Confronting Chronic Neglect: The Education and Training of Health Professionals on Family Violence (2002)
Chapter: 4 Forces Influencing Health Professionals' Education
4
Forces Influencing Health Professionals’ Education
Health professional curricula evolve in the larger societal context and may be influenced by a number of factors. The committee identified a number of forces with the potential to influence curriculum development, implementation, and sustainability and explored the impact of each. The factors considered include training environment issues; accreditation, licensure, and certification requirements; individual issues for health professionals; the influence of health professional organizations and other stakeholder groups; laws mandating reporting and education about family violence; and funding.
Throughout its discussion of challenges to training, the committee struggled with two issues. First, little research has been published regarding factors that challenge or become barriers to educational efforts or the relationship between such factors and education. Second, some research has been published to provide empirical support for the impact of various factors on health professional practice. The committee often had difficulty distinguishing among effects on practice and education, as the experiences of individual committee members suggest that factors that become barriers to practice are also barriers to education. Many teaching faculty are also clinically active practitioners in their fields, and much education received by health professional students takes place in clinical settings (either inside or outside the academic institution). Thus challenges to training are difficult to distinguish from issues related to the clinical care of patients at risk for family violence. Despite perceptions of a relationship or similarities between challenges to education and barriers to practice, without further research, only
inferences can be made. The committee has attempted to distill those concerns pertinent to the education and training of health care professionals.1
INTRINSIC INFLUENCES ON THE TRAINING ENVIRONMENT
Forces intrinsic to settings of health professional training may shape curricula. Such factors include: (1) curricular time and educational priorities and (2) institutional culture and norms. Curricular time refers to the specific course(s), hours, or other time allotted to training on family violence. How the time is used is dictated in part by the recognition of educational needs and determinations of the extent to which those needs will be met, involving setting priorities for the limited time available. Institutional culture and norms refers to the professional values and beliefs within the training environment.
The following discussion relies on the data available, the experience of committee members, and reports of others in health professional education elicited during a public forum the committee held on this topic, as well as other communications. The majority of the available literature focuses on physician and nurse education.
Curricular Time and Educational Priorities
Recognition of the Need for Training on Family Violence
Family violence, although of ancient origins, is newly recognized as a substantial concern for the public health and health care systems. For many in health care, it is perceived more easily as a social or legal problem. In fact, historically, society in general and some health professions in particular have considered family violence to be primarily a social or legal problem and have been slow to recognize its significant health component. As recently as 15 years ago then-Surgeon General C. Everett Koop convened the first workshop linking violence and public health. In Dr. Koop’s words:
Identifying violence as a public health issue is a relatively new idea. Traditionally, when confronted by the circumstances of violence, the health professionals have deferred to the criminal justice system. . . . [Now] the professionals of medicine, nursing, and the health related social services must come forward and recognize violence as their issue. (1991:v)
Koop’s 1985 Conference on Violence as a Public Health Problem (DHHS, 1986) provided leadership in recognizing violence in general, including all forms of family violence, as a health problem. Recommendations from that conference covered inclusion of information about all forms of family violence in basic and continuing education for all health professionals and in certification, licensing, credentialing, and board examinations. The conference also recommended that the professions develop standards of practice and care, to be incorporated into family violence education.
Progress appears to have been made on health professionals’ recognition of family violence as a health issue. For example, in 1991, the American Nurses Association published guidelines for identifying and treating intimate partner violence (ANA, 1991); the American Medical Association did the same in 1992 (AMA, 1992).
Some evidence that the attitudes of individual health professionals have begun to shift also exists. For example, in a 1995 survey of obstetrics-gynecology physicians, 86 percent reported a belief that intimate partner violence is a medical problem (Parsons et al., 1995). This belief appears to be even stronger in the nursing profession. One survey shows that fewer than 4 percent of private office nurses, 5 percent of public health nurses, and 3 percent of hospital nurses agreed with the statement that intimate partner violence is not a medical problem (Moore et al., 1998). In a survey of 107 nursing educators representing associate degree (38 percent) as well as baccalaureate and higher programs, all respondents agreed that all nursing students need to be taught the signs of abuse across the age span (Woodtli and Breslin, 1997). More than 75 percent felt that content on family violence was inadequate, and only 15 percent felt that faculty had adequate knowledge and skills to teach the topic competently. The majority (86 percent) were of the opinion that the content should be integrated throughout the curriculum, but only 33 percent said that resources for faculty and students on the subject were accessible. Only a few programs have a specific course on family violence, and those are generally elective courses. Some clinicians assert that, while family violence is indeed an important health problem, it is not something they themselves encounter (Sugg and Inui, 1992; Reid and Glasser, 1997).
Currently, the sentiment among health care providers that family violence lies outside the purview of the health professions seems most persistent among dentists and dental hygienists. Studies demonstrate that dental professionals vary in their response to receiving education on child abuse in dental school (Ramos-Gomez et al., 1998; Von Burg and Hibbard, 1995). In a 1994 survey of dentists, dental hygienists, physicians, nurses, psychologists, and social workers, providers were asked to respond to the statement: “Professionals in my discipline have as much responsibility to deal with problems of family violence as they do to deal with other clinical problems.” In this study, 98 percent of psychologists, 97 percent of social workers, 87 percent of nurses, and 85 percent of physicians
agreed. However, 47 percent of dentists and 46 percent of dental hygienists disagreed (Tilden et al., 1994).
Educational Needs and Priorities
Health professional curriculum development occurs in an environment of competing needs in which diverse curricular objectives must be sorted and prioritized. With the continuing increase of knowledge and expertise in health care as more research is conducted and published, potential topics for education increase while the educational time available remains the same. The need to add any “new” topic, such as family violence, to an already-packed curriculum may mean reducing or eliminating some other topic. Despite the increasing belief that family violence is an important issue for health care, training efforts on family violence may be perceived as displacing other more established educational topics long considered necessary to prepare health care professionals for clinical practice (Alpert, 1995).
Historically, clinical practice and the education that informs it have focused on acute trauma, physical injury, and disease. The U.S. health care system currently reflects the medical needs of the mid-20th century, when most Americans sought care for acute illness, injury, or childbirth (IOM, 1997). The American health care system is well suited to handle physical illnesses and injuries that used to be the predominant causes of morbidity and mortality, but it is not so well prepared to handle complex health issues with social underpinnings that are in the legitimate purview of health care and of public health (Fox, 1993; Wilkinson and Forlini, 1999).
Family violence is a complex, multifactorial problem that extends beyond these traditional focuses of medicine to social and ethical issues. Treating an acute injury per se does not require that the provider investigate the cause of the injury or evaluate the predisposing factors (analysis of which may help to prevent a subsequent injury in the same patient or a similar injury in a different individual). Symptoms of family violence (e.g., injuries, suicide gestures) can be treated without identification of the underlying cause, leaving the patient at risk for subsequent episodes. Furthermore, some physicians feel that it is ill advised to commit time toward learning how to evaluate a frustrating and often incurable situation, especially when there are other, more pressing treatable issues that can be addressed (Mashta, 2000, http://www.bmj.com/cgi/content/full/320/7229/208/a). According to one physician (Sugg and Inui, 1992):
I think we tend to look more on the technical side of medicine, things we can help, like appendicitis. Domestic violence is a big morass which we will never escape. I get a headache thinking about it. And that attitude translates into the type of care we give those patients. (p. 3159)
Existing clinical care and education around family violence issues attend disproportionately to physical injury, despite the broad spectrum of abuse pre-
sentations seen in pediatric, adult, and elder populations (Talley et al., 1994; McCauley et al., 1995; Domino and Haber, 1987; Drossman et al., 1990; Drossman et al., 1995; Walker et al., 1999; Post et al., 1980; Schei, 1990; Jacobson and Richardson, 1987; Longstreth and Wolde-Tsadik, 1993; McCauley et al., 1997; Eby et al., 1995; Eisenstat and Bancroft, 1999). Even when physical injury is documented, clinicians tend to record facts (injury location) without sufficient context (e.g., who inflicted the injury and the circumstances surrounding the event; Warshaw, 1989).
Determining educational needs and priorities becomes even more difficult when little is known about a particular condition, treatment, or outcome. Thus, existing research gaps may limit education on a subject or suggest that it is not a priority. The research base on family violence interventions is deficient (NRC and IOM, 1998). For example, little is currently known about effective methods to detect intimate partner violence, and no data are available to determine the impact of screening and treatment on the incidence, morbidity, and mortality of intimate partner abuse (Cole, 2000). Without such knowledge, providers may be ill equipped to detect intimate partner violence in the health care setting, and appropriate education is difficult to determine (Abbott et al., 1995).
As the perceptions about important topics for health professional education continue to grow, prioritization is likely to become even more difficult. The figures on the magnitude of family violence in society, the health care implications for patients, and the health care services provided by health professionals (discussed in Chapter 2) indicate that family violence is a significant issue for health care, and the available research provides content that can be taught. While the need for family violence education does not ameliorate the need for education on other important topics, neglecting health professional training on family violence will not make the need for it disappear.
Allocation of Training Time and Adequacy of Training
Despite the numbers of existing curricula and beliefs about the need for family violence education, the amount of time allocated to this subject matter has been minimal (MMWR, 1989; Alpert, 1995; Alpert et al., 1998; Kassebaum, 1995). A total of 33 percent of a sample of physicians, nurses, social workers, psychologists, dentists, and dental hygienists reported that they have received no education about child abuse, intimate partner violence, or elder abuse during graduate school, residency training, or continuing professional education (Tilden et al., 1994). Sugg and Inui (1992) found that 61 percent of their sample of primary care physicians reported having had no training on intimate partner violence in medical school, residency training, or continuing education. Although the percentage of subjects who reported having some family violence education increased as the year of graduation became more recent, the lack of training appears to remain prevalent, with social workers reporting the most overall
education in each type of abuse and dentists and dental hygienists the least (Sugg and Inui, 1992). Another survey of 705 academic emergency physicians indicated that only 25 percent could recall receiving any training about elder abuse during their residencies, only 20 percent during continuing education, and only 31 percent had a written protocol for the reporting of elder abuse in their current environment (Jones et al., 1997). Since 1998, the Association of American Medical Colleges (AAMC) has surveyed graduating medical students to assess the treatment of the topic of domestic violence in their medical school curricula. Nationally, the student perception of inadequate treatment decreased from 33 percent in 1998, to 31 percent in 1999, and 28.4 percent in 2000 (AAMC, 2000). The survey addresses only student perceptions and does not evaluate the content or intensity of the curricula. In another study, 86 percent of 111 medical schools reported existing curricula in adult intimate partner violence, yet a comparison of deans’ and students’ perceptions about curricular coverage of intimate partner violence yielded significant differences about the adequacy of coverage (Alpert et al., 1998).
Even in professions expressing concern about inadequate training in family violence, training may not be inadequately addressed. The American Psychological Association’s (APA) Presidential Task Force on Violence and the Family (1996) has addressed the issue, yet most clinical psychologists in a national sample rated their graduate training on child maltreatment as poor and their internship training about the issue as only slightly better (Pope and Feldman-Summers, 1992). In a 1992 study, approximately 90 percent of clinical, counseling, and school psychology programs reported that they had no courses specifically addressing child abuse and neglect (Howe et al., 1992). In addition, approximately two-fifths of mental health workers reported that they had not received any training on intimate partner violence (Campbell et al., 1999). Recognizing these issues, the APA Working Group on Implications for Education and Training of Child Abuse and Neglect (Haugaard et al., 1995) noted a number of impediments to curricular reform to reduce the gap between psychologists’ modal and optimal levels of expertise in responding to child maltreatment. Among these was a “lack of appreciation of the importance of including information about child abuse and neglect in current curricula by administrators, teachers, and trainers” (p. 79).
Institutional Culture and Norms
Institutional culture can create subtle messages regarding the educational and practical value of particular topics to health professionals and the status of those who teach and work with those topics (see, e.g., Hafferty, 1998; Hundert et al., 1996; Marinker, 1997). Challenging cultural issues include inertia or resistance to change, the dynamics of power, the need for leadership, professional socialization, multidisciplinary collaboration, and marginalization. Curricular revision requires attention to the culture and norms within the institution.
Studies suggest that faculty resistance to change is a major barrier to curricular reform, as the drive to maintain the status quo often overrides the desire to make educational innovations (Bloom, 1989; Robins, 2000). Even when medical curricula do undergo major reform, the changes that are instituted tend to revert or “drift” back to previous educational patterns (Robins, 2000). The drift that is observed is quite consistently in the direction of a decrease in social science, humanities, and ethics instruction in the first-year curriculum, due at least in part to a feeling among basic scientists that this material is taught prematurely at the expense of essential basic science(s).
Moreover, establishing programs is more challenging if the topic is not embraced by academic leaders or widely recognized by the faculty (Hendricson et al., 1993; Kendall and Reader, 1988). Unless there is an internal mandate from an influential institutional leader (e.g., the dean or a department chair) or an external mandate from an accrediting body or legislative authority, curricular innovation may be difficult to achieve (Alpert et al., 1997a; Bussigel et al., 1988).
Health care professional students and trainees are socialized within this culture and power structure to emulate the beliefs and practice patterns of their teachers and role models in the clinical setting. Norms reinforced through practices that students observe in clinical training may reflect beliefs about professional roles and functions (Brandt, 1997). Issues such as family violence, often requiring multifaceted responses, frequent interdisciplinary cooperation, and attention to social or personal issues may challenge the norms underlying the professional socialization of many health care professionals, such as those related to independent practice, clinician-patient relationships, and awareness of social issues (Warshaw, 1997).
In addition, these professional norms can be understood against a backdrop of deeply embedded social norms and values regarding family violence in society. Like the general public, health professionals are raised and trained in a society in which public intervention in “private” family matters has been proscribed until recent years and in which victims of family violence, particularly women and children, historically have had relatively little public recourse.
American society has a long history of maintaining the privacy of family matters. For example, from the early colonial period onward, American courts affirmed a husband’s right to physically “discipline” his wife (O’Faolain and Martines, 1974, p. 188). It was not until the late 19th century that states finally began to move away from actually condoning a husband’s use of physical force against his wife (e.g., Fulgham v. State, 46 Ala. 143, 146-47 [1871]; Commonwealth v. McAfee, 108 Mass. 458, 461 [1971]; Gorman v. State, 42 Tex. 221, 223 [1875]).
No such laws exist on the books today, and over the past 30 years every state has enacted a protective order statute that allows judges to prohibit batterers from assaulting or threatening their intimate partners and to provide victims with a broad range of protective measures (Epstein, 1999). However, remnants of the reluctance to intervene on behalf of victims persisted into the 1990s. For example, a nation-
wide survey of intimate partner violence service providers documents that some judges hearing civil protection order cases apply artificially heightened standards of proof (e.g., requiring physical evidence or unbiased witnesses) that make it more difficult for victims to succeed (Kinports and Fischer, 1993).
Similarly, courts have long tolerated parental authority to discipline children in the name of family privacy (e.g., State v. Jones, 95 N.C. 588, 588 [1886]). However, in the 1960s, the United States began to take an active approach to decreasing violence against children. Since then, every state has designated a wide range of behaviors as illegal child abuse and neglect and has enacted mandatory reporting legislation, requiring certain professionals to report instances of child maltreatment. But the emphasis on the private domain of families persists; for example, most states still exempt parents from sanctions for forms of corporal punishment that otherwise would constitute criminal assaultive conduct (e.g., Johnson, 1998).
The beliefs about private family matters reflected in the legal system also appear to affect health professionals. Health professionals have expressed concern or discomfort with intervening in situations they view as private matters and may demonstrate these reservations when teaching or supervising students. Studies of the values and beliefs of emergency service staff, including physicians, physician assistants, and social workers at four hospitals, indicate that 90 percent of the study subjects believed that they should try to identify battered women, and 82 percent considered this to be “part of their job.” But the same group failed to respond to intimate partner violence in any way in 40 percent of cases and responded only partially in 49 percent. The study’s investigators hypothesized that medical staff want to help but feel uncomfortable doing so because they view inquiry and intervention about intimate partner violence as invading their patients’ personal affairs (Kurz and Stark, 1988; Yllo and Bograd, 1998).
Open-ended interviews of primary care physicians regarding attitudes about intimate partner violence suggest that privacy concerns were among the most frequently identified barriers to identification and intervention (Sugg and Inui, 1992). Fear of offending the victim “often originated in the physician’s discomfort with areas that are culturally defined as private. . . . The uncertainty of whether patients would consider domestic violence a legitimate area to probe was distressing. . . . Physicians felt that by even broaching the subject of violence, the patient would take offense.” Reluctance to “overstep the bounds of what is private . . . leaves the physician wary of how to approach the issue” (Sugg and Inui, 1992, pp. 1358-1359). In a study of pediatric emergency medicine fellows, 40 percent labeled a reluctance to invade family privacy as either a major (7.7 percent) or a minor (32.8 percent) obstacle to identifying and reporting suspected battering of a child-patient’s mother (Wright et al., 1997). And 58 percent of these physicians also reported some degree of personal discomfort with intimate partner violence cases.
The nursing and social work literature also identify concerns about intrusions into private or family matters when approaching issues of family violence.
For example, a survey of social workers, physicians, and nurses found that 63 percent of those surveyed cited personal discomfort and 57 percent cited concern about family privacy when asked about barriers to their own effective responses in intimate partner violence and sexual assault cases2 (McGrath et al., 1997). Even if intervention on behalf of victims of family violence is accepted, contrary practices may suggest a different message. Instructional settings create learning environments in which what students learn may vary from what is taught (Hafferty, 1998). So, even if taught to intervene, students may not observe or be involved with practicing health professionals who do intervene. Thus, they may not learn to do what they were taught.
In addition to concerns about privacy, the need for multidisciplinary collaboration in responding to family violence may create challenges to training. For example, multidisciplinary and nonclinical teaching partners are considered important to health professional education on family violence, as intervening in abusive situations usually involves interaction among the health, social, and legal systems (e.g., American Academy of Family Physicians, 1994). However, the committee’s review of existing health professional curricula indicates that collaborative practice may be discussed, but it is not usually demonstrated. The materials may suggest a health care team model for responding to family violence victims and may provide information on referral services but rarely involve members of other professions (e.g., social workers, district attorneys) in the educational efforts. What is taught is not reinforced in clinical experiences. For example, while nurses were more than twice as likely as physicians to consult with another professional when detecting situations of abuse, physicians were more likely to try to handle the situation alone with the patient (Tilden et al., 1994).
Social norms may also result in the marginalization of health professionals who do assume leadership roles in family violence. Students may make their career choices, in part, based on others’ perceptions of particular fields (Hunt et al., 1996). A study of the response to family violence in five diverse communities indicates that health care professionals who chose to work consistently with family violence victims were marginalized by their colleagues and institutions. These professionals also reported economic, social, and psychological disincentives to providing care to this population (Cohen et al., 1997).
The presence and efforts of a singular charismatic faculty leader paradoxically can be an impediment to curricular innovation. That leader may singlehandedly take responsibility for family violence curricula or extracurricular activities. However, once the leader moves on to other pursuits, the programs generally wither due to insufficient institutional commitment (Cohen et al., 1997). Although charismatic
leaders are an important impetus for curriculum development, alone they are insufficient for establishing permanence for education and training in family violence without concurrent institutional changes. Sole dependence on such individuals can create challenges for stability, given the fluidity of American society and the frequency with which individuals change their institutional affiliations.
An example of this phenomenon has been published in the intimate partner violence literature (McLeer et al., 1989). The initial success of a novel emergency department screening program for intimate partner violence reverted to its inadequate baseline screening rate following the departure of the individuals primarily involved with the intervention. To maintain such efforts, the reform must be institutionalized. The challenge is to establish systems and procedures that help create a foundation that is sufficiently flexible to sustain innovations and behavioral changes.
ACCREDITATION, LICENSURE, AND CERTIFICATION REQUIREMENTS
Health professions are subject to numerous legal and voluntary requirements or guidelines related to ensuring the competence of practicing professionals, practice standards, and professional and patient protections. These requirements can serve as leverage points for the inclusion of particular educational content in a profession’s various modes of training. For example, students may be more likely to receive training on a particular topic if the requirements for professional accreditation demand it or subspecialty certification exams include it. Even without explicit requirements, a health professional organization can exert influence on training content by encouraging or supporting such efforts. The committee reviewed existing accreditation, licensure, and certification requirements to identify family violence components.
Accreditation
Accreditation of professional disciplines determines the course of study required to be part of the profession.3 In some cases, this may be as explicit as indicating the number of didactic hours of a particular subject area or as broad as specifying the requisite focal areas of study for a profession. Thus, requirements for the accreditation of professional disciplines can influence, if not in part define, the educational content in health professional schools.
The committee reviewed the accreditation standards as of December 2000
for the professions included in this study to identify requirements related to family violence of any or all types (see Appendix A). The review indicates that, overall, few accreditation requirements related to family violence exist. The standards for medicine suggest that programs should (rather than must) assert the ramifications of family violence as a social problem. While social work requirements include no specific mention of family violence in its curriculum guidelines, it does allude to those who are at risk of victimization or are oppressed. Similarly, nursing, dentistry, psychology, and physician assistants do not specifically include family violence education as part of their accreditation process. Certain subspecialty areas do have education or training requirements in specific types of family violence. For example, the American Board of Obstetrics and Gynecology requires intimate partner violence training, and the American Board of Pediatrics requires training on child abuse and neglect.
Licensure
Licensure is the process by which a state, usually through an examination, regulates the practice of a specific profession. This examination can be administered on a national level, medicine being the principal example, but more often is administered by the state issuing the license. This state-directed exam may be a combination of both a nationally developed test and questions specific to certain state laws and regulations, or it may be state generated, with some questions drawn from a national data bank. The exam content can reflect required and desirable areas of study.
While a comprehensive review of state licensing laws for each health profession was beyond the scope of this report, the committee reviewed national exams for content on family violence, with the understanding that these exams play different roles with regard to licensure within the professions. This review revealed that licensure exams from the National Board of Medical Examiners and the National Council on Boards of Nursing provide the most explicit reference to family violence content. The National Board of Medical Examiners issues a three-step United States Medical Licensing Exam, the third step of which may include some questions related to child abuse, elder abuse, and sexual abuse.4 The National Council on Boards of Nursing’s Nursing Certification Licensure Exam contains a psychosocial adaptation section (5-11 percent of the questions). The content includes child abuse and neglect, elder abuse and neglect, and sexual abuse, as well as behavioral interventions, chemical dependency, crisis intervention, and psychopathology. Other organizations also indicate content on family violence on their exams but do not explicitly delineate the breakdown of components.
Certification
Certification of health professionals has two purposes. First, a state may protect a particular professional title, such as social worker or psychologist, by requiring that a person have a certain type and level of education in order to use it. These certification laws do not, however, regulate practice of the profession. Second, certification may recognize that an individual has successfully completed the national exam for a particular specialty and, in so doing, has demonstrated competence in that specialty. For example, certification by the American Board of Pediatrics suggests that a physician has the knowledge, skills, and attitudes to practice pediatrics in congruence with the national standard.5 The Academy of Certified Social Workers certification indicates an individual’s readiness for independent, unsupervised social work practice, including supervision of junior-level practitioners.
A review of current specialty certifications as of December 2000 suggests that several specialties require some training in the area of family violence. This requirement is usually closely linked to the target patient population for the specialty (e.g., pediatrics and child maltreatment). In such instances, a small number of questions on family violence appear on the certifying exam. Only a few specialties require training in all areas of family violence. Emergency medicine, for example, addresses all areas of family violence in section 18 on traumatic disorders (11 percent of the exam questions). The nurse midwife certification exam has specific questions on domestic violence and sexual assault, and the pediatric nurse practitioner exam contains questions on child abuse. However, specific content for exam questions can change from year to year and is dependent on the makeup of the committees assigned by the practice organizations.
INDIVIDUAL ISSUES: PROFESSIONAL AND PERSONAL FACTORS
The development and impact of health professional education on family violence may be affected by professional or personal concerns, beliefs, or experiences. These may explain a lack of clinician initiative, one of the most common reasons cited for failing to detect abused women (Ferris and Tudiver, 1992). The following discussion is intended to demonstrate the extent to which individual factors can affect training about family violence, but it may apply differently to the health professions considered in this report.
Professional Issues
Professional issues at the individual level involve those related to health care professionals’ roles and functions. Among the primary issues affecting individual response to family violence are time, inadequate training, uncertainty about how to respond, perceptions of patient noncompliance, and inadequate incentives for involvement.
Many health care providers feel they lack sufficient time to adequately assist victims of abuse. In one survey (Sugg and Inui, 1992), 71 percent of physicians interviewed stated that time constraints were a major reason they refrained from asking patients questions about family violence. Primary care practitioners frequently chose to refrain from involvement because they felt that the issue would consume their already limited time. One physician said (Sugg and Inui, 1992):
I think that some physicians, and I do the same thing, if you are very busy and have lots of patients waiting, you just don’t ask a question that you know is going to open a Pandora’s box. Even if it crosses your mind, you don’t ask. (p. 3158)
Many primary care physicians were frustrated with what they perceived as an “extra” societal responsibility, stating that they could quickly become overwhelmed in caring for “nonmedical” issues (Sugg and Inui, 1992). For example, in one survey, an estimated 37 percent of California primary care physicians cited lack of time as a major barrier to the identification and referral of patients experiencing intimate partner abuse (Rodriguez et al., 1999). Nevertheless, in a study of Alaskan physicians who provide prenatal care, time constraints were not associated with differences in screening rates (Chamberlain and Perham-Hester, 2000).
Even if time were not an issue, health care providers have expressed concerns regarding inadequate preparation, uncertainty about how to proceed if maltreatment is disclosed, and frustration with the inability to ensure positive outcomes for the victims. For example, one study indicates that many health professionals believe they have not had adequate medical education or training on intimate partner violence (Reid and Glasser, 1997; see also Chapter 3, this volume). In another study of emergency room physicians, an existing protocol recommended referral of victims of intimate partner violence to a social worker or mental health professional and also listed referrals for shelter, legal assistance, and counseling. Despite this, mental health consultation was documented in only 4 percent of 52 cases, social work referral was obtained in only 8 percent, and shelter information or other referrals were offered in only 2 percent, due in part to a lack of knowledge about referral resources and how to access them (Warshaw, 1989).
Receiving continuing education on intimate partner violence has been associated with increased screening for abuse (Carbonell et al., 1995; Chamberlain and Perham-Hester, 2000). However, other studies have shown this association to not be significant after adjustment for other factors (Rodriguez et al., 1999; Chamberlain and Perham-Hester, 2000). Evaluations of multifaceted domestic violence in-
terventions that have included training have documented improvement in screening associated with the intervention (Thompson et al., 2000; Harwell et al., 1998). A review of the literature (Waalen et al., 2000) that examined interventions and barriers to screening for intimate partner violence reveals that interventions limited to the education of providers had no significant effect on screening or identification rates, but interventions that are multifaceted (e.g., education, protocols, posters) were associated with significant increases in screening and/or identification rates. A causal relationship between these interventions that include education and screening, however, has not been established.
Some health professionals indicate that they are frustrated even when they do offer treatment and provide referrals. According to one physician: “I get to the point where I feel discouraged because I feel like, with someone that’s in . . . an abusive situation, until that person’s ready to take care of it, I’m banging my head against the wall” (Sugg and Inui, 1992, p. 3159). Another believes he “is not sure he would have any effect anyway. I certainly find that most of my advice on smoking and alcohol and other self-destructive behaviors has no effect on people and it gets very frustrating” (p. 3159).
This sense of frustration is exacerbated by perceptions of patient noncompliance. Health care professionals work to develop plans of care to address the health complaints and concerns raised by their patients. The provider might want to see the patient get out of an abusive relationship and offer advice to this effect without fully considering the victim’s beliefs, resources, and the context of her or his life at that time. Thus, for reasons that cannot be fully explored in the office setting, the patient may choose not to do “what the doctor says” (NRC and IOM, 1998). The provider inevitably feels frustrated and the patient feels blamed for not doing what she or he was told. The noncompliant patient thus becomes an obstacle for the provider, who then offers less and less attention and reinforcement, which in turn generates less of a reason for the patient to be compliant (Warshaw, 1993). In one study of family physicians, patient unresponsiveness was given as a common reason for failing to detect abused women (Ferris and Tudiver, 1992). The new movement toward shared decision making in health care holds promise of countering real and perceived issues of noncompliance (Angell, 1999). This dynamic is particularly important in family violence; a victim might feel particularly vulnerable in the health care setting and thus be reluctant to disclose abuse or act on the health professional’s advice (Warshaw, 1993; Warshaw and Ganely, 1998).
In addition to a sense of inadequate capacity and frustration, the incentives for health professionals to participate in teaching appear inadequate. Academic faculty incentives, such as promotion, are based largely on publications generated by funded research and by service (patient care and service to the academic institution) and less so on education, particularly in medicine (Guze, 1995). Physicians, for example, who treat family violence victims believe that such work
garners little respect from their peers and will not result in prestigious research grants and other support necessary for promotion and tenure (Cohen et al., 1997).
Personal Issues
Beyond professional issues, individual health professionals may also experience personal issues that create challenges for education related to family violence. Among these are personal values and biases, personal experience with family violence, and vicarious traumatization. Like anyone else, health care students and professionals bring personal values and biases to their educational and clinical experiences. For example, health care professionals and trainees may make assumptions about their patients based on socioeconomic status and lifestyle choices, which may or may not be borne out by the evidence. In some cases, for example, close identification by a health professional with a patient’s lifestyle or socioeconomic class produces an assumption that no violence is occurring, whereas distinct differences in lifestyle and class produce an expectation of violence (Sugg and Inui, 1992; Newberger, 1977). This preconception also can foster a belief that “nothing will be done anyway” (Cohen et al., 1997), as the underlying socioeconomic differences will not change. These attitudes of disillusionment accompany a growing critique of victim “noncompliance” with the referrals and advice of the clinician (i.e., perceptions that victims will not change their situations). For example, an estimated 78 percent of California’s primary care physicians felt patients’ lack of disclosure was a major barrier to physician identification of intimate partner abuse and referral of patients (Rodriguez et al., 1999).
Some personal values regarding family violence and difficulty in addressing it may stem from personal experiences with victimization. Many health professionals report personal experiences with family abuse. For example, 57.5 percent of nurses in an urban trauma center reported such experiences (Ellis, 1999). Feelings of vulnerability related to personal experiences with abuse may pose a challenge to training health care professionals. However, surveys of nurses and physicians have found no significant association between having a personal history of violence and reported screening behavior for intimate partner violence (Rodriguez et al., 1999; Parsons et al., 1995; Moore et al., 1998). Having personally known a victim of abuse has been positively associated with an improved response to abuse (Saunders and Kindy, 1993).
While the evidence on the impact of personal experiences with family violence is inconclusive, some evidence suggests that vicarious or secondary traumatization occurs. A number of clinical reports reveal this phenomenon among professionals who work with victims of crime, abuse, or disasters (McCann and Pearlman, 1990; Neumann and Gamble, 1995; Talbot et al., 1992). Such reports indicate that clinicians, perhaps especially those who are inexperienced, sometimes themselves experience some of the symptoms of post-traumatic stress dis-
order after they hear accounts of victimization. Furthermore, clinicians’ concepts of interpersonal situations (e.g., their perceptions of trustworthiness) may be affected adversely, although such an effect was not observed in the one large survey about therapists’ experience with vicarious traumatization (Brady et al., 1999). Brady et al. did find that post-traumatic symptoms were positively related to therapists’ level of work with survivors of child or adult sexual abuse. Whether this relationship reflected a selection factor or a causal linkage is unclear. The anecdotal reports of vicarious traumatization are sufficiently common to suggest a need for preparation of clinicians in training for the emotional reactions that they may have to victims’ stories.
PROFESSIONAL ORGANIZATIONS AND STAKEHOLDER GROUPS
This section reviews the impact of health professional organizations and several stakeholder groups on professional education in family violence. Included in these stakeholder groups are advocacy groups, victims, and health care payers and providers.
Health Professional Organizations
Health professional organization statements, guidelines, positions, and policies that address health professional education or training on family violence explicitly are noted in Appendix B. Organizations such as the American Medical Association, the American Academy of Physician Assistants, the American Academy of Pediatrics, the American Nurses Association, the American Psychological Association, the American Dental Association, and the National Association of Social Workers have issued positions, policy statements, and guidelines designed to encourage or require training in family violence. For example, in 1992, the American Medical Association (AMA) issued a series of educational pamphlets about family violence to provide practicing physicians with background and clinical direction in caring for victims. Many state medical associations held statewide educational campaigns for their members following that AMA initiative. In 1972, the American Academy of Pediatrics published a slide series on child maltreatment, which was updated in 1996, and published guidelines on child maltreatment for the first time in 1991, updating them in 1999.
The American College of Obstetricians and Gynecologists (ACOG) was the first health care professional organization to address intimate partner violence systematically. In 1989, it sent all members a technical bulletin giving information on abuse during pregnancy, assessment, and referral. ACOG has continued its leadership in this area (see Figure 4.1), and its screening guidelines have been endorsed by other health professional organizations (Frye, 2001).
The American Nursing Association passed resolutions on violence against
women in 1987 and 1991, calling for routine screening for domestic violence and “routine education” of nurses. The Emergency Nursing Association, the Association of Women’s Health, Obstetric, and Neonatal Nurses, the American Association of Orthopedic Nursing, and the National Black Nurses’ Association have also passed resolutions recognizing violence against women and intimate partner violence as areas of nursing concern, calling for increased nursing and other health care professional education. In 1997, the National Nursing Summit on Violence Against Women, under the auspices of the U.S. Public Health Service’s Office on Women’s Health of the Department of Health and Human Services, also called for preprofessional classroom and clinical content on violence against women. This was followed by the American Association of Colleges of Nursing position paper in 1999 calling for the same and detailing the objectives and the type of content to be included (see Chapter 6 for details). With a grant from the Health Research and Services Administration, the American College of Nurse Midwives included violence against women systematically in the education of its professionals. It developed a curriculum for basic education and continuing education materials and ensured ongoing attention to the issue through inclusion in certification exams and monitoring of programs for appropriate content (see Figure 4.2).
The Presidential Task Force on Violence and the Family of the American Psychological Association (1996) provided a general review of relevant research and considered psychology’s potential contributions to responses to child abuse and neglect, intimate partner violence, and elder maltreatment. The task force appeared to start from an assumption that training about family violence for psychologists and other service providers has typically been inadequate, a perception echoed by most clinical psychologists themselves, especially those trained prior to 1985 (Pope and Feldman-Summers, 1992). The task force concluded (APA, 1996):
Each year, large numbers of families who are victimized by violence seek help at a time of critical need, and they often are unable to locate professionals with specific training to help them take steps to stop violence at home and heal from their trauma. This situation is, in part, a consequence of the presently fragmented and irregular nature of professional education and training in family violence evidence interventions. Individual practitioners without institutional support conduct a great deal of family violence intervention training; university programs for training and research in these specialized interventions are rare. There is a pressing need for stable institutional resources with a critical mass of expertise to test promising new interventions, to train newcomers to the field, and to disseminate information about successful intervention models to practitioners in several professions. It is important to begin teaching about family violence in undergraduate psychology curricula and to integrate studies of trauma and violence throughout all levels of psychology education. (pp. 134-135)
The task force specifically recommended that “routine screening for a history
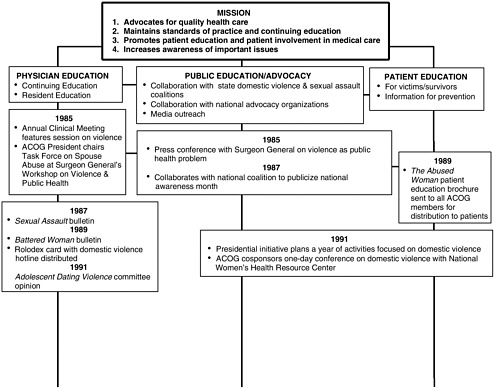
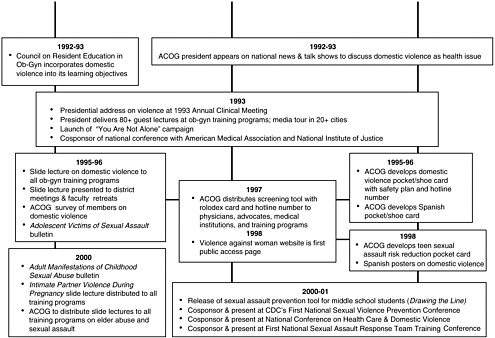
FIGURE 4.1 Overview of the American College of Obstetricians and Gynecologists response to violence against women. Source: American College of Obstetricians and Gynecologists. 2000. Overview of the American College of Obstetricians and Gynecologists’ Response to Violence Against Women. Washington, DC.
of victimization be included in standard medical and psychological examinations and be considered in the development of individual treatment plans” (p. 134) and that the necessary training occur to enable such a change in psychologists’ practice.
The National Association of Social Workers adopted a statement on family violence in 1987, reaffirmed it in 1993, and redrafted it in 2000. No other social work organizations, including the American Board of Examiners in Clinical Social Work and the Clinical Social Work Federation, appear to have specific expectations regarding family violence training for their members.
Advocacy Groups
A number of coalitions and initiatives have been developed to foster knowledge in the area of family violence. Generally, these groups and efforts target a particular type of family violence and appear to have been involved in increasing education on family violence issues. These groups include direct providers at shelters, other victims’ services providers, members of grassroots movements that established those programs, and victims, as well as researchers and educators. However, their full impact is unknown. In addition, a number of advocates have expressed concerns about involvement with the health professions, believing health professionals may create obstacles to advocacy efforts and health professional education on family violence, if they do not understand or support the work the advocates are doing.
Systematic efforts were initiated in the 1960s and 1970s to integrate child maltreatment into the curricula of all of the health professions. The Child Abuse Prevention and Treatment Act of 1974 mandated the establishment of the National Center on Child Abuse and Neglect, which has since become the Office on Child Abuse and Neglect. The legislation resulted in part from efforts by advocacy groups to raise the awareness among helping professions about child maltreatment; it does not specifically address health professional training on child abuse and neglect.
Advocates were a primary force in bringing the issue of violence against women (including child sexual abuse and intimate partner violence) to the attention of health care providers. The first research by health professionals on the subject (outside psychiatry and psychology) was that of Carlson (1977) in social work, Parker and Schumacher (1977) from nursing and medicine, Stark and Flitcraft (1981) in medicine and sociology, Appleton (1980) in emergency medicine, and Campbell (1981) in nursing. Meanwhile, the 1970s were an era when the first battered-women’s shelters were being established in the United States (Schechter, 1982) and when advocates of preventing sexual assault were beginning to address the issue of child sexual assault and rape.
Notable among advocacy efforts is the work of the Family Violence Prevention Fund. This organization has developed an extensive model educational program for health care providers (Ganley, 1998; Warshaw and Ganley, 1998). The
To be viewed as a continuum:
1994 | 1995 | 1996 | 1997 | 1998 | 1999 | 2000 | And Beyond |
* HHS Award to conduct Domestic Violence Education Project (Project MCJ#116084-01) * ACNM Board of Directors creates Ad Hoc Committee on Domestic Violence (later, Violence Against Women) * Committee recommends and BOD approves ACNM Position Statement on Violence Against Women | * ACNM Board of Directors recommends skills in Domestic Violence for all Midwives: Core Competency (ACNM web site: www.midwife.org) * DVEP activities and products in development: Video and manual on clinical skills; education materials for the public (video funded by Pharmacia & Upjohn Foundation) | * Continuing Education activities for ACNM members begin: Regional workshops using the tools; Training of Trainers workshops; workshops and education sessions at the ACNM Annual Meeting and Exhibit * Nurse-Midwifery Education Programs required to include domestic violence education in teaching and clinical skills development | * ACNM Certification Council (ACC) begins including item(s) about domestic violence in Certification Examination for CNMs/CMs * Journal of Nurse-Midwifery Home Study issue (Vol. 41, No.6) on domestic violence. ACNM members and others able to earn continuing education units * Continuing Education Workshops continue | * Proposal developed, together with the International Confederation of Midwives, for a project to work with midwifery associations in developing countries on the issue of domestic violence * Domestic Violence Education Project ends in October, with wide dissemination of materials to other groups and to the Maternal and Child Health Clearinghouse | * ACNM presents a paper on domestic violence and the role that midwives and midwifery associations can play at the Triennial Congress of the International Confederation of Midwives in Manila, the Phillipines * Ad Hoc Committee on Violence Against Women begins work on position statement on female genital mutilation (cutting) | * ACNM Board of Directors and membership approve position statement on female circumcision * ACNM presents at technical consultation on domestic violence sponsored by International Federation of Gynecology and Obstetrics (FIGO) in Naples, Italy * The ACNM’s Domestic Violence Education Project: Evaluation and Results Journal of Midwifery and Women’s Health, Vol. 45, No. 5 | * ACNM’s annual meeting and exhibit, 2001, with several sessions on violence against women |
FIGURE 4.2 The American College of Nurse-Midwives activities and work in domestic violence: a timeline. Source: Vivio et al. (2000). Reprinted with permission.
program provides guidance to many educational and health care delivery institutions around the country that are in the process of developing or implementing training programs. The fund’s training materials appear to have been distributed widely and serve as a reference for many health professionals. Plans to evaluate the program are under way. Other advocacy organizations, including provider advocacy organizations such as Physicians for a Violence-free Society and the Nursing Network on Violence Against Women International, have also been active in developing informational and educational materials and programs.
Advocates recognize the health care needs of victims of family violence, but they have also expressed reservations about the health care system’s response, particularly with regard to victims of intimate partner violence. The concerns include: (1) the potential for the system to revictimize or blame female victims of violence (e.g., Faulk, 1974; Snell et al., 1964; Stark et al., 1981); (2) failure to identify victims (e.g., McLeer and Anwar, 1989); (3) the “medicalization” of a problem believed to be rooted in societal norms and systems; (4) interference with the development of strategies to escape from perpetrators; (5) emphasis on a medical solution to intimate partner violence that may enable society to continue to fail to hold perpetrators accountable; (6) insurance discrimination and loss of health care access (Fromson and Durborow, 1998); (7) overreliance on randomized clinical trials and quantitative measurement of outcomes that miss the complex nuances and intricate contexts of victims’ lives (e.g., Campbell et al., 1999; NRC, 1996; Gondolf et al., 1997; NRC and IOM, 1998); and (8) loss of victim autonomy (NRC and IOM, 1998). Victims of both intimate partner violence and childhood sexual abuse have recounted how the health care system has failed them and how individual health care providers have made the situation worse (Herman, 1992; Sipes and Hall, 1996; Yllo and Bograd, 1998).
To address these concerns and to encourage health professional involvement with family violence issues and victims, advocates have been at the forefront in the training of health care professionals about family violence, particularly violence against women. Many training protocols (e.g., the Family Violence Prevention Fund, the Alaska Family Violence Prevention Project) prescribe the participation of advocates (as well as survivors) in training health care professionals. This joint partnership model of training remains to be evaluated for its efficacy.
In addition, advocates have promoted collaborative research involving partnerships with victims of family violence. Many researchers have undertaken this approach, and descriptions of these collaborations are beginning to be seen in the research literature (Campbell et al., 1999, 2001; NRC and IOM, 1998; Dutton et al., 1999; Gondolf et al., 1997).
Victims
Victims of family violence are being included in at least some of the research and policy decisions on the health care system’s response to family vio-
lence. Many who work with domestic violence and sexual assault are themselves survivors of family violence. They speak, therefore, with the authentic voice of stakeholders as well as professionals in the field (e.g., Buel, 1994). Similarly, adult victims of child abuse have become active in advocacy. Victims of elder abuse, however, are often unable to advocate for themselves due to illness and incapacitation. At least in the area of intimate partner violence, victims have also begun to have a voice in research about needed directions in the health care system (e.g., Gielen, 2001; Rodriguez, 1998, 1999; Sipes and Hall, 1996). Current curricula appear often to include victims of intimate partner violence in educational efforts. These victims share their experiences with students and practicing professionals in an effort to personalize the problem.
The effect of these trends toward the inclusion of victims and victim advocates in professional education remains unclear. No available evaluation research addresses the impact of this trend. Research on educational strategies does suggest that case-based methods are effective (see Chapter 6), and victims and their advocates can provide real-life cases.
Health Care Payers and Providers
Payers have recently begun to express their views about health professional education. Groups such as the Pacific Business Group on Health and the Washington Business Group on Health are attempting to influence professional education in order to improve health care delivery. But neither of these groups to date has made any statements concerning training on family violence.
Blue Shield of California has been actively working in partnership with several large corporations to improve professional education on domestic violence. These programs tend to focus on a specific area of family violence. The extent of their impact has not been studied.
Similarly, several provider organizations (e.g., Kaiser-Permanente in California and Group Health Cooperative of Puget Sound) have included family violence in professional education. Although some of these programs have been publicized and evaluated (see Chapter 5), their impact appears to be limited largely to the areas served by these organizations.
Payers’ reimbursement policies may also impact health professional training about family violence. The literature reflects a heated debate around third-party reimbursement generally, and limited research indicates that reimbursement issues can serve as a disincentive for health professional services for family violence (see, e.g., Krueger and Patterson, 1997; Socolara et al., 2001). One study notes, “[d]octors, nurses and other providers are urged to screen routinely for [intimate partner violence], yet progress is hindered because health systems lack the data, formalized procedures and the reimbursement schemes to fully implement and sustain published screening guidelines” (http://fvpf.org/programs/display.php3?DocID=548/8/01).
Without adequate reimbursement for screening and services provided to victims of family violence, little incentive would seem to exist to train health professionals to provide these services. The literature, however, does not appear to address the implications of reimbursement for training. Acknowledging the importance of this topic, the Agency for Healthcare Research and Quality and the Family Violence Prevention Fund sponsored a meeting in September 2001 of experts on various aspects of either intimate partner violence or coding and reimbursement issues to discuss existing systems, practices, and research. The group specifically addressed variation in reimbursement levels from system to system (e.g., Medicare, Medicaid, and private sector), financial incentives or disincentives associated with the current coding systems, and the implications of coding practices for patients and health care service delivery.6 Further examination of the role third-party reimbursement plays in health professional training about family violence is needed and may result from this meeting.
LAWS MANDATING REPORTING AND EDUCATION
Mandatory reporting and mandated education laws have been conceived as possible means for ensuring that health professionals receive training in family violence. Legislatures may enact such laws, usually with the intention of improving the service system. The committee struggled with the relationship of these laws to the training of health professionals. Little evidence indicates the effect these laws have on health professional education, and the legislation has created much controversy among those who work in family violence. Numerous interpretations of what the laws actually require and how they differ around the country exist, but few comprehensive resources on these laws are available. In the committee’s judgment, mandated reporting laws appear to drive the fields of child protection and elder protection and serve as a backdrop. And, in some states, they serve as a driver in intimate partner protection. Because they do appear to influence (and possibly distort) the content of education and ultimately of practice, the committee considered it important to examine these laws in detail to determine what is known about their actual impact. We sought to understand where such provisions are present, what they contain, and whether they achieve the intended effects. Having done the difficult work of collecting and examining all of the existing laws, the committee offers the details it has complied in the report appendixes and provides here the following descriptive analysis to assist others addressing the issue. The tables in Appendixes C and D describe state laws mandating reporting of and training about child abuse and
neglect, intimate partner violence, and elder maltreatment by health professionals as of August 2000.
In addition to the reporting mandates identified, several states encourage voluntary reporting or provide immunity for those who choose to report. Beyond the educational mandates identified, several states have enacted laws to encourage agencies to provide training to interested health professionals, to fund optional training programs, and to encourage licensing boards to consider educational mandates. Although such laws may serve an important policy objective, they were not included in the appendixes because they do not require individual health professionals to report or obtain training. Finally, a handful of states limit reporting mandates to institutionalized victims, and a few others mandate training solely for health professionals who serve as public employees. Although these are interesting alternatives to comprehensive mandates, these laws were not included because they apply to a relatively small subset of health professionals and victims.
Mandatory Reporting Laws
Requirements
Child Abuse and Neglect. All 50 states and the District of Columbia require health professionals to report child abuse and neglect. Virtually every state requires a report when a health professional either “knows” about abuse or has “reasonable grounds to suspect” or “reasonable grounds to believe” abuse has occurred. The states vary, however, on the question of whether health professionals must report behavior that they believe will result in a child’s suffering abuse in the future, in addition to abuse that has already been perpetrated.
Health professionals are most often required to report directly to a local child protective services agency. Approximately one-half of the states give mandatory reporters the option of reporting to a law enforcement agency. The states vary as to whether reports must be oral, in writing, or both.
In every state, the reporting requirement applies to physicians, dentists, mental health professionals, nurses, social workers, and allied health professionals (except in Washington, where allied health professionals are exempt). Every state also requires reporting by some subset of allied health professionals, but this term is defined differently across jurisdictions and may include paramedics, emergency medical technicians, physical therapists, dental hygienists, chiropractors, “practitioners of the healing arts,” or “persons having responsibility for care or treatment of children.”
Intimate Partner Violence. Several states require health professionals to report injuries caused through the commission of a crime or the discharge of a
firearm. Such injuries inevitably include instances of intimate partner violence.7 In addition to these laws that address the issue indirectly, three states—California, Colorado, and Rhode Island—explicitly require the reporting of intimate partner abuse, and one—Kentucky—requires the reporting of abuse, neglect, or exploitation of any adult
California and Colorado require that reports be made to law enforcement agencies. Kentucky and Rhode Island, in contrast, require reporting solely for the purpose of documenting the incidence of family violence. As a result, it requires health professionals to report to monitoring agencies, rather than to law enforcement.
The typical legal standard that triggers these reporting requirements is “reasonable cause to suspect” or “reasonable cause to believe.” Kentucky requires physicians, dentists, mental health professionals, nurses, social workers, and some allied health workers to report intimate partner violence. California and Rhode Island do not apply this requirement to mental health professionals or social workers. Colorado requires only physicians to report intimate partner violence.
Elder Maltreatment. In all, 43 states and the District of Columbia mandate the reporting of elder maltreatment by health professionals. (The exceptions are: Colorado, New Jersey, New York, North Dakota, Pennsylvania, South Dakota, and Wisconsin.) These states vary in terms of the types of injury that must be reported. Most states require reporting of “abuse, neglect, or exploitation.” Others also require reporting of “mistreatment” (Minnesota); the “need [for] protective services” (Delaware, District of Columbia., Kansas, North Carolina, Missouri, and Pennsylvania); “isolation” (Nevada); “abandonment” (Alaska, California, Connecticut, Rhode Island, and Wyoming); or “financial exploitation” (California, Illinois, and Washington).
Some states have built in special exceptions to their elder maltreatment reporting requirements. For example, a California health professional need not report evidence of elder abuse if he or she “reasonably believes” that abuse did not occur in his or her “best clinical judgment.”
The legal standard that triggers the reporting requirement also varies. In all, 39 states have adopted a “reasonable cause to believe” or “reasonable cause to suspect” standard. Other states dictate that a health professional “know,” “observe,” or “suspect” abuse before a report is required.
Just over half the states require reporting directly to the local department of health and human services or protective services agency. An additional 15 states also permit reporting to law enforcement officials. Two states—Alaska and
Florida—limit reporting to data collection purposes, by mandating that reports be made only to local agencies responsible for maintaining elder abuse registries.
Most of the states require physicians, dentists, mental health professionals, nurses, social workers, and allied health workers to report, with a few exceptions. In Alaska, California, Nebraska, and Oregon, dentists are not required to report; in Idaho, mental health professionals are not required to report.
Impact
Research on health professionals’ typical practice in cases of maltreatment and its divergence from optimal practice has focused in large part on clinicians’ decisions about whether to report suspected maltreatment to authorities (Melton et al., 1995; Kalichman and Brosig, 1993; Kalichman, 1999). It is not uncommon for health professionals to refrain from reporting suspected child maltreatment that they do not regard as serious or clear-cut (Finlayson and Koocher, 1991; Kalichman and Brosig, 1993; Kalichman and Craig, 1991; Kalichman et al., 1988, 1989; Watson and Levine, 1989; Zellman, 1990a). Studies on elder abuse indicate that some health professionals do not report due to questions about the usefulness of reporting (i.e., repeated reports about the same patient do not appear to improve the situation; Clarke-Daniels et al., 1989, 1990) and beliefs that community resources are insufficient for appropriate responses (Jones et al., 1997). The tendency to ignore or bypass reporting mandates appears to be most prevalent among mental health professionals (Kalichman et al., 1988).
Although requirements for reporting suspected maltreatment are commonly recognized by health care professionals (Zellman, 1990a), many express concerns that reporting can be as harmful as helpful. Potential advantages of mandatory reporting, particularly for intimate partner violence, that have been cited include improvement of the health care response to family violence, aid in victim referral, and assistance with perpetrator prosecution (Rodriguez et al., 1999; Tilden et al., 1994). Concerns include beliefs that mandatory reporting may (1) breach confidentiality and so undermine autonomy, trust, and privacy in the health care setting (Kalichman and Craig, 1991; Kalichman et al., 1989; NRC and IOM, 1998; Rodriguez et al., 1998, 1999; Vulliamy and Sullivan, 2000; Warshaw and Ganley, 1998); (2) interfere with efforts to enhance patient safety (Levine and Doueck, 1995; NRC and IOM, 1998; Rodriguez et al., 1998, 1999; Tilden et al., 1994; Warshaw and Ganley, 1998; Zellman, 1990b); (3) serve as a deterrent to perpetrators obtaining treatment (Berlin et al., 1991; Kalichman et al., 1994); (4) precipitate violent retaliation by perpetrators against victims or health care professionals (Gerbert et al., 1999; Rodriguez et al., 1999); (5) decrease the utilization of health care services by abuse victims (Gerbert et al., 1999; Rodriguez et al., 1999); and (6) discourage inquiries by health care professionals who believe that if they do not ask, they have nothing to report (Gerbert et al., 1999).
Victims of family violence also express concerns about mandatory reporting. In studies of intimate partner violence (Gielen et al., 2001; Rodriguez et al., 2001a; Sachs et al., in press), a majority of participants supported reporting by health care professionals (73 to 91 percent) with the victim’s consent. However, significantly more battered than nonbattered women favored nonmandatory options that would give decision-making authority to abused women (Gielen et al., 2001; Rodriguez et al., 2001a; Sachs et al., in press). Furthermore, one study found that women who had been abused within the past year were more likely to oppose mandatory reporting than women who had been abused more than one year ago (Rodriguez et al., 2001b). Battered women cited considerable concern about increased risk (44-54 percent) and resentment about loss of control (45-61 percent), and the majority (68-77 percent) believed that women would be less likely to tell their health care provider about abuse if disclosure would result in a mandatory report (Gielen et al., 2001; Sachs et al., in press).
Research on issues related to mandatory reporting requirements appears to focus on investigation and forensic assessment rather than the provision of therapeutic and preventive services8 (Melton, 1994; Melton et al., 1995, 1997; NRC, 1993; U.S. Advisory Board on Child Abuse and Neglect, 1993).9 Few studies indicate what happens over time once reports are made (Melton et al., 1995) or how effective health professional involvement is.
The relationship between mandatory reporting requirements and education is unclear, although it appears in some instances that training focuses on the legal reporting requirements, particularly in curricula on child abuse and neglect. Based on its review of existing health professional curricula, the committee concludes that mandatory reporting requirements may be both beneficial and detrimental to education. Reporting requirements appear to succeed in providing a place within health professional curricula for the issue of family violence and increasing attention to health professionals’ responsibility for identifying and reporting it. However, existing curricula may focus on required reporting procedures to the exclusion of health professionals’ roles in treating, referring, and preventing family violence. Research on the implications of mandatory reporting requirements for health professional education and practice is needed.
Mandatory Education Laws
Requirements
Child Abuse and Neglect. Only three states—California, Iowa, and New York—mandate education on child abuse for health professionals. The training requirements appear to be driven at least in part by mandatory reporting laws; in all three states, training must focus on child abuse identification and the local statutory reporting requirements. The amount of required training varies. New York requires a one-time, 2-hour training session. California has a one-time training requirement of 7 hours over the course of a professional’s career; Iowa goes further and requires at least 2 hours every 5 years.
Iowa requires physicians, dentists, mental health workers, nurses, and social workers to receive this form of education; New York does the same with the exception of social workers. California imposes this requirement only on its mental health professionals and social workers.
Intimate Partner Violence. Three states—Alaska, Florida, and Kentucky— mandate that health professionals receive education about intimate partner violence. The states require training on such topics as the nature and extent of such violence, safety planning, lethality and risk issues, and available community resources.
The amount of training required varies greatly: Florida mandates 1 hour every 2 years; Kentucky requires a one-time-only 3-hour training session; and Alaska does not specify. Florida and Kentucky require training for doctors, dentists, mental health workers, nurses, social workers, and allied health workers. Alaska does the same, except for allied health workers.
Elder Maltreatment. Iowa is the only state that requires its health professionals to receive training on elder maltreatment. Its law mandates education regarding identification and reporting dependent elder abuse, with a 2-hour initial session followed by two additional hours every 5 years. The education requirement applies to doctors, dentists, mental health professionals, nurses, social workers, and allied health workers.
Impact
The committee could find no formal evaluations of the impact of legally mandated family violence education. Studies demonstrate that health professionals who have obtained any continuing education (not necessarily mandated) about child maltreatment are no more likely—and in some samples are less likely—to report child abuse and neglect than are those who have not attended such workshops (Beck and Ogloff, 1995; Kalichman and Brosig, 1993; Reiniger et al., 1995). Accordingly, although one can hypothesize that such laws may have an array of positive as well as negative effects, until sound process and outcome
evaluation data are acquired, in the committee’s view these mandates are driven by assumptions and good intentions, rather than by a sound evidence base. What is known about continuing education for health professionals (summarized in Chapter 6) is that didactic instruction may result in increases in knowledge or changes in attitudes, but there is limited evidence that it influences practice behaviors. Therefore, there is no reason to believe that 1- to 3-hour instructional programs, the form that many of the mandates take, will result in lasting positive effects on screening or intervention in family violence. Critical evaluation questions for any educational program, particularly for those that are required by state statute or agency mandate, include: whether knowledge improvements can be demonstrated, whether any knowledge improvements are sustained over time, whether attitudes about family violence are affected, whether any attitudinal changes are sustained over time, whether and to what extent clinicians’ practice behavior changes, and whether any such behavioral changes are sustained over time. Furthermore, questions are needed to assess the adequacy of the program, from the provider perspective, including measures of acceptance and satisfaction with the program and suggestions for improvement. Whether costs of care, severity of presentation, case mix, morbidity, and ultimately mortality are affected by mandatory training must be determined. Finally, it is necessary to question if any changes observed can be attributed to the education program itself.
RESOURCE ISSUES
Funding
Education development, implementation, maintenance, and evaluation require funding; however, federal funds for such activities appear to be meager, and state governments have actually decreased such funding (Reiser, 1995). Private investor funds appear be decreasing as well. Private investors tend to concentrate capital in areas that can demonstrate promising financial returns or, at the very least, clear savings to teaching institutions or society. Education and training programs often cannot produce such concrete results, especially in the short term, and therefore are at a serious and chronic disadvantage in terms of securing sufficient funding to develop and evaluate educational interventions (Mechanic, 1998; Blumenthal and Meyer, 1996).
Federal funding10 may be provided through agencies such as the Health Resources and Services Administration of the Department of Health and Hu-
TABLE 4.1 Selected Recent Federal Research Grant Opportunities
Agency | Title | Grant No. (Date) | Funding Allocation |
Agency for Healthcare Research and Quality | Violence Against Women: Evaluating Health Care Interventions | RFA:HS-00-006 (FEB 2000) | $1 million FY2000 |
Centers for Disease Control and Prevention | Extramural Injury Research Grants for the Prevention of Intimate Partner Violence and Sexual Assault | PA: 00042 | $1.2 million FY2000 |
Office of Community Services, Administration for Children and Families | Family Violence Prevention and Services Program | FA OCS-2000-06 (FEB 2000) | Varies (four priority areas) |
Children’s Bureau, Administration on Children, Youth, and Families | Administration for Children and Families: Child Abuse and Neglect (2000B) | CB-2001-01 (FEB 2000) | $3.5 million FY 2000 |
man Services when specific health professional training needs are identified.11 Funds are provided for general health care professional training through the Public Health Services Act, but the act does not require training in family violence. In 1998, however, language was added that encourages grantees to “prepare practitioners” (physicians) or “provide care” (nurses) to “underserved populations and other high risk groups such as the elderly, individuals with HIV-AIDS, substance abusers, homeless, and victims of domestic violence [emphasis added].”
Federal agencies do occasionally fund family violence-related research in health care (see Table 4.1). However, for the most part these calls for proposals do not specify health professional training in family violence.
A review of individual federally funded projects indicates that few involve the training of health professionals in family violence research. The National Institute of Mental Health currently funds five pre- or postdoctoral research training grants related to family violence (see Table 4.2). General violence training grants (such as those from the National Consortium on Violence Research) may also include fellowships addressing family violence.
Family violence rarely emerges in a review of funding priorities among the
TABLE 4.2 Family Violence Training Grants
various institutes at the National Institutes of Health (NIH) (A.A. Perachio, personal communication, March 27, 2001). Among the seven research priorities of the National Institute of Nursing Research for 2001, for example, none specifically applies to developing new knowledge for nurses in the area of family violence (or to any other violence category). Although the National Institute on Aging included elder abuse and neglect as a Selected Future Research Direction, that topic is not named in the list of Areas of Special Emphasis (biology of brain disorders, new approaches to pathogenesis, new preventive strategies against disease, new avenues for the development of therapeutics, genetic medicine, and health disparities).
Other federal sources of training funds include projects set up in response to routine funding cycles (in which investigators submit proposals in their area of competency) and projects in direct response to requests for proposals (RFPs) or program announcements (PAs), the government’s mechanism to encourage research in priority areas. A search of the NIH Health Information Index for family
violence research by NIH or NIH-supported scientists revealed no entries for “family violence,” “spouse abuse,” “domestic violence,” or “child abuse.” The only family violence entry was for “elder abuse,” accompanied by a link to the National Institute on Aging. The Computer Retrieval of Information on Scientific Projects (CRISP) database revealed 93 projects including the phrase “child abuse,” 63 including “spouse abuse” (38 for “domestic violence”), and 4 for “elder abuse” currently (1999-2000) funded by several federal agencies (the National Institutes of Health, the Substance Abuse and Mental Health Administration, the Health Resources and Services Administration, the Food and Drug Administration, the Centers for Disease Control and Prevention, the Agency for Healthcare Research and Quality, and the Office of Assistant Secretary of Health). Some projects are listed twice (due to multiyear funding across the reporting year) and some projects only mention, rather than focus on, family violence. In other cases, currently funded projects are not included in the database. Funding amounts for these projects are not disclosed.
The allocation of federal funds for child abuse and neglect has been primarily in response to federal legislation, the Child Abuse Prevention and Treatment Act of 1974 (CAPTA—P.L. 93-247), which was reauthorized in 1996. As mentioned earlier, CAPTA established the National Center on Child Abuse and Neglect (NCCAN), defined child abuse and neglect, and supported other demonstration programs and projects to prevent, identify, and treat child abuse and neglect. In addition to allocating funds directly, CAPTA authorizes aid to states for child abuse and neglect programs. The program authorizes funds through 2001 and $99.3 million has been requested for 2001. These funds finance four broad programs, none of which explicitly include training: child abuse state grants, child abuse discretionary grants, community-based family resource and support grants, and an adoption opportunities program. The discretionary grants may include training. NCCAN did do a one-time funding of multidisciplinary training programs, a few of which remain (e.g., the Center on Child Abuse and Neglect, University of Oklahoma Health Sciences Center). NCCAN was reorganized as the Office of Child Abuse and Neglect (OCAN) in 1996 with 80 percent fewer staff. Among other activities, OCAN published the “Child Abuse and Neglect State Statutes Series” (NCCAN, 1997) to provide some information for health care providers about reporting mandates for child abuse and neglect. OCAN does not actively disseminate the information to health care providers or evaluate the impact of the information provided. State Victim Compensation and Assistance and Victim Assistance and Law Enforcement funds, allocated through the U.S. Department of Justice, have sometimes been used for the continued training of professionals in evaluating criminal forms of maltreatment, but the focus is not on health professionals.
Funding for health professional training for child abuse and neglect appears to be decreasing in proportion to the growth of the problem (Theodore and Runyan, 1999). For example, between 1980 and 1986, while the reported inci-
dence of child abuse and neglect increased by 74 percent, the federal research budget for this topic increased only 2 percent (Kessler and New 1989), and between 1981 and 1995, while reported incidence increased by 150 percent, research funds decreased by 44 percent (Thompson and Wilcox 1995). Few efforts support training researchers and professionals (Jenny, 1997). For example, in 1996, the federal government spent $29.9 million or $28.47 per case on child abuse (Putnam, 1998, 2001) while spending $2.26 billion or $1,734.61 per case on cancer, despite the higher incidence of child abuse (NCI, 1996). In terms of research expenditure per lost life, violence accounted for $31, cancer for $794, heart and lung disease for $441, and AIDS for $697 (NRC, 1993).
Much of the funding for initiatives related to intimate partner violence is provided under the Violence Against Women Act (VAWA) of the Violent Crime Control and Law Enforcement Act (P.L. 102-322) of 1994. The goals of the legislation include preventing violence against women, increasing penalties for batterers, and supporting programs to prosecute offenders and assist women victims of violence. It is administered by the Department of Health and Human Services and the Department of Justice, and in fiscal year 2000, $223.6 million was appropriated to the Department of Health and Human Services for VAWA programs. The VAWA reauthorization bill, passed in October 2000, requested an increase to $660 million each year for the next 5 years. Services to victims account for the majority of the funds, and none is earmarked for health care professional training. The act does acknowledge (and dictate) funds for training for persons in the judicial and law enforcement domains.
The Older Americans Act (OAA) and the Social Security Act provide services for elders, including nutritional and caregiver services, and, to a limited extent, for abuse prevention. Pursuant to the OAA, the Department of Health and Human Services created the National Center on Elder Abuse in 1993 to help promote understanding among state and local networks of community workers, physicians, elderly volunteers, and others working to prevent elder abuse; it was reorganized in 1998. The center involves a consortium of six partners led by the National Association of State Units on Aging and was funded at $400,000 in 1998-1999, a similar amount for 1999-2000, and $800,000 for 2000-2001, under HHS grant no. 90-AP-2144. One purpose of the center is to facilitate training on elder abuse recognition and services through educational materials and technical assistance. Title IV-E of the Social Security Act also provides for training in the area of elder welfare. That training can include activities to educate health professionals collaborating with workers in social services. Table 4.3 summarizes the federal legislation authorizing funding for initiatives related to family violence.
Two National Research Council reports (1993, p. 318; 1996, pp. 152-155) have recommended that centers be funded to address family violence research needs, specifically that each of three centers be funded at $1 million. In actuality, a single center was funded by the Centers for Disease Control and Prevention,
TABLE 4.3 Family Violence Federal Funding Acts
Type of Violence | Legislation Authorizing Funding for Initiatives on Family Violence | Provision of Funding | Years | Funding |
Intimate partner violence | Violence Against Women Act | DHHS DOJ-OJP | (1994-2000) 2000 | 435.75 million |
Child abuse and neglect | Child Abuse Prevention and Treatment Act; Social Security Act | Child Protective Services |
|
|
Elder maltreatment | Older Americans Act (Titles III and VII) | Social Services Block Grant | FY2000 (for all sx)a | $1.5 bil |
Social Security Act (Title XX) | Adult Protective Services | |||
Family violence | Family Violence Prevention and Services Act |
| (1984) 1984 | 0 |
Victims of Crime Act | ||||
aThrough appropriation laws. | ||||
the National Violence Against Women Prevention Research Center. That center award, a consortium of the Medical University of South Carolina, the University of Missouri at St. Louis, and Wellesley College, was funded at approximately $500,000.
Federal funds for health professional training are closely linked to the priorities that are named by institutions such as HHS. However, earmarking of federal funds for health professional training in family violence is dependent on political considerations, not just on evidence that such training will make a difference. Moss recently stated, “It may be closer to the reality to say that politics is the basic science of public health,” rather than epidemiology (Moss, 2000). Documents such as Healthy People 2000 (and Healthy People 2010) and federal agency strategic plans set the health agenda for the nation in writing, reflecting, at least in part, the political priorities of the nation.12 Even with such priorities,
the allocation of funds is another political process and is competitive within and across health care issues.
Overall, the information reviewed in this section suggests that funding for family violence is limited and inconsistent and that funds for health professional education research or training development on family violence specifically are even sparser. Until funds are proportionate to the known extent of the problem in society and in health care, progress in the area of health professional training on family violence is likely to be limited. Some potential for additional funding lies in the link between NIH’s mission and the achievement of Healthy People 2000 (and Healthy People 2010) objectives in which family violence has been identified as a national priority. The objectives related to family violence have yet to be achieved.
Human Resources
Although adequate and sustained financial resources are necessary to support curricular innovation, it is people who drive program development, staff classrooms and clinical practica, work to enhance training programs, and establish the systems needed to sustain education. Institutions are constrained financially by available funds, but they may have more control over the human resources involved. The nation is experiencing a shortage of faculty who are qualified and willing to teach in the health professions (Griner and Danoff, 1995). Furthermore, there are few researchers or educators nationwide who are recognized as scholars in family violence, and few programs appear to exist to prepare researchers or educators to achieve scholarship in this area. Health professional training programs, whether in undergraduate schools, graduate training programs, or continuing education, are in need of experienced, dedicated, sensitive, versatile, and experienced clinician-educators who can effectively teach this material (Alpert, 1995). Given the paucity of experts-educators in the field, it is also difficult to recruit and train educators, monitor their performance, and help them become more effective (Kassirer, 1995; Greenberg, 1995; Lesky and Hershman, 1995). Furthermore, developing the human resources necessary may not be achieved among health professionals at the teaching rates and hours currently evidenced in the literature (Alpert et al., 1998; Woodtli and Breslin, 1996). The problem becomes circular: research and training deficits yield few well-prepared educators, and an inadequate supply of educators and researchers results in inadequate training and research.
The committee could find little evidence of the educational infrastructure that is needed to teach about family violence. One study indicates that organized institutional response is not common (Cohen et al., 1997). Teaching about family violence could be enhanced by having an available cadre of survivors, standardized or simulated patients trained to portray actual patients accurately, library and computer resources, and community-based advocates and other direct service providers. Hu-
man, computational, and logistical infrastructure support for the evaluation of educational programs also appears to be unavailable in most institutions. The APA Working Group on Implications for Education and Training of Child Abuse and Neglect, for example, noted that “a lack of time and resources for teachers to develop curricula appropriate for the educational level of their students” and a “lack of readily available material to use in conjunction with child abuse and neglect curricula (e.g., textbooks and videotapes)” are impediments to curricular reform to reduce the gap between psychologists’ modal and optimal levels of expertise in responding to child maltreatment (Haugaard et al., 1995, p. 79). An array of resource materials is available, including slide sets, handouts, videos, articles, book collections, and the like, but the extent to which these are distributed and in use is unknown. Attention to developing a research and training infrastructure in other health areas (e.g., muscular dystrophy, alcoholism) appears to have resulted in the growth of targeted funding and of a critical mass of faculty to ensure that the work will go on and the care for patients will improve (see, e.g., http://cysticfibrosis.com/centers.htm; http://www.mdausa.org/clinics/alsserv.html; http://www.niaaa.nih.gov/extramural/ResCtrs1198.htm).
CONCLUSIONS
The committee’s assessment of the potential influences on health professional training on family violence suggests the following conclusions:
Institutional culture, norms, and priorities can influence the education offered, and they may also create challenges for developing, implementing, or sustaining family violence training for health.
Common pathways for these challenges appear to include inadequate financial and human resources and institutional commitment to the problem at the national and local levels.
Accreditation, licensure, and certification requirements do not consistently and explicitly address family violence and thus do not appear to be a significant influence on family violence training for health professionals.
Individual health professional concerns, beliefs, and experiences can create challenges to educating health professionals about family violence.
Notable individual concerns include perceptions of inadequate time or preparation, personal values, and personal experience with victimization and traumatization.
A review of health professional organization statements, guidelines, positions, and policies reveals that the degree to which the various professions call for training differs greatly not only by profession but also by specialties within those professions.
Health professional organizations can influence the existence and extent of family violence education within a profession.
The American College of Obstetricians and Gynecologists, the American Academy of Pediatrics, and the American College of Nurse Midwives are excellent examples of health professional organizations actively working to encourage and implement education initiatives on family violence among members of their professions.
Stakeholder groups, including advocates, victims, and payers, have been or are becoming active in family violence issues, including education, but their impact on family violence education for health professionals is difficult to assess.
No studies indicate the impact these efforts have had. However, curricula developed by organizations such as the Family Violence Prevention Fund appear to have been widely disseminated and in use by health professional educators.
The impact of mandatory reporting laws on family violence for health professionals is unclear, but the existence of such laws suggests a need for educational content about them.
Based on the expressed concerns and research on rates of reporting, the committee sees a need for clear explanations of reporting laws for students and practitioners, as well as the provision of opportunities to discuss and resolve ethical issues that reporting raises for many health care providers. Additional studies are needed to determine whether reporting requirements are the appropriate mechanism for achieving the goals of increasing reporting rates and ensuring the necessary services for victims. Regardless of the existence of legal requirements, in the committee’s view, students must learn to identify, report, and refer cases according to legal requirements, professional practice standards, and patient care goals. In addition, the training needs of health professionals extend beyond fulfilling legal requirements. The committee understands the intent underlying reporting requirements for health professionals generally to be the enhancement of their responses to family violence and ensuring that victims receive needed treatment and services. These goals suggest that health professionals need to know more than just how to report suspected and actual cases of family violence. Given the concerns about mandatory reporting cited by both health professionals and vic-
tims, it may be productive to orient training programs more toward planning and delivery of broad-based prevention and treatment services, rather than exclusively on case identification and forensic services.
The effect of mandated education requirements on health professional education is unknown.
Funding for training programs in family violence education in the health professions does not appear to be a priority and does not appear to be consistently available. Information about funding is fragmented.
The extensive effort required even to identify funding sources is noteworthy. The information must be collected piecemeal from numerous web sites for federal agencies and private foundations, rendering it difficult to determine if and when funds are available.






































