The Future of Health Services Research: Advancing Health Systems Research and Practice in the United States (2018)
Chapter: 2 Health Services Research Ecosystem
2
HEALTH SERVICES RESEARCH ECOSYSTEM
Health services is continuously evolving, in concept and practice. In 1979, a National Academy of Medicine (then Institute of Medicine [IOM]) committee defined health services research as “inquiry to produce knowledge about the structure, processes, or effects of personal health services” (IOM, 1979). Since then, as noted in chapter 1, the purview of health services research has substantially broadened, and AcademyHealth, the professional organization devoted specifically to engaging health services researchers, now draws on a description defining health services research as “the multidisciplinary field of scientific investigation that studies how social factors, financing systems, organizational structures and processes, health technologies, and personal behaviors affect access to health care, the quality and cost of health care, and ultimately our health and well-being.” (Lohr and Steinwachs, 2002). In other words, understanding the systemic factors in play, and how they impact health and health care throughout institutional and uniquely personal forces, has substantially broadened the necessary analytic terrain. At several points during the workshop, presenters and participants discussed the concepts, history, development, and funding of health services research since its origins. Elements of those discussions are combined and summarized here, along with a broad overview of the related interests and activities of federal agencies and other funders that support health services research, and observations on how those funding agencies interact with one another.
HISTORY AND FUNDING OF THE FIELD
Health services research began to emerge as a formal and distinct field in the 1960s as investments in personal health services began to expand, leading President Johnson to propose legislation to establish the National Center for Health Services Research and Development in 1967, noting that attainment of national health care objectives and efficient management of the federal government’s disparate research activities required a coordinated effort. When questions arose about
the relevance of health services research to the needs of decision makers, the White House Office of Science and Technology Policy commissioned an IOM study published in 1979 that called for greater coordination across the federal government and for a greater proportion of funding to go to investigator-initiated extramural research (IOM, 1979).
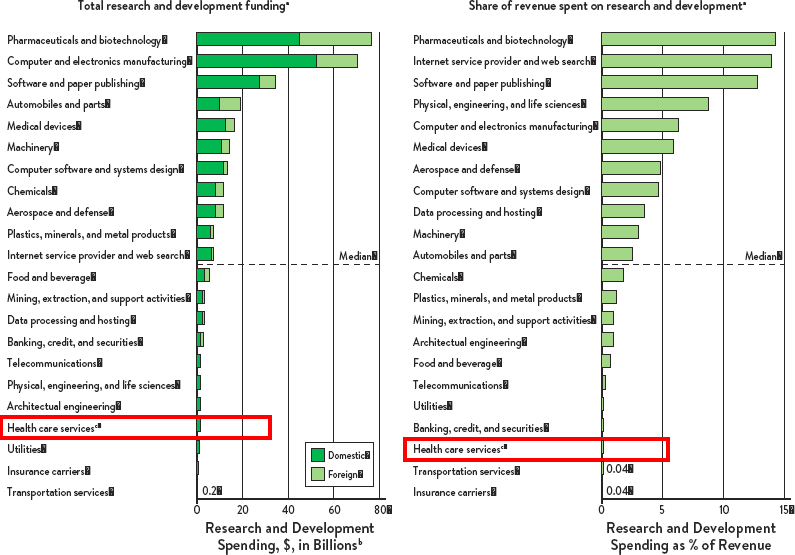
SOURCE: Moses et al. 2015
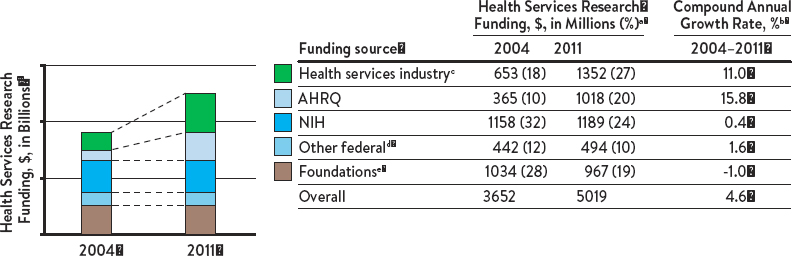
SOURCE: Simpson, 2018
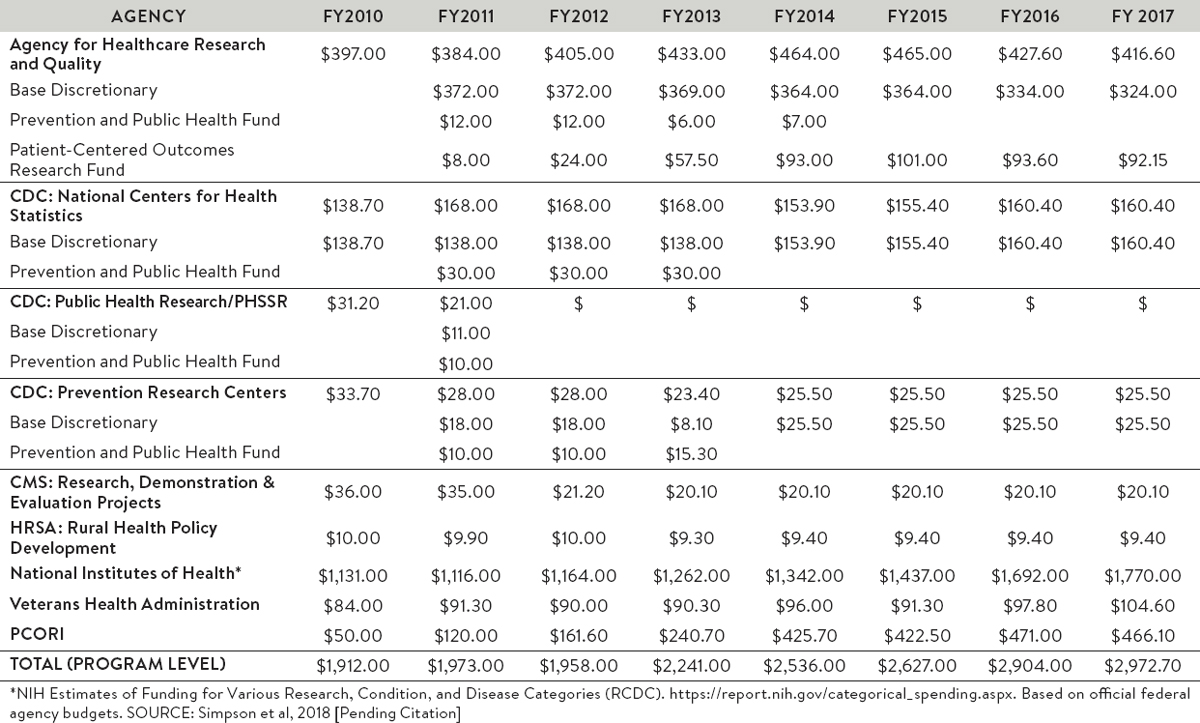
SOURCE: Simpson, 2018
Lisa Simpson, president and chief executive officer of AcademyHealth, noted that although funding for health services research has grown, it remains a very small percentage of total spending on health care (0.3 percent) (Figure 2-1). The total funding for health services research, as calculated by Moses et al. (2015), increased from 2004 to 2011 (the last date covered in the analysis) and, in that year, exceeded $5 billion (Figure 2-2), with a boost in 2011 because of federal funds being spent to recover from the recession under the American Recovery and Reinvestment Act.
A number of federal agencies, each with its own goals, fund health services research. Together, this funding amounted to about $2.5 billion in Fiscal Year 2017, with approximately two-thirds of that from the NIH (Figure 2-3). As a result of this funding distribution, NIH-funded research, with its particular emphasis on investigator-initiated academic research, provides incentives that heavily influence health services research. Simpson also pointed out that the
Department of Defense (DOD) is not included in this total because of the difficulty of separating out its funding, but DOD funds health services research and, Simpson stated, is “interested in doing more.”
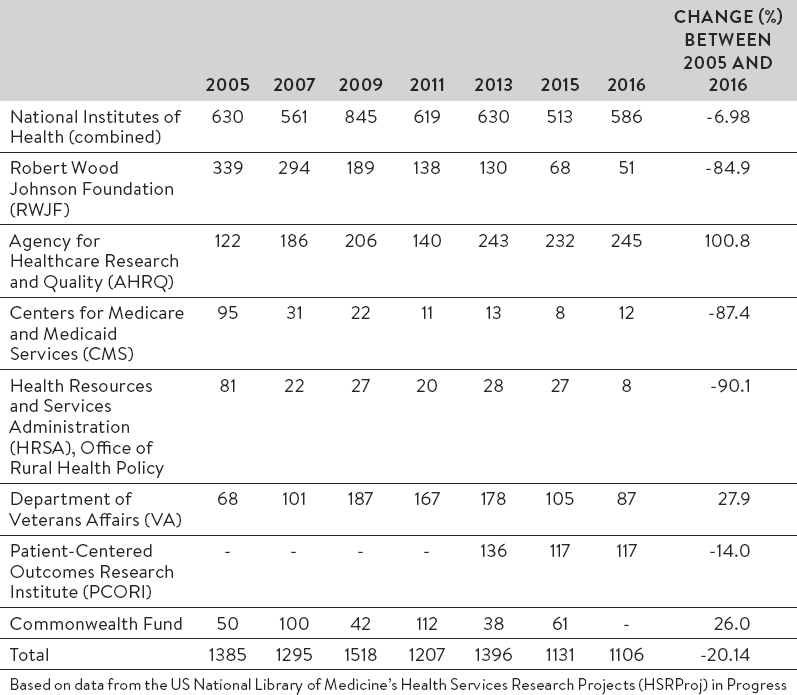
Simpson also reported specifically on funding for AHRQ, which was established in 1989 as the Agency for Health Care Policy and Research and acquired its current name during a 1999 reauthorization. AHRQ funding has increased from approximately $173 million in 1999 to $381 million in 2012, according to an analysis of an appropriations conference report by the Association of American Medical Colleges. This represented 0.68 percent of total Public Health Service funding in 1999 and 0.83 percent of the total in 2012. However, Simpson also noted that AHRQ has not been reauthorized and the president’s recent budget submission proposed reorganizing the agency into a National Institute for Research on Safety and Quality as part of the NIH. Another element of uncertainty for the field is the decline in the number of projects supported by top funders, which dropped overall from 2005 to 2016 (Figure 2-4). Though some projects have become bigger, the overall numbers reveal a significant reduction in the number of projects in health services research which are funded.
PHILANTHROPIC LEADERSHIP
Many private foundations support health services research, including organizations such as the Robert Wood Johnson Foundation (RWJF), the Peterson Center on Healthcare, the Commonwealth Fund, the California Healthcare Foundation, and the Blue Shield of California Foundation, among many others. Richard Besser, president and chief executive officer of RWJF, commented on the role of foundations in supporting health services research. RWJF “has spent four decades helping to develop a generation of exceptional [health services] researchers who are dedicated to putting evidence to work in the rocky terrain of the real world,” said Besser. “We have supported research and leadership development programs that take a multidisciplinary approach to the way care is organized, financed, delivered, and consumed.” Most recently, a new set of research programs explore how other sectors such as education, criminal justice, housing, transportation, and agriculture influence health outcomes.
Besser highlighted several examples of research supported by RWJF that aim to improve the delivery, quality, cost, and coordination of health care. Recent research in Kentucky on Medicaid work requirements found that about 357,000 recipients who are currently not working could be affected by proposed policy changes. Nearly half of these people are more than 50 years old, a quarter do not
have a high school education, and three-quarters have a serious health limitation or no car or Internet access. This is “the kind of rapid turnaround health services research that is critically needed to help inform the policy debate,” he said. “It doesn’t mean that the policy debate will go in the direction that those of us in health would like it to go. But at least it can be informed with facts.” Another example is health services research involving implementation and evaluation of the first locally designed and financed public health program for the Cheyenne River Sioux tribe in South Dakota. The research is using a community-based participatory research approach to elicit tribal preferences in designing and implementing the program. It is also examining the relationship that develops between state and federal agencies in meeting the tribe’s needs. “We are hopeful that this kind of work will help inform the design of other health programs built to answer the wants and needs of specific communities.”
Besser also underscored the importance for public and private cooperation and collaboration in building the evidence base to improve health and health care. The section below highlights the important roles of major federal agencies using and supporting the field.
AGENCY FOR HEALTHCARE RESEARCH AND QUALITY (AHRQ)
AHRQ’s role is to focus on the health care system as a whole, said the agency’s director, Gopal Khanna. It funds research and works with doctors, nurses, health systems, and others to foster the provision of safe, high-quality health care for all Americans. It tracks progress and gets information to those who need it quickly by synthesizing diffuse data points and turning them into usable information, thereby translating and operationalizing knowledge for end users. This means working with primary care providers, hospitals, and nursing homes to help them understand what works best and to operationalize innovations.
Though AHRQ is smaller than many other federal agencies, it collaborates with a variety of partners to leverage its capacities. It works with the Centers for Medicare and Medicaid Services (CMS) to support the Hospital Improvement Innovation Network and the Community-based Care Transitions Program.1 It works with the Patient-Centered Outcomes Research Institute (PCORI) to disseminate and implement patient-centered outcomes research. It works with the Centers for Disease Control and Prevention (CDC) to combat health
___________________
1 More information about the Hospital Improvement Innovation Network and the Community-based Care Transitions Program is available at https://partnershipforpatients.cms.gov/about-the-partnership/hospital-engagement-networks/thehospitalengagementnetworks.html and https://innovation.cms.gov/initiatives/CCTP, respectively.
care-associated infections, and it does synthesis work with a variety of partners. “I’m eager to sustain and expand on these collaborative partnerships,” Khanna said.
AHRQ’s work falls into three categories: research and evidence, tools and training, and data and measures. It also has three priority areas that capture its goals: patient safety, practice, and data and insight. In the area of patient safety, AHRQ is well known for its achievements in the areas of health care-associated infections. It is also working on medical errors, antibiotic resistance, and diagnostic safety. In the area of practice, AHRQ is investing in implementation research and developing tools and resources that clinicians can use at the point of care. For example, its EvidenceNOW program is working with 1,500 small and medium-sized primary care practices to accelerate the use of evidence to improve heart health.2 In the area of data and insight, AHRQ has developed data resources, such as the Healthcare Cost and Utilization Project (HCUP) and the Medical Expenditure Panel Survey (MEPS), to improve health care delivery.3 It also develops statistical briefs on such high-priority topics as opioid use and misuse, mental health services, and childhood obesity, and it uses predictive analytics to identify problems and develop innovations.
AHRQ has an impact beyond its size, said Khanna, but more resources would mean more opportunities to expand its data resources and leverage its expertise. Additional funding also would provide more opportunities to operationalize innovations to get research disseminated and implemented in everyday practice. “Successful project implementation requires time and money to support infrastructure, tools, and participation,” he said.
NATIONAL INSTITUTES OF HEALTH (NIH)
With 27 institutes and centers, NIH has a two-pronged mission, reported George Mensah, director of the Center for Translation Research and Implementation Science at the National Heart, Lung, and Blood Institute: 1) to advance basic science; and 2) to advance human health. The tag line for NIH is “turning discovery into health,” and, Mensah observed, “fundamental discoveries cannot be turned into health without a focus on health services research.”
NIH is the primary federal funder of basic, clinical, and translational medical research. As an essential component of this investment, NIH supports health services research to understand how to best translate research findings into
___________________
2 More information about EvidenceNOW is available at https://www.ahrq.gov/evidencenow/index.html.
3 More information about HCUP and MEPS is available at https://www.ahrq.gov/research/data/hcup/index.html and https://meps.ahrq.gov/mepsweb, respectively.
evidence that informs medical practice. NIH-supported health services research generally builds upon categorical (e.g., aging) or disease-specific (e.g., HIV/AIDS, cancer) research related to the missions of individual NIH Institutes and Centers, and includes investigator-initiated research as well as targeted research in response to specific funding opportunity announcements. Health services research projects supported by NIH focus on moving NIH-supported clinical and translational discoveries into routine clinical practice, ultimately improving health outcomes.
NIH Institutes and Centers support a broad portfolio of health services research projects, which aim to promote more effective and efficient means of prevention, screening, and treatment, and reduce health disparities by addressing the needs of all populations. The agency also funds the development and maintenance of infrastructure and resources to facilitate health services research, and to enable the dissemination and implementation of health services research findings. The NIH Health Systems Research Collaboratory is an example of a focused NIH-wide investment to develop infrastructure for health services research; specifically, to strengthen the national capacity to implement cost-effective, large-scale research studies that involve health care delivery organizations. As one measure of its commitment to health services research, the National Heart, Lung, and Blood Institute set up the Center for Translation Research and Implementation Science.4
NIH also coordinates with other federal agencies and organizations around synergistic research, training, and dissemination and implementation opportunities. With the CDC, it partners on surveillance to guide its early translation research. It has partnered with PCORI to improve the patient-centeredness of research in areas such as blood pressure control and stroke. NIH has also partnered with AHRQ on guidelines development that ties in with its educational mission.
PATIENT-CENTERED OUTCOMES RESEARCH INSTITUTE (PCORI)
“PCORI shares many priorities with AHRQ and NIH, but it comes at these priorities from a different direction,” said Joe Selby, PCORI’s executive director. The institute’s founding legislation directs it to address the questions of stakeholders, including patients, caregivers, clinicians, and payers and purchasers. It does mostly comparative effectiveness research (CER), and this research is primarily conducted through contracts rather than grants, underscoring PCORI’s applied
___________________
4 More information about the center is available at https://ncats.nih.gov/translation/spectrum.
mission and allowing the agency to work closely with its awardees. PCORI is also focused on real-world organizational challenges related to health care.
As with the other agencies described at the workshop, PCORI works collaboratively with a variety of partners, including CDC, the Food and Drug Administration (FDA), and Institutes and Centers of NIH. To date PCORI has worked with AHRQ to navigate its interest in supporting evidence synthesis, dissemination, and workforce training because these three areas have been ones in which AHRQ has historically made investments. This is also true for PCORI’s work to understand and assess prevention, diagnosis, and treatment options; to improve health care systems with a particular focus on making care more patient-centered; to eliminate disparities in health care delivery and outcomes; and to promote greater efficiency and transparency in research.
A particular challenge for PCORI is to focus its efforts on the right questions, said Selby. “We work extensively and over prolonged periods with stakeholders to try to get the research questions right.” It does less work on comparing new drugs and technologies because “comparative effectiveness research takes time,” Selby observed, and such research is difficult to do when products are evolving rapidly, highlighting the need to develop the infrastructure and culture of continuous learning throughout the care process. PCORI also faces the challenge of “who’s going to pay for a brand-new technology if insurers have not decided to cover it yet.” Finally, it is seeking to establish closer relationships with FDA and CMS to ensure that it can identify the important questions as early in the process as possible.
CENTERS FOR MEDICARE AND MEDICAID SERVICES (CMS)
The Centers for Medicare and Medicaid Services (CMS), the world’s largest health insurer, is also a heterogeneous agency with multiple authorities, explained Shari Ling, deputy chief medical officer in the Center for Clinical Standards and Quality at CMS. Its primary mission is not research, but it contributes a small portion of its budget toward evaluating programs and policies. In that respect, its mission coincides with that of health services research.
Central questions for CMS are what services and treatments should be covered, for which populations are they known to be effective as well as safe, and what quality expectations should be met by facilities that participate in Medicare. CMS is aided in its work by AHRQ-supported technology assessments and evidence reviews. Quality expectations can take the form of measures predicated on the evidence that is available, though in some cases evidence is insufficient. In other cases, the research needed to develop measures is insufficient.
CMS has an “incredible opportunity to be an implementation vehicle to help share and spread best practices,” said Ling. However, in its work with other entities, it needs to focus very clearly on outcomes that matter. “In general, it’s about how do we deliver and pay for care that is of high value.”
This observation leads to four challenges. The first is the need for evidence that is applicable to the Medicare population, which is complex and needs programs and policies tailored to its unique needs. The second is the need for data on meaningful outcomes, including not just administrative data but patient-reported outcomes data. The third is the need to see the big picture while running programs and implementing policies that have different origins and multiple goals. The fourth is the need to be mindful of the end users of the research, the programs, and the policies—clinicians at the point of care. According to Ling, CMS needs to ask clinicians, “What do you need that will make your job more effective and easier to translate this body of evidence into outcomes that matter for patients?”
DEPARTMENT OF VETERANS AFFAIRS (VA)
Carolyn Clancy, Deputy Under Secretary for Discovery and Advancement at the Veterans Health Administration, and David Atkins, director of the Health Services Research and Development (HSR&D) Service, both spoke about issues facing the Department of Veterans Affairs (VA).
Many changes have been occurring in the system, noted Atkins. Suicide and posttraumatic stress disorder are now among the VA’s top priorities, with more than 50 percent of its patient population having mental health conditions. The VA has been increasing the use of health information technology and telehealth to serve a veteran population that is increasingly rural. It has moved toward patient-centered medical homes, is delivering more care outside VA hospitals, has a long-standing interest in equity and access to care, and is always susceptible to changes caused by changing leadership or priorities. A related issue, Clancy noted, is that the overall nature of health care is changing, which will inevitably affect veterans’ health. “We don’t even know what a hospital is or is going to be,” she noted. Innovations such as micro-hospitals with six to eight beds and extensive digital support could transform the industry.
Building on these themes, Clancy commented that, in her current position, organizational issues are the “top 1-through-10 issues” that she deals with. High reliability can be a fairly abstract topic, but it is essential for the people in VA facilities. These facilities are also subject to hundreds of policies and directives. “It starts to feel a bit like the tyranny of performance measurement,” she said.
“We are great at articulating what ought to happen. It is far, far harder to figure out what is happening at any given day in a way that doesn’t produce, at least metaphorically, the equivalent of a bureaucrat following every single person around as they do their work.” Systems approaches that move beyond measuring single outcomes are one way out of this bind, she said.
In addition, genomics has become a major VA issue. More than 600,000 veterans are now enrolled in the Million Veteran Program, which is “phenomenal,” said Clancy.5 But the genomic information collected as part of the project is not clinically certified, which is one reason why clinicians are not sure how to use it.
The reliability and effectiveness of electronic health records is another issue. The electronic health record does not do anything to people directly, but it can create what she called “perfect storms” in which patient expectations are not met. These expectations also differ among age groups, with many older veterans happy to visit with their friends in waiting rooms, while millennials want an application that lets them know a doctor is running late for an appointment.
The HSR&D program has a dedicated budget of about $100 million and is connected to the integrated health care system of the VA, noted Atkins. It takes advantage of more than two decades of EHR experience and data within the VA, a large number of clinician-investigators, and an obvious audience for its research findings.
However, the research branch of the VA “cannot do it all by ourselves,” said Atkins, “so we rely on our other federal partners to share the burden.” In recent years, HSR&D has been working with clinical partners to develop research questions to ensure that the answers produced from research are useful to those organizations. In addition, VA research has a broad focus that is driven more by long-term issues than the needs of the moment, despite the fact that the system is often under the microscope and the timeline of policymakers is often not aligned with the timeline of research.
Atkins identified two major opportunities. The first is to work with other organizations on the big problems in health services research that answer fundamental questions. “Those are things that we probably can’t fund on our own,” he said. The second is to develop ways of sharing information from more limited studies that are useful in addressing broader questions. For example, VA has been developing evaluations of new programs as they are rolled out to answer more basic questions about the design of those programs.
___________________
5 More information about the program is available at https://www.research.va.gov/mvp.
INTERACTIONS AMONG AGENCIES
The moderator of the session on the health research ecosystem—Atul Grover, executive vice president at the Association of American Medical Colleges—asked individuals from the agencies represented at the session to comment on what they found of value in a specific partnership with another agency.
Atkins mentioned the valuable partnership the VA has forged with the National Center for Complementary and Integrative Health in a pain management collaboratory on the use of nonopioid strategies for combating pain, such as acupuncture, yoga, and massage. Together, the two agencies are funding 11 pragmatic trials that are larger than the VA would be able to fund on its own. “It’s a good model of how we can collaborate and bring the advantages of an integrated system [together with] scientific expertise.”
Ling noted that, by statute, CMS has to follow the guidelines developed by the US Preventive Services Task Force, “so without the work of AHRQ, we would not be able to implement some of the effective and important preventive interventions.” CMS is also working with a variety of agencies, including AHRQ, CDC, VA, and DOD, on reducing events of patient harm. “Those are just a couple of examples of the synergy achieved where CMS actions build on partnerships with others,” she said.
Selby pointed to partnerships between PCORI and NIH on pragmatic clinical trials aimed at gathering effectiveness data. PCORI brings a novel perspective to engaging systems and patients within systems, since recruitment remains a challenge. He also mentioned partnerships with AHRQ on dissemination, particularly the dissemination of interventions directed at systems. Mensah cited a partnership with AHRQ on evidence reviews that can be used by professional organizations to develop guidelines in such areas as blood pressure, cholesterol, asthma, and sickle-cell disease. “We don’t have the skill set to do that,” Mensah said. Khanna mentioned the synergy AHRQ has been able to develop with many of the other agencies represented on the panel. “As they position themselves to serve their customers and users in the future, the question is how AHRQ can help them going forward.”
The panelists also briefly discussed their interactions with other agencies not represented at the workshop, such as the Departments of Housing and Urban Development, Transportation, and Labor, which have an important impact on social determinants of health. Such interactions among agencies are rare in Washington, DC, said Atkins, partly because of the way funding oversight is structured in Congress. They typically require “engagement at the highest level,
including among the secretaries and in the executive office of the president.” When such partnerships do happen, they can be powerful, he added, citing an initiative between the VA and the Department of Housing and Urban Development to reduce homelessness among veterans.
Following up on a suggestion from the audience, the panel briefly discussed the prospects of doing pilot studies and scaling up based on the outcomes of an intervention, whether as part of a collaboration or on their own. Phased research studies are one way to try out innovative ideas, they noted. Some will fail, but others will demonstrate enough promise to progress to larger studies. Such plans can be difficult to get through a review committee, some of the panelists added, but investments in small-scale innovative studies can lead to big returns.
In that regard, Selby asked whether peer review is the best way to get projects of this type evaluated and funded. Research sometimes needs to move faster and more flexibly, resulting in rapid cycles of knowledge production, more robust stakeholder engagement, and the use of indirect costs to build infrastructure for this type of work. He also noted that the health care delivery system is decentralized, which means that many things will continue to happen in silos. “Which organizations are responsible for bringing these silos together?” he asked. “Researchers, funders, payers?”
Mensah noted that the workshop is an opportunity for the leaders in the field to articulate where the field ought to be going. “How much of NIH funding for health services research is enough, and how much is too little? . . . We are limited to some extent, and I’m hoping that you can be as forceful as you can as to how to turn discovery into health impact both at the individual but also at the population level.”
This page intentionally left blank.













