The Future of Health Services Research: Advancing Health Systems Research and Practice in the United States (2018)
Chapter: 4 Guiding Health System Performance Improvement
4
GUIDING HEALTH SYSTEM PERFORMANCE IMPROVEMENT
New tools and approaches in health services research are poised to contribute major advances in care quality and efficiency. Developments in predictive analytics and artificial intelligence, models and agreements for large database sharing and analysis, care culture and shared decision-making instruments, and economic and incentive modeling approaches are all examples of advancing health services research capacities. In addition, factors such as how health systems are organized, led, and reformed can improve the care that is delivered, ultimately leading to better outcomes for health care consumers.
PREDICTIVE ANALYTICS AND ARTIFICIAL INTELLIGENCE
Rainu Kaushal, chair and Nanette Laitman Distinguished Professor of Healthcare Policy and Research at Weill Cornell Medicine and chief of healthcare research and policy at the New York-Presbyterian Hospital/Weill Cornell Medical Center, focused on predictive modeling and artificial intelligence, which she described as having “tremendous promise as we start to look forward in health care delivery and in health services research.”
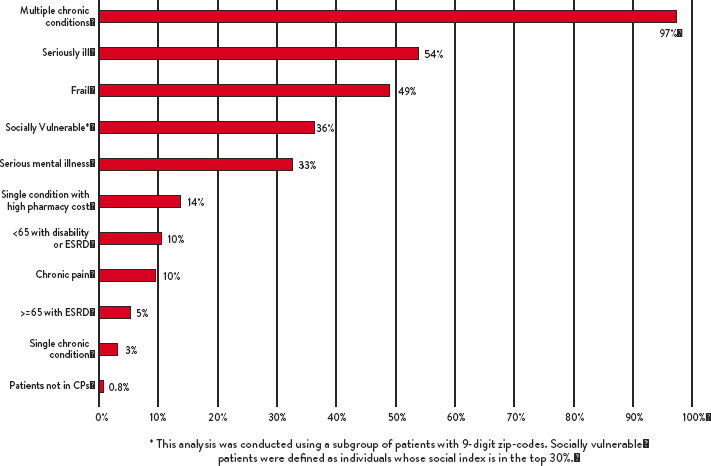
With funding from PCORI, Kaushal and her team have been looking at the 10 percent of high-need, high-cost patients who account for 50 percent of health care costs. Taking advantage of rich clinical, claims, and social determinants data, and incorporating literature reviews and perspectives from patients, clinicians, and health systems leaders, these investigators developed a taxonomy of computable phenotypes to characterize high-need, high-cost patients in order to help target effective interventions. Using data from PCORnet and from Medicare, they were able to link 1 million Medicare beneficiaries with clinical data, and they had nine-digit ZIP codes for 225,000 patients. “That becomes important, because that’s how we began to understand the social determinant
piece,” Kaushal said. Despite the bluntness of ZIP codes as a measure of social determinants, “we were still able to elicit some very meaningful information.”
The team ultimately identified ten medical and behavioral computable phenotypes and calculated the percentage of high-need, high-cost patients within each category. In particular, using the data described above, the team identified a social vulnerability index that described high-need, high-cost patients.
In response to these efforts, three health systems have already pledged funding to translate these computable phenotypes into actionable algorithms using the types of data that the health systems have in hand. Collaborators at the Anthem insurance company are also seeking to translate the data into meaningful variables for the commercially insured. Additional work has focused and will focus on the availability of structured, linkable data, Logical Observation Identifiers Names and Codes (LOINC) laboratory data and the matching of payment and care delivery models to categories of patients.
Kaushal emphasized three principles derived from this work. The first is the importance of multiple sources of data and the ability to link those to social determinants data. The second is that health services research needs to be actionable, whether in terms of new health care delivery models or policy. The third is the importance of patient and stakeholder engagement. “Having patients and stakeholders not only providing input but also actually solving problems together in the same room is what makes the work we do so much richer and so much more meaningful.”
SOURCE: Rainu Kaushal. Presentation to the National Academy of Medicine. February 2018.
IDENTIFYING APPROACHES TO PAYING FOR POPULATION HEALTH
Building on the theme of action-oriented efforts, Dana Safran, chief performance measurement and improvement officer and senior vice president of enterprise analytics at Blue Cross Blue Shield of Massachusetts, described the effort within Blue Cross Blue Shield of Massachusetts to develop a new contract model that would improve quality and outcomes while significantly slowing the rate of growth in health care spending. The result was an approach called the Alternative Quality Contract (AQC). “The uptake of the model happened quite quickly,” said Safran. The model is based on long-term, generally five-year, contracts that establish sustained partnerships and support ongoing investments and commitments to improvement. The contracts specify a global budget for a population, covering the full continuum of care and adjusted by health status. They also employ a set of quality and outcome measures to motivate the improvement of care. The intention is to avoid both overuse and underuse, said Safran. “The quality measures have served a very important role in terms of avoiding the stunting of care that we might fear would happen when you go to a budget model.” Echoing a point made earlier by Leah Binder (see chapter 3), Safran observed that developing these quality measures would have been impossible without health services research.
The AQC was evaluated from its first year (Song et al. 2014). After four years, it had clearly bent the cost curve—“interestingly, more and more each year,” said Safran. Furthermore, it significantly improved quality and outcomes and helped close long-standing health disparities (Song et al. 2017). These disparities were closed even though the AQC does not adjust quality measures by socioeconomic status (SES). “I couldn’t bring myself to say we’re going to set a lower bar in our performance measure for organizations that serve lower SES populations, so we set the same bar for everybody. What happened in our network was pretty remarkable, because organizations that serve the lowest socioeconomic groups were some of the ones that rose from the very lowest levels of performance to surpassing many of the organizations that served a higher SES mix,” said Safran.
One place where health services research has not come into play is in studying how organizations have adapted their delivery system model to achieve the results the AQC has had, Safran pointed out. Still, the absence of that research has not stopped organizations from being creative, testing new methods, learning from others and from best practice-sharing forums, and using the literature to improve quality and cost.
Safran pointed to four domains in which AQC groups have been innovating while reducing overall spending: staffing models, approaches to patient engagement, data systems and health information technology, and referral relationships and integration across settings. She particularly highlighted patient-reported outcomes as “measures that tell us whether what we are doing in health care is working, whether people are feeling better and functioning better because of what we’re doing.” Of the five high-prevalence, high-cost conditions where few quality and outcome measures exist—cardiovascular, orthopedics, oncology, mental health, and obstetrics—Blue Cross Blue Shield of Massachusetts began by introducing patient-reported outcome measures in two areas: depression and hip and knee pain. In 2016, these measures were extended to lower-back pain, prostate cancer, all cancer with active treatment, and coronary-artery disease. The data from these measures can be used to predict who will benefit from certain procedures. Some patients are likely to benefit from a hip or knee replacement, others are likely not to benefit, and for patients in the middle, other factors can impact the care management decision. “Imagine having data like that for shared decision making with our patients in other areas,” Safran concluded. Such information will clearly “get some of the wasteful care out of our delivery system.”
ENGINEERING HEALTH SYSTEM TRANSFORMATION
Bolstered by health services research findings on the results from the application of engineering principles in health care, more and more health care organizations are implementing systems engineering innovations. As an example of successful health systems engineering, Gary Kaplan, chairman and chief executive officer of the Virginia Mason Health System, described the system’s deployment of the Toyota production system to health care. Eighteen years ago, when the process started, Virginia Mason stated that its customer was the patient. But the board “wouldn’t let us accept that,” said Kaplan. “They said, ‘If that’s the case, why do things look the way they do?’” A deep dive into the system then revealed that care was organized around the needs of doctors, nurses, pharmacists, and others working in the system. “The example I always use are waiting rooms, where we spend millions of dollars in this country every year to build spaces so that patients can hurry up to be on time and wait for us. It is the antithesis of patient-centered care.”
The result has been a sustained effort to achieve large-scale culture change through the conscious deployment of a new management system. Virginia Mason found that system not in other health care systems but in the Boeing Corporation. Boeing was using the Toyota production system, which Virginia Mason soon
embraced as not just a process improvement method but as “the way we run the entire organization.”
Kaplan explained that Virginia Mason views quality as a function of delivering appropriate care, improving outcomes, providing high-quality service, and reducing waste. Also critical is ensuring deep respect for individuals within the system through actions such as expressing gratitude and being a team player.
In implementing the Toyota production system, Virginia Mason has seized on an approach known as “experience-based design,” which Kaplan defined as a philosophy and set of methods focused on understanding the experiences and emotions of those who are involved in delivering and receiving health care. For example, it has generated a list of words that are either positive, neutral, or negative and has made them part of the system’s improvement methods, which has enabled it to measure improvements in patient and team member emotional responses.
Among the variables necessary to transform an organization, Kaplan cited a sense of urgency, visible and committed leadership, a shared vision, and aligned expectations. In addition, the current environment requires a continued acceleration of improvement results, he said, given the increased pace of change, the need for increased quality outcomes and reduced costs, and the threat of stress and burnout. Documenting these improvements requires a focus on measurement, which Virginia Mason has achieved by working with other organizations.
Virginia Mason is now in version 2.0 of its production system, which incorporates respect for people and continuous improvement to enhance the flow of health care. At this point, organizations from Japan and other countries are sending teams to the medical center to learn how to apply the Toyota methods, said Kaplan. He concluded by quoting the philosopher Eric Hoffer: “In times of change, learners inherit the earth, while the learned find themselves beautifully equipped to deal with the world that no longer exists.”
Speaking to the challenges faced by organizations seeking to make culture changes of the magnitude required, Kevin Schulman, now professor of medicine at Stanford University, pointed out that a business model is a fixed characteristic of an organization that is resilient and resistant to incremental change. Organizations are designed to produce predictable results, and they do that by building stable cultures. Changes in an organization’s leadership do not automatically make a difference, because people in the organization know the culture and how to behave. This observation applies as much to medical centers as to other organizations, Schulman said. When leaders ask organizations to make changes, “it’s going to be a long time before you get the kind of performance changes you want.”
One way to spur innovation in an organization is to name a chief innovation officer, Schulman observed. But when one of his students surveyed 25 chief innovation officers at large health systems in the United States, she found that the median budgets of the offices of the Chief Innovation Officer were $3.5 million, in organizations with annual budgets that can measure in the billions of dollars (Shah et al, 2018). “The marketing budget when you do a name change is [typically] bigger than the chief innovation officer budgets,” Schulman observed.
In recent years, the greatest changes in the values of goods and services have come from the high-tech side of the economy. Health care, meanwhile, has struggled to bend the cost curve. “That’s our challenge,” Schulman said. “What kind of innovation do we want? How does health services research help us describe the innovation that is needed?” Innovation, according to Schulman, is likely to come from nimble and flexible organizations. “That’s where we’re going to see the huge value creation in the economy.” As one example of where innovation could make a difference, he pointed out that billing for primary care services accounts for 14.5 percent of the total cost, and billing for emergency services takes 25 percent (Tseng et al. 2018). “There are plenty of places where we could see huge innovations,” and where engineering principles can foster improvement.
PROMOTING AND MEASURING CULTURE CHANGE
The panel was challenged by the moderator, Jay Want, executive director of the Peterson Center on Healthcare, to say whether it was possible to identify high-value systems, given the importance of culture in those systems and the difficulty of measuring it. Schulman pointed out that culture builds up over a long period of time and that it is difficult to measure culture objectively. It is also difficult, he added, to measure the impact of leaders on an organization’s culture.
Kaplan argued that health services research needs to develop ways of measuring culture, though Virginia Mason has made progress on measuring subcultures to link staff engagement, patient satisfaction, and a culture of safety to strong managers or weak managers. But measures of end-user value are also important, he said. “The evidence-based process measures that are clearly associated with superior outcomes need to continue to be measured.” To this, Kaushal added that it is critical to use clinical, rather than claims, data for outcome measurement, which will become increasingly possible with the increased structuring of clinical data and more advanced natural language processing.
In response to a question, Kaplan pointed out that the changes instituted in his system have not been based on research, because not much research is available on such changes, particularly as they relate to institutional culture. “When you
are the first to go forward, you’re kind of flying blind.” But these and similar experiences could lend themselves to research on the impact of culture, he added. However, Charles (Chip) Kahn, of the Federation of American Hospitals (FAH), made the additional point that most hospital organizations have relatively small market shares, which makes widespread cultural change more difficult. The centrality of culture to sustained organizational success, in combination with the underdeveloped state of the science base on factors that shape culture change, is testament to its importance as a health services research focus.
MEASURING VALUE
Similarly, Safran pointed out that measuring value is difficult, especially since most current measures have grown out of a fee-for-service era. By measuring results, it is possible to link value-based payments to outcome-oriented measure sets. “If we systematically incorporated patient-reported outcome measures into all of the clinical areas [to show] a measurable change in how somebody is feeling or functioning, then we could tell you who to invest that capital in and who not to, but we don’t have that today. We have just a few outcome measures on things that you know are important, but they’re not everything, and they’re certainly not what’s important to patients.”
Lee Fleischer, from the University of Pennsylvania Perelman School of Medicine, raised the issue of complications in measuring outcomes and understanding value such as the placebo effect, since patients may feel better after having a procedure even though the procedure would not be judged appropriate on other measures. Kaplan acknowledged the “complex interaction between a needy consumer and a willing provider.” As an example, he pointed out that, among the patients sent by physicians to Virginia Mason for complex spine surgery, only 1 percent of those subsequently go on to have surgery. “It’s not that people have malintent,” he said. The problem is the unintended consequences of overuse by both consumers and providers, “and we have to attack both of those.”
Mark Pauly, Bendheim Professor in the Department of Health Care Management at The Wharton School and Professor of Economics in the School of Arts and Sciences at the University of Pennsylvania, commented that most businesses do not get tangled up in outcome measures. Their outcomes are whether people are willing to pay money for the goods and services they provide. Health care is different in that people are not used to thinking that way, though they can be encouraged to ask and answer such questions—such as how much money they would be willing to pay for an extra quality-adjusted life year. The health care system also can be structured so that consumers must make choices across health
plans affiliated with different systems so that they can consciously think about their tradeoffs. Schulman pointed out that one issue is the disconnect between the amount consumers are willing to pay for insurance and the costs of expensive procedures and treatments, such as treatments for cancer. For this reason, he said, “implementing a low-cost health plan can be impossible.”
As health services research is increasingly called upon to define and elaborate on the value proposition under circumstances in which the balances among individuals, societal, and commercial perspectives contribute substantial complexity, it will be all the more important to have systematic, transparent, and multistakeholder public engagement.







