Accelerating Medical Evidence Generation and Use: Summary of a Meeting Series (2017)
Chapter: 4 Needs, Opportunities, and Strategies for Accelerating Progress
4
NEEDS, OPPORTUNITIES, AND STRATEGIES FOR ACCELERATING PROGRESS
A number of needs, opportunities, and strategies exist for the National Patient-Centered Clinical Research Network (PCORnet) Health Systems Demonstration Project to accelerate progress. These were discussed in five breakout groups focused on the data and analytic needs of importance to executive-level decision makers; the value of PCORnet and PCORnet studies in improving health care delivery locally and nationally; and possible next steps for further development of PCORnet. Following the breakout session, participants reconvened in a plenary session, where group facilitators reported back on the discussions, and also talked about five themes identified by the Patient-Centered Outcomes Research Institute (PCORI) from the questions submitted by the Clinical Data Research Networks (CDRNs, as discussed by Carton in Chapter 3). Rainu Kaushal, chair of the Department of Healthcare Policy and Research at Weill Cornell Medicine, New York-Presbyterian Hospital, presented an overview of the five themes and key research questions for each and facilitated an open discussion in which participants considered strategic opportunities and the specific steps needed to move priorities forward, both in participant’s own institutions and collaboratively. Highlights and main points are summarized in Box 4-1.
PCORNET: HARNESSING THE POWER OF HEALTH CARE DATA
The presentations provided examples of the importance of systems-level data for improving the efficiency and effectiveness of care. The examples also demonstrated the need for systems-level data to be better organized, standardized, and validated, and for better facilitation of collaboration across systems. The need to better engage health system clinicians in these efforts to improve performance was mentioned. Speakers also discussed the need to bring operations and research together. To set the stage for the breakout discussions, Selby provided a brief primer on PCORnet.
PCORnet Mission and Structure
Getting complete data for research purposes is challenging and requires extensive coordination. Patients get care at multiple institutions and sites, and data are stored within multiple, disparate systems that are not generally interoperable. In addition, there are other factors critical to health that are not captured in inpatient or ambulatory EHRs or claims (e.g., social determinants of health, patient-reported outcomes,
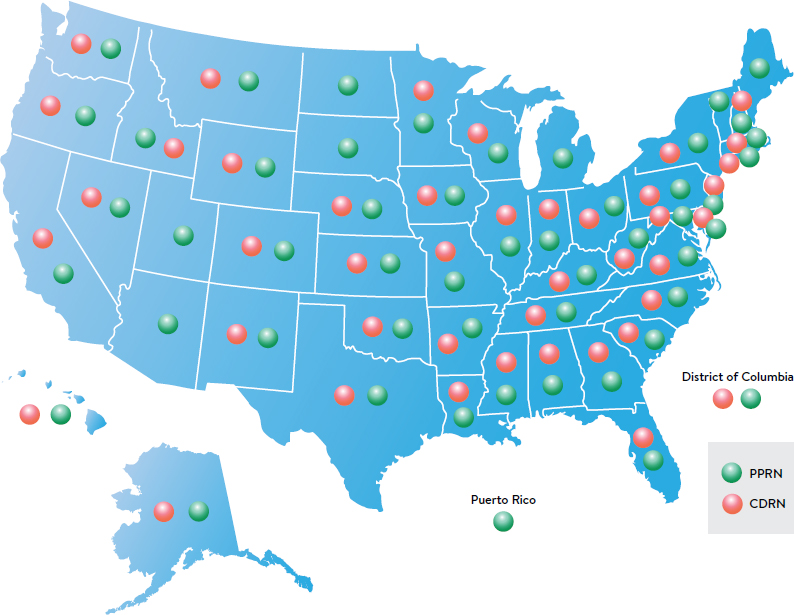
genomic data, prescriptions paid out of pocket, biospecimens, registry data, and death data). PCORnet is a “behind-the-scenes” infrastructure that offers a standard way of organizing and aggregating data to enable the collection of “complete” data on large numbers of patients to facilitate multisite research. PCORnet’s mission is to harness these data and research findings to facilitate health system improvement and, in the process, transform the culture of clinical research from one directed by researchers to one driven by the needs of patients and those who care for them. PCORnet collects, organizes, and aggregates data from EHRs from more than 130 health systems across the country, as well as claims data and other data sources. The network is organized into 13 PCORI-funded CDRNs and 21 Patient-Powered Research Networks (PPRNs; see Box 4–2, Box 4–3, and Figure 4–1).5
Organizationally, PCORnet is led by the PCORnet Council, including representatives from each of the CDRNs and PPRNs, which advises on strategy and operations. An executive committee serves the council and provides oversight of operations. There is also an advisory group that includes all potential funders of
___________________
5 PPRNs are networks of patient organizations focused on a particular health condition that are interested in sharing health information and engaging in research. See also https://academic.oup.com/jamia/article/21/4/583/2909240/Patient-powered-research-networks-building. (accessed January 3, 2018).
PCORnet (both government and private sector). The council has three critical working committees: (1) the Data Committee, which promotes the acquisition, standardization, and sharing of data; (2) the Engagement Committee, which works on bringing patients, clinicians, systems representatives, and leadership together with researchers; and (3) the Research Committee, which aims to identify and promote the kinds of research at which PCORnet excels. Finally, the Coordinating Center coordinates operational activities, maintains data infrastructure, identifies research opportunities, and coordinates multisite research.
SOURCE: Selby presentation, January 21, 2016.
The Common Data Model
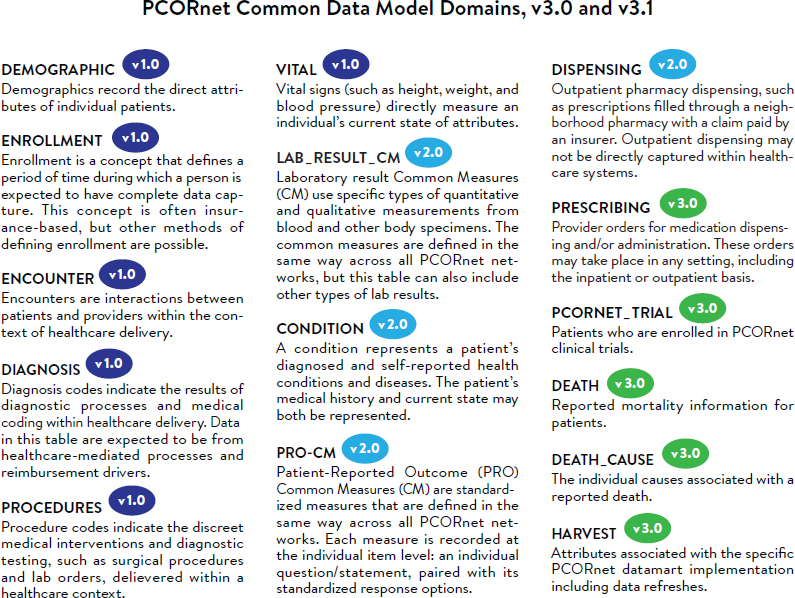
To organize the disparate data from hospitals and health care delivery systems into a standard structure such that they can be more effectively used for research, PCORnet developed the Common Data Model (see Figure 4-2). Each PCORnet partner network maps data to the same consistent format (e.g., with the same variable name, attributes, and other metadata). Undertaking this step before initiating any PCORnet research studies creates a platform that enables much more rapid responses to research-related questions. The vision is that the Common Data Model will expand to go deeper within each of the current categories but also add new categories over time (e.g., biospecimen and genomic data, patient satisfaction information, and death index data).
Data from more than 70 million people across the 130 health systems participating in PCORnet are currently arrayed in over 60 nodes or “data marts.” In essence, Selby explained, there are 60 instances of the Common Data Model.
SOURCE: http://www.pcornet.org/wp-content/uploads/2014/07/2015-07-29-PCORnet-Common-Data-Model-v3dot0-RELEASE.pdf.
PCORnet-Sponsored Research
PCORnet demonstration projects enable the network to build out aspects of its function and its infrastructure and demonstrate its capacity to do particular types of research. There are three major PCORI-funded demonstration projects currently under way. Two are observational studies, including a study of the outcomes of the three common types of bariatric surgery for severe obesity, and a study investigating the use of broad-spectrum versus narrow-spectrum antibiotics and the development of childhood obesity. The third is a randomized clinical trial comparing the effectiveness and safety of two different doses of aspirin (81 mg versus 325 mg) in high-risk patients with coronary artery disease. Multiple CDRNs are involved in each of the studies.
PCORnet contributes importantly on multiple levels. It creates the capacity for standardized and more efficient project start-up and provides a reusable infrastructure, which limits project shutdown costs. PCORnet is a learning model, and each new project benefits from prior studies. The scale and diversity of patients
and providers in the network are also assets. The ability to study and understand personalized medicine, for example, requires much larger populations than can generally be built in any one system. The network engages patients and clinicians to help develop the research questions, plan and conduct the studies, and disseminate the findings. According to Selby, investigators will find that accessing and using PCORnet resources is easy and cost effective. PCORnet creates a culture of collaboration and a network of relationships among researchers and all players in health care delivery. Finally, there is health system commitment to sustaining PCORnet and building a track record of success.
Selby reiterated the concept of the PCORnet Health Systems Demonstration Project. As discussed, this meeting was designed to be the culmination of the first phase of the project, generating a list of priority topics of interest to health systems leaders and clinicians. Funded projects will bring researchers and health system leaders together to plan research activities that help both to cement the relationship between system leaders and PCORnet and to answer important early questions about the utility of PCORnet data and the capacity of those data to support performance improvement and comparative effectiveness questions. Selby encouraged participants to reflect on the ideas discussed at the workshop and submit proposals.6 Following this meeting, PCORI issued a limited funding announcement awarding $5 million to support five quick-turnaround, research demonstration projects.
BREAKOUT DISCUSSIONS
According to Kaushal, this is a critical point in time because there are now enough data available to start asking and answering the questions that prompted these efforts by PCORI 2 years ago. She described the three key aims of the breakout session:
- Identify key data and analytic needs that CEOs and other executive-level decision makers involved in health care administration perceive as important unmet needs;
- Explore the role of PCORnet, as an exemplar of a clinical-data infrastructure, in improving research and health care delivery locally and nationally; and
- Consider important next steps in building and improving PCORnet.
Participants divided into five preassigned breakout groups of about 10 to 12 people. Groups were provided with a set of more specific questions to help guide
___________________
6 The application period closed in April 2016. Funding was awarded in June of 2016, and projects began in September. For the full funding announcement see http://www.pcori.org/sites/default/files/PCORI-PFA-2016-Health-Systems.pdf (accessed May 31, 2016).
their discussions (see Box 4–4), which were facilitated by a CDRN principal investigator and one or two CEOs. Upon reconvening in the plenary session, facilitator group reports were provided by Kaushal; Beth McGlynn, director of the Kaiser Permanente Center for Effectiveness and Safety; Veronique Roger, director of the Center for the Science of Health Care Delivery at the Mayo Clinic; Elizabeth Shenkman, director of the Institute for Child Health Policy at the University of Florida College of Medicine; and Kathleen McTigue, associate professor at the University of Pittsburgh School of Medicine.
Each of the facilitators observed that there was much similarity across the five groups’ discussions. The outcomes they reported are organized by aim, below (Box 4–4).
Pressing Data and Analytic Needs of Executive-Level Decision Makers
A point made by the CEOs, McGlynn reported, was that they must make decisions every day, whether or not data are available, and many decisions are made in an “evidence-free environment.” For evidence to be a part of their
conversations, time is of the essence, and the process of providing data needs to be much more nimble. Roger added that her group also discussed the need for nimble and timely dissemination of data to help decision makers and frontline providers facilitate improvement of care.
McGlynn’s group felt that planning the work that will be done under the health systems demonstration projects should start with clearly defining a set of desired outcomes and then working backward from there. It was suggested that target outcomes would be high level but still focused in a specific area (e.g., no infections in the hospital, or an uncomplicated journey of cancer treatments). Keren’s description of the success in eliminating central line infections (see Chapter 2) inspired Kaushal’s group to consider some specific topics that might be “low-hanging, high-impact fruit,” that is, projects that could readily yield successes. A variety of research topics were suggested in areas such as transitions of care, transitioning to increased antibiotic use, effective sleep apnea screening, choosing appropriate measures and incorporating them more strongly, and trying to move away from iatroepidemics. McTigue’s group noted the need to build on the context in which care is delivered. There was discussion, for example, about the variation in public insurance programs at the state level across the country. A question was also raised about how to measure cultures within health systems, which can impact implementation and translation.
PCORnet’s Impact on Health Care Delivery Locally and Nationally
McGlynn’s group discussed that there is a great opportunity to learn using PCORnet by leveraging the variation that exists across systems in outcomes and in the processes that produce those outcomes. Shenkman reported that there was much discussion about the value of being able to do studies across different health systems for a variety of purposes. Examples of such cross-system studies included benchmarking, trending, and forecasting; variability in outcomes related to new technologies or procedures as well as high-cost, complex procedures; outcomes related to rare diseases or unusual patient populations; and evaluating the success of dissemination efforts. Participants in McTigue’s group discussed further the concept of precision measurement raised by Pronovost in his talk (see Chapter 3), and how big data could be leveraged to more effectively define and measure quality.
Participants in Kaushal’s group suggested utilizing the PCORnet infrastructure to facilitate training and workforce development on how to use data for health system improvement. It was observed that a new generation of providers needs to be trained in working with this type of big data. Selby concurred with the
importance of workforce training and noted the need to train researchers to think as members of systems and to work with system leaders to ask and answer important questions.
Roger’s group noted the array of different health systems present at the workshop and emphasized that the value proposition for PCORnet will not be a “one size fits all.” For example, the needs of a tertiary coronary referral setting will be different from those of an integrated health system that focuses more on population health. It is important to keep this diversity in mind as the value proposition of PCORnet is refined. Participants in Roger’s group also noted that many health systems are already part of data networks, and it will be important for PCORnet to differentiate itself and demonstrate its value relative to those other data networks.
Important Next Steps in Building and Improving PCORnet
Participants identified a variety of ways that PCORnet could be enhanced to assist health system leaders in addressing topics of interest. McGlynn emphasized that there is an increasing focus on social determinants of health by health systems, and her group highlighted the need to capture data on social determinants in the PCORnet Common Data Model. Kaushal reported that her group also suggested the need for additional data sources, including, for example, patient-reported data, not only on outcomes but also on education level, social structure, mental health conditions, and the like. Participants raised the question of whether social media or marketing data could be more effectively utilized to round out a patient’s profile. Shenkman highlighted several additional types of data that her group suggested would be useful to include, such as pharmacy data, data on postacute care, data on the true cost of care, and data from wearable devices (e.g., physical-activity monitors). Selby agreed that incorporating socioeconomic and demographic influences on health status, for example, could lead the work of PCORnet in expanding and promising directions.
The ability to capture longitudinal data was highlighted as a need by McGlynn’s group so that questions could be asked not just about episodes of care, but about the care trajectory that people experience over a longer period of time. Roger agreed and noted that her group discussed the fragmentation of care, and how the ability to reconstitute the timeline for a patient’s course of care would be important in terms of developing knowledge.
McGlynn’s group noted that even though PCORI is prohibited from funding cost-effectiveness or cost-comparison studies, there does need to be some way in PCORnet to capture costs of care. It may be that this will need to be done
through funding from sources other than PCORI, and this could be possible as PCORnet evolves as an independent entity.
McGlynn’s group suggested that the ability to characterize diverse systems would be helpful; that is, some sort of systems-level variable would help researchers understand something about the systems that are producing the outcomes that are being demonstrated. The group also suggested that PCORnet could be more powerful if there were systems to help translate national-level findings into local action and change. McTigue reported that her group raised the issue of data quality and interpretation. Even with the Common Data Model, it was noted that there could still be variations in what the data mean. The group also discussed the importance of the development of standardized common definitions in PCORnet, which impact studies related to triggering events, super utilizers, and risks for poor outcomes, for example.
HEALTH CARE SYSTEM RESEARCH QUESTIONS
For the first phase of the PCORnet Health Systems Demonstration Project (July 2015 to January 2016), each of the CDRNs was charged with developing and submitting three research questions to PCORI that would be feasible to accomplish within 12 months (utilizing data that were likely to be available by the July 2016 start date); leverage PCORnet and the Common Data Model; be relevant to the delivery of health care and the health of large populations; and be of potential impact and importance.7 PCORI then collated and organized the submitted questions according to five major themes: high health care utilizers, specific populations, new models of health care delivery, novel analytic tools and models, and assessment of value. Two to three priority research topics per theme were then selected for further discussion and prioritization at this meeting. Kaushal provided an overview of the major themes, and key research questions for each, adding that they were chosen to be illustrative and to prompt a discussion and are not in any way a final product (topics are summarized in Box 4–5). She also noted that many CDRNs submitted similar questions, and that many of the questions cut across themes.
___________________
7 Discussed by Carton in Chapter 3. See also https://www.pcori.org/sites/default/files/PCORI-PFA-2016-Health-Systems.pdf (accessed May 31, 2016).
Identifying and Managing High Health Care Utilizers
Classifying High Health Care Utilizers
The first set of questions in this theme revolves around the most useful methods for classifying patients, and subsets of patients, who utilize the most health care services. Could socioeconomic status, claims data, and clinical data be used to enhance classification? How might methods of classification be routinized and incorporated into care delivery? Is it possible to determine epidemiology across health systems, and start to understand which health systems have the highest utilizers or subsets of utilizers? Is it possible to determine and address modifiable factors of high utilization? Are there successful examples of utilization management that could be more rapidly and effectively shared?
Readmissions
The second set of questions related to high health care utilizers focuses on readmissions. Kaushal noted that her breakout group discussed readmissions as a marker of quality. When patients are readmitted, what hospitals are they readmitted to, what are their predictors, and how well do available data sources capture those readmission patterns or predict readmission? Can data available through EHRs improve the characterization of patterns of readmission or the predictive validity of existing models? A combination of claims and clinical data
could allow for much more effective research on the epidemiology of readmissions than has been done thus far using solely claims data. It was also noted in a breakout session that there is often a time lag in the ability to access Medicare data. How might the accessibility of data sources through PCORnet change this?
Specific Populations
The second major theme was identifying and managing the needs of specific populations by diagnoses (e.g., behavioral or physical health) or patient characteristics (e.g., socioeconomic status).
Co-occurring Behavioral and Physical Health Conditions
What are the utilization patterns and outcomes of patients who have co-occurring behavioral and physical health conditions? Are certain combinations of behavioral and physical health conditions associated with higher utilization and/or poorer outcomes? What interventions are most successful for patients with co-occurring conditions (e.g., focusing on the behavioral health condition or co-locating behavioral and physical health treatment), particularly in the context of population health programs?
Social and Nonmedical Needs
What specific programs are most effective in meeting the social/nonmedical needs of patients (e.g., food insecurity, transportation, and housing)? Which programs should be adopted by the health system?
New Health Care Delivery Models
Palliative Care Consults
How commonly are palliative care consults recorded, and for which patients? Is there an identifiable subset of patients who could have benefited from palliative care but who were not offered the option? What is the effect of palliative care on health outcomes and utilization? Kaushal noted the intentional use of the word “utilization” to conform with the PCORI process, but the real question is what are the effects on cost.
Accountable Care Organizations (ACOs) and Patient-Centered Medical Homes
How do individuals enrolled in ACOs or patient-centered medical homes (PCMHs)8 compare with those not enrolled in an ACO/PCMH in rates of admission, 30-day readmission, and emergency department (ED) utilization,
___________________
8 Also referred to as primary care medical homes.
with a focus on subsets of individuals with pneumonia, chronic obstructive pulmonary disease, heart failure, acute myocardial infarction, total hip arthroplasty, total knee arthroplasty, and coronary artery bypass graft? Kaushal added that questions about bundled payments also fit into this category.
Novel Analytic Tools and Methods
Risk-Adjustment Model for High Utilizers
A topic raised in many of the CDRN interviews and in the breakout group discussions was risk-adjustment models for high utilizers, making use of the novel data sources available through PCORnet. Can a risk-adjustment model that incorporates claims, clinical, and socioeconomic data more accurately predict high utilization than existing claims-based risk-adjustment models? If so, how could these prediction models be incorporated into care delivery settings?
Patient and System Predictors of Future Utilization
Also under the theme of analytic tools and methods were questions about patient and system predictors of future utilization, especially given the potential availability of new data sources. What characteristics of the patient and the system predict visits to the ED for ambulatory-sensitive conditions, or predict admission from the ED to inpatient care for ambulatory-sensitive conditions or among patients with particular conditions of interest (e.g., heart failure, deep vein thrombosis, and dehydration)?
Assessment of Value
The assessment of value in health care includes cost, quality, safety, access, and patient experience.
Prescribing and Using New, Expensive Drugs for High-Morbidity Conditions
The first questions related to value centered around the effective prescribing and use of new, expensive drugs for high-morbidity conditions such as hepatitis C, multiple sclerosis, rheumatoid arthritis, and cancer. What is the epidemiology across different health systems, and how can recommendations take into account morbidity, mortality, and the effective use of limited resources?
Variability and High-Cost Imaging
What is the variability (risk adjusted) in high-cost imaging such as computed tomography and magnetic resonance imaging for patients with head trauma seen in the ED and patients with headache seen in outpatient settings (primary and specialty care)?
Overuse of Testing and Treatment
How can overuse of testing and treatment be efficiently identified and/or predicted?
Prioritization of Themes and Questions
Following the overview of the five major themes and corresponding research questions as submitted by the CDRNs, Kaushal called on participants to consider additional themes to be included (or themes to remove), additional pressing research questions, and prioritization of topics. One suggestion was the challenge of prioritizing the specific disease conditions, or clusters of disease conditions, mentioned in the major theme areas. Kaushal reiterated that the questions were organized into themes to help facilitate the meeting discussion and that some questions could easily be categorized under more than one major theme area. Participants made comments relevant to the five major themes and raised additional topics, including implementation science/iterative learning and the sustainability of PCORnet.
It was observed that answering some of the questions will require specific data elements such as social determinants and markers of behavioral health, and it was suggested that the demonstration projects might incorporate the ability to test different approaches for gathering this type of information that is not typically part of the health system. According to Kaushal, adding additional time to the patient–physician interaction for data gathering is infeasible. She highlighted the need for other, more tenable methods to increase collection of data from patients. One suggestion was that the Office of the National Coordinator for Health Information Technology (ONC) develop a star-based rating system for EHR technologies to guide health care organizations in selecting a system and that ONC collaborate with those organizations on research about the different characteristics of available EHR systems.
The importance of planning for dissemination and implementation across all of the research topics was also emphasized.
Identifying and Managing High Health Care Utilizers
David Blumenthal of The Commonwealth Fund pointed out that high health care utilizers are not a homogeneous group. The Commonwealth Fund is investing in trying to understand and segment the population of high health care utilizers and develop care delivery models that are adapted to the different segments. However, the data opportunities for studying the heterogeneity of the high health care utilizer population are currently limited to modest-sized national samples (e.g., the Medicare Current Beneficiary Survey and the Medical Expenditure
Panel Survey) and claims data. According to Blumenthal, the information available through PCORnet would be a substantial addition to defining the needs and requirements of caring for those populations. Blumenthal suggested that the topic of frail elders, discussed below in the context of special populations, also fits within the major theme of high health care utilizers. In addition to the need to address the health and well-being of the frail elderly, there is increasing public policy interest in their use of health care resources and the associated costs.
During the open discussion that followed, participants concurred that most studies are looking at all high utilizers together, and relayed an interest in looking at specific populations to try to identify which patients could become high utilizers and potentially intervene. High utilization is a problem that bridges both inpatient and outpatient services, and that it has a strong behavioral and mental health element.
Concern was expressed about the likelihood that year-long, observational studies done with PCORnet data could determine which programs work with regard to high utilizers. This is a complex problem that researchers have been working on for quite some time. Some institutions, for example, have developed disease-specific programs, often organized around Centers for Medicare & Medicaid Services (CMS) penalties, which work in the short run and prevent penalties but are costly in the long run and probably not sustainable. In contrast, characterizing the nature of the populations of high utilizers in health systems (similarities, differences, and how different programs and populations overlap) may be more practical and useful in the short run than trying to understand whether programs work. Such characterization could provide critical evidence for preparing to answer longer-term comparative effectiveness questions. Kaushal observed that this also ties in to the major theme of novel tools and methods and the topics of risk-adjustment models for high utilizers and predictors of future utilization.
Specific Populations
Several suggestions related to specific populations were raised during the course of the discussion. One suggestion was to link records from mothers and babies and study how resource utilization patterns for pregnant women are connected to outcomes for babies. Another suggestion was to look at early childhood behavioral health issues and outcomes for children. Other participants mentioned current examples of where this is being done, such as a study looking at early childhood exposure to antibiotics and subsequent development of obesity. One of the aims of that study is mother–baby linkages to understand prenatal exposures.
Palliative and supportive care for the frail elderly was raised as a topic needing attention, as was the extent of care, services, and community-based supports
required in the last decade of life. Participants also discussed long-term care; avoidable admissions and readmissions of the elderly; and the sharing of data and records among nursing homes, health systems, and primary care and other care facilities.
New Health Care Delivery Models
With regard to health care delivery models, participants suggested that a more precise distinction is needed in the proposed questions between those enrolled in an ACO or a PCMH versus those who are not. It was also pointed out that much of the discussion had been centered on hospitals and hospital systems, but that health care is most often delivered by providers who are not necessarily integrated in a hospital system; it is important to make PCORnet relevant to those providers as well. To accomplish this, it is necessary to consider what themes and questions will resonate with them as they seek to influence outcomes.
Palliative care for frail elders, discussed above as an issue of a special population, could also fit within the major theme of new health care delivery models. The issues surrounding death (at any age) were also raised as an area in need of research attention.
Novel Analytic Tools and Methods
According to Lloyd, a particular interest to Premier is risk adjustment and predictive modeling across a broad group, with the ability to overlap with the identification of subgroups of high-risk patients. Katherine Newton of Kaiser Permanente Washington Health Research Institute noted that a consistent theme among the breakout groups was having the ability to compare data across sites. It would be helpful if, for example, PCORnet could interact with the health systems to incorporate Medicare claims data and census tract data globally (rather than each health system having to do the work itself). Kaushal agreed and noted that this concept is embedded in the methodological issues but may need to be made more explicit. For example, for reliable comparisons, do at least two CDRNs have to be involved?
Assessment of Value
Also highlighted was the need for the development of measures that can be used to assess what combinations of value-based payments, team-based care, and other structural elements are most effective for patients, providers, and payers.
In considering other questions for demonstration projects, participants discussed developing a portfolio of strategies to bring down costs (e.g., in areas such as high-cost imaging, specialty drugs, oncology drugs, and high utilizers).
However, the challenges of obtaining cost data were noted. Another idea was using the Common Data Model to study various aspects that could be proxies for cost (e.g., readmissions) that might occur in association with a new care event (e.g., the availability of a new oncology service).
Implementation Science and Iterative Learning
Another point discussed is that care delivery is iterative. As such, the discussion should address not only whether these are the right themes and questions, but how the answers to the questions are best obtained. How can the dynamic, iterative nature of health care practice be taken into account in seeking answers to the questions or in defining new directions to investigate? For example, there are multiple approaches to predicting high utilizers; different researchers looking at different cuts of data will use those data in different systematic approaches to study utilization. It was suggested that, in some ways, a learning organization is an experimental model in and of itself. A learning organization incorporates new findings, learns from them, modifies the approach, and then learns and modifies again and again. Kaushal summarized that she heard calls for an increased emphasis on the implementation science aspect of the research questions, and a focus on both the process of learning as well as the outcome of a specific study.
Sustainability of PCORnet
Kaushal raised the issue of sustainability and the need for ongoing commitments to support the CDRNs and fund studies utilizing the CDRNs. There are grants and other funding opportunities, as well as support from health systems and medical schools and nontraditional sources of funding. A participant recommended thinking both locally and nationally and starting the dialogue with potential funders now to demonstrate the value of working together and the strength in numbers that comes with PCORnet. Kaushal agreed and referred back to Selby’s overview of PCORnet and the organizational structure for the demonstration projects that emphasizes the importance of bringing together multiple partners for the projects.
Participants discussed the concept of funding five short-term, specific demonstration projects versus demonstrating the value of the process by showing how the entire network could be engaged to address one or two broad questions. It was suggested that the opportunity for learning is greater with five projects than a single project, and there were concerns about the risk and implications of failure of a single project. Participants suggested that having more projects is a better approach, but cautioned against spreading projects over too many disease populations, noting that
there is a lot of alignment or overlap among the questions in the five theme areas and that spreading across too many disease areas could reduce the opportunity to demonstrate that alignment. Instead, straightforward, short-term demonstration projects addressing questions that are highly relevant to a large patient population, and that could provide actionable results, would be of value.
OPEN DISCUSSION OF NEEDS, OPPORTUNITIES, AND STRATEGIES
Selby invited participants to reflect on the discussions of the day as well as their previous interactions with PCORnet. PCORnet is a learning collaborative across the networks, and he urged participants to share their thoughts on needs, opportunities, successes, failures, and strategies that could help inform the PCORnet demonstration projects. Participants expanded their discussions on the topics of dissemination and implementation, cost/value, and sustainability, and also raised the issues of connecting health system data to payer data and training and workforce development.
Linking Care Delivery Data to Health Plan Data
Russell Rothman of Vanderbilt Health System observed a strong interest during his group discussion in expanding health system connectivity to payer data, and CMS data in particular. This could allow health systems to have a better understanding of predictors of care over time and could also expand the ability to incorporate data on social and behavioral determinants into the Common Data Model for potential use as predictors of care. Selby agreed that care delivery system data without linked health plan data hinders the ability to do certain types of research, in particular, longitudinal follow-up for outcomes. He noted that PCORnet is investing in bringing payer plans into the network. He observed that many health care systems still view health plans only as business partners, rather than also as research partners on issues of mutual interest (e.g., high utilization). PCORnet will be looking to fund projects where there is mutual interest in the questions and the outcomes and will be particularly looking to those stakeholders that can provide data.
Participants emphasized the critical importance of collaboration between and among health plans and researchers, but cautioned against a data mining approach in which researchers simply ask health plans to hand over the data. Selby agreed, and noted that the current PCORnet strategy is one of data sharing and individual-level patient linkage of data around a common question of interest to both payers and delivery systems.
TRAINING AND WORKFORCE DEVELOPMENT
Training and workforce development was discussed, and it was pointed out that training is an aspect of dissemination and engagement. A participant suggested that training and workforce development also sharpens research questions and brings diverse constituencies together in new ways. Selby agreed, and reminded participants that under the Patient Protection and Affordable Care Act (ACA), the Agency for Healthcare Research and Quality (AHRQ) was charged with building capacity for patient-centered outcomes research through workforce training programs and grants. He added that AHRQ is also interested in system-based research, training people to work with delivery system data and in partnership with delivery system leaders, and an advisory committee is exploring how to ensure that those with training and capabilities in these areas are part of the delivery system team. Another participant emphasized the value of other mechanisms for training and workforce development (beyond formal training grants) that are more modular and more accessible for a broader group of individuals.
Dissemination and Implementation
Steve Weinberger of the American College of Physicians highlighted dissemination and implementation as one of the major challenges for PCORnet. There need to be systematic ways to educate the physician community—including providers beyond the organizations that are part of PCORnet—about the results of studies coming from PCORnet. Selby responded that studies funded by PCORnet generally engage national specialty organizations or national provider payer organizations; however, he emphasized that PCORnet would look for additional ways to link to physician groups.
The goal of dissemination and implementation is for information to be used, yet much information is disseminated and goes nowhere. Participants emphasized the need for engagement of clinicians up front regarding what questions are of most interest. In order for clinicians to start putting the information into practice, they need to be assured that the data are reliable and apply across a broad population as well as to their own patients.
Veronique Roger highlighted the power of patient engagement in dissemination. She shared that, when asked what part of research they would most like to be engaged in, patients in her network overwhelmingly responded that they were keen to be involved in the dissemination of research findings. She observed that pharmaceutical companies leverage this interest very effectively with direct-to-consumer advertising that tells patients to “ask your doctor”
about whatever product is being promoted. She suggested that PCORI explore engaging patients in dissemination to help fill the gap. Selby responded that PCORI began its process with patient engagement first to ensure that it was asking the “right” questions, and then to ensure that the results would be analyzed meaningfully so that there would be buy-in among the various stakeholders. Over time, it became clear that patient engagement was also important for facilitating dissemination.
Also discussed was that health care is evolving in a digital age, and studies of systems-level interventions need to clearly define “usual care” so that future readers of the studies will understand the comparators and whether those comparators are still relevant.
High-Value Care: Prices, Costs, Access, Incentives, and Outcomes
Issues surrounding price were raised, especially price transparency from the patient’s perspective. In other words, what will health care really cost the patient in light of increased copayments and other factors? Selby noted that although PCORI cannot fund studies that directly compare costs of care, it does have an interest in out-of-pocket cost to the extent that increased cost for patients influences the ability to access care or to adhere to care, and influences the intended outcome.
The topic of cost is prominent in the news, especially with regard to drug prices. Selby observed that there are a lot of privately directed efforts to measure value and to use that value to justify price (e.g., given the effectiveness of this agent, and the availability or nonavailability of alternatives, and the development cost, what should the price of this product be?). From the PCORI perspective, Selby asserted, value needs to be measured after consideration of the full range of outcomes. PCORI promotes a broader range of outcomes assessments so that the different potential benefits and harms are understood. Value is also driven by relative worth to the patient. If, for example, a drug is given to a subset of the population that does not stand to benefit, it has no value. If it is given to people who have been shown to truly benefit, it has a much better chance of having value. According to Selby, PCORI does assess value, but it assesses the clinical aspects of value, while others consider the direct costs.
Participants also discussed the concept of price and costs as incentives or disincentives for care. It was noted that, at one time, it was thought that having a copayment engaged the patient further in terms of compliance with behavioral therapy goals. It was suggested that in developing consumer-directed health care plans, it is helpful to consider when a copayment is appropriate or not, relative to its effect on achievement of the therapeutic goal. There is much to be learned
regarding the use of incentives to reduce wasteful care and promote high-value care. What are the incentives or structures, including copayments, that promote the value of care and patient-centered outcomes (e.g., drive patients to make the choice to maintain a therapy)?
Sustainability
Participants noted that sustainability comes from partnerships among the health systems and highlighted the importance of buy-in and support from partner health systems. This comes in the form of, for example, information technology support (e.g., to meet data sharing security requirements) and time from executives and people in high-level research positions within the health systems. Steve Safyer of Albert Einstein College of Medicine commented on sustainability based on his experiences with the Weill Medical College of Cornell University NY-CDRN. The CDRN has been a very successful collaboration across five large institutions and others (e.g., community-based organizations and medical schools). He attributed this success to leadership and to an understanding that this is a time of change and, to make that change, questions need to be addressed with funding of research and implementation of findings. Regardless of how many PCORnet demonstration projects are implemented, sustainability is the biggest task because the potential for a high yield in the long-term is substantial.
Sustainability of PCORnet was a key focus during the second meeting of the series. Throughout the meeting, it was emphasized that the contributions from this community of health executives and researchers had helped PCORI develop the PCORnet Health Demonstration Project (a key emphasis of the meeting in January 2016). In his presentation, Selby reflected that, in 2014, the National Academy of Medicine and PCORI first partnered to explore the alignment of research with the pace and priorities of health-delivery centers and systems. Now, PCORI has the engagement of two major health plans as partners in PCORnet and PCORI is hopeful that both plans and systems will find opportunities to work together on issues related to performance, efficiency, and clinical effectiveness research, precisely by agreeing to share data for these purposes and participating together in identifying the questions and helping to design the research. He reflected on the importance of researcher–health executive collaboration and emphasized that PCORI has, and continues to make, an investment in PCORnet in order to create infrastructure in the form of data, people (relationships), tools, and policies to enable more rapid clinical research. However, he also emphasized that PCORI is not planning to support PCORnet alone. PCORnet is a way of doing research and he hopes that more systems and researchers join the network and that sponsors see its value.
This page intentionally left blank.























