Meeting Psychosocial Needs of Women with Breast Cancer (2004)
Chapter: Appendix B Tables and Boxes Summarizing Evidence from Clinical Trials
TABLE B-1 Randomized Trials in “Early” Breast Cancer
|
Citation |
n |
Intervention(s) |
Duration |
Outcomes |
|
Maguire 1980 1983 |
172 |
Individual counseling by nurse specialist vs. control |
Every 2 months after surgery until woman had “adapted well” |
• Nursing interventions did not reduce morbidity directly; however, it led to increased recognition of the need for psychiatric referral which, in turn, reduced psychiatric morbidity, anxiety and depression. (follow-up to 12-18 months) |
|
Christensen 1983 |
20 |
Postmastectomy couple counseling vs. control |
Weekly x 4 weeks |
• No overall treatment effects (small sample size may have precluded identification of effects) • Adjusted analyses suggested tentative benefits in sexual satisfaction and psychological status (husbands and wives) and depression (wives). (follow-up to 1 week post intervention) |
|
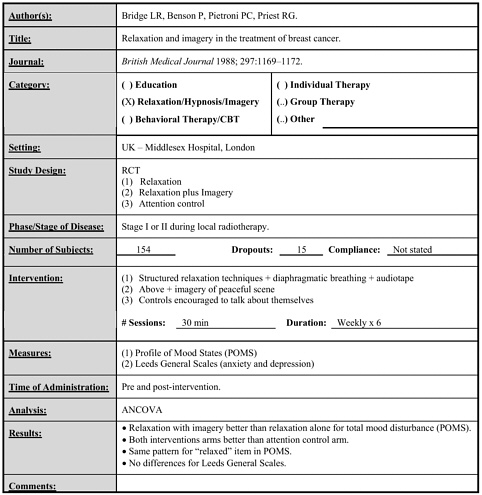
Bridge 1988 |
154 |
Structured relaxation vs. relaxation plus imagery vs. attention control |
Weekly x 30 minutes x 6 weeks |
• Overall mood and relaxation better for relaxation plus imagery than for relaxation alone. • Both better than attention control arm. (follow-up to immediately post intervention) |
|
Cimprich 1993 |
32 |
“Restorative intervention” - individualized protocol to identify and practice restorative experiences |
20–30 minutes 3x/week x 7 weeks |
• Intervention improved attentional capacity and total attentional score. (follow-up to immediately post intervention) |
|
Citation |
n |
Intervention(s) |
Duration |
Outcomes |
|
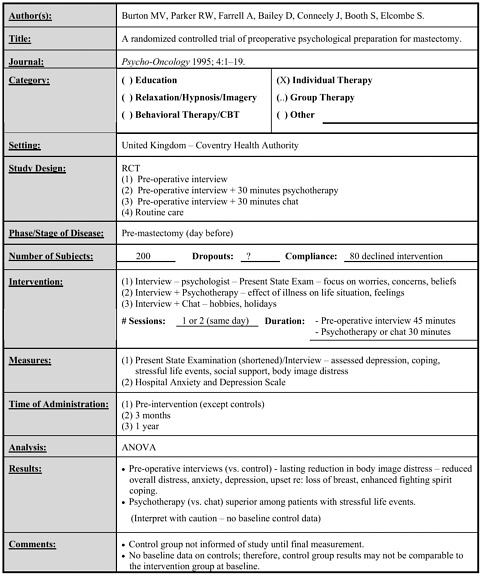
Burton 1995 |
200 |
Psychological interview vs. interview plus 30 minutes psychotherapy (surgeon) vs. interview plus 30 minutes chat vs. control (all pre-mastectomy) |
One day – 45 minute interview, 30 minute psychotherapy or chat |
• Psychological interview led to lasting reduction in body image distress and reductions in overall distress, anxiety, depression, upset regarding loss of breast and enhanced fighting spirit coping. • Psychotherapy better than chat among women with stressful life events. (follow-up for one year – controls unaware of study until end of study, did not provide baseline data) |
|
Maunsell 1996 |
259 |
Telephone screening of distress (with social work referral) vs. routine care |
Monthly x 2 (average 7.6 minutes each) |
• No significant effects. (follow-up to 12 months) |
|
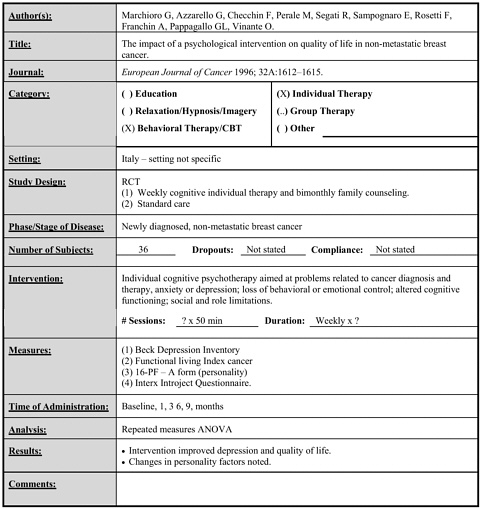
Marchioro 1996 |
36 |
Individual cognitive therapy focusing on problems relating to cancer therapy vs. standard care |
Weekly x 50 minutes x ? duration |
• Intervention improved depression and quality of life. • Some changes in personality factors were noted. (follow-up to 9 months) |
|
McArdle 1996 |
272 |
Nurse specialist support vs. voluntary organization support vs. both vs. neither |
Variable |
• Support from nurse specialist resulted in improved somatic symptoms, social dysfunction and depression. • Nurse support significantly better than voluntary organization support. |
|
Richardson 1997 |
47 |
Group support (non-structured, supportive) vs. imagery/relaxation group with one individual session vs. standard care |
Weekly x 1 hour x 6 weeks |
• Enhanced coping skills in Support (p<0.01) and Imagery group (p<0.07) vs. control. • Women in both types of groups sought more support from others. • Women in support group had greater acceptance of death. (follow-up to immediately post intervention) |
|
Citation |
n |
Intervention(s) |
Duration |
Outcomes |
|
Samarel 1992 1993 1997 |
228 |
Structured support group with coaches (family, friend, spouse) vs. structured support group without coaches vs. control |
Weekly x 2 hours x 8 weeks |
• Support group with coaching resulted in higher quality relationships at the end of the intervention but not 8 weeks later. • No effect on symptom distress or mood. (follow-up to 8 weeks) |
|
Kolcaba 1999 |
53 |
Guided imagery audiotape vs. control |
Audiotape use daily during radiation and for 3 weeks after |
• Intervention significantly improved comfort. (follow-up to 3 weeks post radiation) |
|
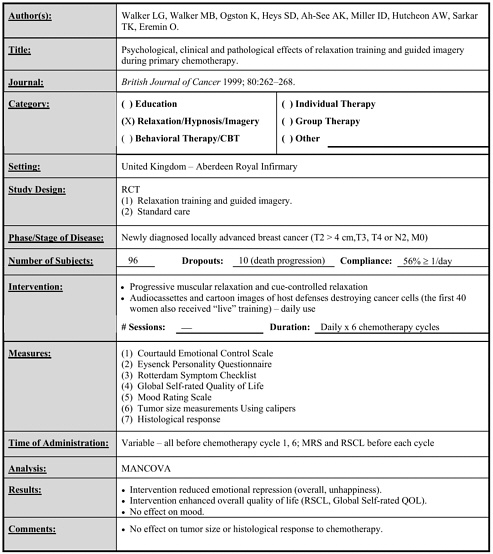
Walker 1999 |
96 |
Relaxation and guided imagery vs. standard care |
Daily for 6 chemotherapy cycles |
• Intervention enhanced overall HRQOL and reduced emotional repression (overall, unhappiness). (follow-up to end of intervention) |
|
Wengström 1999 2001 |
134 |
Individual nursing intervention based on Orem’s model for self-care vs. standard care |
Weekly x 30 minutes x 5 weeks |
• Intervention led to fewer distress reactions but no difference in HRQOL or toxicity. • Intervention resulted in “Stronger motivation to be emotionally involved” in those over 59 years old. (follow-up to 3 months post intervention) |
|
Citation |
n |
Intervention(s) |
Duration |
Outcomes |
|
Sandgren 2000 |
62 |
Telephone-based individual cognitive–behavioral therapy vs. assessment only |
Weekly x 4, then every 2 weeks x 6 (each < 30 minutes) |
• No consistent effects of the intervention over time. • Borderline effects for stress (early benefit, late detriment), anxiety and confusion (benefit), physical role functioning (early detriment) and mental health (early benefit). (follow-up to 10 months) |
|
Bultz 2000 |
36 |
Psycho-educational group for partners of breast cancer patients vs. control |
Weekly x 90–120 minutes x 6 weeks |
• No significant effects. • Borderline improvement in mood of partner (p=0.07) and breast cancer patients (p=0.06) 3 months after intervention. (follow-up to 3 months post intervention) |
|
Ritz 2000 |
210 |
Advanced practice nursing interventions (individual) vs. control |
Not specified |
• Intervention led to reduced uncertainty at 1, 3, 6 months (but not at 12 months). • Effect greatest in unmarried women. • Beneficial effect on mood at 1, 3 months in subgroup without a family history. (follow-up to 12 months) |
|
Fukui 2000 |
50 |
Cognitive–behavioral group therapy with muscle relaxation and guided imagery vs. control |
Weekly x 90 minutes x 6 weeks |
• Intervention significantly improved mood, vigor and fighting spirit coping at the end of the intervention. • Effects were marginal at 6 months. • No effect on depression or anxiety. (follow-up to 6 months) |
|
Citation |
n |
Intervention(s) |
Duration |
Outcomes |
|
Helgeson 1999 2000 2001 |
312 |
Education group vs. Peer discussion group vs. Education and peer discussion group vs. control |
Weekly x 60 minutes x 8 weeks |
• Education group resulted in enhanced vitality, mental health and social functioning compared to peer discussion. • Education group resulted in above plus enhanced role functioning and reduced bodily pain compared to controls. • No benefits observed for peer discussion. • Effects “dissipated over time.” (follow-up for 48 months) |
|
Simpson 2001 |
89 |
Structured group psychotherapy vs. control (self-study) |
Weekly x 60 minutes x 6 weeks |
• Intervention reduced depression and severity of psychiatric symptoms and enhanced mood and HRQOL at 2 years (but not at earlier times). (follow-up for 2 years) |
|
Lev 2001 |
53 |
Individual counseling plus videotape plus self-care booklet vs. control (educational booklet) |
Monthly x ? minutes x 5 months |
• Small to large effect sizes for HRQOL, psychiatric symptoms. • No statistical significance testing. (follow-up to 8 months) |
|
Antoni 2001 |
100 |
Structured cognitive–behavioral group intervention vs. 1 day seminar (controls) |
Weekly x 2 hours x 10 weeks |
• No overall effects. • Intervention reduced the prevalence of moderate depression and it increased benefit finding and optimism. (follow-up to 9 months post-intervention) |
|
Citation |
n |
Intervention(s) |
Duration |
Outcomes |
|
Molassiotis 2002 |
71 |
Progressive muscle relaxation training (individual session, audio and videotapes) vs. control |
Daily x 30 minutes x 6 days |
• Intervention reduced total mood disturbance, duration of nausea and vomiting (trend to reduced frequency of nausea and vomiting). • No effect on intensity of nausea and vomiting. (follow-up for 14 days) |
|
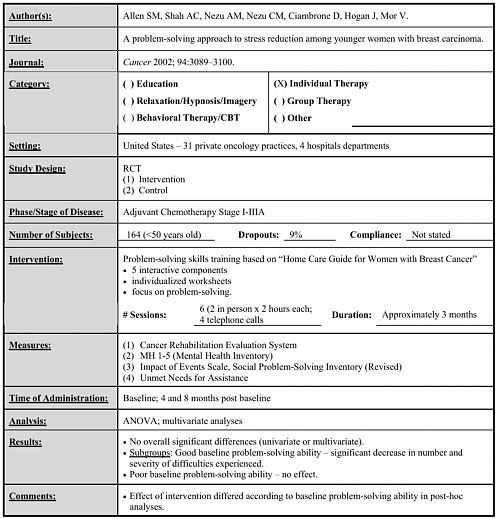
Allen 2002 |
164 |
Individual problem skills training vs. control |
6 sessions over 4 months (2 in person, 4 by telephone) |
• No overall effects. • Subgroup analysis indicated benefit in women with good baseline problem-solving ability. (follow-up for 8 months) |
|
Targ 2002 |
181 |
Standard psychoeducational group vs. mind–body–spirit (CAM) group |
Standard – 12 sessions x 90 minutes weekly x 12 weeks CAM – 24 sessions x 150 minutes twice weekly x 12 weeks |
• Both interventions improved HRQOL and psychosocial functioning. • CAM led to greater spiritual integration and satisfaction. (follow-up for 12 weeks) |
TABLE B-2 Randomized Trials in “Metastatic” Breast Cancer
|
Citation |
n |
Intervention(s) |
Duration |
Outcomes |
|
Spiegel 1981 1983 1989 |
86 |
Supportive–expressive group therapy vs. control |
Weekly x 90 minutes x ≥ 1 year |
• Intervention improved mood, reduced maladaptive coping responses and phobias. • Intervention prolonged survival (mean 36.6 vs. 18.9 months intervention vs. control). (psychological follow-up x 12 months, survival > 10 years) |
|
Arathuzik 1994 |
24 |
Individual structured relaxation and visualization with or without cognitive–behavioral therapy vs. written handouts about pain distraction |
1 x 75 minutes (relaxation and imagery alone) |
• No effects of intervention. (same day follow-up) |
|
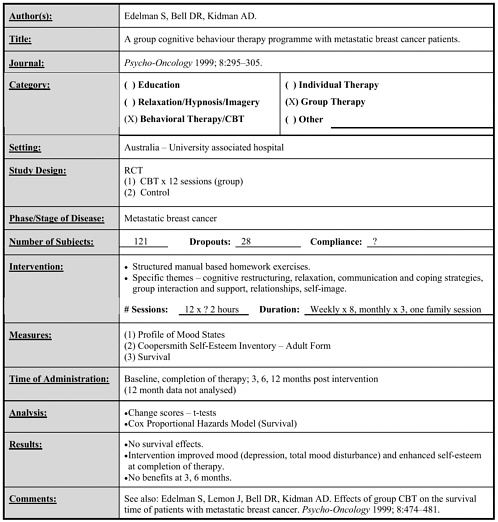
Edelman 1999 |
121 |
Group cognitive–behavioral therapy vs. control |
Weekly x 8, monthly x 3, one family session (each 2 hours) |
• Intervention improved mood and reduced depression, enhanced self-esteem. • Effects present at end of intervention but not 3 or 6 months later. • No effect on survival. (follow-up 12 months for psychological outcomes, 2 to 5 years for survival) |
|
Edmonds 1999 Cunningham 1999 |
66 |
Supportive plus cognitive–behavioral group therapy vs. home cognitive–behavioral study program |
Weekly x 2 hours x 35 weeks (longer in some women) plus one weekend |
• Intervention subjects experienced more anxious-preoccupied coping and less helplessness coping. • No survival effects. (psychological follow-up x 12 months, survival to > 5 years) |
|
Citation |
n |
Intervention(s) |
Duration |
Outcomes |
|
Classen 2001 |
125 |
Supportive–expressive group therapy vs. control |
Weekly x 90 minutes to end of life |
• Intervention significantly reduced traumatic stress symptoms – enhanced mood if final assessment during the year prior to death was excluded. • Survival effects pending. (follow-up to 12 months) |
|
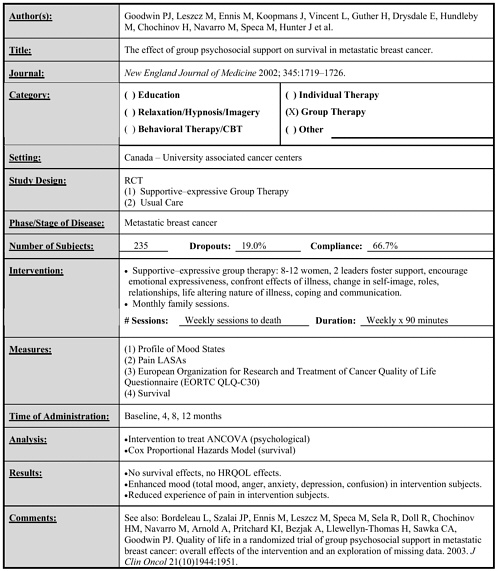
Goodwin 2002 |
235 |
Supportive–expressive group therapy vs. control |
Weekly x 90 minutes to end of life |
• Intervention significantly enhanced overall mood, depression, anxiety, anger, confusion and experience of pain. • Intervention had no effect on survival. (follow-up to end of life) |
TABLE B-3 Summary of the Effectiveness of Psychosocial Interventions in Breast Cancer
|
I. Relaxation/Imagery* |
|||||||
|
Citation |
Phase |
n |
Intervention |
Duration of Intervention |
Effectiveness |
Duration of Benefit |
Duration of Follow-up |
|
Bridge 1988 |
Early |
154 |
• Relaxation (audiotape) • Relaxation/Imagery |
6 weeks |
• Improved mood, relaxation. • Imagery and relaxation had additive effects. |
6 weeks |
6 weeks |
|
Richardson 1997 |
Early |
47 |
• Relaxation/Imagery group intervention |
6 weeks |
• Greater acceptance of death, enhanced coping – no effect on mood. |
6 weeks |
6 weeks |
|
Kolcaba 1999 |
Early |
53 |
• Guided imagery audiotape |
Radiation and 3 weeks after |
• Improved “comfort”. |
3 weeks post radiation |
3 weeks post radiation |
|
Walker 1999 |
Early |
96 |
• Relaxation/guided imagery (audiotape) |
6 cycles of chemotherapy |
• Improved overall HRQOL • Reduced emotional repression. |
To end of chemotherapy |
To end of chemotherapy |
|
Molassiotis 2002 |
Early |
71 |
• Progressive muscle relaxation – audio and videotape |
6 days |
• Improved mood, reduced duration and frequency but not intensity of nausea, vomiting. |
14 days |
14 days |
|
Arathuzik 1994 |
Metastatic |
24 |
• Relaxation plus visualization with or without cognitive–behavioral therapy |
1 session |
• No effect. |
1 day |
1 day |
|
* Does not include studies in which relaxation/hypnosis/imagery was delivered as a minor part of another intervention. |
|||||||
|
II. Group Interventions |
|||||||
|
Citation |
Phase |
n |
Intervention |
Duration of Intervention |
Effectiveness |
Duration of Benefit |
Duration of Follow-up |
|
Richardson 1997 |
Early |
47 |
• Non-structured support group |
6 weeks |
• Greater acceptance of death, enhanced coping |
6 weeks |
6 weeks |
|
Samarel 1992 1993 1997 |
Early |
228 |
• Structured support group with or without coaches |
8 weeks |
• Coached groups resulted in higher quality relationships |
8 weeks |
16 weeks |
|
Helgeson 1999 2000 2001 |
Early |
312 |
• Education group • Education group plus peer discussion group • Peer discussion group |
8 weeks |
• Education group enhanced vitality, mental health, social functioning, role functioning and reduced bodily pain. • No benefits of peer discussion. • Effects “dissipated” over time. |
48 months |
48 months |
|
Simpson 2001 |
Early |
89 |
• Structured group psychotherapy |
6 weeks |
• Reduced depression and severity of psychiatric symptoms, enhanced mood and HRQOL |
24 months |
24 months |
|
Targ 2002 |
Early (<10% metastatic) |
181 |
• Psychoeducational group • Mind–body–spirit group (CAM) |
12 weeks |
• Both groups improved measures of HRQOL, psychosocial function. • CAM improved spiritual integration, satisfaction. |
12 weeks |
12 weeks |
|
Citation |
Phase |
n |
Intervention |
Duration of Intervention |
Effectiveness |
Duration of Benefit |
Duration of Follow-up |
|
Spiegel 1981 1983 1989 |
Metastatic |
86 |
• Supportive–expressive group therapy with relaxation |
≥ 1 year |
• Improved mood, reduced maladaptive coping responses and phobias. • Prolonged survival. |
12 months |
12 months |
|
Classen 2001 |
Metastatic |
125 |
• Supportive–expressive group therapy with relaxation |
Indefinite |
• Reduced traumatic stress symptoms • Enhanced mood if final measurement during the year prior to death excluded |
12 months |
12 months |
|
Goodwin 2002 |
Metastatic |
235 |
• Supportive–expressive group therapy with relaxation |
Indefinite |
• Improved mood, reduced experience of pain |
12 months |
12 months |
|
Fukui 2000 |
Early |
50 |
• Cognitive–behavioral group with relaxation and guided imagery |
6 weeks |
• Improved mood, vigor, fighting spirit |
8 weeks |
6 months** |
|
Antoni 2001 |
Early |
100 |
• Structured cognitive–behavioral group |
10 weeks |
• No overall effects • Reduced prevalence of moderate depression, increased benefit finding/optimism |
_______ |
9 months |
|
Edelman 1999 |
Metastatic |
121 |
• Cognitive–behavioral group |
5 months |
• Improved mood, reduced depression, enhanced self-esteem |
5 months |
11 months |
|
** Marginal effect at 6 months. |
|||||||
|
III. Individual Interventions |
|||||||
|
Citation |
Phase |
n |
Intervention |
Duration of Intervention |
Effectiveness |
Duration of Benefit |
Duration of Follow-up |
|
Edmonds 1999 Cunningham 1999 |
Metastatic |
66 |
• Supportive plus cognitive–behavioral |
35 weeks |
• Increased anxious-preoccupied coping, reduced helplessness, coping “Little psychometric effects” |
12 months |
12 months |
|
Cimprich 1988 |
Early |
32 |
• Individualized intervention to restore attentional capacity |
? (short-term) |
• Enhanced attentional capacity |
90 days |
90 days |
|
Burton 1995 |
Early |
200 |
• Psychological interview • Psychological interview plus psychotherapy • Psychological interview plus chat |
1 day |
• Psychological interview led to lasting reduction in body image distress, overall distress, anxiety, depression, enhanced fighting spirit. • Psychotherapy beneficial among women with stressful life events. |
1 year |
1 year |
|
Maunsell 1996 |
Early |
259 |
• Telephone screening for distress |
12 months |
• No effects. |
_______ |
1 year |
|
Marchioro 1996 |
Early |
36 |
• Cognitive–behavioral counseling |
? (short-term) |
• Improved depression and quality of life. |
9 months |
9 months |
|
Maguire 1980 1983 |
Early |
172 |
• Nurse specialist counseling |
“Until woman had adapted well” |
• Increased recognition of need for psychiatric referral. • Psychiatric intervention reduced morbidity. |
12 to 18 months |
12 to 18 months |
|
Citation |
Phase |
n |
Intervention |
Duration of Intervention |
Effectiveness |
Duration of Benefit |
Duration of Follow-up |
|
McArdle 1996 |
Early |
272 |
• Nurse specialist support • Voluntary organization support • Both • Neither |
? |
• Nurse specialist led to improved somatic symptoms, social dysfunction and depression. |
12 months |
12 months |
|
Wengström 1999 2000 2001 |
Early |
134 |
• Nursing intervention based on Orem’s model for self-care |
5 weeks |
• Fewer distress reactions, stronger motivation to be emotionally involved. |
3 months |
3 months |
|
Sandgren 2000 |
Early |
62 |
• Telephone-based cognitive–behavioral therapy |
16 weeks |
• No consistent effects. • Borderline effects on stress, anxiety, confusion, physical role functioning and mental health varied over time. |
10 months |
10 months |
|
Ritz 2000 |
Early |
210 |
• Advanced practice nursing interventions |
? |
• Reduced uncertainty (especially in unmarried women). • Beneficial early effect on mood in those without a family history. |
3 to 6 months |
12 months |
|
Lev 2001 |
Early |
53 |
• Nurse counseling plus videotape plus self-care booklet |
5 months |
• No significance testing “Small to large effect sizes for HRQOL, psychiatric symptoms”. |
8 months |
8 months |
|
Allan 2002 |
Early |
164 |
• Problem-solving skills training (2 session in person, 4 by telephone) |
4 months |
• No overall effects. • Subgroup analysis suggested benefit in women with good problem-solving skills. |
8 months |
8 months |