The Future of Health Services Research: Advancing Health Systems Research and Practice in the United States (2018)
Chapter: 5 Bridging Health and Social Services to Improve Care Access
5
BRIDGING HEALTH AND SOCIAL SERVICES TO IMPROVE CARE ACCESS
A long-time priority of health services research has been a focus on issues affecting access to care, including community factors, the availability of social services, and the social determinants of health. Social determinants of health have been defined by Healthy People 2020 as “conditions in the environments in which people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks.” These issues, among others, result in a rich network of interlinked issues for health services researchers.
UNDERSTANDING SOCIAL DETERMINANTS OF HEALTH
The social determinants of health are ubiquitous and have a significant impact on health outcomes, said Sandro Galea, dean and Robert A. Knox Professor at Boston University School of Public Health. “You can’t avoid thinking about ubiquitous determinants if you want to get insight that informs the kind of questions that health services research is trying to get at.”
Health systems are starting to realize the power of this observation. For example, the Boston Medical Center is investing $6.5 million in affordable housing to enhance health in the community, improve patient outcomes, and reduce medical costs. On its website, the CDC has called attention to several such factors that have a direct and measurable effect on health:
- With rehabilitating housing, 62 percent of adults have excellent health versus 33 percent without such housing.
- In a city of a million residents, a 40 percent expansion in transit development has an annual health benefit of $216 million.
- Early childhood education has a benefit-to-cost ratio of 5 to 1 with a reduction in crime rates, child maltreatment, teen pregnancy, and academic problems.
- Each time the Earned Income Tax Credit increases by 10 percent, infant mortality drops by 23.2 per 100,000 population.
Galea is the coauthor, with Katherine Keyes, of the book Population Health Science, from which he drew two conclusions that are directly relevant for health services research (Keyes and Galea, 2016). The first is that the magnitude of an effect of exposure on disease is dependent on the prevalence of the factors that interact with that exposure. For example, three studies might look at the effects of an intervention on hypertension, with one finding no effect and the other two finding effects of different sizes. One interpretation is that two of the studies were wrong, but that is “not necessarily the case,” said Galea. Rather, the intervention may need to happen along with exposure to other conditions to have an effect. If the intervention and a social condition are both necessary but insufficient causes of an outcome, then the outcome will occur only when both are present. If all, none, or some members of a population are exposed to the social condition, outcomes will vary accordingly when they are exposed to the intervention. The challenge with ubiquitous conditions is that their influence cannot be separated out because they “affect everybody, all of us, all the time,” said Galea. Proper inferences in health services research, therefore, need to take these ubiquitous forces into account.
The second principle he cited is that small changes in ubiquitous causes may result in more substantial changes in the health of populations than larger changes in rarer causes. Galea cited the metaphor of goldfish in a fishbowl that are given plenty of food but die because their water is never changed. Another example is early research on babies whose mothers used crack cocaine that found an association between crack cocaine use and developmental delay. However, long-term studies found that the overriding predictor of developmental delay was exposure to extreme poverty and lack of environmental stimulation. “We missed the presence of the ubiquitous factor.”
Galea drew three implications from these observations. First, “you simply can’t forget ubiquitous causes.” Second, researchers need to focus on what matters most. Third, health is not a dichotomous outcome and needs to be considered more broadly as a continuous outcome. “We hinge our inference on stories that are simpler than the reality,” he concluded. All research endeavors must therefore focus on the systemic context of issues being studied.
MOVING RESEARCH INTO COMMUNITIES
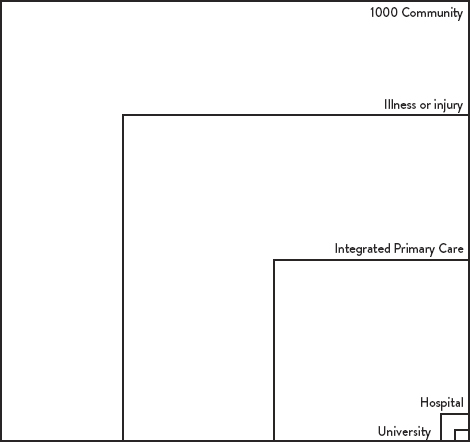
Building on the themes from Galea’s presentation, Jack Westfall, medical director of whole-person care at Santa Clara Valley Medical Center, observed that most of the people in the community are not getting health care in the places where health services researchers get much of their data. In a classic article on the ecology of medical care, White et al. (1961) displayed graphically that of 1,000 people in a community, 750 experience illness or injury in a given month, 250 seek primary care, 10 are hospitalized, and 1 is hospitalized in an academic health center (Figure 5-1). This assessment was repeated in 2000 and in 2016 (Green et al. 2001; Johansen et al. 2016) with similar conclusions.
Not much is known, Westfall pointed out, about the interface between the 10 people who are hospitalized and the 250 people who are seen in an ambulatory setting, or between the people seen in the ambulatory setting and the 500 who experience illness or injury during that month but do not seek care, or between the 750 who experience an illness or injury and the 250 who remain well in a given month.
Innovation moves into the community through the types of research along stages of a translational continuum represented as T1 through T4 in Figure 5-2, connoting the progress from basic research to the implementation of research in the community. T1 and T2 research occurs mostly at academic institutions. Laboratory discoveries are translated into human pathophysiology. New pills, procedures, and devices are translated into treatments and disease-modifying management programs. But new discoveries also must be translated into clinical practice in real-world settings, where patients and communities can provide the context for new discoveries and lead to locally relevant and meaningful programs and language. T3 and T4 research moves findings from academic institutions into the world of integrated primary care and population health, where data to ask and answer questions about translating discovery in a few to the many begin to accrue. These different kinds of research line up with the boxes in the ecology of medical care, Westfall observed. Much of the early research is done in the institution, while much of the practice-based and community research is done in the larger boxes.
These observations are not new, Westfall pointed out. In 1967, Marion Folsom published the book Health is a Community Affair, which made the point that education, food security, safe housing, legal services, and other factors all combine to impact individual and community health (Folsom, 1967; Folsom Group, 2012). From this perspective, health care problems occur in the community, not in the
smaller boxes of the ecology of health care (Figure 5-2). They encompass public health, community services, and primary care. The judicial system, food deserts, education levels, safe housing, and human services “all conspire to impact health care and health care utilization.”
SOURCE: White at al. 1961
Health services research must ensure that it is assessing the ultimate impact of forces on system-wide performance and health outcomes, Westfall observed. It can work at the level of integrated primary care, at the community level, or with people who are experiencing the social determinants of health but are not yet suffering consequences to their health. Traditional academic research increases understanding of what happens when prevention does not occur or illness is not treated. Health services research can define the parameters of prevention, measure the impact and develop interventions for the disintegrated social determinants of health, and ask and answer questions that matter to more people more of the time. “However, we’ve seen a disproportionate share of health services research time and resources spent on the small boxes in the lower right-hand corner,” said Westfall, where hospital claims data and electronic health record data tend to be available. “Health services research has gravitated to where the data are.” A primary challenge for the field is shaping the capacity to account for and assess system factors in play.
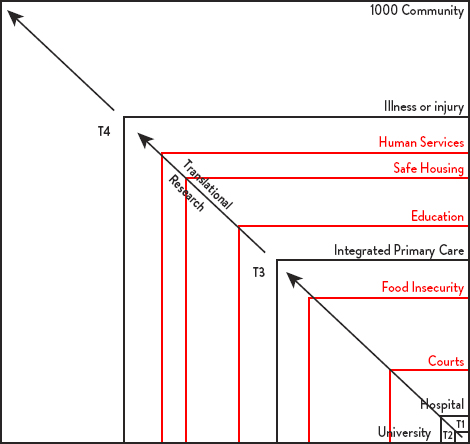
SOURCE: Adapted from White et al. 1961
Focusing on the ubiquitous determinants of health in social and community settings can link the small boxes with the much larger boxes. It can also help meet needs in the clinic, community, and broader population. In the exam room, providers need discoveries to work for individual patients given their unique biology, family, neighborhood, values, and choices. In an integrated primary care clinic, providers and their staff need discoveries that they can offer safely with high fidelity and quality. At the community level, they need discoveries that patients will seek out and accept, that are available, and that align with the values of the community. At the population level, they need discoveries that are affordable, that make the world a better place, and that balance the needs of the individual, practice, and community.
EFFECTS OF HEALTH INSURANCE BENEFIT DESIGN
Within the health care system, consumers can be engaged in their care through a variety of mechanisms, including shared decision-making, case management, health navigators, and benefit design. Michael Chernew, Leonard D. Schaeffer Professor of Health Care Policy and director of the Healthcare Markets and Regulation Lab in the Department of Health Care Policy at Harvard Medical School, discussed the last of these options. It is not the only and may not even
be the best way to involve consumers in health care decisions, he said, but it has been the focus of much innovative health services research.
Annual health care deductibles have been rising much faster than inflation or earnings since 2011. Deductibles are designed to improve incentives for health care consumers by reducing excess use of health care and encouraging price shopping. However, there are three problems with this approach. Prices for health care are high, some health care services are overused, and some are underused. Patients do respond to cost sharing (Brook et al. 2006). When they are charged more, they use less care. However, “consumers aren’t great shoppers,” Chernew noted. “They cut back on appropriate use and inappropriate use in the exact same amount.” Copays reduce the use of preventive services and beneficial pharmaceuticals (Sui et al. 1986). “It’s amazing how little you can charge somebody and have them not take their preventive medicines or use preventive services.” The overall picture, said Chernew, quoting a friend, is that “the United States has Star Wars medicine and Flintstone financing.”
“Nuances” can be a critical influence in benefit design, said Chernew. For example, use of a tiered network design can steer patients away from nonpreferred to preferred hospitals (Frank et al. 2015). Benefit designs can affect whether patients choose high-price or low-price hospitals for knee- or hip-replacement surgery (Robinson and Brown, 2013). The structuring of copayments can increase adherence to medications (Chernew, 2008).
The problem with nuances is that they can be complicated, Chernew admitted. “The challenge for health services research going forward is how nuanced can we be” and to identify innovative nuances that decrease spending without negatively impacting outcomes for patients. For example, straightforward price transparency tools are not associated with lower outpatient spending (Desai et al. 2016); instead, patients tend to do what their doctors say. Better incentive designs have the potential to work, he insisted, so long as consumers are not overwhelmed. “You have to both give them tools but understand that they’re not going to use tools and be as rational as you might think they would be.”
DEALING WITH COMPLEX HEALTH CARE NEEDS
Gerard Anderson, professor of health policy and management and director of the Johns Hopkins Center for Hospital Finance and Management, pointed out that one important finding from health services research is that most spending and utilization are by people with complex health care needs, including people with multiple chronic conditions and/or functional limitations. For example, health services research has revealed that people with complex health care needs have
much higher readmission rates on average. This finding has led to new initiatives involving clinical and community interventions, though a major challenge is finding and implementing programs that control spending while improving satisfaction and clinical outcomes.
The issues raised by people with complex health care needs run counter to the severe siloing that occurs in health care, Anderson pointed out. For example, most clinical trials exclude people with complex needs, but “they are the ones who are mostly taking the drugs.” Health services research has developed approaches to fill in the missing information but not always successfully. Similarly, most fee-for-service payment systems focus on one problem at a time, though health services research has developed risk adjusters that allow for approaches like capitation. In addition, most quality metrics are disease or procedure specific, and most clinical education programs still teach about the body organ by organ. It is incumbent on health services research to break down these silos—for example, through research on care coordination.
More work is needed on adjusting outcome measures for people with chronic conditions and determining the most significant interventions and settings for people with particular sets of conditions, said Anderson. Reconciling who benefits and who pays in such situations is a critical problem, because in many cases the benefit for which an insurer pays does not occur until much later.
Anderson also took an international perspective on health services research. The United States actually uses fewer medical services than most other industrialized countries. In 2015, it had 19 percent fewer doctors, 20 percent fewer nurses, and 26 percent fewer hospital beds compared to the median country in the Organisation for Economic Co-operation and Development (OECD). However, the price of its health care makes the United States unique. This raises several new questions for health services research. For example, Anderson asked why the private sector is willing to pay 50 percent more than the public sector for the same service. One answer is that providers will spend whatever they are given, which then becomes their cost, he said. Another question is why the United States is willing to pay 50 to 100 percent more for brand name drugs than other industrialized countries. Members of Congress with whom Anderson has talked are “very concerned about this particular issue.” Clearly, a research priority is making more transparent the systemic factors that shape the course of health costs and value.
Relatedly, Anderson mentioned tiered benefits in the context of pharmaceuticals. The greatest challenges for pharmaceuticals are access and adherence. Surveys by the Commonwealth Fund suggest that the US population has the most difficulty purchasing drugs among OECD countries (Sarnak et al. 2017). This finding, too, raises several compelling questions:
- How can tiered benefits be designed for very expensive drugs?
- What are the tradeoffs between who pays and who benefits?
- What can consumers understand about tier, cost, and treatment tradeoffs?
A prominent example involves hepatitis C, now responsible for the most infectious disease deaths in the United States. There are effective treatments for hepatitis C with minimal side effects, yet many people with hepatitis C are not getting care because of costs. Medicare beneficiaries must pay an average of $7,000 out of pocket, and states cannot afford to provide hepatitis C drugs to all prisoners, Medicaid recipients, and the uninsured, Anderson observed.
SUPPORTIVE AND PROTECTIVE FACTORS
Meeting participants also considered the importance of a better understanding of the protective community factors that keep people out of the health care system, such as patient health behaviors, social supports, and social services. For example, Lucy Savitz, vice president for health research for Kaiser Permanente Northwest Region, said that she helped rebuild the primary care system in Biloxi, Mississippi, after Hurricane Katrina, which impressed on her the importance of protective factors like strong social support and family cohesion. Later, at Intermountain Healthcare Institute for Healthcare Delivery Research, she observed that even people with fairly serious mental health conditions could be safely cared for in a primary care setting if they had strong social support and family cohesion.
Galea observed that research shows that one of the best ways to mitigate mental illnesses after a disaster is to focus on social support and social services. “Make sure people have houses, people have care for their elderly parents, people can get their kids into school,” he said. “That mitigates the consequences on mental health.” In fact, he thought it an artificial distinction to say that delivering mental health services is a health service while delivering housing is a social service. “Ultimately, they are restoring people to health or improving population health.” Health services researchers are partly responsible for this, he continued, by limiting their scope to medical services and leaving other services to other people.
Westfall connected the issue to the ecology of medical care, pointing out that the 250 people each month who do not experience illness or injury is the same size as the group of people who seek medical care, but it is half the size of the group of people who experience an illness or injury but do not seek care. “Something is going on in that group that’s half of the population, but they’re not seeking care,” he observed. “What are the factors that are occurring in the community that are protective? . . . What occurs in that box of 500 people who
experience illness or injury but who don’t seek care? That’s a group that health services research could learn a lot from.”
Ann Beal, global leader of patient solutions at Sanofi, noted that factors intrinsic to patients are also important to health care, such as patient health behaviors. “Now that we’re in an era when so many of the conditions require significant patient self-management, this will help us to be much more accurate in our ability to understand not only health outcomes but also how patients then navigate the health care system.” She also pointed out that, by focusing on the average, half the people are outside one standard deviation from the mean. Could a more personalized set of analyses enable health services researchers to move from observational analyses to more predictive analyses and ultimately prescriptive analysis? Anderson commented that considerable work is being done on trying to characterize people into categories in such areas as “need for social services” and “adherence to treatments.” The policy challenge is that categorization tends to divide people into categories that get different levels of service.
This page intentionally left blank.









