Valuing America's Health: Aligning Financing to Reward Better Health and Well-Being (2024)
Chapter: 3 Prioritizing Whole Person and Whole Population Health and Well-Being
3
PRIORITIZING WHOLE PERSON AND WHOLE POPULATION HEALTH AND WELL-BEING
This section presents illustrative examples of innovative payment and delivery models centered on improving whole person and whole population health and well-being, and that represent key areas of progress aligned with the six key pillars of the Steering Group’s vision described in Chapter 2. In doing so, this chapter aims to:
- demonstrate that U.S. health system alignment with whole person and whole population health is achievable;
- provide insight into the core elements essential to the success of innovative models; and
- illustrate the positive health outcomes and savings that payers, providers, individuals, and populations can achieve through a whole person, whole population health approach.
Each of the models described in this section has a unique set of characteristics that can be scaled and replicated across the nation to produce outcomes that are aligned with the six core pillars listed in Box 2. The most critical of these elements are described below. However, it is essential to note that the key factor undergirding each pillar is the prioritization of person-driven supports for health: empowering individuals to make decisions about their health and well-being within a trusted provider relationship, health care setting, and their communities.
The Steering Group also derived key lessons from the successes of the models described in the chapter. The following core elements provide the foundation for future efforts to achieve the vision for whole person and whole population health:
- Aligning financing across payers toward the same goals in a consistent and sustainable way
- Leadership and structured payment methodologies to incentivize providers and health systems to design and implement multidisciplinary, team-based, and person-driven care to reinforce accountability for whole person and whole population health
- Addressing the medical and social needs of individuals and populations across the care continuum to achieve equity across different populations
- Respecting and centering the whole person to consider their culture, family, caregivers, individual needs, preferences, and decisions in the provision of care
- Improving patient engagement and satisfaction, health outcomes, utilization of health services, and ensuring continuity of care in the design and implementation of health systems
- Providing services and supports using integrated, innovative, and accessible technology and delivery systems to improve the quality of care through an increased continuum of care, clinical integration, and increased access to services
Although the models described in this chapter do not fully achieve and embody every pillar of the vision as described, they are steps in the right direction. Additionally, each example can act as a case study that engages varying systemic levers to create progress within the present system. Despite the creative attempts and advances in the examples presented below to address systemic issues, they indicate that much progress needs to be made toward whole person and integrative care, which is necessary to address the nation’s health crisis.
Key Pillar 1—U.S. health status is at least that of other middle- and high-income countries, with inequities eliminated.
By prioritizing person-centered care, both the Nuka System of Care and the Veterans Health Administration’s (VHA’s) Whole Health System of Care demonstrate the importance of providing personalized care that addresses patients’ concerns, improves health outcomes, and mitigates inequities. The lessons of these models—if more broadly scaled as part of a whole-of-society effort to center whole person, whole population health as the nation’s primary goal—would transform health care and public health by focusing on disease prevention, health promotion, and comprehensive care delivery, thereby improving overall health outcomes. Additionally, by incorporating social, environmental, community, and individual factors influencing health, both the Nuka System of Care and the VHA Whole Health System of Care help target the unique and heightened needs of underserved populations and communities nationwide.
SOUTHCENTRAL FOUNDATION’S NUKA SYSTEM OF CARE
Southcentral Foundation’s (SCF’s) Nuka System of Care, commonly shortened to Nuka, is a whole person–centered health model in Alaska that uses a relationship-based and customer-owned approach to transform health. Nuka provides integrated health services, including medical, dental, behavioral, traditional, and support services to more than 65,000 Alaska Native and American Indian people with a mission of “working together with the Native Community to achieve wellness through health and related services” (Southcentral Foundation, n.d.). The system of care serves 227 federally recognized tribes whose members live in urban, rural, and remote settings across a 108,000-square-mile area (nearly three times the size of Texas).
Implemented following state legislation passed in the late 1990s that allowed Alaska Native populations to take greater control over their health services, Nuka embodies several key features that set it apart from traditional health care models (The King’s Fund, n.d.). First, the Alaska Native–owned system emphasizes the community taking ownership of health care, referring to patients as customer-owners. At a system level, customer-owners provide guidance to SCF on system improvement and the development of new programs and services. At an individual and family level, customer-owners drive their health by making informed decisions about health care treatments (Gottlieb et al., 2008). Customer-owners’ needs, goals, and values are the system’s focus, and they are in control and make decisions rather than a clinician deciding the best treatment. Customer-owner input is routinely solicited through surveys, focus groups, and telephone hotlines (The King’s Fund, n.d.).
To ensure the Native community achieves wellness, Nuka uniquely integrates a wide range of professionals in teams providing services such as home and outpatient primary care, dentistry, residential and outpatient behavioral health, traditional healing, integrative medicine, and health education. Across these multidisciplinary care teams, Nuka serves as an administrative conduit that facilitates human resources, information technology, compliance, grants, communications, finance, facility maintenance, and quality management. Cultural recognition and respect are core tenets of this strategy, which is emphasized by appropriate cultural competency training for new employees (Gottlieb, 2013).
In practice, Nuka’s management, culture, and technology have removed barriers to quality care for Alaskan communities. The system deploys clinical teams via air or boat to deliver its services in remote areas; utilizes telemedicine to consult on assessment and treatment; and supports the necessary digital infrastructure to collect, aggregate, and share data across care teams to enable complex case
management, such as when customer-owners require transportation from a rural community to urban Anchorage for tertiary and specialty services (Gottlieb, 2013).
The outcome improvements behind their numerous awards exemplify the results that a focus on whole person, whole population health can achieve. As of 2013, more than 95 percent of the Alaska Native population was empaneled to an integrated primary care team that understands their histories, preferences, and family context—a stark contrast to the mere 30 percent of the Alaska Native population that had a designated primary care provider in 1996 (Gottlieb, 2013). Additionally, 96 percent of customer-owners reported having input into their care decisions, and 94 percent reported feeling that their culture and traditions are respected (Southcentral Foundation, 2017). More traditional clinical measures of success include:
- Wait times to schedule a routine appointment decreased from 4 weeks to same-day access to a clinician via phone, email, and, if applicable, in-person (Gottlieb, 2013).
- A 40 percent reduction in emergency room visits, 53 percent reduction in hospital admissions, and 65 percent reduction in specialty care usage between 2000 and 2017 due, in large part, to same-day access to care to proactively treat medical conditions before they require more complex care (NIST, 2017).
- 75th-90th percentile rankings for Healthcare Effectiveness Data and Information Set quality measures for diabetes care, cardiovascular LDL, cervical and breast cancer screenings, outpatient and emergency room visits, and pediatric immunization and HPV vaccination rates (Southcentral Foundation, 2017).
- 97 percent of customer-owners and 95 percent of employees reported being satisfied with their experience (Business Insider, 2018).
Although the program has been successfully implemented and measured, the diverse funding sources are a challenge to replicate in non-tribal health care settings, where the same mix of funding sources may not overlap. SCF uses key elements of accountable care organizations (ACOs) to operationalize its services, with third party payers such as Medicare, Medicaid, and some private insurers providing approximately 48 percent of its operating revenue (Salinsky, 2017; Southcentral Foundation, n.d.). The federal Indian Health Service makes up the majority of the remainder, providing approximately 45 percent through a payment mechanism similar to a block grant that is not based on the volume of services (Salinsky, 2017). The remaining 5 percent comes from grants and 2 percent from investment and other sources (Salinsky, 2017).
Nevertheless, this model exemplifies the benefits of a relentless focus on individual experience and centricity—from cost savings to health outcomes and overall well-being (Salinsky, 2017). The model’s outcomes also demonstrate the benefits of transforming systems; the Nuka System of Care realigned financial incentives toward prioritizing access to primary care and a wide continuum of services and supports such as behavioral health services. A cultural transformation was also implemented, with patients recognized as “customer-owners” with unique experiences, contexts, and preferences (Salinsky, 2017).
VETERANS HEALTH ADMINISTRATION’S WHOLE HEALTH SYSTEM OF CARE
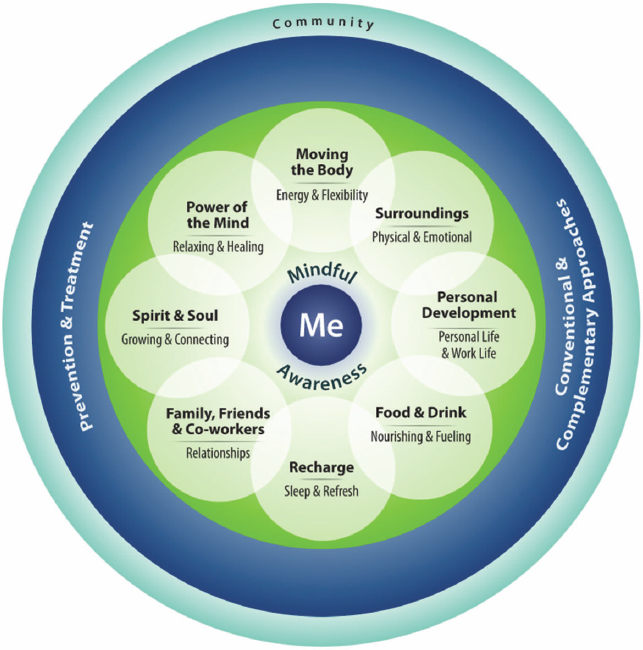
The VHA funds and promotes the Whole Health System of Care (WHS), an advanced form of patient-centered care that empowers veterans to become engaged in their own health and well-being. The approach shifts the traditional conversation with each patient from “What is the matter with you?” to “What matters to you?” (Bokhour et al., 2020a). Complemented by a robust online resource and information center, veterans engaged in the WHS establish their own personal health plan based on a personal health inventory created via self-assessment. This allows veterans to create individualized sets of services and supports based on what matters most to the individual (VA, 2022).
A central feature of creating the personal health plan involves veterans considering the VA Circle of Health, which illustrates the connections between an individual, their clinical health, their well-being, and the healing relationships, environment, and community that surrounds each aspect (see Figure 3). This tool can be used to help individuals to determine their current position relative to their health, their personal goals, the actions they can take, and the interventions that can help them achieve their goals (VA, 2021).
In the WHS program, allopathic medicine and behavioral medicine are combined with an integrative set of health interventions, each structured to meet the priorities and goals of individual patients. Key services at the core of WHS include:
- Personalized health planning helps individuals to identify the health foci most important to their own personal goals;
- Peer-led whole health courses build a community of veterans working toward whole health; and
- Whole Health Pathway services, well-being programs, and coaching to support veterans working to achieve their whole health goals.
SOURCE: VA, 2021.
Veterans engaged in WHS are encouraged to explore complementary services as well, including chiropractic care, massage, acupuncture, yoga, tai chi, meditation, guided imagery, biofeedback, and hypnosis as possible ways to exercise, reduce stress, and recover from injuries.
Access to WHS services is provided through online resources such as telehealth and a robust set of digital resources that have been in place since before the COVID-19 pandemic. In 2019, more than 10,000 complementary and integrative health visits were had among almost 4,000 veterans, a four-fold increase in usage since 2018 (Whitehead and Kligler, 2020). In response to the COVID-19 pandemic, the utility of this approach was fully realized and implemented, with WHS sites using telehealth to conduct patient wellness calls and institute self-care strategies, complementary and integrative health therapies, and stress-management tools for providers and patients alike. The utility of these strategies for staff as well as veterans was a key tool to combat the clinician burnout that has accompanied the many tragedies of the COVID-19 pandemic. In doing so, it
allowed for a healthier, more resilient workforce, empowered to provide for the individuals they serve (Reddy et al., 2021).
In 2018, the VHA launched 18 Whole Health Flagship facilities to evaluate WHS and to examine utilization data and health outcomes. In sites in which WHS was implemented, 31 percent of veterans suffering from chronic pain engaged in one or more Whole Health pain services. At one site, 55 percent of veterans with chronic pain were reported to have used at least one Whole Health service. From 2017 to 2019, utilization by veterans of Whole Health services grew across VA sites, including a 193 percent increase in utilization among veterans with chronic pain, a 211 percent increase among those with mental health diagnoses, and a 272 percent increase among those with chronic conditions (see Table 1). During these years, the use of complementary or integrative health services more than doubled (Bokhour et al., 2020b).
This increase in utilization seems to have had a positive impact on participating veterans. Studies have demonstrated that opioid use decreased among Whole Health users, dependent on their level of engagement with Whole Health services. Among veterans with chronic pain who used Whole Health services, opioid use declined by up to 38 percent, a three-fold greater reduction than the 11 percent decline in opioid use by veterans who did not use Whole Health (Bokhour et al., 2020b).
Other preliminary data from these flagship sites revealed that, compared to non-participating veterans, individuals who participated in Whole Health services reported greater improvements in perceptions of care, engagement in health care, self-care, life meaning and purpose, pain reduction, and perceived stress. Preliminary research compiled in 2019 from the Flagship sites is being studied to estimate the impact of the program on health care costs, although data from 2018 indicate an estimated 24 percent drop in total health care costs among participating veterans, particularly surrounding pharmacy costs (Bokhour et al., 2020b).
The successes of the Nuka System of Care and the VHA’s Whole System of Care—both in terms of traditional process and outcomes measures as well as patient-defined indicators of success—provide key learnings to realizing a nationwide vision of whole person, whole population health. The Nuka System of Care involves significant buy-in from organizational leadership, employees, and customers in delivering and accepting transformational change and a realignment of resources and services (Salinsky, 2017). These drivers of success, if scaled nationally, have the potential to unlock widespread health and well-being if stakeholder priorities, resources, and actions are aligned. To implement these changes, as exemplified by the VHA’s Whole System of Care, personalized health planning with the engagement, trust, and voice of patients is required. The power
TABLE 1 | Whole Health Service Use Among Veterans with Chronic Pain, Mental Health Diagnoses, and Chronic Conditions from the First Quarter of 2017 to the Third Quarter of 2019*
| Veterans with Chronic Pain | Veterans with a Mental Health Diagnosis | Veterans with Chronic Conditions | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Q1FY17 | Q3FY19 | % Change | Q1FY17 | Q3FY19 | % Change | Q1FY17 | Q3FY19 | % Change | |
| Any Whole Health System Service | 10.5% | 30.7% | 193% | 7.4% | 23.2% | 211% | 4.4% | 16.4% | 272% |
| Any Complementary or Integrative Service | 10.3% | 26.4% | 158% | 7.2% | 19.3% | 169% | 4.2% | 12.8% | 206% |
* The identified sample includes 114,357 veterans with chronic pain; 149,621 veterans with anxiety, depression, and post-traumatic stress disorder (PTSD); and 229,646 veterans with a common chronic condition. The groups are overlapping.
SOURCE: Bokhour et al., 2020b.
of science and medicine must also be combined with the lived realities, context, and complexities of all individuals who access and receive care.
Key Pillar 2—Health and health equity are nationwide commitments spanning beyond organizations in health care and public health.
Improving the health of populations, communities, and individuals requires a whole-of-society approach in which all actors, including those outside of the traditional domains of health care and public health, prioritize health and health equity. Adventist Health’s Blue Zones, employer-based worksite wellness programs, and school-based health centers exemplify the need to prioritize health in the critical and impactful settings of work, school, and the community at large.
ADVENTIST HEALTH’S BLUE ZONES
Acquired by Adventist Health in 2020, Blue Zones takes a systems-focused and community-based approach to improving well-being at the population level. The organization provides consulting, convening, and implementation services that help strengthen population-level health and well-being. For example, instead of aiming to change individual behavior (e.g., urging people to diet and exercise), the Blue Zones Life Radius model focuses on making healthy choices the default (i.e., easier) in all the places where individuals spend the most time—where they live, work, learn, play, and pray. By making lasting changes to the human-made surroundings and systems that determine health and life outcomes, people are collectively nudged to move and connect more, eat better, and develop a healthy outlook as they move throughout their day.
Rather than a siloed approach that concentrates on specific health challenges, Blue Zones represents a paradigm shift that focuses on root causes. This recognition of the built environment that individuals live within has been shown to be sustainable, increasing dividends for future residents. Examples of optimizing the built environment to improve community well-being include improving roads and transportation options, parks, and public spaces and building healthier options in the places people spend most of their time, such as restaurants, schools, and grocery stores. Additional Blue Zones interventions include building indoor sports arenas, expanding community garden space, increasing walking times to school, and restricting tobacco use.
These community initiatives are public-private partnerships, with the majority of funding typically sourced from a singular private entity (e.g., health care systems, health insurers, health organizations, or a coalition of entities). A major
driver of funding is the notion that people with higher measures of well-being live a fuller life in which they can contribute to their community without the financial hardships that often accompany acute health care costs. Simply put, optimizing well-being is in the best interest of the vast majority of actors within a community and, as such, community partners and sponsors have often come together to empower Blue Zones, as they have been shown to reduce the burden of lower well-being and chronic disease on their neighbors, local economies, health care systems, and productivity. Participating communities have seen double-digit reductions in obesity and smoking and significant improvements in health risks and productivity (IOM, 2015).
The implementation of the Blue Zones model in Albert Lea, Minnesota, for example, was associated with a 40 percent reduction in health care costs for city workers, 2.9 years added to life spans within 1 year of participation, a collective weight loss of 7,280 pounds, and a downtown streetscape revitalization that has increased private investment, tourism, and the community’s tax base (Blue Zones, 2022a). Since Blue Zone programs were implemented in Fort Worth, Texas, in 2014, the city moved from the 185th healthiest city in the nation to the 31st healthiest city in the nation (Blue Zones, 2022b). Neighborhoods and sectors of Fort Worth with citizens who exhibited the highest well-being disparities in 2014 also showed gains in well-being as of 2022: a major bright spot at a time when higher risk populations disparately experience poorer health outcomes and higher health care costs (Blue Zones, 2022b).
EMPLOYER-BASED WORKSITE WELLNESS PROGRAMS
American employers are the largest providers of health coverage in the United States, serving approximately 163 million workers and their families through private-sector employment-based plans (Mattke et al., 2015). These employers are witnessing rising rates of diabetes, obesity, and heart disease, among other chronic conditions, many of which are driven by social determinants of health (SDoH) and unhealthy behaviors such as smoking, excessive alcohol use, poor nutrition, and inactivity (Mattke et al., 2015). These chronic conditions are among the costliest to treat and often lead to a lower quality of life, higher health care costs, early-onset disability, and premature death. Therefore, in a national sector-wide transformation, employer-based health programs can contribute to improved whole health.
It is clearly in the best interest of employers to invest in employee well-being, especially when faced with the stark reality of annual per capita costs associated with health risks. High employee blood glucose is associated with a $129 increase
in per capita costs; stress is associated with a $118 increase in per capita costs; depression is associated with a $71 increase in per capita costs; and physical inactivity is associated with an $82 increase in per capita costs (Goetzel et al., 2020). Since 2019 the cost to employers for employees’ mental disorders alone equals more than $200 billion annually—mostly in lost productivity (Goetzel et al., 2018).
As major health care payers, it benefits employers to find innovative solutions that address ever-rising health and health care costs (Blumenthal et al., 2018). Additionally, given that most Americans work full-time jobs, a major opportunity exists to promote health and wellness in the context of the work setting and the social networks it provides. Through a creative redesign of traditional corporate and organizational care delivery and wellness programs, work settings can further empower individuals to make healthy lifestyle changes by creating environments, programs, practices, expectations, and habits that naturally move people toward healthier choices. Large-scale interventions include paying all employees a living wage, re-evaluating sick leave policies to maximize their use, and sliding scale health insurance premiums based on income. More frequently embraced small-scale interventions include onsite smoking bans, healthy food choices, and socially connective groups such as workplace book clubs, cooking classes, or exercise programs. Employers can build on these approaches by linking provider incentives with employee incentives so the two parties work toward common goals. To address transportation and child care costs, decrease carbon emissions, as well as improve worker well-being, employers could also consider hybrid and/or remote work policies that maintain social cohesion and organizational performance.
The goal of worksite health promotion programs focusing on the root causes of poor health is to reduce the need for avoidable care and medications and to enhance employee well-being. These programs offer a convenient, supportive venue for employees to learn about healthier lifestyles that can prevent, treat, and reverse disease and embrace the broader construct of whole person and whole population health. As an example, employers such as Cummins, Inc., an American multinational corporation that designs, manufactures, and distributes power generation products, has included integrative and complementary practices in their onsite clinics. In their largest clinic located in Columbus, Indiana, Cummins, Inc., successfully integrated chiropractic, acupuncture, and therapeutic massage with traditional physical therapy and orthopedic referrals for the care and treatment of musculoskeletal conditions.
Another company, Statistical Analysis System (SAS), has extensive health care and wellness programs, including onsite health care with free physician appointments that encourage workers to seek treatment for physical and mental
health as soon as needed. Colocation of physicians at the worksite reduces travel time to doctors’ offices, helping employees overcome locational barriers to access. An evaluation of SAS’s wellness offerings found that each dollar spent on the onsite clinic saves $2.24, producing $6.6 billion in annual savings and supporting 96 percent worker retention (Sholl, n.d.). While these findings are promising, it is important to recognize that common methodological challenges, such as lack of a control group and a short-term pre- versus post-analyses, render many evaluations of this type more suggestive than probative.
SCHOOL-BASED HEALTH CENTERS
A significant amount of care for children is provided in or through schools and is often paid for by Medicaid. This offers an innovative opportunity—both for integrated health service delivery and flexible financing—that is supportive of the vision described throughout this publication (MACPAC, 2018). In fiscal year (FY) 2016, Medicaid covered more than 4.5 billion for school-based care and related administrative services provided to students that meet certain criteria (MACPAC, 2018). School-based health centers (SBHCs) leverage this funding as a key driver of community-wide pediatric health, providing students with a single point of access for trustworthy, person-centered, culturally informed, and integrated care across multiple colocated providers. These centers have been found to improve educational outcomes, including school performance, grade promotion, and high school completion, while also improving health outcomes, including the delivery of vaccinations and other recommended preventive services, decreasing asthma morbidity, and decreasing emergency department use and hospital admission (Community Preventive Services Task Force, 2015).
Key examples of these vast and varied health centers include New York City’s (NYC’s) SBHCs within roughly 387 schools that help students manage their health needs throughout the school day. Such care centers have provided primary care for more than 25 years, lowering school absences and decreasing parents’ time away from work (NYC DOE, 2022). The centers are run by local hospitals, medical centers, and community organizations and are overseen by the New York State Department of Health and the NYC Department of Health and Mental Hygiene. They provide care regardless of insurance status but remain funded through Medicaid and private insurance billing, where applicable.
SBHCs have also demonstrated positive impact in underserved rural areas. In Montana, the Assiniboine and Sioux Tribes of the Fort Peck Reservation experience high rates of poverty, life expectancy more than 20 years lower than the state average, 50 percent unemployment, and a less than 70 percent high
school graduation rate (Harvard Project, 2015). Tribal youth experience higher rates of smoking, alcohol use, exposure to violence, trauma, and suicide. Almost 50 percent of children attending the reservation’s schools are overweight or obese, and more than 60 percent have untreated tooth decay (Harvard Project, 2015). In response to these challenges, the tribes created a SBHC initiative to offer integrated services for their children in schools, employing evidence-based medicine in concert with the local culture and traditions of the tribes. The centers serve more than 1,100 children, with participation varying across centers from 75 percent to 95 percent of enrolled students, and are primarily funded by Medicaid reimbursement (Harvard Project, 2015).
Depending on their design and implementation, there is strong evidence that SBHCs generate myriad benefits (County Health Rankings & Roadmaps, 2023). By increasing access to care, including immunization, nutritional, physical activity, and screening services, SBHCs can reduce emergency room visits and hospital utilization; prevent sexually transmitted infections, teen pregnancies, and substance abuse; improve mental health; and enhance educational outcomes (County Health Rankings & Roadmaps,2023). These impacts, especially when applied in a culturally competent manner in historically or presently marginalized communities, offer a key opportunity to reduce systemic discrimination and health care access gaps across race, geographic location, sexual orientation and gender identity, income, and disability status (County Health Rankings & Roadmaps, 2023).
Despite documented successes, it is important to note that attaining the full promise of integrated health and community services within and aligned with schools remains a challenge. While for many children, schools are a center for education, nutrition, and food security, the limited number of SBHCs nationwide leaves many children without access to these services. Creative use of blended and braided funding models, increased coverage of services delivered in schools by Medicaid and private insurers, a more robust school health workforce, and community support of care within schools can translate to a fully realized potential of better education and health outcomes for many school-aged children.
Despite operating under the above-mentioned constraints, Adventist Health’s Blue Zones, employer-based workplace wellness sites, and SBHCs demonstrate the ability to promote whole person, whole population health without the leadership of the traditional health care and public health ecosystem. By targeting the myriad of influences, factors, and drivers of health where people live, work, and learn, these and other efforts to reform social, behavioral, and environmental infrastructure at the local level; comprehensively support employee health and well-being; and pool state and national funds to promote student health are integral to equitably improving the nation’s health.
Key Pillar 3—Health care expenditures as a percentage of gross domestic product (GDP) do not constrain and displace other important social services that directly impact health and equity.
Current U.S. health care expenditures far exceed the norm for peer countries globally, especially when considered alongside a set of population-level health outcomes that are worse relative to comparable nations. While aligning resources and incentives with innovative care is a major priority for health system transformation, the scope of these efforts should be widened to reduce health care expenditures to a percentage of GDP that better aligns with Organisation of Economic Co-operation and Development (OECD) benchmarks. By introducing cost containment strategies, barriers to accessing care are reduced and care delivery organizations would be compelled to innovate to provide better care quality. The state of Maryland provides an excellent case study on how to reduce health care costs in a way that fosters high-quality care.
MARYLAND ALL-PAYER AND TOTAL COST OF CARE MODEL
Maryland’s unique all-payer model aims to promote the health and well-being of state residents while controlling the cost of health care. This model is based on a hospital rate-setting system that dates back to the 1970s, during which an independent Health Services Cost Review Commission set fee-for-service rates for each hospital that applied to all of the hospital’s payers, including the uninsured (Jain et al., 2022). A provision in the Social Security Act permitted Medicare to participate in Maryland’s program and, as other states abandoned rate-setting efforts in the 1980s, Maryland opted to continue. This approach led to slower growth in the hospital rates charged in Maryland than in the rest of the country (Murray, 2009).
Maryland’s historic experience prepared the state for change in 2014. By this time, it had become clear that fee-for-service rate-setting had limits; for example, while rate growth had been limited, volume growth had not been constrained. After extensive discussions within the state and with federal regulators, the Center for Medicare & Medicaid Innovation (CMMI) approved a new iteration of the Maryland Model in 2014. This reform fundamentally changed the state’s approach to hospital payment in that it required the Health Services Cost Review Commission to set prospective global budgets for hospitals. Generally speaking, these budgets would cover hospital inpatient and outpatient charges, regardless of patient volume, and rate-setting mechanisms would be used to help hospitals receive the revenue set by their global budgets from payers.
As the new Maryland Model was implemented, the financial incentives facing hospitals changed dramatically. Previously, under fee-for-service rate-setting, preventing hospitalizations attributed fixed costs to each hospital’s bottom line. With global budgets, however, preventing hospitalizations could be financially advantageous, as the hospital’s revenue would be unaffected. Hospitals across Maryland began to invest in a wide range of programs to keep patients from needing hospital care.
An independent evaluation from RTI International found that the Maryland Model led to major changes in care delivery, including a range of partnerships to support care coordination and transitions, as well as the fact that “nearly all hospitals invested in care coordination, discharge planning, social work staffing, patient care transition plans, and systematic use of patient care plans in response to the All-Payer model” (RTI, 2019). In terms of costs, RTI found the Maryland Model to be associated with a 2.8 percent decline in Medicare expenditures (including a 4.1 percent decline in hospital expenditures) without cost shifting elsewhere (RTI, 2019). This represented Medicare savings of about $1 billion. There were also substantial and statistically significant reductions in all hospital admissions and potentially avoidable hospital admissions for Medicare beneficiaries, and evidence of benefits to commercial payers (RTI, 2019).
In 2019, the state updated the Maryland Model, agreeing to a new 8-year arrangement with CMMI (Sapra et al., 2019). The new version, termed the Total Cost of Care model, added a primary care program to support care transformation and a care redesign program to allow hospitals to make incentive payments to specialist providers and suppliers; it also facilitated investments in outpatient and crisis behavioral health services and added more explicit expectations for reductions in the Medicare total cost of care (to total $2 billion in savings over the 8-year period) (Machta et al., 2021). In the first year, Maryland generated $365 million in Medicare savings. The state has also set population health goals for diabetes, addiction and overdose, childhood asthma, and maternal mortality (Machta et al., 2021).
The statewide scale of Maryland’s model and its initial successes are unique in the health policy landscape, but several concepts are inspiring others to apply and scale it to their own jurisdictions. Pennsylvania has expanded global budgeting to rural hospitals, and through the Community Health Access and Rural Transformation (CHART) model, CMMI may allow other rural hospitals to follow a similar path. Even as the state attracts more attention, the model is still a work in progress. Key efforts include producing more cost savings, creating more capacity and support for behavioral health care, closer community-hospital connections, and more ambitious population health efforts.
Health care models that promote cost savings while delivering high-quality care and optimal outcomes at scale remain an elusive goal. As the nation experiences successive health crises, there is a pressing need to expand involvement beyond the health care system. While transforming the health care system will impact 15-20 percent of the U.S. economy, there should also be clear economic and cultural incentives that encourage health-promoting actions and investments across the U.S. economy.
Key Pillar 4—Economic and cultural incentives encourage every stakeholder sector to take health promoting actions and make health promoting investments.
Aligned financing mechanisms help reinforce accountability for whole person and whole population health outcomes. This section describes programs and models that exemplify the concept of sustainable incentives for health improvement, including the Healthy Neighborhoods Equity Fund and Third-Party Investor Collaboration in Community Wellness. The section also describes the experience of the Casey Health Institute, which, despite its innovative vision, was stymied by an unhelpful payment structure.
HEALTHY NEIGHBORHOODS EQUITY FUND
Healthy Neighborhoods Equity Fund II (HNEF II) is an innovative $50 million private equity real estate fund that addresses the SDoH by investing in community-responsive development intended to:
- expand housing choice and affordability;
- provide access to transit, jobs, green space, and healthy food;
- support local wealth creation; and
- increase resilience to climate change (Church and Flatley, 2020; HNEF, 2022a).
The fund is cosponsored by Conservation Law Foundation (CLF), a nonprofit environmental advocacy organization, and Massachusetts Housing Investment Corporation, a community development financial institution (CDFI). HNEF II supports high-impact development in historically disinvested communities that are experiencing significant health and economic disparities, as well as opportunity-rich communities with excellent public schools where the fund can help deepen affordability for families with children. The fund, which operates in Massachusetts, Connecticut, and Rhode Island, fills a critical financing gap by
providing lower-cost, longer-term equity capital that is otherwise unavailable in the market. HNEF II pools funding from multiple institutional and individual investors, including hospitals, health plans, banks, and high net worth individuals to make these investments possible.
To ensure that HNEF investments achieve meaningful health and community impacts, all development projects are screened through HealthScore—a comprehensive impact scorecard developed and managed by CLF. HealthScore is a holistic, place-based, context-specific assessment tool that integrates both quantitative and qualitative measures in order to understand the need, opportunity, and likelihood of impact across multiple domains, such as housing affordability, job creation, walkability, climate resilience, and energy efficiency (CLF, 2021). Importantly, the fund only invests in development that has strong community support and has demonstrated responsiveness to the needs and priorities of local residents. In total, HealthScore includes more than 100 objective measures that help inform and support investment decision-making while also providing guidance to developers about what they can do to maximize health benefits for residents (CLF, 2021). To be considered for an HNEF investment, development proposals must receive a minimum score of 50 out of 100; developments that score higher receive more favorable consideration (HNEF, 2022b). HealthScore was originally created in 2014 for Healthy Neighborhoods Equity Fund I and is based on two health impact assessments conducted by the Metropolitan Area Planning Council as well as findings from the Healthy Neighborhoods Study (HNS), a longitudinal Participatory Action Research study conducted by CLF in partnership with the Massachusetts Institute of Technology, nine community-based organizations, and more than 40 resident researchers (Larson, 2021). HNEF’s use of HealthScore to screen and score investments has been a particularly important aspect of the fund for health care investors seeking to use their financial assets to improve the health of communities beyond the provision of acute clinical care (Church, 2018).
As neighborhoods across the country grapple with the combined impacts of housing and health crises exacerbated by COVID-19 and worsened by climate change, it is even more imperative that the health care sector be an active participant in long-term, sustainable solutions. HNEF provides a platform for health care to invest in healthier, more inclusive, and more resilient neighborhoods in a way that benefits the individuals who need them the most (Church and McGilvray, 2018). Before HNEF I investments, existing residents in the selected neighborhoods were 50 percent more likely to be admitted to the hospital for diabetes, and nearly 57 percent were housing cost-burdened, constraining their ability to afford other basic necessities (HNEF, 2020). In response to these and other challenges, HNEF I and II have supported the creation of 688 new mixed-income homes
to date, including both rental units and those that are now owned outright, that are affordable to households earning between 30 percent and 110 percent of Area Median Income (HNEF, 2020; UnitedHealth Group, 2022).
HNEF I and II investments have also supported the creation of more than 139,000 square feet of commercial space, enabling local entrepreneurs to open new health-promoting businesses, including healthy food outlets and gyms that cater to residents of the surrounding neighborhood (HNEF, 2022a). Additionally, the fund cosponsors have committed to addressing the racial wealth gap by ensuring that the benefits of their investments flow to local workers, including workers of color that are often left out of large construction contracts or have been hurt most by COVID-19 (Dana-Farber Cancer Institute, 2021). For every dollar of HNEF I investment, 91 cents went to Minority Business Enterprises (MBEs); in total, HNEF I supported nearly $20 million in MBE construction contract volume. These types of upstream investments in the SDoH are particularly important for communities that have been disinvested over generations, many of which are now experiencing the additional stressors of gentrification and displacement (Binet et al., 2021). Responding to these structural challenges through place-based and people-centered investment is essential to population health improvement. Health care is an essential partner in this work.
CHI HEALTH CARE/THE CASEY HEALTH INSTITUTE
In 2012, CHI Health Care (formerly the Casey Health Institute) piloted a grant-funded, public, nonprofit integrative primary care community health center in Gaithersburg, Maryland. CHI Health Care was an early adopter of the patient-centered medical home framework with a clinical team that included an interdisciplinary staff combining conventional primary care with a wide array of natural and complementary healing disciplines and integrative health. Team collaboration was emphasized through regular weekly meetings, electronic communication avenues, and informal interactions. The staff of practitioners included family medicine, internal medicine, integrative medicine, naturopathic medicine, acupuncture, traditional Chinese medicine, chiropractic care, psychology, psychotherapy, mindfulness, behavioral health, nutrition, yoga therapy, health coaching, therapeutic massage, and extensive health, wellness, and lifestyle medicine programming.
CHI increased access to high-quality, cost-effective health care across community members spanning the socioeconomic spectrum by accepting commercial health insurance, Medicare and Medicaid, and offering a sliding scale for the uninsured and underinsured. CHI allocated the resources necessary to build the
infrastructure to transition from fee-for-service reimbursement to value-based care and population health payment models. It participated in initiatives such as the Centers for Medicare & Medicaid Services’ (CMS’s) Medicare Shared Savings Plan and the CareFirst patient-centered medical home (PCMH) incentive program, thereby increasing access to CHI Health Care’s services and supports.
CHI was founded on the principle of embracing payment models that incentivized primary care while discouraging the overuse of invasive procedures and unnecessary treatments. It focused resources on health information technology through a robust patient portal, telemedicine with video medical appointments, electronic health record data tracking, outcomes research, team member electronic collaboration, and care coordination by capturing real-time data from the Maryland state health information exchange. The data CHI collected during its 6-year pilot demonstrated that 95 percent of patients were highly satisfied with their care and experienced fewer urgent care services, less prescription medication, and lower hospital admissions and readmission rates compared to patients of comparable conventional practices.
CHI Health Care succeeded in significantly improving health outcomes with lower downstream costs and consistently high levels of patient and staff satisfaction. However, the project ultimately failed because key population health infrastructure, care coordination, and essential health and wellness professional staff were not adequately compensated by either the existing fee-for-service environment or the value-based payment platforms available in Maryland at that time. CHI’s business plan was based on the projection that by rewarding value and not volume, value-based care programs would become more widely available and the incentives rewarding such practices would increase over time in the form of higher rates.
HNEFs I and II succeeded due to their ability to balance a respectable return on investment while investing in infrastructure to improve housing affordability and encourage MBEs. Meanwhile, CHI Health Care’s failure exposes the difficulties for providers to remain competitive in a landscape dominated by fee-for-service payment. While CHI generated value for their patients, the process of rewarding value over volume remains highly challenging. In the current payment environment, a few key insights might make a similar model successful today. These key facilitators include:
- Appropriately compensated collaborative interdisciplinary team care is an essential part of a comprehensive whole person health care system. This team includes all levels of primary care clinicians, practice support staff (including care coordination and population health positions), and a broad representation of integrative health professionals.
- A salaried staff model with a non-hierarchical organizational structure that facilitates essential ongoing collaboration is critical for success.
- Economies of scale are necessary. Optimal health creation and preservation in a primary care environment is expensive if implemented in a free-standing community-based practice. Shared resources for practice administration, human resources, information technology, medical supplies, and salaried personnel are needed across practices to provide negotiating power to capture optimal value-based contracts.
- An end goal of negotiated capitated contracts with two-sided risk on a per member, per month basis. This goal would ensure that CHI would not only share in care savings but also be held accountable for spending above cost benchmarks. Value-based payments based on this structure would allow for the best and sustainable use of a collaborative, interdisciplinary team model.
THIRD-PARTY INVESTOR COLLABORATION IN COMMUNITY WELLNESS
Social impact investing has increased in recent decades, along with three broad phenomena:
- Growing wealth and income inequality, which also created large classes of investors looking to do good while earning acceptable returns;
- Declining trust in government and corresponding strains on the capacity to meet underserved communities’ basic needs; and
- Increasing evidence that solutions exist for common problems but financing at scale is precluded by current law or traditional capital market failures.
The U.S. Impact Investing Alliance identifies several sources of community investments and financing, including corporations, Community Reinvestment Act–motivated banks, CDFIs, foundations and family offices, high-net-worth individuals, fintech1/crowdfunding, and community-investing participation models (U.S. Impact Investing Alliance, 2021). For example, corporations such as PayPal and the Black Economic Development Fund by Local Initiatives Support Coalition (LISC) provided deposits and other support to Black-owned banks in response to calls for racial justice (U.S. Impact Investing Alliance, 2021). The Grow with Google Small Business Fund supports the financing needs of small
___________________
1 Fintech refers to financial technology and describes “new tech that seeks to improve and automate the delivery and use of financial services”; see https://www.investopedia.com/terms/f/fintech.asp (accessed September 29, 2022).
businesses in distressed communities (U.S. Impact Investing Alliance, 2021). The Ujima Fund is a participatory model for local restorative wealth building and small dollar investor engagement (U.S. Impact Investing Alliance, 2021).
Place-based investments, traditionally in the realm of CDFIs, have been arranged by increasingly entrepreneurial health anchor institutions, such as Intermountain Healthcare, which has created a self-sustaining fund from its community benefit dollars that makes loans and investments to local community-based organizations (CBOs) to address a range of SDoH needs, including affordable housing, rural community development, and complex case management (Build Healthy Places Network, 2021). The Healthcare Anchor Network is an umbrella group with 70 health systems that are doing similar work to Intermountain Health across the country (Healthcare Anchor Network, 2022). Additionally, Quantified Ventures, an investment and consulting firm, designs a continuum of outcomes-based financing approaches for SDoH by aligning CBOs and impact investors on a set of outcomes that are valued by all. Impact investors deliver flexible capital to build capacity and scale services to more people, CBOs focus on improving outcomes through service delivery, and payers ultimately repay investors if and when pre-specified outcomes are achieved. Investors secure both a social and financial return on their investment if project outcomes are achieved. Recent examples of their work in SDoH include food delivery, medical respite for patients experiencing homelessness, and substance use treatment and prevention for prospective moms and babies (Quantified Ventures, 2021a,b,c).
Key Pillar 5—Efforts from all sectors, including government programs and regulations, are organized to prioritize the health of individuals, communities, and society.
Designing public and private programs and services to maximize the health of individuals and communities can help to ensure that the most underserved members of society have equitable access to economic and social support interventions. Initiatives such as the Program of All-Inclusive Care for the Elderly, Medicare Advantage Special Needs Plans, and Medicaid Long Term Services and Supports are effective examples of this concept in action.
PROGRAM OF ALL-INCLUSIVE CARE FOR THE ELDERLY
The Program of All-Inclusive Care for the Elderly (PACE) model of care is built on the belief that community-based whole person care is better for the well-being of seniors with chronic care needs, as well as their families and caregivers
(PACE, 2022). This integrated model of care serves individuals 55 or older who meet nursing home level of care requirements and are able to live safely in the community. PACE provides the entire continuum of care and services, including medical care and support services such as adult day care, transportation, laundry support, meals, nutritional counseling, social services, home health care, personal care, and respite care. Unlike many other models of care, a fundamental requirement in PACE is a coordinated, cross-sector interdisciplinary team of providers. This team includes drivers, personal care attendants, recreational therapists, and activity directors who collaborate with primary care physicians, nurses, and social workers who convene regularly to discuss patient care needs.
PACE is a statutorily combined Medicare and Medicaid payment and delivery system model that is designed specifically to enhance whole person care in the community. The program’s unique status as a model authorized directly by federal statute is critical to its success as an integrated, whole person model. Its permanent statutory authorization guarantees a clear, consistent, and sustained financing source within Medicare and Medicaid and a transparent methodology that allows providers to make long-term investments. The PACE statute also specifies Medicare and Medicaid benefits and eligible provider types, providing clarity and sustainability for both in the financing methodologies. Taken together, the three statutorily defined aspects of PACE—financing, benefits, and provider types—are intertwined into one sustainable care model.
As of July 2021, PACE has expanded across 30 states. More than 270 PACE centers provide services to 55,000 seniors, 95 percent of whom live in their communities (PACE, 2020). The program is primarily financed through a prospective risk-adjusted monthly capitated payment methodology (CMS, 2011). The vast majority (90 percent) of PACE members are dual-eligible enrollees, who are individuals enrolled in both Medicare and Medicaid. Nine percent of remaining PACE members are covered through Medicaid only, while 1 percent are either covered by Medicare or through other means. Medicare-only enrollees pay monthly premiums equal to the Medicaid capitation amount and do not pay deductibles, coinsurance, or any other cost-sharing (CMS, n.d.-a).
Despite the fact that PACE participants experience fewer emergency department visits, reduced hospital admissions and readmissions, and lower costs of care (PACE, 2020), the program continues to struggle with scaling to the much larger population of potential beneficiaries. Barriers to wider dissemination include:
- high start-up and expansion costs for providers;
- the unwillingness of potential beneficiaries to change physicians, plans, or residential facilities or to attend adult day centers;
- the resource-intensiveness of care planning and coordination;
- the current narrowly defined beneficiary population that is eligible to participate;
- lack of flexibility within the model to tailor benefits packages and financing; and
- high costs for regulatory compliance (Thomson Reuters, 2011).
Strides toward greater uptake of the model could be made through additional action by Congress to address these concerns or by requiring CMS to test the expansion of a model similar to PACE in additional populations, such as for pregnant women in Medicaid, CHIP, or for individuals with intellectual or developmental disabilities, regardless of age.
The struggle to scale PACE surfaces issues around long-term funding of future care models as well as the disconnected statutory authority of CMS and the Social Security Administration in creating and disseminating comprehensively integrated care models. First, while innovative care models, such as those developed and implemented by CMMI, provide an opportunity to test integrated benefit design and payment methodologies across funding streams, they carry greater uncertainty with respect to the availability of future funding. By law, the sustainability of each CMMI model is dependent on its own success and future decisions by policy makers. The lack of guaranteed long-term Medicare and Medicaid financing acts as a deterrent for larger-scale disruption to create integrated care models as well as for investment in such models. Because these models necessarily carry more risk, they are less attractive to providers, who would be required to implement disruptive innovations to improve care and outcomes within the relatively short 2-to 5-year time frame of a model. Additionally, without the guarantee of statutorily protected blended financing across Medicare and Medicaid, states, health plans, and providers have, in large part, lacked sufficient incentives to overcome rational risk aversion.
Second, there is limited legal authority to create and implement models similar to PACE. PACE is unique as the PACE statute allows the program to go beyond the limits of CMMI’s statute as a key provision of the Affordable Care Act as well as the authority of section 1115A of the Social Security Act. As a Medicare program, PACE can be provided to Medicaid beneficiaries should states elect to provide PACE services to Medicaid beneficiaries (Medicaid, n.d.).
Limited waiver authority makes it challenging to craft truly integrated models or to innovate whole-person care models. As a result of this limited waiver authority, Medicare and Medicaid cannot be synced or permitted by law unless Medicare aligns with the Medicaid statute. In comparison, the PACE statutory language in
Medicaid exactly mirrors that of Medicare, creating a fully integrated program across the two funding streams—such that the same definitions and specifications for benefits, providers, and payment apply. Therefore, policy makers should clarify the legal authority of Medicare, Medicaid, and the Social Security Administration so that these programs can build more coherent and complementary policies that promote whole health.
MEDICARE ADVANTAGE SPECIAL NEEDS PLANS
The Medicare Modernization Act of 2003 (MMA) established Medicare Advantage Special Needs Plans (SNPs) to provide integrated care specifically for individuals who are:
- institutionalized;
- Medicare-Medicaid enrollees (dually eligible); and/or
- experience severe or disabling chronic conditions (SSA, 2003).
Dual Eligible Special Needs Plans (D-SNPs), which serve Medicare and Medicaid enrollees by better coordination of Medicare and Medicaid benefits, provide person-centered care via the identification of barriers to health, understanding each member’s needs and preferences, and developing care plans that include community supports. Like other Medicare Advantage plans, SNPs can offer supplemental benefits. The model incorporates a comprehensive health risk assessment to identify the medical, functional, cognitive, psychosocial, and mental health needs of each SNP beneficiary, and the findings are directly incorporated into the development of an individualized care plan and ongoing coordination among the care team and enrollee.
D-SNPs are working creatively to address alignment in providing targeted services and supports to their enrollees in recognition of the fact that strong connectivity with community organizations (e.g., food banks, community health centers, county social services, supportive housing providers, and employment services) is critical to providing whole person care (ACAP, 2020). In one example, a plan is providing a monthly per member payment to a community housing organization that funds housing support services for individuals who meet unstable housing criteria. Early findings show emerging improvements in housing and health outcomes, as well as a decrease in health care spending and utilization once an individual experiences 10 months of stable housing (ACAP, 2020).
D-SNPs are also using technology to better understand enrollees’ needs and connect them to whole person care (ACAP, 2020). For example, one D-SNP plan
has a team that analyzes data from multiple sources, including population health data, as well as the social and financial impacts of SDoH investments. Another is connecting data across county health services departments to better understand member needs and identify optimal partnership strategies (ACAP, 2020).
The operational coherence among D-SNPs supports greater integration among plans and nonclinical community organizations to provide a full range of care, services, and supports to members. The personalized, data-driven, and coordinated nature of D-SNPs could also influence how health systems approach treatment for people who are not Medicare and Medicaid beneficiaries.
Depending on contexts, states could consider other forms of special needs plans that could provide better care integration for dual eligible beneficiaries. Fully Integrated Dual Eligible Special Needs Plans (FIDE-SNPs) integrate care for beneficiaries under a single managed care organization and cover primary, acute, and long-term services and supports benefits. FIDE-SNPs also cover behavioral health services in most contexts. Meanwhile, Highly Integrated Dual Eligible Special Needs Plans (HIDE-SNPs) include coverage of long-term services and supports benefits, behavioral health services, or both (MACPAC, 2021).
MEDICAID LONG-TERM SERVICES AND SUPPORTS
As the largest payer for long-term care in the country, Medicaid provides coverage of long-term services and supports (LTSS) through a continuum of settings and applies the following principles to promote health (CMS, n.d.-b):
- Person-driven: Older people, people with disabilities, and people experiencing chronic illness have the opportunity to decide where and with whom to live, exert control over the services they receive and who provides the services, how to work and earn money, and include friends and supports to help them participate in community life.
- Inclusive: The system encourages and supports people to live where they want to live with access to a full array of high-quality, community-based services and supports.
- Effective and accountable: High-quality services improve quality of life. Accountability and responsibility are shared among the programs, providers, individuals, and caregivers.
- Sustainable and efficient: Economy and efficiency are achieved through the coordination of a personalized package of services in accordance with the individual’s needs and goals.
- Coordinated and transparent: Services from various funding streams are coordinated to provide a seamless package of supports and make effective use of available technology.
- Culturally competent: Services account for cultural and linguistic needs.
Across this long-term care continuum, Medicaid covers a variety of whole person care initiatives through a highly variable collection of home- and community-based services (HCBS) in all 56 states and territories. Medicaid HCBS benefits create the conditions by which older adults and individuals with disabilities can leverage their independence and freedom of choice to receive care in their homes and communities rather than in institutionalized settings such as nursing homes.
Given this choice, individuals have overwhelmingly preferred the option of staying in their own homes and communities. In Medicaid, the majority of long-term care services are now HCBS. As of 2018, 56 percent of Medicaid long-term care consisted of HCBS on the national level, with a few states exceeding 75 percent (CMS, 2021). The $21 billion of investments in HCBS infrastructure in section 9817 of the American Rescue Plan Act will support the payment and delivery of high-quality, cost-effective, whole person care, allowing millions to stay in their homes and communities while receiving high-quality health and social care services and supports (HHS, 2021). Whether this infusion of funds will address concerns that Medicaid LTSS funding does not sufficiently cover the cost of delivering nursing home-level care at home is yet to be determined.
The keystone of HCBS programs is the person-centered plan that addresses health and long-term services and support needs, reflecting the individual’s preferences and goals. The person-centered planning process must be directed by the individual, including representatives whom the individual has freely chosen to contribute, and results in a person-centered plan with individually identified goals and preferences that help guide the individual in achieving personally defined outcomes in the most integrated community setting. The plan also ensures the delivery of services in a manner that reflects personal preferences and choices while contributing to the assurance of health and welfare. Some states, like Colorado, provide complementary and integrative health services as part of HCBS, including acupuncture, chiropractic, and massage therapy, including within their spinal cord injury HCBS waiver program. All benefits and services are provided in accordance with the individual’s care plan.
Medicaid is by far the largest driver of HCBS services and the largest funder of such care in the country, incurring approximately 57 percent of all HCBS
expenditures—an estimated $114 billion in federal FY 2021 (Musumeci, 2021). Other payers have been slow to embrace HCBS, with private insurance covering only 12 percent of the nation’s HCBS costs, despite a proven, well-developed, and comprehensive blueprint for providing and monitoring the quality of HCBS in a healthy, safe, and person-centered way (CMS, n.d.-b). A major disincentive is that HCBS rates are often too low, leading to inefficiencies such as the unpayment and overwork of direct-care workers, who are often more likely to belong to a marginalized community (Sullivan, 2021). Moreover, existing HCBS systems are overwhelmed, with hundreds of thousands of people on waiting lists for HCBS across the nation (Sullivan, 2021)—yet another manifestation of our current health crisis. The federal government and private insurance stakeholders must find ways to increase the capacity of HCBS systems, including through sustaining long-term training, career growth, and competitive payment of its providers (Sullivan, 2021).
Aligning policies, programs, and regulations to prioritize the health of individuals and communities remains an uphill task due in significant part to the political realities of federal health care reform today (King, 2017). Despite these challenges, federal legislators, policy practitioners, and health systems can take more incremental actions that circumvent the unfortunate status quo. First, government agencies must be empowered with the statutory authority required to finance, implement, and integrate care models across government departments, such as Medicare and Medicaid. Second, health programs must promote the dignity of people with disabilities through care that leverages independence, freedom of choice, and individual control over their care in both home- and community-based settings. Finally, patients must be better served through meaningful engagement of individuals, health systems, and community-based organizations. These partnerships should collect and apply data to better understand community-specific care needs and preferences, barriers to health, and gaps in services and supports relative to individual and community goals.
Key Pillar 6—Individuals and communities are empowered as organization and delivery decision-makers for matters pertaining to their health.
Engaging and empowering individuals and communities as decision-makers in their own health and the health of their communities is essential to investing in whole person and whole population health. The Community Aging in Place: Advancing Better Living for Elders Model (CAPABLE), Self-Directed Medicaid Services, Collaborative Approach to Public Good Investments, and Federally
Qualified Health Centers are each important examples that adhere to this pillar and provide helpful guidance on the ways in which individual and community empowerment might be centered in efforts for health system transformation.
COMMUNITY AGING IN PLACE: ADVANCING BETTER LIVING FOR ELDERS
Community Aging in Place: Advancing Better Living for Elders (CAPABLE) is a multidisciplinary intervention developed and tested to reduce health disparities among older adults by helping them “age in community.” Developed at the Johns Hopkins School of Nursing, CAPABLE teams include an occupational therapist, a nurse, and a handy worker to address the participating older adults’ home environment and use their unique strengths to improve independence and safety in their home setting. This program uncovers and leverages intrinsic motivation surrounding what matters to each individual, such as bathing without difficulty, preparing food, or leaving the house and getting into a car for a family event.
Throughout a 4-month service period, CAPABLE members will identify their priorities and goals. Occupational therapists and nurses use a standardized approach tailored to each individual to assess and brainstorm a plan that addresses needs in the individual’s home environment. In developing this plan, the team sees the person in their home context, helping to offset biases that might come into play in more traditional clinical settings. Using this plan, a handy worker implements fixes and adaptations (e.g., lighting on the stairs or adaptive cutting boards) according to individual preferences, needs, and clinical expertise.
CAPABLE program sites provide services to older adults without cost, reducing spending on hospital admissions, skilled nursing facility admissions, and specialty care (Szanton, n.d.). Comparing the health care cost expended for participants in CAPABLE to the health care cost for a nonparticipating group, CAPABLE saved, on average, $2,765 per quarter—or more than $10,000 per year—for Medicare for at least 2 years. Inclusive of all patient visits, home repairs, and modifications, CAPABLE costs $2,825 per year while decreasing inpatient and outpatient costs, readmission rates, and observation status stays (Szanton, n.d.).
Despite these successes, CAPABLE is limited in its reach. Only approximately 4,000 older adults have participated in CAPABLE, and an estimated 16.1 million could still benefit from this service when assuming around 35 percent of the 46 million older people above the age of 65 can benefit from home-based interventions due to difficulties with activities of daily living (ACL, 2021; JHU School of Nursing, 2022). To enable access to more supports and services for older people, Medicare could scale and pay for CAPABLE as a Medicare bundle
of services, incorporate CAPABLE specifically into value-based care models, or include quality star metrics more clearly to beneficiaries’ functional goals.
CAPABLE is currently implemented in 43 sites in 23 states (including rural, frontier, urban, and micropolitan areas) within a variety of policy settings from two accountable care organizations, one hospital readmission project, and a state Medicaid HCBS waiver, as well as in some free-standing clinics and home-based primary care. With American Rescue Plan Act funding, three new states will implement CAPABLE. While the American Rescue Plan Act will enable some scaling of the CAPABLE model, the provided funding and resources will not be sufficient to support the needs of older adults. Through scaling promising models such as CAPABLE, older adults can access care that builds, maintains, and supports physical capacity and independence. Finally, because health remains an essential component to people across all ages, caring for older adults will be integral to a system of whole person, whole population health.
SELF-DIRECTED MEDICAID SERVICES
Self-direction is an expanding and fully person-driven system of care. As of January 2021, 267 programs across the United States empowered more than 1.2 million individuals to direct care resources and services to meet their own needs and preferences (Edwards-Orr et al., 2020). Medicaid is the largest payer of this model, accounting for 66 percent of self-direction funding in 2019, and the VHA is another significant supporter (Edwards-Orr et al., 2020). In 2019, the Veteran-Directed Home and Community Based Services program served more than 2,000 veterans in 71 programs in 41 states.
In self-directed care, participating individuals or their designated caregivers have decision-making authority and take responsibility for managing their services with the assistance of a system of supports. The self-directed service delivery model is an alternative to the traditional service model, such as an agency or health plan responsible for paying for services. Self-direction allows participants to have independence in managing all aspects of service delivery in a person-centered planning process.
Self-direction promotes personal choice and control over the delivery of services, including a choice of who provides the services and how the services are provided. Self-directed care is based on a service plan developed by an individual (with assistance) that identifies individuals’ strengths, capacities, preferences, needs, and desired measurable outcomes. While specific services within self-direction vary by state and by program, services are targeted to address problems identified in the individual’s service plan, and could include acupuncture, therapeutic
horseback riding and equine-assisted activities, hypnotherapy, peer mentoring, art and recreation programs, chiropractic care, massage therapy, family support services, biofeedback, and Native American healers.
In practice, state Medicaid programs provide or arrange for the provision of a system of supports that are responsive to an individual’s preferences in developing these plans, managing services and support workers, and performing the responsibilities of an employer. Participants have the authority to recruit, hire, train, and supervise the individuals who provide their services and decide how the Medicaid funds in their budget are spent.
Medicaid has a strong tradition of self-directed care, including Wisconsin’s IRIS (Include, Respect, I Self-Direct) program. Since 2008, IRIS has provided self-direction for Medicaid-enrolled frail older adults and adults with disabilities, giving them the freedom to decide how they want to live and allowing for up to 32 services to be self-directed while giving participants full employer and budget authority (WI DHS, 2021). IRIS is built on the belief that everyone holds the potential for meaningful societal contribution, deserves a quality life experience, and has a right to full citizenship (Genz and Urban, 2020). Participants highlight the program’s benefits in enhancing independence for individuals and caregiver support to create fuller, healthier, and more meaningful lives. The program has more than 21,000 participants, and its popularity is reinforced by the fact that no waiting list space is available in any of the 72 counties in the state.
COLLABORATIVE APPROACH TO PUBLIC GOOD INVESTMENTS
The Collaborative Approach to Public Good Investments (CAPGI) is a financial model and governance process designed to help multi-stakeholder coalitions sustain new investments in SDoH. This process occurs within communities and uses local capital, stakeholder self-interest, and a collaborative bidding process to source and pay for new services that (1) any single stakeholder could not support and (2) could benefit multiple organizations and the community.
CAPGI is unique because funding for new investments does not rely on third-party private investment capital, which expects to be repaid, or new government expenditures. Rather, it leverages the combined self-interest of existing community partners, some of which may be private or public insurance plans or hospital systems with deep connections to a larger organization. Investing stakeholders could also be local philanthropies, local government, such as law enforcement, and employer or social service organizations. A key feature of the model is the trusted broker, or an organization capable of convening relevant stakeholders, maintaining
trust in the confidentiality of their financial bids, and executing the performance contract with the social service provider(s). The deeply interconnected structure of the program, along with the convening power of the trusted broker, is essential to CAPGI’s goal of forming partnerships to attract financing for public goods. Additionally, the financing must be sustained over long periods due to the slow yielding nature of CAPGI investments, including increasing access to housing, nutrition, and transportation (Nichols and Taylor, 2018).
Based on a previously developed and modified economic auction model, the novel funding approach was first described in 2018 (Nichols and Taylor, 2018). Currently, three communities are in the first year of using CAPGI–Cleveland, Ohio; Albany, New York; and Waco, Texas—and others are working toward implementation in the next year. The program has attracted commitment and energized involvement from a multi-stakeholder network of cities, states, and communities across racial and ethnic backgrounds, as well as community size. These promising signals indicate that the model has a high likelihood of being scaled to new communities and sustained in existing communities (Nichols et al., 2020). The model is not intended to fix system-wide deficits but could influence future collective action efforts to encourage public good investments that finance social drivers of health infrastructure, including transportation, nutrition, and housing (Nichols and Taylor, 2018).
FEDERALLY QUALIFIED HEALTH CENTERS
Established in 1965 by the federal Office of Economic Opportunity, Federally Qualified Health Centers (FQHCs) aim to deliver integrated, “comprehensive, culturally competent, high-quality primary health care services” (HRSA, 2021b). In exchange for federal grants and special reimbursement by Medicaid and Medicare, FQHCs provide basic health services to all in their geographic community regardless of their ability to pay. In addition to reimbursement for Medicare and Medicaid beneficiaries, FQHCs receive access to 340B discounts on outpatient pharmaceutical products, free vaccines for uninsured and underinsured children, and assistance in recruiting and retaining primary care providers through the National Health Service Corps (HRSA, 2021b).
In exchange for these benefits, and as codified in section 330 of the Public Health Services Act, FQHC entities agree to be organized as nonprofit corporations with their Boards of Directors being:
composed of individuals, a majority of whom are being served by the center and who, as a group, represent the individuals being served by the center, and
meets at least once a month, selects the services to be provided by the center, schedules the hours during which such services will be provided, approves the center’s annual budget, approves the selection of a director for the center, and … establishes general policies for the center. (United States Code, 2022)
The rationale for insisting on consumer governance in FQHCs is consistent with the sixth pillar for whole person health: to make the organization responsible to the community it serves. By adhering to a community-based, patient-led governance structure, FQHCs also integrate access to pharmacy, mental health, substance use disorders, and oral health services in underserved areas. Access is also improved through health education, translation, transportation, and access to a sliding fee scale (HRSA, 2021b).
Furthermore, FQHCs are able to develop systems of patient-centered and integrated care that can be personalized to diverse populations. These practices include incorporating acupuncture, meditation, tai chi, reiki, mindfulness, and yoga into health programs (Bharath, 2019). A program in Oregon included partnerships to combat food insecurity and health inequities through funding from Medicaid Coordinated Care Organizations, screening through FQHCs, and the distribution of produce from local farmers markets (Kaye, 2021). Some FQHCs, such as the NATIVE project in Spokane, Washington, practice integrating spiritual, cultural, and traditional Native values as part of care. Underpinned by these values, the NATIVE project also prioritizes physical, mental, and emotional health centered alongside education and awareness, drug- and alcohol-free lifestyles, and the integration of mind, body, spirit, and healing paths for patients (NATIVE Project, 2021).
FQHCs now serve more than 30 million people nationwide across the life course, including children, pregnant women, and older adults (HRSA, 2021a). Their patients are disproportionately poor and uninsured, including one in three people living in poverty and one in five rural residents (HRSA, 2021a). With standards of care and service developed, promoted, and enforced by the Health Resources and Services Administration of the Department of Health and Human Services, FQHCs perform as well as or better than privately organized practices serving patients with less complex health care needs (Goldman et al., 2012).
Although the composition of FQHC boards sets this intervention apart from others, its positive performance may not be directly linked to this innovative approach. Moreover, implementing a mechanism that embodies true patient engagement remains a challenge for FQHCs. For example, there remain distinctions between the formal representation of consumers on boards and descriptive representation. There is also the challenge of developing effective governance skills, whether
selected consumers are truly representative of community positions, and the power of technical knowledge in board agenda setting (Wright, 2015).
These cautions notwithstanding, with its focus on community governance, public-private partnerships, and active patient participation, consumer-majority health care organization boards as modeled by FQHCs represent a “new governance paradigm” (Campbell, 2011) that challenges traditional models of the governance of large and consolidating nonprofit health systems and exemplifies the sixth pillar of whole person health: communities being empowered as decision-makers in terms of investments intended to benefit their health.
CONCLUSION
While the highlighted models and programs demonstrate the potential of person-centricity, cross-sector collaboration, equity, and aligned financing in achieving better health and well-being, they do not fully achieve the Steering Group’s vision of whole person, whole population health. They are vehicles of change and are directionally correct but are not comprehensive, large, or exhaustive enough to effect the change the Steering Group described in Chapters 1 and 2 of this publication.
Although ongoing innovation and work in this space can lead to positive outcomes on smaller scales, the current health and health care system is highly constrained, delaying the transformation required to achieve the Steering Group’s vision. Instead, the ideas, innovation, and advances in these models need to be further nurtured and unlocked through leveraging new sources of funding, involving a new and different mix of stakeholders, and scaling the innovative approaches of the presented cases into comprehensive, system-wide change. In the next two chapters, the authors will further discuss the gap between where we are and where we need to be, and highlight the systems-wide action, collaboration, and financing required to achieve the Steering Group’s vision of whole person and whole population health.
REFERENCES
ACAP (Association for Community Affiliated Plans). 2020. Addressing Social Determinants of Health Through Dual-Eligible Special Needs Plans. Available at: https://www.communityplans.net/research/11927 (accessed April 13, 2022).
ACL (Administration for Community Living). 2021. 2020 Profile of Older Americans. Available at: https://acl.gov/sites/default/files/aging%20and%20Disability%20In%20America/2020Profileolderamericans.final_.pdf (accessed October 13, 2022).
Bharath, D. 2019. Integrative Medicine Becomes a Focus for Treating the Uninsured. Available at: https://centerforhealthjournalism.org/integrative-medicine-becomes-focus-treating-uninsured (accessed August 16, 2022).
Binet, A., G. Rio, M. Arcaya, G. Roderigues, and V. Gavin. 2021. “It feels like money’s just flying out the window”: Financial security, stress and health in gentrifying neighborhoods. Cities & Health 6(3):536-551. https//doi.org/10.1080/23748834.2021.1885250.
Blue Zones. 2022a. Blue Zones Results Albert Lea, MN. Available at: https://www.bluezones.com/blue-zones-results-albert-lea-mn/#section-1 (accessed June 21, 2022).
Blue Zones. 2022b. Blue Zones Project News: Fort Worth’s Transformation from One of Unhealthiest Cities in America. Available at: https://www.bluezones.com/2019/05/blue-zones-project-news-fort-worths-transformation-from-one-of-unhealthiest-cities-in-america (accessed June 21, 2022).
Blumenthal, D., L. Gustaffson, and S. Bishop. 2018. To Control Health Care Costs, U.S. Employers Should Form Purchasing Alliances. Available at: https://hbr.org/2018/11/to-control-health-care-costs-u-s-employers-should-form-purchasing-alliances (accessed October 12, 2022).
Bokhour, B. G., J. N. Haun, J. Hyde, M. Charns, and B. Kligler. 2020a. Transforming the Veterans Affairs to a whole health system of care: Time for action and research. Medical Care 58(4):295-300. https//doi.org/10.1097/MLR.0000000000001316.
Bokhour B. G., J. K. Hyde, S. Zeliadt, and D. C. Mohr. 2020b. Whole Health System of Care Evaluation—A Progress Report on Outcomes of the WHS Pilot at 18 Flagship Sites. Veterans Health Administration, Center for Evaluating Patient-Centered Care in VA (EPCC-VA). Available at: https://www.va.gov/WHOLEHEALTH/professional-resources/clinician-tools/Evidence-Based-Research.asp (accessed October 12, 2022).
Build Healthy Places Network. 2021. Intermountain Healthcare & the Utah Housing Preservation Fund. Available at: https://buildhealthyplaces.org/sharing-knowledge/publications/community-close-ups/intermountain-healthcare-the-utah-housing-preservation-fund (accessed October 13, 2022).
Business Insider. 2018. Southcentral Foundation Accepts Second Malcolm Baldrige Award. Available at: https://markets.businessinsider.com/news/stocks/southcentral-foundation-accepts-second-malcolm-baldrige-award-1021346598 (accessed June 21, 2022).
Campbell, Y. 2011. New governance in action: Community health centers and the Public Health Service Act. St. Louis University Journal of Health Law and Policy
4(2). Available at: https://scholarship.law.slu.edu/jhlp/vol4/iss2/6 (accessed June 21, 2022).
Church, M. S. 2018. Investing in Health from the Ground Up: Building a Market for Healthy Neighborhoods. Available at: https://investinresults.org/sites/default/files/book-chapter/WM_29_Super-Church_0.pdf (accessed August 11, 2022).
Church, M. S., and J. Flatley. 2020. Healthy Neighborhoods Equity Fund II: Theory of Change. Available at: https://static1.squarespace.com/static/5f31ae81bcb71e20e39311bb/t/5f875712a87a740f5b668f48/1602705172416/HNEF+II+ToC+Full+Text+Final+06.02.20.pdf (accessed August 11, 2022).
Church, M. S., and K. McGilvray. 2018. Improving health and environment through place-based investing: The Healthy Neighborhoods Equity Fund. Journal of Affordable Housing & Community Development Law 27(2):353-366. https://www.jstor.org/stable/26496809.
CMS (Centers for Medicare & Medicaid Services). 2011. Chapter 13 Payments to PACE Organizations. Available at: https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/pace111c13.pdf (accessed April 6, 2022).
CMS. 2021. Medicaid Long Term Services and Supports Annual Expenditures Report: Federal Fiscal Years 2017 and 2018. Available at: https://www.medicaid.gov/medicaid/long-term-services-supports/downloads/ltssexpenditures-2017-2018.pdf (accessed April 6, 2022).
CMS. n.d.-a. Programs of All-Inclusive Care for the Elderly Benefits. Available at: https://www.medicaid.gov/medicaid/long-term-services-supports/pace/programs-all-inclusive-care-elderly-benefits/index.html (accessed April 6, 2022).
CMS. n.d.-b. Long Term Services and Supports. Available at: https://www.medicaid.gov/medicaid/long-term-services-supports/index.html (accessed April 6, 2022).
CMS. n.d.-c. Independence at Home Demonstration. Available at: https://innovation.cms.gov/innovation-models/independence-at-home (accessed June 21, 2022).
Community Preventive Services Task Force. 2015. School-Based Health Centers. Available at: https://www.thecommunityguide.org/sites/default/files/assets/OnePager-SBHC.pdf (accessed June 21, 2022).
Conservation Law Foundation. 2021. HealthScore Metrics That Matter for Healthy and Resilient Neighborhoods. Available at: https://www.clf.org/wp-content/uploads/2021/12/CLF-HealthScore-WEB.pdf (accessed July 28, 2022).
County Health Rankings & Roadmaps. 2023. 2023 County Health Rankings National Findings Report. Available at: https://www.countyhealthrankings.org/reports/2023-county-health-rankings-national-findings-report (accessed May 15, 2023).
Dana-Farber Cancer Institute. 2021. Healthy Neighborhoods Fund Gets Major Boost. Available at: https://www.dana-farber.org/newsroom/news-releases/2021/healthy-neighborhoods-fund-gets-major-boost (accessed August 11, 2022).
Edwards-Orr, M., M. Morris, C. DeLuca, K. Ujvari, and M. Sciegaj. 2020. National Inventory of Self-Directed Long-Term Services and Supports Programs. Available at: https://www.longtermscorecard.org/publications/promising-practices/2019-self-directed-ltss-inventory (accessed June 21, 2022).
Genz, B., and S. Urban. 2020. IRIS Self-Directed Personal Care: Gateway to Community and a Self-Determined Life. Available at: http://www.advancingstates.org/sites/nasuad/files/u24453/Self-Directed%20Personal%20Care%20Gateway%20to%20Community%20and%20a%20Self-Determined%20Life.pdf (accessed April 11, 2022).
Goetzel, R. Z., E. C. Roemer, C. Holingue, M. D. Fallin, K. McCleary, W. Eaton, J. Agnew, F. Azocar, D. Ballard, J. Bartlett, M. Braga, H. Conway, K. A. Crighton, R. Frank, K. Jinnett, D. Kellar-Greene, S. M. Rauch, R. Safeer, D. Saporito, A. Schill, D. Shern, V. Strecher, P. Wald, P. Wang, and C. R. Mattingly. 2018. Mental health in the workplace: A call to action proceedings from the mental health in the workplace: Public health summit. Journal of Occupational and Environmental Medicine 60(4):322-330.
Goetzel, R. Z., R. M. Henke, M. A. Head, R. Benevent, and K. Rhee. 2020. Ten modifiable health risk factors and employees’ medical costs—An update. American Journal of Health Promotion 34(5):490-499.
Goldman, L. E., P. W. Chu, H. Tran, M. J. Romano, and R. S. Stafford. 2012. Federally Qualified Health Centers and private practice performance on ambulatory care measures. American Journal of Preventive Medicine 43(2):142-149. https://doi.org/10.1016/j.amepre.2012.02.033.
Gottlieb, K. 2013. The Nuka System of Care: Improving health through ownership and relationships. International Journal of Circumpolar Health 72. https://doi.org/10.3402/ijch.v72i0.21118.
Gottlieb, K., I. Sylvester, and D. Eby. 2008. Transforming your practice: What matters most. Family Practice Management 15(1):32.
Harvard Project. 2015. School-Based Health Centers: Fort Peck Assiniboine and Sioux Tribes. Available at: https://hwpi.harvard.edu/files/hpaied/files/schoolbasedhealthcenters-final_2.pdf?m=1639579174 (accessed July 15, 2022).
Healthcare Anchor Network. 2022. Healthcare Anchor Network. Available at: https://healthcareanchor.network (accessed October 13, 2022).
HHS (U.S. Department of Health and Human Services). 2021. CMS Issues Guidance on American Rescue Plan Funding for Medicaid Home and Community Based Services. Available at: https://www.hhs.gov/about/news/2021/05/13/
cms-issues-guidance-american-rescue-plan-funding-medicaid-home-andcommunity-based-services.html (accessed April 6, 2022).
HNEF (Healthy Neighborhood Equity Fund). 2020. Transformative Impacts of Healthy Neighborhoods Equity Fund I. Available at: https://static1.squarespace.com/static/5f31ae81bcb71e20e39311bb/t/5f641b3640e1a14ef6b3c9e5/1600396097669/HNEF+Impact+Infographic+Final+02.14.20.pdf (accessed August 11, 2022).
HNEF. 2022a. Investment. Available at: https://www.hnefund.org/investment (accessed July 28, 2022).
HNEF. 2022b. Eligibility & Screening. Available at: https://www.hnefund.org/eligibilityscreening (accessed July 28, 2022).
HRSA (Health Resources and Services Administration). 2021a. Health Center Program: Impact and Growth. Available at: https://bphc.hrsa.gov/about-health-centers/health-center-program-impact-growth (accessed August 16, 2022).
HRSA. 2021b. What Is a Health Center? Available at: https://bphc.hrsa.gov/about-health-centers/what-health-center (accessed August 16, 2022).
IOM (Institute of Medicine). 2015. Business Engagement in Building Healthy Communities: Workshop Summary. Washington, DC: The National Academies Press.
Jain, A., J. Levy, D. Polsky, and K. E. Anderson. 2022. Medicare Advantage and the Maryland all-payer model. Health Affairs Forefront March 18. https://doi.org/10.1377/forefront.20220316.50044.
JHU (Johns Hopkins University) School of Nursing. 2022. CAPABLE FAQs. Available at: https://nursing.jhu.edu/faculty_research/research/projects/capable/capable-faqs.html (accessed October 12, 2022).
Kaye, N. 2021. Oregon’s Community Care Organization 2.0 Fosters Community Partnerships to Address Social Determinants of Health. Available at: https://www.nashp.org/oregons-community-care-organization-2-0-fosters-community-partnerships-to-address-social-determinants-of-health/#toggle-id-6 (accessed August 16, 2022).
King, M. W. 2017. Health Care Efficiencies: Consolidation and Alternative Models vs. Health Care and Antitrust Regulation—Irreconcilable Differences? American Journal of Law & Medicine 43(4):426-467. https://doi.org/10.1177/0098858817753407.
Larson, S. 2021. What’s Different When the Community Collects the Data? Available at: https://shelterforce.org/2021/08/10/what-happens-when-the-community-collects-the-data (accessed August 11, 2022).
Machta, R., G. Peterson, J. Rotter, K. Stewart, S. Heitkamp, I. Platt, D. Whicher, K. Calkins, K. Krankler, L. Barterian, and N. McCall. Evaluation of the Maryland
Total Cost of Care Model: Implementation Report. Available at: https://www.mathematica.org/publications/evaluation-of-the-maryland-total-cost-of-care-model-implementation-report (accessed June 21, 2022).
MACPAC. 2018. Medicaid in Schools. Available at: https://www.macpac.gov/wp-content/uploads/2018/04/Medicaid-in-Schools.pdf (accessed June 21, 2022).
MACPAC. 2021. Medicare Advantage Dual Eligible Special Needs Plans. Available at: https://www.macpac.gov/subtopic/medicare-advantage-dual-eligible-special-needs-plans-aligned-with-medicaid-managed-long-term-services-and-supports (accessed March 16, 2023).
Mattke, S., K. Kapinos, J. P. Caloyeras, E. A. Taylor, B. Batorsky, H. Liu, K. R. Van Busum, and S. Newberry. 2015. Workplace wellness programs: Services offered, participation, and incentives. RAND Health Quarterly 5(2).
Medicaid. n.d. Program of All-Inclusive Care for the Elderly. Available at: https://www.medicaid.gov/medicaid/long-term-services-supports/program-all-inclusive-care-elderly/index.html (accessed October 12, 2022).
Murray, R. 2009. Setting hospital rates to control costs and boost quality: The Maryland experience. Health Affairs 28(5):1395-1405.
Musumeci, M. 2021. How Could $400 Billion New Federal Dollars Change Medicaid Home and Community-Based Services? Available at: https://www.kff.org/medicaid/issue-brief/how-could-400-billion-new-federal-dollars-change-medicaid-home-and-community-based-services (accessed August 16, 2022).
NATIVE Project. 2021. About Us. Available at: https://nativeproject.org/about-us (accessed August 16, 2022).
Nichols, L. M., and L. A. Taylor. 2018. Social determinants as public goods: A new approach to financing key investments in healthy communities. Health Affairs 37(8):1223-1230.
Nichols, L., L. Taylor, P. Hughes-Cromwick, G. Miller, A. Turner, C. Rhyan, and R. Hamrick. 2020. Collaborative Approach To Public Goods Investments (CAPGI): Lessons learned from a feasibility study. Health Affairs Blog, August 13. https://doi.org/10.1377/forefront.20200811.667525.
NIST (National Institute of Standards and Technology). 2017. Southcentral Foundation: Malcolm Baldrige National Quality Award 2011Award Recipient Health Care. Available at: https://www.nist.gov/baldrige/southcentral-foundation (accessed June 21, 2022).
NRC (National Research Center). 2019. Complementary and Integrative Health Services Evaluation: Annual Report SFY 2018-19. Available at: https://hcpf.colorado.gov/sites/hcpf/files/NRC%20Annual%20Report%20to%20HCPF%20SFY1819-June%202019.pdf (accessed April 6, 2022).
NYC DOE (New York City Department of Education). 2022. School-Based Health Centers. Available at: https://www.schools.nyc.gov/school-life/health-and-wellness/school-based-health-centers (accessed June 21, 2022).
PACE (National PACE Association). 2020. PACE by the Numbers. Available at: https://www.npaonline.org/sites/default/files/images/NPA%20infographic%203%2020%20%281%29.pdf (accessed April 6, 2022).
PACE. 2022. The History of PACE. Available at: https://www.npaonline.org/policy-advocacy/value-pace (accessed April 5, 2022).
Quantified Ventures. 2021a. Drug Free Moms and Babies Program. Available at: https://www.quantifiedventures.com/drug-free-moms-and-babies-program (accessed August 18, 2022).
Quantified Ventures. 2021b. Hope Has a Home Medical Respite Program. Available at: https://www.quantifiedventures.com/hope-has-a-home-medical-respite-program (accessed August 18, 2022).
Quantified Ventures. 2021c. Together in Care Meal Delivery Program. Available at: https://www.quantifiedventures.com/together-in-care-meal-delivery-program (accessed August 18, 2022).
Reddy, K. P., T. M. Schult, A. M. Whitehead, and B. G. Bokhour. 2021. Veterans Health Administration’s whole health system of care: Supporting the health, well-being, and resiliency of employees. Global Advances in Health and Medicine 10:21649561211022698. https://doi.org/10.1177/21649561211022698.
RTI (RTI International). 2019. Evaluation of the Maryland All-Payer Model. Available at: https://downloads.cms.gov/files/md-allpayer-finalevalrpt.pdf (accessed May 19, 2022).
Salinsky, E. 2017. The Nuka System of Care. Available at: https://scfnuka.com/wp-content/uploads/2016/09/NUKA-CaseStudy.pdf (accessed June 21, 2022).
Sapra, K. J., K. Wunderlich, and H. Haft. 2019. Maryland total cost of care model: Transforming health and health care. JAMA 321(10):939-940.
Sholl, J. n.d. The Profits of a Healthy Workplace. Available at: https://experiencelife.lifetime.life/article/the-profits-of-a-healthy-workplace (accessed June 2, 2022).
Southcentral Foundation. 2017. Malcolm Baldrige National Quality Award 2017 Application. Available at: https://www.baldrigeinstitute.org/HigherLogic/System/DownloadDocumentFile.ashx?DocumentFileKey=cd2dbc11-58b5-97b8-4d8f-6432ff6b5e3f&forceDialog=0 (accessed June 21, 2022).
Southcentral Foundation. n.d. About Us: NUKA FAQs. Available at: https://scfnuka.com/about-us/#toggle-id-6 (accessed June 21, 2022).
SSA (Social Security Administration). 2003. Medicare Modernization Act. Available at: https://www.ssa.gov/privacy/pia/Medicare%20Modernization%20Act%20(MMA)%20FY07.htm (accessed October 13, 2022).
Sullivan, J. 2021. States Are Using One-Time Funds to Improve Medicaid Home- and Community-Based Services, But Longer-Term Investments Are Needed. Available at: https://www.cbpp.org/research/health/states-are-using-one-time-funds-to-improve-medicaid-home-and-community-based (accessed October 13, 2022).
Szanton, S. n.d. Community Aging in Place: Advancing Better Living for Elders (CAPABLE). Available at: https://www.aannet.org/initiatives/edge-runners/profiles/edge-runners--community-aging-place (accessed June 23, 2023).
The King’s Fund. n.d. Nuka System of Care, Alaska. Available at: https://www.kingsfund.org.uk/publications/population-health-systems/nuka-system-care-alaska (accessed March 22, 2023).
Thomson Reuters. 2011. Evaluation of Practice Models for Dual Eligibles and Medicare Beneficiaries with Serious Chronic Conditions. Available at: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Medicare-Geographic-Variation/Downloads/PACESiteVisitReport.pdf (accessed April 6, 2022).
United States Code. 2022. 254b. Health Centers. Available at: https://uscode.house.gov/view.xhtml?req=granuleid:USC-prelim-title42-section254b&num=0&edition=prelim (accessed August 16, 2022).
UnitedHealth Group. 2022. UnitedHealth Group Commits $25 Million to New England Healthy Neighborhoods Fund. Available at: https://www.unitedhealthgroup.com/newsroom/2022/2022-07-12-uhg-commits-25mil-to-healthy-neighborhood-fund.html (accessed June 23, 2023).
U.S. Impact Investing Alliance. 2021. Impact in Place: Emerging Sources of Community Investment Capital and Strategies to Direct it at Scale. Available at: https://www.newyorkfed.org/medialibrary/media/outreach-and-education/community-development/emerging-sources-of-community-investment/community-investing-bank-report-final-20210518 (accessed August 17, 2022).
VA (U.S. Department of Veterans Affairs). 2021. Whole Health Circle of Health. https://www.va.gov/WHOLEHEALTH/circle-of-health/index.asp (accessed March 28, 2022).
VA. 2022. Whole Health. https://www.va.gov/wholehealth (accessed March 28, 2022).
Whitehead, A. M., B. Kligler. 2020. Innovations in care: Complementary and integrative health in the Veterans Health Administration whole health system. Medical Care 58:S78-S79.
WI DHS (Wisconsin Department of Health Services). 2021. Include, Respect, I Self-Direct. Available at: https://www.dhs.wisconsin.gov/iris/index.htm (accessed April 11, 2022).
Wright, B. 2015. Voices of the vulnerable: Community health centers and the promise and peril of consumer governance. Public Management Review 17(1):57-71. https://doi.org/10.1080/14719037.2014.881537.
This page intentionally left blank.









































