Meeting Psychosocial Needs of Women with Breast Cancer (2004)
Chapter: 8 Research
8
Research
The National Cancer Policy Board, in an effort to understand how resources for research are applied to questions regarding psychosocial services for women with breast cancer, undertook a review of the status of research. Such a review provides only a snapshot as of 2003, but it does give an indication of the prominence and priority of psychosocial subjects as components within the field of breast cancer research, and a sense of the emphasis on different concerns and services within psychosocial breast cancer research. With these understandings, the Board was able to suggest ways in which a research program could be structured in the future to support better responses to psychosocial needs of women with breast cancer.
This chapter first describes publication trends in breast cancer-related research and then summarizes major sources of support for research within the following organizations:
Federally Sponsored Research
Department of Health and Human Services
National Institutes of Health (National Cancer Institute, National Institute of Nursing Research)
Department of Defense
Privately Sponsored Research
American Cancer Society
Foundations (e.g., Komen Foundation, Avon Foundation)
Although these organizations are not the only sponsors of breast cancer-related psychosocial research, they represent the major funding sources for such research. Excluded from this review is research supported by health plans, insurers, pharmaceutical companies, and other private organizations. Much of the research in these settings is proprietary. The chapter concludes with the Board’s identification of priority areas for research and recommendations to increase research opportunities.
STATUS OF BREAST CANCER-RELATED RESEARCH
Publications
Evaluating trends in research publications is one way to assess the level of activity within a discipline. A resource for tracking such studies in the National Library of Medicine (NLM) Medline bibliographic database, which stores information about individual citations including index terms used to characterize each article (articles are indexed according to a dictionary of medical subject headings called MESH terms).
The volume of breast cancer-related psychology research articles appears to have almost tripled from 1990 to 2000 (from 150 to 431 citations), but throughout the period such articles represent a small fraction of breast cancer-related research, less than 7 percent according to Medline searches (Figures 8-1 and 8-2). These trends reflect publications in English, but not limited to articles written by United States investigators. Figures 8-1 and 8-2 therefore reflect trends in the general medical literature, not necessarily trends in the United States. These trends must be interpreted with caution because they may reflect changes in the way MESH headings are applied to index the literature rather than real increases in breast cancer-related psychological research.
Research Support
A more direct way to assess the status of United States-based breast cancer-related psychosocial research is to describe topics of investigation and levels of research spending. There is no one comprehensive source of information on research support; as part of its review, the Board relied on the following sources:
-
Listings of research projects provided by some organizations (e.g., National Cancer Institute);
-
The federal listing of research projects (CRISP);
-
Review of agency web sites (e.g., Department of Defense); and
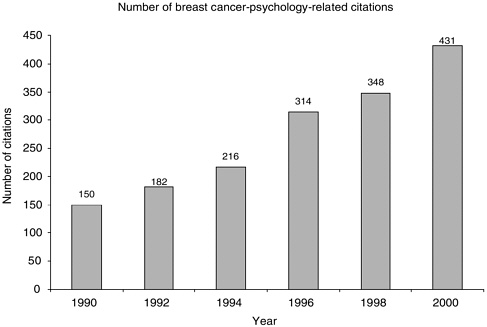
FIGURE 8-1 PubMed citations for breast cancer psychological research, 1990–2000. Citations were identified in the National Library of Medicines’s PubMed database using the MESH term “breast neoplasms,” and the MESH subheading “psychology.” Only articles published in English are counted.
-
Informal contacts with agency representatives known to be involved in research (e.g., foundations).
Despite the best efforts of the Board, the description of the nation’s breast cancer-related psychosocial research portfolio that follows may under- or overestimate the actual level of research. Some research activities may have been missed because of limitations of research tracking systems. The review is limited to currently active research projects for most organizations.
Federally Sponsored Research
National Cancer Institute, Office of Cancer Survivorship
The main locus of cancer-related psychosocial research support within the Department of Health and Human Services (DHHS) is the National Cancer Institute (NCI). Table 8-1 describes the NCI’s overall budget request for 2004, which includes $46 million for cancer survivorship research as detailed in Table 8-2 (0.7 percent of the total FY 2004 budget request). Cancer survi-

FIGURE 8-2 PubMed citations for psychology related breast cancer research as a percentage of all breast cancer-related research, 1990–2000. Percentages were calculated as the number of psychology-related breast cancer citations (as described in Figure 8-1) divided by the number of citations categorized under the MESH term “breast neoplasms.” Only articles published in English are counted.
vorship research has been designated by NCI as an “Extraordinary Opportunity for Investment.” A research initiative focused on long-term survivors was announced in 2003, providing $20 million to support awards for studies of individuals who are five years or more beyond cancer diagnosis (http://grants1.nih.gov/grants/guide/rfa-files/RFA-CA-04-003.html, accessed April 14, 2003).
NCI’s work on survivorship is administered through its Office of Cancer Survivorship (OCS), which was established in 1996 to promote research and to provide information to cancer patients, their families, health-care providers, advocates, and the research community (http://dccps.nci.nih.gov/ocs/, accessed April 18, 2003). OCS grants relating to breast cancer are shown in Table 8-3. About half of these are on psychosocial or quality of life subjects.
National Cancer Institute, Office of Behavioral Research
Psychosocial research is also supported through the NCI’s Office of Behavioral Research (BRP). Research supported in this office ranges from basic behavioral research to research on the development, testing and dis-
TABLE 8-1 NCI’s Budget Request for Fiscal Year 2004 (in thousands)
|
Fiscal Year 2003 President’s Budget |
$ 4,637,869 |
|
Increase to core budget |
294,014 |
|
Capacity building increase |
|
|
Enhancing investigator-initiated research |
69,887 |
|
Expanding the capacity of centers, networks, and consortia |
79,530 |
|
National clinical trials program in treatment and prevention |
340,100 |
|
Developing bioinformatics for cancer research |
88,000 |
|
Subtotal capacity building |
577,517 |
|
Discovery and application increase |
|
|
Genes and the environment |
51,800 |
|
Signatures of the cancer cell and its microenvironment |
41,200 |
|
Molecular targets of prevention and treatment |
54,800 |
|
Cancer imaging and molecular sensing |
78,700 |
|
Cancer communications |
39,750 |
|
Subtotal discovery and application |
266,250 |
|
Public health emphasis increase |
|
|
Improving the quality of cancer care |
27,000 |
|
Reducing cancer-related health disparities |
61,350 |
|
Cancer survivorship |
46,000 |
|
Research on tobacco and tobacco-related cancers |
76,000 |
|
Subtotal public-health emphasis |
210,350 |
|
Total FY 2004 budget request |
5,986,000 |
|
SOURCE: The Nation’s Investment in Cancer Research: A Plan and Budget Proposal for Fiscal Year 2004, Prepared by the Director of the National Cancer Institute. |
|
semination of disease prevention and health promotion interventions in areas such as tobacco use, screening, dietary behavior and sun protection. The BRP programs support five areas (http://www.dccps.nci.nih.gov/brp/index.html):
-
Applied Cancer Screening Research. Facilitates and supports effectiveness trials and related social and behavioral research to promote the use of effective cancer screening tests, as well as strategies for informed decision making regarding all cancer screening technologies, in both community and clinical practice.
-
Basic Biobehavioral Research. To serve as a national model for promoting, sponsoring, and supporting basic biobehavioral research and training.
-
Health Communication and Informatics Research. To advance communication and information science across the cancer continuum—prevention, detection, treatment, control, survivorship, and end of life. Communication and information science systematically examines the fundamental processes and effects of human and mediated communication.
-
Health Promotion Research. Coordinates research on non-tobacco behavioral prevention of cancer in the areas of diet, physical activity, energy balance, virus exposure, and sun exposure.
TABLE 8-2 Cancer Survivorship Component of NCI’s Budget Request for Fiscal Year 2004 (in millions)
|
Research—biological, physical, psychological, and social response to disease, treatment and recovery |
$9.50 |
|
Physiologic and psychosocial effects on post-treatment survivors |
3.00 |
|
Late effects case studies |
5.00 |
|
Socio-cultural, behavioral, emotional, and spiritual factors |
1.50 |
|
Intervention research—to reduce cancer-related late morbidity and mortality |
12.00 |
|
Research of cost-effective medical, educational, and psychosocial interventions |
9.00 |
|
Development of interventions for families, minorities, and medically underserved |
3.00 |
|
Development of assessment tools for quality of life and post-treatment care |
5.50 |
|
New instruments for quality of life assessment (e.g., toxicity criteria for late effects) |
2.00 |
|
Screening tools for high risk physical, psychosocial, or behavioral outcomes |
2.00 |
|
Use of applied/theoretical statistics to establish criteria for clinically significant changes |
0.50 |
|
Collaboration with other NIH institutes to develop measures to evaluate comorbidities |
1.00 |
|
Enhance NCI’s capacity to track outcomes for cancer survivors |
5.50 |
|
Expansion of data collection on health-related outcomes for survivors in SEER registries |
1.00 |
|
Development of infrastructure for clinical trials groups to follow patients long-term |
2.00 |
|
Establishment of separate registry for pediatric cancer survivors |
2.50 |
|
Development and dissemination of new interventions and best practice guidelines |
3.50 |
|
Best practice guidelines for follow-up care and surveillance for survivors |
1.25 |
|
Support studies to test adoption and impact of best practices in post-treatment care |
1.50 |
|
Develop/disseminate curricula and standards for delivery of effective psychosocial care |
0.75 |
|
Expansion of scientific base for understanding the biologic mechanisms in adverse late effects |
9.00 |
|
Funding of pre-clinical studies examining incidence/mechanism of late effects treatment |
3.00 |
|
Support research that seeks to investigate the neuropsychologic impact of cancer therapy |
6.00 |
|
Management and support |
1.00 |
|
Total |
46.00 |
|
SOURCE: The Nation’s Investment in Cancer Research: A Plan and Budget Proposal for Fiscal Year 2004, Prepared by the Director of the National Cancer Institute. |
|
-
Tobacco Control Research. To reduce cancer incidence and mortality caused by tobacco use through a comprehensive research program. To provide recommendations to the scientific and public health communities by synthesizing and disseminating research findings.
A selection of some of the grants from this office that have focused on psychosocial research is displayed in Table 8-4.
TABLE 8-3 Selected Current Breast Cancer-Related Survivorship Research, Office of Cancer Survivorship, NCI
|
|
|
SOURCE: http://dccps.nci.nih.gov/ocs/portfolio.asp, accessed April 18, 2003. |
Department of Defense
Beginning in FY 1992, the U.S. Congress directed the Department of Defense (DoD) to manage several appropriations for an extramural grant program directed toward specific research initiatives. The United States Army Medical Research and Materiel Command (USAMRMC) established the office of the Congressionally Directed Medical Research Programs (CDMRP) to administer these funds. Between FY 1992 and 2003, $1.37 billion has been appropriated by Congress to DoD for research on breast cancer. In addition, $7.0 million was generated in sales of the U.S. Postal Service’s first-class stamp (Public Law 105-41, Stamp Out Breast Cancer Act [H.R. 1585]). The CDMRP strives to identify gaps in funding and provide award opportunities that will enhance program research objectives without duplicating existing funding opportunities.
TABLE 8-4 Selected Grants from NCI’s Office of Behavioral Research, FY 2001 and 2002a
|
Project Title |
|
Fatigue, Sleep and Circadian Rhythms in Breast Cancer Psychological Intervention for Women with Breast Cancer The End-of-Life Family Workshop Pain Assessment via Role-Play Internet Simulation Health Promotion for Women at Risk for Breast Cancer Breast Cancer Risk-Tailored Messages for More Women Self-Advocacy and Empowerment for People with Cancer We Can Cope—Family Support When a Parent Has Cancer Vicarious Dissonance, Attitude Change & Identity Web-Based Support for Informal Caregivers in Cancer Culturally Targeted Health Information Network Spiritually-Based Breast Cancer Communication Cognitive Behavioral Aspects of Cancer Related Fatigue Breast Cancer Patients Relatives—Response Over Time Interactive CD-ROM for Coping with Breast Cancer Quality of Life, Ethnicity, and Breast Cancer Survivors Hormones, Quality of Life & Breast Cancer Support Groups |
|
aThe list contains grants carried over from prior fiscal years (FY 2001 and prior) and new grants awarded in FY 2002. SOURCE: NCI website, accessed on 2/27/03: http://dccps.nci.nih.gov/brp/research.asp. |
The Breast Cancer Research Program (BCRP) has sponsored over 2,800 awards for peer-reviewed breast cancer research at the community, state, and national level (Table 8-4). The BCRP divides the awards into three categories:
-
research (basic and clinical),
-
infrastructure, and
-
training and recruitment.
In addition, an Innovator Award was initiated in FY01 that grants $5 million to individuals engaged in “visionary research.” Within the BCRP, psychosocial research awards fall within the category of “Biobehavioral Sciences.” A total of 35 of the 105 biobehavioral awards of the BCRP pertain to psychosocial issues (Table 8-5).
TABLE 8-5 BCRP Study Awards with Psychosocial Component
|
Name of Research Study |
Institution |
$ Amount |
Fiscal Year |
|
Evaluation of a Peer-Staffed Hotline for Families Who Received Genetic Testing for Risk of Breast Cancer |
Univ. of Pennsylvania |
$79,250.00 |
2000 |
|
Assisting Survivors in Meeting Challenges at End of Treatment: A Problem Solving Approach |
Univ. of Pennsylvania |
$79,250.00 |
2000 |
|
Hatha Yoga and Breast Cancer: Integrating a Mind/Body Intervention During Adjuvant Chemotherapy |
Columbia Univ. |
$81,725.00 |
2000 |
|
A Longitudinal Study of Emotional Distress and the Use of Complementary Alternative Medicine in Women with Breast Cancer |
Univ. of Hawaii |
$66,000.00 |
2000 |
|
Breast Cancer Protective Behaviors Among Low-income, Ethnically Diverse Women: The Role of Biopsychosocial Factors |
Florida State Univ. |
$22,000.00 |
2000 |
|
Spirituality-Based Intervention for African American Women with Breast Cancer |
Wayne State Univ. |
$334,599.00 |
1999 |
|
Interdisciplinary Research Training in Breast Cancer |
Yale Univ. |
$749,432.00 |
1999 |
|
Medical Decision-Making About Breast Cancer Among African Americans: Evaluating the Roles of Beliefs, Knowledge, Medical Care Access, and Social Support |
Univ. of Texas at Houston |
$73,513.00 |
1999 |
|
Internet Support and Information for Women with Breast Cancer |
Univ. of Alabama at Birmingham |
$61,519.00 |
1999 |
|
Stress and Immunity Breast Cancer Project |
Ohio State Univ. |
$808,568.00 |
1998 |
|
Identifying Quality of Life and Psychosocial Risk Factors and Their Sociocultural Mediators in African American, Filipino, Latino, and White Breast Cancer Survivors |
UCLA |
$761,421.00 |
1998 |
|
Postdoctoral Training Program in Biobehavioral Breast Cancer Research |
Mount-Sinai (NY) |
$782,413.00 |
1998 |
|
Psychological Distress, Cognitive Bias, and Breast Cancer Surveillance Behavior in Women Tested for BRCA1/2 Mutation |
Mount Sinai (NY) |
$125,737.00 |
1998 |
|
The Effect of Emotional Disclosure Interventions on Psychological and Physical Well-Being of Breast Cancer Patients |
Virginia Commonwealth University |
$44,622.00 |
1998 |
|
Name of Research Study |
Institution |
$ Amount |
Fiscal Year |
|
The Development and Evaluation of an Innovative Internet-Based Breast Cancer Psychosocial Intervention |
Stanford Univ. |
$327,015.00 |
1998 |
|
Inherited Susceptibility to Breast Cancer in Healthy Women: Mutations in Breast Cancer Genes, Immune Surveillance and Psychological Distress |
Sloan-Kettering |
$481,210.00 |
1997 |
|
Psycho-Endocrine-Immune Profile: Implications for Quality of Life in Breast Cancer Patients |
Loyola University– Chicago |
$325,626.00 |
1997 |
|
Development of an Integrated Program of Health related Quality of Life Research for the National Surgical Adjuvant Breast and Bowel Project (NSABP). |
Univ. of Pittsburgh |
$227,876.00 |
1996 |
|
Social Support and Endocrine Function: A Randomized Trial with Breast Cancer Patients |
Ohio State Univ. |
$82,932.00 |
1996 |
|
Preventive Psychosocial Intervention for Young Women with Breast Cancer |
Univ. of Pittsburgh |
$292,243.00 |
1996 |
|
Stress and Coping in Genetic Testing for Cancer Risk |
Univ. of Michigan |
$837,296.00 |
1995 |
|
Effects of Psychosocial Intervention in Women Following Breast Cancer Diagnosis |
Univ. of Rochester |
$149,991.00 |
1995 |
|
Delays and Refusals in Treatment for Breast Cancer among Native American and Hispanic Women with Breast Cancer |
Univ. of New Mexico |
$72,043.00 |
1995 |
|
Psychobehavioral Impact of Genetic Counseling and Breast Cancer Gene Testing in Healthy Women of African Descent |
Sloan-Kettering |
$579,581.00 |
1995 |
|
Psychological Intervention for Women with Breast Cancer |
Ohio State Univ. |
$86,896.00 |
1993 & 94 |
|
Enhancing Positive Reactions to Breast Cancer Risk Appraisal |
Hutchinson Cancer Center |
$597,673.00 |
1993 & 94 |
|
The Effects of a Comprehensive Coping Strategy on Clinical Outcomes in Breast Cancer Bone Marrow Transplant Patients and Primary Caregiver |
Johns Hopkins Univ. |
$783,572.00 |
1993 & 94 |
|
Name of Research Study |
Institution |
$ Amount |
Fiscal Year |
|
Effects of Meditation-Based Stress Reduction in Younger Women with Breast Cancer |
Univ. of Massachusetts |
$799,843.00 |
1993 & 94 |
|
Psycho Educational Group Intervention for Women at Increased Risk for Breast Cancer |
Strang Cancer Center |
$799,837.00 |
1993 & 94 |
|
The Effects of Brief Psychotherapy on Coping with Breast Cancer |
North Dakota State Univ. |
$143,510.00 |
1993 & 94 |
|
Incidence and Psychophysiology of PostTraumatic Stress Disorder in Breast Cancer Victims and Witnesses |
Harvard Univ. |
$724,375.00 |
1993 & 94 |
|
Knowledge and Beliefs of Breast Cancer Among Elderly Puerto Rican Women Rico |
Univ. of Puerto |
$771,159.00 |
1993 & 94 |
|
An Evaluation of A Peer Support Program to Improve Quality of Life with Breast Cancer |
Kaiser Foundation |
$595,732.00 |
1993 & 94 |
|
Emotional Processing and Expression in Breast Cancer Patients: Effects on Health and Psychological Adjustment |
Univ. of Kansas |
$145,839.00 |
1993 & 94 |
|
A Community Study of Psychological Distress and Immune Function in Women with Family Histories of Breast Cancer |
Sloan-Kettering |
$200,000.00 |
1993 & 94 |
|
SOURCE: Department of Defense Breast Cancer Research Program: Search Awards Database, http:Hcdmrp.army.mil/cgi-bin/search/search-bcrp.pi, accessed November 21, 2002. |
|||
Privately Funded Research
Private philanthropic organizations have been major sponsors of breast cancer research. This section of the report reviews the research activity of the American Cancer Society, the Avon Foundation, the Susan G. Koman Foundation, and the Bristol Myers Squibb Foundation.
American Cancer Society
The American Cancer Society is the largest non-governmental source of cancer research funding in the United States and supports psychosocial and behavioral research. In FY 2001-2002, approximately 20 percent of the total research program was devoted to these areas (see Table 8-6).
The Society’s intramural research program includes a Behavioral Research Center, which is conducting two large population-based surveys of
TABLE 8-6 ACS Extramural and Intramural Funding in Selected Priority Areas:a FY 2001-2002 (in thousands)
|
Area of Research |
$ Awarded |
|
Total |
102,415 |
|
Prevention |
13,648 |
|
Nutrition |
4,013 |
|
Tobacco control |
3,141 |
|
Other prevention |
6,494 |
|
Detection |
6,051 |
|
Treatment |
22,849 |
|
Psychosocial and behavioral |
20,471 |
|
Poor and underserved |
10,780 |
|
Childhood cancer |
4,257 |
|
Environmental carcinogenesis |
909 |
|
Epidemiology |
6,112 |
|
Cause/etiology |
36,637 |
|
Major organ sites |
|
|
Breast |
27,312 |
|
Leukemia |
14,000 |
|
Colon/rectum |
14,990 |
|
Lung |
12,711 |
|
Lymphoma |
5,534 |
|
Prostate |
8,071 |
|
Ovary |
5,108 |
|
Melanoma |
4,679 |
|
Pancreas |
7,845 |
|
Brain/nervous system |
2,165 |
|
aNot mutually exclusive categories: e.g., a grant that is both prevention and detection is counted twice, as is a grant that studies both breast and prostate cancers. A grant emphasizing nutrition in breast and prostate cancer is counted in full in all three places. Dollar amounts are rounded off to the nearest $1,000. SOURCE: American Cancer Society, http://www.cancer.org/docroot/RES/content/RES_7_3_Funding_By_Research_Area.asp, accessed May 1, 2003. |
|
cancer survivors. The first is the Study of Cancer Survivors–I (SCS-I), a longitudinal study of the needs and quality of life of adult cancer survivors. Participating survivors complete questionnaires at 1, 2, 5, and 10 years after diagnosis, allowing a comparison of changes over time and an assessment of the long-term impact of cancer on survivors. The participants in this study are selected with the cooperation of state cancer registries from the lists that they maintain of people diagnosed with cancer, thus allowing a more inclusive sample to be selected from this population than is usually employed in studies done by academic cancer centers. An additional strength
of the research design of this study is its inclusion of more types of cancer than are usually included in a single study, thus allowing comparisons of the psychosocial effects of multiple cancer types. The study’s sample includes adults diagnosed with 1 of 10 common cancers (prostate, female breast, lung, colorectal, bladder, non-Hodgkin’s lymphoma, skin melanoma, kidney, ovarian, and uterine). SCS-I also has the advantage of being designed to include a sufficient number of minority and younger survivors to allow assessments of the unique needs of these understudied groups.
SCS-I also includes a family caregiver research component to explore the impact of the family’s involvement in cancer care on the quality of life of the cancer survivor and the family caregiver. This research will identify the prevalence of the family’s involvement in cancer care, identify unmet needs of caregivers at 2 and 5 years after diagnosis, and examine the impact of the caregiving on the quality of life and health behaviors of the caregiver.
The second population-based survey of cancer survivors is the Study of Cancer Survivors –II (SCS-II), a national cross-sectional study of 2-, 5-, and 10-year cancer survivors that focuses on quality of life and psychosocial functioning. Over 30,000 survivors of breast, prostate, colorectal, urinary bladder, skin melanoma, and uterine cancer from across the nation are participating in this study. This study will evaluate the psychological needs, adjustment, and quality of life of cancer survivors and provide information now on longer-term cancer survivors. The results will provide a basis for advocacy and planning by the American Cancer Society as well as by other health organizations and agencies.
Other research that the ACS Behavioral Research Center is conducting includes a study of the use of complementary therapies by breast and prostate cancer survivors, as well as a corresponding survey of physicians who treat cancer patients. The physicians’ survey explores physician-patient communications about complementary therapies. The Behavioral Research Center has also conducted surveys of primary care providers to determine their knowledge, use, and evaluation of cancer screening guidelines.
Avon Foundation
Avon Products, Inc., a manufacturer of cosmetics, founded the Avon Breast Cancer Crusade in 1993 to support breast cancer research and to improve access to care, especially among medically underserved women. With $250 million raised since its inception, the program supports programs for breast cancer in the United States and in 50 countries around the world. Originally designed to provide education, screening, and breast exam services to the underserved community, Avon expanded the crusade in 2000 by funding:
-
Community outreach and referral programs.
-
Support services for breast cancer patients and survivors, including financial assistance for biopsies for uninsured women, counseling, transportation, and childcare
-
Educational seminars that teach the “science” of breast cancer and methods of effective advocacy.
-
Medical research on breast cancer.
Selected programs that support psychosocial care are shown in Table 8-7.
Avon also collaborates with the National Cancer Institute “Progress for Patients” award program. The purpose of the program is to accelerate and expand translational research in breast cancer. Funding goes directly to United States scientists who compete for the awards. Avon Foundation dollars support direct costs of early phase breast cancer clinical trials and other studies in prevention, diagnosis, and treatment, including studies focusing on the needs of minority and other medically underserved patients. The NCI supports other costs of managing the program and the peer review process.
The Susan G. Komen Breast Cancer Foundation
The Susan G. Komen Breast Cancer Foundation is one of the nation’s largest private funders of breast cancer research, awarding more than 700 grants totaling $90 million since its inception in 1982. The Komen Foundation’s Research Program is funded by 25 percent of all funds raised by Komen Affiliates and Komen Race for the Cure events across the United States, as well as by certain private and corporate donations.
In addition to research programs, Komen Affiliates throughout the United States fund community-based breast health education and breast cancer screening and treatment projects (STEP) for the medically underserved. In order to ensure that they are funding programs that address the specific unmet breast health needs of their communities, Komen Affiliates work with local medical experts and community leaders to conduct comprehensive community needs assessments. These profiles are then used to establish local grant application and review processes. From 1998 to 2002 $97 million was awarded through the STEP program. Selected psychosocial programs supported through the program are shown in Table 8-8.
A Population Specific Program of the Komen Foundation funds innovative projects studying the prevention and control of breast cancer within certain at risk populations (Table 8-9). The focus of the program is to support research designed to assess and identify unique needs, trends, barriers and solutions to breast health care among populations such as African American, Asian American, Native Hawaiian and Pacific Islanders, Hispanic/
TABLE 8-7 Selected Programs Supported by the Avon Breast Cancer Crusade
|
Program |
Amount Awarded Through October 2002 (in millions) |
|
Avon Foundation Comprehensive Breast Evaluation Center, Massachusetts General Hospital • Funding brings the hospital’s leading edge breast cancer screening, diagnostic, and research capabilities to one location; it also supports a high risk breast evaluation center, new research projects in breast cancer genetics and biology, expands ongoing research and enhances access to clinical care and breast cancer treatment for women in community-based health care centers. |
$12.2 |
|
Cancer Care, Inc. (NY) • New York City-based Cancer Care has established the national "AVONCares" Program for Medically Underserved Women, which provides financial assistance for breast cancer clinical diagnostic services; transportation and an escort to and from treatment and diagnostic workups; and elder- or childcare while undergoing breast cancer treatment or diagnostics. Women assisted by the "AVONCares" program are able to receive Cancer Care's other services, including professional counseling, education and information, breast prostheses and wigs. |
$11.2 |
|
National Breast Cancer Coalition • Support to develop leadership skills among cancer advocates and to develop A Guidebook to Quality Breast Cancer Care: a consumer guide that helps women define quality breast care and secure access to evidence-based and patient-centered treatment and care. |
4.0 |
|
Y-Me National Breast Cancer Organization (US) • Funds support expansion of the Y-Me support of Latino, Chinese and Vietnamese women. The programs educate these underserved women and link them directly to screening; assist women who have abnormal screening results in obtaining proper follow-up care; provide translation services; expand the Y-Me husband/partner hotline; and expand the Y-Me teen program, which trains high school seniors in early detection and encourages them to educate their families and neighbors. |
2.5 |
|
The Cleveland Clinic (OH) • Funds support community outreach and care for the underserved and improved clinical facilities in the Women's Health Pavilion. |
2.1 |
|
Program |
Amount Awarded Through October 2002 (in millions) |
|
Food & Friends (DC) • Organization runs a delivery service of meals and groceries to women with breast cancer to ensure that women suffering from breast cancer, along with their families, have access to better nutrition, reduced stress and improved outlook. The program also provides nutritional education and counseling. The Avon funding will cover delivery of more than 1,500 meals a week to women referred by numerous community partners and construction of the Avon Foundation Kitchen at the organizations' new facility opening October 2003. |
1.0 |
|
“Rise Sister Rise‘” of Breast Cancer Resource Committee (DC) • National implementation of a model support group program for African-American women recovering from breast cancer. |
.7 |
|
Inova Health System Foundation/Fairfax Hospital (VA) • Funds support maximizing relationship between the Women's Center and Fairfax Hospital Cancer Center, focusing on Asian and Hispanic women who are medically underserved. Women are taught to understand early detection, risk reduction, how to obtain access to clinical screening, diagnostic and treatment services, including clinical trials. |
.6 |
|
Boston Medical Center (MA) • Funds support a comprehensive breast cancer screening and diagnostic program targeted to women challenged by language, cultural and economic barriers. The Women's Health Group at BMC launched the Avon Foundation Breast Health Initiative linking clinicians, outreach/inreach workers, advocates, and researchers in order to better serve women in poor, urban communities, thereby improving the rate of undetected breast cancer and overall health outcomes. |
.5 |
|
Stroger Hospital of Cook County/Hektoen Institute for Medical Research (IL) • Funds bring state-of-the-art quality breast oncology care to minority-underserved populations in their own communities through participation in NCI-approved clinical trials that specifically recruit for minority participation; extend and promote these research opportunities with emphasis on the particular needs of the community served, promoting outreach and education; focus on prevention and control as methods for reducing breast cancer incidence, morbidity and mortality, with special emphasis on involvement and education of patient advocacy groups, women's support groups, and primary care physicians. |
.5 |
|
Program |
Amount Awarded Through October 2002 (in millions) |
|
Karmanos Cancer Institute (MI) • Funds support three related projects: the Community Resource Liaison Project, designed to make clinical trials more readily available to underserved women; the Mobile Detection Center, which will travel around Michigan throughout the year, increasing access for mammography screening; and the Image Checker, which converts film screen to digital images and identifies areas of suspicion. |
.5 |
|
Univ. of Miami/Sylvester Cancer Center (FL) • Funds are enhancing the infrastructure of the breast clinic at Jackson Memorial Hospital, a public hospital that serves the poor in Miami, in particular, women born in Latin America and the Caribbean and African Americans. |
.5 |
|
Moores Univ. of Calif. At San Diego Cancer Center (CA) • Funds enable the Cancer Center to expand its efforts to build on existing programs in community outreach, clinical cancer genetics, diet intervention and state of the art breast care with underserved populations. |
.5 |
|
Univ. of Texas Southwestern Medical Center/Parkland Hospital (TX) • Funding supports the Avon Foundation Breast Cancer Program, focusing on facilitating easier access to care and clinical trials for the medically underserved, and identifying and monitoring women in populations at greater risk for breast cancer. |
.5 |
|
SOURCE: Accessed from Avon website at www.avoncompany.com/women/avoncrusade/services/beneficiaries_factsheet.shtml), accessed Feruary 20, 2003. |
|
Latina, Native American, Lesbian, Low Literacy, Breast Cancer Survivors, Women with Disabilities, and other defined communities. Areas of interest include cancer prevention and control, behavioral science research, epidemiology, and health service delivery programs. Komen gives preference to applicants who demonstrate collaboration with a community-based organization. This program offers funding of up to $250,000 (combined direct and indirect costs) over a 2- or 3-year period.
Bristol Meyers Squibb Foundation
The Bristol Meyers Squibb Foundation has sponsored a demonstration project (currently in its second phase) to bring more psychosocial services
TABLE 8-8 Selected Programs Supported Through the Susan G. Komen Breast Cancer Foundation, 2000-2002 Psychosocial STEP Grants and Funding
|
Grant Program |
Institution |
Komen Affiliate |
|
Educational Support Program for Women with Breast Cancer |
The Wellness Community |
South Florida |
|
Outreach Services for Women with Breast Cancer |
Center for Hope, Inc. |
Greater New York City |
|
Cancer Patient Matching and Support |
Cancer Hope Network |
North New Jersey |
|
Psychosocial Support for Latino Women with Breast Cancer |
The Wellness Community |
Los Angeles County |
|
Art and Educational Therapy Pilot Program |
Presbyterian Healthcare Services |
Central New Mexico |
|
Complementary Alternative |
Charlotte Maxwell |
San Francisco Bay Area |
|
Medicine, Education & Advocacy for Breast Cancer |
Complementary Clinic |
|
|
LatinaSHARE: Medical/Community Outreach and Mentoring Project |
SHARE: Self-Help for Women with Breast or Ovarian Cancer, Inc. |
Greater New York’City |
|
Psychosocial Support Services for Breast Cancer Patients |
The Wellness Community |
San Diego |
|
Counseling for Breast Cancer Patients |
UNC Lineberger Comprehensive Cancer Center |
NC Research Triangle Area |
|
Breast Cancer Education and Support Project |
Cancer Care, Inc. |
New Jersey Race for the Cure® |
|
Year 2001 Casting for Recovery Retreats |
Casting for Recovery |
Vermont |
|
A Healing Journey Pre-Operative |
St. Mary’s Foundation Robert Wood Johnson |
Greater Evansville, IL New Jersey Race for the |
|
Education/Complementary Therapy Consultation |
University Hospital Foundation |
Cure® |
|
Outreach to the Underserved Check It Out |
Gilda’s Club Nashville St. Louis Chapter of Hadassah |
Greater Nashville St. Louis |
|
Breast Cancer in Young Women: Establishing an Outreach and Mentoring Program |
Washington University School of Medicine |
St. Louis |
|
Grant Program |
Institution |
Komen Affiliate |
|
Group Therapy for Newly Diagnosed African American Breast Cancer Patients |
Wake Forest University Baptist Medical Center |
North Carolina Triad |
|
Psychosocial Support for Latino Women with Breast Cancer |
The Wellness Community |
Los Angeles County |
|
Support Services for Breast Cancer Patients with a Focus on Underserved Populations |
The Wellness Community |
San Diego |
|
Casting for Recovery 2002 |
Casting for Recovery |
Vermont |
|
Cancer Patient Matching and Support |
Cancer Hope Network |
North New Jersey |
|
LatinaSHARE: Medical and Community Outreach and Mentoring Project |
SHARE: Self-Help for Women with Breast or Ovarian Cancer, Inc. |
Greater New York City |
|
WomensCare Center Breast Health Program |
St. Rose Dominican Hospital and St. Rose Dominican Health |
Las Vegas |
|
Breast Health Resource Guide |
Orange County Breast Cancer Coalition |
Orange County |
|
Counseling for Breast Cancer Patients |
UNC Lineberger Comprehensive Cancer Center |
NC Triangle Area |
|
Support for Life: Women Focused on Recovery |
The Wellness Community |
Phoenix |
|
Complementary Alternative Medicine, Psychosocial Support, Complementary Clinic Advocacy, and Education for Low Income Women with Breast Cancer |
The Charlotte Maxwell |
San Francisco Bay Area |
|
WINGS |
WINGS |
San Antonio |
|
Breast Cancer Registry, Psychosocial Screening, and Improvement of Compliance and Reduction of Distress |
Barbara Ann Karmanos Cancer Institute |
Detroit Race for the Cure® |
|
Breast Health Education for Nurses Breast Cancer Support and Education Project for Underserved Women |
Intermountain Health Care Cancer Care |
Salt Lake City Connecticut |
|
Education and Psychosocial Support for Women with Breast Cancer |
Cancer Wellness Organizations of Metropolitan Chicago Area |
Chicago |
|
SOURCE: http://www.komen.org/grants/step/stepresults.asp, accessed February 20, 2003. |
||
TABLE 8-9 The Susan G. Komen Breast Cancer Foundation 2001 Population Specific Grants
|
Grant |
Institution |
Amount (in US$) |
|
Health Care Experiences of Lesbians with Breast Cancer |
Boston University |
$120,638 |
|
Variation in Stage at Diagnosis in Breast Cancer |
Public Health Institute |
$128,867 |
|
Across California: Effects of Race/Ethnicity and Rural/Urban Residence |
|
|
|
Influence of Behavioral Factors on Breast Cancer Risk and Survival |
Howard University |
$215,168 |
|
African American Lesbian Breast Cancer Screening Study |
Mautner Project for Lesbians with Cancer |
$237,847 |
|
Korean American Breast Health Project in Maryland |
The Johns Hopkins University |
$249,442 |
|
Breast Cancer Control: Needs and Practices of African American Women and Their Providers |
University of Southern Mississippi |
$248,483 |
|
Genetic Epidemiology of Breast Cancer in African Americans |
Wayne State University |
$249,493 |
|
Impact of Culture on Breast Cancer Screening in Chinese American Women |
Georgetown University |
$249,998 |
|
Project Hoffnung: Delivering Hope with Culturally Appropriate Breast Health to Amish and Mennonite Communities |
University of Utah College of Nursing |
$249,969 |
|
“Comadre A Comadre” A One-on-One Peer Support Project for Hispanic Women with Breast Cancer |
University of New Mexico |
$250,000 |
|
Not Yet Well: the Self Management of Post-Treatment Symptoms by Breast Cancer Survivors |
University of California, Los Angeles |
$248,183 |
|
Grant |
Institution |
Amount (in US$) |
|
The Helping Path, Four Directions: A California Indian Breast Cancer Education |
University of California, Los Angeles |
$247,065 |
|
Lay Health Advisors to Promote Breast Cancer Screening Among Asian Americans |
University of Michigan |
$250,000 |
|
|
Total |
$2,945,153 |
|
SOURCE: Accessed from website: http:Hwww.komen.org/grants/awards/O I awards. asp?id=1, accessed February 20, 2003. |
||
to patients and their families at a local level. A second goal is to test the feasibility of training master’s level counseling psychologists in psychosocial oncology in order to increase the cadres of professionals available to patients in smaller communities.
To date, 150 psychologists in Florida have been given face to face and online training in psychosocial counseling in oncology. A current plan is to explore the development of this group further in an effort between the American Psychosocial Oncology Society (APOS) and the Bristol Meyers Squibb Foundation in which APOS will provide a core online curriculum and an examination to those who wish to add qualifications in psychosocial oncology. Counselors in Employment Assistance Programs and family service organizations, already trained in counseling should be rather easily trained in psychosocial issues in oncology. If so, the demonstration will have been able to increase the number of psychosocial oncology counselors with a wider geographic distribution who can be reached through the APOS Referral Directory and toll-free number, along with the traditional psychosocial oncology professionals (www.apos-society.org; 1-866-APOS-4-HELP).
SUGGESTIONS FOR FUTURE RESEARCH PRIORITIES
Relative to other areas of research in breast cancer, psycho-oncology is still in its infancy. Just over 20 years have elapsed since the first randomized psycho-oncology trial in breast cancer was reported by Maguire in 1980 (Maguire et al., 1983), and for this report Goodwin was able to find and review a total of 31 randomized trials in women with breast cancer in the literature (see Chapter 5). These trials cover a broad spectrum of interven-
tions (relaxation/hypnosis with or without imagery, group interventions involving structured or unstructured groups, supportive–expressive therapy, cognitive–behavioral therapy, mind–body–spirit interventions, psycho-educational interventions and/or peer discussion, as well as individual interventions involving telephone counseling, specialized nursing interventions, cognitive–behavioral therapy and problem-solving skills training). The reported trials have enrolled from 24 to 312 women, and the interventions evaluated have ranged from 75 minutes to lifelong. Some general conclusions can be drawn regarding the effectiveness of these psychosocial interventions in breast cancer. For example, there is fairly consistent evidence that relaxation/hypnosis/imagery interventions are beneficial in a variety of acute care settings, particularly in the short-term. Furthermore, there is growing evidence of the efficacy of a variety of group and individual interventions, using different strategies for different periods of time at different points along the breast cancer trajectory.
Despite this, many unresolved questions remain which should be the focus of future research activities. Based on discussions at its workshop, the analysis of Goodwin in her commissioned paper, and its own deliberations reviewing the trials presented and analyzed in Chapter 5, the Board was able to formulate some suggestions for areas of needed research and priorities. Along with some brief comments on the relevance of psychosocial research in other than breast cancer and on indexing, coordination, and collaboration issues, these suggestions are discussed below. The Board believes that much of value can be learned building on the base of the existing trials.
Determining Relative Benefits of Different Interventions
Most of the reported randomized trials have compared an active intervention to a no-treatment control group, an attention control group, or a control group that passively received educational materials. Few have compared different active interventions. As a result, there is little information available regarding whether one intervention is better than others and, if so, whether such interventions are more effective in all settings, and with all types of patients, or whether specific interventions are more effective with specific groups of patients. With some types of interventions, such as relaxation/imagery, the approach to the intervention does not appear to be as important as the fact that the intervention was delivered. In other types of interventions, for example, individual interventions, the specific approach appears to be critical in determining benefits of the intervention. Furthermore, although there is early evidence that group interventions (of a variety of types) are beneficial in both early stage and advanced breast cancer, it is unclear whether one type of group intervention is better than others, what the optimal duration of such intervention should be, whether the type or
duration of the intervention should be tailored to individual patient characteristics or phase of illness, and, if that is the case, what those characteristics are. Existing research suggests that the psychological profile of the patient may be one such characteristic (Goodwin et al., 2001; Hosaka et al., 2001b, 2000a, 2000b, 2000c).
Additional research to directly compare different interventions that have been shown to be effective in breast cancer (e.g., expressive–supportive group therapy versus cognitive–behavioral group therapy) is important in order to determine the relative effectiveness of these interventions overall and in subgroups of interest (e.g., distressed versus non-distressed). Ideally, this research should be conducted in early stage and advanced breast cancer separately as it is possible that effects may differ. Similarly, group interventions should be compared to individual interventions and efforts made to identify the benefits of different components of the more complex interventions (e.g., the contribution of relaxation and imagery to a cognitive–behavioral intervention). In this comparative research, outcome measures should be selected that target attributes likely to be influenced by the intervention (e.g., psychological status—mood, traumatic stress symptoms, coping—as well as overall quality of life, patient satisfaction, and cost-effectiveness). Given the current evidence of a variety of benefits of psychosocial interventions in breast cancer, the use of no-treatment control arms may become increasing difficult for ethical reasons; this will enhance the likelihood of comparative research in future.
Determining Optimal Timing and Duration of Psychosocial Interventions
In general, randomized trials of relaxation/hypnosis have tended to involve short interventions (one session to 6 months), whereas interventions in early stage breast cancer have been somewhat longer (4 weeks to 3 or 4 months), and interventions in women with metastases have been the longest (6 months to the end of life). However, none of the randomized trials to date has evaluated the effect of duration of the intervention on the magnitude and persistence of psychosocial benefits or on cost-effectiveness. Randomized trials to evaluate the optimal duration of intervention will be important, and these trials should be conducted separately in early stage and late stage breast cancer, as it appears likely the optimal duration of the intervention differs according to the disease stage. Within each phase of illness, research is also needed to identify the optimal timing of psychosocial interventions.
Identifying Patient Characteristics Associated with Intervention Benefits
A number of the published trials have suggested that psychological benefits vary according to patient characteristics. For example, Goodwin et al.
found that psychological benefits of supportive–expressive therapy in metastatic breast cancer were limited to women who were distressed at the time the intervention began (Goodwin et al., 2001). Similar differential effects in subgroups of women have been reported by others, although there is little evidence that predictors of benefit are consistent across studies (Hosaka et al., 2000c, 2001a, 2001b, 2000b). Many of the predictors will likely be psychosocial in nature (e.g., presence of acute distress, underlying psychosocial illness or adjustment disorder, personality traits, social and family support). However, some may involve demographic characteristics (e.g., age, social status) or medical factors. For example, relaxation/imagery has been shown to be effective in early-stage breast cancer, but the single trial in women with metastases yielded no benefit (Arathuzik, 1994).
Although these results should not be interpreted as proof of benefit only in early disease, they point to the need for more formal evaluation in the metastatic setting. Because it is possible that some women may benefit more from certain interventions and, indeed, that certain interventions may benefit certain types of women to a greater extent than others, research is desirable to further examine the patient characteristics that are predictive of greatest benefit of psychosocial interventions in breast cancer. Some of this research might involve re-analysis of existing trials, but it is likely that new trials will also be necessary. One of the goals of this research should be to determine whether some women do not require psychosocial intervention, in the same way that some women do not require adjuvant chemotherapy.
Understanding the Role of Nursing Interventions
A considerable number of randomized trials, predominantly in early stage breast cancer, have evaluated nursing interventions. There is some evidence of benefit for these nursing interventions. However, these studies all evaluated different interventions, some used small sample sizes, and some of the studies had significant methodologic limitations. Because nurses are so intimately involved in the care of breast cancer patients, better understanding is needed of the precise benefits of specialized nursing interventions on the psychosocial status of women with breast cancer and how these interventions are best integrated into a more comprehensive psychosocial intervention program.
Evaluating Peer Support/Peer Discussion Groups
Peer support groups have gained widespread acceptance among women with breast cancer. However, there is little clear evidence of benefit, and the single randomized trial that evaluated facilitated peer discussion failed to identify any psychological benefits (Helgeson et al., 2000, 1999). Although
many testimonials exist as to the benefits of individual peer support (Cella and Yellen, 1993), formal evaluation of the benefit of this support is lacking. Given the nature and widespread availability of peer support, the use of randomized designs may be challenging; however, evaluation using the strongest methodology possible is needed.
Evaluating Novel Interventions
There is growing interest among breast cancer patients and their families in the potential benefits of non-traditional, complementary and alternative medicine approaches to psychosocial support. These approaches include Internet chat groups and peer support groups, as well as a variety of non-traditional therapies, many of which focus on helping patients distract themselves from their breast cancer experience or turn their focus to other areas of their lives. Such interventions include yoga, reflexology, reiki, t’ai chi, music therapy, and art therapy. Because these interventions are of great interest to patients, and because they are often pursued by patients with little evidence of benefit apart from anecdotal testimonials, formal evaluation of their benefit in the setting of randomized trials would be useful. Such trials could include wait list control groups if resistance to randomization is encountered. The importance of research in this area is highlighted by the observations of Targ and Levine that a complex mind–body–spirit group intervention was at least equivalent to a standard psychoeducational support group intervention and that it led to enhanced satisfaction, fewer dropouts, and greater spiritual integration.
Addressing the Needs of Breast Cancer Survivors
Only one randomized trial of a purely psychosocial intervention was conducted in breast cancer survivors, and it did not address the psychosocial needs of breast cancer survivors (Fogarty et al., 1999). Instead, it used them as a convenience sample to evaluate the benefits of an enhanced compassion videotape. Research into survivorship issues is just beginning, but it is an important area involving millions of people. This research should be facilitated, and, as problems are identified, targeted interventions should be developed and tested to address the unique needs of this large population.
Addressing Family Issues
Only a small number of the randomized trials reported to date have involved partners or family members of breast cancer patients. Yet it is widely recognized that these individuals are often greatly affected by the illness of the breast cancer patient and that they may suffer significant emo-
tional distress that may continue long after the breast cancer patient dies. The Board believes that research should be pursued to identify the psychosocial needs of this population and to develop interventions to ameliorate their psychological distress.
Addressing Cultural/Minority Issues
None of the randomized trials in the United States addressed cultural and/or minority issues. Although there is some evidence from some countries outside of the United States that psychosocial interventions may have similar effects in different cultures, the influence of cultural and/or minority background requires further investigation (Fukui et al., 2000; Hosaka et al., 2000a, 2000b, 2000c, 2001a, 2001b). Specifically, descriptive research should be carried out to examine the unique needs of different cultures and/ or minority groups, followed by development of interventions that target these unique needs.
Developing Appropriate Measures of Psychosocial Outcomes
Many of the randomized trials reported to date have used a fairly consistent group of well studied psychosocial questionnaires, including the Profile of Mood States, the Impact of Events Scale, the Beck Depression Inventory, and the State Trait Anxiety Index. However, many others have used novel instruments, some of which are not well validated or are not well known. Furthermore, the standard psychosocial measurement instruments do not address all of the outcomes that are of interest in psychosocial intervention trials in breast cancer. A critical review is needed to identify domains and attributes that are not well addressed by well characterized questionnaires commonly used in breast cancer psychosocial intervention studies (e.g., cognitive functioning), to identify instruments used in other settings that measure those attributes, and to identify areas where there should be development of new instruments. The importance of different psychosocial outcomes should be prioritized (to the extent possible), and the magnitude of psychosocial benefit that is clinically important should be explored. This research might involve a consensus conference to identify a small number of clearly defined outcomes that could be used across a broad spectrum of trials so that the results of trials are more readily compared, followed by targeted research studies.
Translation of Research Findings to Community Practice
There is considerable evidence of efficacy of some types of psychosocial interventions in breast cancer; however, the extent to which these interven-
tions are used in clinical practice is unclear. Therefore, the current use of psychosocial interventions in breast cancer in academic and private medical practice should be evaluated. This evaluation should address access to, and utilization of, relaxation/hypnosis, peer support, and novel forms of support discussed above as well as more traditional group and individual interventions. An assessment of barriers to more widespread use of psychosocial interventions in breast cancer may be useful. Such barriers include (but are not limited to) cost, patient acceptability, physician acceptability, availability and preferences of psychosocial practitioners, logistical barriers to delivery, and knowledge of (or belief in) the effectiveness of psychosocial interventions. Evaluations are needed of psychosocial interventions implemented in “real world” settings, in which cost and integration into breast care in various community settings are assessed (Redman et al., 2003).
Applicability of Findings from Other Research to Women with Breast Cancer
In addition to the psychosocial research conducted in breast cancer patients reviewed here, there is also a large body of literature describing psychosocial research in other cancer types and in patients with other serious illnesses. The extent to which the results of this research in other settings are generalizable to women with breast cancer is not clear. A critical review of the published literature in other illnesses, focusing predominantly on other cancers, could provide evidence of generalizability, or lack of generalizability, of psychosocial research findings in these other settings to breast cancer.
Tracking Results of Psycho-Oncology Studies
Indexing of psycho-oncology studies is inconsistent and may be delayed depending on the journal used. Because these trials may be published in journals related to different disciplines, they are often difficult to find, even in exhaustive literature searches. Encouragement of a more standardized and timely approach to indexing would be helpful. A prospective registry of psychosocial intervention trials would facilitate tracking of ongoing studies and assist in planning of new intervention trials.
FINDINGS AND RECOMMENDATIONS
These research priorities will be addressed most effectively if the psycho-oncology research community works together to build on the strengths of previous research and to ensure that future research provides clinically meaningful information. Unless there is a compelling reason to study en-
tirely new intervention approaches, the comparative research outlined above should compare two or more therapies that have previously been shown to be effective; the most effective therapy can then be used in subsequent comparative work. Similarly, if one or more patient characteristics are identified as being predictive of benefit in one intervention study, future studies should examine those characteristics (as well as others if desired) in an attempt to replicate the earlier finding and contribute to a body of knowledge regarding predictors of benefit. This approach may be facilitated by more widespread conduct of multicenter trials of psychosocial interventions, a move away from many of the single-center studies that have been reported to date. In order to facilitate this broader type of research, it may be necessary to establish psychosocial intervention research networks, similar to those that exist for evaluation of other breast cancer treatments (chemotherapy, radiation, surgery). These collaborative networks might be “free standing,” but the benefits of integrating these networks into already established clinical trials groups should also be explored.
To continue progress in the research base that is necessary for sound development of interventions to address psychosocial, psychiatric, and quality of life issues in breast cancer, the Board recommends:
1. Research sponsors (e.g., NCI, ACS) and professional organizations (e.g., American Society of Clinical Oncology, American College of Surgeons, American Association of Colleges of Nursing, American Psychosocial Oncology Society, American Society of Social Work, American Society for Therapeutic Radiology and Oncology, Oncology Nursing Society) need to support efforts in collaboration with advocacy groups (e.g., National Breast Cancer Coalition; National Alliance of Breast Cancer Organizations) to enhance practice environments to promote coordinated, comprehensive, and compassionate care. Rigorous evaluations are needed of the cost and effectiveness of delivery models that show promise in improving access to psychosocial support services. These might include:
-
Collaborative practices in which a psychologist or other mental health provider forms a partnership with an office-based oncology provider to make psychosocial services available within the oncology practice;
-
Comprehensive breast cancer centers that generally integrate supportive care into a “one-stop-shopping” model of clinical practice;
-
Breast cancer nurse managers who provide case management, education, and supportive care within oncology practices;
-
Novel models of psychosocial services, such as ICAN project, in phase 2 demonstration, which utilizes master’s level counselors who receive a core curriculum in psychosocial oncology;
-
Demonstration projects to test the effectiveness of clinical practice guidelines on the management of psychosocial distress in improving psychosocial outcomes;
-
Development of measures of quality of cancer care that pertain to supportive care (including psychosocial services). Measures might include provider assessment of psychosocial concerns, the provision of information regarding community supportive care resources, and satisfaction with care.
In general, investigators working in this field should recognize that studies in the past would in many cases have been stronger if they had been on other than selected patients mostly in tertiary settings, or had not been unblinded, with small sample size, of insufficient power, of short duration, and the like. Future study designs should try to minimize such weaknesses.
2. Research sponsors (e.g., NCI, ACS) should continue to support basic and applied psycho-oncology research. This might include:
-
Further development of simple, rapid screening tools for identifying the patient with distress in outpatient offices and training of primary oncology teams in diagnosis of distress that exceeds the “expected” and when referral to supportive services should be made;
-
Studies that assess the relative effectiveness of various psychosocial interventions, using population-based patient samples of adequate size, the timing and duration of interventions, and innovative and inexpensive modes of administration (e.g., Internet-based approaches);
-
A consensus conference to develop a battery of standard instruments for outcome measures to permit comparison of data from studies carried out by different research groups;
-
Organization of a psychosocial clinical trials group in which a network of researchers could address key questions in multicenter studies that would allow access to large, population-based samples;
-
Clinical trials of psychosocial interventions that are conducted within routine breast cancer care in which cost and quality of life are outcome measures;
-
A registry of ongoing psychosocial research/trials to assist researchers in identifying and tracking new areas of study.
3. The NCI should support a special study to ascertain the use of, and unmet need for, cancer-related supportive care services (including psychosocial services) in the United States. The results of such a study could provide benchmarks against which care can be measured and performance monitored. Such a study would document existing disparities in service use by age, race/ethnicity, geography, and insurance coverage.
REFERENCES
Arathuzik D. 1994. Effects of cognitive–behavioral strategies on pain in cancer patients. Cancer Nurs 17(3):207–214.
Cella DF, Yellen SB. 1993. Cancer support groups: The state of the art. Cancer Pract 1(1):56–61.
Fogarty LA, Curbow BA, Wingard JR, et al. 1999. Can 40 seconds of compassion reduce patient anxiety? J Clin Oncol 19(17):3793–3794.
Fukui S, Kugaya A, Okamura H, et al. 2000. A psychosocial group intervention for Japanese women with primary breast carcinoma. Cancer 89(5):1026–1036.
Goodwin PJ, Leszcz M, Ennis M, et al. 2001. The effect of group psychosocial support on survival in metastatic breast cancer. N Engl J Med 345(24):1719–1726.
Helgeson VS, Cohen S, Schulz R, Yasko J. 1999. Education and peer discussion group interventions and adjustment to breast cancer. Arch Gen Psychiatry 56(4):340–347.
Helgeson VS, Cohen S, Schulz R, Yasko J. 2000. Group support interventions for women with breast cancer: Who benefits from what? Health Psychol 19(2):107–114.
Hosaka T, Sugiyama Y, Hirai K, Okuyama T, Sugawara Y, Nakamura Y. 2001a. Effects of a modified group intervention with early-stage breast cancer patients. Gen Hosp Psychiatry 23(3):145–151.
Hosaka T, Sugiyama Y, Hirai K, Sugawara Y. 2001b. Factors associated with the effects of a structured psychiatric intervention on breast cancer patients. Tokai J Exp Clin Med 26(2):33–38.
Hosaka T, Sugiyama Y, Tokuda Y, Okuyama T. 2000a. Persistent effects of a structured psychiatric intervention on breast cancer patients’ emotions. Psychiatry Clin Neurosci 54(5):559–563.
Hosaka T, Sugiyama Y, Tokuda Y, Okuyama T, Sugawara Y, Nakamura Y. 2000b. Persistence of the benefits of a structured psychiatric intervention for breast cancer patients with lymph node metastases. Tokai J Exp Clin Med 25(2):45–49.
Hosaka T, Tokuda Y, Sugiyama Y, Hirai K, Okuyama T. 2000c. Effects of a structured psychiatric intervention on immune function of cancer patients. Tokai J Exp Clin Med 25(4–6):183–188.
Maguire P, Brooke M, Tait A, Thomas C, Sellwood R. 1983. The effect of counselling on physical disability and social recovery after mastectomy. Clin Oncol 9(4):319–324.
Redman S, Turner J, Davis C. 2003. Improving supportive care for women with breast cancer in Australia: The challenge of modifying health systems. Psycho-Oncology 12(6):521–531.





























