Mental Health, Suicide Prevention, and Addiction Mitigation in Construction and Maintenance (2026)
Chapter: 2 Literature Review

CHAPTER 2
Literature Review
Introduction
The global construction sector is valued at $16.6 trillion, with the United States contributing $1.36 trillion—approximately 6.3% of its gross domestic product (GDP) (Best 2021b; Business Wire 2021). This sector not only supports housing, transportation, and energy but also drives employment and economic growth (Blake et al. 2023). In the United States, over 733,000 employers support a workforce of seven million employees, who deliver nearly $1.4 trillion in building and infrastructure projects annually (AGC 2021). Safety has long been a concern in this labor-intensive industry, with fatal injuries affecting at least one in 10 workers on job sites (BLS 2019). From 2011 to 2022, fatalities rose by nearly 40%, reaching 1,092 deaths in 2022 alone (Trueblood et al. 2024). A survey by 360training (2019) found that one in four workers feared daily injury, especially from falls, electrical hazards, and struck-by incident risks that are often encountered on transportation projects managed by state DOTs.
Beyond physical safety, worker wellbeing, including mental health, has gained attention in recent years. The CDC (2018b) defines wellbeing as a meaningful indicator of how people perceive their lives, encompassing both physical and mental health dimensions. Mental wellbeing affects energy, emotional resilience, and daily function (Australian National University 2020; SAMHSA 2020). Promoting wellbeing can enhance productivity, reduce illness, and increase longevity (CDC 2018b), all of which are critical for sustaining a healthy workforce on long-term infrastructure projects.
Although physical safety has been the traditional focus, mental health among construction workers demands urgent attention. Lorek (2021) reported that 83% of construction workers experience mental health issues, yet these concerns are often underrepresented in research and policy (Deacon et al. 2005; Eaves et al. 2016; Valsangkar and Sai 2012). As one safety executive noted, “Mental health not only affects our wellbeing, but impacts how we make choices, handle stress, and relate to others, both on and off the job site” (Themanson 2021).
Mental health concerns such as stress, anxiety, suicidal ideation, and substance misuse are often influenced by socioeconomic conditions and domestic stressors. These issues are especially relevant to DOTs, which manage large-scale, high-pressure projects with workforce populations vulnerable to such risks. This research focuses on identifying mental health indicators and the factors driving them, with the goal of informing more holistic workforce support in the transportation and construction industry.
Mental Health Issues
In the United States, there is a growing epidemic of poor mental health, with an increasing number of young adults experiencing at least one mental health condition (Mental Health
America 2021). According to the CDC (2021), approximately half of the population is expected to experience and be diagnosed with a mental health condition at some point in their lives. Currently, around 40% of the population is dealing with significant mental health concerns that require clinical attention (CDC 2021). The National Institutes of Health (NIH 2021) categorizes mental health conditions under 12 major themes: mental illness, autism spectrum disorder, major depression, post-traumatic stress disorder (PTSD), anxiety disorders, bipolar disorder, obsessive-compulsive disorder (OCD), schizophrenia, attention-deficit/hyperactivity disorder (ADHD), eating disorders, personality disorders, and suicide. These conditions collectively impose a substantial burden on the U.S. economy, amounting to $193.2 billion annually in lost earnings and productivity (NAMI 2021).
Compounding the issue, many individuals with mental health conditions face stigma and discrimination, which often discourages them from seeking help (WHO 2021). The American Psychiatric Association (APA 2020) reports that nearly half of those experiencing mental health issues do not seek assistance due to stigma, which it categorizes into three types: public (negative societal attitudes), self (internalized shame), and institutional (systemic barriers to accessing care). These forms of stigma can result in isolation, reduced social opportunities, avoidance of treatment, insurance gaps, and loss of confidence. In the construction industry, where stoicism and toughness are often culturally reinforced, stigma surrounding mental health discussions may be even more pronounced, preventing workers from seeking the help they need. As such, strong peer and organizational support systems are critical for addressing mental health in the construction workforce (Eyllon et al. 2020).
Understanding the scope of mental health issues in the U.S. construction sector is essential. Currently, about 83% of construction workers report experiencing at least one mental health issue (Lorek 2021). The industry has one of the highest suicide rates in the country, particularly among middle-aged white men, who represent a large portion of its workforce (Relojo-Howell 2020). The CDC (2018a) reports 53.2 suicides per 100,000 construction workers annually, four times the national average and higher than all other causes of construction-related fatalities combined. Additionally, opioid addiction is a growing concern within the industry, further elevating suicide risks and exacerbating mental health struggles (Relojo-Howell 2020). A NIOSH (2020) study also found high rates of tobacco use, binge drinking, limited downtime, and general substance misuse among both workers and managers.
Mental Health Issues in the Construction Sector
The major construction trades in the United States include general laborers, carpenters, electricians, construction supervisors, plumbers, painters, HVAC (heating, ventilation, and air conditioning) workers, roofers, drywallers, concrete workers, flooring workers, and steel workers (DataUSA 2019). Trade workers, who form the backbone of many infrastructure and transportation projects—including those administered by DOTs—face both work- and non-work-related stressors that may increase their risk of poor mental health (Haynie 2021).
Compared to other construction workers, trade workers are more likely to work long and irregular hours and to travel extensively for project-based assignments, often spending prolonged periods away from family. Employment is frequently project-based and short-term, leading to precarious work arrangements. During economic downturns, these workers are often among the first to lose employment. Such stressors contribute significantly to poor mental health outcomes among trade workers (Haynie 2021).
Despite the clear risks, there is limited research focused specifically on mental health among construction trade workers. One major study by Boal et al. (2020), involving 25,842 workers, identified five prevalent behavioral risk factors: smoking, tobacco use, lack of physical activity,
binge drinking, and not wearing seatbelts. These behaviors were especially common among carpenters, laborers, and roofers. Roofers and electricians were frequently observed engaging in binge drinking, and equipment operators exhibited high rates of smoking (Boal et al. 2020; NIOSH 2020). This remains one of the most comprehensive U.S. studies in this area. In another study covering the broader construction trades, Ompad et al. (2019) found higher rates of marijuana, cocaine, and nonprescription opioid use among trade workers. Substance misuse, particularly opioid abuse, is a critical mental health concern in the construction industry.
Opioid misuse surged in the late 1990s due to overprescription, giving rise to what is now known as the opioid epidemic. Trades such as bricklaying, carpentry, and labor-intensive roles, which are prevalent on DOT projects, are associated with musculoskeletal injuries, often leading to opioid prescriptions and subsequent misuse of drugs like fentanyl, oxycodone, morphine, and heroin (Monga 2021).
Binge drinking is another issue, affecting approximately 16.5% of construction workers (SAMHSA 2016). Roofers, painters, laborers, carpenters, and concrete finishers are particularly vulnerable (Lubin and Giang 2011). Excessive smoking is also prevalent—construction workers reportedly smoke an average of six cigarettes per workday, resulting in a 15.2% loss in productivity (Yung and Agyekum-Mensah 2012). In a survey of 1,817 trade workers, factors such as age, race, ethnicity, income, education, and health status were linked to smoking habits. Ironworkers were the most affected, followed by equipment operators, electricians, bricklayers, and painters. Moreover, suicide rates are alarmingly high among specific trades. Steel workers, masons, and roofers rank highest in suicide rates (Peterson et al. 2020). According to Sanati (2009), suicide is often associated with underlying medical or psychiatric conditions, underscoring the urgency of addressing mental health concerns early.
Mental Health Indicators
Various mental health indicators provide insight into the status and severity of mental health concerns. According to the Mayo Clinic (2021), signs of deteriorating mental health include persistent sadness; reduced concentration; frequent confusion; excessive fear, worry, or guilt; social withdrawal; sudden mood changes; chronic low energy; insomnia; delusions; paranoia; hallucinations; difficulty handling stress; feelings of alienation; disordered eating; changes in libido; excessive anger or aggression; and suicidal thoughts. The National Alliance on Mental Illness (NAMI) echoed many of these indicators and further noted the presence of physical symptoms such as headaches, stomach pain, or other persistent ailments (NAMI 2015).
These findings underscore that mental health issues present not only as psychological or emotional symptoms but often include physical manifestations. One study (Omohundro 2018) considered several of these indicators, including depressive episodes, in its analysis of mental health data collected in Tennessee. Additionally, Wilkinson et al. (2008) identified self-harm as a distinct and critical indicator of mental health deterioration.
These indicators can be generally classified into two categories: activity based and thought or emotion based. Activity-based indicators include physical symptoms such as headaches, stomachaches, and fatigue. Thought- or emotion-based indicators include emotional distress such as sadness, difficulty concentrating, insomnia, and mood swings.
The root causes or stressors behind these indicators can also be grouped into the following four major categories (Gurin and Goleman 1993; Slavich 2020):
- Physical stress (e.g., musculoskeletal strain, physical labor, trauma, radiation exposure);
- Psychological stress (e.g., cognitive overload, emotional trauma, self-loathing);
- Psychosocial stress (e.g., interpersonal conflict, financial instability, lack of social support); and
- Psycho-spiritual stress (e.g., lack of purpose, job dissatisfaction, existential distress).
In physically demanding environments such as those encountered by construction personnel employed by or contracted to DOTs, these stressors may be particularly pronounced. DOT projects often involve long hours, remote locations, and rigid timelines, all of which may amplify stress and negatively impact workersʼ mental health. Although there may be some overlap between these categories, psychosocial and psycho-spiritual stressors are frequently cited as key contributors to the onset of the mental health issues outlined here. These will be further explored in the following section.
Mental Health Stressors
There are key socioeconomic determinants that influence mental health outcomes. Mckenzie et al. (2014) identified four primary socioeconomic factors: labor force status, annual household income, individual deprivation, and area deprivation. Similarly, Meyer et al. (2014) highlighted socioeconomic status, neighborhood safety, age, and physical activity as influential drivers of mental health. Their findings indicated that although socioeconomic status, age, and physical activity were positively associated with mental wellbeing, perceptions of inadequate neighborhood safety had a negative effect. The Mental Health Commission of Canada (2015) developed a mental health dashboard that provides a broader societal perspective, incorporating factors such as access to mental healthcare, caregiving responsibilities, youth awareness, economic prosperity, housing and homelessness, population wellbeing, recovery supports, and stigma reduction.
Other studies have further elaborated on socioeconomic-related stressors, including sociodemographic factors (e.g., age, education, and employment status), social and financial support systems, access to public welfare services (e.g., insurance and health programs), and conditions in the labor market such as job insecurity and unemployment (European Union 1998; Ruiz-Pérez et al. 2017). For instance, an individual facing financial hardship and lacking social support may be compelled to take on multiple jobs. This can lead to cognitive fatigue and, over time, escalate into more severe mental health conditions.
In the context of the construction industry, Chan et al. (2020) ranked 32 factors that influence workersʼ mental health. The top eight were the following:
- Job demands,
- Job control,
- Family responsibilities,
- Welfare and socioeconomic conditions,
- Exposure to work-related hazards,
- Coping mechanisms (or lack thereof),
- Workplace support (or lack thereof), and
- Workplace injustice.
Tijani et al. (2020) provided a more detailed classification of mental health risk factors, grouping them into organizational, task-related, personal, physical, and gender-related categories. Their findings are summarized in Table 1.
Tijani et al. (2020) also emphasized the need for further research in order to better understand gender-related factors, which this review addresses in later sections. In a separate study, Fordjour and Chan (2019) categorized psychological health indicators specific to the construction industry into four domains, as shown in Table 2.

Long Description.
The column headers of the table are Category and Factors. The data given in the table row-wise are as follows: Row 1: Organizational: Home–work conflict, lack of career guidance, poor organizational support, inadequate structure, unfair treatment. Row 2: Task-related: Project overload, role ambiguity, tight deadlines, long hours, unpredictable schedules. Row 3: Personal: Poor workplace relationships, perfectionist behavior, conflict with supervisors, harassment, and language barriers. Row 4: Physical: Unsafe environments, lack of protective equipment, poor transportation, injuries, inadequate medical services. Row 5: Gender-related: Inequality, sexual harassment, and limited career opportunities for women.
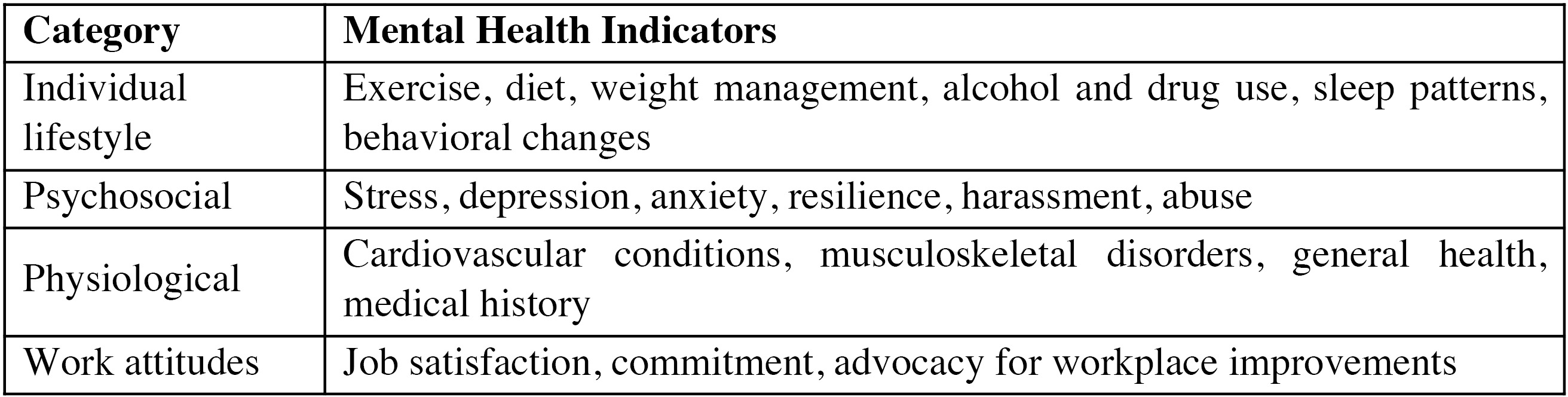
Long Description.
The column headers of the table are Category and Mental Health Indicators. The data given in the table row-wise are as follows: Row 1: Individual Lifestyle: Exercise, diet, weight management, alcohol and drug use, sleep patterns, behavioral changes. Row 2: Psychosocial: Stress, depression, anxiety, resilience, harassment, abuse. Row 3: Physiological: Cardiovascular conditions, musculoskeletal disorders, general health, medical history. Row 4: Work attitudes: Job satisfaction, commitment, advocacy for workplace improvements.
Consistent with earlier findings, Chan et al. (2020) reaffirmed that job demands, job control, family pressures, socioeconomic status, and work hazard exposure are among the most significant factors influencing mental health in the construction sector. Collectively, the research suggests that organizational and job-related conditions are the most dominant influences, followed by socioeconomic stressors. Understanding these factors is critical to assessing the mental health landscape in the construction industry, especially in high-risk, labor-intensive sectors—including transportation infrastructure. The following section explores tools and frameworks used globally to assess mental health status and outcomes.
Physical and Job-Related Demands
Construction work is characterized by intense physical demands, including long hours, repetitive heavy lifting, and frequent exposure to unsafe or extreme conditions. These factors often lead to chronic pain, fatigue, and physical injuries, which are closely associated with mental health issues (Jia et al. 2016; Karthick et al. 2022; Oswald et al. 2019; Turner and Lingard 2020). For example, chronic pain resulting from work-related injuries is strongly correlated with increased stress and anxiety among construction workers (Oswald et al. 2019; Turner and Lingard 2020). Additionally, the persistent threat of severe injuries or fatalities contributes to a high-stress work environment, further compounded by the lack of adequate mental health support (Oswald et al. 2019). Prolonged exposure to such conditions underscores the critical need to address the link between physical strain and mental health in the construction industry.
Financial Challenges
Job insecurity presents another major stressor in the construction sector. As a result of the project-based nature of construction employment, many workers experience unstable income and limited access to long-term benefits. This financial instability is particularly pronounced
among lower-skilled laborers, who often lack the resources necessary to maintain or improve their mental wellbeing (Construction Industry Council 2023). Greiner et al. (2022) found that financial insecurity significantly increases anxiety levels and discourages investment in self-care or mental health resources because of affordability concerns. Furthermore, the transient nature of construction work frequently disrupts work–life balance, exacerbating mental health stressors linked to career unpredictability (Construction Industry Council 2023; Greiner et al. 2022).
Social and Cultural Challenges
Every industry develops a unique culture shaped by its values, practices, and goals (Aurelius et al. 2024). In construction, a deeply rooted “macho” culture often discourages open conversations about mental health, fostering stigma and associating vulnerability with weakness (Nwaogu et al. 2022). This cultural pressure, particularly impactful among the male-dominated workforce, frequently inhibits help-seeking behaviors, intensifying conditions such as depression, anxiety, and substance abuse (Blake et al. 2023). As a result, stigma significantly undermines the reach and impact of mental health programs, deterring participation and limiting access to essential support (Nwaogu et al. 2022).
Team dynamics on construction sites are also strained by hierarchical structures and high-pressure environments, which can lead to interpersonal conflicts, bullying, and harassment—factors known to worsen mental health outcomes (Blake et al. 2023; Nwaogu et al. 2022; Oswald et al. 2019). Nwaogu et al. (2022) emphasize that poor workplace relationships and harassment are widespread contributors to psychological stress, highlighting the need for strategies that foster respectful, supportive work environments.
Mental Health Assessment
Mental health assessment is a structured process used to evaluate an individualʼs psychological and emotional wellbeing. When conducted by a licensed mental health professional, this assessment can aid in diagnosing mental health disorders and identifying appropriate treatment options (Rainey 2018; Romito et al. 2017). According to Mercy Health (2021), common indicators assessed include anxiety, confusion, apathy, and changes in sleep and mood. Comprehensive assessments may also involve physical examinations, laboratory tests, mental health history, personal history, and cognitive evaluations (Rainey 2018).
In addition to identifying the presence of a mental health condition, it is critical to assess its severity. Zimmerman et al. (2018) recommend using standardized tools such as the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (also known as the DSM-5) for this purpose. However, one key challenge in conducting mental health assessments for specific population groups, such as those within the construction industry, is the heterogeneity of the population. Inconsistencies in demographic characteristics can hinder diagnostic accuracy (Newson et al. 2020). Therefore, ensuring a sufficiently representative sample is essential for generating reliable and generalizable findings.
In the Netherlands, a large-scale mental health assessment was conducted among 1,500 bricklayers using the Dutch Questionnaire on the Experience and Evaluation of Work. Variables such as fatigue, recovery, psychological distress, and PTSD were measured to evaluate the workersʼ mental wellbeing. The findings identified a set of key psychosocial drivers of mental health in this trade group (Boschman et al. 2013).
Chan et al. (2020) conducted a systematic review and validation of tools used to assess mental health in the construction industry. These tools, listed chronologically in Table 3, illustrate the progression of mental health assessment methods over time.
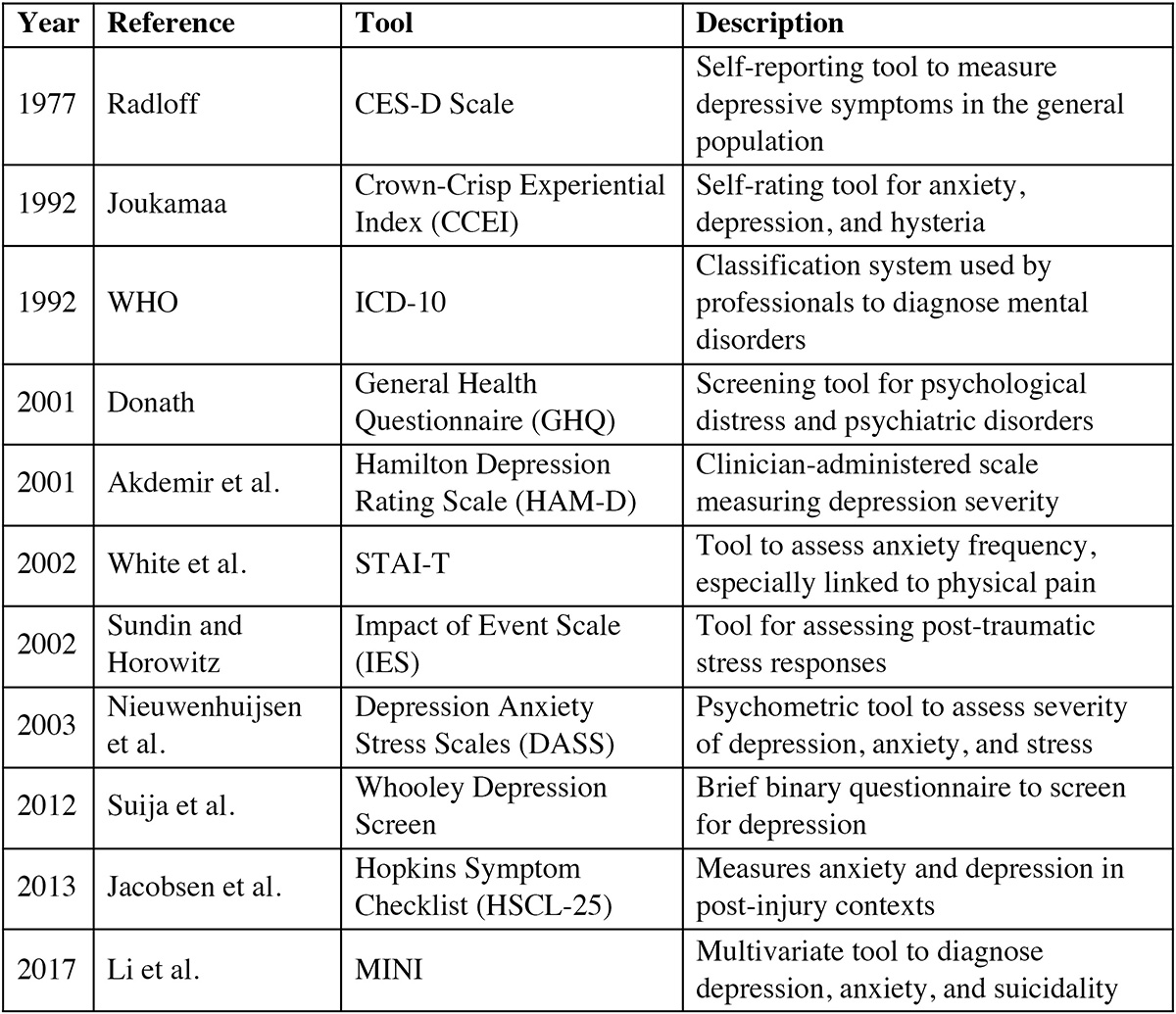
Long Description.
The column headers of the table are Year, Reference, Tool, and Description. The data given in the table row-wise are as follows: Row 1: 1977: Radloff CES-D Scale; Self-reporting tool to measure depressive symptoms in the general population. Row 2: 1992: Joukamaa; Crown-Crisp Experiential Index (CCEI); Self-rating tool for anxiety, depression, and hysteria. Row 3: 1992: WHO: ICD-10; Classification system used by professionals to diagnose mental disorders. Row 4: 2001: Donath; General Health Questionnaire (GHQ); Screening tool for psychological distress and psychiatric disorders. Row 5: 2001: Akdemir et al.: Hamilton Depression Rating Scale (HAM-D); Clinician-administered scale measuring depression severity. Row 6: 2002: White et al.; STAI-T; Tool to assess anxiety frequency, especially linked to physical pain. Row 7: 2002: Sundin and Horowitz; Impact of Event Scale (IES); Tool for assessing post-traumatic stress responses. Row 8: 2003: Nieuwenhuijsen et al.; Depression Anxiety Stress Scales (DASS); Psychometric tool to assess severity of depression, anxiety, and stress. Row 9: 2012: Suija et al.; Whooley Depression Screen; Brief binary questionnaire to screen for depression. Row 10: 2013; Jacobsen et al.; Hopkins Symptom Checklist (HSCL-25); Measures anxiety and depression in post-injury contexts. Row 11: 2017: Li et al.; MINI; Multivariate tool to diagnose depression, anxiety, and suicidality.
Despite the availability of these tools, Chan et al. (2020) emphasized the need for improved specificity in assessing mental health in construction settings. Many tools lack the granularity to capture trade-specific, gender-specific, or race- and ethnicity-based variations in mental health conditions.
Emerging technologies offer new opportunities for real-time mental health monitoring. Studies by Jebelli et al. (2018a) and Xing et al. (2019) suggest that wearable devices may help track physiological indicators such as brain electrical activity, electrodermal responses, heart rate variability, and interbeat intervals—offering dynamic, data-driven insights into workersʼ mental states.
Nevertheless, most existing mental health studies in construction have relied on convenience sampling, often overlooking the intersectional dimensions of race, ethnicity, gender, and job roles (Jacobsen et al. 2013; Turner and Lingard 2020). Although these studies underscore the critical importance of mental health in the industry, they fall short in producing accurate and actionable results across diverse worker populations. More importantly, mental health assessment represents just the initial step. Effective interventions and support mechanisms are essential for managing and mitigating mental health challenges in the construction industry. The next section explores these strategies and their implementation.
Workplace-Based Programs
Peer Support
Mental health concerns such as anxiety, stress, and depression are prevalent among construction workers and necessitate effective interventions (Nwaogu et al. 2022). A landmark initiative in mental health intervention within the construction industry is the MATES in Construction
(MIC) program, which was launched in Queensland, Australia, in 2008. Developed to reduce suicide rates and address the stigma surrounding mental health, MIC applies evidence-based suicide prevention principles while fostering a supportive, peer-led environment. The program trains on-site peers to recognize signs of mental distress, encourages open conversations about mental health, and promotes help-seeking behaviors and treatment engagement (Gullestrup et al. 2011; Gullestrup et al. 2023; Martin, Swannell, et al. 2016; MATES 2008). Evidence demonstrates that MIC significantly improves mental health literacy and increases workersʼ willingness to seek support. To further strengthen its impact, Campbell and Gunning (2020) recommend integrating structured group activities such as scheduled discussions and on-site health screenings—in order to provide regular, non-stigmatizing opportunities for engagement. Garbett (2022) supports these enhancements, noting that consistent participation not only reduces stigma but also enables early identification of mental health concerns.
Organizational Policy Change
Beyond peer-led models, other workplace-based interventions focus on shifting organizational culture and policy. Chan et al. (2020) advocated for regular psychosocial risk assessments and the implementation of policies that balance job demands, enhance job control, and support leadership development. Similarly, Blake et al. (2023) highlighted the importance of leadership modeling. When leaders openly address mental health issues, it helps normalize these conversations and fosters a culture of support.
An Integrated Framework of Interventions
Nwaogu et al. (2022) and Newaz et al. (2022) emphasize the need for an integrated mental health framework that includes primary, secondary, and tertiary interventions. These are distinguished by timing, purpose, and delivery method, described as follows:
- Primary interventions are proactive measures designed to identify and mitigate workplace stressors before they lead to mental health issues. Examples include reducing excessive workloads, simplifying job complexity, and limiting shift work (Turner and Lingard 2020). These system-level strategies align with the proactive measures advocated by Nwaogu et al. (2022) and Newaz et al. (2022).
- Secondary interventions target individual workers, aiming to strengthen their resilience and ability to cope with stress. Turner and Lingard (2020) cite programs promoting smoking cessation, healthy eating, and physical exercise as examples. Notably, food insecurity—common on some job sites—can significantly affect mental health, further emphasizing the importance of these individual-level interventions.
- Tertiary interventions focus on treatment and recovery. When proactive and preventive strategies fall short, tertiary interventions provide critical support through counseling, therapy, or medical treatment. Although these interventions are reactive in nature, they remain a vital component of a comprehensive mental health strategy.
Turner and Lingardʼs (2020) integrated approach, although not explicitly labeled as using this framework, nonetheless incorporates elements across all three intervention levels. Their model includes Occupational Safety and Health compliance (primary) and workplace health promotion (secondary), illustrating alignment with the tripartite framework promoted by Nwaogu et al. (2022).
Both research teams underscore the importance of structural strategies such as compressed workweeks, flexible work arrangements, job sculpting, and supportive workplace cultures (Gruttadaro and Beyer 2021; Nwaogu et al. 2022). These strategies promote work–life balance, reduce stress, and improve wellbeing. However, their long-term impact warrants further investigation. A longitudinal study could reveal how these measures affect mental health over time, support cultural change, and guide future improvements.
Technology-Driven Interventions
With growing technological integration across industries, digital tools now offer new avenues for addressing mental health in construction. These solutions enhance accessibility, provide real-time support, offer anonymity, and help reach workers in remote or isolated locations (Jebelli et al. 2018a; King et al. 2023; NIMH 2024). In the United States, services such as the 988 Suicide and Crisis Lifeline provide 24/7 support, ensuring that help is always within reach (NIMH 2024).
Blended Interventions
Combining digital tools with traditional in-person approaches has proven especially effective. For instance, King et al. (2023) evaluated the MATES mobile app, which integrates with MIC by providing mobile access to mental health resources, peer support, and professional help. Their randomized controlled trial showed that pairing this digital platform with face-to-face training significantly increased help-seeking behavior and mental health literacy. The hybrid model, leveraging both in-person interaction and digital convenience, offers flexibility while maintaining critical human support, particularly in environments where stigma still poses a barrier to care.
EEG and Machine Learning
Jebelli et al. (2018b) explored cutting-edge applications of electroencephalogram (EEG) combined with machine learning to monitor construction workersʼ stress levels in real time. This wearable tool achieved over 80% accuracy in detecting stress by analyzing brain activity, providing continuous feedback on workersʼ mental states. Such technology enables early detection of stress, allowing supervisors to intervene through means such as adjusting workloads or scheduling rest breaks before mental health issues escalate. It also informs organizational strategies by identifying high-stress roles or environments that may require systemic change.
Enhancing Mental Health Literacy Through Digital Platforms
Digital literacy tools are also being adopted to improve understanding of mental health across the workforce. Delivered through apps, these programs offer educational content on stress, emotional regulation, and coping strategies (Chan et al. 2020). By increasing awareness and reducing stigma, these tools empower workers to recognize mental health issues and seek support proactively. As research has shown, higher mental health literacy correlates strongly with increased help-seeking behavior.
Workplace-based and technology-driven interventions vary significantly in their focus, delivery approaches, and intended populations, with each presenting unique strengths and limitations; these are outlined in Table 4. Workplace-based programs aim to improve organizational conditions through initiatives such as peer support networks, leadership training, and policy reforms. These efforts help cultivate a supportive workplace culture but often depend on strong organizational commitment. In contrast, technology-driven interventions are designed for individual use, providing anonymity and on-demand access through apps and digital platforms. Although convenient, their effectiveness can be limited by usersʼ technological proficiency and ability to recognize when help is needed. A promising hybrid model should integrate elements of both approaches, combining the systemic reach of workplace interventions with the accessibility of technology to offer a more holistic strategy for addressing mental health challenges in the construction industry.
Although both approaches offer unique benefits, the most effective interventions often combine elements from each to offer immediate, accessible support through technology while simultaneously building a supportive workplace culture.
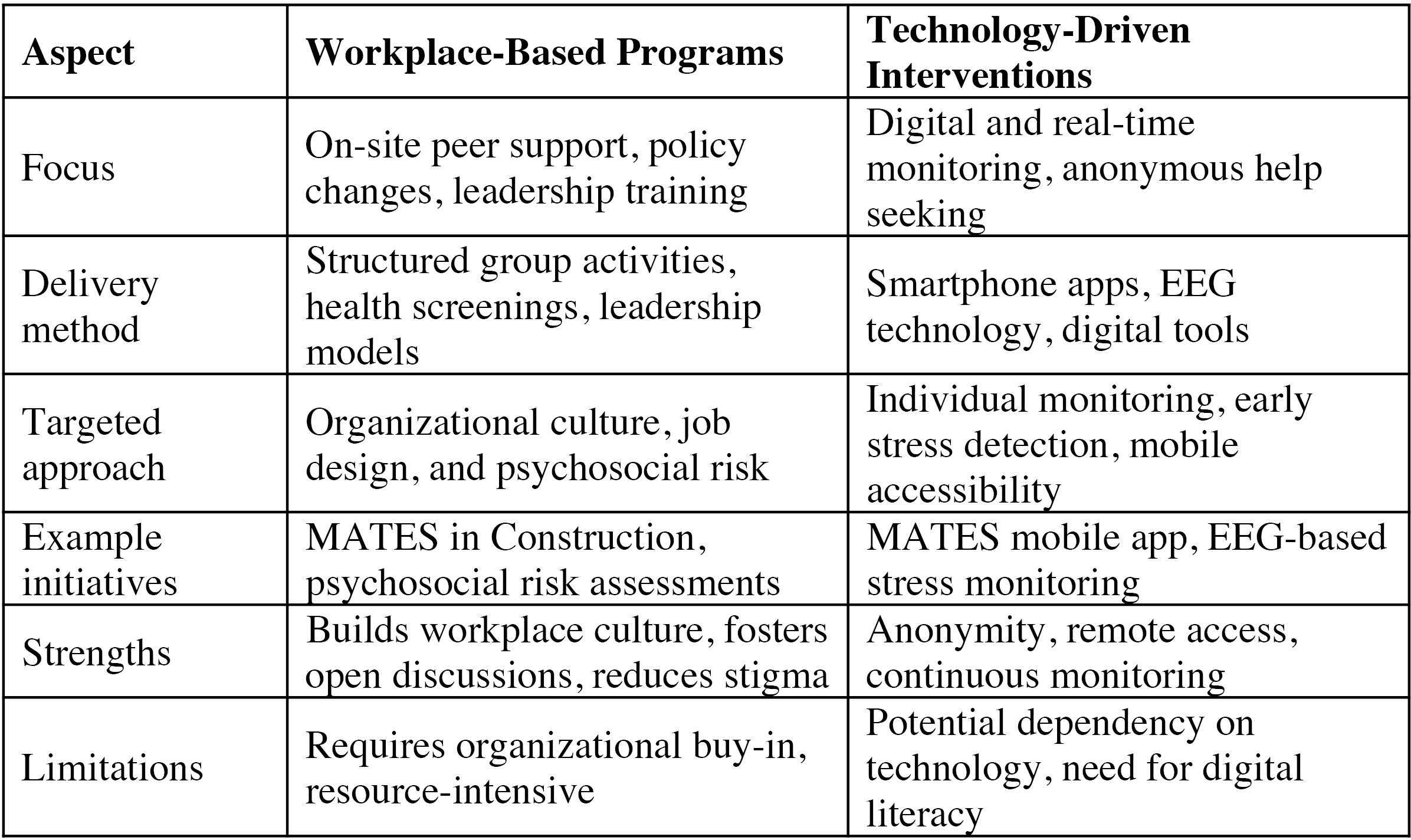
Long Description.
The column headers of the table are Aspect, Workplace-Based Programs, and Technology-Driven Interventions. The data given in the table row-wise are as follows: Row 1: Focus: On-site peer support, policy changes, leadership training; Digital and real-time monitoring, anonymous help-seeking. Row 2: Delivery Method; Structured group activities, health screenings, leadership models; Smartphone apps, EEG technology, digital tools. Row 3: Targeted Approach; Organizational culture, job design, and psychosocial risk; Individual monitoring, early stress detection, mobile accessibility. Row 4: Example Initiatives: MATES in Construction, psychosocial risk assessments; MATES mobile app, EEG-based stress monitoring. Row 5: Strengths: Builds workplace culture, fosters open discussions, reduces stigma; Anonymity, remote access, continuous monitoring. Row 6: Limitations: Requires organizational buy-in, resource-intensive; Potential dependency on technology, need for digital literacy.
Reactive to Proactive Approach: Promoting Positive Mental Health
Contemporary mental health discourse is shifting from a reactive focus on symptoms to proactive strategies that cultivate wellbeing. Dr. Tiffany Sauber Millacci (2019) emphasizes simple, evidence-based practices such as mindfulness, gratitude exercises, and group interactions that help individuals build emotional resilience and psychological balance. Mindfulness promotes present-moment awareness without judgment; gratitude practices strengthen positive emotions and social ties; and group interactions enhance empathy and emotional intelligence, fostering a sense of belonging and psychological safety.
Frimpong et al. (2024) build on this approach by advocating for a positive mental health model rooted in postmodern theory, which critiques traditional power structures and highlights systemic influences on mental health. They argue for holistic approaches that address economic, cultural, and social factors, not just individual symptoms. Their work aligns with Nwaogu et al. (2022), reinforcing the importance of an integrated model that balances individual practices with broader institutional and societal changes. Together, these perspectives support a multidimensional framework for mental wellbeing in construction, one that blends personal resilience, organizational reform, and systemic advocacy to create lasting change.
While this synthesis focuses on analyzing mental health and wellbeing programs, including those addressing suicide prevention and addiction mitigation across various DOTs, providing an overarching view of selected efforts offers valuable insight into broader trends and emerging practices across state agencies.
Mental Health and Wellbeing Programs in State DOTs
Several state DOTs and affiliated agencies have adopted diverse strategies to promote mental health and wellbeing among their workforces. Washington State DOT (WSDOT), for example, focuses on building psychological resilience through structured models such as “ADAPT and THRIVE.” In this approach, ADAPT involves recognizing and responding to mental health challenges with flexibility and support, and THRIVE focuses on fostering resilience, growth, and sustained wellbeing in the face of adversity. These frameworks aim to reduce burnout, manage compassion fatigue, and mitigate moral injury by encouraging healthy work–life boundaries, recognizing small victories, and addressing external stressors rather than internalizing blame (WSDOT, n.d.). Other states rely on Employee Assistance Programs (EAPs) to deliver mental
health support. Idahoʼs EAP offers confidential and cost-free access to professional resources designed to support emotional wellbeing and life balance (Idaho Office of Group Insurance 2024). Similarly, Missouri DOT (MoDOT)ʼs program provides local counseling services, referrals, and brief solution-focused therapy to help employees manage mental health issues (MoDOT, n.d.). In Michigan, behavioral health services are offered through a comprehensive digital and in-person health plan that includes stress management tools, inpatient and outpatient services, and substance use treatment programs (Blue Cross Blue Shield of Michigan 2024). This layered approach enhances accessibility while catering to various mental health needs. Oklahoma takes a training-focused approach by offering “Mental Health First Aid” and “Talk Saves Lives,” two programs aimed at equipping supervisors and employees with suicide prevention and mental health response strategies. Mental Health First Aid is a training program that teaches people how to identify, understand, and respond to signs of mental health or substance use challenges. Like physical first aid, it equips individuals with the skills to provide initial support and guide someone toward appropriate professional help. These programs are part of a broader effort to integrate proactive education into workplace culture (Oklahoma Department of Mental Health and Substance Abuse Services, n.d.).
New Hampshire emphasizes both individual and managerial support through its EAP. Services include early intervention, personalized counseling, and management consultation to address group-level issues. These are designed not only to resolve personal problems but also to enhance overall workplace communication, cooperation, and productivity (New Hampshire Department of Health and Human Services, n.d.). In Wyoming, the focus lies on crisis preparedness. The state provides Mental Health First Aid training for both adults and youth, teaching participants to recognize warning signs, respond to crises, and connect individuals to professional help (Wyoming Department of Health, n.d.). Tennesseeʼs Here4TN initiative links employees to virtual resources supporting work–life balance, mental health, and sleep. This comprehensive digital platform reflects a growing trend toward integrating wellness support within broader benefits ecosystems (Tennessee Department of Finance and Administration, n.d.).
Collectively, these state-led efforts reflect a growing recognition of mental health as a critical component of workforce sustainability and operational resilience. The diversity of approaches, from digital tools and training to comprehensive EAPs, suggests a trend toward more integrated, employee-centered mental health strategies in public-sector infrastructure agencies.
Mental Health and Wellbeing Programs in Adjacent Sectors – Transit Sector
The mental health crisis among workers in the transit and construction industries has gained national attention due to the high-stress environments, exposure to trauma, erratic schedules, and lack of institutional support that characterize these sectors. In response, federal agencies and research institutions have begun identifying targeted initiatives and policy recommendations to address mental health, reduce suicide risks, and mitigate substance use in these labor-intensive and safety-critical fields.
The FTA highlights an urgent need for trauma-informed practices and wellness initiatives tailored for transit workers, particularly those serving in frontline roles. Their mental health and wellness portal underscores the importance of implementing comprehensive wellness programs, increasing access to EAPs, and engaging leadership in creating a culture of psychological safety (FTA, n.d.). The FTA also emphasizes cross-agency collaboration and data-informed strategies to guide suicide prevention and addiction recovery efforts.
Expanding on this, Brennan et al. (2024) provided a nuanced picture of the lived experiences of frontline transit workers and suggested an array of programmatic and organizational interventions. Key recommendations include the following:
- Improving physical safety through infrastructure changes (e.g., platform barriers, protective enclosures) to reduce passenger under train incidents;
- Restructuring leave and scheduling policies to support mental health and work–life balance, addressing concerns about punitive absenteeism policies and forced overtime;
- Enhancing communication and outreach strategies to increase awareness of mental health services, especially for workers without consistent email access;
- Evaluating and customizing EAPs and mental health programs to consider worker preferences for privacy, off-site one-on-one counseling, and professional-led support rather than peer groups;
- Building peer support networks and mentoring programs to combat isolation and boost morale;
- Training for de-escalation, crisis response, and empathy to prepare employees and managers to handle traumatic situations and foster understanding between frontline staff and leadership; and
- Embedding mental health awareness in workplace culture through trust-building efforts that involve unions and frontline staff in wellness program design and implementation.
Although it was focused on the transportation construction sector, OʼBrien et al. (2024)—in a Mineta Transportation Institute research report—drew critical parallels, particularly regarding the impact of mental health on labor retention and workforce stability. The study emphasized that poor mental health and addiction contribute to high turnover and labor shortages in highway construction. Recommendations center on improving workforce conditions to mitigate these issues, including the following:
- Incentivizing mental health support through better benefits and wellness programs;
- Embedding mental health in recruitment and retention strategies, such as linking subsidized training programs with mental health education and support resources;
- Designing workforce development pipelines that include awareness and support for behavioral health, especially in hard-to-staff regions; and
- Creating interdisciplinary forums to learn from other sectors (e.g., healthcare) that have faced similar challenges with stress, burnout, and workforce shortages.
Highway construction and maintenance workers, like train operators, are routinely exposed to traumatic incidents, including fatal crashes and injuries occurring in or near active work zones. Similar to train crews—who often witness suicides by train and report lasting psychological impacts such as PTSD, anxiety, and survivorʼs guilt (FRA 2013)—highway workers face comparable emotional tolls, particularly when responding to vehicle fatalities or witnessing the deaths of coworkers (Brennan et al. 2024; OʼBrien et al. 2024). Although the Federal Railroad Administration has implemented peer support systems and critical incident protocols to support train operators, structured mental health resources for highway workers remain limited. Drawing from these rail sector interventions, there is growing recognition of the need to develop trauma-informed mental health programs for the highway workforce to address similar risks and promote resilience.
Collectively, these sources converge on the need for holistic, systemic responses that go beyond surface-level wellness programs. Instead, they advocate for a restructuring of workplace culture, policy, and infrastructure to center employee mental health, reduce stigma, and support long-term wellbeing in demanding transportation and construction environments.
Literature Review Summary
Mental health and wellbeing have become critical areas of concern within the construction and transportation sectors, especially among public agencies such as state DOTs and transit organizations. Research shows that workers in these sectors face unique stressors, including long hours, physical demands, stigma, and limited access to support, all of which increase risks for psychological distress, substance use, and suicide. A substantial body of literature exists on stressors, vulnerabilities, and targeted interventions in the construction industry, with growing attention to upstream approaches such as peer support networks, mental health leadership training, and technology-based tools. Similarly, state DOTs have adopted a range of strategies, including robust EAPs, mental health training, and digital wellness platforms. While these programs vary in structure and emphasis, they collectively reflect a shift toward more proactive, systemic approaches to workforce wellbeing. Adjacent sectors such as transit also provide relevant insights, with federal and academic sources recommending infrastructure improvements, culture change, and embedded mental health strategies to enhance workforce resilience. However, despite growing interest, the literature is still evolving, and few studies evaluate long-term effectiveness or cross-sector integration of mental health initiatives. This literature review served as the foundation for developing a comprehensive survey of mental health, suicide prevention, and addiction mitigation practices across state DOTs. The findings from that survey are presented in the next chapter.












