Exploring Risks of Repeated Head Impacts in Youth and Strategies to Minimize Exposure: Proceedings of a Workshop (2026)
Chapter: 4 Examining Strategies to Address Repeated Head Impact Exposure in Youth
4
Examining Strategies to Address Repeated Head Impact Exposure in Youth
Key Points Highlighted by Individual Speakers1
- Reducing youth exposure to repeated head impacts (RHI) is an important goal, even in the absence of definitive evidence linking RHI exposure to long-term health outcomes (Caccese).
- Limited availability of sensitive outcome measures beyond concussion counts affects the ability to evaluate interventions and to determine whether health outcomes are related to RHI exposure (Caccese).
- Reducing youth exposure to RHI requires multifaceted strategies including policy and rule changes, behavior modifications, equipment evaluation, education and training, and policy enforcement with consideration for sport-, age-, sex-, and community-specific needs (Caccese, Gioia, Urban).
- Policy changes can reduce concussion and RHI rates, but consistent enforcement and appropriate training are critical (Emery).
- Behavior-focused interventions such as progressive skill instruction and helmetless tackling drills can reduce head impacts when implemented consistently but require commitment across those involved in the sport (Swartz, Urban).
___________________
1 This list is the rapporteurs’ summary of points made by the individual speakers identified, and the statements have not been endorsed or verified by the National Academies of Sciences, Engineering, and Medicine. They are not intended to reflect a consensus among workshop participants.
- Modifying equipment or play characteristics—such as ball properties in soccer—has potential to reduce head impact forces, though further study is needed (Chiampas).
- Cultural and behavioral changes are essential for lasting reductions in RHI, requiring buy-in from leagues, coaches, parents, and athletes (Caccese, Chiampas, Emery, Gioia, Swartz, Urban).
- Sex-specific differences in biomechanics, contact technique, and training opportunities may contribute to higher RHI rates in female athletes. Targeted training and improved enforcement of policies intended to reduce RHI could help reduce disparities (Chiampas, Emery).
- Community-engaged approaches can be used to codesign evidence-informed, practical, and acceptable interventions to address RHI exposure during youth sports (Emery, Urban).
- Sports practice settings account for a large proportion of RHI exposure in youth sports and are highly adaptable, making them a prime opportunity for implementing changes to reduce RHI (Urban).
- Inconsistent governance structures, reliance on volunteer leadership, varying requirements, and reliance on voluntary participation in training and policy adoption contribute to variability in the reach, implementation, and enforcement of RHI reduction strategies across youth sports (Chiampas, Gioia, Urban).
- Education at all levels—from coaches and referees to parents and athletes—supports the adoption and consistent application of safety strategies, reinforces policy implementation, and helps shift standards toward reduced RHI exposure (Caccese, Chiampas, Emery, Swartz, Urban).
- Resource limitations, lack of infrastructure, and minimal oversight in many youth sports programs can make it challenging to implement and sustain RHI reduction strategies, particularly in lower-resourced communities (Urban).
- Organizational readiness assessments and preimplementation frameworks can help determine whether youth sports programs can adopt safety interventions. Aligning safety messages with performance goals and using credible peer mentors can improve uptake (Urban).
- Shared decision-making frameworks, adapted for adolescent–parent dyads, can support high-quality return-to-sport decisions after concussion by aligning information, values, and available options with the athlete’s overall well-being (Kroshus-Havril).
- Differences in resources and access to safer sport options can constrain family decision making and may contribute to disparities in RHI prevention opportunities (Kroshus-Havril).
This chapter examines emerging strategies to reduce youth exposure to repeated head impacts (RHI), including evidence-informed interventions in sports, opportunities for community engagement to codevelop feasible and acceptable approaches, and best practices in decision making about return to activity. Presentations across two sessions highlighted rule-based and behavior-based approaches for reducing RHI exposure, discussed challenges in implementation and evaluation, and considered how research, policy, and education can support safer participation.
EXPLORING INTERVENTIONS TO MINIMIZE EXPOSURE TO RHI
Gerard Gioia, chief of the division of pediatric neuropsychology at Children’s National Hospital, introduced and moderated a session on interventions to reduce exposure to RHI in youth. While growing awareness of potential long-term risks such as chronic traumatic encephalopathy (CTE) has drawn attention to RHI, Gioia emphasized the importance of focusing on what can be done now to limit exposure during critical periods of brain development. Panelists discussed practical strategies already in use—including rule changes and behavior-based modifications—drawing on examples from a range of sports and settings. While challenges remain in translating evidence into widespread practice, speakers underscored the need for continued evaluation, clearer metrics of effectiveness, and broader support for implementation at the youth level.
Intervention Evaluation
Jaclyn Caccese, an assistant professor at the School of Health and Rehabilitation Sciences at The Ohio State University, outlined a multitiered framework for evaluating and implementing interventions to reduce
exposure to RHI. Evaluation strategies span from laboratory testing of protective equipment to on-field monitoring and brain structure/function metrics—highlighting the need for sensitive outcome measures beyond concussion surveillance. Caccese emphasized that most research has focused on football, underscoring the need for sport-specific and population-specific strategies, particularly for underrepresented groups such as girls and younger athletes. Effective interventions may include training to improve tackling techniques and neck strength, identifying high-risk individuals, coach and stakeholder education, and use of head impact monitoring systems. Caccese emphasized that no single intervention is sufficient; instead, a multifaceted approach—including limiting contact during practices and updating rules or policies—is essential to meaningfully reduce RHI exposure in youth sports.
Policy Considerations
Ice Sports
Carolyn Emery, professor in kinesiology at the Cumming School of Medicine, University of Calgary, discussed evidence-informed policy to reduce risk of RHI exposure in youth ice sports. For example, disallowing body checking in youth ice hockey led to substantial reductions in concussion rates (Emery et al., 2022), as well as significant decreases in overall physical contact and player-to-player head contacts in adolescent players (Kolstad et al., 2022). Additional analyses demonstrate that policy change alone is insufficient. A zero-tolerance policy for head contact by Hockey Canada did not reduce head contact incidence until enforcement was strengthened, she said. Additional penalties yielded a 30 percent reduction in head contacts (Williamson et al., 2022). However, less than 20 percent of head contacts result in penalties, Emery noted, suggesting a role for increased referee training.
Drawing on findings from a broader set of ice sports played by boys and girls, Emery argued that consistent penalty enforcement and referee training are critical to effective prevention. In girls’ hockey—where body checking is prohibited—head contact rates are nearly three times higher than in boys’ non-body-checking leagues. Similarly, girls’ ringette2 has high rates of head contact, approximately four times that of boys’ non-bodychecking hockey. Across both girls’ hockey and ringette, the proportion of penalized head contacts remained low (Heming et al., 2024). These findings, Emery noted, point to enforcement gaps and the need for referee
___________________
2 Ringette is a winter team sport played on an ice rink using ice hockey skates, straight sticks with drag-tips, and a blue, rubber ring.
education and training to support implementation of safety policies and reduce RHI exposure across all youth ice sports.
Soccer
George Chiampas, an assistant professor in emergency and sports medicine at Northwestern University and chief medical officer for U.S. Soccer, described how U.S. Soccer has implemented policy and education initiatives to reduce youth exposure to head impacts. In 2015, U.S. Soccer became the first international governing body to implement age-based heading restrictions—prohibiting heading under age 10 and capping headers per week for older youth. This decision was informed by studies showing that most concussions in youth soccer arise from aerial challenges rather than purposeful heading, Chiampas said. Preceding this decision, a 2014 class-action lawsuit filed by parents and former youth players sought rule changes—rather than damages—alleging inadequate concussion management by the Federation Internationale de Football Association (FIFA) and corresponding U.S. governing bodies (Strauss, 2015).3
Chiampas highlighted a few studies that monitored outcomes related to this policy change (Kaminski et al., 2020; Lalji et al., 2020; Sullivan et al., 2024). A recent study comparing emergency department data before and after the heading restrictions found a 25.6 percent relative reduction in soccer-related head injuries and a drop in the proportion of concussion-related visits—from 8 percent to 6 percent (Sullivan et al., 2024). Survey data indicate high awareness and adherence among U.S. coaches, with over 90 percent reporting knowledge of and compliance with the heading policy (Kaminski et al., 2020). These findings suggest that coaches and national governing bodies can successfully implement and scale safety interventions when paired with education and infrastructure, he said. Research has also begun examining modifiable risk factors that influence head impact exposure, such as ball size, mass, inflation pressure, and stiffness. A recent systematic review suggests that adjusting these factors may reduce injury risk (Oliva-Lozano et al., 2024).
Education has been instrumental in supporting the implementation of U.S. Soccer’s heading policy, Chiampas noted. One example is the Recognize to Recover platform—a central resource for coaches, parents, clubs, and players that offers guidance on concussion awareness and broader health and safety topics.4 Another education intervention, the Pregame Safety Huddle, promotes concussion awareness and symptom reporting through brief, structured conversations among coaches, referees, and players before
___________________
3 Mehr v. Fèdèration Internationale de Football Association.
4 See https://www.recognizetorecover.org/ (accessed September 4, 2025).
each match. Preliminary results suggest this approach increases the likelihood of athletes reporting symptoms (Kroshus et al., 2023). A larger multistate study is planned to further evaluate and expand the program.
To provide consistent, evidence-informed instruction on heading technique, U.S. Soccer also launched the Get aHEAD Safely in Soccer initiative. In partnership with the University of Delaware, the program aims to develop and disseminate a standardized training pathway for coaches and clubs that incorporates safe heading practices and addresses modifiable risk factors, such as ball size and inflation, Chiampas said.
Behavior-Based Interventions
Erik Swartz, director of the Hawaii Concussion Awareness Management Program at the University of Hawaii, described behavior-based interventions designed to reduce head impact exposure in football, highlighting both evidence gaps and promising practices. Head impact exposure tends to increase with age and level of play, but Swartz argued that ideally exposure should decrease as athletes gain proficiency in technique. A recent position statement from the National Athletic Trainers’ Association (NATA) outlines behavior-focused strategies to minimize headfirst contact in football through behavior-based approaches (Swartz et al., 2022). Recommendations include progressive, evidence-based instruction in blocking and tackling techniques, particularly for first-time participants and during preseason, with an emphasis on skill mastery and maintenance.
Swartz also discussed a helmetless tackling intervention aimed at improving technique and reducing head impacts by removing helmets during controlled practice drills. In a nested randomized controlled trial with high school students in New Hampshire, the intervention group experienced fewer head impacts during early to midseason games, although this difference did not persist through the full season (Swartz et al., 2019). A subsequent 3-year randomized trial in Hawaii demonstrated reduced head impact exposure among athletes with high adherence to the intervention (Swartz et al., 2024). Across studies, Swartz emphasized that consistent implementation was critical to success.
Discussion
Gioia moderated a wide-ranging discussion that explored practical, cultural, and systemic dimensions of efforts to reduce RHI in youth sports. Panelists examined the limits of technical interventions in the absence of behavioral change, underscored the importance of community buy-in across all levels of youth sports, and emphasized the need for inclusive, collaborative approaches to implementation. The conversation highlighted that
durable change likely depends not only on evidence-based strategies, but also on shifting entrenched norms, adult behaviors, and shared expectations around safety in sport.
Cultural Change as a Prerequisite
Gioia opened the discussion by noting that reducing RHI exposure in youth is not only a technical challenge but a cultural one. Speakers emphasized that changes to rules, equipment, or training must be accompanied by shifts in adult behavior and youth sport norms. Caccese and others noted that effective interventions hinge on buy-in by leagues, coaches, parents, and players alike. Swartz likened the coach’s role to that of a caregiver ensuring treatment adherence, emphasizing that consistent delivery and reinforcement of evidence-based practices at the team level is essential for meaningful risk reduction. Emery echoed the importance of having all at the table to codesign interventions to get the most efficient translation of research to best practice.
Uneven Governing Structures
Arbogast posed a question to the panel about the unevenness of governing structures in youth sports. In particular, she noted that not all youth leagues are affiliated with national organizations, making it difficult to ensure that evidence-based interventions reach coaches and players. In his response, Chiampas further underscored the decentralized nature of youth sports in the United States, citing state-by-state legal variations, inconsistent coach training requirements, and divergent local practices. These discrepancies, he said, “muddy the waters” for implementation.
Gioia supported this by highlighting that less than 20 percent of youth football organizations are part of major leagues (e.g., Pop Warner, USA Football affiliates). While millions of coaches have voluntarily completed trainings like Heads Up Football, the lack of a mandate means coverage is incomplete. Caccese further noted that in the current landscape, digital platforms may represent one of the most powerful dissemination tools, especially in a context where federal agencies may not have the resources or reach to lead.
Contact Progression for Youth Football
In response to a question from Yeates about whether youth football is moving away from full-contact formats toward noncontact options like flag football, Gioia noted that many programs across the country are adopting the American Development Model (ADM). This model introduces children
to football in progressive stages—starting with flag football, then moving to modified-contact versions, and, eventually, full-contact formats. Each stage is designed to be age- and developmentally appropriate, aiming to reduce exposure to head impacts while still teaching the fundamental structure and flow of the game.
However, Gioia acknowledged that many leagues are uncertain about how to implement this progression in practice. Across the country, coaches and administrators are unsure about when and how to place athletes into the appropriate level of contact. This, he said, reflects a need for more research on how to align entry into contact play with developmental readiness—not just age. Specifically, determining whether a child has the cognitive, physical, and motor skills to handle the demands of tackling and blocking safely is essential, he said. Gioia cautioned that policies advocating for a blanket age cutoff (such as prohibiting tackle football before age 14) may overlook individual variability and inadvertently create new risks.
Swartz also raised concerns that delaying exposure to contact altogether may have unintended consequences. Without graduated exposure or adequate instruction, athletes entering tackle football later—at the high school level, for instance—may be less prepared technically and physically. This lack of preparation could paradoxically increase the risk of injury.
Caccese added that preliminary data from her ongoing studies suggest that athlete age, size, and strength do not correlate strongly with head impact exposure. Rather, environmental factors—such as the type of drills used in practice—may have a much greater influence. She also reflected on observational data showing a steady decline in head impact exposure in youth tackle football players over the past decade (Dorman et al., 2022). Notably, this improvement occurred without any intervention, suggesting that increased awareness, combined with evolving practice standards and policy shifts, may already be making a meaningful difference, she said.
Age-Specific Considerations
Fred Rivara asked how U.S. Soccer arrived at its current age-based restrictions on heading. In response, Chiampas explained that U.S. Soccer convened a panel of multidisciplinary experts—including pediatricians and other clinicians—to evaluate a range of variables. These included child developmental stages, the style of play that U.S. Soccer aims to promote nationally, and an analysis of how and when concussions typically occur in youth soccer.
The group determined that most injuries occurred during aerial challenges—scenarios in which players attempted to head the ball in contested, often chaotic situations. They then examined the developmental readiness of children to safely execute such plays. The panel concluded that younger
children, particularly those under age 10, are still learning how to jump, fall, and visually track a ball. These are foundational motor and perceptual skills, and the ability to coordinate them reliably had not yet developed in most children in that age group.
Based on these insights, U.S. Soccer established a policy that heading should be eliminated entirely for players under age 10. The focus at those levels, Chiampas said, should be on enjoyment and skill building—keeping the ball at the players’ feet, not in the air. For players aged 11 to 13, heading is introduced as a skill, but only in a controlled and limited manner. Guidelines specify the amount of time that may be spent teaching or practicing heading to avoid excessive repetition.
Chiampas noted that the same committee reconvened in 2024 to reassess the available science and determine whether these policies should be revised. After reviewing the latest evidence, they concluded that the current age-based guidance remained valid and appropriate, he said. He contrasted U.S. Soccer’s policy with that of the English Football Association, which has instituted stricter heading limitations at higher ages. One concern, he said, is that delaying heading too long could leave adolescents unprepared to safely execute the skill when it becomes a part of the game—especially given that older players are bigger, stronger, and faster.
Sex-Specific Considerations
Gioia asked about research investigating why female hockey players appear to have higher concussion rates than their male counterparts, despite playing in noncontact leagues. Gioia and Emery suggested that one possible explanation is the lack of training on safe body contact due to the noncontact nature of the girls’ game. Without formal instruction on how to initiate, absorb, or avoid contact, players may be more vulnerable to injury when contact inevitably occurs. Emery added that video analyses reveal high rates of body checking in girls’ hockey leagues, even though it is technically disallowed. Moreover, few penalties are called for such infractions. The implication, she noted, is that rule enforcement may be inconsistent, and that newer players may lack the technique or situational awareness needed to protect themselves. In such settings, the absence of both enforcement and training can leave players particularly exposed.
Extending this discussion to soccer, Chiampas highlighted that differences in neck strength and heading technique between boys and girls may also play a role in differential rates of head impact exposure and injury. He pointed to training as a potentially effective intervention to address these biomechanical and neuromuscular differences.
Emerging Interventions to Mitigate Effects of RHI
An audience participant asked about the use of jugular vein compression collars (e.g., Q-Collar) as a strategy to prevent concussion or mitigate the effects of RHI. Emery noted that while there are “interesting physiological findings,” current epidemiological evidence does not demonstrate meaningful changes in clinical outcomes (Delgadillo et al., 2025). Swartz cautioned that such devices may inadvertently alter athlete behavior: If players believe they are better protected, they may engage in riskier play—a phenomenon known as risk compensation. Caccese added that, unlike helmets or rule changes that can physically reduce the magnitude or frequency of impacts, jugular vein compression collars are designed to work by modulating internal physiology. Specifically, they are intended to slightly increase intracranial blood volume to stabilize the brain during impact. Even if effective in that regard, Caccese noted, these collars would not reduce the number or intensity of head impacts themselves.
Bazarian concluded the exchange by broadening the question, suggesting that the field could consider additional options to mitigate the physiological effects of RHI. He mentioned nutritional supplements such as fish oil and cognitive interventions like educational enrichment as examples of strategies that might reduce harm without necessarily reducing exposure. These approaches, he said, reflect a growing recognition that some interventions may work not by preventing impacts, but by buffering the brain’s response to them—a hypothesis that warrants further study.
ENGAGING COMMUNITIES AND FAMILIES TO REDUCE RHI EXPOSURE
Christina Master, professor of pediatrics and orthopedic surgery at the University of Pennsylvania Perelman School of Medicine and pediatric sports medicine specialist at the Children’s Hospital of Philadelphia, introduced the session with a call for collaborative action to reduce the risk from RHI in youth. Emphasizing that no single individual or discipline can address the issue alone, Master urged the development of concussion- and RHI-aware communities that build trust and support informed decision making, balancing risks with benefits of participation in sports. Drawing a parallel to the field of sports cardiology—which has evolved toward shared decision making that supports safe sports participation for youth with cardiac conditions—Master expressed hope that the field of RHI is on a similar trajectory. She framed the session as an opportunity to hear from expert speakers, reflect on current practices, and identify meaningful next steps for research, education, and policy.
Opportunities for Community Engagement to Develop Policy and Systemic Changes
Jill Urban, associate professor at Wake Forest University School of Medicine, presented findings from a community-engaged research initiative to develop and pilot test an intervention aimed at reducing RHI exposure in youth football. She examined the practical challenges of implementing injury prevention strategies in community-based sports environments and highlighted the potential of community engagement to build trust, strengthen adoption, and codesign feasible, evidence-based interventions.
Implementation Challenges in the Youth Sports Environment
Urban discussed the unique challenges of implementing policies and intervention in the youth sports environment. Youth have the greatest number of sports participants but often participate in community organizations with limited resources, limited oversight to enforce rules and regulations, and volunteer coaches, making implementation and enforcement of injury prevention strategies a challenge. For example, “youth in communities with greater poverty and lower socioeconomic status were more likely to participate in youth football leagues where coaches had not completed concussion education programs for youth football coaches” (Kroshus-Havril et al., 2017).
Although a survey of youth football parents, coaches, and leaders found that nearly 80 percent agreed that subconcussive head impacts should be avoided, support declined when respondents were asked about changing existing rules to reduce RHI exposure (Urban et al., 2024). Urban emphasized the importance of designing strategies that align with community values and are feasible to implement: “How can we create practical strategies to reduce RHI in sports that coaches and leaders will be willing to adopt?” she asked.
Community Engagement as a Strategic Approach
Community engagement is a promising strategy for codeveloping effective, acceptable interventions in youth sports. This approach fosters sustained partnerships between researchers and community members to build trust, improve communication, and produce actionable, context-relevant solutions (Rhodes et al., 2018). Although community engagement has not been widely used in youth sports, it is gaining traction in injury prevention research (Bruder et al., 2024; Kroshus-Havril et al., 2024). Lessons from related efforts highlight the value of including individuals from the target population on the research team to ensure relevance, clarity, and community participation (Rizzone et al., 2025).
Designing a Community-Informed Intervention for RHI in Youth Sports
Urban’s team used a multiphase process to develop and pilot an evidence-based intervention for youth football coaches. The first phase included field-based monitoring of head acceleration using mouthpiece-mounted sensors with video verification. These data indicated that most head impacts occur during practice and are influenced by how coaches run practice (Urban et al., 2024). “Practices are unique environments in that they’re amenable to change,” Urban noted. “It’s going to be quite challenging to change the game of football, but the practice environment we can actually kind of work together and see what we can do here.”
The team reviewed current guidelines, synthesized existing evidence, and conducted focus groups and surveys with parents, coaches, and youth football leaders to explore beliefs and perceptions about RHI. Key insights included widespread parental trust in coaches, and expectation that the coaches have the knowledge and skills to coach safely, along with concern over gaps in training and an overemphasis on winning. Coaches expressed a need for better tools and guidance on safe practice design (Urban et al., 2025).
From these insights, they launched a stakeholder process that included monthly meetings with high school and youth coaches, organizational leaders, parents, and sports medicine professionals. Participants identified two core intervention targets: (1) improving coaches’ knowledge and skills for practice planning and safe drill selection, and (2) changing beliefs and attitudes about contact during practice. High school coaches, who were already following stricter state-level contact policies, served as mentors and early adopters. The intervention was structured to align with evolving practice guidelines, beginning with North Carolina’s 15-minute contact limit and later adjusting to the National High School Federation’s allowance of a total of 30 minutes of live contact per day (Urban et al., 2024).
Development of the COACH Program
The final product of the community engagement process was the COACH program—Communities Aligned to Reduce Concussion and Head Impact Exposure. This multicomponent intervention includes guided practice plans, a safety-focused coaching booklet with QR-linked demonstration videos, a clinic for youth coaches led by high school coaches and players, and a peer-mentorship program pairing youth coaches with experienced high school counterparts (Urban et al., 2024). The program design was refined through a 5-month stakeholder engagement period, which maintained over 90 percent attendance and continued stakeholder involvement across multiple seasons, Urban said (Figure 4-1).
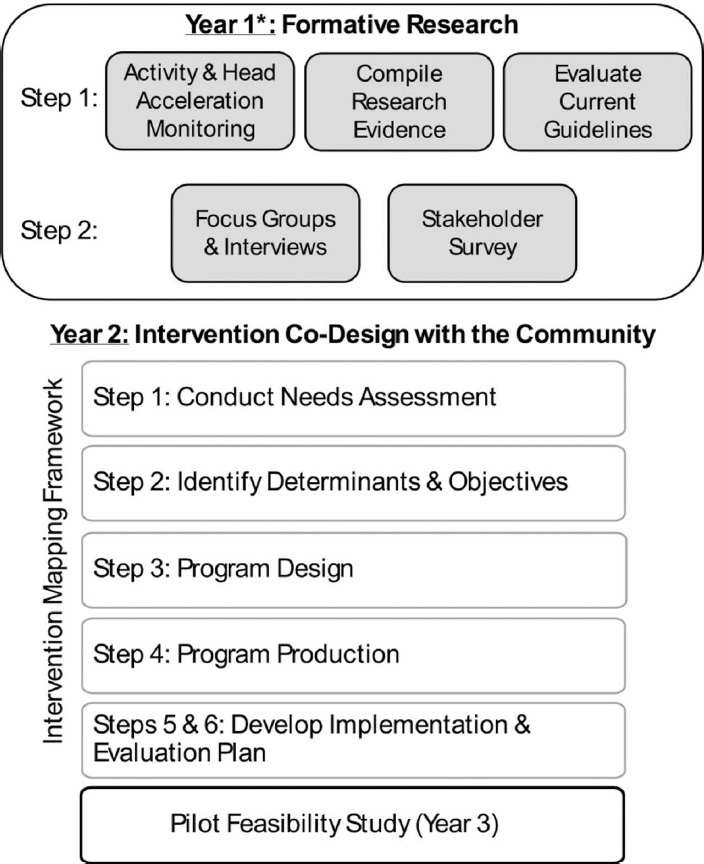
NOTE: *Several years of observational research assessing on-field activities and head acceleration monitoring in youth football informed the study. This was compiled from prior research evidence.
SOURCE: Presented by Jill Urban, April 16, 2025. From Urban et al., 2024. Used with permission from Elsevier; CC BY-NC-ND 4.0.
Pilot Testing and Early Outcomes
The COACH program was pilot tested with four youth football teams. While implementation fidelity varied—from full adherence to one instance where assistant coaches resisted the shift away from aggressive contact—preliminary data indicate that teams that closely followed the intervention experienced fewer head acceleration event rates, Urban said. In contrast, control teams had more live-contact drills and recorded higher RHI exposure.
Urban emphasized that the program’s success depended on trust, long-term relationships, and sustained community involvement. She concluded that community engagement offers a powerful model for designing evidence-based injury prevention strategies that are both practical and widely supported. A stepped-wedge evaluation5 is underway to assess broader implementation and effectiveness.6
Shared Decision Making About Return to Activity
Emily Kroshus-Havril, a professor in pediatrics at the University of Washington School of Medicine and a principal investigator at Seattle Children’s Research Institute Center for Child Health, Behavior, and Development, examined shared decision making (SDM) as a model that can support high-quality decisions about returning to activity after concussion recovery.
SDM Frameworks: Opportunities and Challenges for Dyadic Decision Making
Kroshus-Havril discussed the uncertainty that families face when making return-to-play decisions following pediatric concussion, especially given the evolving and incomplete evidence on the risks of RHI. While prevention through policy change and reduced exposure remains essential, Kroshus-Havril emphasized that families will continue to face individual decisions—both because not all risks can be eliminated, and because different communities and families operate within different constraints and values. The central question, Kroshus-Havril suggested, is not only whether it’s safe to return—but how to define a “good” decision in these situations, and how to support families in making one.
___________________
5 A stepped-wedge evaluation is a controlled randomized trial where a new intervention is implemented across naturally occurring clusters, such as schools or hospitals. See https://jamanetwork.com/journals/jamainternalmedicine/article-abstract/2831201 (accessed September 26, 2025).
6 See https://clinicaltrials.gov/study/NCT06624202 (accessed September 2, 2025).
SDM was offered as a promising framework for facilitating decisions in this context. SDM is designed for cases in which multiple medically reasonable options exist and the best path forward depends on individual preferences and values. Models like the Ottawa Decision Support Framework emphasize that a good decision is not just informed, but it is also value aligned and made through a process that addresses individual decision-making needs—such as adequate knowledge, emotional readiness, or support for deliberation without pressure (Légaré et al., 2006; Stacey et al., 2020).
However, existing SDM frameworks typically presume a single decision maker, or a parent proxy for young children. This structure fails to account for the dyadic nature of decisions for adolescents considering a return to sports. While adolescents are still minors, ethical frameworks and professional guidelines, including from the American Academy of Pediatrics, support involving them in decisions that affect their health (Katz et al., 2016; Salter et al., 2023).
Kroshus-Havil highlighted several challenges that current SDM frameworks do not fully address in this context. Adolescents and parents may differ in their health literacy, understanding of risk, or priorities. The parent–adolescent dynamic can itself introduce pressure, limiting open reflection. Even when information needs are met and values are clarified, families may still disagree—raising the unresolved question of whose preference should ultimately guide the decision.
Parental and Adolescent Perspectives on Dyadic Decision Making
To explore these dynamics, Kroshus-Havril’s research team conducted individual interviews with adolescents recovering from sports-related concussions and their parents, asking about experiences with return-to-play decisions. Adolescents often focused on the benefits of returning to play and showed limited interest in learning about risks—not because they thought risks did not exist, but because they assumed their parents were asking the right questions and would intervene if something was not safe, she said. At the same time, parents commonly relied on clinicians or informal research and were not always aware of the uncertain and evolving evidence base. Some deliberately withheld detailed risk information to avoid discouraging their teen. Teens prioritized short-term goals, like rejoining their team, while parents often assumed they understood their child’s values without probing more deeply. In many families—especially those involved in early sport specialization—youth sports were deeply embedded in routines and social life. Stepping back could feel like a loss not only for the athlete, but for the entire family.
Teens generally viewed themselves as the decision makers, and parents often deferred to their child’s preference to return as long as the clinician
said it was safe. Many families described weighing risks and benefits but often felt there were few realistic alternatives. Teens with narrow, sport-based identities found it harder to adjust; those with broader interests were more open to reconsidering their sport involvement, Kroshus-Havril reported. Some families adopted a strategy of “planning for the next one”—agreeing it was okay to return now, but that another concussion might lead to a different decision. This helped parents feel they were setting guardrails, while teens were comfortable with the plan because it did not feel real or immediate—they did not think another concussion would happen.
Clinician Perspectives on Dyadic Decision Making
Kroshus-Havril’s team also conducted qualitative interviews with pediatric sports medicine specialists to understand how clinicians navigate these dyadic considerations (Kroshus-Havril et al., 2022). Clinicians used a range of strategies to elicit and elevate athlete preferences. This included speaking separately with adolescents so they could be candid, or using indirect cues to gauge their enthusiasm about returning to sport. Clinicians also recognized that a young person’s preferences might reflect a narrow sport-based identity, shaped by early specialization or family culture. While these preferences were respected, clinicians also saw opportunities to support youth in imagining alternative paths. When discordance arose between teens and parents, clinicians used mediation strategies—such as clarifying reasons for disagreement, sharing information, and emphasizing shared values like adolescent well-being.
Importantly, when athlete preferences were deemed medically reasonable, clinicians generally tried to elevate those preferences. Often this meant supporting return to play, but in cases where adolescents expressed burnout or a desire to change sports, clinicians aligned their recommendations with the athlete’s stated goals.
Valued Action—An SDM Intervention
To support higher-quality decisions, Kroshus-Havril’s team developed Valued Action, a web-based SDM intervention tailored to postconcussion return-to-sport decisions. The tool allows parents and teens to separately learn key facts, reflect on their values, and consider aligned activities. Some responses are piped into a family conversation guide that highlights areas of agreement and discordance, and a summary is shared with clinicians to support a more productive discussion during the clinical encounter. The tool also incorporates brief assessments of adolescent burnout, anxiety, and depression, and helps families prepare questions for their provider (Figure 4-2).
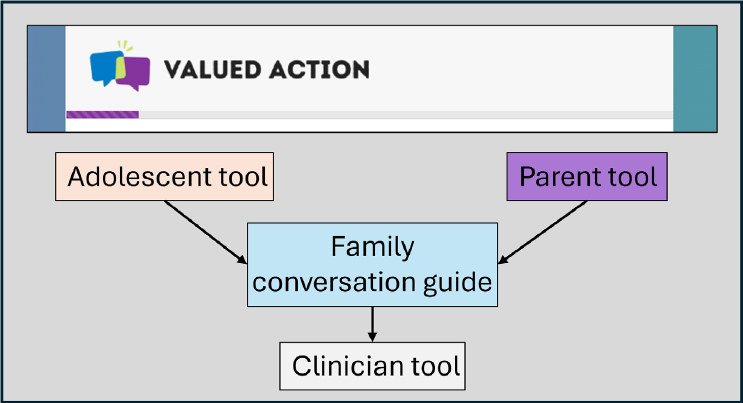
SOURCE: Presented by Emily Kroshus-Havril on April 16, 2025.
Kroshus-Havril concluded by emphasizing that return-to-play decisions are not just medical—they unfold within interpersonal, emotional, and cultural contexts. Tools that help families reflect on what matters, explore viable alternatives, and navigate disagreement are essential to supporting good decisions.
Discussion
Master moderated a dynamic discussion exploring how readiness for change, parental values, and practical fairness, access and equity considerations shape the implementation of safety interventions for youth at risk for RHI exposure. Urban and Kroshus-Havril shared insights from their research and practice on translating emerging evidence into meaningful community change.
Readiness for Change
In response to a question from Donald Berwick, Institute for Healthcare Improvement, about coaches’ readiness for change as evidence emerges and evolves, Urban shared that in youth football, there is a clear appetite for improving safety among coaches, parents, and organizational leaders. However, she noted a misalignment between perceptions of safety and what safety improvements actually entail. Urban emphasized that researchers
are not always the most effective messengers for delivering safety information. Instead, the codeveloped intervention COACH relies on high school coaches to disseminate safety strategies and influence youth programs. This peer-to-peer model builds on a culture shift observed among high school coaches who increasingly recognize that player health is essential for team competitiveness, she said. Urban suggested that reframing safety as beneficial for performance can help build buy-in and that identifying trusted messengers is key.
Assessing Organization Readiness for Change
Master asked about variability in intervention uptake across youth teams and how to assess whether a group is ready to adopt safety practices. Urban described using a validated measure called Organizational Readiness for Implementing Change (ORIC) (Shea et al., 2014). She added that youth sports organizations are often run by volunteers and lack the infrastructure needed to support injury prevention efforts. To address this, Urban’s team has begun using preimplementation science frameworks—specifically PRISM (Practical, Robust Implementation and Sustainability Model) (Feldstein and Glasgow, 2008)—to evaluate organizational capacity before introducing interventions. She emphasized that if basic operational structures are missing, the timing may not be right to introduce safety programs, regardless of their potential value.
Shared Decision Making to Clarify Values
Turning to the individual level, Master asked Kroshus-Havril whether decision-support tools help families navigate competing values around sport participation. Kroshus-Havril responded that while she could not provide specific data from her research, there is a broader pattern of parenting-related anxiety in the United States that extends into youth sports. Many parents want to do what is best for their child but also seek external validation through sport-related milestones, such as making a travel team or advancing to the next level, she said. This can create internal tensions between stated priorities (e.g., fun, health, personal growth) and less visible goals rooted in anxiety and social comparison. To that end, Kroshus-Havril added that in developing mental health interventions for youth athletes, her team was prompted by athlete feedback to pivot toward creating supports for parents to address parental anxiety. While shared decision-making tools can help parents pause and reflect on their priorities, Kroshus-Havril emphasized that they are not sufficient on their own.
Access and Inclusion Considerations
Master asked both panelists to consider how their work can ensure fair access to relevant information and safer options “to make sure that it’s accessible to all of our athletes and their families and in different sports and different communities.” Kroshus-Havril responded by noting that structural inequities can constrain choice, and access to safer options—such as flag football instead of tackle—may correlate with community socioeconomic status. She expressed concern about overrelying on individual decision making in contexts where options are not equitably distributed. Additionally, she noted that clinical decision making can be influenced by assumptions about an athlete’s potential or academic ability, which may introduce bias. To address this, Kroshus-Havril emphasized the importance of community-level approaches “so everyone has safe options” and the need for universal decision-support tools to minimize potential provider bias and create fair and inclusive processes.
Urban added that involving a wide range of stakeholders in decision making is one way to address challenges. She noted that different communities and organizations will have varying needs, and interventions must be flexible enough to accommodate those realities. By involving stakeholders in the process, implementers can identify what supports are needed and tailor programs to better fit the local context.
Closing Thoughts
In closing, Master shared comments from the audience underscoring the need to employ multiple societal levers—from broadscale education to policy change—to reach all communities, promote awareness, and ensure families have access to trustworthy information amid an increasingly fragmented media environment. Master highlighted the importance of continued federal investment in this area, especially given historical underfunding of pediatric research relative to adult-focused studies. She urged funders and decision makers to recognize children as a central part of the solution space and to support efforts that translate emerging research into practical, community-relevant tools. These actions, she noted, are essential for ensuring the health and safety of all young athletes and moving the field forward.
REFERENCES
Bruder A. M., B. E. Patterson, K. M. Crossley, A. B. Mosler, M. J. Haberfield, M. Hägglund, A. G. Culvenor, S. M. Cowan, and A. Donaldson. 2024. If we build it together, will they use it? A mixed-methods study evaluating the implementation of Prep-to-Play PRO: An injury prevention programme for women’s elite Australian football. British Journal of Sports Medicine 58(4):213-221.
Delgadillo, B. E., F. Montz, B. Ward Jr., A. B. Herson, and J. P. Toldi. 2025. Current evidence for the use of jugular vein compression collars in sport: A systematic review. Current Sports Medicine Reports 24(1):18-27.
Dorman, J. C., D. N. Poel, V. D. Valentine, and T. A. Munce. 2022. Head impact exposure of a youth football team over eight consecutive seasons. Medicine & Science in Sports & Exercise 54(1):3-11.
Emery, C. A., P. Eliason, J. M. Galarneau, V. Warriyar, L. Palacios-Derflingher, A. M. Black, M. Krolikowski, N. Spencer, S. Sick, S. Kozak, and K. J. Schneider. 2022. Body checking in non-elite adolescent ice hockey leagues: It is never too late for policy change aiming to protect the health of adolescents. British Journal of Sports Medicine, 56(1):12-18.
Feldstein, A. C., and R. E. Glasgow. 2008. A Practical, Robust Implementation and Sustainability Model (PRISM) for integrating research findings into practice. Joint Commission Journal on Quality and Patient Safety 34(4):228-243.
Heming, E., A. Kolstad, B. Dennett, S. West, and C. Emery. 2024. 806 BO34 – Ice-cold truths: Comparing rates of bodychecking, head contacts, and suspected injuries across adolescent ice-sports. British Journal of Sports Medicine 58(Suppl 1):A63.
Kaminski, T. W., G. T. Chiampas, M. Putukian, D. Kirkendall, J. Fokas, and A. P. Kontos. 2020. Purposeful heading in U.S. youth soccer players: Results from the U.S. soccer online heading survey—Epidemiological evidence: Original survey research. Science and Medicine in Football 4(2):93-100.
Katz, A. L., S. A. Webb, Committee on Bioethics, R. C. Macauley, M. R. Mercurio, M. R. Moon, A. L. Okun, D. J. Opel, and M. B. Statter. 2016. Informed consent in decision-making in pediatric practice. Pediatrics 138(2):e20161485.
Kolstad, A. T., M. Chin, G. Martinez, L. Janzen, M. Krolikowski, C. Goulet, L. Nadeau, B. E. Hagel, and C. A. Emery. 2022. Evaluating the effect of policy prohibiting body checking on physical contacts in U15 and U18 youth ice hockey leagues. Clinical Journal of Sport Medicine 32(6):e614-e619.
Kroshus-Havril, E., Z. Y. Kerr, and J. G. L. Lee. 2017. Community-level inequalities in concussion education of youth football coaches. American Journal of Preventive Medicine 52(4):476-482.
Kroshus-Havril, E., D. J. Opel, T. M. Jinguji, M. K. Steiner, K. Senturia, J. P. MacDonald, C. L. Master, C. C. Giza, M. S. Burton, C. Quitiquit, and B. J. Krabak. 2022. Shared decision-making about returning to sport after recovery from pediatric concussion: Clinician perspectives. Clinical Journal of Sport Medicine 32(2):97-110.
Kroshus-Havril, E., S. P. Chrisman, A. Glang, T. Hunt, R. Hays, S. Lowry, A. Peterson, K. Garrett, D. Ramshaw, K. Hafferty, and E. Kinney. 2023. Concussion education for youth athletes using pre-game safety huddles: A cluster-randomised controlled trial. Injury Prevention 29(1):22-28.
Kroshus-Havril, E., S. P. D. Chrisman, T. Hunt, R. Hays, K. Garrett, A. Peterson, F. P. Rivara, G. Chiampas, B. D. Ramshaw, and A. Glang. 2024. Stakeholder-engaged development of a theory-driven, feasible, and acceptable approach to concussion education. Health Education & Behavior 51(2):197-203.
Lalji, R., H. Snider, N. Chow, and S. Howitt. 2020. The 2015 US Soccer Federation header ban and its effect on emergency room concussion rates in soccer players aged 10–13. Journal of the Canadian Chiropractic Association 64(3):187.
Légaré, F., A. M. O’Connor, I. D. Graham, G. A. Wells, and S. Tremblay. 2006. Impact of the Ottawa Decision Support Framework on the agreement and the difference between patients’ and physicians’ decisional conflict. Medical Decision Making 26(4):373-390.
Oliva-Lozano, J. M., C. D. Gómez-Carmona, J. M. Muyor, G. T. Chiampas, B. Pauwels, and R. Cost. 2024. Potential effects of soccer ball characteristics on ball-to-head contact: A systematic review. Journal of Functional Morphology and Kinesiology 9(4):210.
Rhodes, S. D., A. E. Tanner, L. Mann-Jackson, J. Alonzo, F. M. Siman, E. Y. Song, J. Bell, M. B. Irby, A. T. Vissman, and R. E. Aronson. 2018. Promoting community and population health in public health and medicine: A stepwise guide to initiating and conducting community-engaged research. Journal of Health Disparities Research and Practice 11(3):16-31.
Rizzone, K. H., M. Agnew, S. A. Kliethermes, M. N. Arthur, M. Burton, C. Day, C. Nicholson, J. Ray, N. Stern, J. A. Drezner, E. Kroshus, and C. Blauwet. 2025. Methodology for promoting equity-informed research in sport and exercise medicine: Recommendations from the AMSSM collaborative research network. British Journal of Sports Medicine 59(4):272-282.
Salter, E. K., D. M. Hester, L. Vinarcsik, A. H. Matheny Antommaria, J. Bester, J. Blustein, E. Wright Clayton, D. S. Diekema, A. S. Iltis, L. M. Kopelman, and J. R. Malone. 2023. Pediatric decision making: Consensus recommendations. Pediatrics 152(3):e2023061832.
Shea, C. M., S. R. Jacobs, D. A. Esserman, K. Bruce, and B. J. Weiner. 2014. Organizational readiness for implementing change: A psychometric assessment of a new measure. Implementation Science 9(1):7.
Stacey, D., F. Légaré, L. Boland, K. B. Lewis, M. Loiselle, L. Hoefel, M. Garvelink, and A. O’Connor. 2020. 20th Anniversary Ottawa Decision Support Framework: Part 3 overview of systematic reviews and updated framework. Medical Decision Making 40(3):379-398.
Strauss, B. 2015. U.S. Soccer, resolving lawsuit, will limit headers for youth players. New York Times. https://www.nytimes.com/2015/11/10/sports/soccer/us-soccer-resolving-lawsuitwill-limit-headers-for-youth-players.html (accessed September 4, 2025).
Sullivan, G. R., E. A. Lin, A. Hoffer, M. Richardson, and A. Chhabra. 2024. Pediatric concussion injuries in soccer: Emergency department trends in the United States from 2012 to 2023. Orthopaedic Journal of Sports Medicine 12(12).
Swartz, E. E., J. L. Myers, S. B. Cook, K. M. Guskiewicz, M. S. Ferrara, R. C. Cantu, H. Chang, and S. P. Broglio. 2019. A helmetless-tackling intervention in American football for decreasing head impact exposure: A randomized controlled trial. Journal of Science and Medicine in Sport 22(10):1102-1107.
Swartz, E. E., J. K. Register-Mihalik, S. P. Broglio, J. P. Mihalik, J. L. Myers, K. M. Guskiewicz, J. Bailes, M. Hoge, and National Athletic Trainers’ Association. 2022. Position statement: Reducing intentional head-first contact behavior in American football players. Journal of Athletic Training 57(2):113-124.
Swartz, E. E., J. L. Myers, J. S. Lee, S. P. Broglio, T. Furutani, R. Oshiro, G. A. Gioia, D. Brothers, K. Glodowski, I. Lloansi, and L. Meyer. 2024. Head impact exposure in Hawaiian high school football: Influence of adherence rates on a helmetless tackling and blocking training intervention. Journal of Athletic Training 60(6):458-467.
Urban, J. E., J. B. Moore, M. E. Marks, T. D. Holcomb, R. Patterson, A. McCoy, C. M. Miles, J. D. Stitzel, and K. L. Foley. 2024. Protocol for COACH, an evidence-based intervention for improved head impact safety in youth American football developed using a community-engaged approach. Contemporary Clinical Trials Communications 42:101371.
Urban, J. E., K. D. Wiseman, J. B. Moore, M. E. Marks, T. D. Holcomb, B. B. Lazzara, C. M. Miles, L. A. Flashman, J. D. Stitzel, and K. L. Foley. 2025. Implementing injury prevention strategies in community-based youth football: The role of parents, coaches, and organizational leaders. PLOS ONE 20(5):e0322373.
Williamson, R. A., A. T. Kolstad, L. Nadeau, C. Goulet, B. Hagel, and C. A. Emery. 2022. Does increasing the severity of penalties assessed in association with the “zero tolerance for head contact” policy translate to a reduction in head impact rates in youth ice hockey? Clinical Journal of Sport Medicine 32(6):e598-e604.
This page intentionally left blank.





















