Fed Up!: Winning the War Against Childhood Obesity (2005)
Chapter: 1 The Fattest Generation
CHAPTER 1
The Fattest Generation
Meagan gets up early, before her father and brother are awake, and fries up a batch of soy bacon. Ten and a half years old, she is a committed vegetarian who likes the taste of meat, and she is ravenous. She washes the bacon down with a glass of water, then gets ready for school. She’s in the fifth grade at a public school about 2 miles from her home in Palos Verdes, a seaside Los Angeles suburb. Meagan has shiny brown hair in a ponytail and new glasses. Smart and funny, she’s an extrovert who loves to sing and dance and to tend goal in soccer games. Recently, though, she has gained a lot of weight, especially around her middle—a fact that has started to provoke occasional teasing by classmates and to worry her parents, both of them doctors who have been treating heart disease, high blood pressure, and other complications of obesity in adults for their entire careers.
Meagan has seen a dietitian, who taught her about portion sizes and how to rate her hunger on a scale of 1 to 10. She would like to be
leaner, to put a stop to the teasing, and to be able to move faster in soccer, but she also wants to be in charge of her own life and of what she eats. She loves sweets and can name all the doughnut and ice cream stores near her neighborhood. She’s especially partial to one ice cream parlor where you can choose your favorite candy bar or chocolate chips and they “mush it in.”
This morning traffic is bumper to bumper on the way to school. Although there’s a bike lane beside the road, Meagan rarely rides to school. Despite their concerns about the traffic, her parents have been urging her to do so for the sake of the exercise, but she has difficulty pedaling the steepest part of the route, and she can’t transport her cornet by bicycle on band practice days. Driving her to school is usually easier for her mother and father than overcoming her resistance.
The elementary school is a cluster of single-story buildings connected by courtyards and walkways, backed by playgrounds and a large grassy field for soccer and other games. After the first bell rings, students are allowed a few minutes on the playground. Meagan waits for a turn to spin on a big tire swing. Ten minutes and one spin later, the second bell sends her off to homeroom.
This morning Meagan and her best friend, Julia, are assigned a special activity: they are to research bridge design on the Internet and build an example using dried pasta and glue. Hoping to make an arch, they painstakingly glue tubes of macaroni end to end, but their constructions keep falling apart. Eventually they settle for laying out noodles side by side to make a beam bridge. Ninety minutes go by, and the girls get hungry. They munch on pieces of dried spaghetti.
At recess the two go outside to the courtyard. Julia, chatty, slender, and constantly in motion, unscrews a thermos of steaming hot chocolate and opens a plastic bag of marshmallows.
“Meagan, you want hot chocolate?”
“Mmm, tasty,” says Meagan, slurping a cupful. “Maybe we can dip the noodles.”
Friends join them and Julia passes around the marshmallows. The girls throw them in the air and catch them in their mouths. They compete to see who can do the highest cancan kicks, then the widest split. “I’m going to break my jeans if I do a split,” Meagan predicts. Instead,
she breaks into a spirited rendition of “Freedom Bound,” a song from the fifth-grade play, and the others join in. The girls end recess on a high note, dancing and shouting out the song.
Back in homeroom, Meagan’s teacher, Lydia Day, assigns a writing exercise, then conducts a poetry lesson. At 12:30 the bell rings for lunch.
The day’s main offering in the school cafeteria is a chicken leg served with barbecue sauce or ketchup. Meagan decides on the vegetarian alternative, a bean and cheese burrito. Both entrees come with hash brown potatoes, a large roll, and a strawberry ice, and students are free to complete their lunch with celery, apples, orange slices, or wilted-looking lettuce from a salad table. Meagan grabs some celery sticks and a carton of chocolate milk. She and five friends squeeze onto benches around a table. Julia passes around tortilla chips, salsa, marshmallows, and hot chocolate, collecting in return four strawberry ices. Meagan eats her burrito and hash browns, some celery and chips, and then goes back to the cafeteria to buy an ice cream bar. By the time everyone’s finished eating only five minutes of lunch period remain. Meagan and two friends head quickly for the playground and a brief tug-of-war over who will get to play with a tetherball suspended from a pole. The bell rings.
Back in class, Meagan and her schoolmates read aloud from a children’s novel, Mrs. Frisby and the Rats of NIMH, and write answers to questions on a worksheet. At 2:15 the bell rings for the twice-weekly physical education class.
“Three laps,” barks a P.E. teacher as about 100 fifth-graders spill out onto the soccer field. The kids start running around the perimeter; Meagan and her friends slow to a walk on the far side, then begin jogging as they approach the teachers. They finish their laps and a game of capture-the-flag, a chaotic form of mass tag, gets under way. The goal is to run past enemy team members without being tagged, get inside a hula hoop marking a safe zone, and capture a Frisbee. Anyone tagged goes to “jail” and waits by one of the soccer goals to be liberated. At any moment dozens of people are running in all directions while dozens of others are standing in safe territory or waiting in jail. Periodically Ms. Day yells “Jail break!” and the prisoners rush back onto the field. Meagan at one point successfully evades opposing team members and
makes it all the way to the hula hoop but can’t capture the Frisbee. When the bell rings at 3:15 she lingers for a few minutes to talk to friends before heading home.
Meagan’s street, a quiet cul-de-sac, looks deserted. Since her parents are still at work, she gets a canned juice drink from the pantry and lounges on their bed with a favorite magazine. At length, recalling that her science project is due the next day, she begins her homework. Most of Meagan’s afternoons are spent like this. She’d like to play soccer instead, but the sport is available only through after-school leagues, and girls in her age group must compete for spots. She tried out for a select team, but wasn’t chosen. There isn’t a noncompetitive soccer league for girls in the area, so for now she has no opportunity to play the game.
Meagan’s brother comes home from middle school, and her father returns from his office at a local hospital. Her dad gets out the fish that’s been marinating in the refrigerator and broils it while boiling potatoes and steaming string beans. Meagan eats a banana and requests meatless chicken noodle soup and orange juice for dinner, along with the vegetables; she doesn’t eat fish. When her mother arrives, the family sits down to eat. Finishing before her parents do, she entertains them by belting out her version of “Freedom Bound”—singing all the parts, dancing in the style of Britney Spears, and laughing uproariously. It’s the most vigorous exercise she’s gotten all day.
![]()
Compared with many kids in the United States, Meagan is lucky: she has well-educated and successful parents, she has a pantry stocked with nutritious foods, and she attends a good public school in one of the most health-conscious districts in the nation. At 10 she already knows more about the importance of good eating and exercise habits than many adults, yet like many other American kids, she is struggling with a problem that is causing her emotional distress and that may imperil her future health, a problem that poses an unprecedented threat to millions of children. She is overweight.
Throughout human history, until the end of the twentieth century, the vast majority of the world’s children have been lean. Now, all
of a sudden, at beaches, playgrounds, and amusement parks, overweight children—as well as overweight adults—are numerous and conspicuous. In the past 30 years rates of child obesity in the United States and in many other countries have soared, and diseases caused by excess weight are correspondingly on the rise, even in the very young.
As Americans, many of us have become resigned to hearing that we are citizens of one of the world’s fattest nations. Almost two-thirds of U.S. adults are overweight or obese, according to standardized definitions based on the links between excess body-fat stores and the risk of disease. We regularly read depressing new statistics about our national weight problem or listen to warnings from doctors about its likely future effect on our collective health. We feel guilty. We vow to eat less or to exercise more. Sometimes we act on those resolutions; perhaps more often we end up feeling defeated by the difficulty of making lasting changes in our habits.
But we cannot afford to remain helpless or resigned in the face of what is now happening to children and adolescents in our own country and in much of the rest of the world, including Latin America, Canada, Europe, the Middle East, Australia, Japan, India, and China. Since the 1970s the prevalence of obesity in the United States has more than tripled among children aged 6 to 11 and has more than doubled among children aged 2 to 5 and adolescents between 12 and 19. An estimated nine million boys and girls over the age of 6, representing about 15 percent of the nation’s children, are currently obese. An approximately equal number weigh more than is desirable for their health and are considered “at risk” of becoming obese. The epidemic has spread to preschool-age children, even toddlers. No group is spared: children of all races, ethnicities, and socioeconomic strata are experiencing rising rates of obesity, although African Americans, Hispanic Americans, and American Indians are among those most affected.
This unprecedented increase in childhood obesity is a true public health emergency. For many of today’s children it signals future health consequences that are likely to be far worse than those suffered by previous generations who became overweight only in adulthood. About half of obese elementary school–age children and about three-quarters of obese adolescents grow up to become obese adults who will

Trends in childhood obesity in U.S. girls and boys aged 6 through 19 years. Obesity is defined as a BMI at or above age- and gender-specific 95th percentile cutoff points taken from the 2000 CDC BMI charts.
Source: See Notes.
likely carry the burden of unhealthy fat throughout their lives, since obesity in adulthood is extremely difficult to overcome. They may become sick in their prime with diseases once associated with old age. And for many children, the medical, emotional, and social consequences of being overweight are already happening. Obese children are often teased, bullied, or ostracized by other kids and may react by losing self-confidence and becoming socially isolated, depressed, or even aggressive. Their bodies, too, are affected: a majority of overweight kids and teenagers have already developed at least one additional risk factor for heart disease, and one-quarter of them have two or more. Unprecedented numbers of U.S. children are being diagnosed with an obesity-related type of diabetes that until recently was called “adult-onset” diabetes.
Indeed, it is time to recognize obesity as a disease in its own right. Even in an otherwise healthy child, excess fat can subtly alter normal metabolic processes and may, over time, damage or disrupt the function of many of the body’s organs and systems. In adulthood, people
who remain seriously overweight have elevated rates of heart disease, diabetes, high blood pressure, high cholesterol, breathing disorders, cancer, liver and gallbladder disease, arthritis, and depression. Many of these complications of obesity are increasingly showing up in children and teenagers.
The growing numbers of obese children in the United States and in many other countries are victims of an epidemic just as surely as if they were infected with a virus. We tend to think of an epidemic as an outbreak of a contagious illness. But to public health scientists the sudden upswing in obesity rates that occurred at the end of the twentieth century is every bit as dramatic and unexpected as an outbreak of a new infectious disease and has begun to trigger the kind of alarm that might greet the global resurgence of polio. In the fall of 2003, Julie Gerberding, the director of the federal Centers for Disease Control and Prevention (CDC), the government agency best known for fighting infectious diseases and bioterrorism, declared obesity the number one health threat facing the United States.
![]()
The seventh-graders in Christine Mattis’s health class at D. W. Griffith Junior High, in East Los Angeles, have not heard the words “obesity” and “epidemic” before. Most of them come from Mexican American families, a population with especially high obesity rates. Many youngsters in Mattis’s classroom have bellies that strain the fabric of their T-shirts or spill over the waistbands of tight jeans. Mattis, an active woman in her early thirties, sometimes takes her students on hikes or field trips. She says she is shocked by their poor stamina. On this Monday morning Mattis has asked her class to write down everything they ate on Saturday. Except for orange juice at breakfast, only 2 of the 27 students list a single fruit. Vegetables, other than French fries, are also rarely mentioned; a few youngsters list salad, broccoli, or squash.
One boy writes, “Breakfast: pizza, chips, cereal, ice cream, donuts. Lunch: pizza, cupcakes, Cheetos. Dinner: pizza, soup, bread. Snacks: pizza, chips, sugar.”
A girl writes, “Breakfast: none. Lunch: hot dogs. Dinner: rice, beans, hamburger, macaroni salad. Snacks: chips, soda, ice cream, cup-cake, gum.”
During the lesson, Mattis’s students are surprised to learn that being overweight is causing health problems for kids, but when I ask them what they think might be causing an obesity epidemic in American children, they come up with plenty of theories. Their top suggestions: junk food, fast foods, candy, soda. The discussion turns to physical activity. Most of the children tell me they live close enough to walk to school. In their physical education classes, the school’s playing field is so crowded with students, and teachers are so few, that many kids spend the period standing or sitting on the sidelines.
I ask them why they suppose that kids might be getting less exercise than they did 20 years ago.
“Technology.”
“Too lazy.”
“Crime.”
“Traffic.”
“Some don’t like to go outside and play,” offers one boy. “They’re depressed.”
Just as the cause of the deadly respiratory illness SARS was unknown when it emerged in China and triggered an international epidemic in 2003, the cause of the obesity epidemic is a mystery so far. However, many people claim to know why it is happening. They look at their children’s lifestyles and point to super-sized sodas, TV and video games, and snack foods. They look at their own habits and blame their weight problem on eating too much fast food, too many sweets, or spending too much time in their cars. Chances are, they are partly right: all of these factors are likely contributors.
Americans of all backgrounds and socioeconomic groups share many aspects of the modern lifestyle: Meagan and Christine Mattis’s students like to eat sweets and high-fat snacks, sit for hours each week in front of computers or TV sets, and spend too little time playing outside. Still, no one knows for certain which aspects of our modern environment—which of the many and complex changes in most people’s diet and lifestyles during recent decades—have played the greatest role in unleashing the epidemic of excess body fat that now threatens the future health of children and adults in the United States and elsewhere.
Scientists can at least state with confidence that the causes are environmental, because 25 or 30 years is far too short a time for millions of people all over the planet to have acquired some new genetic mutation that is making them fat. Something about modern life is apparently making increasing numbers of children and adults take in more calories as fuel than they burn during their daily activities, so that the excess is being stored on their bodies as unhealthy quantities of fat. The human body has evolved extremely precise mechanisms to maintain a balance between the energy it consumes as food and the energy it expends to function and move around. It has a set of sensors and signals that keep its weight exquisitely stable over the months and years. Yet the rapid rate of change occurring in today’s environment, propelled by our actions, seems to have outpaced the human body’s ability to adapt. Our internal weight-regulating mechanisms, which evolved during our species’ long history of privation in order to protect us from starvation, have rendered us ill suited for a lifestyle that offers an abundant supply of calories and too little opportunity for physical activity.
All the same, researchers have not pinpointed which aspects of the modern environment are most responsible for rising rates of obesity. They haven’t even ruled out the possibility that the epidemic might be caused by a virus or a toxin that affects nerve cells in the brain that regulate appetite. Although such an explanation is considered highly unlikely, compared with the myriad and obvious forces in the environment that encourage people to eat more and to move around less, in the words of obesity scientist Rudy Leibel of Columbia University, “It’s a formal possibility.”
![]()
Even the words we use to talk about obesity make it difficult to confront the realities of the epidemic in children. “Obesity” is an accepted medical term when applied to adults, but pediatricians shy away from the word, perceiving it as pejorative. In pediatric journals and treatment guidelines, doctors who study and treat children use the term “overweight” rather than “obese.” I visited a specialty clinic dedicated to treating obese children that was euphemistically named the “fitness
clinic.” Because fatness is considered unattractive in mainstream American culture, many people, when discussing their own obesity or that of family members, avoid words like “obese,” “fat,” or “overweight” in favor of words they consider more tactful, such as “big” or “heavy.”
The language used by medical professionals and the public reflects unspoken social and cultural attitudes about obesity, particularly the belief that obese individuals are fat through their own fault, because they lack willpower or self-control. As I will explain in the next chapter, this belief is false.
Euphemisms prevent us from facing the situation. Americans must accept that the obesity epidemic, especially in children, is a public health emergency. To learn about it and figure out how we should respond, we need to use language that is clear and easy to understand. In 2005 a group of experts recruited by the nonprofit Institute of Medicine (IOM) of the National Academies, in Washington, D.C., offered recommendations to the federal government, policymakers, and the general public on how to prevent obesity in children. In issuing their report—Preventing Childhood Obesity: Health in the Balance—these experts consciously chose to use the word “obese” rather than “overweight.” (Throughout this book I use these two words interchangeably when discussing children who have unhealthy levels of body fat.)
What standards are used to decide whether a person is overweight? Healthy weights for children and adults have been determined by studying large population samples. Weight is not necessarily a direct measurement of body fat stores, since our bodies are made up of bone, muscle, and other tissues as well as fat. However, since it is expensive and impractical to measure body fat stores in large numbers of people, researchers and health care workers have chosen a surrogate measurement that correlates reasonably well with fat stores in all but the most muscular people. A figure called the body mass index, or BMI, has been adopted as a practical tool for determining whether a person’s weight (adjusted for height) falls within the range of weights considered to be healthy. The BMI is calculated by dividing weight in kilograms by the square of the height in meters. Charts or BMI calculators, available on the Internet, make it easy to look up the BMI that corresponds to a particular height and weight.
In studies of adults, much research data support the concept that certain BMIs fall within the healthy range while others are associated with a higher-than-average risk of illness and death. Adults who have a BMI of 30 or higher are considered “obese” and those with a BMI between 25 and 29 “overweight” because the risk of many diseases, as well as overall mortality, rises with increasing BMI, especially with BMIs above 30.
For children there are not enough data to define precisely what level of fatness begins to pose health risks or whether that level varies depending on a child’s age. The situation is complicated by the fact that as long as a child is growing, his or her BMI is a moving target: it changes continually as height and weight change. For this reason, in children, obesity (or, as pediatricians call it, overweight) is defined as a BMI that is higher than the 95th percentile for children of the same age and sex.
To establish a standard range of BMIs for children of different ages, the federal Centers for Disease Control and Prevention developed growth charts using national survey data collected during decades before the childhood obesity epidemic in the United States reached its present level of severity. When BMI measurements of a large group of same-aged boys and girls are plotted on a graph, the resulting distribution curve is roughly bell shaped. The majority of the children represented have BMIs that fall somewhere in the middle of the range, and a minority have BMIs that fall toward the extremes.
Health professionals use the CDC growth charts to determine how a child’s BMI compares with those of other children of the same age and sex. A girl’s BMI is said to be at the 50th percentile if 50 percent of girls her age have lower BMIs and 50 percent have higher BMIs. If a boy’s BMI is at the 90th percentile for his age, it means that 90 percent of boys his age have lower BMIs and only 10 percent have higher ones. For U.S. children, obesity is defined as a BMI that is higher than the 95th percentile. Children whose BMIs fall between the 85th and the 95th percentiles are considered “at risk” of obesity or overweight, which means their weight is high enough to warrant concern and possible medical treatment.
To understand the obesity epidemic in America’s children, con-
sider what has been happening to the curve representing BMI distribution during the past few decades. For children of both sexes and every age group, average BMI has increased significantly since the 1960s. But that shift in the average BMI value doesn’t mean that all kids in today’s population are heavier than kids were in the 1960s. Rather, most of the change in the curve has occurred on the right-hand side (heavier side) of the bell, which has shifted toward heavier weights, making the downward slope less steep and pushing the curve’s end farther to the right. This means that children represented by the “heavy” half of the curve have gotten heavier, while the leaner children represented by the “light” half have remained about the same. This general pattern also holds true for adolescents.
Not only are more American children and adolescents obese than in the past, but the fattest kids in the U.S. population are much more obese than ever before. These changes are not explained by immigra-
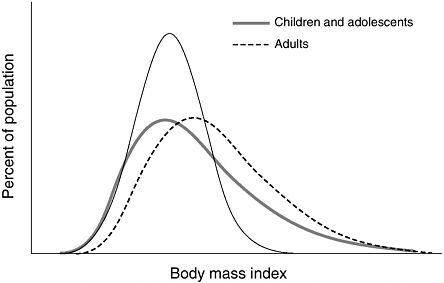
This schematic graph, although not based on actual data, helps illustrate the concept of BMI distribution shifts. The fine solid line represents a standard bell curve, where the curve’s peak represents the largest cluster of individuals. As BMI increases or decreases from this mean (midpoint), the number of individuals decreases. As seen by the dashed line, adults have grown heavier, on average, over time; but generally speaking for children and adolescents, heavy youth have grown heavier, while leaner youth have remained more or less at the same weight.
tion or other factors that have produced shifts in the racial or ethnic makeup of the population. Obesity is becoming more prevalent in all racial and ethnic groups, and the increase in prevalence seen among non-Hispanic white children is as large as that seen in other groups.
One way of interpreting the change in the shape of the bell is to say that our modern environment is “obesigenic”: it’s making an increasingly large fraction of the population gain too much body fat, and it’s making that weight gain begin at younger ages. Children whose genes make them moderately vulnerable to obesity, children who probably would not have been overweight in the United States of the 1970s, are becoming overweight today. And those kids with the greatest genetic vulnerability to obesity, who probably would have been fat back then, are gaining much more body fat in today’s environment than they would have in the past. This shift toward greater degrees of fatness may help to explain why diseases that were once considered “adult-onset” complications of obesity are now showing up in so many children.
The pattern is somewhat different for adults. The BMI distribution curve for adults has shifted entirely to the right, meaning that virtually the whole population has been affected. Men and women of all ages tend to be heavier today than U.S. adults were during the 1960s. But as in children, the increases in BMI in recent decades have been most dramatic among those adults whose BMI falls on the “heaviest” part of the curve, meaning that the number of severely obese adults in the population has greatly increased.
“We don’t really know the magnitude of the health effects here, because we have never before in history had a population that was this overweight,” notes obesity researcher Steven L. Gortmaker of the Harvard School of Public Health.
Because being obese threatens the health of affected children, part of our nation’s response to the epidemic must include more aggressive efforts by health workers to identify, counsel, and treat children (and the families of those children) who are already overweight or who are at risk of becoming so. Treatment for obesity is more likely to succeed in children than in adolescents or adults, especially if it is started early, before a child has become very overweight. But the childhood obesity epidemic cannot be reversed by relying on medical treatment alone. It’s easy to understand why if we consider once again what’s been hap-
pening to the bell-shaped curve of children’s BMIs. The increasing trend toward unhealthy weight gain already affects a sizeable percentage of U.S. children; it is a populationwide phenomenon caused by common factors in our environment, and fixing it will require a populationwide response. Simply focusing on treatment for those kids who are already obese, although vitally important, will not be enough to halt the epidemic, because the percentage of children who are overweight has been rising steadily and that trend shows no sign of slowing down. For every overweight child who is treated, additional children will become obese, eventually overwhelming treatment resources. To halt or reverse the epidemic, we must focus on preventing obesity by favorably changing the environment for all children—for those who are already overweight and for those who are not.
Our desire for a just and equitable society is also a compelling reason for taking populationwide measures. Children of various racial and ethnic groups show dramatically different obesity rates, even though (as I mentioned previously) the prevalence of obesity has been increasing steadily for all groups. This fact probably reflects differences in genetic vulnerability to weight gain, as well as social and cultural differences in children’s environments. For example, 46 percent of African American girls aged 12 to 19 are overweight or at risk of becoming so, compared with 25 percent of white girls in the same age group. Among kids of both sexes between the ages of 6 and 11, 40 percent of Mexican Americans and 36 percent of African Americans are overweight or at risk of becoming overweight, compared with 30 percent of whites. The prevalence of obesity among 7-year-old American Indian children is estimated to be almost 30 percent, about twice as high as the prevalence among all U.S. 7-year-olds. These large differences are linked to similarly large ethnic and racial disparities in the risk in adulthood of developing diabetes, high blood pressure, cardiovascular disease, and other obesity-related illnesses. In our obesity prevention efforts we must pay special attention to children who belong to racial and ethnic groups at highest risk.
A child’s chances of becoming overweight also appear to be greater if that child is poor. Obesity rates among adults in the United States have increased most rapidly during recent decades in states with the
lowest per capita income. Among women, food insecurity (being unsure of having enough to eat, or not having enough of the kinds of food desired) has been shown to be linked with being overweight. Foods that are “energy-dense,” providing many calories per pound because of their high sugar or high fat content, are much cheaper than non-energy-dense foods such as fresh fruits, fresh vegetables, and whole grains—the very foods recommended as the basis of an optimally healthy diet. Processed foods also have a longer shelf life than fresh ones. Epidemiologist Adam Drewnowski of the University of Washington argues convincingly that the higher rates of obesity seen among poor populations may reflect the fact that it is far cheaper to eat an unhealthy diet of predominantly energy-dense foods, high in fats and sugars, than it is to eat a “healthy” diet. However, it’s probably much more difficult to avoid ingesting too many calories on the energy-dense diet. In addition, low-income neighborhoods often lack access to supermarkets, farmers markets, and other sources of fresh, unprocessed foods, and children in such neighborhoods may not have safe places to go to burn off extra calories through physical activity.
![]()
What does the future hold for our nation’s children if we do not act to halt the obesity epidemic? Obesity in adults is the number two preventable cause of death in the United States, second only to tobacco use. During the 1990s researchers estimated the annual number of deaths attributable to obesity and lack of physical activity at about 300,000. In the face of steadily rising obesity rates, epidemiologists at the CDC published an updated estimate in 2004 that placed the annual toll of obesity and inactivity at 400,000 deaths per year—and predicted that obesity would soon overtake smoking as the nation’s leading cause of preventable death. Although other researchers have criticized the statistical methods used to arrive at this revised estimate, obesity is clearly a major contributor to preventable illness and death.
The direct and indirect medical costs of obesity currently consume about 10 percent of the U.S. health care budget, a percentage that is expected to continue to rise. Overweight people have high rates of diabetes, high cholesterol, high blood pressure, atherosclerotic heart dis-
ease, gallbladder disease, and osteoarthritis. Almost 80 percent of obese adults in the United States have one of those conditions, and almost 40 percent have two or more. Obesity is also a risk factor for stroke, congestive heart failure, liver disease, musculoskeletal problems, several kinds of cancer, breathing disorders such as asthma and sleep apnea, and infertility in women, as well as for depression and other psychiatric illnesses.
Until recently, most of our knowledge of the medical consequences of being overweight has come from studies of adults. But in the past two decades, doctors treating the growing numbers of fat children in our society have begun to find cases of what were formerly considered “adult” obesity-related diseases occurring in overweight teenagers and even in kids as young as 6 or 7 years old. The cost of hospitalizations of children aged 6 to 17 for obesity-related illnesses tripled between 1979 and 1999. Meanwhile, a growing body of epidemiological research suggests that childhood obesity by itself may shorten a person’s life expectancy, whether or not the individual remains obese as an adult. Such findings underscore the urgency of intervening to prevent obesity in children and treating it when it is present, in order to maximize children’s chances of living a long and healthy life.
More than any other factor, it is the rapid rise in type 2 diabetes among children and teenagers that has awakened doctors and health officials to the grim future consequences of the obesity epidemic. In just 12 years, between 1982 and 1994, the incidence of this type of diabetes in children rose tenfold, according to a report by Cincinnati researchers. Type 2 diabetes is a consequence of obesity. Once rare in children, this kind of diabetes now accounts for at least one-third of new cases of diabetes in adolescents—and in some populations up to one-half of new cases. Thirty percent of boys and 40 percent of girls born in the United States in 2000 will become diabetic at some point in their lives unless current obesity trends are reversed, according to projections by epidemiologists at the CDC. Among African American and Hispanic children, almost half will develop diabetes.
Diabetes is a disease in which the body doesn’t produce enough insulin, a critically important hormone that regulates the concentration of blood sugar (glucose)—the body’s major source of energy—
and directs its use and storage by tissues such as liver and muscle. Unlike someone with type 1 or “childhood” diabetes, a person with type 2 diabetes still makes some insulin, but having too much stored fat renders the body insensitive to the hormone’s effects. Type 2 diabetes develops in part because this extra fat tissue puts excessive demands on the body to make insulin, resulting in “insulin resistance.” When insulin resistance occurs, specialized cells in the pancreas called beta cells must churn out extra-high levels of the hormone in response to the rise in blood glucose that takes place when a person eats. Eventually the beta cells can’t make enough insulin to lower the blood glucose level to within the normal range. Chronically high glucose levels ultimately destroy beta cells, the only cells that can manufacture insulin. Over a period of years, type 2 diabetes causes just as much mayhem to tissues as type 1 diabetes. In both types, high blood glucose levels and other metabolic abnormalities eventually produce damage to blood vessels and nerves, sometimes leading to blindness, kidney failure, heart attack, stroke, and amputation of the feet or legs. Indeed, type 2 diabetes may be a more rapidly progressive disease in children than in adults. Because the frequency of complications is also related to the duration of the disease, experts fear that many obese youngsters now developing type 2 diabetes may suffer heart attacks or other complications by the time they reach their forties.
Although the increase in type 2 diabetes drew attention to the potential impact of the obesity epidemic on children’s health, diabetes is only one component in a web of linked derangements of metabolism that obesity can produce in a child or an adult. Doctors and researchers use the term “metabolic syndrome” to refer to a pattern of abnormalities that often occur together. The metabolic syndrome includes five possible features: abdominal obesity, high blood pressure, glucose intolerance (a prediabetic condition in which insulin levels, although high, are insufficient to handle glucose normally), a high blood level of triglycerides (a fat present in the circulation), and a low blood level of high-density lipoprotein or HDL cholesterol (sometimes nicknamed “good” cholesterol because it helps protect against blood vessel damage). A person who has at least three of these five features is said to have the metabolic syndrome.
Having too much fat tissue contributes to development of the metabolic syndrome. Fat cells, once considered inert little bags of oil, have been discovered to make an array of hormones used to communicate with the brain and with other tissues and organs. Some stored fat is necessary for health, but an excess of it, particularly in certain locations, can be life-threatening. Visceral fat, located inside the abdominal cavity, is considered the most metabolically active fat in the body. It produces a somewhat different mix of hormones than fat tissue found elsewhere, and the chemical messages it releases into the circulation travel directly to the liver and other nearby organs, influencing their function.
Research evidence now suggests that disorders such as diabetes, high blood pressure, and heart disease, instead of being separate and unrelated problems, are really interconnected diseases that can all be caused by the metabolic syndrome. Even several years before developing overt diabetes, many obese children already have undiagnosed glucose intolerance as well as other features of the syndrome. Almost 30 percent of overweight children between the ages of 12 and 19 in the United States, and about 4 percent of all U.S. teenagers, have the metabolic syndrome, according to a recent study of a national sample of adolescents. The syndrome is also appearing in younger kids: in fact, doctors who treat pediatric obesity have diagnosed the metabolic syndrome in children as young as 5 years old.
In parallel with the nationwide increases in obesity and in metabolic syndrome, a recent national study found that between 1988 and 2000 the average blood pressure of children in the United States edged upward by a couple of points, a seemingly small shift that nevertheless places many more kids at risk of developing high blood pressure as young adults. Researchers have also documented worrisome changes in the hearts and arteries of obese children, including thickening of the walls of carotid arteries—large vessels that supply blood to the brain—in children as young as 9 years old. Findings such as these may be early warnings of a future surge in adult cases of heart attack, stroke, kidney failure, and other illnesses that seem an almost inevitable consequence of the current epidemic of obesity in children. Some experts have speculated that today’s kids may be the first American generation to live shorter lives, on average, than their parents.
![]()
Once a boy or girl is overweight, what are the chances of ultimately becoming a lean adult? And what’s the evidence that being fat as a child does any lasting damage to health?
Not all fat children grow up to be fat adults. In addition, overweight kids are not all at equal risk of developing medical problems. An overweight child’s risk of adult obesity, as well as his or her risk of diabetes, high blood pressure, or other disorders, varies depending on the child’s age, racial or ethnic background, and other factors, particularly whether one or both parents are obese and whether there is a family history of obesity-related illnesses.
In the United States today, most obese adults were not obese as children. About two-thirds of people who are overweight or obese as adults were not overweight during the first 20 years of their lives. That pattern may change in the future, however, since so many more children are overweight today. A key 1997 study examined the risk of adult obesity for kids who were fat at different ages. It found that among children under 3 years old, being fat by itself does not significantly increase the likelihood of becoming a fat adult. But after the age of 3, the older an obese child is, the greater the likelihood that obesity will persist. After age 6, the probability of an obese child becoming an obese adult is greater than 50 percent, compared with about 10 percent for non-obese children. The risk of adult obesity rises higher for kids who are obese after the age of 10. In addition, the more overweight a child is, the greater the chance of being obese as an adult.
Having one obese parent also was found to multiply a child’s risk of adult obesity about twofold to threefold, compared to that of a child with two lean parents. If both parents are obese, the child’s risk is further increased. The authors of the study suggest that children between the ages of 3 and 9 who are overweight, especially those who have at least one obese parent, “may be ideal candidates for treatment because the parents still have the opportunity to influence their children’s activity and diet positively.” A child of any age and body weight whose parents are both obese should probably receive particular attention in order to establish a healthy diet and physical activity habits before obesity develops.
How does being fat affect a child’s life expectancy? Clearly, part of the answer depends on whether obesity persists into adulthood, since the longer a person is significantly overweight as an adult, the greater the risk of medical complications such as heart disease, diabetes, and cancer. But a growing body of research indicates that childhood obesity by itself may shorten life span.
The Harvard Growth Study described death rates and disease patterns during the course of a half-century in 508 people who had enrolled in the study as teenagers between 1922 and 1935. At enrollment they were classified as “lean” if their BMI fell between the 25th and 50th percentiles; if it was greater than the 75th percentile, they were classified as “overweight.” Among the men in this study—but not the women—being overweight as a teenager was associated with a higher mortality rate in adulthood from all causes. The men who had been overweight as adolescents had a death rate almost twice as high as those who had been lean, and their death rate from heart disease was more than double that of their lean counterparts. The frequency of heart disease was greater in both sexes among people who had been overweight as teenagers. The men who had been overweight adolescents had higher rates of colon cancer and gout; the women had higher rates of arthritis. These findings were independent of adult weight. In other words, people’s risk of developing these diseases was more closely linked to whether they had been fat as teenagers than to whether they were fat as adults. The sex difference in mortality rates seen in the Harvard Growth Study is puzzling but may only be a statistical artifact.
Recently a much larger study found that being overweight in adolescence affects adult mortality rates about equally in both sexes. In that study, Norwegian researchers tracked the health of 227,003 adolescents aged 14 to 19, whose height and weight were measured between 1963 and 1975. Participants were followed for an average of 31 years. Men and women whose BMI as teenagers fell between the 85th and 95th percentiles (a category U.S. pediatricians currently term “at risk of overweight”) had a death rate as adults that was 30 percent higher than that seen in people of the same sex who had been lean adolescents (BMI between the 25th and 75th percentiles). Among women whose BMI as teenagers was above the 95th percentile (classi-
fied under current U.S. pediatric standards as “overweight”) the adult death rate was twice that of women who had been lean; among men who had been similarly overweight as teenagers, the adult death rate was almost twice as high as for men who had been lean. Interestingly, the difference in death rates remained small and not statistically significant while participants were in their twenties. The impact of adolescent overweight on adult death rates did not become sizeable until study participants were between 30 and 58 years old.
This study offers powerful evidence that being fat in the teenage years has a lifelong effect on health. The finding of higher death rates among people who had been overweight teenagers was independent of participants’ adult weight. Since deaths among young adults are rare, it required a very large and carefully conducted study, lasting for decades, to show this impact. The Norwegian study had remarkably complete follow-up: out of more than 227,000 participants, the status of only 33 was unknown at the study’s end. However, the researchers were unable to collect information about causes of death or about other potential risk factors such as smoking, lack of exercise, and socioeconomic class.
So far it has been difficult for researchers to determine whether the impact of obesity on life expectancy differs among racial and ethnic groups. One recent study of U.S. mortality data concluded that being severely obese as a young adult reduces life expectancy more in black men than in white men, but more in white women than in black women. These findings, however, have been criticized on various technical grounds (for instance, failure to make statistical adjustments for lower socioeconomic status, which also reduces life expectancy). As yet, few studies have addressed the same question for Hispanic Americans or American Indians, although these groups have a high incidence of obesity and diabetes.
What is clear, though, is that obesity increases the risk of many specific diseases, such as diabetes and high blood pressure, in people of all racial and ethnic groups. Conversely, weight loss has been shown to reduce the risk of diabetes, high blood pressure, and various other diseases among overweight people of all racial and ethnic backgrounds who are not yet sick and to improve health for those who already have such disorders.
![]()
Bruce and his mother, Lottie, have radically changed their family’s environment. They did it a few months ago, after Bruce, who is African American, was diagnosed at age 18 with high blood pressure and was sent by his pediatrician to a Charlottesville, Virginia, clinic that helps children lose weight. Obesity runs in Bruce’s father’s family, and Lottie considered Bruce’s diagnosis a wake-up call. Bruce and his mother and sisters still live in the same small brick house in a modest neighborhood on the east side of town. And Bruce, a shy, round-faced boy with oval glasses, still goes to technical school each day, studying to get his high school degree and be certified as an auto mechanic. But the dishes in the cupboards, the snacks and drinks in the refrigerator, and the family routines—even the way the kids watch television—are all new.
Lottie gave away her tall glasses and bought short ones that hold only 8 ounces. She bought plastic plates that are subdivided into three sections, with the biggest section—occupying half of the surface area—reserved for vegetables. She stopped purchasing fried potato chips and corn chips, opting instead for rice cakes and single-serving cups of nonfat yogurt with fruit. She switched to low-fat milk and diet sodas instead of regular soft drinks, and she stocks up on fresh fruit, whole wheat bread, and multigrain cereal. She’s cut back on trips to fast food restaurants and orders pizza only on rare occasions.
At the clinic, the dietician gave Bruce a pedometer to clip onto his belt so he could count the number of steps he took each day. He started walking up and down the stairs during commercials while watching television to try to reach his daily goal of 7,000 steps. He began working out on the family’s manual treadmill or doing aerobics along with the exercise shows. His older sister, Latoya, enticed him outside on sunny afternoons to shoot baskets at the hoop up the street. Sometimes Lottie and all three of her children went to the local high school and walked around the track.
During the first month in his new home environment, Bruce lost 6 pounds. His mother and sisters lost weight too. In the months since, Bruce has continued to lose fat and to add muscle. His blood pressure has come down. Even more important, the foods and drinks he chooses, his portion sizes, and his exercise habits have all been trans-
formed—probably for good. He no longer eats French fries or drinks soda for lunch at school. He still hates to run around in hot weather, but he has far more energy and he has slimmed down so much his mother had to buy him a new wardrobe.
What is heartening about Bruce’s story, and about the stories of other families whose children are being treated at the Charlottesville clinic, is that they prove it’s not really so hard to change an overweight child’s environment and to see big improvements in habits and overall health. Bruce’s experience is not unique. Staff members at the clinic say that as they monitor their young patients, they see pants sizes changing and laboratory results improving even before kids’ weights start to go down. Simply providing a better diet and getting children to be more physically active is enough to start to build stronger bodies and reverse some of the incipient medical problems caused by excess weight.
Most parents are eager to take action when told their child is sick. It’s much more difficult to persuade families to make major alterations in their lifestyle when children seem to be well, merely to prevent disease sometime in the future. Yet that’s what we must do. When doctors and public health officials tell us that almost one-third of our children are sick with obesity or are at risk of becoming so, it’s time for us to change our children’s environment, both inside and outside the home, in ways that will help them build leaner and healthier bodies.
Changing the environment for our entire society will mean changing prevailing attitudes and social norms in much the way they have changed with regard to smoking. Addressing the obesity epidemic will be much more complicated than that of tobacco-related illness, however. For tobacco, the solution was obvious: simply reduce the percentage of people who smoke, chew, or sniff the substance. Still, there is a positive side to the fact that there appear to be many contributors to the increase in childhood obesity. It means there are many ways of taking action to improve children’s habits and environment. Even as we wait for clearer scientific answers to the question of which factors are most responsible, we can act on the information we already have to try to improve the health outlook for all children.
Preventing Childhood Obesity: Health in the Balance, the 2005 IOM
report, contains a road map for action at home, at school, in the community, and at both state and national levels. For parents, key recommendations include providing healthy food choices and modeling healthy eating; encouraging children to be physically active for at least an hour a day and maximizing the time they spend outside; and carefully limiting how much time kids spend watching television or using computers and video games. It advises that all foods and beverages sold or served in schools meet new government nutritional standards and recommends the overall improvement of their nutritional quality. In addition, schools should provide a minimum of 30 minutes of moderate to vigorous physical activity and expand opportunities for kids to play sports and be active both at school and in child-care or after-school programs. The report endorses efforts to make neighborhoods more walkable, bikeable, and exercise-friendly and to promote broader access to fresh, healthy foods and to exercise or recreation facilities, especially for children and adolescents in urban or low-income communities that often lack such resources.
It also calls for campaigns on the local and national levels to educate children and teenagers about how to make healthy dietary choices and about the importance of daily activity. And it sounds alarms about the potential long-term damage being done to children’s health by our nation’s food industry through ubiquitous, child-targeted marketing and advertising of high-calorie, high-sugar, and high-fat foods and drinks, and by the entertainment industry’s promotion of video games, television shows, and other sedentary activities. It recommends the development and implementation of new national guidelines to reduce the role of such advertising in promoting childhood obesity and calls on Congress to give the Federal Trade Commission (FTC) the authority and funds to monitor advertisers’ compliance with such guidelines.
In this book I provide an overview of current scientific understanding about what factors in the environment are contributing to the epidemic of obesity in children and offer suggestions about what parents and other adults can do to prevent kids from becoming overweight. In the next chapter I explain what we know about genetic vulnerability to obesity and about how the human body regulates its appetite and energy expenditure to maintain a constant weight.
Chapter 3 examines the complicated relationship between children’s weight (or BMI) and body image, as well as the effect of being overweight on a child’s mood and relationships with other kids. It includes advice for parents and others on how to address a child’s weight as a medical issue without damaging self-esteem.
Chapters 4 and 5 focus on fostering healthy eating habits in kids and on promoting physical activity. Chapter 6 explores recent evidence that children’s food preferences, calorie intake, and even their bodies’ innate ability to regulate weight and appetite are influenced by their environment in the uterus before birth, as well as by choices that parents make regarding breastfeeding and infant feeding during the first year of life.
Chapter 7 deals with making our schools a healthier environment for children and especially describes efforts to make the kinds of food and drink sold at schools more consistent with the nutrition lessons that are being taught in classrooms.
Chapter 8 offers information on finding good treatment for an overweight child, including specialized programs for children who are severely obese. It also examines the ongoing debate about the long-term risks and benefits of weight-loss surgery and about whether such procedures should be made available, in certain cases, to adolescents.
Chapter 9, the last chapter, suggests ways people can work to prevent obesity at the community, state, or national level. It is followed by a list of resources for readers who want to explore opportunities for political action or learn more about specific aspects of childhood obesity.
If we do not try to turn back the childhood obesity epidemic the consequences will be dire. As David L. Katz of the Yale School of Medicine puts it, “Children growing up in the United States today will suffer more chronic disease and premature death because of the way they eat and their lack of physical activity than from exposure to tobacco, drugs, and alcohol combined.”
If you want to protect children—your own and those of others—from the greatest threat to their future health, start now.