Health Data Sharing to Support Better Outcomes: Building a Foundation of Stakeholder Trust (2020)
Chapter: 6 Conclusion
6
CONCLUSION
To share and receive feedback on the vision statement (see Chapter 2), the definition of health data, and the stakeholder statements (see Chapters 3, 4, and 5), and to begin building support for implementing the short-term action steps identified, the National Academy of Medicine Leadership Consortium: Collaboration for a Value & Science-Driven Health System hosted a meeting on August 23, 2019, in Washington, DC, which brought together representatives of the steering committee and stakeholder groups that prepared the statements in Chapters 3–5 along with a broad array of other experts and health system leaders. The goal of the meeting was building partnerships and implementing principles and priorities to overcome the cultural, regulatory, financial, and ethical barriers identified by the stakeholder groups and achieve the vision described in Chapter 2 (see Appendix C). Drawing on that discussion, this chapter describes the overlapping barriers and solutions from the stakeholder statements and a number of priorities for the nation that are critical to addressing the outstanding barriers to health data sharing, linkage, and use.
OVERLAPPING BARRIERS AND SOLUTIONS
As was observed at the meeting, the statements produced by each of the stakeholder groups revealed a remarkable amount of overlap among the cultural, ethical, regulatory, and financial barriers to greater data sharing, linkage, and use (see Figure 6-1).
- The groups representing health care executives and patient and family leaders identified a misalignment of financial and other incentives as common barriers.
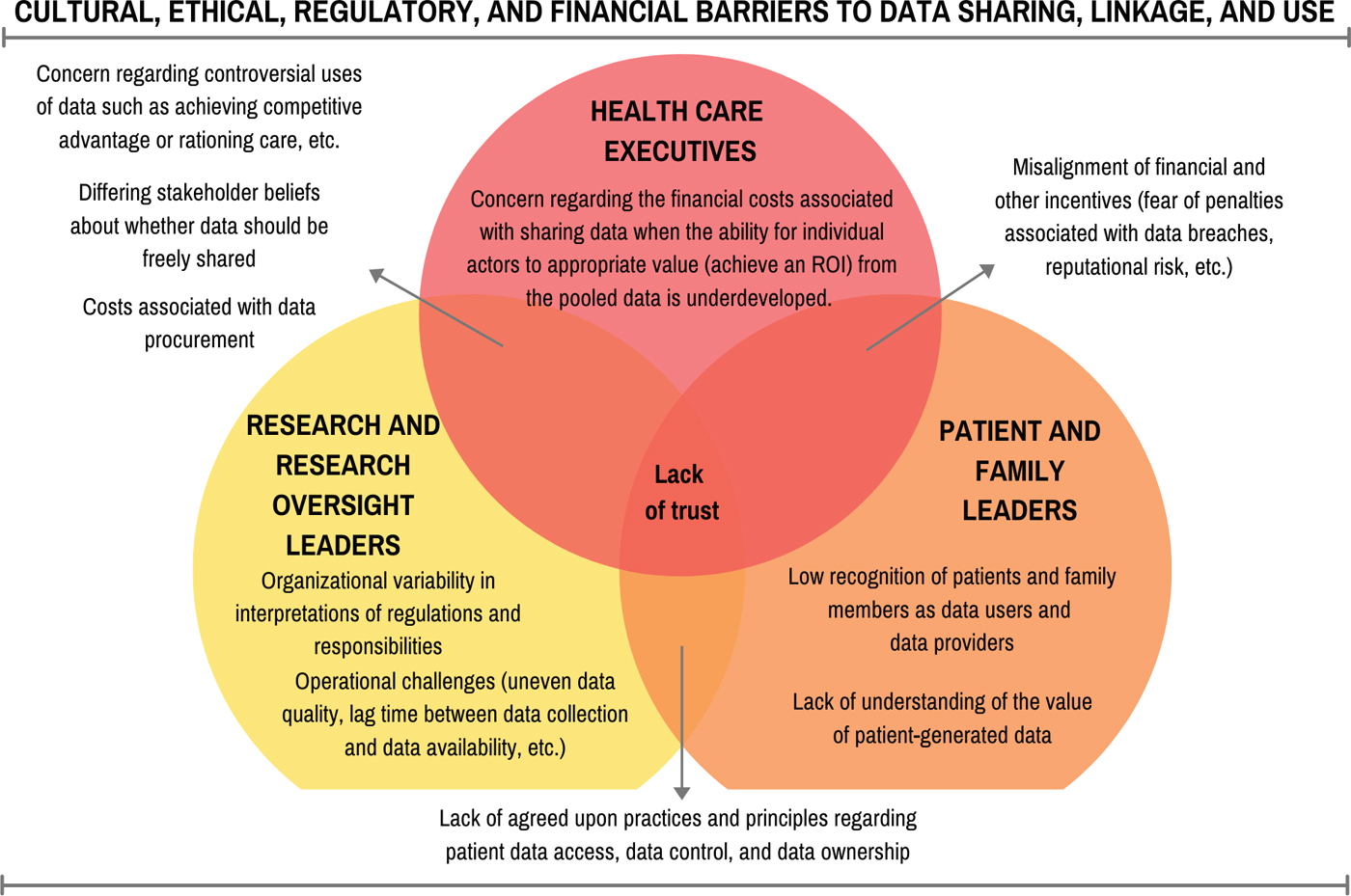
- The groups representing patient and family leaders and researchers and research oversight leaders identified a lack of agreed-upon practices and principles regarding patient data access, data control, and data ownership.
- The groups representing research and research oversight leaders and health care executives identified concerns regarding controversial uses of data, differing beliefs about whether data should be freely shared, and costs associated with data procurement.
A concern shared by all three stakeholder groups was a lack of trust in the intentions and actions of other groups. The members of the patient and family community lack trust that health care systems and researchers will make data and the conclusions based on those data available to them and will not misuse data they provide by rationing care and sharing those data with unauthorized third parties. Researchers share a similar mistrust in the intentions of third-party users. Health systems are concerned that patients will misinterpret data or use data inappropriately, such as allowing them to be combined with other elements so as to identify individuals. Specific examples of these problems were mentioned at the meeting, such as the dialysis clinic that refused to share a patient’s data that he wanted to share with researchers, or the lack of cooperation between two health systems that refused to even refer to each other by name because of the competition between them. Ultimately, such lack of trust stems from the diverging interests of each group and the lack of common cause for data sharing among the three groups.
The stakeholder statements reveal several imperatives for addressing data-sharing challenges that are common to one or more stakeholder groups, including
- developing a set of principles and commitments on data ownership, accessibility, and control;
- reframing the risk discussion or business case related to data sharing to highlight patient safety and evidence-based arguments about the risks of not sharing data;
- devising a national educational campaign tailored to specific stakeholder groups that highlights the benefits of bidirectional data exchange and prepares these stakeholder groups for using and contributing to shared data;
- conducting and disseminating research on stakeholder preferences and beliefs regarding whether and how data should be shared;
- standardizing data collections and use over the long term by identifying and implementing common data models and data standards, establishing data
- continuing efforts to address the misalignment of financial incentives by implementing payment models that reward value-based care and population health.
enclaves or safe harbors, and clarifying what kinds of data various groups are trying to access; and
These common solutions formed the basis for much of the discussion at the August 23 meeting.
PRIORITIES FOR THE FIELD
Over the course of the meeting, several priorities emerged as the most important to addressing the barriers identified by the stakeholder groups. Many of these priorities reinforced ideas generated in prior discussions of the stakeholder working groups.
ENGAGING IN A PUBLIC INFORMATION CAMPAIGN
Greater knowledge is essential to move data sharing forward. In particular, a widely disseminated public information campaign could help change attitudes and behaviors by showing people how the use of health data could improve their health and the health of people they know. Such a campaign could target not only the general public but also care providers, policy makers, health care administrators, and others in a position to influence data issues as described in the Statement of Patient and Family Leaders in Chapter 3. Given the importance of this issue to the future of health care, reaching out to school-aged children and building data literacy early in life will be important.
An educational campaign could entail commercials, social media campaigns, public service announcements, webinars, newsletters, and many other forms of communication. Information from the campaign also could be extracted into PowerPoint presentations, infographics, narratives of personal experiences, accounts by early adopters of new approaches, and other flexible and usable forms. Such stories could emphasize that past instances of data sharing have not only created benefits but also not resulted in problems. An article in Science or another high-profile journal could address data sharing. Even movies and television shows could help make the case.
Several wedge issues could prove important in such a campaign. One is that the lack of data access is an issue of patient safety. Health care executives and organizations, insurers, clinicians, patients, families, and others all resonate
with this issue. Another is the intersection of data sharing with privacy and security as subsets of health data are governed differently. In the absence of an overarching privacy law in the United States, the Health Insurance Portability and Accountability Act (HIPAA) protects health data that flow among health systems, payers, and other covered entities but not consumer-generated data that originate from mHealth apps or wearable devices or data that are shared with third-party technology companies.. Therefore, guides to privacy and security could be disseminated as part of the campaign to educate consumers of health care about the issue.
Change will occur when there is sufficiently high demand by all of health care’s stakeholders, from the public to the clinical and research communities. Today, however, the public does not fully understand the benefits and value of data sharing, and the demand is not commensurate with the need for change.
CREATING AND PRIORITIZING USE CASES
Foundational to devising a national educational campaign, the development of use cases that promote various reasons for sharing and linking health data could help build demand for data sharing, demonstrate how to overcome the barriers identified by the stakeholder groups, and achieve the vision described in Chapter 2. These use cases should highlight the benefits of sharing data and information not only with patients or for research but also for artificial intelligence applications, machine learning, performance improvement, best practice guidelines, and many other uses.
Use cases could highlight potential cost savings and analytics that drive value. They could reveal the interdependencies of complex systems and show how to build on success by extending successful innovations into new areas.
A matrix of all of the providers and users of data and their interconnections would reveal many potential use cases. This matrix could describe who provides data, who consumes data, what data elements need to be shared, and the benefits and risks of sharing data. Such a matrix could also identify gaps, both in the private and public sectors, and demonstrate the returns on investment of specific actions.
Use cases can focus on short-, medium-, and long-term objectives and on the critical levers for each. Within each use case category, it would also be helpful to identify exemplar organizations that have shared or linked data to positively impact health outcomes. By demonstrating how greater sharing and use of data can improve health, use cases and exemplars can drive the adoption of a variety of initiatives. For example, a use case that embodies value-based care or
personalized medicine could be structured around the exchange and broader use of data. Use cases also could spur greater involvement by organizations and groups that are not yet heavily involved in data sharing, such as small health care systems or communities that have been disenfranchised.
Use cases can range widely across sectors and incorporate many types of data, including clinical, claims, social determinants, and consumer-generated data. To take just one example, standardized patient-reported outcomes could provide the basis for a use case, enabling robust comparison of these outcomes across health systems and care settings.
MAKING THE BUSINESS CASE
Each stakeholder in the health care system will need to see the advantages of moving toward greater data sharing. Particularly in the private sector, this will require the development of compelling business cases that clearly demonstrate these advantages and return on investment.
Developing a business case will require the involvement of different people and stakeholder groups. It also will require estimates of the costs and potential benefits of sharing data and of not sharing data. The business case should lay out not only the financial impact but also the other potential gains and losses (e.g., cost of patient harm, reputation/brand, market share). The existing market for health data, where organizations already attach value to curated databases, could help in understanding and deriving these costs.
A business case can demonstrate how data sharing is useful and brings benefits to multiple parties, including consumers, in preventing medical error and enhancing the care delivery experience. It can show how data sharing has the potential to produce competitive advantages rather than disadvantages. In these and other ways, a strong business case can inspire organizations to be early adopters of new procedures rather than waiting for others to go first. Discussions or partnerships with business groups on health or similar state-based alliances of employers and purchasers could help inform the development of the business case.
BASING PAYMENT ON VALUE
New payment models that incentivize paying for value and outcomes, rather than paying for the volume of care that is delivered, could have concurrent benefits to the imperative for more seamless data sharing. Population health management depends on shared knowledge of patients’ experiences of care
across time and across setting. For example, value-based arrangements with care providers and health systems can result in tools that consumers can use to better navigate health care. Value-based health care also can support data exchange, infrastructure development, technology support, and research (Kent, 2018).
There are already a number of initiatives under way to incentivize value-based payments. For example, the Centers for Medicare & Medicaid Services (CMS), an early adopter of value-based care delivery, has identified several alternative payment models that incentivize value over volume. The Medicare Access and CHIP (Children’s Health Insurance Program) Reauthorization Act of 2015 (MACRA) creates a new framework for rewarding Medicare patients’ physicians for providing higher quality care. One of the performance tracks in MACRA, Merit-Based Incentive Payments Systems, emphasizes promoting interoperability through focusing on patient engagement and the electronic exchange of health data (Quality Payment Program, 2020). Additionally, new payment models, such as CMS’s Primary Care First Model—which offers an innovative payment structure to support primary care delivery for patients with complex chronic needs and high need, seriously ill patients—are being developed (CMS, 2019b). Private payers are also testing alternative payment approaches and are using approaches such as Shared Savings and Shared Losses Models, Bundled Payment Models, and Alternative Quality Contract to control spending growth and increase care quality (Chernew et al., 2011).
A complication of basing payments on value is that the United States does not have a single health care system. Rather, it is comprised of multiple health care systems that sometimes cooperate and sometimes compete. Business priorities drive some of this competition, as do cultural factors. Nevertheless, increased adoption of value-based care can lead to potential returns on investment and engage communities in exploring and identifying related principles and actions that improve health.
INSTITUTING SUPPORTIVE GOVERNMENT POLICIES
Government policies can support data sharing in a variety of ways, as elaborated in the health care executives’ statement. Such policies can establish ground rules and standards for data exchange across networks, as well as support the development of technologies and systems that promote rather than impede data sharing. They can send clear signals about how existing technologies should be used and what new technologies are needed. One example is CMS’s Interoperability and Patient Access final rule, which mandates Medicare
participants to share data via open, secure, and standardized application programming interfaces (CMS, 2019b; see Chapter 5). Another example is the 21st Century Cures Act, which includes provisions requiring data sharing and management plans among recipients of federal research funds (ONC, 2020c).
Direct financial incentives can also drive change—for example, by encouraging hospitals and clinicians to share data through interoperable systems. Negative incentives can have an effect as well, such as public identification or the levying of financial penalties on systems that are blocking or not doing enough to share data. The aforementioned 21st Century Cures Act sets limits for data blocking (CMS, 2019a; ONC, 2019).
All funders of research, not just government, can require researchers to make their data available to other researchers and to research participants. However, as acknowledged by the National Institutes of Health’s request for public comments on the Draft Policy for Data Management and Sharing, the complexity and cost of preparing, curating, and sharing research data for secondary analyses could complicate the ability of research entities to comply with this. Funders also can support data-gathering efforts among other groups and organizations to generate datasets and make them publicly available.
BUILDING TRUST
Greater trust and transparency among stakeholder groups can both foster and support data sharing. Standards of conduct can build trust, because people know what to expect. For example, making the return of research results to participants the norm rather than the exception could inform people about the value of research and help build trust. Collaborative efforts built on trust can convert zero-sum relationships into positive-sum relationships, where data sharing serves everyone’s interests.
Trust has to be built and sustained thoughtfully and intentionally, given that it is a fragile commodity and can easily be lost. Even if an organization’s mission statement says that the consumers of health care come first, business plans and actions of those in the organization need to reflect that mission. Patients and consumers are often unaware that HIPAA protections do not extend to third-party health data companies, and a well-publicized breach in this area could undermine public confidence and set back the move toward data sharing. Ensuring that non-HIPAA-covered entities are protected by robust and enforced laws for data privacy will be critical in maintaining public trust. Hoping for trust when the customers’ interests are not being served will not work, especially given that contextual factors can influence
trust in an entire sector. Additionally, trust can be maintained even when things go wrong. For example, a compensation plan funded by the users of data would be one way to make amends for data breaches.
ALLOCATING RESOURCES FOR ACHIEVING PRIORITIES
At the August 23 meeting, participants discussed a wide array of resources that are both needed and available to achieve the goal of both improved and more frequent data sharing.
One point made repeatedly at the meeting is that health data extend far beyond the data most directly related to health care and health outcomes. Health data include such widely varied data sources as geospatial data; census data; consumer data from groceries, media companies, and smartphone applications; and fitness- and wellness-related data. Many of these forms of data, alone or in combination, can be used to infer health status or inform health care.
Though the stakeholder groups were directed not to address the technical barriers to greater data sharing, computational technologies are a major part of the resources needed to achieve the priorities the groups identified. These technologies are advancing rapidly, highlighting the need for flexibility in responding to new capabilities and circumstances. Technologies can provide solutions to some barriers to data sharing, such as enabling audit trails to enforce compliance with regulations or balancing access with security and privacy. Technology development also can involve innovators and entrepreneurs in the health care system, further speeding progress.
As an example of a technological advance, many health care providers and hospitals are on the verge of meeting requirements for meaningful use by enabling consumers to use third-party applications to access clinical data. By enabling the consumers of health care to interact much more directly with their health data, this advance could mark the beginning of a transformation in health care. For example, given that not enough providers are available to manage the chronic diseases of an aging population, the use of such applications could greatly increase the number and agency of people who are taking an active role in co-managing their health care.
Some data-sharing initiatives can begin with small groups, such as patients with particular diseases, and then spread more widely as exemplified by the creation of many of the Patient-Centered Outcomes Research Institute’s Patient-Powered Research Networks. Others may start with particular institutions and then be adopted or adapted in other settings. Other industries offer examples of data sharing that the health care system could adopt. For example, the August
23 meeting featured a presentation about the spread of data sharing within the airline industry. Convening information technology experts who work outside of the health care industry with health care experts could help to drive innovative solutions to addressing the barriers to health data sharing.
A consortium of organizations committed to stewarding progress on data linkage, sharing, and use could produce greater collaboration and faster progress. Lessons can be derived from the Clinical and Translational Science Awards’ Connecting Data to Health program (NCATS, 2020). Similarly, a shared framework and commitment to data sharing could rally all stakeholders around the idea, and a website that compiles ongoing data-sharing initiatives and resources could be a source of information and momentum.
TOWARD A CONTINUOUS LEARNING HEALTH SYSTEM
Health data are the foundation for a continuously learning health system in which science, informatics, incentives, and culture are aligned to yield continuous improvement, innovation, and equity. In such a system, new knowledge is seamlessly embedded in the delivery of health care, individuals and families are active participants in all elements of care, and new knowledge is generated as an integral product of the delivery of care. Addressing the cultural, ethical, regulatory, and financial barriers to data sharing that currently exist, and building support and demand for data-sharing efforts among key stakeholders including patients and caregivers, clinicians, health care executives, and researchers is paramount to achieving the vision of a continuously learning health system and improving health and health care outcomes.









