Innovating Scholarship of Teaching and Learning in Health Professions Education: Proceedings of a Workshop (2025)
Chapter: 2 Preworkshop Session
2
Preworkshop Session
The July 16, 2024, introductory session was opened by Jonathan Amiel, director of the Office of Professionalism and Inclusion in the Learning Environment at New York-Presbyterian and professor of psychiatry, Columbia University’s Vagelos College of Physicians & Surgeons. The goals, said Amiel, were to review the history of and terms used in the Scholarship of Teaching and Learning (SOTL)1 and lay a foundation for a shared understanding of it and how it is applied in health professional education (HPE). The session featured a speaker who presented the general history of traditional SOTL, followed by a roundtable discussion in which panelists delved into its practical applications in HPE. Amiel emphasized that the goal of the workshop series was to advance health professional workforce development to improve patient outcomes.
Amiel briefly introduced participants to the origin of SOTL. The traditional model of academic scholarship, he said, has long been focused almost exclusively on basic and clinical research that is peer reviewed and published in major journals. In 1990, Ernest Boyer proposed that this concept be broadened to include other valuable aspects of work; he argued that scholarship should include four categories:
___________________
1 According to Jensen in the preworkshop, SOTL can be defined as evidence of impactful teaching that is interwoven with evidence of student learning. Importantly, it is the educator’s inquiry—and learning by the educator and learner—that drive the process, and making the results public for others to review further informs the teaching and learning content and process.
- Scholarship of discovery,
- Scholarship of integration,
- Scholarship of application, and
- Scholarship of teaching and learning.
SOTL IN HPE
Gail Jensen, vice provost for learning and assessment, dean emerita, and professor of physical therapy, Creighton University, began by sharing Shulman’s (2001) description of scholarship: “We cannot only count and name in scholarship; we can recount and teach … in recounting, we transform and connect to integrate new forms of creations what might otherwise have been experienced individually.” Shulman often said that teaching is like dry ice, said Jensen, because it “evaporates the second you stop.” Due to this ephemeral nature, Jensen said, it is necessary to codify the connection between teaching and learning by recounting and integrating the process of teaching. Boyer (1990) laid a foundation for SOTL by pushing for a broader definition of scholarship that moved beyond the “teaching versus research” dichotomy, said Jensen, and other scholars built on this work. Glassick (2000) added the importance of standards for scholarship, and Shulman (2001) emphasized the need for inquiry related to student learning and for making the evidence of student learning publicly available. The scholarship of teaching, said Jensen, is a condition for excellent teaching (Hutchings and Shulman, 1999) and facilitates the traditional process of public peer review and critique by the community. In turn, she added, SOTL leads to scholarly teaching that is grounded in evidence, arguments, methods, and values (see Figure 2-1), so there is an iterative relationship between SOTL and scholarly teaching, with each impacting the other.
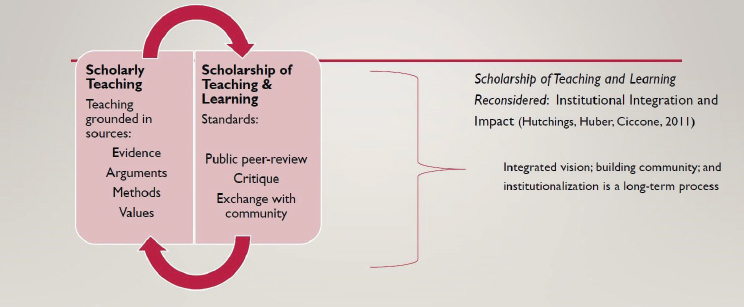
NOTE: SOTL = Scholarship of Teaching and Learning.
SOURCES: Presented by Gail Jensen on July 16, 2024; Hutchings and Shulman, 1999; Hutchings et al., 2011.
The world of HPE has a natural connection between education and practice, said Jensen. Academic and clinical communities are connected through performance-based learning and assessment. Approaches such as practice-based learning and competency-based education provide opportunities for educators and learners to engage in education while reflecting on the process and outcomes. For health professionals, the ability to make judgments in uncertain conditions is critical, said Jensen, and learning in a clinical setting allows them to think critically and practice this skill. Several unique characteristics in HPE present opportunities to use SOTL to improve education and patient care: HPE is heavily grounded in performance-based learning and assessment, the faculty are a diverse group of educators and practitioners, and learning often occurs in settings of interprofessional collaborative practice. Furthermore, said Jensen, forming professional identity is critically important for HPE learners, as is the ability to bring “head and hand and heart” together when caring for patients. HPE has rich opportunities to use SOTL to move professions forward and drive change, said Jensen; however, supporting scholarship in HPE will require funding and collaboration among educators and their leadership.
ROUNDTABLE DISCUSSION
Amiel led a roundtable discussion with panelists representing different areas of HPE. He began by asking each one to describe what successful HPE SOTL would look like from their perspective. Pamela Jeffries, dean of the Vanderbilt University School of Nursing and planning committee cochair, said that it would result in both improved learning outcomes and increased knowledge about what teaching approaches lead to them. She noted that such improvements could be measured in a number of ways, from readiness for transition to practice to patient outcomes. Grace C. Huang, dean for faculty affairs and professor of medicine, Harvard Medical School, said that just as educational research is important, educational innovations are the “bread and butter” of SOTL. HPE has had a number of notable innovations in recent years, including simulation-based classrooms, implicit bias training, and trauma-informed care. Huang noted that when authors are seeking to publish their innovative ideas in a journal, their manuscripts are much stronger if their ideas are grounded in conceptual frameworks and theories. Loretta M. Nunez, senior director of academic affairs and research education, American Speech-Language-Hearing Association, said that successful SOTL provides the evidence for educational practices that address issues in HPE. For example, HPE has embraced evidence-based practices, such as competency-based education, culturally responsive teaching, and interprofessional education (IPE). Demonstrating the value of these practices through SOTL can be encouraged, funded, disseminated, and acknowledged as a valuable contribution to HPE, she said. Yasuharu
(Haru) Okuda, forum representative for the University of South Florida Health Center for Advanced Medical Learning and Simulation, spoke last and said that while SOTL is aimed at education and training, the ultimate goal can be to use its lessons to implement evidence-based education that improves patient safety and clinical outcomes.
Benefits of SOTL
Amiel noted the competing priorities in hospitals and health systems, and HPE and training are not always the highest. However, he said, prioritizing SOTL can enhance and amplify the impact of innovations on patient outcomes. Amiel asked panelists to share examples of how SOTL has led to meaningful change in patient outcomes or care. Okuda agreed that education and training are often lower priorities and can be the “first thing to go when times are tough”; education and training are expensive, and leaders may question the return on investment (ROI). Okuda said that in response to these types of concerns, he often shares an example about simulation-based training and its impact on health care costs: Barsuk and colleagues (2009) demonstrated that deliberate practice and mastery learning improved learning and clinical outcomes. Multiple studies on deliberate practice and mastery learning in the area of central line training showed that deliberate practice improved clinical outcomes and reduced infections and other complications (Allen et al., 2014; Barsuk et al., 2014). In one study, researchers estimated the cost savings related to reduced infections after simulation-based education for residents. Taking into account the cost of implementing the program, said Okuda, they found that the net annual savings were greater than $700,000 (Cohen et al., 2010). This is a great example of how SOTL can be used to determine the best way to do training and study the impact of training on outcomes and costs, he said. Instead of “training for the sake of training,” SOTL can ensure that resources are invested in programs that lead to outcomes with a substantial ROI. Jeffries shared another example in which the value of a simulation-based training program was demonstrated. A major multi-site study of 10 nursing schools looked at whether simulations could replace hands-on clinical time without negative consequences for the nursing students or their patients (Hayden et al., 2014). The study looked at board exam pass rates and clinical practice outcomes after graduation; it had major implications for nursing education both in the United States and globally, said Jeffries. Using evidence from the study, regulators have created guidelines and standards for their states. While every state has different rules, the study suggested that simulations could replace up to 50 percent of clinical time. This example, said Jeffries, demonstrates that SOTL can have a substantial impact on not just HPE but also policies and practices that affect patient outcomes. Through these efforts, she noted,
health professionals are getting evidence on best teaching practices and better understanding of how policies and practices impact outcomes.
Challenges of Implementation
Given the potential value of SOTL, Amiel asked panelists about the challenges in implementing it in health professions schools and programs. Jeffries said that leaders—such as school deans—play an important role in propelling SOTL forward and adopting teaching approaches that are grounded in evidence. A leader can question long-standing approaches and suggest new approaches and can facilitate and encourage the key studies to gather evidence on these approaches. Some faculty may resist because they have “always done it this way,” said Jeffries, which presents an opportunity to conduct a direct comparison between existing approaches and new ones. She noted that the decision about how to teach a subject should not be based on someone’s opinion about what works but rather on evidence from a variety of sources. Sources of data for comparing educational approaches could include student evaluations, patient outcomes in practice, and metrics of successful transition from learning to practice. Success in academia can be thought of as a three-legged stool, said Jeffries; academics have a duty to excel in teaching, research/scholarship, and service. Promotion and tenure criteria are often overly focused on research/scholarship, and faculty often seek funding for research on health and medicine rather than education topics. SOTL can shift these priorities by bringing together the “legs” of research/scholarship and quality teaching. There may be opportunities, said Jeffries, to offer innovative funding to faculty to pursue research on teaching and learning to propel the field of SOTL forward. Okuda added that another challenge in HPE is that faculty and leaders sometimes assume that new technology-based teaching tools are effective and implement them without evidence that they are as good as or better than existing methods. The COVID-19 pandemic accelerated their development and implementation, he said. Okuda said that he is conducting research that compares traditional forms of teaching to tools that use extended reality, to assess whether these tools should be adopted. For example, one study compared the effectiveness of using a two-dimensional screen versus virtual reality. Virtual reality is far more expensive, he said, so there is no reason to use it if it is not more effective. He urged stakeholders to consider the marginal benefit of new technologies rather than adopting something “just because it’s cool.”
SOTL and Interprofessional Collaboration
Amiel asked panelists to comment on the value of SOTL in the area of IPE and collaborative practice. Okuda said that “everybody knows” the
importance of IPE that brings faculty and students together across professions to accelerate and improve learning. However, it can be challenging to measure the actual value of these approaches and particularly to see whether and how IPE impacts practice. This gap can be filled by further research in this area and adequate funding to support it, he said. Nunez agreed about the gap in high-quality educational research on IPE and noted that one of the ways to get this evidence is through SOTL. It is a fundamental component of the relationship between IPE, collaborative practice, and improved health outcomes, said Nunez. It has been demonstrated that high-functioning collaborative teams have a positive impact on health outcomes (Weaver et al., 2014; Wu et al., 2018), she said, and SOTL can be a means of determining and informing the best practices to prepare a collaborative practice-ready workforce. Educational research on this topic could determine the relationship between teaching practices and learning, learning and practice, and practice and outcomes.
SOTL and Faculty
While SOTL has shown value in improving education and ultimately patient outcomes, said Amiel, faculty and institutions may need additional incentives to adopt it. He asked panelists to comment on how its value could be acknowledged and enhanced in the academic world, such as in promotion and tenure. Nunez said that higher education administrators, faculty, and journal editors could better understand the different types of scholarship and their importance to the field as a whole. As Boyer proposed in 1990, scholarship is a broad term that encompasses the individual scholarships of discovery, integration, application, and teaching and learning. Leaders could acknowledge how these categories are interrelated and integrated, said Nunez. SOTL has a “huge value proposition” that is not often recognized, she said, and contributes to improving HPE and ultimately health practice and outcomes. If that connection were better understood, SOTL might be valued more. To make SOTL and its value better understood, said Nunez, it would be helpful to have a common language across disciplines. Working collectively to advocate for SOTL will “raise all boats” and make it easier to gain the support, professional development, mentoring, funding, and recognition that could propel SOTL forward. Huang added that teaching is often framed as a service and an expectation in the academic world. Promotion and tenure decisions are based on other factors, such as impact and reputation, while teaching is sometimes forgotten. Promotion and tenure committees could be better informed that success in SOTL does not necessarily result in high-impact journal publications or a high number of citations, said Huang, but instead is seen as dissemination and adoption in other institutions.
Aside from promotion and tenure, Amiel asked Huang how institutions can support faculty development for those engaged in SOTL. All institutions have faculty development, said Huang, but they do not necessarily have author or scholar development. Scholarship is a critical part of faculty development in elevating one’s impact and reputation. Devoting more resources toward educational scholarship could, for example, be used to set up writing accountability groups. Huang acknowledged that professional development is already “resource crunched” but said that an emphasis on SOTL can help recruit and retain talented educators and highlight innovative work happening in HPE institutions.
CLOSING REMARKS
The four categories of scholarship in Boyer’s framework—discovery, integration, application, and teaching and learning—are equally important and often interrelated, said Huang. The scholarship of discovery leads to new knowledge, which is expanded through the scholarships of integration and application taught through SOTL. SOTL includes forms of educational research, which is scholarship of discovery, and includes educational innovations in integration and application. Amiel added that traditional research has changed a lot over the past several decades, with a new focus on areas such as implementation science and community-based participatory research. SOTL offers an opportunity to think about how traditional research and education practices have come to be and can be improved, he said.
Jeffries noted that an essential part of a health professional’s work is the ability to problem solve and think critically; clinical care has constant uncertainty, and every patient and scenario is different. Critical thinking is a desired outcome in every HPE discipline, and SOTL presents an opportunity to determine and implement best practices for cultivating this skill. For example, said Jeffries, simulations can help students practice using their critical thinking skills in a clinical scenario and then immediately debrief with a facilitator to discuss errors or questions. She noted that finding the time for this in traditional clinical education can be challenging. SOTL is an approach for discovering and adopting such educational innovations to improve HPE and patient outcomes.
Kim Dunleavy, forum representative for the American Council of Academic Physical Therapy and planning committee cochair, closed the preworkshop session by reflecting on some of the main points of panelists and looking ahead to the workshop. One observation she noted is that SOTL can drive innovations to respond to challenges in the workplace, new technologies, and health crises. To leverage the potential of SOTL, Dunleavy commented that it would be necessary to support and train faculty,
disseminate information, and collaborate across disciplines. Furthermore, Dunleavy noted that panelists had discussed the importance of showing the ROI of SOTL and the desire for academic leaders to understand and acknowledge its value. Dunleavy expressed that the workshop would highlight and delve more deeply into what it would take for wide adoption of HPE SOTL across all the health professions.







