Meeting Psychosocial Needs of Women with Breast Cancer (2004)
Chapter: 6 Delivering Psychosocial Services
6
Delivering Psychosocial Services
Important advances in the diagnosis and treatment of breast cancer over the last quarter century have changed the makeup of the population of women surviving with breast cancer and dramatically altered how care is delivered, moving it from largely in-hospital to primarily ambulatory care. This chapter reviews the implications of these advances with respect to the prevalence and management of psychosocial distress. This chapter describes the structure and delivery of psychosocial services to women with breast cancer, including information on how services are delivered and the extent to which clinical and psychosocial services are integrated. Lastly, evidence is presented on how frequently women with breast cancer use psychosocial services.
THE EVOLUTION OF BREAST CANCER CARE AND ITS IMPLICATIONS FOR THE PROVISION OF PSYCHOSOCIAL SERVICES
Quality of life following a diagnosis of breast cancer is influenced by how and when the disease is diagnosed, the treatment, and the manner in which care is delivered. Breast cancer diagnosis, treatment, and care delivery have evolved greatly in the past 25 years, altering the composition of the population of women living with breast cancer, the health status of survivors of the disease, and how care is delivered. In the area of diagnostics, the widespread use of mammographic screening has resulted in women being diagnosed at younger ages and with smaller tumors. The 20 to 30 percent decrease in mortality associated with mammographic screening has con-
tributed to a growing population of breast cancer survivors, estimated at 2.1 million women as of 1997. High screening rates have also resulted in more women being diagnosed with ductal carcinoma in situ (DCIS), a type of non-invasive breast cancer (see Chapters 2 and 3). In 2002, there were an estimated 47,700 women diagnosed with DCIS (54,300 with in situ cancer: lobular and ductal) (American Cancer Society, 2001, 2002). These women were not counted as among the 203,500 cases of invasive breast cancer, but because women with DCIS usually receive the same treatment as women with invasive early breast cancer, the rise in DCIS detection has increased the use of breast-cancer-related services and created a new cohort of women worried about their future risk of invasive disease.
Research conducted in the 1980s and early 1990s demonstrating that breast-conserving therapy followed by radiation is an efficacious alternative to mastectomy in most women has contributed to less disfigurement and reduced morbidity among women. This evolution in treatment has also reduced hospital stays and shifted care to outpatient settings. This trend has been accelerated with the dominance of managed care since the 1980s and efforts to reduce health-care costs. Mastectomy and other breast surgical procedures have been increasingly performed in outpatient day-hospital settings. According to one study, cancer-related complete mastectomies were rarely outpatient procedures in 1990, but by 1996, 8 percent of these procedures were outpatient in Connecticut, 13 percent were outpatient in Maryland, and 22 percent were outpatient in Colorado. By 1996, 43 to 72 percent of cancer-related subtotal mastectomies were outpatient procedures in these states, and 78 to 88 percent of lumpectomies were performed on an outpatient basis (Case et al., 2001). The implication of this shift in site of care is that women cared for in outpatient settings no longer have access to the many supportive care personnel that are hospital-based, such as social workers, nurse educators, psychologists, and clergy. The move to outpatient care and shorter hospital stays also has implications for caregivers and families. Much of the assistance with post-surgery recovery and rehabilitation is now assumed by families rather than by nursing personnel.
A greater reliance on pharmacological interventions for women with breast cancer follows findings that adjuvant systemic therapy reduces the risk of distant recurrence by about 40 percent and reduces mortality by 10 to 20 percent. New chemotherapeutic and hormonal agents have been introduced that are active in both early and metastatic breast cancer. These developments, while beneficial, have contributed to increased complexity of breast cancer care. Women treated for breast cancer in the 1960s would have typically been treated surgically with mastectomy in the hospital, with cancer care managed by a surgeon. In contrast, a woman with breast cancer today is likely to encounter a surgeon, radiation oncologist, and medical oncologist during her initial breast cancer treatment. With a number of
treatment options to consider, women have increasingly become active participants in their care and often seek second opinions regarding treatment options. The breast cancer advocacy movement has encouraged informed decision-making among women facing alternative treatment choices (Lerner, 2001; National Breast Cancer Coalition, 2002).
The many steps along the trajectory of contemporary breast cancer (see Figure 4-1 in Chapter 4) and the multiple providers a woman encounters as she completes her care add to the complexity of cancer and highlight the need for care coordination. The complexity of care and the absence of coordination are often in themselves a source of psychosocial distress. The question of “Who is my doctor?” arises often and adds to the sense of vulnerability and uncertainty.
The evolving nature of breast cancer treatment has resulted in a heterogeneous group of breast cancer survivors. Elderly survivors treated 20 to 30 years ago, for example, had fewer treatment options and likely experienced radical mastectomy. The issues of concern to those women were often linked to late effects of surgery such as lymphedema and body image. Younger cohorts of women, in contrast, have benefited from a wider range of options, but may be concerned about a broader set of late effects related to their treatment. Among the late effects of contemporary breast cancer treatments are cognitive deficits, early menopause, heart conditions, and sexual dysfunction. During the late 1990s, many women with metastatic breast cancer underwent bone marrow transplantation, which was later shown not to be more effective than chemotherapy alone for advanced disease. Women who survived this treatment experienced not only the late effects but also the financial costs of this expensive procedure.
Evidence emerged in the mid 1990s that there was no medical benefit of frequent specialized follow-up of women after initial breast cancer in terms of time to diagnosis of recurrence and quality of life (Rosselli Del Turco et al., 1994; The GIVIO Investigators, 1994). Prior to that time, women with breast cancer visited their surgeon or oncologist for as many as 10 years after diagnosis for history taking, physical examination, blood tests, imaging, and mammography. It was thought that women preferred specialized care and intensive follow-up after primary treatment, but according to a randomized controlled trial conducted in England in 1996, routine, less intensive follow-up care could be provided by primary care practitioners without compromising patient satisfaction (Grunfeld et al., 1999, 1996). Professional guidelines now recommend against extensive blood tests and imaging and encourage periodic physical examinations, mammography, and pelvic exams (www.PeopleLivingWithCancer.org). This plan for follow-up implies that primary care physicians and not oncology providers will be responsible for addressing long-term issues related to late effects and psychosocial distress. In the United States, however, follow-up by oncologists
continues as common clinical practice, driven perhaps by their availability and patient preferences, among other things. Women are still fearful about reduced frequency of visits and continue to believe that earlier diagnosis of recurrence is clinically important for a better outcome.
THE STRUCTURE AND DELIVERY OF PSYCHOSOCIAL SERVICES TO WOMEN WITH BREAST CANCER
Patterns of Breast Cancer Care
Assessing how well psychosocial services are being delivered depends on knowing where women with breast cancer seek care and who provides that care. There are very few descriptions of cancer-related health care delivery, but according to national population-based surveys, each year an estimated 4.8 million ambulatory care visits are made and 150,000 hospitalizations occur for breast cancer care (Table 6-1). These sources do not provide a great deal of clinical data, making it difficult to distinguish primary treatment from longer-term survivorship care. These data do provide rough estimates of who is getting care, where it is delivered, and some characteristics of care, for example, the source of payment for care.
Information on ambulatory care comes from two large population-based surveys conducted by the National Centers for Health Statistics, the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Care Survey (NCPB special tabulations of NAMCS and NHAMCS, 1995–2000). Each year, data are collected on a sample of 20,000 to 40,000 visits to physicians’ offices and a sample of 25,000 to 30,000 visits to hospital outpatient departments. Data are provided by physicians in their offices or by their office staff. Estimates of ambulatory care use are somewhat hampered by the exclusion of radiologists from the sampling frame of providers (some cancer-related radiology care is identified from data from hospital outpatient departments). According to these two surveys, the vast majority of ambulatory care occurs in private practice settings, with 90 percent of visits made to physician’s offices and 10 percent to hospital outpatient departments. Of the visits to physicians’ offices, 52 percent are made to oncologists, 19 percent to general surgeons, 5 percent to specialty surgeons, and 23 percent to specialists in medicine and primary care. Visits to hospital outpatient departments are most often to general medicine and surgery clinics. These findings suggest that efforts to improve the provision of psychosocial care should target oncology and surgery providers in private practice settings.
Although 45 percent of new cases of cancer occur among women age 65 and older, more than half of cancer-related outpatient visits are made by women under age 65 (Table 6-2). This likely reflects the use of ambulatory
TABLE 6-1 Characteristics of Breast Cancer-Related Ambulatory Care Visits, by Site of Care, United States, 1995-2000 [preliminary data]a
care services by cancer survivors, who as a group are younger than women who are newly diagnosed (incident cases). The age and racial/ethnic distribution of patients seen in physician offices and hospital outpatient departments differs. Younger women and members of minority racial/ethnic groups are more likely to frequent hospital outpatient departments. Patients seen in outpatient departments are also more likely to be uninsured or insured through the Medicaid program. Any effort to improve services to members of minority racial/ethnic groups could focus on these sites of care.
Reasons for visits (as stated by patients) were similar by site. Generally, they were to monitor progress, to obtain breast cancer care and examinations, and to receive post-operative care. Patients visiting hospital outpatient departments are more likely to spend more time with the physicians—
TABLE 6-2 Characteristics of Breast Cancer-Related Ambulatory Care Visits, by Site of Care, United States, 1995-2000a
|
Characteristic |
Physician Office-Based Visits (percent) |
Hospital Outpatient Department Visits (percent) |
|
Total number of visits |
4,353,000 |
483,000 |
|
Percent |
100.0 |
100.0 |
|
Age |
|
|
|
Less than 45 |
13.0 |
20.2 |
|
45 to 64 |
45.5 |
50.4 |
|
65 to 74 |
25.0 |
17.6 |
|
75 and older |
16.5 |
11.8 |
|
Race/ethnicity |
|
|
|
White, non-Hispanic |
86.3 |
76.5 |
|
White, Hispanic |
4.7 |
7.3 |
|
Black |
6.3 |
13.5 |
|
Other |
2.6 |
2.7 |
|
Main source of payment |
|
|
|
Private insurance |
59.8 |
57.6 |
|
Medicare |
25.0 |
14.5 |
|
Medicaid |
2.5 |
6.9 |
|
Other, unknown source |
8.8 |
10.5 |
|
Uninsured (self pay/no charge) |
3.9 |
10.6 |
|
Reason for visit (as reported by patient) |
|
|
|
Progress visit |
14.3 |
19.5 |
|
Breast cancer care |
13.2 |
18.1 |
|
General medical exam/breast exam |
8.8 |
9.2 |
|
Post-operative visit |
8.2 |
4.4 |
|
Chemotherapy |
7.3 |
10.6 |
|
Medical counseling |
— |
3.7 |
|
Radiation therapy |
— |
2.5 |
|
Other |
48.1 |
32.0 |
|
Time spent with doctorb |
|
|
|
Less than 15 minutes |
20. 3 |
27.0 |
|
15 to 29 minutes |
54.9 |
17.9 |
|
30 minutes and longer |
24.7 |
55.1 |
|
Saw RN, PA, NP during visit |
|
|
|
Yes |
37.7 |
59.6 |
|
No |
62.3 |
40.4 |
|
Services provided during visit |
|
|
|
Mental health and psychotherapyc |
4.8 |
5.3 |
|
Breast self exam instruction |
50.0 |
34.5 |
|
Diet counseling/education |
15.7 |
7.6 |
|
Exercise counseling/education |
13.3 |
4.7 |
|
aAnalyses of the National Ambulatory Medical Care Survey (NAMCS) and National Hospital Ambulatory Medical Care Survey (NHAMCS), 1995–2000. Breast cancer-related visits are those for which breast cancer (ICID-9-CW=174) was recorded as the first, second, or third diagnosis associated with the visit. bTime spent with physician is not available in hospital outpatient clinics in 1995. cMental health was defined as general advice or counseling about mental health issues; education about mental disorders. Includes referrals to other mental health professional for mental health counseling. Physicians could also indicate provision of psychotherapy, psycho-pharmacotherapy, and stress management (included here). SOURCE: NCPB staff analyses of NAMCS and NHAMCS. |
||
for more than half (55 percent) of visits, patients were seen for half an hour or longer as compared to 25 percent in physicians’ offices. This may reflect the complexity of cases seen in outpatient departments, the provision of more extensive counseling, or the fact that many outpatient departments have teaching functions. Visits to outpatient departments are more likely than those made to physicians’ offices to bring patients into contact with registered nurses, nurse practitioners, or physician assistants (60 vs. 38 percent of visits). According to these ambulatory care surveys, mental health-related services are rarely provided in the context of cancer-related care (in 5 percent or less of visits), and generally are less likely to be provided than counseling regarding breast self-exam, diet, and exercise. These estimates, may, of course, be artificially low if providers failed to document the provision of counseling on the survey.
In the past decade, comprehensive breast centers and breast care programs have been developed to put under one roof the many providers and services that a woman with breast cancer might need to make breast care simpler and to provide “one stop” care. Typically, these programs employ social workers, clinical nurse specialists, or psychologists affiliated with them, who provide some form of systematic psychosocial intake or assessment, education, and counseling. Because the physical and the psychological impacts of the disease and treatment are often inter-related, having psychosocial services available within the breast care setting allows for the flow of patient-centered information to be shared among the center practitioners. For example, if a woman suddenly develops lymphedema of her arm, she will need a variety of physical interventions to address the problem, and she will need someone to assist her with the psychological distress that often accompanies this experience. Women understandably like the comprehensive breast care approach, and it appears to be gaining in popularity. However, it is not known what proportion of women receive care in these settings, but it is surely a small minority given that most visits are to a physician’s office and the small number of comprehensive cancer centers and their uneven geographic distribution (Frost et al., 1999; Rabinowitz, 2002). Furthermore, while multidisciplinary care in breast clinics has gained wide acceptance in theory, in practice it can be a complicated situation. There can be economic constraints as well as turf issues among surgery, medical oncology, and radiology, requiring that some sacrifices be made by at least one or two of these major players so that the patient may be best served. Specifically, this means that one or more of the three players may have to give up their turf and perhaps efficiency in working in the clinic. For example, a member of the treatment team may have to wait while patients move through a surgery clinic, some of whom are not diagnosed with breast cancer and therefore may not be in need of multidisciplinary collaboration. Collaboration can be limited if salaries are at stake and one member of the team stands to gain or lose money depending on how the clinic is managed.
Information on breast cancer-related hospital care is available from the National Hospital Discharge Survey (NHDS), a population-based survey conducted by the Centers for Disease Control and Prevention. Presented here are results of analyses of a sample of 1,850 discharges for which breast cancer was the primary diagnosis associated with the hospitalization (a total of 613,719 hospital discharges [all causes] were in the combined sample from the 1999 and 2000 surveys). According to the NHDS, there were an estimated 106,600 United States hospitalizations annually with the associated principal diagnosis of female breast cancer (Table 6-3). Half (50.1 percent) of the breast cancer-related hospital care was for women age 65 and older. Nearly two-thirds of breast-cancer-related hospitalizations were for mastectomy (65.2 percent), 7.2 percent for subtotal mastectomy, 10.1 percent for lumpectomy, and 17.5 percent are for other indications. Breast cancer-related stays in the hospital were relatively short, with 39.2 percent of women discharged within a day. As many as 7,500 women with breast cancer who were over the age of 75 were discharged from the hospital to their home within one day. The implications of this are that post-surgical care for elderly women, who are often frail and have other chronic illnesses, has to be managed at home, usually by family members and caregivers. Medicare is the predominant payer for hospital care, responsible for 45.0 percent of breast cancer-related discharges. One-in-five (22 percent) of discharges related to breast cancer care were from hospitals with fewer than 100 beds. This has implications for psychosocial care insofar as smaller hospitals are less likely to have extensive support service personnel immediately available.
This descriptive information on ambulatory and hospital care does not fully capture breast-cancer related care. Increasingly breast cancer surgical care is being delivered in free-standing ambulatory surgery centers. There are few sources of national data on care provided in these facilities. A national survey of ambulatory surgery centers was conducted by NCHS in 1995, but it has not been repeated. As mentioned earlier, by 1996, roughly 10 to 20 percent of cancer-related complete mastectomies were outpatient procedures, 40 to 70 percent of subtotal mastectomies were outpatient procedures, and 80 to 90 percent of lumpectomies were performed on an outpatient basis (Case et al., 2001). While much of the surgical care provided to women may be absent in the estimates above, it is likely that pre- and post-surgical consultations take place in ambulatory settings for which data are available and where psychosocial issues would most likely be addressed.
PSYCHOSOCIAL SERVICE USE
While evidence suggests that roughly 20 to 40 percent of women with breast cancer will exhibit psychosocial distress (see Chapter 3), it is not well
TABLE 6-3 Characteristics of Breast Cancer-Related Hospitalizations, United States, 1999–2000
|
Characteristic |
Annual Number |
Percent Distribution |
|
Total |
106,600 |
100.0 |
|
Age |
|
|
|
Under 45 |
12,200 |
11.5 |
|
45–64 |
41,000 |
38.5 |
|
65–74 |
27,200 |
25.6 |
|
75 and older |
26,100 |
24.5 |
|
Principal procedurea |
|
|
|
Mastectomy |
69,500 |
65.2 |
|
Subtotal mastectomy |
7,700 |
7.2 |
|
Lumpectomy |
10,700 |
10.1 |
|
Other |
18,700 |
17.5 |
|
Discharge status |
|
|
|
Routine/discharged home |
93,500 |
87.8 |
|
Long-term care institution |
3,900 |
3.7 |
|
Dead |
2,000 |
1.9 |
|
Other |
7,200 |
6.7 |
|
Length of stay |
|
|
|
1 day |
41,800 |
39.2 |
|
2 days |
31,200 |
29.2 |
|
3 days |
16,500 |
15.4 |
|
4 or more days |
17,100 |
16.1 |
|
Main source of payment |
|
|
|
Medicare |
47,900 |
45.0 |
|
Medicaid |
6,000 |
5.6 |
|
Private |
29,000 |
27.2 |
|
HMO/PPO |
15,400 |
14.5 |
|
Uninsured |
3,000 |
2.8 |
|
Other |
5,300 |
5.0 |
|
Size of hospital (number of beds) |
|
|
|
6–99 |
23,400 |
22.0 |
|
100–199 |
28,700 |
26.9 |
|
200–299 |
14,900 |
14.0 |
|
300–499 |
25,600 |
24.0 |
|
500 and over |
14,000 |
13.1 |
|
Hospital ownership |
|
|
|
Proprietary |
8,100 |
7.6 |
|
Government |
11,200 |
10.5 |
|
Nonprofit |
87,200 |
81.9 |
|
alCD-9-CM codes for procedures: mastectomy (85.4), subtotal mastectomy (85.23), lumpectomy (85.21). NOTE: 1,850 of 613,719 sample hospital discharges were for women whose primary diagnosis was breast cancer (International Classification of Diseases, 9th Revision, Clinical Modification [ICD-9-CM] code 174). |
||
understood how often women with breast cancer are referred for services, how accessible services are to women, and how often services are actually sought. Evidence from the field of mental health suggests that a majority of individuals with mental disorders do not receive mental health services (U.S. Department of Health and Human Services, 2000). According to one of the largest studies of mental health needs and service use, 28 percent of individuals can be expected to have mental or addictive disorders in the course of a year, but only 15 percent of the population obtains services to address these disorders (U.S. Department of Health and Human Services, 2000). When mental health services are obtained, they are largely obtained in the health sector (either mental health specialty or general health sector). Other sectors such as human services or voluntary support networks are also important providers of services.
The National Coalition for Cancer Survivorship (NCCS), an advocacy organization, as a part of its published “Imperatives for Quality Cancer Care” stressed the importance of meeting the psychosocial needs of cancer survivors. The NCCS recommends that psychosocial services be provided for every person with cancer including (http://www.canceradvocacy.org):
-
Availability of a psychosocial program and case manager who provides assessment, education, support, and referral for services;
-
Screening for psychosocial risk and in-depth individual and family assessments conducted on a regular and continuous basis across the disease spectrum by qualified psychosocial specialists and, in conjunction with the medical plan, the development of a psychosocial treatment plan;
-
A choice of intervention modalities including individual, family, marital, peer, and pastoral counseling and access to complementary therapies;
-
Training in cancer-related self-advocacy including information seeking, negotiation, communication, and problem-solving skills.
The NCCS further recommends that the patient and the family be seen as the unit of care and receive:
-
Culturally appropriate education about cancer, its treatment and side effects, and the necessary physical care responsibilities that need to be assumed by the patient and family; and
-
Information about local, state, and national organizations that provide support, education, and concrete services including how to access legal information and services for workplace, insurance and other cancer-related discrimination.
Judging how close the cancer care community is in meeting these goals is difficult because of a relative lack of information on the content of cancer care. The extent of psychosocial service use among women with breast cancer is hard to gauge because of limited data from large representative samples and because survey and regional study data vary in different reports and time periods. The National Cancer Institute added a special supplement to the National Health Interview Survey (NHIS) in 1992 to assess issues related to cancer survivorship. The NHIS is a population-based survey of 49,401 households conducted by the National Center for Health Statistics, Centers for Disease Control and Prevention. According to this supplement, which sampled 24,040 households, only 14 percent of 656 individuals who had had any cancer (excluding non-melanoma skin cancer) within the past 10 years reported that they had received counseling or participated in a support group following their diagnosis (Hewitt et al., 1999). Among those who did not receive counseling, most (64 percent) felt that they did not need it, 12 percent did not want it, and 9 percent did not know that it was available. Another 15 percent said that they did not get counseling for some other reason. Controlling for sociodemographic characteristics, women with breast cancer (and individuals with any cancer diagnosed more recently) were found to be twice as likely as those with other cancers to have received counseling or to have participated in a support group. More than a quarter (27 percent) of women with a history of breast cancer had received psychosocial services following their diagnosis (Hewitt et al., 1999).
In a more recent analysis of data from the NHIS, cancer survivors (4,878) were more likely than individuals without a history of cancer to report using a mental health service within the past year (7.2 versus 5.7 percent) (Hewitt and Rowland, 2002). A mental health service was defined as contact with a mental health professional such as a psychiatrist, psychologist, psychiatric nurse, or clinical social worker. Participation in support groups was not ascertained, and the reason for the mental health visit was not asked. Controlling for socio-demographic characteristics, cancer survivors without other chronic illness were 1.6 times more likely to use a mental health service, and cancer survivors with other chronic illness were 3.0 times more likely to use a mental health service as compared to those without cancer or other chronic disease. According to these results, based on 3 years of NHIS data (1998 to 2000), survivors of breast cancer were not more likely (6.3 percent) than survivors of other cancers to have used a mental health service (Hewitt and Rowland, 2002). This latter might seem at variance with the increased likelihood found in earlier surveys, but the intervention, mental health services for any reason, differed from cancer related counseling and support group participation as did the time period.
Information from regional studies confirms findings of relatively low mental health service use among women with breast cancer. According to a survey of 233 women (151 completed responses, 65 percent response rate) conducted at a regional breast care center in upstate New York and contacted within 3 years of their breast cancer diagnosis, relatively few had used formal psychosocial services. Only 15 percent of women had talked to a professional counselor (e.g., psychologist), 25 percent had participated in a support group, and the majority (60 percent) of women had talked to a friend who had breast cancer (Table 6-4), although there is overlap in these percentages. Of those who did not seek services, the majority did not feel it
TABLE 6-4 Survey of Breast Cancer Patients Regarding Use of Psychosocial Services
was necessary (Trief and Donohue-Smith, 1996). Women were more likely to report needing counseling at the time of diagnosis (41 percent), but a substantial proportion of women felt that counseling was needed during treatment (21 percent) and after treatment (14 percent) (Table 6-4). Among this sample, 28 percent reported a great deal of anxiety, and 14 percent reported a great deal of depression as they had coped with their illness. The percentage that experienced both a high degree of anxiety and depression was not reported, so it is not clear that the percentages can be summed to a level of distress of 42 percent. The authors concluded that although a sizable minority of women need formal psychosocial services, many women work their way through the stressful periods using available support and their own coping skills.
This conclusion is consistent with work of Worden and Weisman, investigators who developed a screening survey to identify cancer survivors at risk for poor coping and distress. Of 372 patients screened, 124 (33 percent) were found to be at risk and about half (60) accepted counseling. There did not appear to be any clear way to differentiate among those who did or did not accept counseling (Worden and Weisman, 1980). A German study conducted among 132 oncology outpatients (72 percent of whom had breast cancer) found that 28 percent participated in psychosocial support, with younger patients more likely to participate (Plass and Koch, 2001). The main reason for not participating was sufficient support from family, friends, or doctors. In an Australian study involving 202 individuals (115 males) with cancer seen in an outpatient setting (all cancer sites), counseling was offered to 48 percent of patients but was only accepted by 28 percent of patients to whom it was offered. A frequently reported reason for refusal of services was “not now” indicating that the offer of psychosocial services needs to be repeated (Curry et al., 2002).
Relatively few long-term survivors of breast cancer continue to receive psychosocial support, according to a large cohort study of women conducted in Los Angeles and Washington DC. In this study of 5- to 10-year survivors, fewer than 13 percent of women reported that they were currently using psychosocial or counseling therapies, while many more said that they had used them in the past. Only 6 percent of the women were currently in individual therapy. Only 5 percent were currently active in cancer support groups, although 30 percent said that they had used them in the past (Ganz et al., 2002).
Other research points to an unmet need for psychosocial services. Ferrell and colleagues asked nearly 300 women, “What resources do you feel you did not receive and are most needed to improve QoL?” (Ferrell et al., 1998; Simmons, 1998). Respondents identified 9 resources related to psychosocial support that were lacking in their care:
-
Support groups (peer-led, newly diagnosed, single women, long-term survivors)
-
Individual counseling
-
Family support
-
Education on delayed side effects
-
Management of menopause/hormone changes
-
Spiritual support
-
Support from/for spouse
-
Sexuality counseling
-
Support for fear of recurrence
In summary, it is difficult to judge the extent of use of psychosocial services among women with breast cancer, but available evidence from national surveys and regional studies of cancer patients’ use and acceptance of psychosocial services suggests that: use is relatively low (perhaps 10 percent and at the most 30 percent, and often of relatively informal nature) (Ganz et al., 2002; Hewitt et al., 1999; Plass and Koch, 2001; Trief and Donohue-Smith, 1996; Worden and Weisman, 1980); it seems to diminish with time; and most individuals who refuse services want to cope using their own resources, or to receive help at another time.
The Delivery of Psychosocial Services
Psychosocial services can be delivered by primary care and cancer care providers, specialty providers such as mental health professionals (psychologists and psychiatrists), advanced practice nurses, social workers, community-based programs, and increasingly by telephone or online computer services (see Chapter 4 for a description of psychosocial providers). Psychosocial services may or may not be integrated with breast cancer clinical care. Some settings such as comprehensive breast care centers have psychosocial providers on staff (Sorensen and Liu, 1995), while in other settings there are parallel systems for clinical and psychosocial care. This section describes examples of the delivery of psychosocial services in private practice, a managed care setting, through community-based programs, and via computer. The examples are drawn from presentations of program providers at the Board’s October 2002 workshop (see agenda in Appendix A).
Private Practice
Most women receive their breast cancer care in community-based private practice settings. Psychosocial services may be provided by primary care physicians or oncology providers in the context of clinical care, but relatively few
clinicians have psychologists or social workers available on site, unless they work in a large group practice or have a hospital-based practice. Physicians may refer individuals experiencing psychosocial distress to a local psychologist or psychiatrist or to community-based support programs available through a local hospital or breast cancer group. A model that is infrequently used, but which holds promise for making psychosocial services more accessible to patients seen in private physicians’ offices is “collaborative practice,” which involves a psychologist in private practice regularly rotating to private oncology, primary care, and other practices (e.g., obstetrics/gynecology) to work in partnership with referring physicians.
At the NCPB October 2002 workshop, the Board heard from Dr. Helen Coons, a psychologist in private practice who works collaboratively with a number of oncology care clinicians to provide psychosocial support services. Among the services that psychologists working in this fashion may provide are counseling related to treatment, depression, body image concerns, symptoms (e.g., hot flashes), sexual, reproductive and parenting issues, and substance abuse problems. Dr. Coons reported that commonly addressed issues in her practice include fears of recurrence, concerns about symptoms, anxiety, and adjustments at the end of life.
Managed Care
The majority of Americans receive their care within a managed care plan. Managed care can be defined as an entity that assumes both the clinical and the financial responsibility for the provision of health care for a defined population (Donaldson, 1998). With an increasingly complex health care system, a number of types of managed care have emerged, and it is difficult to distinguish one type of managed care organization from another (Landon et al., 1998). There is no information regarding how psychosocial care is delivered within managed care plans across the country, but there are a few programs that have been described as improving the quality of breast cancer care, including patient satisfaction with care. The American Association of Health Plans recognized one supportive care program as exemplary; it is offered by one of its members, a large group-model HMO in Southern California (Geiger et al., 2000).
The Southern California Kaiser Permanente Medical Group in collaboration with Women’s Information Network Against Breast Cancer (WIN-ABC) improved patient satisfaction with care following the introduction of a breast cancer patient information and support program (Geiger et al., 2000). The program, called Breast Buddy Care Program, featured a coordinator, information resources, and mentoring from a breast cancer survivor. Following implementation of the program, participants were more likely than non-program respondents to be very satisfied with their care (71 percent versus 56 percent). Use of the program resources was relatively high, with 75 percent of
women using materials from the clinic-based library and 60 percent requesting a patient mentor. Investigators estimate that the annual cost of a fully functioning program at a single hospital with several hundred new breast cancer cases annually would probably range from $25,000 to $75,000.
Cancer Center-Based Programs
Many women with breast cancer will receive at least some of their care within a hospital, either as an inpatient or when visiting an outpatient hospital-based practice or clinic. There are two sets of standards that address cancer-related quality of care, those of the American College of Surgeons’ (ACoS) Commission on Cancer (CoC), and those of the Association of Community Cancer Centers (ACCC). Of the two, the standards of the CoC affect more individuals with cancer because an estimated 82 percent of new cases of cancer are seen in the 1,428 hospitals approved by the CoC. Relatively few individuals with cancer are seen within the 47 NCI-designated comprehensive cancer centers, but these institutions are where many of the research, education, and training programs are located, making them important models of care. This section of the report describes the availability of psychosocial services within hospitals that provide cancer care.
The American College of Surgeons’ Commission on Cancer The CoC sets standards for quality multidisciplinary cancer care delivered primarily in hospitals, surveys hospitals to assess compliance with those standards, collects standardized and quality data from approved hospitals to measure treatment patterns and outcomes, and uses the data to evaluate hospital provider performance and develop effective educational interventions to improve cancer care outcomes at the national and local level (http://www.facs.org/dept/cancer/coc/cocar.html, accessed January 24, 2003). Selected standards of the Commission related to the provision of psychosocial care are shown in Box 6-1.
The CoC had, by 2003, approved 1,428 cancer programs which, as mentioned earlier, are estimated to provide care for 82 percent of the nation’s newly diagnosed patients (http://www.facs.org/dept/cancer/coc/whatis.html, accessed May 1, 2003). The Commission conducts extensive reviews of cancer programs through onsite visits at least every 3 years. Findings of the CoC survey are used as part of the Joint Commission for the Accreditation of Healthcare Organizations (JCAHO) accreditation process for JCAHO-accredited organizations that house a cancer center. The collaboration between the American College of Surgeons’ CoC and JCAHO is an attempt to increase the visibility of approved cancer programs, share information on standards and survey process, and increase consumer access to performance information about health care organizations. CoC staff provided information on supportive care services from institutions surveyed by
|
BOX 6-1 Cancer patients have access to rehabilitative, supportive, and continuing care services. (standard 5.1.0)
Site-specific services are based on the needs of the patients (standard 5.2.0). There is a multidisciplinary team approach to planning and implementing supportive and continuing care services (standard 5.3.0).
Oncology services provide multidisciplinary care (standard 4.1.0).
SOURCE: American College of Surgeons’ Commission on Cancer, 1997. |
TABLE 6-5 Support Services Offered by Cancer Programs Approved and Surveyed by the American College of Surgeons’ Commission on Cancer, 1999–2001
|
Servicea |
Programs Offering Service (N = 1170)b |
|
|
Support services: |
Number |
Percent |
|
Home care |
1081 |
92 |
|
Hospice |
1037 |
87 |
|
Nutritionc |
869 |
74 |
|
Pain management |
1081 |
92 |
|
Lymphedema rehabilitation |
396 |
85 |
|
Providers: |
|
|
|
ONS certified nurses on staff |
994 |
85 |
|
Physical/occupational therapist |
455 |
98 |
|
Pastoral care |
1152 |
98 |
|
Psychiatrist |
1114 |
95 |
|
Psychologist |
1062 |
91 |
|
Social worker |
1155 |
99 |
|
Rehab therapist |
1101 |
94 |
|
Stomal therapist |
1082 |
92 |
|
Support activities: |
|
|
|
Breast cancer specific: |
|
|
|
Reach to Recoveryd |
1048 |
90 |
|
Prostate cancer specific: |
|
|
|
Man to Mane |
489 |
42 |
|
US Toof |
304 |
26 |
|
Any cancer type: |
|
|
|
CanSurmountg |
194 |
17 |
|
I Can Copeh |
651 |
56 |
|
Other Support Groups |
359 |
77 |
|
aServices may be available directly from the institution or by referral to appropriate resource. bCombinedsample results from CoC approved programs surveyed in 1999 (N = 325), 2000 (N = 380), and 2001 (N = 465). cIn 1999 13 percent of surveyed programs reported nutrition services as compared to 98 percent in both 2000 and 2001. This significant change could not be explained by CoC staff. dA support group sponsored by ACS for women with breast cancer. eA support group sponsored by ACS for men who are prostate cancer survivors. fUS TOO provides information, local support groups, counseling and educational meetings to assist people with prostate cancer as they make decisions about their treatment and continued quality of life. gA program that puts a patient in touch with a person who has experienced the same kind of cancer. hA 7-week educational series for cancer patients and their families sponsored by ACS. |
||
CoC during 1999, 2000, and 2001 (personal communication from Connie Blankenship, CoC, to Maria Hewitt, March 31, 2003). The information provided is self reported on the application forms completed by institutions in advance of their on-site survey (Table 6-5). At least some level of supportive care was available in the reporting sites, for example, social workers were available in 99 percent of programs, psychologists were available in 91 percent of programs, and the ACS Reach to Recovery was available in 90 percent of programs.
Association of Community Cancer Centers Standards (ACCC) ACCC is a membership organization that includes 650 medical centers, hospitals, oncology practices, and cancer programs. The organization estimates that its members provide services to 40 percent of all new cancer patients in the United States (http://www.accc-cancer.org/about/, accessed January 24, 2003). The provision of psychosocial services is necessary to meet ACCC cancer program standards (Box 6-2) (http://www.accc-cancer.org/pubs/Standardstemp.html, accessed January 22, 2003). The ACCC revised its Standards for Psychosocial Services based on the NCCN standards (1999) and clinical practice guidelines to note that psychosocial services should be provided by several kinds of professionals, all of whom should have training or experience in the psychosocial problems of patients with cancer (Standard 1). Standard 2 outlines the need for a multidisciplinary committee to tailor the standards to the needs of each clinical setting and to monitor programs to ensure accountability for undertaking recommendations and changes. Unlike the CoC, there is no formal review of compliance to these standards.
National Cancer Institute-designated cancer centers The Cancer Centers Program of the NCI supports cancer research programs in 61 institutions across the United States (Figure 6-1) (http://www3.cancer.gov/cancercenters/description.html). Although the support from NCI is mainly limited to support of research infrastructure, all clinical and comprehensive cancer centers also provide clinical care and services for cancer patients. Three types of centers are supported through the Cancer Centers Program:
-
Generic cancer centers have a narrow research that may focus, for example, on basic sciences;
-
Clinical cancer centers usually integrate strong basic science with strong clinical science; and
-
Comprehensive cancer centers integrate strong basic, clinical, and prevention, control, and population sciences.
As shown by the map, large areas of the United States particularly the midsection of the country, are not near an NCI-designated cancer center.
|
BOX 6-2 Standard I Psychosocial services are provided by several disciplines in order to address the range of problems that patients and their families have as a consequence of cancer and its treatment. The disciplines are represented by social workers, nurses, psychologists, and psychiatrists, who are trained and skilled in the identification of psychological and social problems and are able to work with the primary oncology team and assure triage of the patient to the appropriate resources for assistance and/or treatment. Standard II Psychosocial services, provided by the professional outlined above, will follow clinical practice guidelines that are both consensus and empirically derived. A. Psychosocial services include, but are not limited to:
|
A few studies have examined the availability of supportive care services in these cancer centers. Surveys of NCI clinical and comprehensive cancer centers conducted in the early 1990s indicate that virtually all of the responding cancer centers offered group support programs (Coluzzi et al, 1995, Gruman and Convissor, 1995; Presberg and Levenson, 1993). In a more recent study conducted in 2000, about half of the NCI-designated comprehensive cancer centers (18 of 37 centers) had professionally led support groups for post-treatment cancer survivors (all 37 NCI-designated centers participated) (Tesauro et al., 2002).
At the October 2002 NCPB workshop, a psychologist from the Comprehensive Cancer Center of Wake Forest University/Baptist Medical Cen-
B. A multidisciplinary committee should be established to assume responsibility for the quality of psychosocial services given, implementation of standards of care and quality assurance projects to assure that distressed patients are identified and treated promptly and appropriately. C. The multidisciplinary committee should be responsible for assuring that qualified and trained professionals in each discipline are available to provide the multidisciplinary services, or that they are accessible by consultation. D. The multidisciplinary committee should develop methods for rapid screening of patients for distress, an algorithm to trigger referral for psychosocial services and to assure that the professionals utilize clinical practice guidelines developed for their discipline. E. Institutions, through their multidisciplinary committees, should undertake the educational efforts to inform staff and patients of the fact that psychosocial services are part of the total care provided and inform them of the procedures to obtain care. SOURCE: http://www.accc-cancer.org/pubs/Standardstemp.html, accessed January 22, 2003. |
ter (an NCI-designated center) described its psycho-oncology program (R. McQuellon, workshop presentation, October 2002; McQuellon et al., 1996). The program provides individual and family counseling (inpatient and outpatient), support groups, new patient orientation, patient education, case consultation, veteran patient consultation, volunteer hospitality, and breast cancer risk assessment. Also available to patients are psychiatry, pastoral counseling, physical therapy, and other resources of the hospital/ medical school. To facilitate access to these services, resources have been located near outpatient treatment areas, for example in the hematology and oncology, radiation oncology clinics, and breast care center. The psychosocial needs of about 2,000 hospitalized cancer patients and nearly 5,000
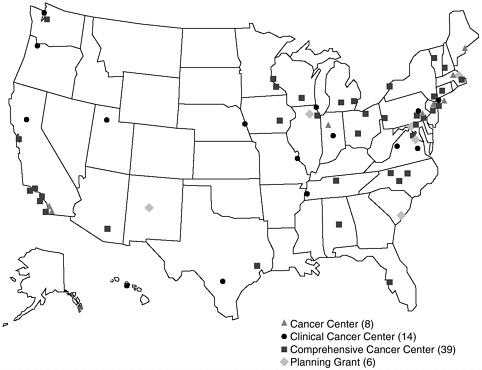
FIGURE 6-1 NCI-supported cancer centers.
SOURCE: http://www3.cancer.gov/cancercenters/description.html, accessed January 24, 2003.
individuals seen in outpatient clinics are met by 4 professional staff. The program is heavily dependent on a group of trained volunteers (about 20 per week participate in care) to extend services. Financial support comes largely through an annual fund raiser (60 percent), Wake Forest/Baptist Medical Center (20 percent), grants (10 percent), fee for service (5 percent), and donations (5 percent). According to the program director, this reliance on private donations and volunteer support is typical of such hospital-based programs.
Psychosocial services for cancer patients have become more constrained due to increasing financial pressures in the health-care setting. Social work departments have contracted as hospital resources have diminished, and in many clinical settings these services only exist through philanthropic support. Under these circumstances, it is only the most needy patients who receive attention for the psychosocial issues associated with their breast cancer experience.
Community-Based Support
There are psychosocial services for women with breast cancer available through voluntary organizations, many of them at no cost. Table 6-6 describes some of the programs that are available nationally. Among the services these programs offer are peer support, individual counseling by telephone, information on nutrition and exercise, and assistance with appearance, for example, wigs and breast prostheses. This section of the report highlights programs represented at the October 2002 NCPB workshop, those offered by the American Cancer Society, the Wellness Community, and a few programs that focus on the needs of Hispanic and African American women with breast cancer.
American Cancer Society Programs The American Cancer Society sponsors several programs for women with breast cancer (see Table 6-6). The Reach to Recovery program, offered since 1960, provides peer support to women with breast cancer. Initially designed for women after mastectomy in hospitals, the program is now offered largely in the community. Attempts are made to match peer counselors with women with cancer by age, type of procedure, and cancer stage. There were 75,000 to 80,000 visits made by 16,000 trained volunteers in 2000. Road to Recovery is an outgrowth of this program that provides rides to individuals with cancer who need transportation to treatment. There are no national estimates of how many people use this program; however, in Massachusetts about 35,000 trips were made in recent years as part of this program.
Since 1989, the Look Good…Feel Better (LGFB) Program has provided assistance with makeup, skincare, and other aspects of appearance (e.g., consultation on wigs, turbans). The program is co-sponsored by the Cosmetic, Toiletry, and Fragrance Association Foundation and the National Cosmetology Association. In recent years the LGFB program has reached 43,000 women. A magazine and catalogue called “tlc,” or Tender Loving Care, combines articles and information about products for women coping with cancer treatment (e.g., wigs, mastectomy forms and products, hats and headcoverings, bathing suits, and lingerie) (www.tlccatalog.org, accessed April 15, 2003).
The I Can Cope program started as a series of classes for individuals with cancer, but has been adapted for use for discussion groups and most recently as a Web-based interactive program. The Cancer Survivors Network is an ACS-sponsored website to support online interaction between cancer survivors. Participants can create a personal website, post pictures, poems and other expression, and engage in online discussions in English, Spanish, and Chinese. A health-care navigator program is under development by ACS that will direct individuals to resources within their community.
TABLE 6-6 Selected National Community-Based Psychosocial Resources
|
Program Name, Sponsor |
Services and Availability |
Content of Services |
Patient Eligibility |
|
Reach to Recovery, American Cancer, Society (ACS) |
Available nationwide |
|
Women facing breast cancer diagnosis, patients Self or doctor referral |
|
I Can Cope, ACS |
Available nationwide |
|
Cancer patient and/or family Self or doctor referral |
|
Look Good … Feel Better, ACS, Cosmetic, Toiletry, and Fragrance Association Foundation, and the National Cosmetology Association |
Available nationwide |
|
Patient concerned about appearance-related side effects of cancer |
|
The Wellness Community, Donations from individuals, corporations, or foundations |
Available in 22 locations throughout the U.S. |
|
Cancer patient and/or family |
|
Cancer Care |
Available nationwide by telephone |
|
Cancer patient |
|
Cancer Hope Network |
Available nationwide by telephone, or in person at some locations |
|
Cancer patient |
|
ACOR (Association of Cancer Online Resources) |
Available nationwide via the Internet |
|
Cancer Patient and/or family professionals |
|
Other groups (Y-Me, Bosom Buddies, Sisters Network, YWCA, Circle of Life, TOUCH) |
Available in regions nationwide |
Cancer patient and/or family |
The Wellness Community The Wellness Community, founded in 1982, provides free education and support services to individuals with cancer and their families (see Table 6-6). The founding principle of the Wellness Community is that patients who participate in recovery improve the quality of their lives and may enhance the possibility of recovery. In 2002, 25,000 patients made 150,000 visits to Wellness Community Programs located in 22 sites across the country (Wellness Community Fact Sheet, undated). Among those served were 8,000 women with breast cancer, 3,000 of whom joined support groups (Mitch Golant, workshop presentation, 2002). All programs are facilitated by health care professionals, including social workers, psychotherapists, nurses, and psychologists, and all programs and training curricula are uniform throughout the country. Its newest program, The Virtual Wellness Community, includes online support groups, Webcasts, mind/body exercises, and information (see Figure 6-2). Evaluations of programs are ongoing in collaboration with investigators at Stanford University and the University of California at San Francisco (Lieberman et al., 2003). A comparison of face-to-face and online support services, an examination of provider best practices, and analyses of outcomes associated with interventions are among the research activities that are underway.

FIGURE 6-2 The virtual wellness community.
SOURCE: http://www.thewellnesscommunity.org.
Community-based support targeted to racial and ethnic minority groups A number of psychosocial support programs are targeted to members of racial and ethnic minority groups. La Vida, a program to meet the needs of Hispanic women in the District of Columbia, was described at the October 2002 NCPB workshop. Established in 1996, La Vida offers support groups, crisis intervention, and peer support to breast cancer survivors. Because many women served are poor, uninsured, and speak Spanish, La Vida provides “patient navigation” services to help women make appointments and get appropriate follow-up care, assistance with health insurance applications and claim translation, and social supports (assistance with transportation, babysitting). Support groups focus on stress reduction, education (e.g., nutrition), and the implications of cancer for families. La Vida is creating a national psychosocial support resource directory for Hispanic women with breast cancer. To date, 63 programs have been identified, many in California and New York (Hinestrosa, workshop presentation, October 2002). The most pressing needs of Hispanic women identified by programs surveyed thus far are related to poor access to health care, information, psychosocial support, and difficulties navigating the health care system.
Sister’s Network was founded in 1993 to address the needs of African American women with breast cancer (www.sistersnetworkinc.org, accessed April 15, 2003). The only national African American breast cancer survivors organization in the United States, Sisters Network has 35 affiliate chapters across the country. Over 2,000 members are involved in breast health training, attending conferences, and serving on various national boards and review committees. Chapters offer individual and group support, community education, advocacy, and research-related activities (e.g., promoting access to clinical trials).
Support available by telephone and online Many psychosocial support services are available by phone to residents of rural areas and those living far from cancer centers, and increasingly online through the World-Wide Web. This section of the report describes three such programs: Cancer Care, The Association of Cancer Online Resources (ACOR), and CHESS (Comprehensive Health Enhancement Support System). A new resource is able to help find psychosocial and mental health services: The American Psychosocial Oncology Society (APOS; http://www.aspboa.org/patient/default.asp. There are other organized online lay information and support groups, for example, FertileHope.org, Living Beyond Breast Cancer (lbbc.org), and cancerandcareers.org, and many Internet chat rooms. There are also radio resources, for example, the Group Room weekly cancer talk radio show (and Internet simulcast) provided by Vital Options® International, which could reach those in rural and other distant areas. The potential for these
resources to help survivors and to serve as collaborators in psychosocial care and research is not clear but merits investigation.
Cancer Care Since 1944, Cancer Care has provided emotional support, information, and practical help to people with cancer and their families. This nonprofit social service agency takes calls through its toll-free Counseling Line, sponsors teleconference programs, and provides support services on site in New York and via the Internet (www.cancercare.org, accessed April 15, 2003). All services are provided free of charge. With a staff of more than 50 professional oncology social workers, Cancer Care in 2001 provided services to more than 80,000 people. Among the services provided are individual and family counseling, group counseling (in-person, online, or by telephone), referrals to other resources, direct financial assistance, and teleconference programs which allow people to listen via telephone to experts in oncology or related fields discuss state-of-the-art treatment options, provide coping strategies for side effects, make recommendations on communicating with one’s healthcare team, and offer advice on how best to maintain quality of life while living with cancer. Cancer Care is also involved in professional education and training offering seminars, workshops, and teleconferences in all fields of oncology care. Distance learning programs are conducted entirely on the website.
The Association of Cancer Online Resources (ACOR) ACOR provides opportunities for individuals with cancer to interact with other cancer patients, therapists, or doctors through chat rooms, e-mail, or listserves. Psychosocial support is available through listserves dedicated to breast cancer, cancer-related depression, and caregivers. Another feature of ACOR is the provision of information about cancer from sources deemed to be credible (www.acor.org, accessed April 15, 2003).
CHESS (Comprehensive Health Enhancement Support System) CHESS provides information, social support, and decision-making assistance via a personal computer and modem that are placed in patients’ homes. Women of all ages and varied socioeconomic backgrounds have successfully used the program to become active participants in their care following a diagnosis of breast cancer. CHESS allows participants to talk anonymously with peers, question experts, learn where to obtain help and how to use it, read stories about people who have survived similar crises, read relevant articles, monitor their health status, consider decision options, and plan how to implement decisions (Gustafson et al., 1993; Shaw et al., 2000). Support group use is the most popular aspect of CHESS. CHESS support groups are monitored by a facilitator. Several major medical centers and health plans are involved in CHESS research dissemination (http://chess.chsra.wisc.edu/chess/consortium/consortium_members.htm, accessed April 15, 2003).
American Psychosocial Oncology Society (APOS) Members of APOS include professionals from all disciplines who are involved in providing
psychosocial and mental health services for cancer patients and their families. Established in 1986, APOS has recently addressed the information gap for patients whose psychosocial needs are not met by the services of the advocacy organizations and who are in need of more formal mental health services. The APOS Referral Directory (available online at www.apos-society.org, accessed April 15, 2003) and their toll-free number (1-866-APOS-4-HELP) provide patients and their families with information about qualified professionals with skills in psycho-oncology and who are located in their community. In addition, APOS offers a core curriculum in psycho-oncology, free online, to professionals who wish to ensure their basic skills in the psychosocial care of patients. APOS presently serves as backup to Cancer Care, The Wellness Community, and the National Coalition of Cancer Survivors (NCCS).
SUMMARY
Advances in breast cancer diagnosis and care have changed the composition of women with breast cancer and the way in which they receive care. Widespread use of mammography has, for example, led to women being diagnosed at younger ages, which likely has increased the need for psychosocial services because younger people, in general, report higher rates of mental problems, and their mental health service use tends to be high.
There have been dramatic shifts in the site of breast cancer care, from the hospital to outpatient settings, making access to psychosocial support services more difficult because psychologists, social workers, and nurses, the mainstays of psychosocial care, are usually based in hospitals. While evidence is limited, it appears unlikely that most women with breast cancer receive hospital care of any duration. There are only about 150,000 hospitalizations for breast cancer each year, with two-thirds of these hospitalizations for mastectomies. And among women hospitalized for breast cancer care, relatively few stay in the hospital longer than 2 days.
Most contemporary breast cancer care takes place during nearly 5 million ambulatory care visits made annually, most of these to private physicians’ offices. Here, only 5 percent of breast cancer-related visits include psychosocial care. Contact with nurses who might be expected to provide some supportive care appears to be limited during visits to physicians’ offices, with fewer than 40 percent of visits bringing women seeking breast cancer care into contact with a registered nurse, nurse practitioner, or physician assistant.
Use of psychosocial services may be limited because the delivery of breast cancer care has become so complex, involving multiple treatment modalities and providers. As women go from office to office for consultation and treatment, there may be no coordinator of care and no one respon-
sible for making the patient aware of psychosocial services that are available. Comprehensive breast centers have emerged that put providers and services “under one roof,” but there are no estimates of the number of women receiving care in these settings.
The involvement of oncology providers in post-treatment follow-up care has been questioned by findings, largely outside the United States, that specialized surveillance has no benefit for survival or patient satisfaction. Long term follow-up of women with breast cancer may eventually move to the hands of primary care providers, who may not have extensive experience in cancer-related psychosocial issues or the expected long-term treatment effects with psychosocial consequences.
Collaborative practice is a promising approach to providing psychosocial services to the vast majority of women with breast cancer who receive their care in ambulatory care settings. This approach involves integrating a psychologist (usually in private practice) into the outpatient oncology practice team; however, current reimbursement for mental health services cannot fully support a salary for such a person. Managed care programs that improve satisfaction with breast cancer care by enhancing educational materials and supportive care also show promise. Although a minority of women appear to be getting breast cancer care in hospital-based settings, these programs are important sites of training and research. Many hospital-based programs have standards in place to assure the provision of at least some level of psychosocial support. Hospital-based programs, however, even at comprehensive cancer centers appear to have unstable support for their programs, relying extensively on philanthropy and volunteer staff.
There are many free, community-based psychosocial programs available and increasingly services are accessible by telephone and the Internet. Little is known regarding their use, and few have been formally evaluated. There are few estimates with which to gauge how often women with breast cancer use psychosocial services, but generally use appears to be low, with up to 30 percent of women reporting some level of service. Psychosocial service use seems to decline into the survivorship period, with some studies suggesting that between 10 and 15 percent of long-term breast cancer survivors use psychosocial services.
REFERENCES
American Cancer Society. 2001. Breast Cancer Facts & Figures 2001–2002. Atlanta: American Cancer Society.
American Cancer Society. 2002. Cancer Facts & Figures 2002. Atlanta: American Cancer Society.
Case C, Johantgen M, Steiner C. 2001. Outpatient mastectomy: Clinical, payer, and geographic influences. Health Serv Res 36(5):869–884.
Coluzzi PH, Grant M, Doroshow JH, Rhiner M, Ferrell B, Rivera L. 1995. Survey of the provision of supportive care services at National Cancer Institute-designated cancer centers. J Clin Oncol 13(3):756–764.
Curry C, Cossich T, Matthews JP, Beresford J, McLachlan SA. 2002. Uptake of psychosocial referrals in an outpatient cancer setting: Improving service accessibility via the referral process. Support Care Cancer 10(7):549–555.
Donaldson MS. 1998. Accountability for quality in managed care. Jt Comm J Qual Improv 24(12):711–725.
Ferrell BR, Grant MM, Funk BM, Otis-Green SA, Garcia NJ. 1998. Quality of life in breast cancer survivors: Implications for developing support services. Oncol Nurs Forum 25(5):887–895.
Frost MH, Arvizu RD, Jayakumar S, Schoonover A, Novotny P, Zahasky K. 1999. A multidisciplinary healthcare delivery model for women with breast cancer: Patient satisfaction and physical and psychosocial adjustment. Oncol Nurs Forum 26(10):1673–1680.
Ganz PA, Desmond KA, Leedham B, Rowland JH, Meyerowitz BE, Belin TR. 2002. Quality of life in long-term, disease-free survivors of breast cancer: A follow-up study. J Natl Cancer Inst 94(1):39–49.
Geiger AM, Mullen ES, Sloman PA, Edgerton BW, Petitti DB. 2000. Evaluation of a breast cancer patient information and support program. Eff Clin Pract 3(4):157–165.
Gruman J, Convissor R. 1995. Psychosocial Services in Cancer Care: A Survey of Comprehensive Cancer Centers. Washington, DC: The Center for the Advancement of Health.
Grunfeld E, Fitzpatrick R, Mant D, Yudkin P, Adewuyi-Dalton R, Stewart J, Cole D, Vessey M. 1999. Comparison of breast cancer patient satisfaction with follow-up in primary care versus specialist care: Results from a randomized controlled trial. Br J Gen Pract 49(446):705–710.
Grunfeld E, Mant D, Yudkin P, Adewuyi-Dalton R, Cole D, Stewart J, Fitzpatrick R, Vessey M. 1996. Routine follow up of breast cancer in primary care: Randomised trial. Br Med J 313(7058):665–669.
Gustafson D, Wise M, McTavish F, Taylor J, Wolberg W, Steward J, Smalley R, Bosworth K. 1993. Development and pilot evaluation of a computer-based support system for women with breast cancer. Journal of Psychosocial Oncology 11(4):69–93.
Hewitt M, Breen N, Devesa S. 1999. Cancer prevalence and survivorship issues: Analyses of the 1992 National Health Interview Survey. J Natl Cancer Inst 91(17):1480–1486.
Hewitt M, Rowland JH. 2002. Mental health service use among adult cancer survivors: Analyses of the National Health Interview Survey. J Clin Oncol 20(23):4581–4590.
Landon BE, Wilson IB, Cleary PD. 1998. A conceptual model of the effects of health care organizations on the quality of medical care. JAMA 279(17):1377–1382.
Lerner BH. 2001.The Breast Cancer Wars: Hope, Fear, and the Pursuit of a Cure in Twentieth-Century America. New York: Oxford University Press.
Lieberman MA, Golant M, Giese-Davis J et al. 2003. Electronic support groups for breast carcinoma: A clinical trial of effectiveness. Cancer 97(4):920–925.
McQuellon RP, Hurt GJ, DeChatelet P. 1996. Psychosocial care of the patient with cancer: A model for organizing services. Cancer Practice 4(6):304–311.
National Breast Cancer Coalition. 2002. Guide to Quality Breast Cancer Care. 2nd ed. Washington, DC: National Breast Cancer Coalition.
Plass A, Koch U. 2001. Participation of oncological outpatients in psychosocial support. Psycho-Oncology 10(6):511–520.
Presberg BA, Levenson JL. 1993. A survey of cancer support groups provided by National Cancer Institute (NCI) clinical and comprehensive centers. Psycho-Oncology 2:215–217.
Rabinowitz B. 2002. Psychosocial issues in breast cancer. Obstet Gynecol Clin North Am 29(1):233–247.
Rosselli Del Turco M, Palli D, Cariddi A, Ciatto S, Pacini P, Distante V. 1994. Intensive diagnostic follow-up after treatment of primary breast cancer. A randomized trial. National Research Council Project on Breast Cancer follow-up. JAMA 271(20):1593–1597.
Shaw BR, McTavish F, Hawkins R, Gustafson DH, Pingree S. 2000. Experiences of women with breast cancer: Exchanging social support over the CHESS computer network. J Health Commun 5(2):135–159.
Simmons J. 1998. AAHP identifies best practices for breast cancer. Qual Lett Healthc Lead 10(9):13–14.
Sorensen M, Liu ET. 1995 With a different voice: Integrating the psychosocial perspective into routine oncology care. Breast Cancer Res Treat 35(1):39–42.
Tesauro GM, Rowland JH, Lustig C. 2002. Survivorship resources for post-treatment cancer survivors. Cancer Pract 10(6):277–283.
The GIVIO Investigators. 1994. Impact of follow-up testing on survival and health-related quality of life in breast cancer patients. A multicenter randomized controlled trial. JAMA 271(20):1587–1592.
Trief PM, Donohue-Smith M. 1996. Counseling needs of women with breast cancer: What the women tell us. J Psychosoc Nurs Ment Health Serv 34(5):24–29.































