Secret Agents: The Menace of Emerging Infections (2002)
Chapter: 2 Winged Victories
Chapter 2
Winged Victories
In New York City, late August is a seasonal point of suspension between summer languor and autumn snap, when nothing is supposed to happen. In August 1999, Marci Layton, the assistant commissioner for the Bureau of Communicable Disease in the New York City Department of Health, was, like many residents, planning to flee the city—to hike in the northern Adirondacks, the only wilderness nearby where you can actually reach the top of a mountain and gaze out for miles. If Layton relishes a long view, it’s probably because she directs about 100 outbreak investigations a year and closely monitors surveillance for the 52 infectious diseases that the city requires doctors to report. During the five days left before her weekend hike, she faced the usual crises. A rare strain of Salmonella had struck more than 20 toddlers across the city, and Layton suspected a contaminated food.
Drug-resistant pneumococci hit three nursing homes. An untreatable strain of Acinetobacter was spreading across the city’s intensive care units. Layton’s department was winding down a campaign to vaccinate gay men against hepatitis A. And looming just three weeks away was a bioterrorism preparedness field exercise in the Bronx, to be dubbed City Safe—part field exercise, part educational extravaganza for the media, with simulated emergencies at a hospital, an airport, even the Commonwealth Edison plant.
But on Monday, August 23, Layton’s phone rang, and her life— not to mention her weekend plans—changed. On the line was Deborah Asnis, an infectious disease doctor at Flushing Hospital Medical Center in northern Queens. Two cases troubled Asnis. One was a 60-year-old man who had entered the hospital on August 12, weak from days of vomiting and diarrhea. Rather than quickly rebounding with intravenous fluids, he slid downhill. He had become confused and then developed what doctors call flaccid paralysis of unknown etiology of the upper and lower extremities: his limbs froze, and nobody knew why. Transferred to the intensive care unit, he had been treated as if he had Guillain-Barré syndrome, an inflammation of the nerves, but none of the conventional treatments had worked. Asnis was also worried about a 75-year-old man in her care. He had been wheeled in with a high fever, shaking uncontrollably. Like the other patient, he too became extraordinarily weak over the next few days, so weak he couldn’t move his arms or legs. Both men had spinal fluid with high levels of white blood cells and protein, which hinted at a viral encephalitis. But encephalitis doesn’t usually cause muscle weakness. And since one of the differential diagnoses for Guillain-Barré is botulism—one of the diseases, in this case caused by food toxins, that doctors must report— Asnis dialed the health department.
Marci Layton gets this sort of call at least once a week. An infectious disease specialist, she had chosen the field in order to satisfy a taste for exotic locales. Layton had volunteered in a clinic outside Katmandu, Nepal. She had worked in a hospital in Thailand. She had covered for a doctor in a 12-bed hospital in northern Alaska, flying by
helicopter to a clinic on the north slope. When a CDC employee told her she could find the same range of infectious exotica in New York City and still sleep in her own bed at night, she signed on in 1992 as the agency’s epidemic intelligence officer there, later joining the city health department. Slight and of middling height, with curly red hair parted down the middle, she has a way of somewhat shyly looking up with steady blue eyes as she speaks, which is usually at a brisk clip. Unlike many physicians in public health, she had actually enjoyed taking care of patients when she specialized in infectious diseases, and still welcomed the chance to puzzle through a diagnosis.
In one respect, though, this afternoon’s call was unusual. Flushing Hospital Medical Center had been in the news for years. A small fish in a big tank of recent hospital mergers, it had entered into a disastrous alliance with another institution in order to survive. In 1998, Flushing Hospital had filed for bankruptcy. So badly had the facility been tarred in the media, many people in the neighborhood thought it had already been shut down. When Asnis later told her colleagues that she had called the health department for advice, they were aghast. “When we talk to the health department,” she explained, “they’re usually coming in and condemning the place.”
Asnis, however, was unfazed. Forty-three years old, she had come from a medical family. Her father had been a dentist, and two older brothers became doctors. She married a doctor. Her mother had strongly encouraged her to enter the field. “She wanted me to do anything it took to be independent,” said Asnis, a small, striking woman with short dark hair, lively brown eyes, and bright red lipstick and nail polish. Asnis had herself grown up in Whitestone—the same patch of northern Queens, bracketed by the Bronx-Whitestone and Throgs Neck bridges, from which her patients came—before her family moved out to Long Island. She settled on her specialty because, as she put it, “All the enigmas and fascinomas were in infectious disease.”
During the phone conversation, Layton quickly ruled out botulism—the symptoms and the lab findings didn’t fit. She urged Asnis to send blood and spinal fluid to the state health department lab in Albany for testing.
On Friday afternoon at 4:30, the two women talked again. Asnis’s first two patients were failing, and now two others worried her as well. An 80-year-old man had suffered a heart attack and been admitted with a high fever; he too had become too weak to move and was on a respirator. An 87-year-old woman who had come in with a headache, fever, and diarrhea became unexpectedly confused, then paralyzed all over. As Layton and Asnis talked, a neurologist at Flushing Hospital happened to walk into Asnis’s tiny office. Overhearing the conversation, he mentioned that he was treating a similar problem at a nearby hospital in Queens—another patient with encephalitis and severe muscle weakness.
In all of 1998, New York City had logged nine reports of encephalitis. Now four, maybe five, cases had sprung up within a week in the same neighborhood. Layton cancelled her trip to the Adirondacks. That Friday night, she hunkered down in her office with medical books, trying to find out what kinds of encephalitis caused diffuse muscle weakness. According to the textbooks, none did. At Flushing, Asnis had also been wracking her brain trying to find a cause. AIDS, Lyme disease, polio, TB, syphilis: nothing seemed too outlandish to consider.
On Saturday, Layton and a health department colleague, Annie Fine, drove out to Flushing Hospital. It was a warm, sunny day, like so many that summer. They chatted about what might be causing the strange outbreak. Fine parked the car on a residential side street. As Layton slid out of the passenger seat, she sidestepped a dead crow on the grass near the curb.
Founded in 1884, Flushing Hospital is a true community hospital, with health fairs and free blood pressure screenings and complimentary dental checkups. It’s also an international meeting ground, with brochures printed in Spanish, Russian, Korean, and Chinese—a reflection of the rich polyglot culture of Queens, where 167 nationalities speaking 116 languages make it the nation’s most diverse county. But the hospital’s insolvency showed. Its pale blue lobby looked like it hadn’t been redecorated since the 1960s. Its intensive care unit con-
tained only eight beds. In the narrow hallways of the ICU, Layton and Fine examined patients and talked to families, trying to piece together what the victims, three of whom were on respirators, had in common. They asked where the patients lived, worked, shopped, what parks or beaches they visited, what restaurants they frequented. Other than living in the same two-mile-square area, the patients had very little in common. They were strangers to one another. Their medical charts, however, “told an almost identical story,” Layton said. “These were relatively healthy adults who had a febrile illness followed by some GI symptoms followed by the onset of altered mental status, confusion, and gradually this muscle weakness.” Another clue also kept ringing in Layton’s mind. Several of the patients were tanned and toned. That meant they spent time outdoors—which raised the risk that the infection came from mosquitoes.
As Layton and Fine slowly paged through the thick charts and compared notes, they learned that a 57-year-old man with suspicious symptoms had just been wheeled in. Layton walked over to take a look. High fever, hallucinations, fighting so fiercely with the attendants he needed to be restrained: he looked like a classic encephalitis case. Was the outbreak snowballing?
Layton felt queasy. “I call it my gut meter,” she said. “It was maybe one-plus acidic on Monday. It was eight-plus acidic on Friday. By the time I left the hospital on Saturday, it was off the scale.”
Arbovirus Anonymous
From the seventeenth through the early twentieth centuries, infections ferried about by insects—malaria, yellow fever, plague, and typhus, to name the Big Four—killed more people and sowed more disease than all other causes combined. At the turn of the last century, discoveries about the natural history of these organisms promised a health revolution. But in the last 25 years, the revolution petered out. Today, 500 million people are infected yearly with mosquitoborne diseases alone; nearly three million die.
What those diseases have in common, along with the infection that struck New Yorkers in 1999, is that the agents that cause them swim in the blood of arthropods. The largest phylum in the animal kingdom, arthropods are segmented creatures with jointed legs and a tough exoskeleton made of chitin. Among Arthropoda’s uncuddlesome members are lobsters, crabs, centipedes, cockroaches, and scorpions. For humans, the deadliest members of the clan are mosquitoes, ticks, and fleas.
Viruses transmitted by these blood-feeding arthropods are called arboviruses: arthropodborne viruses. And though arboviruses usually cause just mild, flulike infections, they can also kill strapping adults in a matter of days, by playing havoc with the central nervous system, the heart, or the liver and kidneys. Unlike viruses that cause chronic infections, such as the herpes virus, or that spread person to person, like measles, arboviruses don’t need people to propagate; in the human body, they are accidental tourists. And because these viruses haven’t evolved to the point where they can call a truce with human biology, they often end up knocking off their hosts.
However short-lived, the vanquishing of the great arthropodborne diseases was a monumental achievement in public health. For millennia, sharp observers had noted that biting insects and disease go together. By 1848, scientists surmised that such devastating killers as malaria and yellow fever were transmitted, not by personal contact or fetid water (the usual suspects), but by mosquitoes. When the Scottish physician Sir Patrick Manson showed, in 1877, that the female Culex picked up in its bloodmeal the larval form of the roundworm causing elephantiasis, it opened a rich new scientific lode. But not until the discoveries of Ronald Ross and Walter Reed—two of the 29 names chiseled on the frieze of the New York City Department of Health building—was the link made. Their work dramatically changed the course of public health and of history itself.
In 1898, the British protozoologist Sir Ronald Ross demonstrated in India that the malarial parasite Plasmodium whiled away part of an exquisitely complicated life cycle in the stomach of the “dapple-
winged” Anopheles mosquito before entering the human bloodstream by bite. For this insight, Ross won the 1902 Nobel Prize in medicine. (He did not live to savor the award; the year he became a Nobel laureate, the 51-year-old Ross died of appendicitis.) Trench building for the Panama Canal, begun in 1879, had ground to a halt because of malaria and yellow fever. Thanks to mosquito control measures inspired by Ross’s discovery, and to quinine, the channel was completed in 1914. More important, millions of people living in tropical climates escaped the parasitic disease.
Around the same time, U.S. Army Major Walter Reed tackled the equally frightening scourge of yellow fever. That virus had come to the Western Hemisphere in the sailing ships of slave traders, as the highly adaptable mosquito Aedes aegypti found water cisterns a perfect place to lay eggs. For centuries, the best medical minds didn’t make the connection. After Philadelphia’s devastating 1793 outbreak of yellow fever, the eminent colonial physician Benjamin Rush concluded that the epidemic sprang from putrid coffee unloaded on the docks. Not until the turn of the last century did Reed’s Yellow Fever Commission set up shop in Cuba and reveal the mosquito connection. To test the prevailing theory—which held that yellow fever spread on contaminated articles of clothing or bedding, known as “fomites”—Reed’s team built a room in which volunteers slept for three weeks on cots and in bed-clothes soiled with waste and body fluid spewed from every orifice by yellow fever victims. The unimaginably stoic recruits emerged in the pink of health. The human guinea pigs who stayed in a virtually sterilized room—where all domestic items had been disinfected by steam but where mosquitoes that had recently fed on yellow fever victims were let loose—sickened within days.
By 1910, scientists had worked out the life cycles of the bloodsucking carriers of dengue fever, typhus, Rocky Mountain spotted fever, African sleeping sickness, and other diseases. Still, in the 1930s, as many as 600,000 Americans got sick from the locally transmitted malaria. During World War II, the U.S. Public Health Service established in Atlanta, the heart of the American malaria zone, a unit called
Malaria Control in War Areas—largely to protect troops in training and assure the continued production of war matériel. Teams of doctors, entomologists, and engineers toiled together to tackle the problem, a mission soon expanded to include control of Aedes aegypti, the mosquito species that transmits yellow fever. From this wartime project grew the CDC.
Mosquitoes transmit viruses as part of an intricately choreographed dance in nature. To borrow a locution favored by post-structuralist academics, a mosquito’s success as a disease-bearer is highly “contingent.” It begins when a female mosquito bites a warm-blooded animal, usually a bird but sometimes a rodent or other animal. (And yes, it is always the female, who needs proteins in the animal’s blood for her eggs; male mosquitoes are content to dine on nectar.) Should the bitten animal—known as a “reservoir host” for the virus—be infected, the virus will enter the female mosquito’s gut, where it reproduces. The virus then travels to the mosquito’s other organs, including the salivary gland, where it multiplies some more. Within a few days of her original bloodmeal, the mosquito infects the next victim—human or otherwise—on which she feasts. She is known as the “vector,” or carrier, of the disease-causing virus. Humans have earned the sobriquet “dead-end hosts,” because they generally don’t carry enough virus in the blood to infect the next mosquito that bites them, which means the chain of transmission is cut.
But mosquitoes are not merely flitting hypodermic needles. They don’t promiscuously poke their proboscis into any inviting piece of flesh. Many, in fact, don’t bite people at all. They prefer particular species—those reservoir hosts, such as rodents or birds or other animals—that don’t get sick. For a few days, reservoir hosts develop high enough quantities of virus in the bloodstream (a condition known as viremia) to pass on the virus to any other mosquito that happens to bite. Mosquitoes themselves remain infectious for life. In a kind of viral chain letter, mosquitoes bite viremic reservoir hosts, which in turn infect more mosquitoes, which bite more animals. Transmission spirals higher and higher. The more a mosquito bites people rather than animals, of course—following with her antennae invisible plumes of ex-
haled carbon dioxide, body heat, and perhaps a special bouquet of lactic acid and other chemicals from a human target up to 100 yards away—the better the chance of spreading disease. Arboviruses’ most extraordinary trick is their ability to breed in both cold- and warm-blooded species, the upshot of viruses and their mosquito hosts evolving in tandem. So ingenious is arbovirus evolution, in fact, some viruses actually disable the mosquito’s salivary glands, making it harder for the insect to draw blood, so that it must probe many more hosts, spreading the virus far and wide.
All of which is to say there is an irreducible complexity and an inherent mystery in arbovirus disease outbreaks. So tangled are the factors that permit arboviral diseases to thrive—including temperature, rainfall, population densities of mosquitoes and victims, mosquitoes’ or animals’ susceptibility to infection, and human behavior—scientists haven’t been able to devise good forecasting models for outbreaks. “There have been a lot of very smart people working to predict risk of mosquitoborne disease for a long time,” says Roger Nasci, a research entomologist with the CDC. “Nobody’s even come up with the easy stuff.”
House to House
On Sunday morning, August 29, Marci Layton put through a call to John Roehrig, chief of the arbovirus diseases branch at the CDC’s outpost in Ft. Collins, Colorado. Ft. Collins is the World Health Organization’s arbovirus reference center for North and South America—a specialized lab to which other labs can send specimens to help them identify a virus or confirm a diagnosis. In his 20 years at the CDC, Roehrig had never received a weekend emergency call. Roehrig, after all, was a lab man. On this Sunday, he was preparing to watch a Denver Broncos preseason game.
Layton asked if the strange cases at Flushing Hospital could be caused by an arbovirus. Roehrig didn’t think so. Arboviruses don’t usually cause muscle weakness. Besides, there hadn’t been any outbreaks elsewhere in the Northeast.
By that Sunday afternoon, Layton and Fine had flushed out three more cases, all from the same Whitestone, Queens, neighborhood, bringing the official count to eight. Having already ruled out common summer viruses, Layton was starting to focus on St. Louis encephalitis virus: a mosquitoborne arbovirus never before diagnosed in New York City. First identified in the 1930s, SLE has since hopscotched erratically around the country, occasionally erupting in large, deadly outbreaks. Normally, the CDC gets 30 or so reports a year. In 1975, SLE shocked public health officials when it sickened more than 1,200 victims and killed 104 in the United States, mostly in the middle of the country.
If an arbovirus epidemic had alighted in New York City, it would be the first since the yellow fever days, two centuries earlier. But it wasn’t the epochal quality of mosquitoborne disease in New York City that would make a public health official quail—it was the practicalities. For starters, 7.4 million residents were susceptible. Mosquito spraying would have to start immediately. But New Yorkers, unlike residents in southern U.S. cities, never had to face the seasonal ritual of mosquito control—the spraying, the fogging, the daily squirts of mosquito repellent. Living alongside nature required a certain humility, a trait not prominent in the New York psyche. To top it off, New York City had years before abandoned its mosquito surveillance program. To scout out the vectors of SLE, the city health department had to borrow an entomologist from the venerable American Museum of Natural History.
On Wednesday, September 1, a woman named Varuni Kulasekera toured Whitestone, Queens, to search for mosquito breeding sites. Kulasekera specializes in the Culex pipiens mosquito, a drab brown bloodsucker commonly known as the northern house mosquito. In November 1998—nine months before Flushing Hospital’s mysteriously paralyzed patients—Kulasekera had received a call from the city on a different but equally curious matter. As the holiday season approached, residents on Manhattan’s old-money upper east side, not far from the mayor’s residence, Gracie Mansion, were complaining about
mosquitoes. Though snowflakes flew outside, people were running air conditioners to freeze out the buzzing menace, hanging gauzy fabric over their beds, and rubbing citronella on their skin at night. On the day before Christmas, Kulasekera stood in a snowstorm incongruously clutching a mosquito net. With a TV crew recording the action, city workers opened a sewer cover. Hundreds of mosquitoes swarmed out. Even in the whiteout, she recognized them instantly as Culex pipiens. “If they are still alive at this time of year,” she recalls telling a TV reporter, “then we have to be very careful next summer. We might have a new arbovirus outbreak.”
Kulasekera, 42, was something of an entomology prodigy. Having grown up in a well-to-do family in Colombo, Sri Lanka, she had rejected her parents’ expectations that she would become a doctor and instead followed her passion for insects—a passion kindled at age seven when she found an Atlas moth laying eggs on one of her storybooks. While her friends kept dogs and cats and parrots as pets, Kulasekera nurtured giant water beetles and water bugs in an aquarium, studying their life cycles. At a high school science fair, she displayed beetles, butterflies, and moths collected from her backyard. Her exhibit, which earned the school an award, was titled “Insects from My Garden.” After college, she did graduate work on rainforest mosquitoes, living in an open hut in the jungle. “I remember my uncle telling my mom, ‘You can never arrange a marriage for her.’ I was always an outcast. I used to dream about going to America.”
In 1986, Kulasekera did just that, joining the Smithsonian Institution. At the University of Maryland, she dove into what she laughingly calls the most “macho” field in entomology: systematics, which embraces evolutionary biology and taxonomy. The joke is that Kulasekera is a frankly, proudly glamorous woman, an effect abetted by high spiritedness. With large dark eyes and thick curly hair, a gold post in her right nostril, she carries off body-hugging short skirts and high-heeled sandals and dazzling accessories both in the lab and in the field. To cap the larger-than-life, only-in-New York effect, and the gender
joke, her husband happens to be the bassist for the quirky cult band Violent Femmes.
On September 1, Kulasekera inspected the Whitestone homes of the known encephalitis victims, looking for clues. After a mild winter and rainy spring, the summer of ’99 had been hot and dry. Culex pipiens, as it happens, likes drought conditions, which leave stagnant water with lots of organic debris. Septic tanks, rain gutters, and storm drains filled with rotting leaves offered plentiful nutrition to Culex larvae. In one backyard Kulasekera saw thick grass and bushes, an ideal site for Culex. Another home kept a birdbath, in which Kulasekera found mosquito larvae. At a third house, Kulasekera was puzzled to find no traces of mosquitoes—but in broken English, the patient’s wife explained that she and her husband often walked along the East River. When Kulasekera’s team rooted around where the woman had pointed, they found dozens of discarded tires hidden under straw, above which Culex laced the air.
Late that morning, Kulasekera knocked on the door of a fourth home, and an older woman came to the door. She and her family were about to drive to Flushing Hospital. There she would say a final goodbye to her 80-year-old husband—the man who had shared her life for more than 50 years—before asking doctors to remove a mechanical respirator. All their life together, he had been so glowingly healthy and robust that his wife had always assumed she would die before him. She escorted Kulasekera to the backyard. On one side was a brilliant flower garden, which the wife had tended. On the other was a lush patch of vegetables, which her husband had cultivated. Scattered around the yard were five-gallon white plastic buckets for collecting rainwater, her husband’s Good Samaritan gesture during the summer drought. Recently, the wife said, her husband had been suffering insomnia. To keep from waking her, he would sit outside in the middle of the night and smoke. Kulasekera dipped a ladle in a plastic bucket near the man’s chair. Floating on the surface were scores of Culex larval cases. In her report to the health department, Kulasekera described Whitestone, Queens, as the perfect ground zero for an SLE outbreak.
A Diagnosis
On Wednesday, September 1, the 80-year-old Good Samaritan passed away. The next day it was an 87-year-old woman, below whose second-floor apartment a nephew had also collected rainwater. By then, the New York state health department laboratory had found that blood and spinal fluid from the initial cases tested positive for St. Louis encephalitis virus. Because of the potential scope and public health implications of the outbreak, CDC–Ft. Collins would have to confirm those astonishing results before the city health department could announce the news.
To Marci Layton, the SLE diagnosis was a relief. In public health, infinitely worse than rushing into action against a known enemy is holding fire until one learns the enemy’s name. “It’s the not knowing,” said Layton, that keeps her up at night.
If it did turn out to be SLE, the city would have to set up a full-court press to stem the outbreak and reassure the public. With so many cases piling up—there were now more than 30—and a good percentage of those cases either dead or in dreadful shape, the virus looked to be extremely virulent. In a matter of hours, city officials would have to buy directly from the major pharmaceutical supply companies what would amount to nearly the entire national supply of insect repellent— a good half-million cans and bottles. They would have to prepare airplanes and helicopters and trucks to blanket the city with insecticide— while simultaneously securing permission from the state’s Department of Environmental Conservation to spray. They would have to build a website and set up a 24-hour public hotline and write educational flyers in eight languages. They would have to recruit hundreds of city workers to walk through neighborhoods to distribute those flyers. They would even have to make sure the mayor’s van was parked at ground zero in Queens, so that he could stage a press conference to announce the city’s response.
At 1:30 p.m. on Friday, September 3—the day before the Labor Day weekend—Layton got the CDC’s call: positive on SLE. Annie Fine
ran through the hallways on the department’s third floor, shouting like Paul Revere, “It’s positive! It’s positive!”
At 3 p.m., Mayor Rudolph Giuliani held a press conference, trying to wrap his rhetoric around an unaccustomed topic. (A week later, he was more pithy and assured: “The more dead mosquitoes, the better.”) Within hours, helicopters began spraying in northern Queens, close to the Whitestone Bridge, where the first fatalities had lived. After the press conference, which Annie Fine attended, neighborhood residents walked up to tell her they’d seen a lot of dead robins and crows in the area, and asked if it could have anything to do with the human cases. Fine didn’t know. That evening, she helped staff the public hotline during its first hours of operation. A woman calling from Queens had also complained about dead birds, and mentioned a Queens Chronicle article on the avian epidemic that had just run. Fine asked her to read it over the phone. The story described dead birds not just in Whitestone but in Manhattan, the Bronx, Long Island, and Westchester County. Two weeks earlier, a Chronicle article on the dieoff had led with a question: “Has a plague hit the Bayside area?”
Fine felt a shiver of fear. If the bird deaths were related, it suggested a much bigger human outbreak than the one seemingly confined to a small peninsula in northern Queens. As if to confirm her apprehension, human cases had turned up just hours before in the Bronx. That night, Fine called city and state experts to ask if the bird deaths could be tied to the human cases. They repeated the conventional wisdom—SLE doesn’t kill birds—and she tried to put the matter out of her mind.
What Fine didn’t know was that crows had been dropping for months. During the previous decade, the city’s crow population had steadily mounted as warmer winters invited the scavenging birds to stick around. Now, in every borough, these raucous urban denizens were suddenly lifeless and littering the sidewalks. Since June, a veterinarian at a clinic in Bayside, Queens, had been treating eerily docile corvids. One woman brought in a crow perched on her shoulder like a parrot. At Ft. Totten, a Civil War battlement in Queens, guards found
crows stumbling around as if drunk. That August, highway crews had hauled into the state’s Department of Environmental Conservation plastic bags filled with the glossy black bodies of more than 400 dead birds.
Marci Layton and Annie Fine live near each other in a brownstone area of Brooklyn. That night around 2 a.m., after nearly 24 hours of nonstop frenzy, they sat on the stoop of Fine’s apartment building. “I remember us hugging and almost crying,” Layton said, “because we had been there from the beginning together. I said, ‘I know it sounds crazy, but I am so relieved.’ Because I knew what it was. I knew what to do.”
Fine also felt exhilarated. This is what a public health professional dreams of: to catch the wave of a big outbreak. But even in her exhilaration, something didn’t feel right. The dead birds. Had a plague hit New York City?
Second Epidemic
On August 9, 1999, three days before Deborah Asnis had seen her first puzzling encephalitis patient, Tracey McNamara, head of the pathology department at the Bronx Zoo, had begun noticing dead crows on the zoo’s grounds. As McNamara knew, it takes a lot to kill a crow. Connoisseurs of everything from restaurant scraps to road kill, they are able to fend off most pathogens in nature. So hardy is this species, wildlife disease archives had never recorded a crow die-off in the United States. McNamara sent some of the crows to the state’s Department of Environmental Conservation. For two weeks she phoned, eager to hear the results of laboratory tests on the birds. As it turned out, no one had performed lab tests. The state’s pathologist simply cut open the bodies and examined them superficially. He told McNamara he found signs of metabolic bone disease—certainly nothing that could explain a die-off.
As the weeks passed, more dead crows turned up on the zoo grounds. Then some of the zoo’s pheasants started to show
neurological oddities. Worried, McNamara launched her own laboratory investigation. She cut sections of brain, heart, and other organs. She made tissue slides, performed bacterial cultures and stains and toxicology tests. She froze tissue, embedded it in paraffin blocks, submerged it in formalin.
She went through these paces because, in an age in thrall to molecular biology, the distilling of disease down to the level of genetic switches, McNamara resolutely practices old-fashioned pathology with a Zenlike concentration (away from the office, she’s a glass-blower and Buddhist meditator). “I cannot make any assumptions. I look at every tissue every time. Every animal that dies in our facility receives a full postmortem.” Such is the culture of veterinary pathology, a throwback to the earlier era of the generalist, not the specialist. “Expecting the unexpected is a routine part of our job,” she said. “To be a good pathologist, you need a fundamental level of humility, to be able to challenge your own diagnosis. You have to have a sense of inner stillness. The mental discipline to observe and not jump to conclusions.” When her initial examination uncovered subtle brain lesions, she concluded she was looking at a viral encephalitis and continued the postmortems.
On September 3, McNamara heard news reports about St. Louis encephalitis in the city. That Labor Day weekend, she pored over textbooks and filled several legal pads with notes. The books repeated what she and apparently everyone else already knew: birds don’t die of SLE. And flaviviruses—the group that includes SLE—had never been a veterinary problem. Yet she was sure that what was happening in humans was linked with what she was seeing on her laboratory slides. “Encephalitic people, encephalitic birds,” she said. “Could there be a connection? I didn’t have to think about it too long.”
And luckily, she didn’t. Her hunch led her to the most crucial evidence in the outbreak, the key that could have unlocked the mystery weeks earlier than it was solved, had she not been dismissed as, in her own stung interpretation, “some dingbat, premenopausal female veterinarian in New York City.”
Large and energetic, her blond hair combed back in a practical style, sharp green eyes registering everything from behind dark-rimmed glasses, McNamara has natural comic timing. Described by her peers both as “brilliant” and as “entertaining”—not a common adjectival pairing in the scientific world—she tends to shoot from the lip, which both catalyzed and scandalized the new community of scientists that would soon surround her.
McNamara’s earliest childhood memory is of visiting the Central Park Zoo with her parents. In those days, the 1950s, the director of the zoo reared a Kiplingesque black panther and even walked the cat on a leash through the park. When McNamara walked up to his cage, the panther was pacing back and forth. “I said ‘Bagheera?’ And the cat just stopped in his tracks and came up to the front of the cage and looked at me. That was it.” At age three, she had fixed on her life’s work. During college, after a detour into French literature, McNamara took off for Kenya to labor free for a team of wildlife researchers. At first, they turned her down, for lack of experience. “I sat outside of people’s doors for eight hours a day. I wore ’em down. I just wouldn’t take no for an answer.” Eventually, she found herself rattling across the savannah on the back of a pickup truck, helping out on a study of giraffe physiology.
By 1999, at the age of 45, McNamara had risen to the top of an elite professional cadre. She is a veterinary pathologist specializing in wildlife diseases, one of perhaps ten such doctors of veterinary medicine in the country. “Veterinarians enjoy this reputation of James Herriott,” she said. “You know: all creatures great and small, veterinarians take care of them all. Well, baloney. The reality is more like George Orwell’s Animal Farm: all animals are created equal, but some animals are more equal than others. For centuries, the emphasis has been on domestic species, on the economically important species. As a result, even today in the veterinary curriculum, more time is spent on the dog and the cat than on the whale or the bat.” Diagnosing diseases of wildlife—animals that are literally no one’s business—places one on the scientific frontier. Or perhaps outback. Much of what wildlife
pathologists see, they are seeing for the first time. At her office in the Bronx Zoo (now formally known as the Wildlife Conservation Society), McNamara receives samples from field researchers all over the world. She discovered a herpes virus in Malayan peacock pheasants, a cerebral fungus called Cryptococcus in the common anaconda, and a pox virus in South American ruminants known as pudu.
On September 7, the day after Labor Day, McNamara arrived in her office to learn that a Chilean flamingo and a Guanay cormorant had died and more zoo birds appeared sick that morning. The zookeepers were upset—they knew these animals like friends. McNamara performed immediate postmortems. In the flamingo, she found massive myocarditis (“heart transplant city”), in the cormorant extensive hemorrhaging in the cerebellum. “The most frightening lesions I have seen in sixteen years as a comparative pathologist,” McNamara says. “Hair stood up on the back of my neck . . . I could feel in my bones it wasn’t anything that any of us knew.” Whatever was killing the birds, it looked “hot”—lethally infective. Donning a respirator mask and goggles, a disposable jumpsuit and three sets of gloves, she proceeded to do her handiwork under a filtered-air hood. With a new razor blade, she cut fine sections of the fresh, Jell-O-like organs. She took impression smears—a kind of outer cell scraping of the organs, from which a pathologist can quickly characterize cell damage. She took three sets of tissue samples from every organ. She prepared 40 tissue slides for her technician. The next day, the technician called her out from the necropsy suite. Peering at wet sections of tissue sliced 6 microns thick, she saw “the worst meningoencephalitis I have ever seen. And meanwhile, I have more dead birds in the cooler. I have a pheasant with massive cardiac necrosis and hemorrhage. I have a snowy owl with acute coagulative necrosis in the liver. I have two flamingoes on September 9 with GI lesions.” McNamara was desperate. The zoo had never seen anything like it: birds from distant evolutionary lineages apparently struck down by the same disease. Over the next few weeks, 24 zoo birds would die or be euthanized. The victims would include black-billed magpies, bronze-winged ducks, a northern bald
eagle, and a black-crowned night heron. Most had unmistakable central nervous system damage. One flamingo craned its neck low in a weird S-shape. Others staggered on wobbly legs. Laughing gulls drooped their heads. A cormorant swam deliriously in circles.
McNamara mulled the problem like a detective sifting clues, drawing on both logic and intuition. Her thinking went something like this: It could be avian influenza or Newcastle’s disease, but those didn’t quite fit the lesions she was seeing. Besides, those viruses wipe out chickens and turkeys—but in the children’s zoo, the farm birds were doing just fine. Maybe it was an alphavirus, of which the most likely would be Eastern equine encephalitis. EEE, which can be fatal to humans, is mosquitoborne, and McNamara knew the zoo was having a mosquito problem because there had been cases of avian malaria. But EEE is notorious for killing emus, an Old World species, and the zoo’s emus were thriving. What most bothered McNamara was that the only birds the zoo was losing were North and South American species. Normally, those would be the very species that would survive and act as reservoirs for the known arboviruses of the Western hemisphere, such as St. Louis encephalitis.
On September 9, McNamara phoned the CDC’s offices in Ft. Collins. She had a pressing concern on her mind: one of her veterinarians had stuck himself with a needle while euthanizing a flamingo. Surmising that the animal and human outbreaks were related, she wondered: What kind of strange infection might he have caught? But she also wanted the CDC to know that the resonance between SLE in people and what was killing her avian charges was striking, and that exploring one might yield clues to the other. McNamara asked CDC to test serum from the veterinarian who had stuck himself and plasma from the dead flamingo. A biosafety officer in Ft. Collins flatly turned down her request, in part because birds weren’t the CDC’s business or subject of expertise. As McNamara remembers, “He cut me off in midconversation and said, ‘Birds don’t die of St. Louis encephalitis. Birds are a reservoir for St. Louis encephalitis. And you should know better. You’re just dealing with some veterinary thing.’” McNamara’s jaw dropped. She sent the serum anyway.
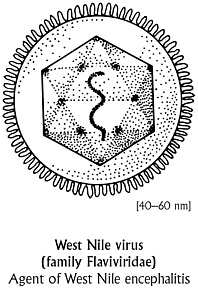
That day, McNamara also called the National Veterinary Services Laboratory, in Ames, Iowa, part of the Department of Agriculture. Since their purview was animals, would they test her specimens for encephalitis viruses? To her relief, NVSL said yes. That weekend, their lab workers called McNamara at home. The zoo’s specimens were negative for Eastern equine and other alpha viruses. But something was growing in their cultures—something they couldn’t identify. A few days later, when the NVSL called again, McNamara was in the zoo’s necropsy suite, wrist deep in more postmortems. She pulled off a glove and grabbed the phone. The mysterious virus had finally started growing. Under an electron microscope, it looked to be about 40 nanometers in diameter: too small for an alphavirus like Eastern equine encephalitis, but just right for a flavivirus such as St. Louis or others. The NVSL didn’t have the technology to further pinpoint the virus.
McNamara felt flushed with triumph. Her intuition was right: there was a connection between the bird and human cases. “That validation of diagnostic skills. Everything I’d ever studied, everything I’ve ever been trained to do—it paid off. It was right.” But after that surge of elation came a jolt of fear. Maybe it was SLE or maybe it was a more dangerous viral cousin. Suddenly it dawned on her that she was slicing up tissue loaded with an unknown flavivirus, and that she was relatively unprotected.
McNamara quickly phoned Ft. Collins to tell them about the NVSL’s discovery of an unknown flavivirus in the zoo’s birds. By now, three of her lab workers had stuck themselves with needles, and she was frantic to know exactly what might have infected them. Birds were piling up in her cooler. Her lab looked like a field hospital in the midst of what public health officials had declared a war zone. Yet despite her best efforts, she couldn’t talk to the generals.
Lab Work
In the fall of 1999, the list of identified arboviruses numbered 538. Of this list, those known to cause human disease ran to 110, and most
had niches far removed from the United States. And for these 110, diagnostic tests existed for fewer than 30.
When the New York City epidemic broke out, lab workers at CDC–Ft. Collins did the practical thing: they tested for the viruses most likely to strike in that geographic area. In early September 1999, the protocol was to initially look for four arboviruses: LaCrosse, Powassan, Eastern equine encephalitis, and St. Louis encephalitis. And that’s just what Robert Lanciotti did. Lanciotti, a tall, broad-shouldered man with reddish hair and a faintly military air, directs the branch’s diagnostic and reference labs. He is respected as a calm, methodical professional, the kind of person you’d want around during an outbreak.
When he received serum and tissue from the first group of patients diagnosed in New York City, Lanciotti ran a blood test known as an IgM and IgG ELISA. IgM is the antibody the immune system produces when a person is acutely ill. According to the textbooks, IgM appears a few days after an illness begins and sticks around for 30 to 45 days or more, then vanishes. By contrast, IgG antibody persists for a lifetime. If somebody is IgM negative and IgG positive for a particular virus, it means the person was infected at some indefinite point in the past. When Lanciotti tested the New York City samples against a battery of four Eastern viruses, the sample came back both IgM and IgG positive for St. Louis encephalitis, the most widely reported mosquitoborne disease in the United States. He considered it a “presumptive case of St. Louis.”
It was “presumptive” because SLE is a flavivirus, and since the 1950s scientists have known about a peculiar hitch in antibody testing for flaviviruses. Far-flung and powerful, like a viral Mafia, the flavivirus family includes the agents that cause yellow fever and dengue fever. (A distant flavivirus cousin, the deadly hepatitis C virus, never evolved in arthropods.) Like a dutiful clan, flaviviruses sport nearly identical proteins on their surfaces. As a result, they cross-react to antibodies targeted for other family members—meaning that serum containing one flavivirus could easily come up positive in tests for other flavivirus kin.
Years ago, virologist Karl Johnson described the problem as a “hall of mirrors.” When Rob Lanciotti got a positive result for SLE, all he knew for sure was that the New York City patients were infected with some sort of flavivirus. The typical confirmation is known as a neutralization test, which reveals whether antibodies in a patient’s serum actually attack the live form of the suspected virus. The CDC began its neutralization tests, which take a week or two for flaviviruses, at the beginning of September.
Serum antibody tests are good in a pinch. But the gold standard for identifying a human virus is to grow it in other mammalian cells, such as monkey cells or in a chicken egg—a technique known as virus isolation. After that, the virus can be pinpointed with antibody or antigen tests, or with polymerase chain reaction, which amplifies sections of the genome. Unfortunately, the CDC was never able to grow the suspected virus from the clinical samples it had received. Nor had lab workers expected to. By the time symptoms have begun, there aren’t a lot of virus particles left in the bloodstream to grow.
Publicly, the CDC and local health agencies were sticking with the SLE diagnosis. But privately, as September wore on, the diagnosis started to look shaky. One problem was Ft. Collins’s serologic tests on new patients’ blood samples: the IgM assays—which signal acute infection—looked suspiciously weak. At the New York City health department, those results bothered Marci Layton. She kept quizzing John Roehrig about their meaning. How can we be sure, she asked him, that we’re really dealing with St. Louis encephalitis? Meanwhile, CDC officials were learning of dead birds not just at the Bronx Zoo but all over New York City. For weeks, the health department’s Annie Fine had been asking CDC officials if the human and bird deaths could be related. Derisively, they cut her off. Feeling like a pest, she eventually stopped bringing it up. But CDC officials were bothered enough to call the nation’s leading arbovirologists to ask whether SLE had ever been known to kill birds. (Rarely, said the experts.) The pieces of the puzzle were not fitting.
Finally, in the third week of September, the puzzle pieces assorted themselves neatly—into a new picture. First, the CDC learned that the
NVSL had isolated a flavivirus from Bronx Zoo birds; that bolstered Tracey McNamara’s suspicion that what was killing her charges might be killing New Yorkers. Early the same week, the Connecticut Agricultural Experiment Station announced that it had isolated a flavivirus from an encephalitic crow and from two pools of mosquitoes; that evidence drew a stronger thread, since presumably the infected mosquitoes were biting both birds and humans. But were those mosquitoes infected with SLE or something else? When Marci Layton and Annie Fine heard the Connecticut news, “Lights started going off in both our brains,” Fine recalls. Their persistent doubts about the SLE diagnosis seemed borne out. Later that week, researchers at the U.S. Army Medical Research Institute of Infectious Diseases, or USAMRIID—to whom Tracey McNamara had sent specimens as a last resort—also found a flavivirus.
On Monday September 20, the NVSL sent their Bronx zoo virus isolates to the CDC. To pinpoint the virus’s identity, Lanciotti ran two kinds of genetic tests simultaneously. In one, he used assays that broadly react with either all flaviviruses (such as SLE) or all alphaviruses (such as EEE), or with a third group known as bunyaviruses. In the other, he ran genetic tests that specifically ferret out SLE and EEE. The results baffled him. The broad tests ruled out alphavirus and bunyavirus, and ruled in flavivirus. Yet his test for St. Louis encephalitis came back negative. It didn’t make sense. Lanciotti wondered if he was dealing with a strange variant of SLE.
Lanciotti then tried a different tack, comparing a patch of the virus’s nucleic acid sequence against the sequences of all known flaviviruses. On Wednesday, September 22, he loaded samples of the virus genome into a machine that automatically sequenced the DNA strands. That evening, to take his mind off the problem, he played golf with some colleagues. The next morning he arrived at work at 6:30, anxious for an answer. Around 7 a.m., he submitted strings of genetic code over the Internet to the National Library of Medicine’s GenBank, a database of all publicly available genetic sequences. Ten seconds later, the match flashed on his computer screen: West Nile virus.
A bolt of heat shot through Lanciotti’s body. His heartbeat sped
up and he became drenched with sweat. “It was absolute shock and horror. I took that data and literally ran upstairs to my boss, and we ran together up to the division director.” Duane Gubler directs the CDC’s division of vectorborne infectious diseases. An old hand in arbovirology— fieldwork on dengue and parasitic diseases in more than 100 countries—he thought he had seen everything. Hearing the news, all the wisdom he could summon was, “Holy shit.”
Global Imports
West Nile virus in New York City. The news was shocking in part because, in all the thousands and thousands of words poured into scientific papers and government guidelines and prolix draft documents of all kinds—all those seers scouting out emerging infections on the horizon—West Nile virus had never come up. That, of course, is the underlying message in emerging infections: they are impossible to predict. West Nile virus, which usually causes only a feverish, flulike illness, isn’t the most dire threat from the insect or animal kingdom— Ebola in Queens easily trumps it. But its breathtaking leap across continents is a reminder of just how mobile today’s pathogens are. What scares experts is that it’s a preview of more dire things to come.
If you were to unfold a map, close your eyes, and point, virtually any place at the tip of your finger can be reached within 36 hours. That’s less than the incubation period—the time between infection and the onset of symptoms—for most infectious diseases. In other words, an infectious agent can slip in and spread before its symptoms
give it away. As cartoonist Gary Larson depicted the situation, “Be a virus, see the world.”
Germs are natural vagabonds. Take an epidemic that hit the United States precisely one century before West Nile did. On June 27, 1899, the S.S. Nippon Maru had sailed through the Golden Gate into San Francisco harbor. Weeks earlier, after the ship had left Hong Kong, two passengers had come down with bubonic plague. By the time the vessel arrived at its stopping-off point in Honolulu, plague-infected rats were scurrying through the holds. In San Francisco, officials quarantined the vessel, though no passengers had shown any signs of illness. While inspecting the ship, however, officials found 11 Japanese stowaways. Within hours, two of those stowaways were missing. Their sodden corpses, clad in life preservers from the Nippon Maru, were later fished from the Bay—full of plague bacilli. Nine months later, San Francisco ushered in the Western Hemisphere’s first epidemic of bubonic plague. On March 6, 1900, a body turned up in the basement of a Chinatown hotel. Despite a massive sanitary campaign by fumigation, sponging, and washing, the outbreak lasted four years and killed 112 individuals, mostly Chinese. After the 1906 earthquake, the city’s rat population exploded and a second epidemic unrolled. So just a century ago, sailing ships were the distribution channels for bubonic plague’s last global pandemic.
Killing 60 to 90 percent of its victims before the antibiotic era, plague had spurred some of the earliest public health laws in Europe, including quarantine of incoming vessels and isolation of victims. Throughout history and up to today, the idea of preventing infectious disease by corralling sick people has had its appeal. In turn-of-the-century San Francisco, the local board of health responded to the plague outbreak with what we would consider impractical, not to mention racist, measures: stretching a rope around the twelve-block Chinatown and stationing police along the line to keep the stigmatized residents inside. Similarly, during the yellow fever epidemic of 1793, bands of vigilantes in New York City patrolled the streets at night to prevent potentially tainted Philadelphia fugitives from slipping in.
But today, neither ropes nor vigilantes, electric fences nor the Marines, can close the door on imported infections. New York City is a pulsing intersection. Between 1987 and 1997, the number of international passengers and cargo flights to and from airports serving the city doubled. In 2000, fully 40 percent of the city’s population had been born abroad, the highest percentage of foreign-born residents since 1910, when waves of immigrants surged through the halls of Ellis Island. Across the United States, tens of millions of foreign-born travelers enter each year, along with one million legal immigrants and refugees and several hundred thousand illegal immigrants—many from countries where infectious diseases are rife. Worldwide, more than 1.4 million people travel across international borders by air each day— more than 500 million travelers each year, a figure that grows by 10 percent a year. Though immigration opponents may lean on the cruel stereotype that “foreigners” bring in disease, the fact is that everyone who travels, including affluent U.S. tourists, can bear bacterial, viral, and parasitic gifts.
In a time of unprecedented travel and trade and transport, West Nile virus was just another tourist. And though it captured the headlines during the summer and fall of 1999, another disquieting import had arrived in its shadow. That summer, at Baiting Hollow Boy Scout Camp, a hilly, wooded site bordered by wetland on Long Island, two 11-year-old boys came down with malaria. Not having traveled outside the United States, the boys could only have acquired the disease from the bite of an Anopheles mosquito. And the mosquito could only have become infected by biting, about two weeks before, someone as close as half a mile away who had harbored in his or her bloodstream the mature male and female stages, called gametocytes, of the malaria parasite—in this case, Plasmodium vivax. Someone experiencing a relapse of the disease years after the initial infection can host malaria parasites in the bloodstream for days or weeks, never experiencing symptoms. In this case, investigators never found that human source, almost certainly a visitor or immigrant from a malarious country.
Nor did public health officials ever find the source of a 1993 ma-
laria outbreak in Queens, that sickened two and perhaps three people who lived within a mile of each other. In those cases, the agent was Plasmodium falciparum—the deadly strain of the infection that kills 3,000 people worldwide every day. Many immigrants in the Queens neighborhood had arrived recently from malaria-endemic areas, including parts of South and Central America. What bewildered officials was that crowded urban areas are usually uncongenial for Anopheles, which prefers clean, slow-moving water. Each year, one or two such outbreaks pop up in the United States, often where the victims are homeless or living in substandard housing, and thus easier targets for mosquitoes. Just as well-documented is the phenomenon of malariainfected mosquitoes riding in the cargo holds and wheel wells of jets traveling from tropical to temperate countries, and on their escape biting the first hapless victims they can find—inspiring the terms “airport malaria” or “baggage malaria.” (France, host of stowaway mosquitoes from West Africa, is the world’s airport malaria leader.)
As a New York Times writer put it, “If the indestructible cockroach is the Sherman tank of the insect kingdom, the fragile mosquito is its DC-7, a pioneer in linking the world by air.” West Nile virus certainly illustrates that. First discovered in the blood of a fever-ridden woman in the West Nile district of Uganda in 1937, West Nile virus had been tracked in Africa, the Middle East, and western Asia (where, because the disease is endemic, most people become immune in childhood). The branch of the flavivirus family to which West Nile belongs—known as the Japanese encephalitis virus antigenic complex— includes the Japanese encephalitis virus in Asia, Murray Valley encephalitis virus and Kunjin virus in Australia, and SLE in the Americas—distinct geographic niches that have recently expanded and blurred.
But because vectorborne pathogens have become jet age gypsies, what’s more surprising than West Nile’s arrival is that other diseasecausing agents didn’t show up here first. Scientists have long been on alert for other pathogenic rovers—and they still can’t quite believe a relative unknown like West Nile, which wasn’t even on the racing card,
crossed the finish line first. Take the virus behind Japanese encephalitis, or JE, which causes symptoms ranging from fever and malaise to convulsions and coma, killing 25 percent of its victims. Once confined to Asia, it has leapfrogged to New Guinea, Australia, and elsewhere in the Western Pacific. During World War II, U.S. officials anxiously monitored the movement of men and matériel from Japan to the West Coast, fearful that the virus would sneak in—or that the Japanese would infect mosquitoes, stow them on one of their submarines, and surface near the United States just to let them loose. During today’s peacetime trade, mosquitoes or mosquito eggs from Asia could easily carry in JE, where the virus would then become amplified in birds, as had West Nile virus. In 1998, scientists cringed when they found the Japanese mosquito Aedes japonicus in the United States (though, like the notoriously spreading Asian tiger mosquito, Aedes albopictus, it probably had arrived earlier, in mosquito eggs deposited in old tires sent here for retreading). “It’s just dumb luck that those things were not infected with Japanese encephalitis virus,” says University of California–Berkeley arbovirologist William Reeves Sr., “because it can be transmitted from a female mosquito to its progeny.” If JE did arrive in the U.S., as many as 30 native mosquitoes could tote it around—and with that many different vectors, eradication would be impossible.
Or consider Rift Valley fever virus, which causes fever, shock, and encephalitis. It could hitch a ride on a viremic person or an infected mosquito from Africa or the Middle East, and would almost surely go on to cause human deaths as well as epidemics among cattle and sheep. In 1977, when the virus jumped from southern and eastern Africa to Egypt, it was said to bear an uncanny resemblance to the biblical description of one of the plagues of ancient Egypt, with more than 200,000 cases and 600 deaths. In 2000, to the dismay of scientists, Rift appeared for the first time outside Africa: in Saudi Arabia and Yemen, now threatening the Arabian peninsula. Could this virus or some similarly undesirable relative come to the United States? “I can’t tell you when, but it will,” says legendary virus hunter C. J. Peters, now at the University of Texas Medical Branch at Galveston. Citing the propensity of animal pathogens to seek new niches, he says, “If we can have
BSE and foot and mouth disease in Britain, and we can have Nipah in Malaysia, and we can have Rift Valley fever in Egypt and in Arabia, what’s different about the U.S.?” An intervening ocean, as well as strong animal quarantine laws, have kept this country safe so far. “But I don’t think we can count on blind luck always.”
Ross River virus proved in the 1980s that it could escape its niche in Australia to erupt in Fiji and Samoa (probably in a viremic person), where it triggered massive epidemics of fever and arthritis. “Just by luck,” says virologist Tom Monath, “nobody got on an airplane” to the United States. If someone had, salt marsh mosquitoes on the coast could spread Ross River virus, as could Aedes aegypti and Aedes albopictus, now buzzing over half of the U.S. If Murray Valley encephalitis virus jumped from Australia to, say, California, Culex mosquitoes, like taxis lined up at LAX, would be ready to transport it.
Not all itinerant arboviruses come to us via mosquitoes from animals. Some are transmitted by mosquito from person to person, with no animal host in the middle, a simpler cycle that makes them potentially more threatening. Dengue fever, the excruciating pain of which has earned it the epithets “breakbone fever” and “devil’s crunch,” is caused by four closely related tropical flaviviruses; at their worst or when different serotypes cause serial infections, they can trigger massive hemorrhaging or circulatory collapse, especially in young children. The rise of dengue is a modern public health morality tale. Starting in the 1940s, the Pan American Health Organization was determined to eradicate its host, Aedes aegypti, from Central and South America—a campaign mainly driven by worries about yellow fever. Unfortunately, the United States never signed on to the effort—several cost–benefit analyses concluded that in a disposable society like ours, the price of cleaning up tire dumps and junkyards was too high compared to the public health gain at home. As a result, whenever a country was successful in eradicating aegypti, the United States ended up reintroducing it. Aedes aegypti eventually reclaimed North and South America, spreading dengue further than ever and setting the stage for several strikes across the Mexican border into Texas.
But what most worries U.S. scientists is the possible importation of yellow fever, whose mosquito vector is also the thriving A. aegypti. Today, the disease strikes about 15,000 victims each year in the tropical regions of South America and Africa. In South America, yellow fever is relegated to the jungle, in a cycle involving mosquitoes and monkeys. Public health officials fear that an infected person—say, a farmer cultivating coca in the jungles of Colombia—could act as a bridge between jungle and city. In a big-city hospital, the patient could infect Aedes aegypti, and that could springboard the virus around the world. “It’s not a matter of whether, it’s a matter of when we begin to see urban transmission of yellow fever again,” says the CDC’s Duane Gubler. “I did a little exercise to find out where a person could go from Santa Cruz, Bolivia—where we had some urban transmission a couple of years ago—and it’s everywhere. Asia and the Pacific are probably the most important destinations. Even if we don’t see major epidemics, I see this as probably one of the next international public health emergencies. You can get on a plane from Santa Cruz and be in Manila or Hong Kong or Bangkok within thirty, thirty-six hours.”
Or the United States in even less time. It takes just one infected person to spark an epidemic. In September 1999, as West Nile was seeding itself in American birds and in American paranoia, the U.S. nearly faced just such a crisis. After a 10-day trip to the rainforests of southern Venezuela, a California man—who, unlike his travel companions, had neglected to get a yellow fever vaccination before his trip—returned with fever and chills, blanketed with mosquito bites. Days later, he died a ghastly yellow fever death: seizures, lung failure, and fulminant hepatitis. Luckily, he didn’t dispatch the disease to anyone else. But if, during the virus’s incubation period, an American tourist in South America had been bitten and returned home—say, to New Orleans—the South could host the first U.S. yellow fever epidemic since 1942. Once that epidemic began to smolder, doctors would probably diagnose it first as infectious hepatitis, because patients’ skin would be yellow with jaundice. A pathologist would catch the disease during an autopsy—but since very few deceased patients get autopsies
today, several weeks could pass before anyone noticed that yellow fever was in our midst. By that time, squadrons of infected mosquitoes would have spread the infection. Although a vaccine is effective, only about one million doses are on hand in the United States—not nearly enough to put out an urban wildfire—and it would take months before a drug company could gear up production for more. Some scientists say the same advantages of modern living that protect us from dengue fever—window screens, air conditioning, prime time TV— would limit the spread of yellow fever. But others fear a sudden yellow fever outbreak could kill 5 to 10 percent of a city’s residents. “It would be about equivalent to what happened in 1918 when we had influenza,” says University of Texas Medical Branch arbovirologist Robert Shope, “and everybody knew somebody who died.” Or, to put it in a modern tense, it would be about equivalent to what people in poor and neglected countries face every day.
Breaking the News
When CDC officials in Atlanta heard that West Nile had landed on our shores, they grilled Rob Lanciotti about his lab technique: Any chance of contamination? No. Ft. Collins officials phoned Tracey McNamara at the Bronx Zoo. She was in the necropsy suite, as she had been for weeks, cutting up more dead birds. Without revealing that the CDC had identified the virus in her flamingo samples as West Nile, they politely asked her for more bird tissues—FedExed on dry ice, that night, if it was no trouble. McNamara was glad she had finally raised the agency’s interest, though she wondered why it had taken so long.
By Friday morning, September 24, investigators in the New York City health department were brimming over with excitement. What exactly had struck their city—a weird new form of SLE? another deadly flavivirus? an enigmatic flavivirus called Rocio, which had killed people and birds in Brazil in the 1970s, then just as mysteriously disappeared? Just when they thought their SLE investigation was winding
down, the roller coaster looked like it was about to climb another hill. Dozens of people joined in on a 10 a.m. conference call as CDC notified state and local health officials of the shocking new diagnosis. Duane Gubler opened the discussion by jokingly asking if everyone was sitting down. Gubler informed the group that four birds in New York City—three from the Bronx Zoo and a crow from Scarsdale— had died of what the agency called “West Nile–like virus,” to which humans might well be succumbing as well.
Unbeknownst to the CDC, an acquaintance had tipped off Tracey McNamara to the news. Realizing that her bird specimens had unlocked the mystery—samples she had tried in vain for weeks to have tested—she phoned a contact at Ft. Collins, playing dumb, asking how the investigation was going. As it turned out, she had called just in time to log into the conference call. After CDC officials delivered the news, there was a brief pause. McNamara jumped in. “Ladies and gentlemen, my name is Dr. McNamara,” she started out. “I’m a pathologist at the Bronx Zoo. And these are my cases we’re discussing. Would anyone care to hear the facts?” A meticulous note-taker, she proceeded to read from a log/calendar that she had been keeping since early August: whom she had called, what she was told, where and when she sent specimens. When she was done, she heard a a collective gasp on the line. Annie Fine, who had never heard of McNamara, was dumbstruck. Just a few miles from the health department’s headquarters, someone had been holding the key that could have unlocked this public health mystery weeks earlier. For her part, McNamara worried that the Bronx Zoo would be publicly identified as the hot zone epicenter of the outbreak, even though dead crows from all over the state had been turning up as early as July. If so, visitors would stay away from the park in droves. Sure enough, that weekend, after the news hit the press about West Nile–infected birds from the Bronx Zoo, the park lost hundreds of thousands of dollars of business. “You guys play hardball,” McNamara told herself. “I’m in the big leagues now.”
Later that day, in a fine bit of understatement, Duane Gubler told the New York Times, “This is exciting. We prefer it didn’t occur, but it
is interesting.” Luckily, the textbook public health retaliation, which New York City had been practicing for three weeks, was the same for both SLE and West Nile: spraying pesticide to kill adult mosquitoes, eliminating potential mosquito breeding places, applying larvicide to collections of standing water, and advising people to avoid mosquito bites. What public health officials didn’t know at the time was that the human outbreak was actually over; the last reported patient had become ill on September 22.
Sneaking In
West Nile virus in America: the finding stirred the blood of nearly every scientist in the country’s small corps of arbovirologists and medical entomologists. One was Bill Reeves, now emeritus professor at UC– Berkeley. Back in 1941, Reeves and his team were the first to isolate St. Louis encephalitis from mosquitoes in nature. He was the first scientist to use dry ice to help attract mosquitoes in the wild, now a standard technique. “You know the old story of Dalmatian dogs that live in firehouses?” Reeves said. “When the gong goes off, the Dalmatian runs over and jumps on the firewagon because he doesn’t want to miss that car ride. My reaction was very much like the Dalmatian. I wanted to get involved. It sounds silly. I’m 83 years old. I’ve been retired for 13 years. But when something like this comes, it’s like the good old days.”
In dog breeding and public health investigations, pedigree counts. To find out where New York’s strain of West Nile virus came from, researchers drew a genetic family tree with help from French researcher Vincent Deubel. The strain that hit the United States was nearly identical to one found in 1998 in a farm goose in Israel. Israeli geese probably caught the virus from migrating birds such as storks, whose annual excursions can take them from the northern tip of Europe down to South Africa. (Superimpose a map of stork migration routes over Old World locales where West Nile epidemics have popped up recently, and the overlap is striking.) So while discovered in Israel, the New York strain may have originated anywhere throughout the Mideast and even Africa.
Whatever its provenance, how did the virus beat a path to New York City?
We’ll never know. “It’s a series of unlikely events—each of which requires a series of unlikely events,” says USAMRIID entomologist Mike Turell. The main schools of thought nominate mosquitoes or humans as the transatlantic smuggler.
Mosquitoes, as we’ve seen, can survive on airplanes and breed on ships. Once in New York, an infected mosquito, like most famished tourists, probably dined at the first establishment that looked inviting—maybe a crow—which in turn infected other mosquitoes, inexorably amplifying the virus. Playing on the notion of “airport malaria,” Turell believes the outbreak began as “airport West Nile.” And he suspects it wasn’t the first time the virus sneaked in. Other infected mosquitoes may have entered from Israel or elsewhere in the previous year, only they couldn’t spread the virus. Maybe they were eaten by a dragonfly. Maybe they were caught by a spider. Or maybe an infected mosquito in search of a bloodmeal settled for a dog instead of a bird or person, halting the chain of transmission. All scientists know for sure is that in the summer of 1999, at least one infected mosquito bit a suitable reservoir host. After that, nothing could stop the virus. If the main vector in the United States turns out to be Culex pipiens, this viral amplification probably took place under cover of darkness, when crows and other carriers roost communally—C. pipiens is a nocturnal feeder. Perhaps the virus multiplied in the Jamaica Bay Wildlife Refuge, adjacent to Kennedy International Airport, a prime stop for migrating birds. More likely the epicenter was northeast Queens, where in 1999 a chilling 50 percent of wild birds became infected. As transmission accelerated, the virus crept closer and closer to people. “It’s a numbers game,” says CDC vertebrate ecologist Nick Komar. “How many mosquitoes are out there? How many are infected? What’s the probability that they feed on a human being? How many human beings are there? If it’s really hot, are people sleeping outdoors or spending longer hours outdoors? All those numbers come together. With a huge population like New York’s, you’re bound to get human infection.”
On the other hand, maybe the original vector wasn’t a mosquito at all. Maybe a human unwittingly conveyed the virus to the New World. Between July 1998 and June 1999, nearly five million people arrived from international destinations to one of New York City’s three airports (La Guardia, JFK, and Newark International). Of those passengers, nearly a quarter came from one of the 59 nations where West Nile virus had appeared in humans or animals. If a newly infected traveler happened to land in New York during the virus’s three- to five-day incubation period, during which time virus in the blood peaks, he or she could have infected a big-city mosquito and kicked off the cycle. Even healthy people symptomlessly infected with West Nile, many virologists say, can raise enough viremia to infect mosquitoes. “My suspicion,” says Tom Monath, the CDC’s former division director in Ft. Collins, now vice president of the biopharmaceutical company Acambis Inc., “is that this was somebody who traveled from Tel Aviv or somewhere to visit a cousin in Queens, sat on a stoop in the late afternoon, and got bitten by Culex.”
Edging toward the outer bounds of probability, imported or smuggled birds may have spirited in the virus. In 1999, 2,770 birds, both commercially bred stock and pets, were legally imported through JFK. Most imported birds are quarantined for 30 days—unless American owners had taken the birds abroad while traveling, then brought them back. Here, these feathered family members get away with a kind of house arrest, monitored at home by their owners. Maybe a bird went to Israel and on its return infected a mosquito in Queens. CDC investigators went so far as to track down several New York City parrots that had made just such a sojourn. Less likely, but not impossible, is an infected migratory bird having flown a wayward path across the Atlantic from Europe. Even ticks, which are hardy travelers, can carry West Nile virus. The closer you look, the more almost anything seems plausible—and the more tightly the globe seems strung together by viral connections, like one of those busy, loop-decorated route maps in airline magazines.
In October 1999, Richard Preston published an article in The New Yorker speculating about whether West Nile had been planted by a
bioterrorist. He cited an excerpt from an article that had appeared that April in a London tabloid, ostensibly written by an Iraqi defector claiming to be Saddam Hussein’s double. According to the account, the Iraqi president had boasted that his country’s labs had perfected a West Nile strain “capable of destroying 97 pc [percent] of all life in an urban environment.” The notion of a terrorist depositing an exotic pathogen into New York wasn’t new, of course. Since 1995, the year a Japanese cult released nerve gas on the Tokyo subways, New York City officials had been bracing for biological warfare. But it wasn’t just intentional malice that they feared. The 1994 outbreak of pneumonic plague in India and the 1995 epidemic of Ebola hemorrhagic fever in Zaire put them on guard for any imported epidemic. When federal investigators learned on September 3 that SLE was afoot in the city— itself a bizarre event—they reflexively began looking into terrorism. When further tests revised the finding to West Nile, more alarms went off. Stoking their suspicions were reports that summer about a West Nile epidemic in southern Russia—a country known to have fanatically perfected bioweapons under the former communist regime.
Ultimately, however, federal officials discounted the bioterrorism theory. West Nile virus, they concluded, not only doesn’t wipe out enough people to be a credible weapon, it depends on the tenuous life cycle of mosquitoes to spread: not a reliable way to sow panic. When scientists later mapped the genetic sequence of the virus, they saw that, far from being a devilish recombinant, it could only have descended by natural mutation from the Israeli 1998 strain.
But some researchers aren’t willing to completely close the door on the bioterrorism hypothesis. USAMRIID scientists, while skeptical that the West Nile outbreak was purposely planted here, don’t rule it out. “As a scientist, you can’t—there’s just no data,” says microbiologist George Ludwig. “This was a natural outbreak,” adds Mike Turell. “The question is, did it arrive naturally or did someone assist it? This could be a very subtle, very carefully arranged attack meant to mimic a natural infection.”
Regardless of how West Nile virus got here, the big question is: What course will it blaze next? To answer that, investigators must figure out every step of its natural history—just as Ross and Reed did in their signal discoveries about malaria and yellow fever at the turn of the last century. What mosquitoes are carrying it and spreading it? Are they biting people or birds? If birds, which birds? Where’s the virus hanging out during the winter? How many dead birds must turn up before human cases emerge? Which birds are sustaining the virus in nature? (House sparrows currently look like a good bet.) And what makes this virus deadlier in birds than other West Nile strains?
“If you want to be a hard-hearted scientist,” says UC–Berkeley’s Bill Reeves, “this is a grand experiment. The fact that these birds are dying is a beautiful example of what happens when any agent gets into a virgin population.” Adds CDC epidemic intelligence service officer Dan Singer, “We’re not jumping on this because it’s going to wipe out the population of North America. We’re keeping a close eye on it because it’s the first time we’ve had a level of technology to see how a disease spreads through a community and the environment. A lot of the public health interest is not West Nile as West Nile, but West Nile as a novel pathogen.” Knowing how West Nile spreads may help scientists forecast how Japanese encephalitis viruses or others will behave in a new land.
In 2000, West Nile virus defied all the scientific oddsmakers’ predictions. Rather than heading south with the previous year’s migration and fizzling out in the Northeast, it wintered comfortably up north and proceeded to carve out a northern and western route, perhaps riding with the spring bird migration, extending as far north as Boston and as far west as the New York–Ohio border, as well as south to North Carolina. Now that it seems here to stay, scientists expect it to fan out into all regions that SLE populates—including South America—on the wings of migratory birds. With one audacious leap, an Old World pathogen became an American virus-in-residence. And it won’t be the last.
A Second Look
And that’s just what unnerves public health officials. West Nile established itself here, leaving clues literally at New Yorkers’ feet, before anybody put the pieces together. When things go wrong like this, officials ruefully haul out the “retrospectoscope”: a crystal-clear lens that focuses the mistakes of a recent investigation. Since 1999, it’s gotten a lot of use.
Critics have described the West Nile investigation as a “failed dress rehearsal” for a still-evolving national plan to respond to bioterrorism. Getting the virus wrong was just part of the problem. Tunnel vision blinded CDC investigators to evidence that contradicted their original judgment. Scientists neglected to remember that every other SLE out-break in this country had begun in the south and crept up along the Ohio or Mississippi river valleys—in other words, that there had always been inklings in the south before anything happened up north. They also ignored the fact that muscle weakness—the most striking symptom in the early cases—had never been a hallmark of SLE. They didn’t quickly probe the reasons for the ambiguous test results on patients’ blood, and dismissed New York City officials’ repeated questions about those results. Perhaps most important, they slighted the concerns of Tracey McNamara, the scientist who early on uncovered the central clues to the mystery.
“Our public health system and the response to this crisis came down to a few personalities. And it’s frightening that some quirks can obstruct an investigation,” McNamara said. And perhaps, she added, a not-so-subtle misogyny also got in the way. The fact that she and the other women who raised early questions do not “speak with a deep baritone was a very important factor. I hate to say it, but that’s still the way of the world.”
Among the onlookers who was not surprised by this series of mistakes was a former director of the CDC’s National Center for Infectious Diseases. Virologist Frederick Murphy, one of the co-discoverers of the Ebola virus who is now at the University of California–Davis, had just a year before prophetically published an article pleading that
government officials listen to those outside the “citadel,” the traditional federal community of investigators and officials—people such as local clinicians, pathologists, veterinarians, and animal scientists, whose observations can be crucial early gleanings of an emerging epidemic. At the time, Murphy’s former federal colleagues castigated him for publishing such a solecism. But today, CDC–Ft. Collins convenes weekly conference calls with all of the 48 mainland states as part of its West Nile follow-up—calls that include public health veterinarians, wildlife experts, and representatives from the United States Department of Agriculture—during which speakers can brainstorm about any suspicious animal-to-human infections.
Another deep-seated problem also hobbled the investigation: the decrepit state of arbovirology. Though the arrival of West Nile virus in the United States would open a rich vein of research, for some researchers it also triggered a kind of professional anguish. “My first reaction was: ‘We’re in a hell of a lot of trouble,’” said Yale University entomologist Durland Fish. “Because the field of vectorborne disease ecology is almost extinct.”
From the 1940s through the 1960s, arbovirology was hot science. After a search for the yellow fever virus uncovered a teeming universe of viruses in the tropics, the Rockefeller Foundation set up a worldwide network of laboratories, from Brazil, Colombia, and Trinidad to India, South Africa, and Uganda. Partly, the goal was to find and catalog hitherto unknown viruses—which the foundation did, by the hundredfold. Partly, it also aimed to nurture new technologies and donate them to the host nations.
“I didn’t know it at the time, but it was as good as it gets,” says arbovirologist Robert Shope, a granddaddy in the field. “We had a lot of freedom. We were not saddled with writing grant proposals.” Back then, arbovirologists were generalists par excellence—in addition to virology, they mastered entomology, vector biology, ecology, mammology, ornithology, and epidemiology. CDC–Ft. Collins amassed a huge library of reagents and built a state-of-the-art lab to identify new mosquito species. According to Tom Monath, “People were in tune with global virology. You had a cadre of people who had tremen-
dous international experience.” Here at home, CDC scientists explored the natural history of St. Louis encephalitis, Eastern equine encephalitis, and Western equine encephalitis.
By the mid-’60s, however, success began to breed indifference. As vectorborne infectious diseases such as malaria, dengue fever, yellow fever, and plague retreated in most parts of the world except Africa, their breeding sites eliminated with chemical pesticides and other means, interest in the field languished. “When I arrived at Johns Hopkins in 1965,” says the CDC’s Duane Gubler, “I was told that I was in a dying field.”
The 1975 outbreak of SLE in the United States temporarily fired up the field again. State and local health departments launched programs to catch mosquitoes, capture sparrows and test their blood, and perfect the use of so-called sentinel chickens, which were placed in mosquito-ridden areas and tested regularly to see if they had been bitten and produced antibodies to the SLE virus. But when there were no subsequent outbreaks for five years, legislatures shifted the money to other programs. Because vectorborne epidemics come and go without warning, health officials lament, it’s always been hard to persuade legislators to keep up the flow of research funds. Along the way, arbovirology became scientifically fragmented. The federal program focused on molecular biology rather than fieldwork. Most state programs, which do the yeoman’s work in picking up and containing epidemics, deteriorated. “We let it go too far,” admitted Gubler. “Many of the states simply don’t have the people or the facilities to deal with these diseases.” According to the CDC’s Steve Ostroff, who since 1999 has been West Nile coordinator for the U.S. Department of Health and Human Services, West Nile in New York City represented the “chickens coming home to roost.”
Today, few training centers or universities are planting the next crop of arbovirologists and medical entomologists. “We need new ideas,” says Yale’s Durland Fish. “We need new methods for surveillance. We need new methods for control. The light traps they’re using is a fifty-year-old technology. Spraying is a one-hundred-year-old tech-
nology. That doesn’t speak very well for the field. We’re almost beyond the point of no return. West Nile came in the nick of time.”
***
On June 27, 2000, Flushing Hospital’s Deborah Asnis—the woman who arguably tipped off the world to West Nile virus in New York City—phoned Annie Fine at the department of health. Asnis had a patient who couldn’t move his arms or legs. For a single suspended moment, it looked like lightning was about to strike twice. But it didn’t. This unfortunate victim had dined on rat poison, and not voluntarily. He died the next day.
Just as it takes a series of coincidences for a traveler like West Nile virus to land here and thrive, so noticing it depended on an astute clinician and vigorous surveillance. Public health officials say they can’t keep pathogens out—they can only hope to notice them early and act quickly. What if Deborah Asnis had never called the New York City health department? Would the outbreak have been noticed only after it had already subsided, forcing public health officials to go back and pick up the pieces? Would it have been noticed at all? The first weekend Layton and Annie Fine looked for cases, 19 West Nile encephalitis patients already lay in the hospital—but only four had been reported.
What if the outbreak had started somewhere else? “There’s 10 million people in metropolitan New York. There were seven deaths,” said the CDC’s Nick Komar. “Say there’s two million people in metropolitan Boston: there would have been one or two deaths—let’s say one. If there was one encephalitis death in a hospital in Boston, would they have ever tracked it down to an arbovirus? Maybe not. . . . And if we didn’t know about West Nile virus in 1999, what would we be seeing in 2000? I’m guessing that we wouldn’t have noticed anything.”
“To expect the unexpected” has for years been the mantra of public health scouts on patrol for new and emerging infections—so much so, the phrase runs the risk of fading into background din. The 1998 CDC report Preventing Emerging Infectious Diseases: A Strategy for the
21st Century, warns that “because we do not know what diseases will arise, we must always be prepared for the unexpected.” In his autobiography, Virus Hunter, C. J. Peters offered a similar and much-quoted piece of wisdom from the obverse side: “Common things occur commonly. Uncommon things don’t. Therefore, when you hear hoofbeats, think horses, not zebras.” For a few weeks late in the summer of 1999, the zebra’s stripes were camouflaged by the shadows of dead crows, and all investigators could see was a horse.
The Zoonotic Threat
Though West Nile virus caught the attention of citizens and the press, what wasn’t played up was the larger threat that the virus exemplifies. West Nile virus is a zoonotic infection—it jumps to us from animals. It is not the most fearsome zoonosis; but zoonoses have shadowed us throughout human history and remain an ever-present menace, a limitless reservoir of pestilential surprise. To understand what’s on the minds of public health officials, it helps to take a quick detour into this territory.
Of the more than 1,700 known viruses and bacteria and other pathogens that infect humans, about half come from animals. Of the more than 150 pathogens linked with emerging infections, about threequarters come from animals. In the past quarter century, scientists have cornered more than 30 new infectious diseases—and all but a few have come from animals. Whatever deadly pandemic next sweeps the world, whatever newly christened scourge dominates headlines, it will almost surely have jumped species in this way, as measles and influenza once did. There is no telling what it will be, where it will come from, whether it will be an isolated curiosity or a ravaging epidemic—or even whether it will come courtesy of a bioterrorist, since many of the viruses and bacteria most likely to be used in such an attack are zoonotic, such as those causing anthrax, plague, brucellosis, and tularemia, as well as equine viruses.
A zoonosis emerges when an agent gains access to a new place or
new conditions that promote its spread. The Ebola virus, a filovirus whose natural host in the wild is unknown, was discovered in 1976 and originally transmitted in jungle and savannah areas where humans had newly encroached; a Zaire outbreak killed 90 percent of its victims. Marburg virus, another filovirus that causes the massive internal bleeding of hemorrhagic fever, was discovered in 1967 in German and Yugoslavian lab workers and vets who handled tissues from African green monkeys. The Nipah virus emerged in 1998, a virus harbored in fruit bats that killed 40 percent of slaughterhouse workers who caught it from pigs and developed encephalitis. Zoonotic infections reach us either directly from animals, or indirectly from animals via insect vector, such as West Nile virus.
For early humans, progress invited zoonotic infections. When they descended from the trees roughly five million years ago, our ancestors picked up parasitic worms from the flesh and feces of animals on the savannah and sleeping sickness from the tsetse flies that preyed on those herds. Meat-eating, tool-wielding Homo erectus set out from Africa to the warmer parts of Europe and Asia one million years ago and traded the chronic illnesses fostered by tropical parasites for a new crop of afflictions. In Man and Microbes, Arno Karlen surveys these new torments: sporadic cases of bubonic plague (transmitted by rats); botulism and staphylococcus infections (from scavenged meat); gangrene and tetanus (from butchering kills); relapsing fever, hemorrhagic fevers, brucellosis, leptospirosis, toxoplasmosis, and salmonellosis (transmitted by wild game); scrub typhus and encephalitis (from insects and ticks).
Not until around 3000 BC, when agriculture had given rise to larger settlements, did what historian William H. McNeill calls the “diseases of civilization par excellence” begin to take hold. These diseases are acute, travel swiftly and efficiently, and tend to be limited to humans. Biologists believe that the measles virus stemmed from canine distemper and rinderpest, an affliction of cattle; that rhinoviruses— agents of the common cold—came to us from horses; that the human form of tuberculosis derived from a mutation in the bovine strain; and
that smallpox is a close cousin of cowpox. As Jared Diamond points out in his book Guns, Germs, and Steel, “when we domesticated social animals, such as cows and pigs, they were already afflicted by epidemic diseases just waiting to be transferred to us.”
Zoonotic agents spread rapidly when they become biologically comfortable enough in Homo sapiens to make us their new home. The most frightening launchpads for emerging zoonoses are nonhuman primates, since viruses that afflict monkeys and apes are most likely to adapt to us. The most shocking example, of course, is the AIDS virus, first discovered in 1981, which continues to evolve and expand. In 2000, it newly infected more than three million people. The AIDS global epicenter is sub-Saharan Africa, where two versions of the human immunodeficiency virus leapt the species barrier: HIV-1, which originated in chimpanzees, and HIV-2, which came from sooty mangabeys. The dominant virus in the global epidemic, HIV-1 seeded itself in humans in the early part of the twentieth century, conceivably when hunters killed and dressed wild chimps and ate their raw meat, a common practice in west central Africa, where the animals’ infected blood infected people through cuts or through mucous membranes. Sooty mangabeys, which carry HIV-2, were not only hunted for food but also kept as pets. According to a genetic family tree drawn by the world’s fastest computer—the Nirvana at Los Alamos National Laboratory— HIV first jumped into humans around 1930. In 1985, scientists from Emory and Harvard Universities found evidence of the AIDS virus in a preserved specimen from an unidentified African man who died in 1959 near present-day Kinshasa, capital of the Democratic Republic of Congo. Beatrice Hahn, a physician/researcher at the University of Alabama at Birmingham, believes at least 24 other African primate species are infected with similar retroviruses. Hahn worries that new commercial logging operations in the tropical forest will foster a “bushmeat” trade—the large-scale hunting and consumption of wild animals, traditionally a subsistence activity. With newly cleared paths of transmission, new human-adapted primate infections could come our way.
Certain conditions prime the pump for animal-to-human infec-
tions. Untouched animal and arthropod habitats—from tropical rainforests to American woodlands—are disease minefields for humans. Though travel and transport thrive more in the developed world, ecological change is most rampant in the developing world, and biodiversity richest in the tropics—making the latter the best hunting ground for emerging infectious agents. Megacities of the tropics, with their crowding and poor sanitation, act as incubators for emerging zoonoses, and porous public health surveillance gives them a free pass. Nearly all of the world’s population growth in the next 25 years will occur in urban areas of developing countries. But disease-incubating conditions aren’t confined to what we think of as the third world. Bucharest in 1996 saw an epidemic of encephalitis caused by West Nile virus in an area where apartment building basements were flooded, creating such massive mosquito populations that the insects blackened the walls and ceilings of apartment buildings. Global transportation further stirs the pot, delivering disease agents to new ecological milieus where they can prove their adaptive mettle. “If you look twenty or thirty years down the road,” says Duane Gubler, “all of the factors that have been responsible for the resurgence of these diseases are going to get worse before they get better.”
In the coming century, climate changes may fuel more vectorborne outbreaks. According to the 2000 United States National Assessment Report, an analysis from experts in academia, government, and private industry, the U.S. will see higher temperatures, more extreme weather shifts, and a different precipitation cycle over the next hundred years. Because vectorborne disease cycles are exquisitely tuned to the environment, the effect of such shifts, whether we will see more or fewer flareups of West Nile encephalitis or other vectorborne diseases, isn’t clear.
Some scientists are skeptical that global warming will unleash a torrent of vectorborne infections. For one thing, notes CDC entomologist Paul Reiter, during the coldest period of the Little Ice Age—from about 1564 to the 1730s—malaria was rife in England. Indeed, during the eighteenth century, the disease reached as high as the Arctic circle.
All this points up the importance of nonclimate factors, such as drainage and land reclamation, the decline of rural populations, mosquitoproof houses, and the capacity to raise more livestock, which in the case of malaria may have diverted biting mosquitoes from human flesh. Nonclimate factors may also protect us today. While dengue has flared in Latin America, for instance, the infection screeches to a halt at the U.S. border. From 1980 to 1996, there were more than 50,000 cases of dengue in the three Mexican states contiguous to Texas—and only 43 in Texas itself. That sudden shift in disease at the border may be partly attributed to the displacement of Aedes aegypti by Aedes albopictus, a poor vector for arboviruses to humans because it is as apt to bite rats, cats, and dogs as people. But more critical has been the U.S. standard of living and our social (or antisocial) habits. “We don’t go out in the evening or the afternoon and talk to our neighbors,” says Gubler. “We’re in, watching television in air-conditioned houses that are hermetically sealed.”
But other scientists contend that as the atmosphere warms, glaciers will melt, sea levels will rise, and storms will become more uninhibited. If temperatures at night and in winter rise, it will speed the reproduction of viruses and parasites. Rising temperatures will also boost the metabolism of insects and other arthropods, forcing them to feed more and thus putting more people at risk for West Nile encephalitis, malaria, and other diseases.
The 1993 hantavirus outbreak in the American Southwest may have had roots in an unusual weather pattern, similar to that prompted by global warming, known as the El Nino/Southern Oscillation. An ancient strain that first caught health officials’ attention in 1993, when it killed more than two dozen people in the Four Corners region of the rural Southwest, it is inhaled in the aerosolized, dustborne wastes of the deer mouse. More than 40 percent of victims die of an infection that first feels like the flu but ultimately turns the immune system into a self-annihilating weapon, destroying capillary walls in the lungs and filling the lungs with fluid. In 1993, after six years of drought, heavy
spring rains pelted the region, leading to a tenfold increase in the population of deer mice, the animal reservoir for the Sin Nombre virus.
Writing in Science, Harvard University physician and climate change researcher Paul Epstein invokes global warming as the stage for New York City’s West Nile outbreak:
The mild winter of 1998–99 enabled many of the mosquitoes to survive into the spring, which arrived early. Drought in spring and summer concentrated nourishing organic matter in their breeding areas and simultaneously killed off mosquito predators, such as lacewings and ladybugs, that would otherwise have helped limit mosquito populations. Drought would also have led birds to congregate more, as they shared fewer and smaller watering holes, many of which were frequented, naturally, by mosquitoes. Once mosquitoes acquire the virus, the heat wave that accompanied the drought would speed up viral maturation inside the insects. Consequently, as infected mosquitoes sought blood meals, they could spread the virus to birds at a rapid clip. As bird after bird became infected, so did more mosquitoes, which ultimately fanned out to infect human beings. Torrential rains toward the end of August provided new puddles for the breeding of C. pipiens and other mosquitoes, unleashing an added crop of potential virus carriers.
***
The same year that West Nile virus hit New York City, dozens of less-publicized pathogens leaped from animals to people every day in every part of the United States. Though not all are important from a public health standpoint, they illustrate a timeless exchange between humans and our planet’s cohabitants. Just as West Nile virus took advantage of human activities to annex new territory, so have local pathogens.
To get a sense of how imperceptibly our paths cross those of pathogenic bacteria and viruses, consider an outbreak that struck in the heart of the Midwest a year before West Nile emerged in New York. Just after dawn on Father’s Day, 1998, 851 men and women, attired in swimsuits and goggles, gathered at the edges of Lake Springfield for the start of the 16th Annual Iron Horse Triathlon. The heavy rains of the previous day and night had cleared. It was sunny and familiarly
humid for the middle of Illinois in summer. In timed waves, the contestants launched an assault across the flat midwestern landscape, first swimming 1.5 miles, then biking 45 miles on country roads edged by corn and beans, finally running ten miles on sticky two-lane blacktop. It was hardly an environment that suggested disease.
Within two weeks of the competition, 97 of these athletes were sick with wide-ranging but eerily similar symptoms. Abruptly and without warning, they had developed fever, chills, muscle pain, and headache. Some went on to suffer more severe GI and neurological problems. Twenty-three were hospitalized.
Several years earlier, these same symptoms had turned up in a very different group of patients: residents of inner-city Baltimore. One, a young woman, had gashed her foot while walking shoeless in an alley where she had seen rats. A man recalled accidentally piercing his hand on glass in a rat-infested passageway between row houses. Another man wandered barefoot near Baltimore’s Inner Harbor.
What connected these mysterious outbreaks in such disparate locales and groups of patients? A tiny, slender, helically shaped bacterium of the species Leptospira interrogans. The signature disease caused by this spirochete is leptospirosis, thought to be the most widespread zoonotic disease on the globe. Workers in rice fields, sugar cane plantations, and mines are highly susceptible. Each year, an estimated 100 to 200 Americans contract leptospirosis, though the number may in fact be far higher. People get leptospirosis from fresh water, wet soil, or vegetation contaminated by the urine of infected animals. The bacterium enters the body through broken skin, mucous membranes in the eyes and nose, or contaminated drinking water. Lake Springfield had likely become contaminated when heavy rains washed animal wastes into the lake, which was then churned by the unwitting triathletes. The Baltimore patients caught the disease by inadvertently touching the urine of city rats, which are known to harbor the bacterium. In fact, some scientists assert that leptospirosis, a disease that contributed to Napoleon’s defeat in Poland and Russia during the winter of 1812, goes vastly underdiag-nosed in this country’s urban patients. One recent study found that of patients whose blood was drawn
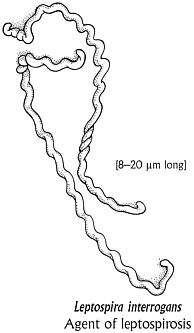
at a Baltimore clinic for sexually transmitted diseases, 16 percent had been exposed to Leptospira. A study from Detroit found that inner-city children were far more likely to harbor antibodies to the bacterium than suburban kids—and no one knows the consequences of these untreated infections.
But leptospirosis pales beside other home-grown zoonoses. Each year, more than 16,000 Americans come down with the fever, fatigue, and rash of Lyme disease, a bacterial infection conveyed by the bite of the deer tick. Untreated, the infection can progress to arthritis, neurological problems, and heart disease. Borrelia burgdorferi spends its life on the white-footed mouse and drinks blood from the whitetailed deer, denizens of the modern suburban and exurban checker-board of vegetation. Here, small, fragmented woodlots and tall grasses have blossomed on forest land originally cleared in the nineteenth century for agriculture, and these species have exploded in number. Lyme disease didn’t come to us; we came to Lyme disease, by intruding on a tilted ecosystem of our own making. Since 1982, when surveillance began, the number of annual cases has increased 25-fold. According to recent studies, forest tracts unbroken by asphalt and human abodes sustain a wider array of small mammals and birds than do today’s carved-up sylvan fragments. In these larger forest expanses, where white-footed mice face more competitors and more predators, fewer ticks carry the Lyme bacterium.
In 1999, Americans were sickened with Sin Nombre virus; bubonic plague, carried by the fleas of prairie dogs, squirrels, and rodents; ehrlichiosis, a burgeoning zoonotic disease caused by a rickettsial organism carried by the same tick that transmits Lyme disease; [8–20 µm long]
tickborne Rocky Mountain spotted fever and babesiosis; mosquitoborne LaCrosse encephalitis and Eastern equine encephalitis; bacterial psittacosis from parrots and Salmonella infections from iguanas, and many other animalborne diseases—including the millions of foodborne infections from livestock that top the list of zoonoses. New York City, the world’s preeminent urban milieu, is not immune to seemingly rusticated ambushes. It has seen cases of tularemia, a rare human infection often found in rabbits, cats, and voles, and Rocky Mountain spotted fever, a tickborne infection that despite its name has been found in almost every state in the country.
If disease cops had a handle on every zoonotic assault that takes place in the United States, the daily police blotter would be as long as a big-city phone book.
Race to the Finish
Though readers got blow-by-blow reports of the public health establishment’s duel with West Nile virus, what they didn’t read about was the behind-the-scenes race to identify the virus. This story is like that of many highly publicized investigations. On Saturday morning, the day after the CDC’s bombshell announcement, the agency’s Rob Lanciotti, John Roehrig, and Duane Gubler were talking in Gubler’s office when the phone rang. It was Ian Lipkin, a scientist at the University of California–Irvine. Unbeknownst to Lanciotti (and to the New York City health department), Lipkin had also been pulling all-nighters to pinpoint the pathogen killing New Yorkers. A neurologist by training, he directed the university’s Emerging Diseases Laboratory. Beginning in the late 1980s, Lipkin had made a name for himself by exploring the hidden infectious causes of neurological diseases, along the way developing innovative molecular biology tools for ferreting out pathogens. In Lipkin’s lab, DNA searches that used to take days now took only hours.
At a scientific conference about encephalitis testing in September, officials at the New York State Department of Health laboratory told
Lipkin that they were having trouble amplifying genetic sequences of the SLE virus from the tissues of New York City’s encephalitis victims. Lipkin, a trim, precise, almost elegant man with wire-rimmed glasses and an aquiline nose, leaped at the chance to put his innovative research methods to the test. By Wednesday evening, September 22, he had found the genetic footprints of a flavivirus in the encephalitis victims. By Thursday, he had unspooled pieces of the virus’s genetic sequence. In doing so, Lipkin was the first to close the loop in an epidemic involving humans, birds, and mosquitoes. The CDC called the virus “West Nile–like”; Lipkin called it “Kunjin/West Nile–like,” after a strain of West Nile virus found in Australia. Because the taxonomy of Kunjin is somewhat ambiguous, both teams were right. The discrepancy arose because Lipkin and the CDC’s Lanciotti were comparing different sections of the genome to different reference strains in GenBank.
When Lipkin called Gubler’s office that Saturday morning, Gubler and his colleages were expecting a technical ironing-out of their divergent results in this high-profile outbreak. Lipkin had something else in mind: a quick joint publication in the New England Journal of Medicine. “I said, ‘Look, you’ve got the data in the animals. We’ve got the data in the humans. In concert, we’ve established that this is an important new zoonosis. We should write this thing up together.” The CDC scientists were silent. Finally, Gubler—a big man with a thick gray moustache, cat eyes, and the appearance of a TV Western frontiersman—spoke up. Gubler was himself an aggressive scientist. But the CDC, he said, was not interested in publishing until the agency had rock-solid data about the virus. For good or ill, any prospective public–private collaboration ended there.
Suddenly, the endeavor to fully sequence the virus was a competition. “It became absolutely clear to me that these guys were going to steal credit for everything that had been done,” Lipkin said. “Because basically, without the human work, they wouldn’t know what they had.” On October 9, Lipkin published his Kunjin/West Nile–like findings in the British medical journal Lancet, seemingly beating the CDC
to the finish line. But in the end, it was the CDC that hit the bull’s eye in an announcement two weeks later: New York’s virus was most closely related to an unpublished 1998 West Nile sequence from Israel, which the CDC had acquired from a French scientist—a sequence to which only the CDC had full access.
Many onlookers praise Lipkin for first discrediting the St. Louis encephalitis diagnosis. “You’ve got to give him credit,” says Tom Monath. “He looked at the sequence and recognized this was West Nile–like virus and snapped off a paper. Well, that’s the world we live in—especially the academic world.” Others were angry with Lipkin for rushing to publication with what the CDC still claims are misleading results.
When egos are roused, it’s hard to get at the truth. Lipkin says that in spurning cooperation, the CDC not only set a bad precedent but also set back science. “They’re bulls in china shops. And I guarantee you that the next time something comes around that’s a little bit squirrely, they’re going to miss it again. . . . My view is that you can get a lot more done working with people than fighting. And life is short.” CDC officials publicly affect a cool respect toward the academician, while suggesting between the lines that he was something of an irritant. The competition left a bad taste for many onlookers and brought up a larger issue: In a public health emergency, can public health and academic researchers collaborate? Clearly, the stakes for each are different. Public health investigators need to solve a crisis, academics to garner recognition and funding. Within the CDC, many branch directors believe they wouldn’t be able to keep their best bench scientists if they didn’t protect those researchers by making sure they were the first to publish new findings. But others believe such protection is unnecessary, and that in any case CDC should rise above proprietary concerns. “In the good old days, CDC didn’t compete,” says Frederick Murphy. “The motivation was driven by the sense that CDC’s unique, that it’s a public service organization—and that the reputation of the scientists will prosper anyway, because of the incredible opportunity that the CDC has to get all this good stuff.”
When a historic outbreak strikes, “everyone wants a piece of it,” Duane Gubler said. “You know, if you’re in science, you don’t get paid a lot. Your rewards are basically building up your ego, right? And the way you build up your ego is to do good science and write publications and be the first to discover things. That’s what drives it. And people’s memories get clouded because of that.”
So were memories clouded? Or is there something about fast-breaking, high-stakes science that makes the protagonists the heroes of their own dramas? Looking back, New York City’s Marci Layton was intrigued by what she calls the “Rashomon quality” of the investigation. Deborah Asnis, Tracey McNamara, Ian Lipkin, Rob Lanciotti— each could plausibly claim to have “discovered” West Nile virus in the Western Hemisphere. The question is: Who will get to write the history books?
Epilogue
In 1999, 62 people were hospitalized with West Nile virus, seven of whom died, including a businessman who had visited New York City from Toronto and had become ill after he returned home. Most patients had become ill during the third and fourth weeks of August. While the greatest concentration of cases was in northern Queens and the south Bronx, investigators also found the virus in birds and mosquitoes in eastern Long Island, the lower Hudson Valley, New Jersey, and Connecticut, as well as in 25 horses (of which nine died) in Suffolk County, New York, and in a cat in New Jersey. New York City’s West Nile hotline logged more than 150,000 calls. In late September, Greenwich, Connecticut, officials temporarily banned “absolutely all outdoor activities” after 5 p.m. In New York state alone, residents reported 17,000 dead birds. Approximately 10,000 crows died in the outbreak. Researchers collected 25,000 mosquitoes for testing. As part of its effort to wipe out mosquito breeding sites, New York City erased one of its aesthetic signatures: abandoned tires.
In October 1999, Annie Fine got married in Prospect Park, at a
ceremony that took place at dusk, when Culex mosquitoes like to bite. She worried about her 96-year-old aunt. The toasts were replete with West Nile jokes. In a footnote worthy of Edgar Allan Poe, a solitary dead crow infected with the virus turned up in faraway Baltimore. The European Union banned horse and poultry imports from affected areas in the United States. That same month, investigators drew blood from Queens residents to find out how many people had been silently infected during the epidemic. They estimated that 2.6 percent of residents, or about 8,200 individuals, had West Nile virus antibodies in their blood; most had experienced no symptoms at all.
In January and February 2000, investigators gathered mosquitoes from sewers near the Bronx Zoo, from under the Whitestone Bridge, and from underground rooms at Ft. Totten. Three Ft. Totten samples yielded virus-positive mosquitoes, meaning the virus would return in the spring. And it did. Federal, state, and city agencies resumed their surveillance for infected birds and mosquitoes, spraying pesticides wherever the virus turned up. That year, for the first time in memory, there was a sudden run on arbovirologists, medical entomologists, and mosquito control experts. In April, New York City began its campaign to kill mosquito larvae, dropping poisonous pellets in the city’s 150,000 storm sewers. In every borough, white leghorn chickens deputized by the health department sat in secretly sited cages exposed to biting mosquitoes all spring and summer, bled each week by a veterinary technician to see if they had developed antibodies. All summer long, cities up and down the eastern seaboard, along the Gulf Coast, and inland as well searched for signs of West Nile virus. Eventually, the pathogen had spread to 12 eastern states and Washington, D.C., sickening 21 and killing two.
In 2001, the virus struck humans and animals in the Deep South and the Midwest. Experts predicted that by 2006 the entire nation would play host to West Nile virus, and that additional species of day-time biting mosquitoes would transmit infection. Dead birds remained the most sensitive way to track the virus in real time over a widening geographic area. Daily newspapers ran front-page bird obituaries. Inevitably, West Nile shock turned into West Nile shtick. A Westchester
County columnist surmised that it was not the virus, but the name of the virus that stirred fear. Had it been called “West Nyack virus,” he wrote, nobody but real estate agents would care. Two years after his scientific coup, Ian Lipkin decamped from UC–Irvine to Columbia University. And today, when she talks to scientific groups about her trials and travails in the West Nile virus investigation, Tracey McNamara never fails to flash on the screen a slide of two bucks locking antlers. “I work in a zoo,” she quips. “I recognize territorial display behavior.”
Duane Gubler, the Utah rancher’s son who spent 21 years outside the United States in tropical countries, felt a bit rueful. He wondered why Americans failed to grasp West Nile’s transcendent message. Why didn’t they see the connection between a stirring little domestic drama and what happens every day far beyond their borders? “Most people who suffer from these diseases are in tropical countries,” he said. “What makes me a little bit sad—not a little bit, but just plain sad—is that you’ve got diseases that kill tens of thousands of children in developing countries, and nobody cares about that until it gets to home.”