Priorities on the Health Horizon: Informing PCORI's Strategic Plan (2022)
Chapter: Appendix A: Topic Briefs for March 1516, 2021 Meeting
Appendix A
TOPIC BRIEFS FOR MARCH 15–16, 2021 MEETING
PCORI PRIORITIES ON THE HEALTH HORIZON MEETING—TECHNOLOGIES TOPIC BRIEF
Definition and Key Components
In this context, the term “technologies” encompasses myriad components, including clinical and computational advances that have led to more precise, predictive, and personalized medicine, therapeutic and device innovations, as well as changes enabled by digital technologies (e.g., virtual care, remote patient monitoring, and integration of devices/wearables to support prevention, diagnosis, treatment, and rehabilitation). The breadth and depth of this topic can include numerous offshoots given the many tools, instruments, and interventions available. Emphasis here is given to examples of how technologies intersect with health and health care and opportunities for emerging technologies to sharpen understanding of the comparative effectiveness of different treatments and illuminate opportunities to reduce health inequities.
Background and Current Profile
Health-related technologies are proliferating, which creates opportunities to optimize treatment at the point of care and to influence touchpoints with patients and consumers outside clinical encounters. The Food and Drug Administration (FDA) Center of Excellence in Digital Health observes that “digital tools are giving providers a more holistic view of patient health through access to data and giving patients more control over their health … [offering] real opportunities to improve medical outcomes and enhance efficiency.” That said, the broad implementation
of electronic health records (EHRs) has yielded beneficial enhancements for care coordination and transparency, even as it has introduced new challenges for clinicians with respect to workflow, efficiency, and administrative burden. The ability to integrate data between EHRs and newer technologies (from smart watches to disease monitoring devices) is as overwhelming as it is exhilarating for those at the front lines of health care.
Potential applications of precision medicine, fueled by “omics” and clinical data and guided by artificial intelligence and machine learning technologies, could eventually offer a more promising treatment journey for patients with cancer, cardiovascular disease, and many other common and rare conditions. The promise of “P4” medicine that is “predictive, personalized, preventive, and participatory” has galvanized researchers, policy makers, patients, clinicians, and other stakeholders (Hood et al., 2012). Technology also offers the ability to engage people and connect them based on affinities—including the shared illness experience. This is evident in the rise of communities such as Patients Like Me, My Health Teams, and other digitally enabled patient groups hosted on social media platforms. Digital technologies support self-management, biohacking, adverse event reporting, and research processes, such as recruitment, symptom reporting, and adverse event monitoring. The rise of the COVID-19 pandemic has sparked new conversations about how digital technology could support not only tectonic shifts in health care toward virtual medicine but also decentralized clinical trials and more efficient research overall.
Illustrative Data Points
- From 2019 to 2020 (specifically, Surveillance Week 13), telehealth visits increased 154%, while emergency department (ED) visits underwent a marked decline over the same period (Koonin et al., 2020).
- More than 50% of individuals are able to access at least some of their own health information electronically (HealthIT.gov, 2018).
- Hospitals’ engagement in interoperability improved by more than 50% in eight major U.S. cities since 2015 (Pylypchuk and Johnson, 2020).
- As of 2017, 94% of hospitals used their EHR data to perform hospital processes that inform clinical practice. EHR data are most commonly used by hospitals to support quality improvement (82%), monitor patient safety (81%), and measure organizational performance (77%) (Parasrampuria and Henry, 2019).
- The cost of sequencing the human genome decreased dramatically in less than 2 decades, from $100 million in 2001 to $1,000 in 2015.
- The National Institutes of Health (NIH) All of Us Research Program is a cornerstone of U.S. precision medicine research, a $1.5 billion initiative with more than 270,000 total participants enrolled as of December 2020 (NIH, 2020).
Emerging Trends and Dynamics That Shape Technologies in Health and Health Care
The COVID-19 pandemic obliged new thinking about health care delivery and unleashed creativity with respect to data-driven medicine. The motivation for rapid learning about the presentation and manifestations of the coronavirus led to rapid development and uptake of online symptom screeners and surveillance trackers and removed long-standing resistance to virtual medicine. Electronic health record data have also shown concerning trends related to the pandemic, namely the reduced use of preventive services, avoidance of needed chronic illness care, and reluctance to seek care for emergent symptoms. Another downside to this growing digital/social media ecosystem is proliferative misinformation about the virus itself and vaccines.
Technology tools also—ironically—illuminate the persisting digital divide. Broadband internet access is still unevenly distributed, as is health care itself. Although data are patchy, distressing trends in COVID-19 severity and vaccine distribution serve as a helpful use case for the varied applications of technology in health care and could help target care or resources where they are lacking. On the consumer level, “apps” and devices that support wellness, care delivery, and disease management are a growing category, underscored by investments in digital health, nearly doubling from $7.4 billion in 2019, to $14.1 billion in 2020 (DeSilva and Zweig, 2021).
Effects on Patients Along the Continuum of Their Health/Health Care Experience
Notwithstanding immense technologic advances, the health care system still maintains legacy modes for storing and transmitting health data, such as fax machines and CDs—modes that have been modernized in almost every other facet of contemporary society. Consequently, stakeholders are innovating around the edges, creating resources (data models, standards, and application program interfaces [APIs]) that enable interoperability and data liquidity. As health records are becoming increasingly digitized, tools that support digital exchange are paramount, especially for patients’ experiences in screening, diagnosis, and treatment. Each of these elements of the care continuum can involve multiple clinicians or systems and demands seamless coordination, fueled by reliable data and connectivity. Technical challenges for clinicians and systems include managing the volume, quality, provenance, and availability of person-generated health data (Cortez et al., 2018). Empowered patient advocates, especially those contending
with complex chronic illnesses or rare conditions, are vocal about the need for technology-enabled care—often taking to social media to push for modernization, interoperability, and inclusivity.
With respect to prevention and health behavior, technology can serve as a potential adjunct. Wearable devices and mobile apps have been developed to support a range of fitness and wellness activities, including exercise, sleep, nutrition, medication tracking, mindfulness, and tobacco cessation, among others. Many of these embed accountability and motivation tools to encourage lasting behavior change. The COVID-19 pandemic led to an attendant surge of interest in fitness and exercise apps, with a 47% year-over-year increase in downloads globally from Q2 2019 to Q2 2020 (Chapple, 2020). Lower-tech interventions, such as text-based behavioral supports (e.g., Text4Baby and SmokeFreeTXT), have shown promise with respect to engagement, reaching underserved populations, and rates of uptake. However, research on efficacy and effectiveness of technology to improve health and health care has not kept pace with the explosive growth of various digital and mobile health technologies, nor has the current evidence sufficiently explored differences by demographic subgroups.
The impact of technology on quality of life is decidedly mixed. Numerous reports cite deleterious effects of social media and gaming on adolescent mental health, including increased depression and anxiety and poorer sleep (Hoge et al., 2017; Riehm et al., 2019). Potential upsides for technology include decreased isolation and loneliness, particularly for older adults with limited in-person social support. Social media platforms are relatively recent, with Facebook and Twitter launching in 2004 and 2006, respectively. Hence, further examination of how personal characteristics intersect with use of digital technologies and social media tools, and the contribution of these technologies to health outcomes, quality of life, and general well-being warrants consideration.
Finally, the era of precision medicine has the potential to affect the entire care continuum. The opportunity to blend systems biology with machine learning offers tremendous promise for improving health and health care, while prompting complex questions about the “expected value of individualized care” (Basu et al., 2015). The heterogeneity of payment and delivery models in the United States suggests that applications of precision medicine discoveries may be equally heterogeneous. Significant research and investments in precision oncology, exemplified by targeted approaches to cancer prevention, diagnosis, and treatment, serve as a harbinger of opportunities in other clinical domains. Hence, understanding the value and equitable diffusion of precision medicine will only grow in importance as new discoveries are made.
Effects of Technologies on Discovery, Research, and Innovation
Emerging technologies—especially with regard to digital health infrastructure and data—are core utilities for transformative health, health care, and biomedical science and progress. If accessed consistently and used effectively, these technologies can help organizations engage in swift, available, and reliable health information sharing that delivers the right information to the right decision point, at the right time, for the best result according to patients’ preferences. Tailoring and utilizing technology to apply this potential to the research industry layers a compounding effect of discovery atop the continuous learning promised. By leveraging electronic data sharing and a myriad of emerging digital tools, insights that have traditionally been out of reach for health care are possible, at a speed and quality that has yet to be experienced (OCTO, 2018). Determining best practices for using these tools, with a keen eye toward equity and health disparities, is expected to be a central priority on the horizon of American health and health care.
Related Initiatives
The potential of emerging technologies in advancing health and health care is evident—a fact that is both recognized and engaged by multiple stakeholders. Many of the efforts herein surround data governance and interoperability, with research networks such as PCORnet® as well as academic institutions, and individual state-level health information exchanges working to advance large-scale data collection, stewardship, and sharing. The federal government is also involved in this regard, with entities such as the Department of Health and Human Services (HHS), The Office of the National Coordinator for Health IT (ONC), and FDA working to advance the capabilities of digital health and data sharing to improve health system capacity and research functionality.
The private sector is also a key player in the technology sphere, with companies such as Microsoft, Google, Apple, and others building and improving tools that advance telehealth, remote patient monitoring, and artificial intelligence in health care. Partnerships between academic researchers, biotechnology/pharmaceutical companies, and technology companies are accelerating the ability to analyze exabytes of structured and unstructured data, which can unlock the true promise of precision health. This work, and the related attention that is given to patient-facing interfaces, population health, and lifestyle management, is a hallmark of innovation to come. Health systems are also building collaborative approaches to using health data to study, predict, and improve health outcomes. Building on
these efforts—especially with regard to equity—and collaborating with stakeholders to use this full spectrum of tools effectively will be critical to the next phase in the evolution of health and health care.
Compelling Questions: What Must We Address in the Years Ahead?
Given the enormity of the technologies space, engagement by all stakeholders is imperative for identifying and prioritizing questions that must be addressed in the years ahead. Along with developing and leveraging new technologies, a corollary aspect is to examine intended and unintended consequences as these technologies diffuse at scale. The following are some key questions:
- How might we advance data sharing in a way that takes advantage of progress made during a global health crisis?
- How can predictive and personalized interventions be deployed most effectively and with a clear focus on equity, given the current configuration of U.S. health care?
- In what ways could technology be leveraged to accelerate evidence generation and mobilization in practice?
- How can virtual care models be optimized and integrated with traditional care delivery, and what are the ways in which virtual care can be tailored to patients’ preferences and needs?
- What knowledge gaps must be addressed related to behavioral, attitudinal, and other psychosocial aspects that affect how patients/caregivers might regard precision medicine?
PCORI PRIORITIES ON THE HEALTH HORIZON MEETING—SOCIAL AND ENVIRONMENTAL FACTORS TOPIC BRIEF
Definition and Key Components
Health is influenced by numerous biological, demographic, environmental, and socioeconomic aspects, many of which are interdependent. Taken together, these aspects can contribute to a more equitable experience of health—or health care—for individuals and populations. Health equity concerns itself with two steps: (1) reducing inequities between people with higher socioeconomic status and people with lower socioeconomic status and (2) meeting the absolute goal of health and well-being for all. By achieving health equity, societies have the opportunity to experience enhanced overall outcomes along with long-term socioeconomic prosperity. Achieving a more equitable society is also a noble goal in and of itself (Canning and Bowser, 2010). Today, the concepts, definitions, approaches, and frameworks underpinning social determinants and attaining health equity are passionately discussed and debated (Equity in health care: a debate, 2008). Moreover, whether the extent to which resources or conditions that help a person meet daily needs is deterministic is also the subject of deliberation. Accounting for past, present, and emerging discussions on health, development, and equity, a report from the Pan American Health Organization (PAHO), Just Societies: Health Equity and Dignified Lives, examines health equity through the lens of structural social, environmental, economic, and political issues and movements (see Figure 1).
Owing to their intersecting nature, components of social and environmental factors of health cannot be defined succinctly. Thus, the key components—a life-course approach to health, environmental factors, and social factors within the care continuum—will be defined and examined separately.
Background and Current Profile for Each Component
A Life Course Approach to Health
Inequities in health begin throughout someone’s life course, starting from before birth and affecting an individual through older age. Disparities typically affect people across various identities, such as race, geographic location, sexual orientation, gender identity, occupation, or disabilities. Knowledge gaps persist that relate to key points in the life course to use prevention or intervention efforts in settings such as schools, workplaces, or long-term care facilities.
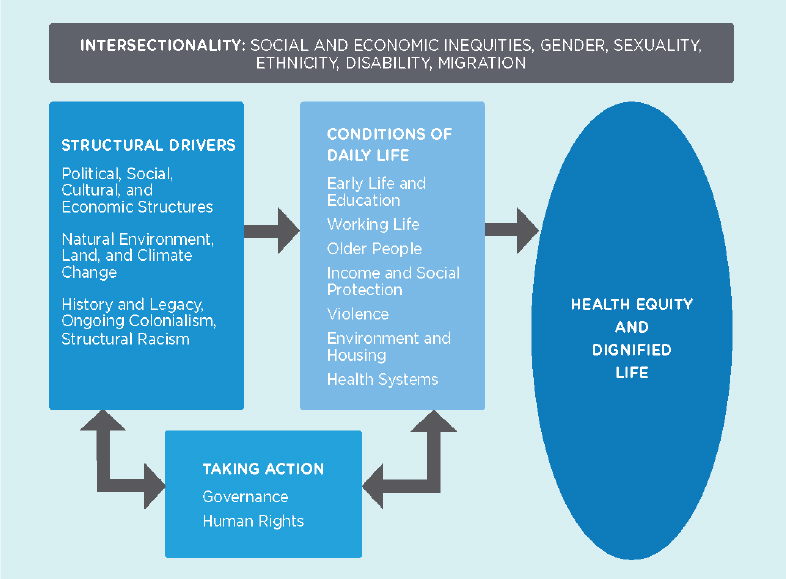
SOURCE: Commission of the Pan American Health Organization on Equity and Health Inequalities in the Americas. 2019. Just societies: Health equity and dignified lives. Report of the Commission of the Pan American Health Organization on Equity and Health Inequalities in the Americas. Washington, DC: Pan American Health Organization.
The life course approach to social and environmental determinants also concerns itself with the impact of exposures to risk factors that worsen socioeconomic and health outcomes throughout a person’s life (Bezruchka, 2010). Exposures include various factors such as environment, education, housing and shelter, food, and access to public services and health care, all of which can impact health throughout the life course (see Figure 2). When accumulated throughout the life course, these exposures can accrete as biological stressors and manifest in older age as worse health outcomes: chronic disease, reduced functional ability, and intrinsic capacity. The disparity in the impact of exposures across the life course can lead to additional gaps between different demographic groups in the United States, with many examples pointed out in the form of life outcomes such as educational attainment, incarceration rates, housing policies, and income, and health outcomes such as developmental disorders, obesity, heart disease, and cancer (NASEM, 2017).

SOURCE: Davies, S. C. 2012. Annual Report of the chief medical officer, volume one, 2011, on the state of the public’s health. London, UK: Department of Health.
The Environment and Human Health
WHO defines environmental health as all the “physical, chemical, and biological factors external to a person, and all the related behaviors.” Environmental health consists of preventing and controlling morbidity and mortality resulting from interactions between people and their environment. The following are several key sources of negative environmental exposures.
- OUTDOOR AIR QUALITY: Poorer air quality is linked to higher morbidity and mortality from chronic diseases such as cancer and cardiopulmonary disease. High levels of unhealthy air emissions still exist for around 127 million Americans (ODPHP, 2020). Exposure to fine particulate matter, ozone, and nitrogen dioxide increases the incidence and burden of disease. In addition to these factors, inequities in location and place affect human health (Environmental Health Sciences Center, 2021).
- SURFACE AND GROUND WATER QUALITY: Contamination by infectious agents, chemicals, and heavy metals can result in highly detrimental health impacts, such as the 2014–2019 Flint water crisis, which saw the drinking water for the city of Flint, Michigan contaminated with lead, Legionnaire’s disease, coliform bacteria, and trihalomethanes (Ruckart et al., 2019).
- TOXIC SUBSTANCES AND HAZARDOUS WASTES: Exposures to toxic substances such as pesticides and herbicides, paints, aerosols, cleaning products, fertilizers, and gasses, are wide and mostly unknown.
- HOMES AND COMMUNITIES: A variety of indoor pollutants, such as indoor air pollution; inadequate heating, cooling, and sanitation; structural safety; electrical and fire hazards; and lead-based paint hazards, can affect health and safety.
- PLACE AND GEOGRAPHIC LOCATION: Geographic location in a marginalized or rural area can reduce physical access to health-promoting amenities such as health care facilities, parks, and supermarkets, and the means to access these facilities, such as public transport (Cushing et al., 2015; Hilmers et al., 2012).
Communities of color tend to live in environments with poorer air quality. High exposure to negative environmental exposures results in increased deaths from COVID-19, with case mortality rates and case fatality rates estimated between 11.3 percent and 16.2 percent. Cross-cutting disparities based on race and ethnicity have been observed with exposure to environmental hazards, poorer-quality and unsafe infrastructure, and fewer health-promoting environmental amenities such as parks (Hilmers et al., 2012).
Social Factors Within the Care Continuum
The social determinants of health manifest throughout health care and population health systems, from prevention to late-life care experiences.
- ACCESS TO CARE: Marginalized populations experience decreased access to social protection, insurance, and health care due to disparities in economic opportunities and other factors such as structural racism and implicit bias. Several factors have been cited, but are not limited to, lower incomes, living in a U.S. state without Medicaid expansion under the Patient Protection and Affordable Care Act, and living in a rural area. However, access to care does not always guarantee the quality of care. While disparities in long-term care facility access exist, research highlights that the wide gap in these facilities’ quality is a larger issue (Barton Smith et al., 2008).
- INEQUITIES IN PATIENT EXPERIENCES: Pervasive and troubling disparities in patient experiences and outcomes are also related to implicit racial bias from care providers and their impacts on patients. False beliefs about Black people’s ability to bear pain have led to disparities in prescribing medications and even life-saving interventions for Black patients (Hoffman et al., 2016).
- WORKFORCE DIVERSITY AND INCLUSION: Tied to implicit racial bias in the workforce are inequities in the demographics of the health care workforce. Nearly 62% of physicians and surgeons are male. White people constitute about 65% of the workforce, with Black people representing approximately only 5.6% of the workforce, far below the 11.6% share of the total U.S. population they constitute (DataUSA, n.d.). Importantly, concordance of physicians and patients has been shown to affect utilization and costs, an area that warrants additional research (Jetty et al., 2021).
Emerging Trends and Dynamics
The Cumulative Social Impact of Exposures Across the Life-Course
The cumulative impacts of health inequities have translated into a decreasing life expectancy in the United States from 2016 to 2019. Life expectancy is expected to decrease in 2020 in light of the severe impact of the COVID-19 pandemic in the United States on Black and Latino populations, which recorded reductions in life expectancy at birth of 2.10 and 3.05 years (Andrasfay and Goldman, 2021). Key statistics across the life course include, but are not limited to, the following from each stage of life:
- PRENATAL: Before birth, Black and African American women are nearly three times as likely to die of complications related to pregnancy and childbirth than White women, a gap that has not narrowed (Lu, 2018). The same report attributes this phenomenon’s causes to poorer health across the life course and disparities in access, safety, and maternal care quality.
- INFANCY: The infant mortality for Native Americans is 1.5 times the rate of White people. While White people experienced decreased infant mortality between 1990 and 2009, Native Americans did not (NASEM, 2017). A factor commonly cited for this occurrence is the historical forced displacement and mistreatment of Native American communities, people, and culture.
- CHILDHOOD: In 2017, 12.6% of Black and African American children had asthma compared with 7.7 percent of non-Hispanic White children (Carratala and Maxwell, 2020). The causes of this phenomenon are unclear, but children living below the poverty line or exposed to secondhand tobacco smoke have higher rates of asthma (OMH, 2021a).
- ADOLESCENCE: The number of suicide attempts by Hispanic females was 40% higher than that of adolescent non-Hispanic White females (Carratala and Maxwell, 2020). The poverty level has been attributed to causing reported psychological distress (OMH, 2021b).
- ADULTHOOD: Black and African Americans were 30% more likely than White people to die prematurely from heart disease in 2010 and twice as likely to die prematurely from a stroke (NASEM, 2017). This statistic demonstrates the compounding effect of severe impacts of exposure to negative social and environmental determinants.
- OLDER AGE: The odds of frailty among non-Hispanic Black and Hispanic older adults were approximately 1.5 times that of older White adults in 2020 (Bandeen-Roche et al., n.d.). Here we observe the reinforced impact of cumulative exposures to negative social and environmental determinants.
Emerging research has also identified several factors causing decreases in life expectancy of White working-class populations without college degrees across their life course, as illustrated in the study by Deaton and Case in their seminal paper on “deaths of despair” (Case and Deaton, 2015). Collectively, these disparities can be attributed to several factors, including societal issues such as environmental pollution, unequal economic systems, and structural racism; to health systems and delivery issues such as the high access and cost barriers to primary and specialty care; and insufficient social protection and insurance coverage. However, more research is needed to assess the impact of factors on individuals, communities, and populations throughout the life course. Additionally, the research priorities could also describe the actions and efforts required to embed the connection between health and well-being at every life stage and the social, environmental, and health systems–related factors needed to enable this future (WHO, n.d.).
Impacts of Environmental Health
Environmental health is closely interrelated with the cumulative impacts of determinants across the life course. Despite this relationship, the compounding interaction between negative exposures can worsen without actions to address the environment.
Compelling Questions: What Must We Address in the Years Ahead?
The following list is intended to provoke contemplation of key knowledge gaps and unanswered questions related to social and environmental factors affecting health and health care.
Gaps in Research and Efforts
- Where are the knowledge gaps with interventions to tackle social and environmental factors that influence health equity? Can these gaps be tackled using a life course approach or at particular points in the care and public health system and continuum?
- While evaluating the multiple actions and efforts mobilized to improve health and well-being and reduce health equity, what populations, people, and communities have not been included or involved?
- How can the research ecosystem, from the workforce to grants and funding, be streamlined to promote comprehensive health equity research? Who are the critical partners from other sectors, including justice, education, and public policy, to engage in new research efforts?
Emerging Trends and Optimization
- How can learning health systems more quickly and effectively anticipate trends, guiding principles, and improvements and better focus interventions, prevention, and health promotion efforts?
- What are the most promising trends, innovations, and movements that will promote and maintain health equity?
- Where are investments needed to cultivate research and action on emerging issues in health equity in its next decade?
Toward the Future
- What actions are needed to translate evidence into actions, policies, and interventions that change systems and organizations to improve people’s health and well-being?
- Looking toward the future and examining previous experiences in the field, what does a vision of health equity look like across societies and care systems? What action is needed to realize this vision?
- How can key national entities/agencies align their efforts and strategic priorities to reduce health inequities?
Related Initiatives
Numerous organizations have redoubled and redirected their attention toward racism, bias, injustice, and health equity. Increasingly, health equity is a cross-
cutting issue guiding the strategic priorities for many public and private entities. Addressing disparities can encompass data sharing, data justice, data ownership, pandemic preparedness and response, environmental and occupational health, and aging and longevity. Further research is needed to discern and target efforts to help historically excluded communities and identities, including but not limited to racial and ethnic populations, people in rural locations, those with low incomes or low socioeconomic status, people with disabilities, people from the LGBTQ+ community, and those with limited English language proficiency. Meaningfully engaging and including these people and communities and advocating for their unique needs will assure concerted focus and maximize potential opportunities for improvement and transformation.
PCORI PRIORITIES ON THE HEALTH HORIZON MEETING—VALUE OPTIMIZATION TOPIC BRIEF
Definition and Key Components
Regarding health and health care, addressing value entails transforming the relationship between health improvement and economic investment. In this sense, optimizing value necessitates maximizing positive health outcomes while minimizing the costs associated with achieving those outcomes, notably via research and service provision. Because the concepts of “health” and “economic investment” can take on different meanings across the care continuum and between various stakeholder groups, “value” and the requisite actions needed to optimize it can vary across domains. Examining value within these contexts and determining its significance as a strategic issue are critical to improving and transforming health care.
Background and Current Profile
Even though the United States spends twice as much per capita on medical services as any other developed nation—and 50% more than the second-highest-spending nation—its health performance ranks below the top two dozen among the community of all nations. This is broadly attributed to financial incentives and system fragmentation that promote volume over value, resulting in unneeded services, inefficient care delivery, high prices, excessive administrative costs, and missed prevention opportunities.
Public mistrust of the U.S. health care system—particularly surrounding profit motives—further challenges conversations about value. Inadequate transparency and low patient engagement create a dearth of public information on value, costs, and treatments, ultimately resulting in misunderstandings of value that further impede efforts to transform health and health care (Richmond et al., 2017). In 2020 and 2021, the dangers of this value gap have been illustrated starkly by the COVID-19 pandemic. The SARS-CoV-2 virus has wreaked havoc on individuals and families residing in the United States and the health system that serves them, and has exacerbated inequities. As compared with White, non-Hispanic persons, Black and African American individuals were 1.4 times as likely to contract SARS-CoV-2, 3.7 times as likely to be hospitalized for SARS-CoV-2, and 2.8 times as likely to die of SARS-CoV-2 (CDC, 2021a). This trend encompassed income disparities as well. As of February 2021, in terms of cumulative cases (per 100,000 individuals), U.S. counties with poverty rates higher than 17.3% expe-
rienced 22% more cases of SARS-CoV-2 than U.S. counties with poverty rates lower than 12.3%. In terms of cumulative deaths, this disparity is even starker; per 100,000 individuals, U.S. counties with poverty rates greater than 17.3% have experienced 50% more SARS-CoV-2 deaths than U.S. counties with poverty rates lower than 12.3% (CDC, 2021b) (see Figure 3).
The financial reckoning that accompanied these trends amplifies the need for change. Shutting down elective surgical procedures because of the pandemic dealt the health care system a deep financial blow, leading to a loss of 1.4 million health care jobs in the month of April 2020 and triggering calls for additional emergency funding for hospitals. The American Hospital Association estimated that U.S. hospitals and health systems experienced a $200 billion shortfall over a 4-month period through June, with most of the lost revenue caused by canceled or postponed elective procedures. Owing to decreased patient volume, an additional $120 billion in hospital financial losses were estimated from July to December 2020. Primary care practices have fared even worse, with 30% to 50% of practices either closing or being unsure of their continued operation. The fragility of our health care system has never been on such clear display, and the need for practice and payment reform has never been greater.
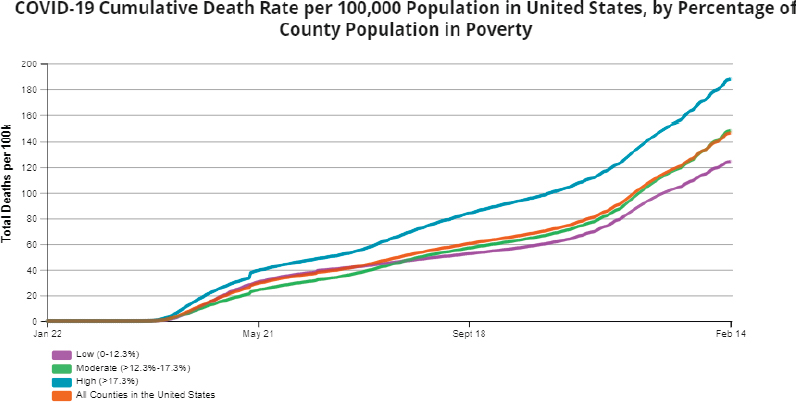
SOURCE: https://covid.cdc.gov/covid-data-tracker/?ACSTrackingID=USCDC_2067-DM45255&ACSTrackingLabel=Winter%20Holidays%20%7C%20COVID-19&deliveryName=USCDC_2067-DM45255#pop-factors_totaldeaths (accessed April 30, 2021).
Key Figures
IN TERMS OF THE NEED FOR A VALUE-ORIENTED SHIFT:
- As a proportion of gross domestic product (GDP), U.S. health care expenditures have consistently been greater than those of any other Organisation for Economic Co-operation and Development (OECD) country. In 2018, this accounted for 16.9% of the U.S. GDP (approximately $3.5 trillion) (BEA, 2019). Despite this, the United States has experienced the lowest life expectancy of any OECD country since 1992 (Tikkanen and Abrams, 2020).
- In 2015, a bypass surgery procedure in the United States cost $78,318. In the same year, Xarelto, a drug commonly used to prevent blood clots, cost $292. In both cases, U.S. pricing far exceeded that of its peers (FHCQ, 2020).
- Medical bankruptcy and financial toxicity have entered the lexicon in the last decade. As an example, research has found that people diagnosed with cancer are 2.5 times more likely to declare bankruptcy (Ramsey et al., 2013).
IN TERMS OF THE POTENTIAL THAT A SHIFT TO VALUE COULD ENTAIL:
- If properly applied, high-value services are projected to reduce negative health outcomes by 40% to 90%, and reduce spending by 20% to 50% (Health Rosetta, 2020).
- In addition to providing more than $1 billion in net savings, Maryland’s evolving approach to value-based care led to a 44% decline in potentially preventable complications between 2014 and 2016 (Maryland Department of Health, 2018; Smith, 2021).
- In 2019, accountable care organizations generated $1.19 billion in total net savings to Medicare and achieved new program savings 3 years in a row (Verma, 2020).
- In terms of both patient care and financial resiliency, value-based models have proven to be exceptionally resilient to the effects of the COVID-19 pandemic (Feeley, 2021).
IN TERMS OF CURRENT TRENDS AND DRIVERS IN THE SPHERE OF VALUE:
- With a cumulative $20 billion in funding, the Centers for Medicare & Medicaid Services (CMS) Innovation Center has launched 54 models aimed at moving the U.S. health care system toward value (OCTO, 2018).
- Value-based services account for approximately 40% of Medicare fee-for-service payments, 30% of commercial payments, and 25% of Medicaid payments (OCTO, 2018).
- In the first year of the value-driven Quality Payment Program (initiated by the Medicare Access and CHIP Reauthorization Act [MACRA] in 2015), 95% of eligible clinicians participated in a Merit-Based Incentive Payment System (HealthIT.gov, n.d.)
- The CMS Primary Care Initiative is estimated to provide better alignment for more than 25% of Medicare fee-for-service beneficiaries (NASEM, 2017)
Emerging Trends and Dynamics That Shape Value in Health and Health Care
Intentional and informed patient-centered value optimization holds significant potential in incentivizing research and services that yield tremendous value for patients, families, and providers across the health and health care industry (see Figure 4). Instead of simply encouraging service provision, a movement toward value should function to drive work that creates positive health outcomes, causing research and services that align with value to become common practice throughout the care continuum (Chernew et al., 2007).
Within this movement, a distinct focus on equity and engagement is both necessary and beneficial. By working with patients to build mutual understandings surrounding “value,” the health system can catalyze both demand and momentum for services that are responsive to patient needs surrounding equity, efficiency, effectiveness, and continuous learning at every moment in care (Community Catalyst, 2021). Doing so with an especial focus toward equity will help advance a future in which, regardless of race or income, all individuals can fully realize their health-related goals.
Value optimization holds potential for discovery, innovation, and research. In aligning incentives with optimal health outcomes, value-centric health system models are natural drivers of continuous learning. The constant pursuit of value—as a multidimensional, individually dependent concept—will necessitate constant innovation in health system infrastructure, delivery practices, patient engagement, and interventions regarding population health. Likewise, in accruing both positive health outcomes and financial gains, success in a value-optimized system requires patient-centricity and constant improvement with regard to best practice (IOM, 2015).

SOURCE: NEJM Catalyst. 2017. What Is Value-Based Healthcare? https://catalyst.nejm.org/doi/full/10.1056/CAT.17.0558 (accessed October 20, 2021).
Related/Supporting Initiatives
Multiple programs from states, providers, payers, and educational institutions are advancing a shift toward value. A selection of programs is listed in Box 4.
Compelling Questions: What Must We Address in the Years Ahead?
Optimizing value in health care has never been more timely or important, and identifying key questions to better understand the pathways to value optimization is a needed conversation across all stakeholders in health and health care. The COVID-19 pandemic further illuminated the necessity of optimizing value by revealing both flaws and opportunities in current care delivery models. In a value-centric conception of health and health care, the United States can also begin the long process of remediating health disparities—but refinement through patient-centered research will likely be essential to this process. Critical questions to address include the following:
- In what ways does the current health and health care system exemplify and defy value for different stakeholders across the care continuum?
- What would a “value-optimized health and health care system” look like to different stakeholders across the care continuum?
- In pursuing value optimization, how would relevant initiatives balance patient-centered outcomes and economic efficiency?
- What would it take to achieve patient-centered value optimization?
PCORI PRIORITIES ON THE HEALTH HORIZON MEETING—INFRASTRUCTURE TOPIC BRIEF
Definition and Key Components
Infrastructure is defined as the foundational organizational and structural elements that enable society to function. In the context of health and health care, the cornerstone elements of infrastructure include the diverse systems and settings where care occurs, data generated by individuals and populations, the health care workforce, and the ability to use information to inform and improve outcomes. Infrastructure is also the backbone of connectivity, enabling individuals and communities to engage with one another and to use information in their daily lives. Infrastructure as a whole is complex—both composed of and influenced by myriad elements. And these elements must function seamlessly to yield better health for all. This topic brief explores the current state of health and health care infrastructure, including its role in engaging people in their health, the dynamics inherent in moving scientific evidence into practice, and the emergent trends and opportunities.
Background and Current Profile
The twin forces of the COVID-19 pandemic and rising awareness of ubiquitous, long-standing health disparities have sharpened focus on deficiencies of the U.S. health care infrastructure as one that is brittle, fragmented, and unevenly distributed. Among other challenges, the pandemic illuminated key shortcomings in the public health infrastructure, not only in the ability to rapidly exchange data and information to track cases and optimize care but also in the ability to efficiently implement effective treatments and COVID-19 vaccines. Early in the pandemic, numerous reports showed that COVID-19 disproportionately affected Black and Brown communities with respect to both incidence and severity (Abbasi, 2020; Azar et al., 2020). Conversations about these disparities have shown how structural racism permeates health care, including its delivery and the use of health data to guide person-centered decisions (Egede and Walker, 2020). An additional consequence of the pandemic is its toll on health care workers. Burnout and primary care shortages, already commonplace, have only accelerated in the last year (Bodenheimer and Sinsky, 2014; NASEM, 2019). A September 2020 survey showed that 64% were experiencing burnout, with the pandemic as a primary driver of increased stress (Frellick, 2020). Lastly, while biomedical research is robust and generative, with thousands of rigorous peer-reviewed articles produced annually, leveraging this evi-
dence at the point of care is an uneven proposition, whether in academic medical systems, small primary care practices, or safety net care settings. Investments in our health care infrastructure have never been more urgent or necessary.
Illustrative Data Points
- As a proportion of the GDP, U.S. health care expenditures have consistently been above those of any other OECD country. In 2018, this accounted for 16.9% of U.S. GDP (~$3.5 trillion), yet the United States has experienced the lowest life expectancy of any OECD country since 1992 (BEA, 2019; Tikkanen and Abrams, 2020).
- Clinician burnout increased by 9% in the period from 2011 to 2014 and has been exacerbated by the COVID-19 pandemic (NAM, 2021).
- Deaths attributed to COVID-19 are 1.1 to 2.8 times higher in people of color (CDC, 2021a).
- Generational shifts will affect site of care. Surveys show that 71% of millennials prefer to schedule appointments, access medical records, and receive appointment reminders via apps. A recent RAND study also showed that the 18 to 44 years age group also accounted for 43% of visits to retail clinics (RAND, 2016).
- Data from the 2003 National Assessment of Adult Literacy show that low health literacy affects approximately 36% of U.S. adults. Only 12% demonstrated proficient health literacy (Kutner et al., 2006).
- Implementation science, a burgeoning but new field, aims to close the gap between research and care by understanding tools, context, and other factors that promote uptake and integration of evidence-based practice. Since 2007, the annual Science of Dissemination and Implementation Conference has grown from a few hundred to 1,500 attendees (Glasgow et al., 2012).
- Local health departments have lost 21% of their operating capacity since 2008. Staffing shortages and uneven resources hindered the COVID-19 pandemic response, from data exchange to contact tracing (NACCHO, 2019).
Emerging Trends and Dynamics That Shape Health-Related Infrastructure
Multiple interdependent forces influence and shape the infrastructure for health and health care. Clinical encounters generate data points, and the aspiration of a learning health system is predicated on effective use of this clinical data for continuous improvement (IOM, 2010). However, the fragmented structure of U.S. health care means that data are collected, analyzed, and reapplied for
improving care inconsistently—if at all. Since health is a continuous, longitudinal experience, unconfined to a brief clinical encounter, data generated outside the encounter—via social media, wearable devices, or geolocation information—are important potential complements to data contained in electronic medical records. Often, these sources of data are siloed and underutilized in clinician–patient interactions, hence this potential remains largely untapped. Data aggregation and governance are corollary issues that could revolutionize care, if remedied.
Many large technology companies are making inroads into health care, recognizing the size of this market and the valuable information it holds about individuals’ behaviors, habits, and preferences. Digital health and “retail medicine” are fast-growing sectors of the health care ecosystem. From creating brick-and-mortar primary care clinics to purchasing virtual care providers, the lines between nontraditional companies (i.e., large technology companies) and health care systems are blurring gradually.
Since people are increasingly responsible for more of their health care expenses, there is a slow but growing shift in perceptions about quality, cost, and experience. Today’s consumers expect convenience, speed, personalization, and access for many facets of their day-to-day life, from buying groceries and airline tickets to entertainment and banking. This expectation has helped foster a drive for more convenient care. Yet, the data component of this infrastructure lags. A simple transaction at a retail pharmacy, such as a flu shot or blood pressure reading, or patient-generated health data from devices, wearables, and monitors, are unlikely to be seamlessly integrated into the medical record held by their clinician. The likely result may be duplicative or missing information about a person’s complete health experience. A related facet of the health care consumerism movement is growth in direct-to-consumer advertising since FDA relaxed prescription drug advertising regulations in 1997, propagating a “quick fix” mindset and a medicalization of formerly ordinary symptoms. Clinicians may be ill-equipped to counsel their patients on underlying evidence about a given treatment owing to time and resource constraints.
Hence, despite substantial accumulations to the evidence base for many acute and chronic conditions, implementation of best-available evidence at the point of care varies widely based on factors such as the clinical topic, provider characteristics, and adaptability of the care delivery setting (Tricoci et al., 2009). Change management in health care is a cottage industry in itself, offering frameworks and models to support change and explain variation (Damschroder et al., 2009; Wagner et al., 1996). But the vast complexity of care delivery and range of permutations of contemporary medicine challenge the agility of even the highest-performing systems. The COVID-19 pandemic illustrated the essential need for
real-time data to drive understanding of care, with many clinicians turning to social media to share insights and inquiries, lacking a more robust information exchange capability. Importantly, the issues of data access for improving care are equally essential in the research context.
Infrastructure, refracted through the prism of data, access to high-performing health systems, and application of evidence could reduce or exacerbate health disparities depending on how society responds. Moral and ethical ramifications of this uneven infrastructure, and the imperative to create an equitable infrastructure, are further magnified when looking at effects on health care workers. A shortage of trained personnel hinders the ability to address patients’ social needs (housing, food, and safety), which are inextricably linked to quality of life. Increased attention to and investment in community supports as a complement to clinical care could alleviate some of the pressure on the health care workforce and attenuate the deleterious effects of unmet social needs.
Effect of Infrastructure on Health and Health Care Experience
Research literature and patients’ own accounts paint a picture of how many health care systems fall short of optimum with respect to preventive care, screening and diagnosis, treatment, and overall quality of life. How do the previously mentioned infrastructure elements contribute to variable health and health care? The following examples show how differences and deficits in U.S. health care infrastructure contribute to suboptimal outcomes and, in many cases, worsen health disparities:
- PREVENTION: based on the beneficial impact of the National Diabetes Prevention Program in clinical trials, the Centers for Disease Control and Prevention (CDC) provided funding to widely disseminate it through community partnerships. However, a recent study of the implementation of the program found uneven access to it in urban versus rural counties (Ariel-Donges et al., 2020). Rural health disparities persist for other preventable conditions. In some cases, these could be mitigated by web- or video-based approaches to care and health education. Yet, reliable broadband access is another infrastructure issue that is a prerequisite to delivering virtual preventive services.
- SCREENING AND DIAGNOSIS: The COVID-19 pandemic magnified deficiencies of the public health and health care infrastructure. Backbone capabilities such as delivery of reliable communication, venues for rapid screening, availability of testing materials, variable laboratory capacity, and demands on the work force, combined to exacerbate surges in COVID-19
- TREATMENT: Given the complexity of cancer treatment, it is imperative to have reliable evidence at the point of care and access to the treatment itself. Research on new treatments is proliferating, including gene sequencing, immunologic therapies, and biomarker-driven treatment decisions. However, the cancer clinical trial infrastructure has long been a topic of concern, given its low accrual (especially of representative populations) and participant burden. Additional structural challenges include availability of skilled surgeons and oncologists and marshaling the unstructured real-world clinical data from disconnected care systems.
- QUALITY OF LIFE: Infrastructure has a compelling impact on quality of life, influencing conditions in which people live, work, learn, and engage with their communities. Access to clean water, transportation, stable housing, public safety, and healthful food are well-studied drivers of health outcomes at the individual and population level. Recent examples include the Flint, Michigan, water crisis, collapse of major interstates and bridges, and illustrations of “food deserts” that are associated with adverse outcomes.
diagnoses in the United States relative to other countries. Factors, including occupation, living arrangements, and transportation access, have contributed to the disproportionate impact of COVID-19 on communities of color.
Effect of Infrastructure on Discovery, Research, and Innovation
Given the heterogeneity of U.S. health care, opportunities for experimentation and innovation abound, as exemplified by new primary and virtual care models, and new data aggregation and sharing ventures by health systems and payers. Approaches to operationalizing the learning health system are accelerating in health systems and academic medical centers (Allen et al., 2021). In the patient/consumer space, recognition of the importance of community as an adjunct to clinical care has sparked new programs to connect individuals to resources that address basic social needs (food, shelter, safety, and transportation). However, despite exhortations to address critical workforce shortages, proposed solutions have had less traction. Rethinking scope of practice, licensure, and interstate regulations and further invigorating science, technology, engineering, and mathematics (STEM) programs in schools are opportunities in medical education that have not yet been fully exploited.
Related Initiatives and Connections
U.S. health care is a work in progress. Many groups are addressing current infrastructure challenges, and many have an explicit focus on reducing disparities in access and quality of care. Newer collaborative ventures, such as Truveta, that seek to leverage health data can be part of synergistic efforts to improve the health care infrastructure. The Healthcare Anchor Network is taking direct aim at the connection between the community conditions that create poor health and the hiring, purchasing, and investment decisions made by health systems. Connecting with these groups, among many other stakeholders, could have a lasting impact in the next decade. While not exhaustive, the following lists offer potential connection points.
Groups Centered on the Application of Evidence in Practice
- The Learning Health Community (grassroots endeavor to manifest a national learning health system)
- Department of Veterans Affairs’ Health System’s Quality Enhancement Research Initiative (QUERI) Programs
- AcademyHealth’s Paradigm Project
- Institute for Health Improvement’s Practical Playbook
Groups Centered on Connecting Stakeholders as a Lever for Health Care Innovation and Improvement
- Community Catalyst
- Families USA
- Network for Regional Health Improvement (now Civitas Networks for Health)
Groups Promulgating and Applying Common Data Models for Real-World Health Care Data
- Observational Medical Outcomes Partnership
- Health Catalyst
- PCORnet®
- FDA Sentinel Initiative
- Health Care Systems Research Network
Compelling Questions: What Must We Address in the Years Ahead?
Readying for another pandemic is widely viewed as an imperative in light of the impact of COVID-19. Preparedness and surveillance have been relegated, but renewed investments in data, workforce, and materiel are essential at the state and federal level. Concurrently, further study and testing of how to activate and actualize the learning health system will yield widespread benefits and ensure that biomedical research successes reap their full potential. This could have the corollary benefit of invigorating and restoring the health care workforce, in that clinicians could see the more immediate benefits of applying knowledge at the point of care. Concerted focus on the basic infrastructure needs of neighborhoods and communities can spur engagement in health and health outcomes. Finally, thoughtful attention to the emergent field of data justice, coupled with scrutiny of embedded biases in artificial intelligence, are two of many needed steps in effectively using data to mitigate health inequity. Compelling questions may include the following:
- What should/will a learning health system look like to meet the needs in the next 5 years?
- What would be necessary to mount a coordinated and accelerated response to the next major public health challenge?
- What are the most effective approaches to dissemination and implementation of evidence, given the heterogeneity of U.S. health care?
- How can the wide range of data sources be leveraged most effectively to accelerate evidence generation and translation?
REFERENCES
Abbasi, J. 2020. Taking a closer look at COVID-19, health inequities, and racism. JAMA 324(5):427–429. https://doi.org/10.1001/jama.2020.11672.
Allen, C., K. Coleman, K. Mettert, C. Lewis, E. Westbrook, and P. Lozano. 2021. A roadmap to operationalize and evaluate impact in a learning health system. Learning Health Systems 5(4). https://doi.org/10.1002/lrh2.10258.
Andrasfay, T., and N. Goldman. 2021. Reductions in 2020 US life expectancy due to COVID-19 and the disproportionate impact on the Black and Latino populations. Proceedings of the National Academy of Sciences 118(5):e201476118. https://doi.org/10.1073/pnas.2014746118.
Ariel-Donges, A. H., E. L. Gordon, B. N. Dixon, A. J. Eastman, V. Bauman, K. M. Ross, and M. G. Perri. 2020. Rural/urban disparities in access to the National Diabetes Prevention Program. Translational Behavioral Medicine 10(6):1554–1558. https://doi.org/10.1093/tbm/ibz098.
Azar, K. M., Z. Shen, R. J. Romanelli, S. H. Lockhart, K. Smits, S. Robinson, S. Brown, and A. R. Pressman. 2020. Disparities in outcomes among COVID-19 patients in a large health care system in California. Health Affairs (Millwood) 39(7):1253–1262. https://doi.org/10.1377/hlthaff.2020.00598.
Bandeen-Roche, K., S. L. Szanton, and R. J. Thorpe. n.d. Double Jeopardy for older adults of color: An Urgent Call to Address Frailty Disparities in the United States. Johns Hopkins University. https://frailtyscience.org/blog/double-jeopardy-older-adults-color-urgent-call-address-frailty-disparities-united-states (accessed October 13, 2021).
Barton Smith, D., Z. Feng, M. L. Fennell, J. Zinn, andV. Mor. 2008. Racial disparities in access to long-term care: The illusive pursuit of equity. Journal of Health Politics, Policy and Law 33(5):861–881. https://doi.org/10.1215/03616878-2008-022.
Basu, A., J. J. Carlson, and D. L. Veenstra. 2015. A framework for prioritizing research investments in precision medicine. Medical Decision Making 36(5):568–580. https://doi.org/10.1177/0272989X15610780.
BEA (Bureau of Economic Analysis). 2019. Gross domestic product, fourth quarter and annual 2018 (initial estimate). https://www.bea.gov/news/2019/initial-gross-domestic-product-4th-quarter-and-annual-2018 (accessed October 13, 2021).
Bezruchka, S. 2010. Health equity in the USA. Social Alternatives 29(2):50–56. https://depts.washington.edu/eqhlth/pages/BezruchkaUSHealthInequality10Cor.pdf (accessed October 13, 2021).
Bodenheimer, T., and C. Sinsky. 2014. From triple to quadruple aim: Care of the patient requires care of the provider. Annals of Family Medicine 12(6):573–576. https://doi.org/10.1370/afm.1713.
Canning, D., and D. Bowser. 2010. Investing in health to improve the wellbeing of the disadvantaged: Reversing the augment of the Marmot Reports. Program on the Global Demography of Aging, Harvard University. https://cdn1.sph.harvard.edu/wp-content/uploads/sites/1288/2013/10/PGDA_WP_78.pdf (accessed October 12, 2021).
Carratala, S., and C. Maxwell. 2020. Health disparities by race and ethnicity. Center for American Progress, May 7. https://www.americanprogress.org/issues/race/reports/2020/05/07/484742/health-disparities-race-ethnicity/ (accessed October 13, 2021).
Case, A., and A. Deaton. 2015. Rising morbidity and mortality in midlife among white non-Hispanic Americans in the 21st century. Proceedings of the National Academy of Sciences 112(49):15078–15083. https://doi.org/10.1073/pnas.1518393112.
CDC (Centers for Disease Control and Prevention). 2021a. Risk for COVID-19 infection, hospitalization, and death by race/ethnicity. https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html (accessed October 13, 2021).
CDC. 2021b. Trends in COVID-19 cases and deaths in the United States, by county-level population factors. https://covid.cdc.gov/covid-data-tracker/?ACSTrackingID=USCDC_2067-DM45255&ACSTrackingLabel=Winter%20Holidays%20%7C%20COVID-19&deliveryName=USCDC_2067-DM45255#pop-fact-ors_totaldeaths (accessed October 13, 2021).
Chapple, C. 2020. Health & fitness app adoption up record 47% so far in Q2 2020. SensorTower, June 4. https://sensortower.com/blog/health-and-fitness-app-record-download-growth (accessed October 12, 2021).
Chernew, M. E., A. B. Rosen, and A. M. Fendrick. 2007. Value-based insurance design. Health Affairs 26(Suppl 2):w195–w203. https://doi.org/10.1377/hlthaff.26.2.w195.
Commission of the Pan American Health Organization on Equity and Health Inequalities in the Americas. 2019. Just societies: Health equity and dignified lives. Report of the Commission of the Pan American Health Organization on Equity and Health Inequalities in the Americas. Washington, DC: Pan American Health Organization.
Community Catalyst. 2021. Valueadvocacy project. https://www.communitycatalyst.org/initiatives-and-issues/initiatives/value-advocacy-project/full-description (accessed October 13, 2021).
Cortez, A., P. Hsii, E. Mitchell, V. Riehl, and P. Smith. 2018. Conceptualizing a data infrastructure for the capture, use, and sharing of patient-generated health data in care delivery and research through 2024. The Office of the National Coordinator for
Health Information Technology. https://www.healthit.gov/sites/default/files/onc_pghd_final_white_paper.pdf (accessed October 12, 2021).
Cushing, L., J. Faust, L. M. August, R. Cendak, W. Wieland, and G. Alexeeff. 2015. Racial/Ethnic disparities in cumulative environmental health impacts in California: Evidence from a statewide environmental justice screening tool (CalEnviroScreen 1.1). American Journal of Public Health 105(11):2341–2348. https://doi.org/10.2105/AJPH.2015.302643.
Damschroder, L. J., D. C. Aron, R. E. Keith, S. R. Kirsh, J. A. Alexander, and J. C. Lowery. 2009. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implementation Science 4:50. https://doi.org/10.1186/1748-5908-4-50.
DataUSA. n.d. COVID-19 in Numbers: Physicians & surgeons. https://datausa.io/profile/soc/physicians-surgeons (accessed October 13, 2021).
Davies, S. C. 2012. Annual report of the chief medical officer, volume one, 2011, on the state of the public’s health. London, UK: Department of Health.
DeSilva, J., and M. Zweig. 2021. 2020 Market insights report: Chasing a new equilibrium. Rock Health, January 11. https://rockhealth.com/insights/2020-market-insights-report-chasing-a-new-equilibrium (accessed October 12, 2021).
Egede, L. E., and R. J. Walker. 2020. Structural racism, social risk factors, and COVID-19—a dangerous convergence for Black Americans. New England Journal of Medicine 383(12):e77. https://doi.org/10.1056/NEJMp2023616.
Environmental Health Sciences Center. 2021. What environmental factors affect health? University of California, Davis. https://environmentalhealth.ucdavis.edu/communities/what-environmental-factors-affect-health (accessed October 13, 2021).
Equity in health care: A debate. 2008. Critical Public Health 18:(1)97–110. https://doi.org/10.1080/09581590801999689.
Feeley, T. W. 2021. COVID-19 hasn’t been a tipping point for value-based care, but it should be. NEJM Catalyst Innovations in Care Delivery 2(1). https://doi.org/10.1056/CAT.20.0641.
FHCQ (Foundation for Health Care Quality). 2020. Value-based care summit. YouTube, November 18. https://www.youtube.com/watch?v=-_F2e4jdDp8 (accessed October 13, 2021).
Frellick, M. 2020. Physician income drops, burnout spikes globally in pandemic. Medscape. https://www.medscape.com/viewarticle/937271#vp_1 (accessed October 13, 2021).
Glasgow, R. E., C. Vinson, D. Chambers, M. J. Khoury, R. M. Kaplan, and C. Hunter. 2012. National Institutes of Health approaches to dissemination and
implementation science: Current and future directions. American Journal of Public Health 102(7):1274–1281. https://doi.org/10.2105/AJPH.2012.300755.
Health Rosetta. 2020. Health Rosetta vs. the status quo. https://healthrosetta.org/learn/health-rosetta-vs-status-quo (accessed October 13, 2021).
HealthIT.gov. 2018. A 10-YearVision to achieve an interoperable health IT infrastructure.https://www.healthit.gov/resource/10-year-vision-achie-ve-interoperable-health-it-infrastructure (accessed October 12, 2021).
HealthIT.gov. n.d. Value-based care. The Office of the National Coordinator for Health Information Technology. https://www.healthit.gov/playbook/value-based-care (accessed October 13, 2021).
Hilmers, A., D. C. Hilmers, and J. Dave. 2012. Neighborhood disparities in access to healthy foods and their effects on environmental justice. American Journal of Public Health 102(9):1644–1654. https://doi.org/10.2105/AJPH.2012.300865.
Hoffman, K. M., S. Trawalter, J. R. Axt, and M. N. Oliver. 2016. Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between Blacks and Whites. Proceedings of the National Academy of Sciences 113(16):4296–4301. https://doi.org/10.1073/pnas.1516047113.
Hoge, E., D. Bickham, and J. Cantor. 2017. Digital media, anxiety, and depression in children. Pediatrics 140(Suppl 2):S76–S80. https://doi.org/10.1542/peds.2016-1758G.
Hood, L., R. Balling, and C. Auffray. 2012. Revolutionizing medicine in the 21st century through systems approaches. Biotechnology Journal 7(8):992–1001. https://doi.org/10.1002/biot.201100306.
IOM (Institute of Medicine). 2010. Redesigning the clinical effectiveness research paradigm: Innovation and practice-based approaches: Workshop summary. Washington, DC:The National Academies Press. https://doi.org/10.17226/12197.
IOM. 2015. Integrating research and practice: Health system leaders working toward high-value care: Workshop summary. Washington, DC: The National Academies Press. https://doi.org/10.17226/18945.
Jetty, A., Y. Jabbarpour, J. Pollack, R. Huerto, S. Woo, and S. Petterson. 2021. Patient–physician racial concordance associated with improved healthcare use and lower healthcare expenditures in minority populations. Journal of Racial and Ethnic Health Disparities. Published ahead of print, January 5, 2021. https://doi.org/10.1007/s40615-020-00930-4.
Koonin, L. M., B. Hoots, C. A. Tsang, Z. Leroy, K. Farris, B. T. Jolly, P. Antall, B. McCabe, C. B. R. Zelis, I. Tong, and A. M. Harris. 2020. Trends in the use of telehealth during the emergence of the COVID-19 pandemic—United States, January–March 2020. Morbidity and Mortality Weekly Report 69:1595–1599. http://dx.doi.org/10.15585/mmwr.mm6943a3.
Kutner, M., E. Greenberg, Y. Jin, C. Paulsen, and S. White. 2006. The health literacy of America’s adults: Results from the 2003 National Assessment of Adult Literacy. Department of Education. https://nces.ed.gov/pubs2006/2006483.pdf (accessed October 13, 2021).
Lu, M. C. 2018. Reducing maternal mortality in the United States. JAMA 320(12):1237–1238. https://doi.org/10.1001/jama.2018.11652.
Maryland Department of Health. 2018. Maryland’s all-payer hospital model results performance year three. https://hscrc.maryland.gov/Documents/Modernization/Maryland%20APM%20Performance%20Report%20-CY2016_3_9_18.pdf (accessed October 13, 2021).
NACCHO (National Association of County and City Health Officials). 2019. National profile of local health departments. https://www.naccho.org/uploads/downloadable-resources/Programs/Public-Health-Infrastructure/NACCHO_2019_Profile_final.pdf (accessed October 13, 2021).
NAM (National Academy of Medicine). 2021. Action Collaborative on Clinician Well-Being and Resilience. https://nam.edu/initiatives/clinician-resilience-and-well-being (accessed October 13, 2021).
NASEM (National Academies of Sciences, Engineering, and Medicine). 2017. Communities in action: Pathways to health equity. Washington, DC: The National Academies Press. https://doi.org/10.17226/24624.
NASEM. 2019. Taking action against clinician burnout: A systems approach to professional well-being. Washington, DC: The National Academies Press. https://doi.org/10.17226/25521.
NEJM Catalyst. 2017. What is value-based healthcare? https://catalyst.nejm.org/doi/full/10.1056/CAT.17.0558 (accessed October 13, 2021).
NIH (National Institutes of Health). 2020. NIH’s All of Us Research Program returns first genetic results to participants. https://www.nih.gov/news-events/news-releases/nihs-all-us-research-program-returns-first-genetic-results-participants (accessed October 12, 2021).
OCTO (Office of the Chief Technology Officer). 2018. The state of data sharing at the U.S. Department of Health and Human Services. https://www.hhs.gov/sites/default/files/HHS_StateofDataSharing_0915.pdf (accessed February 21, 2022).
ODPHP (Office of Disease Prevention and Health Promotion). 2020. Environmental health. https://www.healthypeople.gov/2020/topics-objectives/topic/environmental-health (accessed October 13, 2021).
OMH (Office of Minority Health). 2021a. Asthma and African Americans. US Department of Health and Human Services. https://minorityhealth.hhs.gov/omh/browse.aspx?lvl=4&lvlid=15 (accessed October 13, 2021).
OMH. 2021b. Mental and behavioral health—Hispanics. Department of Health and Human Services. https://www.minorityhealth.hhs.gov/omh/browse.aspx?lvl=4&lvlid=69 (accessed October 13, 2021).
Parasrampuria, S., and J. Henry. 2019. Hospitals’ use of electronic health records data, 2015–2017. The Office of the National Coordinator for Health Information Technology. https://www.healthit.gov/sites/default/files/page/2019-04/AHAEHRUseDataBrief.pdf (accessed October 12, 2021).
Pylypchuk, Y., and C. Johnson. 2020. State of interoperability among major U.S. cities. The Office of the National Coordinator for Health Information Technology. https://www.healthit.gov/sites/default/files/page/2020-10/CitiesDataBrief_10_26_2020.pdf (accessed October 12, 2021).
Ramsey, S., D. Blough, A. Kirchhoff, K. Kreizenbeck, C. Fedorenko, K. Snell, P. Newcomb, W. Hollingworth, and K. Overstreet. 2013. Washington state cancer patients found to be at greater risk for bankruptcy than people without a cancer diagnosis. Health Affairs (Millwood) 32(6):1143–1152. https://doi.org/10.1377/hlthaff.2012.1263.
RAND Corporation. 2016. The evolving role of retail clinics. https://doi.org/10.7249/RB9491-2.
Richmond, J., W. Powell, M. Maurer, R. Mangrum, M. R. Gold, E. Pathak-Sen, M. Yang, and K. L. Carman. 2017. Public mistrust of the U.S. health care system’s profit motives: Mixed-methods results from a randomized controlled trial. Journal of General Internal Medicine 32(12):1396–1402. https://doi.org/10.1007/s11606-017-4172-1.
Riehm, K. E., K.A. Feder, K. N. Tormohlen, R. M. Crum, A. S. Young, K. M. Green, L. R. Pacek, L. N. La Flair, and R. Mojtabai. 2019. Associations between time spent using social media and internalizing and externalizing problems among US youth. JAMA Psychiatry 76(12):1266–1273. https://doi.org/10.1001/jamapsychiatry.2019.2325.
Ruckart, P. Z., A. S. Ettinger, M. Hanna-Attisha, N. Jones, S. I. Davis, and P. N. Breysse. 2019. The Flint water crisis: A coordinated public health emergency response and recovery initiative. Journal of Public Health Management and Practice 25(Suppl 1):S84–S90. https://doi.org/10.1097/PHH.0000000000000871.
Smith, B. 2021. CMS Innovation Center at 10 years—progress and lessons learned. New England Journal of Medicine 384:759–764. https://doi.org/10.1056/NEJMsb2031138.
Tikkanen, R., and M. K. Abrams. 2020. U.S. health care from a global perspective, 2019: Higher spending, worse outcomes? The Commonwealth Fund, January 30. https://www.commonwealthfund.org/publications/issue-briefs/2020/jan/us-health-care-global-perspective-2019 (accessed October 13, 2021).
Tricoci, P., J. M. Allen, J. M. Kramer, R. M. Califf, and S. C. Smith, Jr. 2009. Scientific evidence underlying the ACC/AHA clinical practice guidelines. JAMA 301(8):831–841. https://doi.org/10.1001/jama.2009.205.
Verma, S. 2020. 2019 Medicare Shared Savings Program ACO performance: Lower costs and promising results under “Pathways to Success.” Health Affairs. https://doi.org/10.1377/hblog20200914.598838.
Wagner, E. H., B. T. Austin, and M. Von Korff. 1996. Organizing care for patients with chronic illness. Milbank Quarterly 74(4):511–544. https://pubmed.ncbi.nlm.nih.gov/8941260 (accessed October 13, 2021).
WHO (World Health Organization). n.d. Health at key stages of life—the life-course approach to public health. https://www.euro.who.int/__data/assets/pdf_file/0019/140671/CorpBrochure_lifecourse_approach.pdf (accessed October 13, 2021).

































