Mental Health, Suicide Prevention, and Addiction Mitigation in Construction and Maintenance (2026)
Chapter: 3 State of Practice Survey

CHAPTER 3
State of Practice Survey
Introduction
This chapter presents current practices, tools, and approaches in use by state DOTs for education and promotion of mental health, suicide prevention, and addiction mitigation efforts for highway workers. To gather the most current information on related policies, procedures, and practices, a web-based survey was distributed to the voting members of the AASHTO Committee on Construction and the North American Association of Transportation Safety and Health Officials, which includes representatives from all 50 state DOTs and the District of Columbia. Responses were received from 41 state DOTs, representing an 80% response rate (Figure 1). The findings in this chapter also draw on relevant documents submitted by survey participants.
The chapter begins with an overview of existing policies, procedures, and guidelines that state DOTs have in place to educate and promote employee mental health, suicide prevention, and addiction mitigation efforts. It then outlines the programmatic approaches currently being used, discusses organizational structures and communication challenges, and highlights innovative practices to support mental health, suicide prevention, and addiction mitigation. The chapter concludes with methods used by state DOTs to measure and track the implementation of these efforts.
The 41 state DOT respondents were not obligated to answer all survey questions, therefore the sample size (n) for each question differs. The complete survey questionnaire is available in Appendix A, and Appendix B contains individual agency responses to each survey question. Detailed analysis of the surveyʼs key findings is presented in the following sections.
Policies, Procedures, and Guidelines to Educate and Promote Mental Health and Wellbeing
The survey results indicate that practices on education and promotion of mental health, suicide prevention, and addiction mitigation efforts for highway workers vary among state DOTs. Out of 41 DOT responses, two DOTs (5%) reported that their DOTs do not have practices for implementing mental health and wellbeing efforts, and that another agency in their state manages and supports mental health and wellbeing, suicide prevention, and substance use and addiction efforts.
Figure 2 shows the result of the survey regarding formal policies or guidelines to support employee mental health and wellbeing, suicide prevention, and substance use and addiction mitigation. Out of 39 DOT responses, 19 state DOTs (49%) have formal policies or guidelines for mental health and wellbeing; 23 state DOTs (59%) have formal policies or guidelines for substance use and addiction mitigation; and 14 state DOTs (36%) have formal policies or guidelines

Long Description.
The map of the United States illustrates the response of state departments of transportation to a survey. States are shaded to indicate whether they responded or not. A legend explains the shading: dark gray for states that responded and light gray for those that did not. Washington, D.C., is highlighted with a star symbol. The map includes all fifty states, with Alaska and Hawaii shown separately at the bottom left.

Long Description.
The bar chart illustrates the number of Department of Transportation (DOT) responses regarding three categories: suicide prevention, substance use and addiction, and mental health and well-being. The responses are divided into ‘Yesʼ, ‘Noʼ, and ‘In Developmentʼ. For ‘Yesʼ, mental health and well-being has 49 percent, substance use and addiction 59 percent, and suicide prevention 36 percent. In the ‘Noʼ category, mental health and well-being is at 44 percent, substance use and addiction at 41 percent, and suicide prevention at 59 percent. ‘In Developmentʼ shows 8 percent for mental health and well-being, 0 percent for substance use and addiction, and 5 percent for suicide prevention. The x-axis represents the number of DOT responses ranging from 0 to 40, while the y-axis categorizes the responses.
for suicide prevention. Additionally, three state DOTs (8%) are in the process of developing policies or guidelines for mental health and wellbeing, and two state DOTs (5%) are in the process of developing policies or guidelines for suicide prevention.
The survey respondents were then asked whether their DOT has formal programs or initiatives to support employee mental health and wellbeing, suicide prevention, and substance use and addiction mitigation. Figure 3 summarizes the responses to this question.
Figure 3 shows that out of 39 DOT responses, 34 state DOTs (87%) have formal programs or initiatives for mental health and wellbeing; 30 state DOTs (77%) have formal programs or initiatives for substance use and addiction; and 24 state DOTs (62%) have formal programs or initiatives for suicide prevention. Additionally, one state DOT (3%) is in the process of developing formal programs or initiatives for mental health and wellbeing, and one state DOT (3%) is in the process of developing formal programs or initiatives for suicide prevention.
The survey shows that 25 of the 39 DOTs (64%) have not used contract language that encourages or requires contractors to address mental health and wellbeing for their workforces; two state DOTs (5%) have used such language (Figure 4).
Figure 5 highlights the primary avenues through which state DOT policies, programs, and initiatives contribute to mental health support, suicide prevention, and addiction reduction. The top five avenues include the following:
- Email communications (29 DOTs, 74%);
- Intranet/employee portal (27 DOTs, 69%);
- Workplace posters (24 DOTs, 62%);
- Orientation and onboarding materials (23 DOTs, 59%); and
- Internal newsletters (18 DOTs, 46%).
Additionally, five state DOTs noted that they convey the policies, programs, and initiatives that support mental health, suicide prevention, and addiction mitigation to employees through their EAPs. One state DOT mentioned that the agency conveys these policies, programs, and

Long Description.
The bar chart illustrates the number of Department of Transportation (DOT) responses categorized by ‘In Developmentʼ, ‘Noʼ, and ‘Yesʼ stages. It compares responses on three topics: suicide prevention, substance use and addiction, and mental health and well-being. The ‘Yesʼ category shows the highest responses with 62 percent for suicide prevention, 77 percent for substance use, and 87 percent for mental health. The ‘Noʼ category has 36 percent for suicide prevention, 23 percent for substance use, and 10 percent for mental health. ‘In Developmentʼ shows 3 percent for both suicide prevention and mental health, and 0 percent for substance use. The x-axis represents the number of DOT responses ranging from 0 to 40.

Long Description.
The bar chart illustrates the distribution of DOT responses across three categories: ‘Yesʼ, ‘Noʼ, and ‘Not sureʼ. The horizontal axis represents the number of DOT responses, ranging from 0 to 40. The ‘Yesʼ category shows 5 percent, ‘Noʼ shows 64 percent, and ‘Not sureʼ shows 31 percent. The chart highlights the predominance of ‘Noʼ responses compared with the other categories.

Long Description.
The bar chart illustrates the number of DOT responses for various communication methods. The horizontal axis represents the number of responses, ranging from 0 to 40. The vertical axis lists communication methods, including email communications, intranet or employee portal, workplace posters, orientation and onboarding materials, internal newsletters, training sessions, senior leadership meetings, policy manual, team meetings, toolbox talks, digital screens, and others. Email communications received the highest response at 74 percent, followed by intranet or employee portal at 69 percent, and workplace posters at 62 percent. Orientation and onboarding materials shows 59 percent, internal newsletters 46 percent, training sessions 41 percent, senior leadership meetings 31 percent, policy manual 31 percent, team meetings 23 percent, toolbox talks 21 percent, digital screens 13 percent, and other 28 percent.
initiatives to employees through its human resources (HR) departments. Another DOT stressed the importance of statewide communication for all state employees regarding available resources and training for leaders on recognizing and assisting employees with mental health issues, suicide prevention, and addiction support.
Programmatic Approaches to Educate and Promote Mental Health and Wellbeing
The survey results indicated that state DOTs have implemented various programs to promote mental health and wellbeing. Figure 6 shows the following top five programs or initiatives implemented by state DOTs to promote mental health and wellbeing:
- Employee Assistance Programs (37 DOTs, 95%);
- Drug testing (32 DOTs, 82%);
- Referrals to counseling (20 DOTs, 51%);

Long Description.
The bar chart illustrates different workplace mental health and support programs, detailing the number of Department of Transportation (DOT) responses. The x-axis represents the number of DOT responses, ranging from 0 to 40, while the y-axis lists the programs. Employee Assistance Programs have the highest response at 95 percent, followed by drug testing at 82 percent. The remaining programs are referrals to counseling at 51 percent, crisis hotlines at 46 percent, on-site or virtual mental health training at 46 percent, external partnerships with nonprofits and healthcare providers at 38 percent, suicide prevention training at 18 percent, mental health app or digital platform at 18 percent, peer support groups at 13 percent, substance use employee recovery groups at 3 percent, and other at 10 percent.
- Crisis hotlines (18 DOTs, 46%); and
- On-site or virtual mental health training (18 DOTs, 46%).
Additionally, one state DOT noted, “We only use mandatory referrals for counseling in situations where an employeeʼs behavior has become disruptive or highly concerning.” Another DOT highlighted that in addition to partnering with statewide resources and its EAP, it has brought in local mental health first aid training through its safety and health staff. One state DOT noted, “Drug testing is only for Commercial Driverʼs License (CDL) drivers.”
The survey participants were then asked to evaluate the effectiveness of their DOTsʼ programs or initiatives to promote mental health and wellbeing using 5-point rating scales. This scale ranged from “0” for “Not Effective at All” to “4” for “Very Highly Effective,” with intermediate ratings of “1” for “Slightly Effective,” “2” for “Moderately Effective,” and “3” for “Highly Effective.” Table 5 summarizes their effectiveness rating and weighted importance score for DOTsʼ programs or initiatives to promote mental health and wellbeing. The aggregated important or weighted score is calculated using Equation (1).
 (1)
(1)
where
WSj = The weighted score of the program/initiative j,
nij = The total number of responses to the program/initiative j associated with the rating ri, and
ri = The rating of the program/initiative j.

Long Description.
The column headers of the table are Programs and initiatives, Not Effective (0), Slight (1), Moderate (2), High (3), Very High (4), and Ranking. The data given in the table row-wise are as follows: Row 1: Peer support groups; 0; 0; 1; 3; 1; 3.00. Row 2: Referrals to counseling: 0; 3; 2; 10; 5; 2.85. Row 3: Drug testing: 1; 5; 6; 12; 8; 2.66. Row 4: Employee Assistance Programs (EAPs): 0; 2; 14; 16; 4; 2.61. Row 5: External partnerships (nonprofits, healthcare providers): 0; 1; 7; 5; 1; 2.43. Row 6: On-site or virtual mental health training: 0; 4; 6; 6; 2; 2.33. Row 7: Crisis hotlines: 0; 3; 6; 6; 1; 2.31. Row 8: Substance use employee recovery groups: 0; 0; 1; 0; 0; 3.00. Row 9: Suicide prevention training: 0; 2; 4; 1; 0; 1.86. Row 10: Mental health app or digital platform: 1; 1; 4; 0; 0; 1.50. Row 11: Other: 3; 0; 0; 0; 0; 0.00.
The five programs or initiatives most frequently identified by state DOTs as effective in promoting employee mental health and wellbeing are the following:
- Peer support groups,
- Referrals to counseling services,
- Drug testing programs,
- Employee Assistance Programs, and
- External partnerships (nonprofits, healthcare providers).
Organizational Structures and Communication Challenges of Implementing Mental Health and Wellbeing Programs
The survey respondents were asked whether DOT characteristics (e.g., permanent or temporary employees, union or nonunion workforces, and human resources) influence their policies, procedures, and guidelines on mental health and wellbeing. Out of 39 DOT responses, nine state DOTs (23%) indicated that they hired temporary employees in addition to permanent employees; 21 state DOTs (54%) reported that their DOT workforce is unionized and 29 state DOTs (74%) reported that their DOT workforce is nonunion; and 27 state DOTs (69%) reported that they relied on internal DOT human resources for such policies, procedures, and guidelines.
Fifteen out of 39 DOT responses (38%) indicated that their DOTʼs HR department is responsible for mental health, suicide prevention, and addiction initiatives and programs (Figure 7).
Figure 7 also indicates that 17 DOTs (44%) indicated that other agencies are responsible for mental health, suicide prevention, and addiction initiatives and programs in their DOTs. Eleven DOTs indicated that their statewide HR offices are responsible for these programs. Additionally, one DOT respondent stated, “Much responsibility lies with Statewide HR EAP management, but anything DOT specific is assigned to an in-house unit. Centralization of HR has made this approach more challenging to coordinate.” Another DOT respondent mentioned, “DOT HR

Long Description.
The pie chart illustrates survey results divided into three segments. The ‘Yesʼ segment represents 38 percent, the ‘Noʼ segment accounts for 18 percent, and the ‘Otherʼ segment makes up 44 percent of the total responses.
has an Employee Advocate Office that can refer employees to the Civil Service Commissionʼs EAP that administers the programs.” Another DOT respondent noted, “The state provides resources, but we as an agency have the ability to add to those resources so that the programs meet our agencyʼs needs.”
The survey respondents were then asked to rate whether the DOT organizational structure impacts the implementation of policies and programs regarding mental health and wellbeing. Figure 8 summarizes the responses to this question. Under the centralized organizational structure (in which a central headquarters controls decision-making and core functions) 14 state DOTs (36%) indicated “significant impact,” 10 state DOTs (26%) indicated “somewhat impact,” and

Long Description.
The bar chart illustrates the number of DOT responses across three categories for DOT structure and mental health and well-being program implementation: centralized, semi-centralized, and decentralized. The x-axis represents the number of responses, ranging from 0 to 30, and the y-axis lists the categories. Each category is divided into three segments: ‘Little to Noʼ, ‘Somewhatʼ, and ‘Significantʼ. In the decentralized category, ‘Little to Noʼ responses dominate with 72 percent. Semi-centralized shows 51 percent ‘Somewhatʼ responses, and the centralized category shows 38 percent ‘Little to Noʼ responses. The chart highlights the distribution of responses based on the degree of centralization.
15 state DOTs (38%) indicated “little to no impact” on the implementation of policies and programs regarding mental health and wellbeing.
Under the decentralized organizational structure (in which regional offices have complete autonomy over decision-making and operations) four state DOTs (10%) indicated “significant impact,” seven state DOTs (18%) indicated “somewhat impact,” and 28 state DOTs (72%) indicated “little to no impact” on the implementation of policies and programs regarding mental health and wellbeing.
Under the semi-centralized organizational structure (in which strategic decisions are centralized but regional offices handle local operations) six state DOTs (15%) indicated “significant impact,” 20 state DOTs (51%) indicated “somewhat impact,” and 13 state DOTs (33%) indicated “little to no impact” on the implementation of policies and programs regarding mental health and wellbeing.
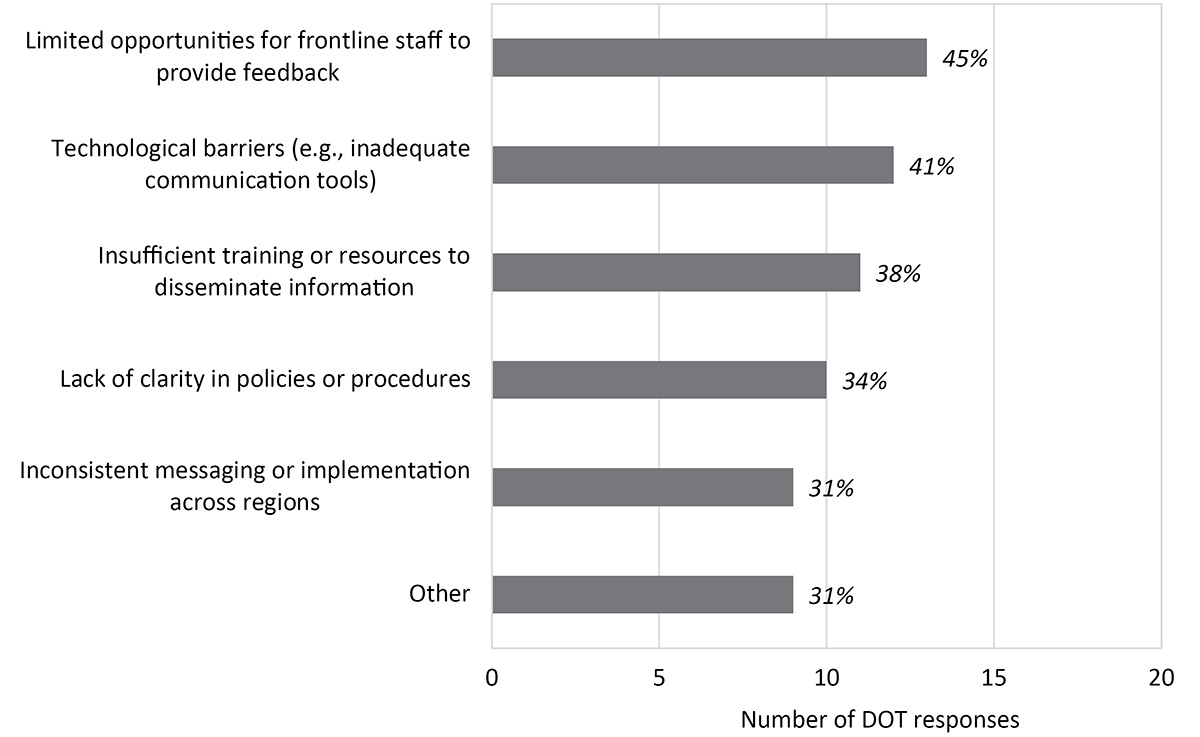
The result of the survey indicated that out of 39 DOT responses, 29 DOTs (74%) have faced challenges in communication between headquarters and frontline staff regarding mental health, suicide prevention, and substance use and addiction initiatives. Figure 9 shows the main communication between headquarters and frontline staff. More than 33% of 29 DOT responses indicated that the main communication challenges between headquarters and frontline staff regarding mental health, suicide prevention, and substance use and addiction initiatives are the following:
- Limited opportunities for frontline staff to provide feedback (13 DOTs, 45%);
- Technological barriers (e.g., inadequate communication tools) (12 DOTs, 41%);
- Insufficient training or resources to disseminate information (11 DOTs, 38%); and
- Lack of clarity in policies or procedures (10 DOTs, 34%).
Additionally, one state DOT mentioned that the most challenging aspect in communication between headquarters and frontline staff involves selling the benefits of these programs because field employees do not like to admit they need help. A representative from another state DOT
Long Description.
The bar chart illustrates challenges faced by frontline staff, with categories on the y-axis and the number of DOT responses on the x-axis, ranging from 0 to 20. Categories include limited opportunities for feedback at 45 percent, technological barriers at 41 percent, insufficient training at 38 percent, lack of clarity in policies at 34 percent, inconsistent messaging at 31 percent, and other issues also at 31 percent. Each bar represents the percentage of responses for each challenge, highlighting the most common issues encountered.
highlighted that a significant barrier is the hesitance among frontline leadership to fully engage in their roles as facilitators for their staff in navigating mental health and wellbeing programs. Another DOT observed that a significant number of its employees tend to seek external resources for mental health support prior to utilizing the agencyʼs established mental health and wellbeing programs, except in instances where the issue may lead to a workersʼ compensation claim.
The survey respondents were asked to identify approaches to address communication gaps between headquarters and frontline staff regarding mental health, suicide prevention, and addiction mitigation initiatives. Figure 10 summarizes the result of this question. More than 33% of the 39 DOT responses have used the following approaches to address communication gaps:
- Development of standardized communication materials (20 DOTs, 51%);
- Use of technology platforms for streamlined communication (17 DOTs, 44%);
- Regular staff meetings or briefings (16 DOTs, 41%); and
- Training programs for managers and staff (15 DOTs, 38%).
Additionally, one state DOT mentioned that the agency has HR field specialists who occasionally remind employees of mental health and substance abuse resources available in addition to providing mental health and wellbeing information during onboarding. Another state DOT noted that the agency is trying to work on consistency by holding regular meetings and seeking guidance from leadership after recent turnover and structural changes. Another DOT highlighted that “we have to convince field managers that it is ok to ask for help.” A representative from one state DOT highlighted that discussions surrounding mental health and wellbeing are not consistently integrated into standard operational dialogues, as a few regional teams are actively managing and addressing these concerns within their operational frameworks.
Innovative Practices to Address Mental Health and Wellbeing
The survey respondents were asked about any innovative practices or technologies state DOTs are exploring or using to promote mental health and wellbeing. Out of 39 DOT responses, nine DOTs (23%) have used innovative practices or technologies to promote mental health and

Long Description.
The bar chart illustrates different communication strategies and their effectiveness based on the number of Department of Transportation (DOT) responses. The strategies are development of standardized communication materials at 51 percent, use of technology platforms for streamlined communication at 44 percent, regular staff meetings or briefings at 41 percent, training programs for managers and staff at 38 percent, and both field toolbox talks and other methods at 28 percent each. The horizontal axis represents the number of DOT responses, ranging from 0 to 20.
wellbeing (Figure 11). One state DOT noted that they are exploring EAP programs beyond what the state offers, considering an on-site counselor or Licensed Clinical Social Worker, and working toward broader employee engagement and mentorship programs. Another DOT highlighted that it began utilizing webinars and providing workplace resource documents and articles to support employees. Other sample innovative practices used by state DOTs to promote mental health and wellbeing include the following:
- Providing lunch and learn sessions with a topic on stress,
- Virtual counseling sessions via the EAP,
- Enhancing the stress continuum program,
- Mental health first aid training,
- Use of a third-party provider to help supplement the services offered through the state,
- Peer support, and
- External mental health presentations presented with a Teams live stream.
Additionally, eight DOTs (21%) are in the process of developing innovative practices or technologies to promote mental health and wellbeing (Figure 11). One DOT noted that it is developing “a toolbox of mental health discussions and resources that can be taken to any DOT to be used.” Another DOT highlighted that “There is a draft bill for this legislative session around having workersʼ compensation insurance coverage for employees impacted by [PTSD] or having mental health issues from workplace injury/trauma.” Another DOT mentioned that its internal Safety Office is working through the development of a collection of useful mental health and wellness tools and training for its employees. One DOT indicated that the agency is working with Associated General Contractors of America industry partners in line with employee work–life balance by initially soliciting ideas for potential improvements in that area for both contractor and DOT field staff.
Figure 12 shows that 13 state DOTs out of 39 responses (33%) have specific initiatives for reaching nonstandard shift workers (a work schedule that falls outside of the typical or standard business hours) with information to promote mental health, suicide prevention, and addiction mitigation. One state DOT noted, “If an employee is referred to the EAP by an Appointing Authority (i.e., DOT), the employee shall be given time off with pay for the intake and evaluation visits. For other situations, the employee may need to use benefit leave for appointments.” Other

Long Description.
The bar chart illustrates the distribution of Department of Transportation (DOT) responses to implementation of innovative practices or technologies to promote mental health and well-being. The x-axis represents the number of responses, ranging from 0 to 20. The y-axis lists response categories: ‘Noʼ with 36 percent, ‘Yesʼ with 23 percent, ‘Not sureʼ and ‘In developmentʼ both with 21 percent. The chart highlights that the majority of responses are ‘Noʼ, followed by ‘Yesʼ, with ‘Not sureʼ and ‘In developmentʼ having equal percentages.

Long Description.
The bar chart illustrates the distribution of DOT responses regarding initiatives for reaching nonstandard shift workers. The x-axis represents the number of responses, ranging from 0 to 30. The y-axis lists response categories: ‘Noʼ at 64 percent, ‘Yesʼ at 33 percent, and ‘In Developmentʼ at 3 percent. The ‘Noʼ category has the longest bar, followed by ‘Yesʼ. ‘In Developmentʼ has the shortest bar.
initiatives used by state DOTs to reach nonstandard shift workers in support of mental health, suicide prevention, and addiction mitigation include the following:
- Peer support programs;
- Safety talks;
- Mobile drug testing;
- Making existing resources available and ensuring communications are shared with all employees, regardless of shift;
- Requiring all employees, regardless of shift, to attend new employee orientation and informing them of available benefits;
- Informing employees that the Suicide and Crisis Lifeline (988) and the EAP are available 24 hours a day for support; and
- Providing training for working alternative shifts.
The survey participants were then asked to identify their partnerships with external organizations to support mental health and wellbeing efforts. Figure 13 summarizes the responses to this question.

Long Description.
The bar chart illustrates the number of Department of Transportation (DOT) responses regarding partnerships with external organizations. The x-axis represents the number of responses, ranging from 0 to 40, and the y-axis lists the eternal organizations. Responses are as follows: Employee Assistance Programs 92 percent, Mental Health Services Providers 28 percent, Government Agencies 26 percent, Industry Groups 18 percent, Community Health Organizations 18 percent, Nonprofit Organizations 13 percent, Private Consultant Firms 8 percent, None 3 percent, and Other 3 percent. Employee Assistance Programs have the highest response rate at 92 percent.
The five most common external organizations that state DOTs have partnered with to support mental health and wellbeing efforts are the following:
- Employee Assistance Programs (36 DOTs, 92%);
- Mental health services providers (11 DOTs, 28%);
- Government agencies (10 DOTs, 26%);
- Industry groups (7 DOTs, 18%); and
- Community health organizations (7 DOTs, 18%).
Additionally, one state DOT highlighted that its geohazards team is undergoing mental health training facilitated by the “Responder Alliance,” a training center for resilience tools to prevent burnout and traumatic stress injury. Any new members who join this team are required to complete the training program.
Figure 14 summarizes the specific contributions of the partnerships with external organizations to state DOTsʼ mental health and wellbeing programs. Out of 37 DOT responses, the external organizations have provided counseling services to 35 DOTs (95%) and awareness campaigns to 25 DOTs (68%). Twelve state DOTs (32%) also noted that the partnerships with external organizations contribute to developing mental health policies and programs.
Performance Measurement and Tracking
The survey participants were asked whether their state DOTs have a system to measure or track the implementation of mental health and wellbeing programs. Figure 15 summarizes the responses to this question. Out of 39 responses, three DOTs (8%) have a system to measure or track the implementation of mental health and wellbeing programs. One state DOT noted that it has used Gallup scoring (i.e., a method to measure and assess various metrics, primarily related to employee engagement, workplace performance, and organizational health) to measure and track its employee wellbeing annually. Another DOT highlighted that it monitors the utilization rate of services and identifies key drivers to inform and shape its training initiatives, ensuring that its training aligns with current operational demands and experiences. Additionally, four DOTs (10%) are in the process of developing a system to measure or track the implementation of mental health and wellbeing programs (Figure 15).

Long Description.
The bar chart illustrates the number of Department of Transportation (DOT) responses for different mental health initiatives. The horizontal axis represents the number of responses, ranging from 0 to 40. The vertical axis lists initiatives: counseling services, awareness campaigns, developing mental health policies and programs, funding, and others. Counseling services received the highest response at 95 percent, followed by awareness campaigns at 68 percent, developing policies at 32 percent, other at 5 percent, and funding at 3 percent.

Long Description.
The bar chart illustrates the distribution of DOT responses regarding measurement or tracking the implementation of mental health and well-being. The x-axis represents the number of responses, ranging from 0 to 40. The y-axis lists response categories: Yes, In development, Not sure, and No. The ‘Noʼ category has the highest response at 62 percent, followed by ‘Not sureʼ at 21 percent, ‘In developmentʼ at 10 percent, and ‘Yesʼ at 8 percent.
Figure 16 shows that 15 of 31 DOT respondents (48%) have used feedback from managers or supervisors; 14 state DOTs (45%) have used statistics of services (e.g., EAP); and six DOTs (19%) have used employee surveys to measure or track the implementation of mental health and wellbeing programs. Furthermore, one DOT indicated that it has collected voluntary feedback from employees who participate in the programs, while another DOT has used incident metrics to monitor the implementation of mental health and wellbeing initiatives. Another DOT stated that “although the statistics are available to the Statewide Benefits Office, DOT doesnʼt have access to this information.”
Finally, the survey participants were asked to identify the key barriers to implementing mental health and wellbeing, suicide prevention, and addiction mitigation programs. Figure 17 summarizes the responses to this question. Perceived barriers to implementing mental health and wellbeing, suicide prevention, and addiction mitigation programs include the following:
- Stigma around mental health, suicide, and addiction (21 DOTs, 54%);
- Lack of expertise among staff (20 DOTs, 51%);
- Challenges in engaging employees in programs (17 DOTs, 44%);

Long Description.
The bar chart illustrates the number of Department of Transportation responses across four categories: feedback from managers or supervisors, usage statistics of services such as Employee Assistance Programs, other sources, and employee surveys. The horizontal axis represents the number of responses, ranging from 0 to 20. Feedback from managers or supervisors has the highest response rate at 48 percent, followed by usage statistics at 45 percent, other sources at 35 percent, and employee surveys at 19 percent.

Long Description.
The bar chart illustrates barriers to implementing mental health initiatives, ranked by the number of DOT responses. The x-axis represents the number of responses, ranging from 0 to 25. The y-axis lists the barriers: Stigma is the highest barrier, with 54 percent, followed by lack of expertise among staff at 51 percent, challenges in engaging employees at 44 percent, lack of funding at 41 percent, resistance to change at 31 percent, insufficient training at 31 percent, concerns about confidentiality at 28 percent, limited management support at 28 percent, complex policy requirements at 18 percent, limited access to external support at 13 percent, and other at 15 percent. The chart highlights the complexity of implementing mental health programs.
- Lack of funding, resources, or budget constraints (16 DOTs, 41%); and
- Resistance to change or new initiatives (12 DOTs, 31%) and insufficient training (also 12 DOTs, 31%).
Additionally, one state DOT mentioned that the implementation of mental health and wellbeing, suicide prevention, and addiction mitigation programs is hampered by the project-based nature of many positions. This leads to a situation in which employees are often dispersed and not co-located, making it challenging to effectively engage with digital communications concerning these initiatives.
Survey Questionnaire Summary
This chapter describes the current practices in use by state DOTs to educate and promote mental health, prevent suicide, and mitigate addiction for highway workers by analyzing 41 DOT responses from the national survey that was distributed to 50 state DOTs and the District of Columbia. Of the 39 DOT responses, 19 state DOTs (49%) have formal policies or guidelines and 34 state DOTs (87%) have formal programs or initiatives for mental health and wellbeing; 23 state DOTs (59%) have formal policies or guidelines and 30 state DOTs (77%) have formal programs or initiatives for substance use and addiction; and 14 state DOTs (36%) have formal policies or guidelines and 24 state DOTs (62%) have formal programs or initiatives for suicide prevention.
For the programmatic approaches, the top five programs or initiatives implemented by state DOTs to promote mental health and wellbeing are the following:
- Employee Assistance Programs (37 DOTs, 95%);
- Drug testing (32 DOTs, 82%);
- Referrals to non-EAP counseling (20 DOTs, 51%);
- Crisis hotlines (18 DOTs, 46%); and
- On-site or virtual mental health training (18 DOTs, 46%).
Regarding organizational structures and communication challenges, 15 of 39 DOT respondents (38%) indicated that their DOTʼs HR department is responsible for mental health, suicide prevention, and addiction initiatives and programs. Seventeen DOTs (44%) indicated that other agencies are responsible for mental health, suicide prevention, and addiction initiatives and programs. Of 39 responses, 29 DOTs (74%) have faced challenges in communication between headquarters and frontline staff regarding mental health, suicide prevention, and substance use and addiction initiatives. More than 33% of 29 DOT responses indicated that the main communication challenges between headquarters and frontline staff regarding mental health, suicide prevention, and substance use and addiction initiatives are the following:
- Limited opportunities for frontline staff to provide feedback (13 DOTs, 45%);
- Technological barriers (e.g., inadequate communication tools) (12 DOTs, 41%);
- Insufficient training or resources to disseminate information (11 DOTs, 38%); and
- Lack of clarity in policies or procedures (10 DOTs, 34%).
Nine out of 39 DOT respondents (23%) have used innovative practices or technologies to promote mental health and wellbeing. Sample innovative practices used by state DOTs to promote mental health and wellbeing include the following:
- Providing lunch and learn sessions on the topic of stress;
- Virtual counseling sessions via the EAP;
- Enhancing the stress continuum program—a mental health framework designed to help individuals and groups understand, recognize, and manage stress responses across a spectrum of severity;
- Mental health first aid training;
- Use of a third-party provider to help supplement the services offered through the state;
- Peer support; and
- External mental health presentations conducted via virtual stream.
The top five external organizations that state DOTs have partnered with to support mental health and wellbeing efforts are the following:
- Employee Assistance Programs (36 DOTs, 92%);
- Mental health services providers (11 DOTs, 28%);
- Government agencies (10 DOTs, 26%);
- Industry groups (7 DOTs, 18%); and
- Community health organizations (7 DOTs, 18%).
Finally, the survey results show that 15 state DOTs out of 31 responses (48%) have used feedback from managers or supervisors; 14 state DOTs (45%) have used statistics of services (e.g., EAP); and six DOTs (19%) have used employee surveys to measure or track the implementation of mental health and wellbeing programs. The top five perceived barriers to implementing mental health and wellbeing, suicide prevention, and addiction mitigation programs are the following:
- Stigma around mental health, suicide, and addiction (21 DOTs, 54%);
- Lack of expertise among staff (20 DOTs, 51%);
- Challenges in engaging employees in programs (17 DOTs, 44%);
- Lack of funding, resources, or budget constraints (16 DOTs, 41%); and
- Resistance to change or to new initiatives (12 DOTs, 31%) and insufficient training (also, 12 DOTs, 31%).














