N/A |
| Candela Corporation Wayland, MA | 1970 | 1983–2004 | Candela Gentlemax Family Of Laser System | 2014 | Laser used to treat a variety of dermatology conditions | CLZR Merger Co: Syneron Medical [ELOS] Year of Merge: 2010 |
| Calypso Medical Technologies, Inc. Seattle, WA | 1999 | 2004 | Calypso 4d Localization System | 2008 | Product for monitoring prostate position during treatment | N/A Acquiring Co: Varian Medical |
| Systems [VAR] Year of Acquisition: 2011 | ||||||
| Intelligent Hearing Systems Miami, FL | 1983 | 1991–2020 | Smartep-Assr, Model M811007 | 2004 | Product for recording auditory steady-state evoked potential data | N/A |
| Sulzer Intratherapeutics, Inc. St. Paul, MN | 2001 | 1998–1999 (Intratherapeutics, Inc.) | Intrastent Ld (Large Diameter) Stent | 2002 | Palliative treatment of malignant neoplasms in the biliary tree | N/A Sulzer Medica acquired IntraTherapeut ics Inc. in 2001 and became Sulzer IntraTherapeut ics which operates as a separate company under Sulzer Medica |
| Quidel Corporation San Diego, CA | 1979 | 2004 | Quidel Molecular Hmpv Assay | 2011 | Detection and identification of respiratory syncytial virus (RSV) and human Metapneumovirus (hMPV) viral RNA using real time RT-PCR | QDEL |
| Rochal Industries, LLC San Antonio, TX | 1986 | 2008–2020 | Rochal Antimicrobial Wound Gel | 2020 | Management of ulcers, first- and second-degree burns, partial- and full-thickness wounds, large surface area wounds, and surgical incisions. | N/A Sanara MedTech Inc. [SMTI] acquired |
| Company Name | Year Founded | SBIR/STTR Awards (First funded year–Last funded year) | Device and Name | Approval Year | Description | Publicly Traded |
|---|---|---|---|---|---|---|
| certain assets of Rochal Industries in 2021 | ||||||
| Bio-Logic Systems Corporation Mundelein, IL | 1979 | 1990-2002 | Cochlea-Scan/Cochlea-Scan Plus | 2006 | Used for diagnostic hearing evaluations by means of otoacoustic emissions | BLSC Acquiring Co: Natus Medical Incorporated [NTUS] Year of Acquisition: 2005 |
| Genzyme Corporation Boston, MA | 1981 | 1983–1997 | Genzyme Osom Influenza A & B Test | 2006 | Rapid diagnostic test for the detection of influenza A and influenza B from nasal swab specimens | GENZ Acquiring Co: Sanofi-Aventis Year of Acquisition: 2011 |
| Cepheid Sunnyvale, CA | 1996 | 1998–2006 | Xpert Xpress Flu/Rsv, Xpert Nasopharyngeal Sample Collection Kit, Xpert Nasal Sample Collection Kit, Genexpert Xpress Ii, Genexpert Xpress Iv | 2018 | Rapid molecular testing for a variety of sicknesses such as influenza and RSV | CPHD Acquiring Co: Danaher [DHR] Year of Acquisition: 2016 |
| Lambda S.P.A. Vicenza, Italy | 1996 | 2004–2021 | Doctor Surgery Diode Lasers Family | 2010 | Portable laser surgical instruments for use in general and plastic surgery and dermatology | N/A |
| Maine Molecular Quality Controls, Inc. Scarborough, ME | 2000 | 2000–2006 | Filmarray Pneumonia/Pneumoniapl us Control | 2019 | Used as reference material to monitor the qualitative detection and identification of respiratory viral and bacterial targets in nasopharyngeal swabs (NPS) obtained from individuals suspected of lower respiratory tract infections | N/A |
| Luminex Corporation Austin, TX | 1995 | 2008–2010 | Luminex Flexmap 3d Instrument System, Luminex Xponent 4.0 Spi Software, Flexmap 3d Ivd Calibration Kit, Flexmap 3d Ivd P | 2013 | Multiplexing platform | LMNX Acquiring Co: DiaSorin SpA [DSRLF] Year of Acquisition: 2021 |
| Cepheid Sunnyvale, CA | 1996 | 1998–2006 | Xpert Mrsa/Sa Nasal Assay | 2010 | Presurgical testing of S. aureus and MRSA with results within an hour | CPHD Acquiring Co: Danaher [DHR] Year of Acquisition: 2016 |
| Intuitive Surgical, Inc. Sunnyvale, CA | 1995 | 2004–2006 | Da Vinci S/Si Endoscopes, Da Vinci Xi Endoscopes | 2017 | Robotic endoscope | ISRG |
| Cynosure, Inc. Bedford, MA | 1991 | 1992–2000 | Cynosure Photogenica Lpir Dermatological Laser | 1997 | Laser surgical instrument for use in general and plastic surgery and in dermatology | CYNO Acquiring Co: Hologic Year of Acquisition: 2017 |
| Company Name | Year Founded | SBIR/STTR Awards (First funded year–Last funded year) | Device and Name | Approval Year | Description | Publicly Traded |
|---|---|---|---|---|---|---|
| Possis Medical, Inc. Minneapolis, MN | 1952 | 2001 | Guarddog Occlusion System, Occlusion Guidewire, 300 Cm, Guarddog Occlusion System Occlusion Guidewire, 200 Cm | 2004 | Designed to control blood flow through blood vessels during peripheral endovascular procedures | POSS Acquiring Co: Medrad Inc. Year of Acquisition: 2008; Medrad is a subsidiary of Bayer AG |
| Candela Corp. Wayland, MA | 1970 | 1983–2004 | Candela Gentlelase Gl Dermatological Vascular Lesion Laser | 1997 | Laser used to treat a variety of dermatology conditions | CLZR Merger Co: Syneron Medical [ELOS] Year of Merge: 2010 |
| Vident Brea, CA | 1984 | 2002 | Vita Pm 7 (20 Gram Bottles), Vita Pm 7 (50 Gram Bottles) | 2005 | Porcelain powder for clinical use | N/A Subsidiary of VITA Zahnfab rik; changed its name to Vita North America |
| Organ Recovery Systems, Inc. Charleston, SC | 1998 | 2000–2004 | Sps-1tm Static Preservation Solution, Models Sps-1-500 Ml, Sps 1-1l, Sps-1-2l | 2010 | Flushing and cold storage of abdominal organs | N/A |
| Cynosure, Inc. Bedford, MA | 1991 | 1992–2000 | Cynosure Apogee-Tks Ii Dermatological Laser | 2003 | Laser hair-removal machine | CYNO Acquiring Co: Hologic |
| Year of Acquisition: 2017 | ||||||
| Intuitive Surgical, Inc. Sunnyvale, CA | 1995 | 2004–2006 | Modification To Intuitive Surgical Da Vinci Surgical System And Endoscopic Instruments | 2005 | Robotic surgical instruments for trained physician use | ISRG |
| Intuitive Surgical, Inc. Sunnyvale, CA | 1995 | 2004–2006 | Single-Site Medium-Large Clip Applier, Single-Site Cadiere Grasper, Single-Site Fundus Grasper, Single-Site Crocodile | 2012 | Robotic surgical instruments for trained physician use | ISRG |
| Intuitive Surgical, Inc. Sunnyvale, CA | 1995 | 2004–2006 | Da Vinci Single-Site Instruments And Accessories | 2013 | Robotic surgical instruments for trained physician use | ISRG |
| Nephros, Inc. New York, NY | 1997 | 2003 | Nephros Olpur H2h Hemodiafiltration (Hdf) Module And Olpur Md 220 Hemodiafilter | 2012 | Renal replacement therapy system | NEPH |
| Volcano Corporation Rancho Cordova, CA | 2000 | 2006 | Syncvision System | 2015 | Online image processing workstation for coronary catheterizations | VOLC Acquiring Co: Royal Philips Year of Acquisition: 2015 |
| Immco Diagnostics, Inc. Amherst, NY | 1971 | 1986–2007 | Immulisa Enhanced B2gp1 Iga Antibody Elisa, Immulisa Enhanced B2gp1 Igg | 2017 | Qualitative or semi-qualitative detection of various antibodies in human serum | Year of Acquisition: 2013 |
| Company Name | Year Founded | SBIR/STTR Awards (First funded year–Last funded year) | Device and Name | Approval Year | Description | Publicly Traded |
|---|---|---|---|---|---|---|
| Antibody Elisa, Immulisa Enhanced B2gp1 Igm Antibody Elisa, Immulisa Enhanced B2gp1 Iga/Igg/Igm Antibody Elisa | Year of Acquisition: 2013 | |||||
| Cardiac Mariners, Inc. Los Gatos, CA | 1992 | 1995 | Sbdx Mobile Fluoroscopy System | 1996 | Medical imaging that shows a continuous X-ray image | N/A |
SOURCE: NIH RePORTER and Food and Drug Administration data.
TABLE 5-2.4 Random Sample of Trademarks Linked to NIH SBIR/STTR Awardees
| Company Name | Year Founded | SBIR Awards (First funded year Last funded year) | Trademark | Description | Trademark Filing Year | Publicly Traded |
|---|---|---|---|---|---|---|
| Millennium Pharmaceuticals Cambridge, MA | 1993 | 1997 1998 | IBDATA | Computer application software for smart phones | 2016 | MLNM |
| Natus Medical Incorporated Pleasanton, CA | 1987 | 1995 | HUSH | Medical electrodes and parts, components, and fittings | 1997 | NTUS |
| Cas Medical Systems, Inc. Irvine, CA | 1984 | 1986 2007 | MAXNIBP | Noninvasive medical device to measure blood pressure | 2002 | Acq. by Edwards Lifesciences, 2019 |
| Zirchrom Separations, Inc. Anoka, MN | 1995 | 1998 2005 | PROTAIN | Chemicals for chromatography in filtration and liquid phase separation systems | 2003 | N/A |
| Diacarta Ltd. Richmond, CA | 2011 | 2008 2019 | QFUSION | Testing kit to detect and diagnose genomic disorders | 2017 | N/A |
| New England Biolabs, Inc. Ipswich, MA | 1974 | 1994 2013 | GPS | Enzymes and precursors for in vitro genetic engineering use | 1998 | N/A |
| Polyglot Systems, Inc. Morrisville, NC | 2001 | 2005 2010 | TIMEVIEW | Patient health care record management | 2014 | Acq. by First Databank, 2017 |
| Blueingreen, LLC Portland, OR | 2004 | 2005 | CO2 CDOX | Device for soil remediation and drinking water treatment | 2015 | Acq. by Chart Industries, 2020 |
| Xechem, Inc. New Brunswick, NJ | 1994 | 1992 2006 | VIDA PRAS | Nutritional supplements and vitamins | 2000 | N/A |
| Advanced Breath Diagnostics, LLC Brentwood, TN | 2001 | 2003 | CAIRN DIAGNOSTICS | Diagnostic testing kits for stomach disorders | 2015 | N/A |
| Company Name | Year Founded | SBIR Awards (First funded year Last funded year) | Trademark | Description | Trademark Filing Year | Publicly Traded |
|---|---|---|---|---|---|---|
| 3gen, Inc. Sugar Land, TX | 1999 | 2006 | LUMIO | Battery-powered magnified light for dermatological examinations | 2007 | N/A |
| Novalon Pharmaceutical Corporation Durham, NC | 1996 | 1997 1999 | BIOKEY | Reagents for scientific or medical research use | 1998 | Acq. by Karo Bio, 2000 |
| Sionyx, LLC Beverly, MA | 2006 | 2009 2011 | XQE | Semiconductor chips and photoelectric sensors | 2012 | SINX |
| Cpm Systems, Inc. Los Angeles, CA | 1883 | 1998 2012 | PCQI | Patient health care record management for physician-based practices | 2006 | N/A |
| Frontier Medical, Inc. Ann Arbor, MI | 1966 | 1998 2002 | TRI-WAVE | Electrical stimulation device for pain control of injuries | 2001 | N/A |
| Ascent Technology, Inc. Boulder, CO | 1986 | 1993 1997 | ARIS/WORKMO DEL | Software to determine staffing needs and task assignments | 2003 | N/A |
| Chemgen Corporation Gaithersburg, MD | 1954 | 1992 1995 | WHEATEASE | Nutritional additives for livestock feed | 1997 | Acq. by Eli Lilly, 2012 |
| Genzyme Corporation Boston, MA | 1981 | 1983 1997 | MACI | Pharmaceutical preparation for treatment of articular cartilage disease | 2012 | Acq. by Sanofi, 2011 |
| Natus Medical Incorporated Pleasanton, CA | 1989 | 1995 | EC2 | Cream used when applying electrodes to human body to monitor brain activity | 2001 | NTUS |
| Mesa Tech International, Inc. San Diego, CA | 2004 | 2011 2014 | OSCAR | Chemical test kits for in vitro use in genetic analysis | 2012 | Acq. by Thermo Fisher Scientific, 2016 |
| Astro-Med, Inc. West Warwick, RI | 1969 | 2003 2006 | SZAC | Computer program for detection of spikes and seizure in epilepsy | 2000 | ALOT |
| Molecular Insight Pharmaceuticals, Inc. Cambridge, MA | 1997 | 2003 2012 | ULTRATRACE | Radiopharmaceutical preparations for targeted radiotherapy of cancer | 2005 | Acq. by Progenics Pharmaceuticals, 2013 |
| Lumencor, Inc. Beaverton, OR | 2006 | 2008 | TARGA | Scanners, light sources composed of light emitting diodes | 2013 | N/A |
| Genzyme Corporation Boston, MA | 1981 | 1983 1997 | BRINGING BIOTECHNOLO GY TO SURGERY | Scientific research in biotechnology and surgery | 2001 | Acq. by Sanofi |
| Idea International, Inc. Las Vegas, NV | 2006 2007 | PLAY-A-DENT | Educational software for instruction in field of dentistry | 2010 | N/A | |
| Pacific Bioscience Laboratories, Inc. Bellevue, WA | 2004 | 2007 | MIA PRIMA | Sonic oscillating brushes for skincare | 2017 | PACB |
| Simbiotic Software, Inc Missoula, MT | 1998 | 2005 2010 | OSMOBEAKER | Software for cell biology education | 2008 | N/A |
| Psychology Software Tools, Inc. Pittsburgh, PA | 1987 | 1993 2019 | MOTRAK | Software to track head movement of patient during MRI | 2009 | N/A |
| Cumberland Pharmaceuticals, Inc. Nashville, TN | 1999 | 2004 2018 | OMECLAMOX | Pharmaceutical antiulcer preparations | 2011 | CPIX |
| Company Name | Year Founded | SBIR Awards (First funded year Last funded year) | Trademark | Description | Trademark Filing Year | Publicly Traded |
|---|---|---|---|---|---|---|
| Natus Medical Incorporated Pleasanton, CA | 1987 | 1995 | SONAMED | Auditory equipment for testing and diagnosis of hearing impairment | 1995 | NTUS |
| Research Genetics, Inc. Huntsville, AL | 1987 | 1994 1999 | GENEPAIRS | Natural and synthetic DNA for scientific and medical research | 1997 | N/A |
| Biotherm Raleigh, NC | 1952 | 1987 1996 | FORCE SUPREME | Cosmetic cream for the face | 2007 | Acq. by L’Oréal, 1970 |
| Medical Diagnostic Laboratories, LLC Hamilton, NJ | 1997 | 2010 | FEMERIS WOMEN’S HEALTH RESEARCH CENTER | Research and development in the pharmaceutical and biotechnology fields | 2010 | N/A |
| Puresyn, Inc. Malvern, PA | 1992 | 1997 2003 | ADENOSERVE | Chemical analysis of adenoviral vectors for gene therapies and vaccines | 2009 | N/A |
| Pacific Bioscience Laboratories, Inc. Bellevue, WA | 2004 | 2007 | PEDI | Foot peels, scrubs, and moisturizers | 2013 | PACB |
| Home Access Health Corporation Hoffman Estates, IL | 1996 | 2003 | LAB TEST AT HOME | Stool sample collection kit for lab testing | 2010 | Acq. by EverlyWell, 2021 |
| Cynosure, LLC Bedford, MA | 1991 | 1992 2000 | SIDELAZE | Laser fibers for medical application in devices and apparatus | 2012 | Acq. by Clayton, Dubilier & Rice, 2019 |
| Advanced Technology Materials, Inc. Danbury, CT | 1998 | 2010 | VACUUM ACTUATED CYLINDER | Chemical gas supply equipment to hold gas in pressurized or liquid form | 1999 | Merger with Entegris, 2014 |
| Healthgate Data Corp. Malden, MA | 1994 | 1996 | HealthGate Data | Providing online information services in field of biomedical and health care information | 1998 | N/A |
| Management Science Associates, Inc. Pittsburgh, PA | 1963 | 1987 2020 | GABRIEL | Software for planning advertising campaigns and reporting operation statistics for cable networks | 2014 | N/A |
| Cynosure, Inc. Bedford, MA | 1991 | 1992 2000 | THERMOKINETIC SELECTIVITY | Laser treatment component of long pulse laser machine for medical use | 1999 | Acq. by Clayton, Dubilier & Rice, 2019 |
| Diacor, Inc. Salt Lake City, UT | 1983 | 1997 2000 | INTEGRA | Head and neck immobilization systems for radiation therapy or diagnostic imaging | 2004 | Acq. by Teveystalo, 2017 |
| Molecular Probes, Inc. Eugene, OR | 1975 | 1986 2003 | SYTOX | Fluorescent chemicals for use in scientific research | 1995 | Acq. by Invitrogen, 2003 |
| Virtual Phantoms, Inc. Albany, NY | 2009 | 2010 2016 | ARCHER | Software for radiation transport simulations | 2013 | N/A |
| Centaur Pharmaceuticals, Inc. Sunnyvale, CA | 1978 | 1994 2000 | CARTILEASE | Veterinary food supplements | 2005 | Acq. by Renovis, 2002 |
SOURCE: NIH RePORTER and U.S. Patent and Trademark Office data.
This page intentionally left blank.









































































