Secret Agents: The Menace of Emerging Infections (2002)
Chapter: 4 Superbugs
Chapter 4
Superbugs
Not long before antibiotics entered our lives, staph in the blood-stream killed 90 percent of its victims. A man who nicked him self shaving could die from erysipelas, a strep infection. Children lost their playmates to scarlet fever, meningitis, osteomyelitis. Bacterial pneumonia, the leading cause of death, killed a third of its victims. Tuberculosis patients were advised to rest and seek clean air, because there was nothing else medicine could offer. In parts of the United States, 10 percent of women died in childbirth. Rocky Mountain spotted fever killed 20 percent of its victims. The state-of-the-art treatment for syphilis was mercury ointment. Gonorrhea had no cure. A blindfolded visitor led through a hospital could identify the surgical ward by the stench of rotting flesh.
Today, antibiotics save tens of thousands of lives yearly in the
United States alone. Without these therapies, modern invasive medicine would come unhinged. Daily life would be an obstacle course of fear. Are we about to return to those times?
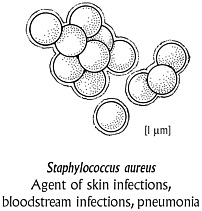
In May 2001, Mary Jane Ferraro was working at her desk when a lab supervisor stepped into her office. The woman had worked with Ferraro for 25 years, and they trusted each other’s judgment completely. “You won’t believe this,” the supervisor began. Ferraro, who directs the clinical microbiology laboratories at Boston’s Massachusetts General Hospital, listened hard. Her job is to make sure that one of the most storied medical institutions in the world—the place where patients go for help when the best outside doctors are stumped—pins down the most unexpected and difficult-to-discern agents of infection. An outgoing woman with a reddish-brown pageboy and a lyrical laugh, Ferraro soon headed down the hall to the lab, a complex of neutral-colored rooms with computers and microscopes and boxy incubation machines that warm bacterial cultures to human body temperature. The supervisor handed her a clear, round plastic plate. Growing inside were creamy yellow colonies of Staphylococcus aureus.
S. aureus is a virulent and aggressive pathogen, endemic in virtually every hospital in the world. On this May morning, the colonies of staph on the culture plate told a frightening story. In a circular arrangement on the plate were little round filter-paper disks, each saturated with a different antibiotic. If the antibiotic was effective against the staph, a wide clear ring formed around the disk, evidence that the nearby bacteria had been killed. If the bacterial colonies grew closer to the edge of the disk, it meant the drug was useless. Ferraro peered at the tiny disk containing linezolid. Barely a year earlier, to much fanfare, the Food and Drug Administration had approved the drug as the “last-resort” antibiotic for multidrug-resistant S. aureus, the most dangerous source of hospital infection. Here was the antidote doctors could supposedly turn to when every other medication failed. Ferraro couldn’t believe her eyes. The creamy colonies of bacteria grew undeterred. It was the first evidence of linezolid-resistant staph in the world. She felt an odd mix of emotions: competitive pride that her laboratory
had caught it, and terror that the infection had already spread to other patients.
Living Pharmaceuticals
Three millennia ago, the Chinese applied spoiled soybean curd to cure carbuncles, boils, and other skin infections. Mayan Indians roasted green corn and let it rot to produce a preparation that relieved skin ulcers and intestinal infections. Renaissance-era Europeans placed loaves of bread on rafters to grow moldy; this staff of life was sliced and mixed with water to make a pasty dressing for wounds. In 1640, the apothecary of London, moonlighting as the King’s herbalist, prescribed a fungus to treat infected wounds. All were applying living pharmaceuticals, now known to be antibacterial toxins produced by fungi.
In the nineteenth century, bacteriologists shed new light on these time-tested practices. They discovered that, in the lab as in nature, the fittest microbes survived by killing other microbes. As Louis Pasteur observed, “In the inferior organisms, still more than in the great animal and vegetable species, life hinders life.” The practical implications were obvious. “If the study of the mutual antagonisms of bacteria were sufficiently far advanced,” two scientists wrote in 1885, “a disease caused by one bacterium could probably be treated by another bacterium.” At the turn of the last century, German physician and bacteriologist Paul Ehrlich likened the immune system’s antibodies to magic bullets that aimed straight for their bacterial targets while leaving everything else in their paths unscathed. Why not, Ehrlich wondered, find chemical bullets that were equally potent and benign? As a 1925 editorial in the Lancet prophetically observed, “Medicinal properties attributed by tradition to certain fungi may possibly represent an untapped source of therapeutic virtue.”
In the warm September of 1928, Scottish bacteriologist Alexander Fleming returned to his London laboratory after spending two weeks at his country home. As Fleming perused a set of glass petri dishes that he had inoculated with bacteria before embarking on his holiday, his
eye stopped. In one, a green contaminating mold had unexpectedly taken residence. Immediately surrounding the mold, the growth medium looked clear. Only around the far edges of the dish grew the colonies of Staphylococcus aureus that Fleming had seeded in the medium. A closer look revealed what Fleming called “ghosts” of the staph bacteria—transparent remnants left when the mold “lysed,” or disintegrated, them. To Fleming, this was curious indeed. Just a few years before, he had identified the enzyme lysozyme, a component of tears and mucous fluids that kills non–disease-causing bacteria. But he knew that Staphylococcus aureus, one of the most dominant and fearsome groups of bacteria—to this day—was notoriously hard to lyse. “Obviously,” he would later write, “something extraordinary was happening.”
In a paper published the next spring, he identified the green contaminant as the fungus Penicillium notatum, from which penicillin got its name. Ultimately, it would be shown to destroy no fewer than 89 different pathogenic bacteria.
Fleming’s new germicide was unstable and difficult to produce. But the chase was on. Prontosil, first prepared by the German dye company I.G. Farbenindustrie in 1932, ushered in the sulfonamides, or sulfa drugs. These “bacteriostatic” agents didn’t actually kill microbes but rather checked their growth so that the immune system could finish them off. Ten years after Fleming’s initial find, a team of Oxford scientists purified his mold juice. In 1940, having inoculated eight mice with deadly doses of streptococci, they injected four with penicillin as well. By the next morning, only the treated animals had survived.
It took a while to produce these magic bullets in bulk. In a legendary 1941 case, an English policeman had scratched the corner of his mouth while pruning roses. He developed staphylococcal septicemia, blood poisoning that left abscesses over all his organs. Administered over five days, penicillin pulled him back from the brink of death. But the purified yellow powder was dwindling, and when the drug ran out, the patient relapsed and died.
To save the lives of Allied soldiers, the U.S. government quietly underwrote the production of larger quantities. After D-Day, penicil-
lin was released for civilian use. It became as common as candy, mixed in over-the-counter salves, throat lozenges, nasal ointments, even cosmetic creams. The drug and its synthetic derivatives transformed the medical landscape, dramatically cutting deaths from staph infections, sepsis after childbirth, pneumococcal pneumonia, ear infections, and bacterial meningitis. As Stuart Levy writes in The Antibiotic Paradox, “It was as if Prometheus had stolen fire from the gods.”
But just as soon as antibiotics were discovered, so was antibiotic resistance. In a 1945 New York Times interview, Fleming warned about the evolutionary selection of resistant bacterial strains. He had seen it in his own lab. When he grew susceptible bacteria in ever-increasing amounts of penicillin, some flourished and took over. “There is probably no chemo-therapeutic drug to which in suitable circumstances the bacteria cannot react by in some way acquiring ‘fastness’ [resistance],” he warned. As early as 1946, a London hospital reported that 14 percent of Staphylococcus aureus strains taken from sick patients could stand up to penicillin. Three years later, that figure leaped to 59 percent. The term “hospital germ” was coined, reflecting the sense that certain microbes thrived in the dense presence of antibiotics—a far cry from the sanitarian view that dangerous infections lurked in the street or at work or on public transportation. By 1955, when most countries curbed the use of penicillin to prescription-only, it was already too late. Today, just under 100 percent of Staphylococcus aureus are penicillin-resistant. And that’s just the beginning.
As scientists began prospecting for new antibiotics, their search led them to the very ground beneath their feet. As far back as the 1880s, it had been conjectured that the reason soil wasn’t the source of perpetual epidemics—despite receiving human and animal wastes and corpses—was because of an invisible, ongoing warfare between microbes. Today, we know [1 µm]
that each teaspoon of soil may contain thousands of different species, a more biodiverse menagerie than the earth’s entire collection of mammals. Whenever resistance emerged, researchers found a new class of drugs or chemically tweaked existing compounds. In 1944, Selman Waksman, a Ukrainian emigré to the United States and renowned soil microbiologist, systematically screened thousands of soil samples before happening upon a species named Streptomyces griseus. From this was extracted the first aminoglycoside: streptomycin, an early cure for tuberculosis. The genus of bacteria known as actinomycetes, which include the soil-loving Streptomyces, has since spun off well over half of the antibiotics used today, including the aminoglycosides, the macrolides, and the tetracyclines. The cephalosporins, refined versions of which are used today to prevent a wide range of hospital infections, were discovered in 1945; chloramphenicol, which cured typhoid fever and typhus, came in 1947; chlortetracycline, which cured pneumonia, in 1948; erythromycin, a broad-spectrum drug that stopped organisms such as Neisseria and Haemophilus, in 1950; vancomycin in 1955; methicillin in 1960; gentamicin in 1963; ciprofloxacin, a low-toxicity fluoroquinolone, in 1983.
Doctors wanted to be able to prescribe something even if they didn’t know what organism was causing a patient’s infection. So the pharmaceutical industry widened the killing swath of each new drug. As the antibiotic age unfolded, these categories would become important. Narrow-spectrum drugs such as penicillin G affect mostly Gram-positive bacteria, such as staphylococci, streptococci, and enterococci, so named because their single cell wall takes up a special stain used to differentiate microorganisms, and turns dark purple-blue. Gram-negatives, a group that includes gonococci, meningococci, and many intestinal bacteria, have a three-layer cell wall and so do not absorb the dye, showing up on a lab slide as a bright pink-red. Drugs that killed Gram-positive organisms often didn’t kill Gram-negatives. Not until researchers perfected “broad-spectrum” antibiotics and later even more widely effective “extended-spectrum” agents, were they able to treat both with the same drug. While on its face this development typified the golden
age of therapeutics, it would have unforeseen downsides. The further antibiotics extended their reach, the wider the bacterial insurgency.
It was 1967 when investigators isolated the first penicillin-resistant pneumococcus, the highly invasive organism that causes middle ear infections, pneumonia, and meningitis. Found in a healthy three-year-old boy in a remote village in Papua New Guinea—and probably bred through a misguided effort to prevent such infections by injecting residents with low-level penicillin—it was seen as a fluke. Looking back, that judgment could be interpreted as myopia, wishful thinking, willful ignorance, or just plain laziness. It’s also true to form. The history of the antibiotic era is littered with blasé dismissals of newly resistant species as exceptions. Ten years later, as if on cue, drug-defying pneumococcus surged, newly equipped with biochemical weapons against several classes of drugs. Resistant strains spread to South Africa in the 1970s, to Spain and Israel in the 1980s, and to this country in the early 1990s.
In the 1970s, other common infections also began a portentous shift. Within a year after the introduction of methicillin, a semisynthetic version of penicillin, methicillin-resistant strains of staph showed up. These became epidemic in Europe before vaulting to the United States. Haemophilus influenzae, a major bacterial cause of ear infections and meningitis in children, became penicillin-resistant—a turn of events revealed when two infants who had attended the same Maryland daycare center died from ampicillin-resistant meningitis. Gonorrhea caused by penicillin-resistant strains of Neisseria gonorrhoeae radiated out from brothels in Vietnam where women received prophylactic doses of the drug, no doubt intended to protect the troops more than the women. For public health officials, all these trends were wake-up calls, signaling that common infections contracted outside of hospitals could soon become untreatable. In the early 1990s, a multidrug-resistant strain of tuberculosis killed nearly 500 people in New York City, mostly AIDS patients. Just as the outbreak seemed to diminish, TB reared up elsewhere in the world, from China to Siberia to Puerto Rico, now resistant to four of the five drugs used to treat it.
With global travel, public health experts worry that these divergent strains will merge and become incurable.
With each passing year, what a researcher in 1957 called the “bugbear of drug resistance” shadowed every antibiotic success. By the mid1990s, the flow of replacement antibiotics slowed to less than a trickle. As infectious diseases resurged in this country, the media warned of “Andromeda strains” and “superbugs.” Those headline prophecies would soon come true.
Resistance Forces
The more we try to eliminate deadly bacteria with new drugs, the better bacteria get at dodging medicine’s magic bullets. So goes the “antibiotic paradox,” to use the succinct phrase of Stuart Levy, director for the Center for Adaptive Genetics and Drug Resistance at Tufts University School of Medicine, and for more than 20 years a cautionary voice. Every antibiotic ever used has hastened its own futility by triggering Darwinian selection. When an antibiotic attacks a group of bacteria, cells susceptible to the drug will perish. Those that can resist the drug, whether because of genetic mutations or because they have acquired protective genes from other bacteria, survive. Facing less competition for space and nutrients—antibiotics having killed off their natural competitors—these resistant cells multiply. The more they spread, the more they add to the pool of resistance genes in all bacteria, raising the odds that these genes will jump to more and more disease-causing bacteria.
In the laboratory, resistance plays out neatly and in full view. Outside the laboratory, the process is wild and sloppy and mysterious. Resistance genes flow in all directions. And though their travels cannot be tracked in real time, they can be extrapolated. Give your teenager antibiotics for acne, and you might soon develop drug-resistant staph on your own skin. Treat a toddler with cephalosporins for an earache, and soon a majority of the daycare center’s young clientele (and their parents) will be suffering resistant pneumococcal infections. Feed a flock of chickens low doses of tetracycline, and within days not only
will their coopmates harbor intestinal bacteria highly resistant to the drug, but so will their human handlers and their human diners. Pull back the camera even further, and it becomes clear that as all the earth’s bacteria became bathed in antibiotics—millions of tons over the past half century—they have, to varying degrees, formed resistance. Resistant bacteria have even invaded U.S. waterways, from the Rio Grande to rural streams; at some sites, half of the waterborne bacteria resist ampicillin, tetracycline, and vancomycin.
Antibiotic resistance develops when two ingredients come together: resistance genes and antibiotic use. If bacteria in a community—a community being a home, a daycare center, a school, a hospital, or a city—don’t have genes that enable them to withstand an antibiotic, that drug will simply mow them down, end of story. If the bacteria do have resistance genes but are not exposed to the antibiotic, they will have no selective advantage against their competitors and will eventually dwindle in number. Or at least, that’s the theory. In reality, things get a little trickier. Bacteria exposed to one drug can sometimes develop resistance to a whole raft of unrelated agents. And long after they’ve stopped being exposed to an antibiotic, bacteria will sometimes hang on to their genetic defenses.
But the general theory holds true: antibiotic resistance requires resistance genes plus exposure to an antibiotic. The more widely an antibiotic is used, the more resistance shows up in many different bugs.
The consequences can be seen all around us. A child with an ear infection that in the early 1990s would have been instantly cured by penicillin may now need two or three or four courses of different drugs. A new mother may no longer die of “childbed fever,” but she might well contract a drug-resistant urinary tract infection that keeps her in the hospital for another day or so. In the 1990s, a Boston hospital twice had to construct a new neonatal intensive care unit (ICU) because its newborns had been colonized with highly drug-resistant staph. In 1999, a New Jersey schoolteacher who went in for surgery to remove small growths from her sinuses wound up with a staph infection that kept her out of the classroom for a year. Every day, hospital patients find themselves alone in a room with a bright
yellow “precautions” warning on the door, declaring that visitors must don latex gloves and other protective accoutrements. What’s not explicitly stated: the patient has an incurable infection that could spread to other patients.
If the trends keep up, our most commonplace infections could turn into life-threatening illnesses. “It’s probably the biggest public health threat to the United States,” says J. Glenn Morris Jr., chairman of the department of epidemiology and preventive medicine at the University of Maryland School of Medicine. “Antibiotic resistance is something that directly affects everybody in this country, in a way that no single disease does.”
“For many common infections, we’re losing the drug of choice,” adds David Bell, who monitors antimicrobial resistance for the Centers for Disease Control and Prevention. Usually, there’s a second or third drug choice—but those medicines may be less effective or more toxic or may have to be given by injection instead of by mouth. And then there are organisms for which the rising tide of resistance has swept away medicine’s second or third choices. In those cases, says Bell, “we’re skating just along the edge.”
Sick Beds
Most resistant infections strike people in hospitals, nursing homes, and long-term-care facilities. That’s no surprise. These are places where antibiotics are used most intensively and so are the natural proving grounds for resistant infections. Because hospitals have been downsized at the same time as intensive care beds have increased, many facilities have in effect become giant intensive care units, where the sickest, most vulnerable patients are concentrated. Five percent of all U.S. hospital in-patients—about two million people annually—contract infections in hospitals. About 70 percent of those infections are caused by microbes that resist one or more antibiotics. Of those, 30 to 40 percent of the infectious organisms rebuff the drugs doctors would choose first. For the seriously ill, the immune-compromised, the very young, and the very old, any delay in curing a resistant infection raises
the risk of death. Each year, according to the World Health Organization, drug resistance contributes to more than 14,000 U.S. hospital deaths.
If resistant pathogens could dream of paradise, their reveries would look like the inside of a hospital. Take Staphylococcus aureus. Staph homesteads in the human body, living benignly on the skin of 20 to 25 percent of us, often in our nostrils, armpits, or groin. The rise of antibiotic-resistant staph has gone hand in hand with the invasionary forces of medical progress, especially central venous catheters, those long plastic tubes that snake all the way to the heart. In intensive care units, oncology and surgical wards, and dialysis patients, these tubes are commonplace because they make it easier for nurses to give medications and blood infusions. The linezolid-resistant S. aureus that Mass General’s Mary Jane Ferraro confronted was a typical example; it had come from an 85-year-old dialysis patient who had a fixed catheter in his abdomen. Starting in the 1980s, having a “plastic” in the body became a major risk factor for resistant infections from either S. aureus or another common type known as coagulase-negative staph. Bacteria—either from the patient’s own skin or from the hands of a health care worker—cling to catheters and other prosthetic material. Patients with open wounds such as bedsores also develop staph infections. Once staph gets into the bloodstream, it can cause heart valve, blood, and bone infections, sometimes leading to septic shock and death.
In the United States, July 1997 was a turning point for public health officials who monitor hospital antibiotic resistance. That month, a 59-year-old Michigan man became infected with a strain of Staphylococcus aureus. Long ago, of course, S. aureus had stood up to penicillin. Now it defied other drugs as well. It defied methicillin, the 1960s synthetic replacement for penicillin. That act of insurrection earned the bacterium a name—MRSA, for methicillin-resistant Staphylococcus aureus. But its recalcitrance didn’t end there. MRSA had gone on to resist chloramphenicol, ciprofloxacin, clindamycin, erythromycin, gentamicin, imipenem, tetracycline, trimethoprim, and others. By the time it reached the Michigan man, MRSA—which now in effect stood for multidrug-resistant Staphylococcus aureus—reliably
caved to one medication only: vancomycin, the drug of last resort. In the laboratory, the smallest concentration of vancomycin that killed the bacterium was 0.5 micrograms per milliliter of solution. This was known as the MIC, the Minimum Inhibitory Concentration.
This time, it didn’t work.
Even at 16 times that dose, the drug didn’t work. In the protocol of microbiology labs, that bumped up this MRSA to a new level of danger, and a new acronym: vancomycin-intermediate Staphylococcus aureus, or VISA. (Today, the less euphonious handle is GISA, with the G standing for Glycopeptide, the class of antibiotics that includes vancomycin.) In practical terms, intermediate resistance is a gray zone. Maybe high, toxic doses of vancomycin would have cured the infection—or maybe not. So far, clinical evidence suggests that VISA infections are impervious to vancomycin therapy. Doctors removed the stomach tube that had caused the man’s infection in the first place—he was a diabetic with kidney failure, and used home dialysis to clean his blood—and the infection eventually cleared, though the patient soon died of his underlying disease.
Only a month later, another GISA patient appeared: a 66-year-old New Jersey man, a diabetic with a staph infection in his bloodstream. He, too, survived the GISA but died of other causes. By 2000, three more elderly and chronically ill patients with GISA succumbed to the infection.
This was what public health officials had been dreading, ever since the world’s first case in a Japanese baby in 1996. The infections were isolated, developing anew in each patient, through mechanisms of natural selection all too familiar to doctors. Luckily, they didn’t spread to other patients. But public health officials feared that someday, as MRSA had in the 1980s, these new infections would race through hospitals. GISA was one step away from becoming untreatable staph. And untreatable staph would be, if not a full-blown reenactment of the preantibiotic age, at least a convincing one-act play. “Once you have the vanco resistance, and then linezolid resistance, there are no antimicrobial agents that could be used right now,” says Mary Jane Ferraro. “Could the problem spiral out of control? Yes. It is a realistic fear.”
In some hospitals, upwards of 70 percent of S. aureus infections are of the multidrug-resistant MRSA strain. To cope with these infections during the 1980s, and with an increasing number of infections with coagulase-negative staph and with a stubborn bacterial pathogen appropriately known as Clostridium difficile, hospitals cranked up their use of vancomycin, sometimes 200-fold. The irony is, doctors had always considered vancomycin a so-so drug. “I hate to see vancomycin termed ‘the drug of last resort,’” says Glenn Morris. “It’s a second- or third-string antibiotic, but if everybody else has already fouled out, that’s all you’ve got left. Vanco is not a superstar.” Nevertheless, this bench-warmer selected not only for resistant staph, but another frightening bacterium as well.
That other fearsome microbe is VRE, for vancomycin-resistant enterococci. First appearing in the United States in 1989, VRE infections rose 20-fold over the next four years. The bacterium owes its success to an ecological stroke of luck. The vancomycin prescribed for resistant staph rearranged the landscape inside patients’ intestines. Enterococci—a part of the normal microflora of the human intestine and until recently considered to be microbial milquetoasts—began to resist vancomycin. And when they escape the intestine, they become unpredictable. Entering the bloodstream through an IV line, a urinary catheter, or any breaks in the body’s defenses, VRE attacks wounds, heart valves, the urinary tract, and can lead to life-threatening infections. In a Pittsburgh hospital outbreak, an epidemic of VRE killed more than 30 patients in a liver-transplant unit. At risk for VRE is any hospital patient who has received an organ transplant, is on hemodialysis, takes an immune-suppressing drug, or has simply been weakened by fighting off infection. The last last-resort drug to be approved for VRE infections was linezolid, which goes under the trade name Zyvox. Barely a year after its approval, John Quinn, a physician at the University of Illinois at Chicago, published the first report of linezolid-resistant enterococcus; it emerged in five chronically ill patients, four of whom had undergone transplants.
VRE’s infamy stems not only from the damage it does today but also from a deadly supporting role it’s poised to play in the future.
MRSA and VRE are bad enough. MRSA plus VRE is a calamity. Researchers fear that because VRE thrives in the same critically ill patients—often in the same wounds—as does MRSA, staph could steal enterococci’s vancomycin-resistance genes. The result: the most widespread hospital infection would be untreatable. (In England, researchers successfully performed this DNA transfer in the lab—and claim to have destroyed the resulting organism.) At the CDC, William Jarvis, who directs investigations for the Hospital Infections Program, worries that most doctors dismiss VRE as “wimp bugs,” less invasive and deadly than S. aureus. “They fail to recognize that VRE is colonizing the same populations of high-risk patients that MRSA colonized in the past. We’re getting this larger and larger pool of patients who are repeatedly admitted to our hospitals, repeatedly placed on antibiotics,” he says. “It’s a time bomb. Sooner or later, that genetic transfer will occur.”
If S. aureus resisted every last-resort antibiotic, a shadow would fall across medicine. Surgeons would think twice before doing elective procedures, from hip replacements to cyst removals, for fear of life-threatening complications. More people would die in hospitals: intensive care patients, surgical wound patients, dialysis patients, transplant patients, even otherwise healthy patients who happen to get a staph infection from an IV. “Clusters or outbreaks of infections could lead to closings of wards, floors, even hospitals,” says Mitchell Cohen, who directs the CDC’s division of bacterial and mycotic diseases. At least a quarter of the 50,000 serious hospital staph infections each year in this country would be fatal. Health care workers could become potential carriers and a threat to patients.
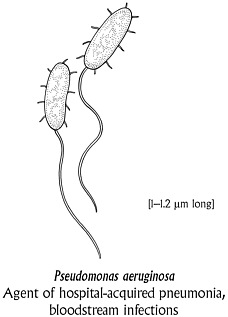
Staphylococci and enterococci are Gram-positive. In the 1990s, after a brief hiatus, Gram-negative organisms ominously rose in hospitals. They have impressive names: Pseudomonas aeruginosa, Acinetobacter baumannii, Serratia marcescens, Burkholderia cepacia, Stenotrophomonas maltophilia, and so on. But like MRSA and VRE, Gram-negatives are the dark side of medical progress. Since many of these newly ascendant Gram-negatives are water-loving bugs, they have made themselves at home in respiratory and gastric tubes, sink drains,
even flowerpots. “The reason nobody talked about Stenotrophomonas a few years ago was that there weren’t many people who lived on respirators as long as people do now,” says Robert Arbeit, an infectious disease specialist at Cubist Pharmaceuticals. “You’ve got this tube and this open airway and this mucosal surface that’s exposed to the environment. Patients get infected and then they get courses of antibiotics, which promotes resistance.” Some Gram-negative organisms resist every available drug. As a result, patients get second surgeries or other procedures. Or they die.
With hospitals whipping up armies of totally and near totally drug-resistant bacteria, what worries public health officials is that these armies may venture outside. The boundary line between hospital and hearth has been blurred lately. Sick patients often go home with intravenous lines dangling from their arms even before an infection is cured. They may trek three times a week to a clinic for dialysis. Chronically ill patients circulate between hospitals and ambulatory care centers and nursing homes. Medical progress, in other words, actually puts more people at risk of infection. “We do surgeries. We do transplants. We knock out bone marrow. We do aggressive chemotherapy,” says Glenn Morris. “All of those procedures are dependent on our ability to kill bacteria, to eliminate the almost inevitable infection that follows when you knock out the body’s immune system.” And because resistant infections take longer to treat, more semi-recovered people spread those infections into their communities.
Most surgeries now take place in outpatient centers. Antibiotic-resistant bacteria are ferried to homes, schools, work, grocery stores—places they have never visited before. Health experts fear that hospi
tals’ stubborn drug-resistance genes will be taken up by otherwise benign community microbes. Today, if you’re healthy and you’re taking care of a sick relative just out of the hospital, chances are you won’t get infected. But you could be the unlucky one, as more and more such bacteria—staph, enterococci, strep—strike out into the world.
***
How did hospitals become boot camps for resistant bacteria? Massive antibiotic use is one reason, of course. Just as important is what kind of antibiotics doctors prescribe in hospitals. Broad-spectrum antibiotics, which target both Gram-positive and Gram-negative bacteria, invite a wider counterforce of resistance. Doctors use broad-spectrum drugs to treat patients at high risk of quickly dying from infection—patients who can’t wait 24 or 48 hours for a lab to culture an organism so the doctor can make a specific diagnosis. Ken Sands, a health care quality specialist at Beth Israel Deaconess Medical Center in Boston, describes a common scenario. “Someone comes into the emergency room deathly ill: sepsis, no blood pressure, about to die. It could be a college student with meningitis, an elderly patient with a urinary tract infection leading to sepsis, a cancer patient with an indwelling line for medications. The doctors will pile on six antibiotics, might as well throw the kitchen sink at it until you know what’s going on.”
There’s a second reason resistant bacteria flourish in hospitals: hospital hygiene has grown lax. More than 150 years ago, the Austro-Hungarian physician Ignaz Semmelweis discovered that puerperal fever, a systemic infection that routinely killed women who had just given birth, spread on the hands of physicians who had also performed autopsies in the same clinic. Washing hands with chlorinated water solved the problem. Later, when the destructive power of microbes was well documented but miracle drugs hadn’t yet arrived on the scene, hospital staffs took extraordinary care to prevent infections. When the germ theory gained credence, nineteenth-century reformers such as Florence Nightingale worried that it would undermine the achievements of sanitary science.
Apparently, she was right. Today, many medical personnel expect antibiotics to cover for sloppy hygiene. Yet, of all the paraphernalia in hospitals, workers’ hands remain the most dangerous. VRE can survive on unwashed fingertips for 30 to 60 minutes. Whenever a nurse changes bandages on a weeping wound, then neglects to wash her hands or change gloves, MRSA gets a free ride. In 1997 and 1998, Pseudomonas aeruginosa, though not resistant, contributed to the deaths of 16 babies in an Oklahoma City hospital—about half the deaths due to contamination from nurses’ long fingernails. With hospital staffs cut, nurses covering a large number of patients don’t have the luxury of scrubbing their hands for 30 seconds between patients— the minimum it takes to wash VRE off their fingers with a good soap. A 1999 study from Duke University found that only 17 percent of ICU doctors properly washed their hands. Even if every hospital worker observed the utmost cleanliness so that the environment was not contaminated, it would eliminate only about a third of nosocomial (hospital-borne) infections, experts say; the rest will continue to arise when patients’ own bacteria encounter germ-fighting drugs.
The Home Front
Not all antibiotic resistance is born in hospitals. The same month that the Michigan man came down with vancomycin-resistant staph, a healthy seven-year-old girl in Minnesota died from a different Staphylococcus aureus infection. Somehow, the bacterium had breached her skin, planted an infection in her right hip, and traveled through her bloodstream to her lungs, overwhelming her body’s defenses. Staph is not supposed to kill healthy children. Her doctors were blindsided. Here was an infection that was highly unusual in the caseload of general practitioners: an MRSA strain that originated not in hospitals but in the community. Unlike most community staph infections, this one didn’t respond to the typical first-line treatments, a group of drugs known as beta-lactams, which include penicillin and cephalosporins. When the girl’s doctor prescribed these drugs, the staph continued to
march through her body, unfazed. By the time her physicians turned to vancomycin, it was too late.
Six months later, in January 1998, a 16-month-old girl from North Dakota died of a bodywide staph infection. A year after that, a 13-year-old girl from Minnesota died of pneumonia caused by staph. The next month, in February 1999, a one-year-old boy from North Dakota died from staph pneumonia. And in January 2001, a strapping 21-year-old Minnesota college student died of a fast-moving pneumonia—just eight hours after his symptoms began. Like the first Minnesota girl, their infections were caused by an MRSA. Having survived the first round of drugs, the organism had time to find a target inside the body. In a common scenario, substances in the outer walls of the staph bacterium send the immune system into overdrive, blood pressure plummets, high fevers spike, and organs shut down. Staph toxins cause internal abscesses to metastasize. Once this cascade of events begins, vancomycin is powerless. In 1999, the CDC had reported the four young deaths as a warning to doctors that this new strain of staph had to be kept on a very tight leash.
The cases should not have come as a complete surprise. There had been scattered reports earlier of MRSA in injection drug users, on Native American reservations, and in daycare centers. After the children’s deaths, CDC and state health department investigators uncovered hundreds of cases throughout the United States, mostly in children and teens—people whose infections, for unknown reasons, didn’t progress with the same deadly ferocity as in the first young victims. Though these patients didn’t die, many barely skirted danger; getting the wrong antibiotic was like getting no antibiotic at all.
If the staph that colonizes our skin starts to fend off many drugs, then the slightest skin infection—and skin infections are commonplace, the bread-and-butter of general practitioners—may someday require heavy-duty therapy. If you cut yourself chopping carrots or get an infected pimple, you could wind up with an IV in your arm. If ordinary skin infections resist more and more antibiotics, physicians will be forced to turn to the drugs of last resort. That could breed resistance in
all sorts of bacteria in our bodies. And what would be left to treat the most life-threatening illnesses?
Another alarming home-grown organism is Streptococcus pneumoniae, better known as pneumococcus. To get a sense of its tenacity, consider the case of Hollie Mullin, who was only three weeks old when she suffered her first ear infection. Her mother, Gail Mullin, a schoolteacher and first-time mom in Olathe, Kansas, thought her newborn daughter needed antibiotics. Hollie’s doctor wasn’t so sure. “Her eardrums are pink—they’re not red. Let’s watch and wait,” he told Gail. “If she starts acting fussy, give us a call.” A day or so later, as Hollie wailed uncontrollably in the background, Gail phoned back the doctor and asked for amoxicillin. She wasn’t sure whether colic or ear pain was causing Hollie’s crying, but she couldn’t stand to see her child in distress. “That started the ball rolling,” she says now, in a voice tinged with embarrassment. She wishes she had never picked up the phone.
It was October 1997. In November, Hollie developed a second ear infection, and Gail pushed for another prescription of amoxicillin.
In December, Hollie suffered a third ear infection, and this time her doctor tried a stronger antibiotic: Augmentin.
On and on it went through 1998. Every month, Hollie came down with a new ear infection and was given either repeat doses of the same drug or was switched to an increasingly potent medication. Zithromax. Rocephin. Omnicef. Lorabid. Cleocin. By her first birthday, Hollie had gone through 17 separate courses of antibiotics. The germs in her ears kept coming back, emboldened with each confrontation.
The drug regimens continued into her second year. Sometime during this period, her doctors say, Hollie’s ears became colonized with antibiotic-resistant bacteria. In June 1999, when she was 21 months old, Hollie came down with the worst ear infection yet—one that defied all the earlier drugs. This time, her physicians took drastic measures. While Hollie was under anesthesia, they threaded a catheter through a vein in her arm into her chest. Then three times a day for 14 days, while Hollie recuperated at home, Gail Mullin painstakingly administered to her daughter the antibiotic of last resort: vancomycin.
When the course of therapy was over, Hollie’s doctors emphatically told Gail that there was nothing else left to try. The vancomycin had killed off all the remaining drug-resistant bacteria; now it was time for Hollie’s immune system to regain strength. For the next six months, they warned her, Hollie absolutely had to stay well. Gail and her husband, Rob, kept their daughter home and shooed away sick visitors. Miraculously, Hollie’s immune defenses rallied so effectively that her ear infections finally ceased. “We created our own monster,” says Gail Mullin, “by using so many antibiotics that nothing worked.”
Pneumococcus is the bane of parenthood, the microbe that causes five million middle ear infections in kids a year, as well as other childhood bacterial infections. In the days before antibiotics, most ear infections went away on their own if left untreated. Today in Europe, doctors ease them with pain killers rather than antibiotics; children return to the office if they’re not better in two days. Ten years ago in the United States, treating pneumococcus with antibiotics was a snap. Daycare centers changed all that. Microbial cesspools where children on antibiotics are constantly exposed to each others’ secretions, they became hot spots for penicillin-resistant pneumococcus. At first, the outbreaks mostly struck kids from the suburbs, who had the best access to medical care and were most likely to get prescriptions. The expensive antibiotics that these children received—the cephalosporins—were not terribly effective against pneumococcus, and quickly spawned resistance. By now, it’s not only the comfortable who are afflicted; resistant pneumococcus has permeated the country.
The more antibiotics your child has taken in the past three months, the better his or her chances of carrying or getting infected by resistant pneumococcus. Depending on where you live, 25 to 40 percent of the bacteria resist penicillin and a growing list of other drugs. Pneumococcus is also starting to show “tolerance,” as microbiologists put it, to vancomycin—that is, it can survive but not reproduce when exposed to the drug. Tolerance is just a step behind full-blown resistance. And if pneumococcus resisted vancomycin, it would be bad news. More children would suffer infections of the bone surrounding the ear. Some would go on to develop meningitis—a grim challenge to doctors be-
cause, since few drugs can reach the spinal fluid, delaying treatment for just a few hours can be fatal. Children wouldn’t be the only sufferers. Pneumococcus also causes about two million cases of invasive pneumonia, mostly in older people, as well as more than 50,000 bloodstream infections a year. Those victims, too, would be more apt to die or suffer medical complications. And the effects of overtreating ear infections with broad-spectrum antibiotics may ripple even further. Drugs such as Augmentin may also be spawning resistant staph in daily life, such as the infectious agents that have killed children and young adults in the Midwest.
In 1998, the U.S. Senate held a hearing about antibiotic resistance. There, the most dramatic testimony came from a Mississippi mother named Angela Littlejohn. Her healthy 14-month-old daughter, Shauna, suffered a series of ear infections and was given a stepped-up arsenal of antibiotics. In 1989, Shauna slipped into a coma caused by drug-resistant pneumococcal meningitis. Today, Shauna remains blind and in a vegetative state, fed through a tube. “This nightmare still haunts me every day of my life,” her mother told lawmakers. And it haunts public health officials as well: Shauna’s was the first case of multidrug-resistant pneumococcus in the United States.
Cultivating Resistance
Not all resistant microbes spring from misguided human medicine. Farms are some of the most insidious sources of antibiotic resistance. As mentioned in Chapter 3, antibiotics are routinely fed in tiny amounts to farm animals—not to fend off disease, but to boost growth. And low-level use of antibiotics is a perfect way to foster resistant organisms. In recent years, livestock industry experts had estimated that 40 percent of antibiotics produced in the United States went to farm animals. In 2001, however, a report from the Union of Concerned Scientists, a Cambridge, Massachusetts–based environmental advocacy group, raised this estimate to a whopping 70 percent. Public health experts have long worried that farmers are squandering human lifesaving drugs on animals that are not even sick.
Take Campylobacter, the most common bacterial cause of food-borne illness. In 1995, American poultry farmers began using a fairly new class of drugs known as fluoroquinolones to treat respiratory infections in poultry. In people, these broad-spectrum, low-toxicity drugs are some of the most prized antibiotics today, because they are slow to breed resistance and are effective against some of the hardest-to-treat infections. Almost immediately after poultry farmers began dosing their birds with the medication, thousands of people who ate undercooked chicken contaminated with fluoroquinolone-resistant strains of campy themselves became infected with the drug-resistant bacteria. Before the drug was used, no Campylobacter specimens cultured from hospital patients had been resistant; today, nearly a fifth are, and the figure is sure to rise.
Even more dangerous than drug-resistant Campylobacter is resistant Salmonella, which is also present in poultry and meat. In human medicine, fluoroquinolones are the preferred treatment for invasive, and often life-threatening, Salmonella infections. Yet today, doctors are resorting to higher and higher doses of fluoroquinolones to treat Salmonella—a possible prelude to full-blown resistance. And now there’s a frightening new wrinkle in treating the organism. In 1998, a 12-year-old Nebraska boy picked up a Salmonella infection from his family’s cattle that was resistant to ceftriaxone—one of the cepha-losporin class of antibiotics—as well as a dozen other antibiotics. Fortunately, he survived when doctors treated him with a combination of other drugs. But when this unprecedented case was reported in 2000, it terrified public health officials. Ceftriaxone is one of the few antibiotics that reliably kills most bacteria. And it is the drug of choice for children whose Salmonella infections have entered the bloodstream— a condition that kills about 1,000 Americans every year. Ceftriaxone is also the drug that doctors turn to when treating young victims; because of worries about bone growth, quinolones are not approved for children. Since 2000, more cases of ceftriaxone-resistant Salmonella in people have turned up. “This Salmonella is so multiresistant,” says the CDC’s David Bell, “there are no good drugs left that are approved for children.” To history-minded physicians, the situation evokes futile at-
tempts at the turn of the last century to treat typhoid fever, another Salmonella infection. Extrapolating from subsequent studies of patients, health officials calculate that tens of thousands of Salmonella cases each year are ceftriaxone-resistant. The clinical problem also touches on a moral quandary: ceftriaxone is not used as a growth promoter, but rather to treat sick animals. “It portends a dilemma,” says the CDC’s Fred Angulo. “Societally, what do you want to do: treat sick people or sick animals?”
Another foodborne infection is VRE—yes, the same bug that wreaks so much havoc in critically ill hospital patients. In this country, VRE isn’t primarily foodborne; the organism is most often bred by massive vancomycin use in hospitals. It’s a different story in Europe. Soon after farmers there began feeding avoparcin, a growth promoter related to vancomycin, to livestock in 1974, the animals developed vancomycin-resistant enterococci. (Because it may be a carcinogen, avoparcin never received approval in the United States.) In 1986, France found its first human patient with VRE. Within a few years, the bacterium spread throughout human intestinal tracts on the Continent. U.S. public health experts believe that at least some of the VRE organisms in this country may have come from Europe and then proliferated under the selective influence of vancomycin in hospitals here.
But while foodborne vancomycin-resistant enterococcus infections are uncommon in the United States, a similar chain of events is starting to happen here with another drug. For more than a quarter century, American poultry farmers have used the growth promoter virginiamycin in chicken feed. In chickens, the drug helped breed enterococci that are resistant to virginiamycin’s human-use cousin, Synercid. Synercid is the other “last-resort” antibiotic, approved for humans in 1999. Yet as a frightening presentiment to the drug’s potential downfall, more than half of grocery-store chickens carry bacteria impervious to this end-of-the-line human drug. People are picking up these resistant bacteria in their meals. At any one time, at least 1 percent of the U.S. population is carrying Synercid-resistant enterococci. Usually, these intestinal bacteria are expelled as food moves through the intestines, never causing a problem. But in the rare instance that
such an individual enters the hospital—say, for a hip replacement— and happens to be treated with Synercid, the resistant enterococcal bacteria in the gut will go wild, threatening an infection that no antibiotic can quell.
One of the most frightening and enigmatic foodborne pathogens is a drug-resistant strain of Salmonella typhimurium. Known as Definitive Type 104, or DT 104, it defies five important classes of drugs in the United States; in Europe, where it surfaced in 1984, it thwarts seven. This monster resistance has helped it spread in cattle, because in animals that receive any one of these drugs, DT 104 gains an advantage. In the U.S., hundreds of thousands of people suffer DT 104 infections annually. Raw milk is a common culprit, the bacterium having infiltrated dairy herds. In 1997, for example, more than 100 Californians became sick from DT 104 in two overlapping outbreaks in Hispanic communities, where residents ate homemade Mexican-style cheese made from unpasteurized milk and sold by street vendors and specialty markets.
When scientists tried to figure out where this renegade came from, they were shocked. DT 104’s resistance genes were a strange combination—so strange, they had never before been seen in Salmonella. Where they had turned up was worlds away: in Asian aquaculture, where fish have been regularly treated with antibiotics since the early 1980s. So how did they land in the American heartland? One theory holds that some of those Asian fish may have been ground up into fish meal, an international commodity often fed to pigs and poultry. Or DT 104’s resistance genes may have found their way into animal breeding stock, perhaps through the rendered protein of other animals. However it happened, DT 104 appeared more or less simultaneously around the world in the 1980s, suggesting that the animals acquired these alien bacteria en masse.
In 1969, Britain’s Swann Committee concluded that antibiotics used in human therapy or those that promote cross-resistance in people should be banned from animal growth promotion. Unfortunately, livestock producers hew to the position that whatever drugs they feed their animals are proprietary secrets. Besides, say industry officials, they
need antibiotics to produce safe and affordable food. A 1999 report published by the Institute of Medicine and the National Research Council questioned this claim. Using the livestock industry’s own estimates, the report calculated that if farmers quit using antibiotic growth promoters, the added costs would be less than $10 per American consumer per year. And a 2001 United States Department of Agriculture report showed that hog farmers actually lose money by giving pigs antibiotics that promote growth; while animals do fatten up more, the extra poundage expands overall supply and drives down market prices.
Poultry and livestock aren’t the only creatures being dosed with drugs. Salmon, catfish, and trout on domestic fish farms get antibacterial drugs in the water. Honeybees get antibiotics in their hives. And each year, an estimated 300,000 pounds of antibiotic pesticides drift down on fruit trees and other crops to control or prevent bacterial infections such as fire blight. That disease is caused by the pathogen Erwinia, a bacterial cousin of E. coli, Salmonella, and Shigella. Erwinia now resists both streptomycin, an old drug, and tetracycline. Researchers don’t know if the fresh fruit invitingly stacked in your supermarket is delivering drug-resistant genes to your intestines. According to microbiologist Abigail Salyers, both the use of untreated or partially treated water for irrigation or for washing vegetables, or the use of manure as a fertilizer for vegetables and fruits could contaminate food plants with antibiotic-resistant bacteria. Proving that no good deed goes unpunished, a 1993 study found higher levels of multidrug-resistant bacteria in intestines of vegetarians than in meat eaters. Whether carnivore or vegetarian, you cannot avoid the aftermath of antibiotics applied lower in the food chain.
Immaculate Misconceptions
Antibiotics have tilted the playing field in favor of resistant bacteria. By snuffing out the motley crew of benign, drug-susceptible bugs in and on our bodies, they cleared a path for drug-resistant strains. Now scientists are worried about an additional selective force on bacteria: the rising tide of antibacterial products. In the last decade, more
than 1,000 new products have flooded the market: hand soaps, lotions, detergents, toothbrushes, toys, cutting boards, kitty litter, socks, bicycle pants, pillows, highchair trays, dog beds, potty seats, shopping carts, fabric cleaners, kitchen counters, even ballpoint pens. In some grocery stores, searching for a cleanser free of antibacterials is like trying to find an eight-track tape of Rod Stewart. A survey released in 2000 by Eli Perencevich, an infectious disease specialist at Boston’s Beth Israel Deaconess Hospital, found that 76 percent of liquid soaps and 29 percent of bar soaps—45 percent of soaps overall—contained antibacterials. Ironically, antibacterial-containing products are no more effective in cleaning away germs than plain soap and water. And they may actually introduce their own risks: getting rid of good bacteria while fostering drug resistance in disease-causing bacteria.
What’s wrong with all this cheerful marketing of a germ-free world? “Life is not sterile,” explains Vincenza Snow, an internist in Philadelphia. “There are actually good bacteria that live on our skin and in our mucosal lining that protect against bad bacteria. It’s not a good idea to sterilize our life or our skin.” If normal bacteria become drug-resistant from everyday exposure to household “germ-fighters,” such life-saving products as the antibacterial soaps used in ICUs and pediatric units could lose their effectiveness.
Until recently, scientists hadn’t paid these products much attention. They assumed bacteria couldn’t gain resistance to such products as the popular triclosan, a growth-inhibitor and bacteria killer that apparently kills indiscriminately, like a bomb. Industry officials chimed in that since antibacterials have been used for decades in hospitals, surely resistance would have shown up by now. But the recent flood of antibacterial products exceeds anything from the past. In 1999, investigators at St. Jude Children’s Research Hospital in Memphis showed that triclosan interferes with a specific biochemical process inside bacterial cells—and that through genetic mutation, bacteria can find a way to resist. In fact, they already do: triclosan-resistant E. coli pump the chemical out of the cell, the same efflux mechanism they use to squirt out tetracycline.
A hyperclean childhood environment may set us up for lifelong
medical problems. According to the so-called hygiene hypothesis, early exposure to certain pathogens may actually be healthy. “The maturation of the immune system requires a certain amount of contact with bacteria and maybe viruses in order to be put straight,” says Stuart Levy. Recent studies demonstrate that a larger proportion of people raised in highly hygienic environments suffer allergies and asthma. A 2000 report found that day care attendance during infancy (even if it increases the risk of drug-resistant infections) or the presence of older siblings in the home protected older children against asthma. “As we’ve added one more dimension to hygiene—use of antibacterials in the home—where will the infants have contact with the normal bacteria?” Levy asks. “My concern is that we’ll see a lot more allergy, but we won’t see it until they’re age nine, ten, eleven, twelve—and by then, you can’t go back, it’s done. If you don’t need these products, why take the chance?”
Secrets of Success
What is it about bacteria that make them preeminent survivors? What attributes do they possess that stir scientists to breathless professions of awe?
“Never underestimate an adversary that has a three-point-five-billion-year head start,” says Abigail Salyers, a microbiologist at the University of Illinois at Urbana–Champaign. A bacterium’s sole purpose is to duplicate itself. A single bacterial survivor can found a teeming colony. Above all, bacteria swap genes more easily than any other living creatures, genes that are often bundled into block grants of trouble. Even the most distantly related species can exchange DNA.
To understand the genius of bacterial defenses, you first need to know a bit about how antibiotics themselves work. Most of the 160 or so around today are variations on 16 basic chemical compounds. Some—macrolides, tetracycline, and aminoglycosides—block the manufacture of proteins needed to make new cells. Others—penicillin, cephalosporins, and glycopeptides—gum up the synthesis of a bacterium’s protective wall, so that the wall falls apart and the cell dies.
Yet others—fluoroquinolones, trimethoprim, and sulfamethoxazole— interfere with the DNA replication needed to live and multiply.
In response, bacteria have learned to hogtie drugs. They can shut the gates, camouflage themselves, spit out the drugs, waylay them, change them, or just plain destroy them. The simplest way to thwart antibiotics is to block them from entering the cell. Tetracycline-resistant bacteria pump the antibiotic out faster than it accumulates inside, a ploy known as a drug efflux mechanism (and aped by cancer cells, fungi, and parasites to bail their own chemotherapeutic nemeses). Other bacteria make enzymes that target and destroy antibiotics like guided missiles: penicillinases destroy penicillins, cephalosporinases wipe out cephalosporins. Enzymes can also hobble antibiotics such as streptomycin and other aminoglycosides by slapping them with a chemical residue. Pneumococci actually rebuild the proteins that penicillin targets, the so-called penicillin-binding proteins in the cell wall. Bacteria resistant to trimethoprim and sulfonamides make a phony copy of the enzymes those drugs normally act on, a diversionary tactic that leaves the bacterial cell safe. Staph bacteria resistant to vancomycin construct a wall that acts like a sponge, absorbing the antibiotic before it can penetrate the cell.
VRE takes the cake. It completely changes the ingredients it uses to make its cell wall, ingredients that are normally targeted by vancomycin. Switching to a brand-new biochemical recipe—a recipe biologists have never seen before—it can make a perfectly functional barrier. “That’s a real tour de force,” says David Hooper, an infection control director at Massachusetts General Hospital. “What that tells me is: No matter what we come up with, over time bugs are going to figure out a way to get around it.”
Most of the microorganisms that have given us antibiotics come from soil. The traditional explanation is that these organisms stage some kind of germ warfare with each other, protecting their turf against the intrusion of other species. Recently, scientists have mulled other theories. Maybe bacteria and fungi make antibiotics in the vanishingly small amounts they do, not to kill off their enemies, but to signal and interact with each other. Maybe antibiotic resistance genes, which have been around eons before the pharmaceutical industry, originally had
more mundane housekeeping tasks in the cell, and just happened to be ready-made for drug resistance when the drugs poured on.
Odd as it may sound, it’s the microorganisms that produce antibiotics that are also the source of resistance genes to that antibiotic. The cluster of genes that VRE uses to fend off vancomycin, for instance, is the same cluster found in the soil organism that makes vancomycin, Amycoloptosis orientalis. It is likely that bacteria need these resistance genes to help them fend off their own toxic products. The practical implication is that whenever scientists stumble on a new antibiotic, they should be able to find in the organism that churns it out genes that other bacteria will deploy to resist the drug—a preview, in other words, of how resistance will arise in humans.
Bacteria live in a tariff-free zone. Resistance genes move freely across species—even between Gram-positives and Gram-negatives, a distance as vast in phylogenetic terms as that separating an amoeba and Albert Einstein. Staphylococcus shares resistance genes with Listeria. E. coli has traded DNA with Pseudomonas and Neisseria. MRSA became the beast that it is by steadily building its genetic stockpile. “The exchange of genes is so pervasive,” writes Stuart Levy, “that the entire bacterial world can be thought of as one huge multicellular organism.” This fluidity may enliven the social lives of these austere one-celled organisms, but it’s a disaster for public health. The history of antibiotic resistance reads like a genetic travelogue.
How do they do what they do? Let’s start with genetic mutation, the basic engine of evolution. In duplicating itself, a bacterium may accidentally alter a gene. That change may give it new armor against certain drugs, and a competitive advantage over its neighbors that lack the new gene. A single mutation helped the tuberculosis bacterium resist streptomycin; in the early 1990s, a sequence of other mutations lent it resistance to other drugs. The newfound strains of linezolid-resistant staph and enterococcus both rely on chromosomal mutations—which can be passed on to progeny—to evade the drug. But it can take many throws of the genetic dice before an organism mutates into resistance. Pneumococcus, for instance, took a quarter century to resist penicillin, and group A Streptococcus hasn’t even managed that.
Some genetic trade routes link two closely related species. In a
process known as transduction, a bacteriophage virus infects a bacterium, incorporates that cell’s resistance genes into its own genome, then copies itself and bursts out to infect new bacterial cells, carrying along the resistance genes. Some scientists think Staphylococcus aureus acquired its methicillin resistance gene this way. In a genetic exchange program called transformation, a bacterium scavenges floating pieces of DNA released by a dead bacterial cell from a closely related species, integrating the “naked” DNA into its chromosome. Through transformation, Pneumococcus first became penicillin resistant.
The best genetic get-rich-quick scheme, however, is not to save or scrounge but to steal resistance genes right off the shelf from a donor cell. “If bacteria had a brain,” says Abigail Salyers, “this would be a no-brainer.”
The particulars of “horizontal gene transfer,” as it is called, first came to light in the 1950s. In 1959, Japanese scientists isolated a Shigella dysenteriae that resisted four different kinds of antibiotics: tetracycline, sulfonamide, streptomycin, and chloramphenicol. Then as now, Shigella was a major cause of dysentery in Asia and Central and South America. The pokey mutability of the bacterium’s own chromosome couldn’t account for this sudden wealth of resistance. In fact, Japanese scientists calculated that the microbe would have had to divide 10 million × 10 million × 10 million × 10 million times—far longer than bacteria have been on earth, or than there’s been an earth—to have pulled off this quadruple hat trick. At the same time, researchers found strains of benign E. coli resistant to the same four drugs. In what direction the gene package traveled—from the E. coli to the Shigella or the other way around—is not known. What’s important is how they rode: on circles of DNA known as plasmids which, carrying genes resistant to several drugs, enabled the consignees to quash agents they’d never seen before.
“It was an incredibly novel aspect of science,” says Julian Davies, professor emeritus of microbiology at the University of British Columbia. So novel that the first papers published in Japan were rejected in the United States, and at least one researcher lost his job over the new proposition. According to Davies, “The convention was that genes just
don’t move around. If genes move around, how could you possibly have species? But genes do move around, and one wonders what ‘species’ really means.”
Plasmids are mobile loops of DNA separate from the bacterium’s chromosome. You can think of them as shopping carts where bacteria store genes that they only need now and then. Plasmids pack genes for all kinds of emergencies: to withstand temperature extremes and ultraviolet light, to survive a torrent of gastrointestinal juices, to degrade environmental pollutants—and to resist antibiotics. Plasmids reproduce and migrate during the tryst known as conjugation, in which two, often unrelated, bacterial cells briefly draw together and pass their genes to the other in several ways. Antibiotics such as tetracycline may act as aphrodisiacs, prompting bacteria to mate with abandon and indulge in an orgy of gene transfer. Over time, plasmids and their bacterial hosts can enter a symbiotic relationship, in which the growth of the host depends on the plasmid—one reason that the drug resistance bestowed this way is hard to reverse.
Resistance genes can also ride on mobile pieces of DNA called transposons. Known colloquially as “jumping genes,” transposons, unlike plasmids, are truly free spirits. They don’t need the host cell to survive; they can dash off whenever they like. A special kind of transposon known as a conjugative transposon plays a major role in antibiotic resistance. Conjugative transposons bearing resistance genes can jump from their seat on the donor chromosome onto a plasmid, then during mating stow away on that plasmid to another bacterium. Once they’re settled again, they can jump from the plasmid to the new host’s chromosome—a stable perch from which to do their job.
This genetic free-for-all creates problems for medicine. At Emory University, population geneticist Bruce Levin has found that resistance to an antibiotic persists long after doctors have stopped using that drug. This is a blow to researchers who hoped that bacteria resistant to over-used drugs would “evolve backward” if spared the drug. Analyzing the fragrant contents of diapers from a daycare center, Levin found that a quarter of the E. coli lurking between the folds resisted streptomycin, a drug rarely used in the past 30 years. Although in evolutionary theory
resistant bacteria are presumed to be more genetically weighed down and therefore less fit to compete, Levin suspects that after E. coli gains drug resistance, it evolves a second compensatory mutation that keeps it from backsliding to a state of drug sensitivity.
“Resistance genes,” says Abigail Salyers, “are easy to get and hard to lose.” The mechanics of plasmid transfer leads to an exponential rise in resistance genes. And a single antibiotic to treat an infection can provoke resistance to other drugs. Take tetracycline for a chlamydia infection, say, and your gut bacteria can suddenly become resistant to half a dozen different, structurally unrelated antibiotics. One reason may be a master switch—dubbed MAR, for Multiple Antibiotic Resistance—on the cell’s chromosome. “It’s almost as if bacteria strategically anticipate the confrontation of other drugs when they resist one,” writes Stuart Levy, whose lab discovered MAR in Gram-negative organisms such as E. coli and Salmonella. Moreover, though resistant strains can drop in number if they lose out in competition with drugsensitive strains, they seldom disappear completely. That means there’s always a residue of resistant bacteria around, ready to multiply if the right antibiotic rains down on them.
Resisting Resistance
At the start of 2001, the U.S. Department of Health and Human Services announced an “action plan” to combat antibiotic resistance. But in the United States, it’s impossible to get a firm grasp on the threat. The National Nosocomial Infection Surveillance system, a CDC-sponsored voluntary reporting effort among U.S. hospitals, is not comprehensive. Indeed, no federal agency tracks all resistant infections or adds up their human and financial costs. And admittedly, statistics can play tricks. If raw data were all that counted, large teaching hospitals with very sick patients would look like they’re doing a bad job—which is why you’ll probably never find out about a hospital’s antibiotic resistance problems before you or someone you love is admitted. Even then, it’s hard to get the lowdown.
Fighting antibiotic resistance is like wrestling Kali, the many-armed
Hindu goddess of life and death. It is not one problem but many. While some observers offer visionary solutions, and others practical nostrums, nearly everyone involved complains that deeper institutional battles are slowing progress. On one fact everyone agrees: the propensity of bacteria to alter themselves in the face of threat will never be halted, merely contained. The most that public health experts hope for is to transform antibiotic resistance from a crisis—as it is now—to a routine annoyance.
One way is to speed up the pharmaceutical production line. Today’s antibiotics belong to a surprisingly small number of structural groups, most descendants of older progenitors harvested from nature. A recent exception is linezolid, a synthetic drug and the first new antibiotic in 35 years. Because the compound is manmade—and would theoretically not encounter any preexisting resistance genes in nature— researchers expected that the drug would have a long shelf life. But dismayingly, as Mary Jane Ferraro and others have discovered, linezolid-resistant forms of both staph and enterococcus appeared almost instantly. Tomorrow’s antibiotics may be plucked from huge collections of synthetic molecules which, with new technology, can be tested in huge numbers against resistant organisms. Gene sequencing will accelerate this process by laying out complete genetic sequences of bacteria—and therefore, new biochemical pathways to target.
A second approach is to take a well-respected antibiotic that has lost its clout and give it a second life. Stuart Levy’s lab, for example, is bioengineering new tetracyclines that can block the pump in bacteria that spit it out.
A third, somewhat theoretical, approach deploys bacteriophages—the viruses that target bacteria. The inspiration for their therapeutic potential goes back to a 1917 report by Felix d’Hérelle, a young French bacteriologist, who observed that the bloody stools of soldiers struck by dysentery contained invisible agents, thought to be viruses, that could destroy the offending bacteria. D’Hérelle went on to predict that these viruses, or phages, could cure all manner of bacterial disease. Since a phage virus makes copies of itself—a single phage produces more than a billion progeny in three to five hours—it is
potentially the only drug that could multiply itself in the body. Since the 1930s, phage work proceeded apace in the (now former) Soviet Union, with claims of success against Enterococcus and other mostly enteric and skin pathogens. More recently, researchers have completed promising experiments with mice and are embarking on human trials. Today, several American biotech companies have taken the baton, hoping to cultivate phages against VRE, MRSA, and other bugs.
Drawing on the fact that no infectious diseases have ever been eliminated by antibiotics, other experts are focusing on vaccines as the ultimate end-run around resistance. During the 1980s, Haemophilus influenzae type B (HiB) was the leading cause of meningitis in American infants and a major agent of blood poisoning and pneumonia. But since 1989, when the HiB vaccine came out, HiB meningitis has virtually disappeared in the United States. A pneumococcal vaccine approved for children in 2000 has likewise proven effective against serious complications such as bloodstream infections and pneumonia, and is expected to curtail not only kids’ ear infections but the resulting overuse of antibiotics. More challenging will be making vaccines against staph or enterococci, since these organisms are benign lodgers against which the body doesn’t mount a strong immune response— making them fuzzy targets for vaccines.
There are also ecologic approaches to defusing resistance. Researchers talk of biodegradable antibiotics that would lose their resistance-breeding potency once released into the environment. Another proposal would harness the evolutionary forces that foster resistance and turn them to our favor. Picture a bacterial reclamation project, in which resistant flora are replaced with friendly—i.e., drug-sensitive— microbial species. In Stuart Levy’s mind, that requires first stopping the use of certain antibiotics so that the selective pressure is off, and then literally restocking the environment with susceptible bacteria— say, by spraying drug-sensitive enterococci in intensive care units. Other scientists, however, worry that these newly added bacteria will also become resistant.
***
But technological fixes take time. At the CDC, researchers estimate that a third of the 150 million annual outpatient prescriptions for antibiotics are unnecessary, either because the illness is not bacterial or because the bacteria aren’t sensitive to the antibiotics. According to a 1998 study, antibiotics were prescribed 66 percent of the time during office visits for coughs, even though most coughs—and sore throats and runny noses—are caused by viruses, which antibiotics can’t touch.
In response, the American College of Physicians in 2001 issued new recommendations urging doctors to use antibiotics for common respiratory illnesses only when they strongly suspect a bacterial cause. Respiratory infections account for three-quarters of all antibiotic prescriptions. “We were all taught in medical school that anybody who was coughing up something green had a bacterial infection. But now we know that this is just the natural evolution of a viral infection,” says internist Vincenza Snow, who coauthored the ACP guidelines. “As physicians, we have to unlearn some of the things we’ve been taught. And we have to reeducate our patients.” In 2000, the federal Agency for Healthcare Research and Quality found that the vast majority of children with middle ear infections recover without antibiotics—so waiting for a few days won’t put kids at risk, even when they require treatment later for their illness. Patients who do take antibiotic drugs are being reminded to take all their pills, so as not to promote resistant bacteria.
Doctors and patients may finally be getting the message. A CDC survey found that between 1989 and 1998, antibiotic prescriptions for children under 15 dropped by 30 percent. Unpublished data show that, among adults, antibiotic prescriptions fell by 10 to 15 percent between 1995 and 1999. But according to experts, these declines must double before the upward trend in antibiotic resistance reverses.
To curtail antibiotics, doctors need to know precisely what’s ailing their patients. That’s not always easy. Today, there are no tests to instantly pin down what bug is causing an infection and what drugs it resists. Besides, managed care groups are trying to save money by cutting back on tests, including microbiologic cultures, because it’s cheaper to prescribe broad-spectrum drugs and wait to see if patients
get better. If new gene-based tests were around tomorrow, would doctors use them? More to the point, would health maintenance organizations pay for them?
Meanwhile, the Food and Drug Administration has focused on cutting agricultural antibiotics crucial in human medicine—playing a long-delayed game of catch-up. In 1977, when the agency first proposed removing penicillin and tetracycline from growth promoters, Congress blocked the move. “That set back the national agenda for 20 years,” says the CDC’s Fred Angulo. By 2005 or so, the agency intends to establish regulations that will automatically remove an antibiotic from farm use if it’s proven to cause high levels of drug-resistant infections in people. The focus will be on preserving drugs crucial for human medical therapy. For their part, consumers may think twice about buying household products that trumpet their “germ-fighting” prowess.
Many public health experts are betting on an up-to-the-minute information system that could tell doctors what resistant organisms are in their community and therefore what drugs to steer away from. But there are times when all the information in the world won’t help a doctor make a tough call—times, in fact, when a doctor’s drive to deliver the best clinical care seems at odds with public health campaigns against resistance. Doctors, after all, are advocates for their patients— not for all patients, not for global ecology. “It gets into some extremely difficult philosophical questions,” says the University of Maryland’s Glenn Morris. “I’m the bad guy. I wear the black hat. Because I tell doctors they can’t use drugs that they think they need for their patients.” The tension between what’s right for the individual and what’s right for public health becomes especially poignant at the end of life. Should a doctor give last-resort antibiotics to a patient who is sure to die soon anyway—even if it means raising the risk of drug resistance in another patient five feet away?
“When you’re looking a patient in the eye, or when you’re looking a farmer in the eye who’s got a flock of sick chickens, it’s very difficult to say, ‘I’m not sure you need that antibiotic,’” says Morris. “If it’s your grandmother sitting in the hospital with a bad infection, would you
prefer that the doctor gave her three antibiotics to make sure he’s covered whatever’s causing the infection, or that he said, ‘Let’s just give her one and wait for the culture to come back’? The answer is, of course, ‘Do everything you can, Doc!’ Multiply that by hundreds of thousands of cases, and you have overuse in hospitals.”
The daunting challenge of antibiotic resistance owes itself to institutional complacency as well. Few researchers today have been trained in the basic biology of bacteria—because few university laboratories are left to specialize in the problem of drug resistance. Discouraged by the dearth of funding for the field, young investigators have chosen other disciplines.
Nor has the pharmaceutical industry been keen to tackle drug resistance. The biological paradox that antibiotics sow the seeds of their own failure is matched by an economic paradox: if a new antibiotic is good, regulators will ask doctors to use it sparingly and the drug won’t quickly recoup its investment. Despite the development of linezolidresistant staph and enterococcus, will its manufacturer push the new drug? “The pneumonia market is many orders of magnitude larger than the enterococcus market,” says John Quinn, a physician at the University of Illinois at Chicago, who first published evidence of linezolid-resistant VRE. “And if you’re sales manager for a new agent, and your compensation is linked to the number of doses of that drug being administered, it’s got to be awfully tempting to promote the use of the drug in respiratory infections. I’m not making a specific accusation that the company is doing that. But certainly the history of antibiotics is one of enthusiastic use followed by overuse followed by resistance.”
Making matters worse, most of the easy drug targets have already been discovered, so that it’s even more costly to find chinks in bacterial armor. This dilemma could discourage drug companies from investing in what typically takes at least seven years and costs $350 million to bring a new antibiotic to market. At the end of that road, what companies want is a blockbuster like Viagra or Prozac, something that will stand out from its competitors and make an immediate $2 billion to $4 billion. “In most companies, antibacterial discovery and development
is a Cinderella field,” says David Shlaes, vice president of infectious disease research at Wyeth-Ayerst Research. “In the 1980s, drug companies started getting out of this business in droves, and that hasn’t stopped. It remains for the pharmaceutical companies a tight market and a competitive market.” To offset the economic losses of a rationed drug, companies might need to be compensated with longer patents, fast-track approval, or other marketing incentives for drug development, as orphan drugs for rare diseases now receive. “When we find a drug effective against VRE,” says Glenn Morris, “we should use it only against VRE, even if we’re only talking ten thousand to twenty thousand cases a year.”
Controlling hospital infections would also help cut down drug resistance. In the last two decades, the rate of hospital-acquired infections has risen in part because today’s patients are sicker and more vulnerable. Yet there are few incentives for hospitals to monitor infection rates. A head-in-the-sand attitude prevails in this country: If hospitals don’t look for resistant infections, they won’t find them and they won’t have to fret about them. Besides, the thinking goes, why should one institution pay a public relations price for a problem entrenched in every hospital? In our competitive and cost-cutting times, infection control departments are perceived as nests of unbillable activities. “If I’ve got to make a choice between adding an infection control nurse or a hospital epidemiologist versus a cardiac surgeon,” explains the CDC’s William Jarvis, “I’m choosing the cardiac surgeon, who can bring me several million dollars a week.”
Yet a mathematical model developed by Emory University’s Bruce Levin and Harvard School of Public Health’s Marc Lipsitch underscores the need for infection control. It says that the influx of fresh, drug-sensitive bacteria carried by newly admitted patients should be able to outcompete resistant strains in hospitals—as long as those hospitals vigorously try to prevent antibiotic resistance. Judging from the few documented interventions attempted in this country—controlling VRE rates by segregating colonized patients, reducing resistant bloodstream infections among cancer patients through infection control, and
others—prevention can save money in the long run. But that will happen only if every hospital and doctor shoulders the task equally.
Hospital administrators claim that outside pressures force doctors to err on the side of prescribing antibiotics, even when unnecessary. Four floors above the emergency room of Boston’s Beth Israel Deaconess Medical Center, ambulance sirens repeatedly pierce the air. From that perch, Robert Moellering Jr., chair of the Department of Medicine, must grapple with the legal repercussions of pressured medical decisions. “We’re in this position of trying to get physicians not to overuse antibiotics,” he says. “But I have never yet seen a physician sued for giving antibiotics inappropriately. I’ve seen all kinds of them sued for not giving antibiotics.” This fear of malpractice suits, Moellering says, also stokes antibiotic resistance.
We’re not yet on the brink of a post-antibiotic age. Compared to the last turn of the century, we have better hygiene, sanitation, and nutrition, safeguards that have always prevented disease from starting and spreading. And even though 70 percent of the bugs that cause hospital infections defy at least one antibiotic, there are usually four or five others to try.
But like love, drug resistance is here to stay. “We have squandered an immense resource, much of it a true natural resource, by using it frivolously, inappropriately, and ineptly. . . . Above all, we polluted our hospitals, and in doing so we set up a truly global laboratory: a colossal Darwinian experiment in enhanced evolution,” writes the physician Imre J. P. Loefler, in the Lancet. “We wasted resources that, if husbanded, would have helped us treat infections perhaps for hundreds of years. We squandered because of ignorance, consumerism, mercantilism, cynicism, and carelessness.”
Tracking the relentless rise of resistance at the University of Maryland Medical Center, which had the dubious honor of being one of the first to report VRE in this country, Glenn Morris feels a sense of dread. “This is the gradual, inexorable movement of a glacier headed directly toward your town. It’s slow, silent, unexciting. But every year you look at the ‘Percent Resistant’ isolates in your hospital. At times it feels like we’re hanging on by our fingernails.”