Meeting Psychosocial Needs of Women with Breast Cancer (2004)
Chapter: 3 Psychosocial Needs of Women with Breast Cancer
3
Psychosocial Needs of Women with Breast Cancer
Most women experience at least some psychosocial distress during the course of their breast cancer diagnosis and treatment. The level of distress varies from woman to woman and, within an individual, over the course of diagnosis and treatment. Cancer-related distress can be expected to dissipate with time for the majority of individuals diagnosed with cancer. For others, however, such distress may interfere substantially with comfort, quality of life, and the ability to make appropriate treatment decisions and adhere to treatment (Irvine et al., 1991; Massie and Holland, 1991). Psychosocial distress can be related to physical problems like illness or disability, psychological problems, and family issues and social concerns such as those related to employment, insurance, and supportive care access.
The frequency and patterns of psychosocial distress that occur among women with breast cancer depend greatly on which concerns are included in the operational definition of distress and how it is measured. However, most of the literature on the psychosocial aspects of breast cancer suggests that the vast majority of women adjust well to the diagnosis of breast cancer and manage the complex and sometimes aggressive treatments associated with primary treatment and recurrent disease (Bloom et al., 1987; Frost et al., 2000; Ganz et al., 1996, 1998a, 2002; Maunsell et al., 1992; Schag et al., 1993). Recent studies that have examined quality of life and depression among disease-free breast cancer survivors using standardized instruments with norms available from the general population suggest high levels of functioning in the early and later years after primary treatment (Dorval et al., 1998; Ganz et al., 1996, 1998a, 2002). Even for women with recur-
rence of breast cancer, psychological well-being is often maintained (Bull et al., 1999; Frost et al., 2000; Ganz et al., 2002). For a minority of women however, a diagnosis of breast cancer contributes to significant psychosocial distress that can interfere with functioning and well-being. Assessing the factors that contribute to resilience, effective coping with cancer, and positive psychological outcomes associated with the cancer experience is of increasing interest to researchers (Brennan, 2001; Cordova et al., 2001; Justice, 1999; Petrie et al., 1999; Tomich and Helgeson, 2002), and some of these studies show reductions in the need for medical visits with benefit finding (Stanton et al., 2002) (see section on Measuring Psychosocial Distress). This chapter reviews some of the psychosocial concerns that have been described among women at various points along the disease continuum.1 Estimates of the prevalence of psychosocial distress are then presented. The chapter concludes with a discussion of risk factors associated with psychosocial distress and methods that are available to identify women who are distressed and who may benefit from intervention.
PSYCHOSOCIAL NEEDS OF WOMEN BY PHASE OF CARE
Some of the most common psychosocial concerns reported by women with breast cancer include:
Fear of recurrence,
Physical symptoms such as fatigue, trouble sleeping, or pain,
Body image disruption,
Sexual dysfunction,
Treatment-related anxieties,
Intrusive thoughts about illness/persistent anxiety,
Marital/partner communication,
Feelings of vulnerability, and
Existential concerns2 regarding mortality.
To some degree, these concerns are expected and are experienced by all women at some point after their diagnosis and treatment for breast cancer. There is variation, however, in the extent to which women accept these concerns, cope with them, and adapt to living with a degree of uncertainty about the future. Some women live in a state of persistent rumination about the illness and are overwhelmed with concerns about the inability to control what
will happen. Effective strategies for enhancing coping are actively being studied by many research groups. For most women with breast cancer, coping strategies focusing on realistic expectations can facilitate the adaptation to the illness that occurs over time. For certain women, however, adaptation and coping may be extremely difficult and intervention may be needed.
The breast cancer experience has several distinct phases, each characterized by a unique set of psychosocial concerns. These phases coincide with aspects of the clinical course of the illness and related treatments. What follows is a review of the distinctive psychosocial needs associated with diagnosis, primary treatment, the special issues related to non-invasive breast cancer, completing treatment and re-entry to usual living, survivorship, recurrence, and palliation for advanced cancer. Oncology and primary care practitioners must be prepared for the range of psychosocial issues that may arise among their patients who are at various points along the breast cancer treatment continuum. The psychosocial impact of breast cancer must also be understood in the context of other issues that affect women’s coping, quality of life, and well-being, such as socioeconomic factors and cultural factors, the availability of social support, access to health care, and the presence of other chronic illness or life crises.
Diagnosis
Although women clearly vary in their responses, most who are told that they have a diagnosis of breast cancer acutely experience fear and disbelief. Prior to being diagnosed with cancer, most do not perceive themselves to be at higher than usual risk for the disease, in part, because most often (about 75 to 80 percent of cases) there is no family history of breast cancer. Although unprepared for this event, once the diagnosis has been made they nevertheless face an array of medical consultants and the necessity to make crucial treatment decisions. The first few days and weeks after a biopsy will involve further evaluation to determine the stage of the disease and the prognosis, largely based on tumor characteristics (e.g., size, histology, hormone receptor status, nodal involvement). The results of these predictive and prognostic factors performed on the primary tumor can be difficult for physicians to interpret and are frequently confusing to patients as well. Decisions about type of surgery (mastectomy, mastectomy with reconstruction, lumpectomy), subsequent adjuvant therapy (standard vs. investigational), and radiation therapy, and even where to have treatments performed (which hospital and which specialists) can be challenging. Suddenly, the woman must deal with vital issues about which she usually has little knowledge and background, and she must choose a medical team to provide and coordinate her care. Second opinions are often helpful during this process (Clauson et al., 2002), and it is inadvisable for a woman to make hasty medical decisions that she might later regret (reviewed in Rowland and Massie, 1998).
However, women do not always share fully in the decision about treatment choices (Chou, 2002). Some women rely on their physicians to make the decision and in some settings, like HMOs, women are not routinely included in the decision-making process. A recent dissertation (Chou, 2002) found that when women did participate in treatment decision making to the extent they wanted, they chose more conservative options (breast-conserving surgery plus radiation therapy) than when they did not participate as fully as they would have liked.
A concern during this phase is information overload for the patient and her support system (spouse, family, and friends). The medical care team often sees the complexities of decision making around breast cancer treatments as being routine, but for the woman, the presentation of treatment options (e.g., mastectomy versus lumpectomy; adjuvant chemotherapy or not) is far from routine. There are two extremes of responses in this situation: she may rush to treatment because of anxiety and concern that the cancer must be taken care of immediately, or she may have difficulty in making a decision, thereby creating a substantial delay while obtaining second, third, and fourth opinions (reviewed in Rowland and Massie, 1998).
Treatment
Primary Treatment
Once the treatment plan is decided, women with breast cancer may experience some relief of anxiety and distress, but new fears may arise in anticipating and receiving the planned treatment. Surgery, particularly lumpectomy and axillary dissection, is often done as an outpatient or short stay procedure. Even the length of hospital stay for mastectomy has been shortened from what it was just a few years ago (see also Chapter 6). This means that someone must be available to assist the woman at home, particularly with household tasks or other activities that require arm mobility) and some nursing care (e.g., management of surgical drains and dressings). Women undergoing mastectomy and immediate reconstruction, especially with soft tissue flaps from the abdomen, will have longer hospitalizations and a more protracted recovery from surgery. A woman needs to be prepared for what to expect with each of these procedures, and such preparation is important for her psychological well-being and recovery (Wickman, 1995). Extensive reviews of the safety of breast implants and specific information for women about this have recently been completed (Bondurant et al., 1999; Griff et al., 2000) and should reassure women that reconstruction is a reasonable, effective, and safe procedure, although not without some local complications. The psychological issues with women and breast im-
plants and their satisfaction with results were extensively reviewed in the report by Bondurant and colleagues (Bondurant et al., 1999).
Similarly, women benefit from being prepared for the experience of radiation therapy. Many women feel anxiety associated with being in the treatment room “all alone,” while the therapy is being delivered. They must become accustomed to baring their breast and disrobing among technical staff. In addition, the variation in skin reactions, local symptoms, and fatigue associated with 6 weeks of daily radiation therapy all need to be explained to women, so that they understand what to expect as treatment proceeds. It is important for the medical staff to attend to these symptoms when they arise and to provide reassurance about their normalcy and the expected eventual recovery and successful result. Some women electing breast conservation will experience lingering doubts about the comparable efficacy of this treatment approach to mastectomy, and they may need continued support and reassurance about their treatment choice. Finally, the waiting room of the radiation therapy department is sometimes distressing to breast cancer patients, especially when they see patients who are much sicker and are receiving palliative therapy for advanced cancer. Nursing and physician staff should acknowledge these issues and directly address them when breast cancer patients report their concerns about their own health and mortality.
Adjuvant Therapy
There is a wide range of adjuvant therapies—from tamoxifen as a single agent, to complex chemotherapy regimens with or without tamoxifen, to newer hormonal therapies. As new treatments emerge and the latest results of clinical trials presented at scientific meetings are widely publicized, patients have many questions about whether or not to take the standard, established therapies or to elect to take the newer ones for which there is limited or less robust data. Other decisions may focus on whether or not to enter a clinical trial. Many breast cancer patients compare notes with other patients, and often learn that their treatments are different from those of the other women in their support group or in the office waiting room. It is important to reassure women about the varied prognoses of women with breast cancer and that many different treatment strategies can be used for the same stage of disease. It is advisable for a woman to receive as much information and consultation as necessary before embarking on a course of adjuvant treatment. This helps to ensure that she understands the treatments that are most appropriate for her, given her specific medical, personal, and social situation. The process of gathering information is often stressful, but usually leads to better understanding and acceptance of the treatment plan.
Most adjuvant chemotherapy is well tolerated, and women often continue many of their usual activities (childcare, household activities, paid employment) albeit often on a reduced schedule, especially modified by treatment administration. Hair loss, nausea, and vomiting are among the most distressing side effects, followed by fatigue and changes in body image and weight (Shimozuma et al., 1999). The difficulty here is that adjuvant treatment takes someone who is trying to recover physically and psychologically from a diagnosis of cancer and surgery, and adds additional associated physical symptoms for a period of 4 to 6 months. While perceived by most women as a reasonable “insurance policy” against subsequent breast cancer recurrence, adjuvant treatment significantly decreases quality of life while it is being given. Many women have a love–hate relationship with adjuvant treatment, feeling protected by it and even wanting more intensive therapies, but nevertheless feeling distressed and overwhelmed by some of the physical symptoms that they experience while receiving treatment.
Tamoxifen therapy may be used by itself or in combination with adjuvant chemotherapy in some women. While the medical evidence for its benefits in improving survival and preventing breast cancer recurrence is overwhelming, in the eyes of many women it is still seen as a controversial and potentially toxic therapy. Women may be especially concerned about the risk of endometrial cancer, and physicians must directly address the risks and benefits of tamoxifen therapy with each patient. Other frequent concerns of women about tamoxifen relate to psychological well-being, weight gain, hot flashes, and sexual functioning. Many of these problems are common in breast cancer survivors and are not specifically related to the drug tamoxifen (Day et al., 2001, 1999; Fallowfield et al., 2001). In addition, studies with aromatase inhibitors in advanced or adjuvant settings (or even for prevention) suggest that these agents which block estrogen formation, may be an improvement over tamoxifen for breast cancer treatment. Women may wish to have this more recent information and to discuss its implications (Santen, 2003). There are many possibilities in therapy, and women may wish to explore variations consistent with good practice to fit their needs.
Over 70 percent of women become amenorrheic following breast cancer treatment. For younger women who develop breast cancer, amenorrhea is accompanied by a host of hormonal changes either coming on prematurely or intensifying menopausal symptoms in the more mature. These changes are intimately interwoven with psychosocial and behavioral symptoms: mood, anxiety, cognitive impairment, fatigue, and even weight gain. Serotonin reuptake inhibitors are FDA approved for both autonomic and affective symptoms of “pre-menstrual” disorder (late-luteal phase disorder) and for treatment-related menopausal symptoms. Patients often describe cognitive impairment with hormonal treatment or chemotherapy for breast cancer (described in Warga, 2000).
Much of the distress, after the initial shock of diagnosis and adjustment to treatment, is interwoven with decisions that may impede quality of life, and the need to adjust to such physical and emotional changes. Type of surgery, choice of chemotherapy when more than one choice is acceptable, type of radiation therapy (external beam, brachytherapy), and the decision to forgo hormonal suppression are some of the issues that have emotional consequences because they affect anxiety, mood, and stamina.
Non-Invasive Breast Cancer
With the increasing use of screening mammography, the rate of diagnosis of non-invasive ductal carcinoma in situ (DCIS) has increased substantially (see Chapter 2). In some communities, DCIS cases account for as many as 20 percent of the incident cases of breast cancer. Although there are potential benefits of diagnosing an early non-invasive cancer, for many women the anxiety associated with this condition is tremendous. Many women feel confused when they are told that their condition is not serious, yet they receive the same local treatments as women with invasive breast cancer. In spite of the efficacy of local treatment with breast conservation, women with a diagnosis of DCIS face a continuous risk of recurrent disease in the involved breast as well as the contralateral breast. For many younger women, this situation can be very distressing, with the uncertainty and risk labeling which this diagnosis causes. As women with DCIS face menopause, they may struggle, given the results of recent trials of hormone replacement therapy, with whether hormone replacement therapy is safe for menopausal symptom relief given their medical history. This combination of breast cancer risk status and menopausal symptoms can affect quality of life for this unique group of breast cancer patients.
Genetic Risk and Its Psychological Management
An added issue for women with breast cancer is today’s high level of awareness of enhanced genetic risk for daughters and sisters. This adds a burden of guilt and immediately raises the issue of whether genetic testing should be done to determine actual gene status. In addition, genetic testing raises questions about who and what to tell about the results, which could affect health and life insurance coverage; how to deal with children who are minors; and how to advise daughters about risk and surveillance (beginning at what age and with what kind of follow-up?). These issues are well addressed with women today in the major cancer centers, where there are genetic counselors who take a careful medical and psychological history, explain the meaning of the tests, their possible inconclusive information, and offer help in how to decide who to tell about the results. In general,
women appear to handle the information relatively well, whether they are found to be positive or negative. After an initial response of distress with preoccupation with potential bad news, the impact is generally transient and women regain emotional control. However, those testing positive who carry the burden of added risk or recurrence often describe feeling like “walking time bombs” and psychosocial support groups for these women have been found to be helpful in reducing anxiety and distress.
Additional decisions must be made by the woman who is BRCA 1/2 positive about what surveillance she will undertake to reduce her risk and assure an early diagnosis. Regular clinical breast examinations and mammograms are often the chosen route. Control of anxiety and depressed feelings about the genetic risk is important to assure that they adhere to their surveillance program. For some women, however, the level of anxiety (and their perception of risk) is so high that they consider prophylactic bilateral mastectomies. While many consider it, only a small percentage actually go through with it, largely because of an especially high level of risk or a level of anxiety which is intolerable. In most centers, a psychiatric evaluation is done to assure that the woman has a full understanding of the issues and that psychological factors have been taken into account. At Memorial Hospital in New York, Mary Jane Massie, psychiatrist, is requested to evaluate each women preoperatively, and this evaluation is taken into account as a factor in the decision to proceed with surgery.
Decisions about childbearing, in the face of high risk or actual breast cancer, confront many women, and the emotional toll is very high as they contemplate, with knowledgeable oncologists, what course of action they should take. The need for psychological or psychiatric intervention can be very helpful to control anxiety when weighty decisions must be made that will influence future life. Supportive visits and anti-anxiety medication, if needed, should be available for these women (J. Holland, personal communication, September 18, 2003).
Post Treatment
At the end of primary breast cancer treatment—whether it is at the conclusion of 6 weeks of radiation therapy or after 4–6 months of adjuvant chemotherapy—most women experience a mixture of elation, fear, and uncertainty (reviewed in Rowland and Massie, 1998). Although they have mastered the many aspects of their treatment regimen, they have little preparation and information to guide them in their recovery from treatment. This is coupled with their planned discharge from intensive interaction with the health-care system. No longer do they have daily or periodic visits to the treatment center. In fact, they may not have a scheduled return visit for several months after the completion of therapy. In some managed care set-
tings, a woman is referred back to her primary care physician and may have no further contact with the oncology treatment team. During this transition or re-entry period, women may have questions about their symptoms and their care. Who will she talk to about the non-specific joint pains that are bothering her, or the fatigue and difficulty sleeping she is still experiencing? Could these be signs of recurrence? Why is she still experiencing so much fatigue when her treatments ended several weeks ago? Why is her family not paying as much attention to her, and why do they expect life to go back to normal when for her it has been changed forever? The post-treatment transitional period is a time of considerable psychosocial distress. The paradoxical increase in anxiety has been observed at the end of both radiation and systemic chemotherapy (Holland and Rowland, 1991). Nevertheless, many women find positive meaning and describe posttraumatic growth from the cancer experience (Ganz et al., 1996). Nevertheless, fear of recurrence is frequently a dominant emotion that is difficult to control, especially before or during follow-up visits.
There has been growing interest in the late effects of breast cancer treatment and the quality of life of long-term survivors beyond the acute phase of treatment. Several published studies have compared breast cancer survivors to healthy, age-matched populations of women and have found few differences in their long-term physical or emotional well-being (Andersen et al., 1989; Dorval et al., 1998; Ganz et al., 2002, 1998a). A recent study of long-term adjustment of women 20 years after treatment in a large multicenter clinical trial found cancer worries to be negligible; however, 18 percent of women had posttraumatic stress symptoms, and many reported lymphedema (27 percent) and numbness (20 percent) as persistent problems (Kornblith et al., 2003). There is some evidence that women who receive adjuvant therapy may have more physical disruption than those who receive no further therapy, and that women who receive chemotherapy may have more sexual dysfunction and possibly more cognitive dysfunction than survivors who did not receive similar therapy (Ahles et al., 2002; Brezden et al., 2000; Ganz et al., 1999, 2002; Meyerowitz et al., 1999; Schagen et al., 1999; van Dam et al., 1998). With the growing number of breast cancer survivors, as well as increased research funding targeting this population, new evidence will be forthcoming regarding these cognitive and psychosocial concerns (Gotay and Muraoka, 1998).
Recurrence
The overall survival for early stage breast cancer is excellent, and many women can anticipate a normal life expectancy. That is why so much of the patient’s and the medical team’s efforts are invested in primary treatment decisions and the delivery of initial treatment—to ensure the best chance for
long-term disease-free survival and optimal quality of life. However, even under the best of circumstances, a significant number (about 30 to 40 percent overall) of women will experience recurrence of breast cancer, and this can occur many years after the initial breast cancer diagnosis. While shock and disbelief are common emotions at diagnosis, hopefulness and a treatment plan that is expected to lead to long-term disease-free survival usually counter these emotions. In contrast, recurrence of breast cancer is experienced as a failure by both the patient and her treatment team. One recent study of 378 long-term breast cancer survivors showed that many women attribute their disease to stress (42 percent) and a lack of recurrence to having a positive attitude (60 percent) (Stewart et al., 2001). This suggests that many women with breast cancer blame themselves for their disease or its recurrence.
Recurrence is almost always associated with clinical symptoms from the cancer—insidious onset of pain, cough, or the development of skin nodules, for example. The clinical symptoms of recurrence provide tangible evidence of the seriousness of the situation, and the emotions that had been elicited at the time of diagnosis tend to recur and are intensified, particularly with respect to depressive symptoms. This is often a challenging time for the patient, her family, and the treatment team. In a recent study, significant impairments in physical, functional, and emotional well-being were found among women with recurrent breast cancer, and family members reported significant impairments in their own emotional well-being (Northouse et al., 2002).
Recurrence can be local, treated with combinations of excision, radiation, and chemotherapy, depending on individual circumstances. Systemic recurrence can be treated to prolong survival and enhance quality of life, but cannot be cured, so treatments with minimal toxicity are preferred. These medical circumstances have psychosocial implications and given the frequency of recurrence deserve continued research attention (NCCN, 2000:46).
Nevertheless, women who faced initial aggressive treatments are often unwilling to accept less intensive treatments at recurrence. In the 1990s many women sought high-dose chemotherapy programs in spite of insufficient evidence for efficacy. Often this occurred because these women were reluctant to contemplate long-term and unending therapies. They saw intensive, time-limited, “potentially curative” therapies as an alternative. To some extent, this approach fulfilled a psychological need to gain some control over a situation that felt out of control. Physicians often shared in this misconception regarding treatments that were unproven. For many of these women, taking an action, obtaining second opinions, and seeking experimental therapies became the focus of their efforts when they faced metastatic breast cancer. Today, many women are beginning to view recurrent
breast cancer as a chronic condition that can be controlled long-term, even if it cannot be cured. The comparison to the control of diabetes is often helpful. Awareness of second- and third-line therapies for recurrent disease makes this concept more plausible. Women may reach their decisions either on the advice of their physician or by sharing in decision making in various ways (Chou, 2003)
Advanced Breast Cancer
Attention to the symptomatic and pain relief needs of the woman with advanced breast cancer is central to her emotional and physical well-being (Massie and Holland, 1992). The management of pain syndromes, including post-mastectomy pain syndrome, was well described in the 1980s by Foley (1985). The early study of Spiegel and Bloom (Spiegel and Bloom, 1983) documented interventions to reduce distress and pain in metastatic breast cancer. Breitbart and colleagues (Breitbart et al., 2000) have shown the association of pain and the increase in symptoms of depression and anxiety. A biopsychosocial model, illustrating the interplay of somatic (pain) with psychosocial aspects was outlined by Syrjala and Chapko (Syrjala and Chapko, 1995). In the presence of uncontrolled pain, the woman with breast cancer will function at a lower level and will likely become less able to maintain her usual social role as mother, spouse, worker, or caretaker, although many women continue their normal activities in the face of major functional impairments. Concern for spiritual and existential matters often marks this phase of the illness, as women focus on their legacy to their families and children and engage in planning for their future (Butler et al., 2003, Foley, 2000, McGuire et al., 1989).
PREVALENCE OF PSYCHOSOCIAL DISTRESS
An estimated one-third to one-half of individuals diagnosed with any type of cancer experience significant levels of distress (Derogatis et al., 1983; Zabora et al., 2001a). Distress varies by cancer site. According to one study conducted at the Johns Hopkins Cancer Center, individuals diagnosed with cancers known to be associated with the highest mortality and poorest prognosis (e.g., cancers of the lung, pancreas, and brain) had greater levels of distress than individuals with cancer associated with more favorable prognoses (e.g., cancers of the breast, colon, and prostate) (Zabora et al., 2001a) (study results shown in Table 3-1). Other predictors of distress were younger age, fewer social supports, and lower socioeconomic level.
Estimates of the prevalence of psychosocial distress among women with breast cancer depend on how distress is defined and measured. Some estimates are based on a diagnosis of mental disorder as determined by a psy-
TABLE 3-1 Prevalence of Distress by Cancer Diagnosis
Cancer Site or Type | Prevalence of Distress (%) |
All cancers | 35.1 |
Lung | 43.4 |
Brain | 42.7 |
Hodgkin’s | 37.8 |
Pancreas | 36.6 |
Lymphoma | 36.0 |
Liver | 35.4 |
Head and neck | 35.1 |
Adenocarcinoma (unknown primary) | 34.9 |
Breast | 32.8 |
Leukemia | 32.7 |
Melanoma | 32.7 |
Colon | 31.6 |
Prostate | 30.5 |
Gynecological | 29.6 |
SOURCE: Adapted from Zabora et al., 2001a. | |
chiatric interview, while others are based on measurement of psychological states using scores from self-administered assessment tools. Many of the prevalence studies of cancer-related psychosocial distress have been conducted among women recruited from cancer centers or major universities, though a minority of cancer patients receive their care in such settings.
A multi-center study published in 1987 by Bloom and colleagues focused on the psychosocial distress of women in the year following breast cancer diagnosis. They were compared to “healthy” women (no present illness), women after cholecystectomy (an operation with less impact on self image), and women who had had a negative breast biopsy. Five cross-sections of women were interviewed at 3-month intervals for the first 12 months post-diagnosis. The earliest cohort was assessed longitudinally. Over 400 women with breast cancer were studied in five centers from 61 hospitals in 11 states. The findings indicated that early distress from breast cancer was dissipated within 1 year following diagnosis so that the group of women with breast cancer did not differ as to distress levels from the women in the other groups. However, among the women who had received adjuvant chemotherapy during the year, levels remained elevated at 1 year (Bloom et al., 1987).
Individuals who agree to participate in research studies may differ from those who choose not to participate. Further complicating estimates of prevalence of cancer-related psychosocial distress is the frequency with
which psychiatric problems occur among the general population (Massie and Holland, 1989; Rowland, 1999). A study by Morris and colleagues (Morris et al., 1977) found that women who were depressed prior to breast cancer were depressed in the period following diagnosis. Many studies assess psychosocial distress within a group of cancer patients without examining a control or comparison group. Prevalence estimates also vary by the reference period used. Some studies report psychosocial distress within a year (1-year prevalence), while others report distress at a point in time (point prevalence). Studies of psychosocial distress have usually been conducted among patients with recently diagnosed cancer. Increasingly, however, researchers are beginning to assess the psychosocial adjustment of cancer survivors who have lived with cancer for many years.
This section reviews what is known about the prevalence of psychiatric morbidity in the general population, the definition of cancer-related psychosocial distress, and methods to measure the prevalence of psychosocial distress among individuals with breast cancer.
Prevalence of Psychiatric Morbidity in the General Population
Estimates of the prevalence of mental disorders in the United States come from two large community surveys, the National Institute of Mental Health Epidemiologic Catchment Area Program (ECA) and the National Comorbidity Survey (NCS) (Box 3-1) (Kessler et al., 1994; Regier et al., 1984). Although the studies differed somewhat in methodology, they concluded that overall 1-year mental and addictive disorder prevalence rates in the United States approach 30 percent.3
Further analyses of data from these studies, limiting prevalent cases to those whose symptoms were clinically significant, reduced the prevalence of mental or substance use disorder to 18.5 percent (see Table 3-2) (Narrow et al., 2002). Clinically significant cases were symptomatic individuals who: (1) had mentioned their symptoms to a doctor or other professional, (2) had symptoms that interfered with their everyday life, or (3) took medication for symptoms. Of note is the higher prevalence of clinically significant mental and substance use disorders among younger individuals between 18 to 54 years of age. Anxiety, phobia, mood disorder, and depression are among the most common clinically significant mental disorders in the general adult population.
Relatively high rates of psychiatric morbidity, especially depression, have been foud among individuals with chronic medical conditions (Evans et al., 1996–1997; Katon and Ciechanowski, 2002; Katon and Schulberg, 1992; Krishnan et al., 2002; Musselman et al., 1998; Nemeroff et al., 1998). Ac-
BOX 3-1 National Institute of Mental Health Epidemiologic Catchment Area Program (ECA) The ECA was conducted from 1980 to 1985 in 5 sites, and included 18,571 household and 2,290 institutional residents 18 years and older. Two face-to-face interviews were conducted 12 months apart. Diagnostic and Statistical Manual of Mental Disorder (DSM-III) psychiatric diagnoses were assessed with the Diagnostic Interview Schedule (DIS). National Comorbidity Survey (NCS) The NCS was a cross-sectional survey of a nationally representative household sample of 8,098 adolescents and adults aged 15 to 54 years, conducted from 1990 to 1992. The University of Michigan version of the Composite International Diagnostic Interview (UM-CIDI) was used to obtain DSM-III-R diagnoses. Generalized anxiety disorder and post-traumatic stress disorder were assessed only in the NCS. Obsessive-compulsive disorder, anorexia nervosa, somatization disorder, and cognitive impairment were assessed only in the ECA. SOURCE: Narrow et al., 2002. |
cording to one recent review, approximately half of patients with Parkinson’s disease or Alzheimer’s disease have major depression and one in five patients have depression at the time of diagnostic catheterization following acute myocardial infarction or following stroke (Krishnan et al., 2002).
Prevalence of Psychiatric Morbidity Among Individuals with Cancer
An oncologist or other health-care provider seeing a patient with cancer for the first time should reasonably assume that the patient has the same baseline risk of mental and substance use disorders as an age-sex counterpart in the general population, plus the additional risk introduced by cancer and its treatment. What evidence is there that individuals with cancer have higher rates of mental disorders? One of the first studies reporting relatively high rates of psychiatric disorder among cancer patients was conducted by Derogatis and colleagues (Derogatis et al., 1983). As part of their study, 215 cancer patients, randomly selected from new admissions to three collaborating cancer centers, were evaluated by psychiatrists and psychologists using a formal psychiatric interview along with
TABLE 3-2 Estimates of the 1-Year Prevalence of Mental Disorder in the United States, adjusted for clinical significance
patient self-report assessments. Patients terminally ill or who were very disabled were excluded from the study. Roughly half of the patients had breast cancer, lung cancer, or lymphoma with the remainder having other types of cancer. Almost half (47 percent) of the patients had psychological symptoms consistent with a psychiatric disorder (Diagnostic and Statistical Manual of Mental Disorder, DSM-III)4 which was primarily (85 percent) Adjustment Disorder with symptoms of reactive anxiety, depression, or a mix of both. Men and women were equally likely to receive a psychiatric diagnosis. Of note was the variation in prevalence across the three study sites: 24 percent in Baltimore (Johns Hopkins Medical Institution), 46 percent in Rochester (University of Rochester Medical Center), and 69 percent in New York (Memorial Sloan-Kettering Cancer Center). This may reflect differences in interview technique, interpretation of diagnostic
criteria or, more likely, differences in the patients seeking care at each center. In general, patients with an Adjustment Disorder respond to psychological counseling, psychotherapy, and at times, medication, for the control of sleep disturbance, anxiety, and depressive symptoms.
A recent report from the Agency for Healthcare Research and Quality (AHRQ), “Management of Cancer Symptoms: Pain, Depression, and Fatigue,” concluded that major depression and depressive symptoms occur frequently in cancer patients. According to their review of the literature, prevalence rates varied from 10 to 25 percent for major depressive disorders, a rate at least four times higher than in the general population (Agency for Healthcare Research and Quality, 2002). The timing of the assessment, concurrent treatment, medical morbidity, pain, gender, and age of subjects contributed to the wide range of estimates. The higher rates are usually seen in patients with more advanced illness and uncontrolled pain or other physical symptoms. Included in this spectrum of depressive disorders among patients with cancer is the DSM-IV diagnosis of Mood Disorder Related to Medical Illness, which is common in patients with severe or uncontrolled physical symptoms, especially pain.
Health-Related Quality of Life
Depressive symptoms that may not reach criteria for a DSM diagnosis, and are thus considered subsyndromal depressive symptoms, are far more prevalent in cancer, but they often represent a significant detriment to quality of life. Since the Derogatis study was published in the early 1980s, investigators have developed conceptual models to describe the range of impacts that cancer has on psychological and physical health, functional status, symptoms, and other aspects of life such as family relationships and spiritual or existential concerns. A large body of research has been devoted to conceptualizing and measuring health-related quality of life. Instruments that have emerged from this body of science have provided valid tools to measure social, physical, psychological, and sexual function. Some instruments have been developed with a core to measure overall functional areas and include modules that assess functional problems associated with specific sites of cancer. The EORTC-QLQ developed by Aaronson and Cella’s FACT quality-of-life are both widely used instruments and have been translated into many languages (Aaronson et al., 1993, Cella, 1995; Mandelblatt and Eisenberg, 1995; Montazeri et al., 1996). Other generic tools have been developed for the assessment of distress, psychological problems, or specific psychiatric disorders (e.g., anxiety, depression) among patients with chronic illness or among the general population.
Nevertheless, quality of life remains a less-explored facet of survivors’ lives. Given recent improvement in survival times, this broader concept of psychological health and well-being is becoming more important. Most studies show
that many survivors continue to experience negative effects of cancer or cancer treatment on their lives after primary therapy. These effects include sexual and psychological functioning concerns. Also, some reports have shown positive coping strategies and enhanced quality of life. Additional quality of life studies are needed to understand the needs of longer term survivors and what kinds of support they want (reviewed in Gotay and Muraoka, 1998).
Definition of Psychosocial Distress
According to the DSM-IV, a mental disorder is “a clinically significant behavioral or psychological syndrome or pattern that occurs in an individual and that is associated with present distress (e.g., a painful symptom) or disability (i.e., impairment in one or more important areas of functioning) or with a significantly increased risk of suffering death, pain, disability, or an important loss of freedom” (American Psychiatric Association, 1994: xxi). Individuals with cancer may experience a mental disorder as a result of cancer or treatment, or they may experience an exacerbation of a prior psychiatric disorder (e.g., recurrent depression). Other concerns range from cancer-specific concerns, such as fear of recurrence, to more generalized symptoms of worry, fear of the future, fear of death, trouble sleeping, fatigue, and trouble concentrating. The term “psychosocial distress” has been coined to reflect this broader set of concerns (National Comprehensive Cancer Network, 1999). As conceived, distress is a “multi-factorial unpleasant emotional experience of a psychological (cognitive, behavioral, emotional), social, and/or spiritual nature that may interfere with the ability to cope effectively with cancer, its physical symptoms, and its treatment. Distress extends along a continuum, ranging from common normal feelings of vulnerability, sadness, and fears to problems that can become disabling, such as depression, anxiety, panic, social isolation, and existential and spiritual crisis.” Distress may be experienced as a reaction to the disease and its treatment and also as a result of the consequences of the disease on employment, health insurance, and social functioning including family relationships (Kornblith, 1998; McEvoy and McCorkle, 1990). Breast cancer may, for example, impose an economic hardship because it affects women’s ability to work. In one recent study, the probability of breast cancer survivors working was 10 percentage points less than that for women without breast cancer (Bradley et al., 2002). However, this study found no reduction in hours worked among the women who continued in their jobs.
Measuring Psychosocial Distress
This section describes selected instruments that have been used to measure psychosocial distress in United States women with breast cancer and upon which estimates of the prevalence of psychosocial distress are based.
Among these are two generic instruments (i.e., the Hospital Anxiety and Depression scale (HADS) and the SF-36 of the Medical Outcomes Study) and six cancer-specific instruments:
Brief Symptom Inventory (BSI)
Cancer Rehabilitation Evaluation System (CARES)
Distress Thermometer and Problem List from the National Comprehensive Cancer Network Guidelines for Management of Psychosocial Distress
European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire (QLQ-C30)
Functional Assessment of Cancer Therapy-Breast (FACT-B)
Quality of Life Breast Cancer Instrument
Many of the instruments useful in capturing the various dimensions of psychosocial distress among individuals with cancer attempt to measure what is referred to as health-related quality of life (HRQOL) (Cella, 1995; Mandelblatt and Eisenberg, 1995; Montazeri et al., 1996). HRQOL assessments are self-rated subjective evaluations of health and well-being generally in at least four areas: psychological functioning, physical functioning, social functioning, and symptoms and side effects (Figure 3-1). Aspects of

FIGURE 3-1 Quality of life: conceptual model.
SOURCE: Tchekmedyian et al., 1990.
HRQOL life that predominate in the assessment of psychosocial distress are those related to psychological functioning and social functioning. Health-care providers traditionally measure aspects of physical functioning, symptoms, and side effects.
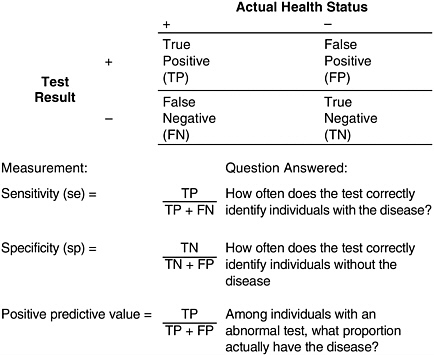
Most of the instruments described in this section were developed for research purposes and were designed to categorize groups of patients as distressed or not. Although the tools meet the needs of researchers, they may not be suitable for use by health-care providers in clinical settings who are interested in evaluating individual patients to determine their need for psychosocial intervention. Instruments developed in research settings need to be carefully evaluated before being used clinically to evaluate patients. An instrument’s validity, in this context its ability to correctly identify the presence and absence of distress, needs to be determined as does its reliability, its ability to provide consistent results. These and other important attributes of clinical screening tools are described in Box 3-2.
While it would be desirable to have well-validated instruments to use as screening tools to help health-care providers identify women who may benefit from psychosocial interventions, not all of the instruments that have been used in research settings have psychometric prerequisites for their use in individual patients and should be considered discriminative instruments only for use with groups of patients (McHorney and Tarlov, 1995). Few of these instruments have actually received rigorous testing with breast cancer patients. The National Cancer Institute (NCI) through its HRQOL Intergroup Committee has recently summarized the use of HRQOL instruments in clinical trials (Trimble et al., 2001). While additional research is needed, some of these instruments hold promise as clinical assessment and screening tools for clinical use (see also Chapter 6).
Hospital Anxiety and Depression Scale (HADS)
One of the most widely used instruments to screen for depression, anxiety, or psychosocial distress in cancer patients, especially in Europe, is the Hospital Anxiety and Depression Scale or HADS (Bjelland et al., 2002; Herrmann, 1997; Zigmond and Snaith, 1983). This tool provides separate scores for anxiety and depression, with cutpoints that have been determined to identify possible mood disorder (Carroll et al., 1993) (see Box 3-3). The HADS has the advantage of being brief, and its items do not overlap with somatic complaints (e.g., fatigue) that may be caused by cancer (Zigmond and Snaith, 1983). The HADS has been used to assess depression and anxiety among women with both early and advanced stage breast cancer. In one study of 211 women with advanced breast cancer, 27 percent were categorized as probable cases of anxiety and/or depression. Among the 155 women who completed an assessment 1 to 3 months later, 13 percent were classified
Yield The yield of a screening test depends on the sensitivity of the test and the prevalence of unrecognized disease. When there are many undiagnosed cases in a population, the yield of a screening test will be high. SOURCE: Mausner et al.,1985. |
BOX 3-3 Doctors are aware that emotions play an important part in most illnesses. If your doctor knows about these feelings he will be able to help you more. This questionnaire is designed to help your doctor to know how you feel. Read each item and underline the reply which comes closest to how you have been feeling in the past week. Don’t take too long over your replies; your immediate reaction to each item will probably be more accurate than a long thought out response.
|
|
as being persistently anxious or depressed (Hopwood et al., 1991a). When investigators compared the classification of 81 of these patients with findings from an independent interview by a psychiatrist, the HADS correctly identified 75 percent of women diagnosed by the psychiatrist. The HADS, however, misclassified 26 percent of “normal” patients as having anxiety or depression. The authors concluded that HADS could be used to screen patients with advanced cancer for affective disorders (Hopwood et al., 1991b).
In a more recent study, HADS classified, at the time of diagnosis, 39 percent of 80 women with metastatic breast cancer as having anxiety and 31 percent as being depressed. When monitored every 8 weeks over a 16-month period, no statistically significant difference in mood was detected over time, although there was a trend for mean anxiety and depression to decrease (Fulton, 1998).
Several investigators have raised questions about the usefulness of the HADS. In one recent Danish study, for example, the prevalence of anxiety and depression as measured by HADS was similar among 538 newly diagnosed breast cancer patients at low risk of recurrence and 872 women randomly selected from the general population (Groenvold et al., 1999). The investigators suggest that the HADS may not be suitable for use in the general population, thereby calling into question the validity of their comparisons. Others have suggested that the HADS is not a sensitive enough instrument, noting that in a study of 266 women with early breast cancer HADS, using the recommended cut point of 11 or greater, identified only 24 percent of women with a clinical diagnosis of anxiety and 14 percent of women with a clinical diagnosis of depression. According to clinical interviews, 50 percent of the women were depressed and 37 percent of women had an anxiety disorder (Hall et al., 1999). Similar concerns were raised in a study of 303 women with early stage breast cancer where the HADS identified only 5 percent of women who were determined to be depressed and 8 percent of women with anxiety. Lowering the cut-off scores for the HADS improved identification (Love et al., 2002).
In addition to these assessments of prevalence and of the value of the screening instrument itself, the HADS has been used to monitor outcomes in a number of psychosocial intervention studies of breast cancer patients (Montazeri et al., 2001; Spiegel et al., 1999). There has been limited use of the HADS in North American clinical practice settings, although its brevity and psychometric properties suggest that it may be very useful. Investigators in the United Kingdom have validated automated screening for psychological distress among hospitalized cancer patients (the study was not limited to women with breast cancer). Responses using computer touchscreens based on the HADS instrument were comparable to those obtained by psychiatric interview (Cull et al., 2001; Velikova et al., 1999). The computerized screening system enabled data to be collected, scored, collated, and reported in real time to identify patients who warranted further clinical assessment.
Other Instruments to Assess Depression and Anxiety
Several instruments have been critical to the characterization of the frequency of anxiety and depression among breast cancer patients participating in research studies (van’t Spijker et al., 1997), but are not yet recommended for use as assessment and screening tools in the clinical setting. These psychological assessment instruments include the General Health Questionnaire (GHQ), the Profile of Mood States (POMS), and the Center for Epidemiologic Studies Depression Scale (CES-D).5 Few of these instruments have been used outside the research setting. Some of these instruments have normative values for the general population making comparisons possible between research subjects and the general population. For example, the expected frequency of depression in the general population using the CES-D (with a cut-point equal to or greater than 17) is 21 percent. The CES-D was used to assess depression among 864 disease-free survivors of breast cancer as part of a large cross-sectional study conducted in two metropolitan areas, Los Angeles and Washington, DC. In this sample, CES-D scores in this range among breast cancer survivors (23 percent) were similar to those observed in the general population (Ganz et al., 1998a). The CES-D has been assessed among women with breast cancer and found to be valid and reliable (Hann et al., 1999).
The Medical Outcomes Study SF-36
The Medical Outcomes Study Short Form (SF-36) was designed for use in clinical practice and research, health policy evaluations, and general
population surveys. The instrument measures eight aspects of functional status, well-being, and self-perceived health (Ware and Sherbourne, 1992):
Functional status
Physical functioning (10 items)
Social functioning (2 items)
Role limitations attributed to physical problems (4 items)
Role limitations attributed to emotional problems (3 items)
Well-being
Mental health (5 items)
Energy and fatigue (4 items)
Pain (2 items)
Overall evaluation of health
General health perception (5 items)6
The SF-36 has been widely used to assess populations with chronic illness (Stewart et al., 1989; Wells et al., 1989), including women with breast cancer and breast cancer survivors (Frost et al., 2000; Ganz et al., 1996; Ganz et al., 1998a). A shorter version, the SF-12, is now available and provides a rapid screen for QoL without providing the greater details from the longer form in terms of the richness of the sub-scale information. The SF-36 was, for example, used as part of the study by Ganz et al. described in the preceding section above. For each of the eight areas of the SF-36 profile, scores for their sample of 864 disease-free survivors of breast cancer were at or above (indicating similar or more positive outcomes) those from the age-matched population norms for healthy women (Figure 3-2) (Ganz et al., 1998a).
The SF-36 was used in a follow-up study of this cohort of 5- to 10-year survivors of breast cancer (Ganz et al., 2002). Among disease-free survivors, physical well-being and emotional well-being were excellent with minimal changes between the baseline and follow-up assessments reflecting expected age-related changes (Figure 3-3). Energy level and social functioning were unchanged. Past systemic adjuvant treatment was, however, associated with poorer functioning on several dimensions of HRQOL. Among women who had experienced a recurrence of cancer, declines in physical and social functioning were observed from baseline to follow-up, but emotional well-being was stable (Figure 3-4).
The mental health items (referred to as the MHI-5) from the SF-36 might have relevance for screening, since general population and chronic

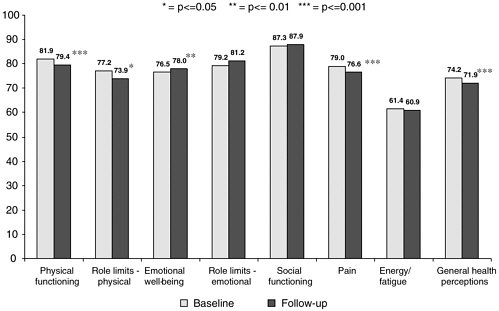

FIGURE 3-4 Baseline and follow-up SF-36 scale scores for 54 patients with recurrence of cancer.
SOURCE: Ganz et al., 2002.
illness norms are available (see Box 3-4) (Ware, 1993). To date the instrument has largely been used for research to characterize groups of patients, including women with breast cancer (Bloom et al., 2000), and not for clinical use for individual patients. Investigators in the United Kingdom tested the use of a computer touchscreen for use in routine oncology practice and found a combination of responses to the MHI-5 and HADS performed best in identifying patients who had been diagnosed through psychiatric interviews as being in need of clinical intervention (Cull et al., 2001; Velikova et al., 1999). This study was conducted among chemotherapy outpatients and was not limited to women with breast cancer.
Brief Symptom Inventory (BSI)
The Brief Symptom Inventory has been used in an early multicenter study of 430 women in the year following initial diagnosis of breast cancer, one cohort of whom was followed longitudinally over 12 months (Bloom et al., 1987). The BSI was able to measure the changes in level of distress over the year as they returned to levels seen in the comparison group of women who had a cholecystectomy, a negative biopsy, or who had no illness in the prior year.
For over a decade the Brief Symptom Inventory (BSI) has been used for psychosocial screening of patients seen at the Johns Hopkins Oncology Cen-
BOX 3-4 During the past 4 weeks, have you had any of the following problems with your work or other regular daily activities as a result of any emotional problems (such as feeling depressed or anxious)?
These questions are about how you feel and how things have been with you during the past 4 weeks. For each question, please give the one answer that comes closest to the way you have been feeling. How much of the time during the past 4 weeks:
NOTE: Items in bold make up the Mental Health Index (MHI-5). SOURCE: Ware and Sherbourne, 1992. |
ter (Derogatis et al., 1983; Zabora et al., 2001a, 1990). Using this approach, patients who are identified as showing distress can then be evaluated in greater detail by a trained social worker or mental health professional. The original BSI instrument includes 53 items in nine areas (Zabora et al., 2001a):
somatization
hostility
anxiety
depression
phobic anxiety
interpersonal sensitivity
obsessive-compulsive
paranoid ideation
psychoticism
The BSI is a 53-item measure of psychological distress written at a sixth-grade reading level requiring 5–7 minutes to complete. For each item, the patient responds in terms of “how they have been feeling during the past 7 days” (Zabora et al., 2001a). Using the BSI, psychosocial distress was identified in 35 percent of cancer patients (n = 4,496) seen at the Johns Hopkins Oncology Center with distress more common among patients with cancers associated with higher mortality and morbidity (Table 3-1) (Zabora et al., 2001a).
A shorter 18-item version of the BSI (BSI-18) has been developed (Zabora et al., 2001b). The BSI-18’s sensitivity, specificity, and positive predictive value—important attributes of a screening test—have been examined to evaluate its usefulness as a screening tool, and were found to be adequate (Zabora et al., 2001b). As Zabora suggests, “these findings are an important step in the development of a prospective psychosocial care delivery system for cancer patients” (Zabora et al., 2001b). Indeed, this important work needs replication and specific evaluation in a breast cancer sample, so that it can be considered as a brief clinical screening instrument.
Cancer Rehabilitation Evaluation System (CARES)
The Cancer Rehabilitation Evaluation System (CARES) instrument was one of the first cancer-specific quality of life instruments whose initial development was influenced by the role it would play in identifying the specific rehabilitation needs of cancer patients (Heinrich et al., 1984; Schag et al., 1991, 1990, 1983).7 Subsequently, Schag and Heinrich (Schag and Heinrich, 1990) developed a computerized report writing program so that the CARES could be used in clinical practice. Two different types of reports are generated: one for health care professionals and the other for the patient/respondent. The CARES has been used by social workers in the Revlon/ UCLA Breast Center’s follow-up clinic to assist in needs assessment, and it
7 | The earliest version of the CARES was called the Cancer Inventory of Problem Situations or CIPS. Drs. Coscarelli Schag, Heinrich, and Ganz began a collaboration in 1980—as part of a randomized group intervention trial for patients with cancer—for which the need to develop an instrument to identify cancer specific needs was conceptualized. The instrument evolved over the subsequent decade and was used in research with diverse cancer patient samples and extensively with breast cancer patients. Although used mainly in these research studies, it has also been adopted by clinicians throughout the country in various clinical settings. Unfortunately, there is no widely available database on the clinical experience with the instrument in this setting. |
BOX 3-5 How much does it apply to you in the past 4 weeks?
SOURCE: Ganz, workshop presentation, 2002. |
has been used in other clinical centers throughout the United States, including a study at UCLA of management of menopausal symptoms in women with a history of breast cancer (Ganz et al., 2000). In this study, a nurse practitioner provided a symptom management intervention and used the CARES as an efficient means to identify psychosocial issues of concern to the patient (Ganz et al., 2000). Use of the CARES in this research study closely simulated the way in which the tool should be used in clinical practice, and efficiently facilitated the assessment of these problems for the nurse’s clinical intervention.
Patients complete the CARES by rating problem statements on a 5-point scale ranging from 0 “Not at all” to 4 “Applies very much” during the last month. The instrument contains 139 items, although not all items are rated by every patient (Schag and Heinrich, 1990). Certain subsections apply to some patients and not others. For example, the 9 chemotherapy items are answered only by those patients who have had chemotherapy within the last month. Patients rate a minimum of 93 items and a maximum of 132 items (Box 3-5). It takes approximately 25–30 minutes for patients to complete the full CARES. The CARES is scored into a Global Score, 5 higher order factors referred to as summary scales, or 31 more specific subscales. The 5 higher order summary scales represent the following domains:
Physical: the physical changes and disruption of daily activity caused by the disease
Psychosocial: psychological issues, communication, relationship (other than partners) problems
Medical Interaction: problems interacting and communicating with the medical team
Marital: problems associated with any marital or marital-type relationship
Sexual: problems related to interest and performance of sexual activity
The Global Score takes into consideration the varying number of possible problems for each patient and in addition has demonstrated its validity as a measure of quality of life (Ganz et al., 1990; Schag et al., 1990). The CARES Global Score and Summary Scales have also been shown to be responsive to change over time in patients with breast cancer (Ganz et al., 1992b, 1992), and in one study the CARES Psychosocial Summary Score administered shortly after diagnosis of breast cancer was helpful in classifying women at subsequent risk for psychosocial distress in the year after breast cancer (Ganz et al., 1993). In another study, women determined to be at risk by a clinical social worker had significantly more problems with greater severity than the low-risk women in all areas measured in CARES (Schag et al., 1993). A short form of CARES was incorporated into the Foundation for Accountability (FACCT) quality measures for breast cancer (Foundation for Accountability, 1997). These measures were developed for health plans and other health-care organizations to assess the quality of several dimensions of care, including the experience of disease (see also Chapter 6).
The CARES has two forms: one for research and one for clinical use. On the clinical form, there is an extra column where the respondent can indicate whether or not she “wants help” with a problem. In addition, the CARES Scoring Manual provides normative data on samples of women with breast cancer so that one can determine where an individual patient scores in comparison to normative values. A short-form of the CARES was developed for use in clinical trial settings (Schag et al., 1991).
In one study, CARES was administered to 235 women with breast cancer representing four treatment phases: new diagnosis, undergoing adjuvant therapy, stable disease, and recurrent cancer (Frost et al., 2000). The overall CARES score and 5 subscores are shown in Figure 3-5. Of note are the relatively stable psychosocial scores by phase. Scores in several areas are high across the phases of care indicating problems, especially in terms of sexual functioning.
Distress Thermometer and Problem List
The National Comprehensive Cancer Network (NCCN), Inc., has published guidelines for distress management in clinical practice (NCCN, 2002)

FIGURE 3-5 Influence of disease phase on CARES-SF scores.
SOURCE: Frost et al., 2000.
(see also Chapter 6). They recommend use of the NCCN Distress Thermometer and Problem List that ask patients in the waiting room how distressed they have been during the past week on a scale of 0 to 10 (see Figure 3-6). Accompanying the Distress Thermometer is the Problem List on which patients check the areas of concerns. This can be used by the primary oncology team to determine the particular psychosocial services needed (e.g., mental health, social work, or pastoral counseling). Based on a study in prostate cancer patients (Roth et al., 1998), a score of 5 or greater on the thermometer scale indicated a significant level of distress as assessed by the HADS. The recommendation is that the primary oncology team use 5 or greater as an algorithm to refer a patient for evaluation by a psychosocial professional. This instrument is being further evaluated as part of a 4-center trial to determine appropriate cut-points for screening and to assess levels of functional impairment associated with distress.
This brief screen may be well suited for use in busy oncology clinics because it uses a familiar 0–10 scale that has been successfully used to ask patients about their pain levels. Its administration also provides an opportunity to open a dialogue between patients and their providers about their psychosocial problems.
Needs assessment surveys performed in ambulatory clinics using these screens show that 20–35 percent of patients have significant levels of distress (National Comprehensive Cancer Network, 1999). The sensitivity and specificity have been tested in a three-center study, confirming that a score of 4 to

FIGURE 3-6 The NCCN distress thermometer and problem list.
SOURCE: NCCN Guidelines, 2003.
5 offers maximal sensitivity and specificity (P. Jacobsen, personal communication). While this simple screening approach has appeal, it needs further testing in the clinical setting before it can be accepted for widespread use. Specifically, one would need evaluation of its sensitivity and specificity in breast cancer patients at several points along the disease continuum.
Figure 3-7 shows the NCCN recommended use of the brief screening tool (Distress Thermometer and Problem List) and the clinical assessment by the primary oncology team. A score of 4–5 or greater (moderate to severe) serves as the trigger (algorithm) for referral to psychosocial services.
The European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire (QLQ-C30)
The European Organization for Research and Treatment of Cancer (EORTC) has developed an integrated, modular approach for evaluating the quality of life of individuals with cancer who participate in international clinical trials. The core instrument, the Quality of Life Questionnaire (QLQ-C30), incorporates nine multi-item scales: five functional scales (physical, role,

FIGURE 3-7 Overview of evaluation and treatment process.
SOURCE: NCCN Guidelines, 2003.
cognitive, emotional, and social); three symptom scales (fatigue, pain, and nausea and vomiting); and a global health and quality-of-life scale (Aaronson et al., 1993). The QLQ-30 has been used in evaluations of psychosocial interventions for women with breast cancer, and a breast cancer-specific quality-of-life questionnaire module has been developed, the QLQ-BR23, which consists of 23 items covering symptoms and side effects related to different treatment modalities, body image, sexuality, and future perspective (Curran et al., 1998; McLachlan et al., 1998; Sprangers et al., 1996).
The significance of changes in quality-of-life scores was assessed by comparing the extent of change in EORTC scores over time as patients perceived changes in their physical, emotional, and social functioning and overall quality of life. The magnitude of changes in scores was interpreted as small, moderate, and large on the basis of these comparisons (Osoba et al., 1998).
Investigators in the Netherlands conducted a randomized controlled trial (not limited to breast cancer) to test the effect of administering a computerized version of the QLQ-30 as part of routine practice to patients undergoing palliative chemotherapy (Detmar et al., 2002). Incorporating the assessments in daily clinical oncology practice facilitated the discussion
of quality-of-life issues and heightened physicians’ awareness of their patients’ concerns.
Functional Assessment of Cancer Therapy-Breast (FACT-B)
Functional Assessment of Cancer Therapy-Breast (FACT-B) is a 46-item self-report instrument designed to measure multidimensional quality of life (Brady et al., 1997). There are 27 items in five areas of well-being (physical, social/family, emotional, and functional) that are measured on a 5-point rating scale. An additional 19 items are specific to breast cancer, including items assessing breast cancer-related emotional concerns (e.g., worried about risk of cancer in family members, worried about effects of stress on illness), physical concerns (e.g., feeling short of breath, being bothered by swollen/tender arms), body image, and sexual functioning. The FACT instrument is written at a sixth-grade reading level and has been translated into several languages (Bonomi et al., 1996; Cella et al., 1998; Dapueto et al., 2001; Fumimoto et al., 2001; Yu et al., 2000). The authors report that the instrument is easy to administer, brief, reliable, valid, and sensitive to change and recommend its use in oncology clinical trials and clinical practice (Brady et al., 1997). The FACT-B has been administered to patients attending an ambulatory breast cancer clinic at Dana Farber using a hand-held computer. Scores are tabulated and are available to the oncologist prior to the visit thereby facilitating a discussion of psychosocial concerns (Jane Weeks, personal communication to Jimmie Holland, March 2003).
Quality of Life Breast Cancer Instrument
The Quality of Life Breast Cancer Instrument includes 46-items representing four areas of well-being (physical, psychological, social, and spiritual) (Box 3-6). The instrument can be administered in person or by mail and was designed to be used in both clinical practice and research. The instrument has been subjected to assessments and shows reasonably high levels of reliability and validity (Dow et al., 1996; Ferrell et al., 1996, 1997a, 1997b, 1998a, 1998b).
National Population-Based Surveys
According to estimates from the National Health Interview Survey (NHIS), a population-based household survey conducted by the National Center for Health Statistics, adults with a history of cancer (excluding superficial skin cancer) are more likely than others to report psychological problems (Hewitt et al., 2003). To assess psychological problems, inter-
BOX 3-6 We are interested in knowing how your experience of having cancer affects your Quality of Life. Please answer all of the following questions based on your life at this time. Please circle the number from 0 to 10 that best describes your experiences (scale not shown below): Physical well-being
Psychological well-being
How distressing were the following aspects of your illness and treatment?
|
To what extent are you fearful of:
Social concerns
Spiritual well-being
SOURCE: Ferrell and Grant, undated memo. |
TABLE 3-3 Prevalence of Psychological Problems Among Adult Survivors of Cancer, by Cancer Type, NHIS, United States, 1998–2000
Characteristic | Psychological Problems Percent (SE) |
Total | 5.4 (0.4) |
Site or Type of Cancer by Sex |
|
Breast | 3.6 (0.6) |
Cervix | 9.3 (1.3) |
Prostate | 3.5 (0.8) |
Colon, rectum | 4.0 (1.0) |
Uterus | 6.1 (1.2) |
Melanoma | 5.2 (1.7) |
Larynx, lung, pharynx | 9.2 (2.6) |
Leukemia, lymphoma | 6.2 (1.7) |
Ovary | 9.0 (2.4) |
Other | 5.4 (0.9) |
Male | 4.8 (1.0) |
Female | 6.2 (1.4) |
SOURCE: Hewitt et al., 2003. | |
viewers asked about certain feelings (i.e., at least some of the time feeling sad, nervous, restless or fidgety, hopeless, worthless, or that everything was an effort) and whether such feelings had, in the last 30 days, interfered with their life or activities. Cancer survivors were more likely than others to report that these feelings had interfered with their life or activities a lot (5.4 vs. 2.8 percent), but there were no significant differences in prevalence of mental health problems by cancer type (Table 3-3). Cancer survivors without other chronic illness were twice as likely as individuals without cancer or other chronic illnesses to have psychological problems, after controlling for age, history of other chronic illness, age at interview, sex, race/ethnicity, education, health insurance coverage, and marital status. Survivors of cancer with other chronic conditions were 6 times more likely to have psychological problems (Hewitt et al., 2003).
RISK FACTORS ASSOCIATED WITH PSYCHOSOCIAL DISTRESS
A number of risk factors have been identified that are associated with psychosocial distress among women with breast cancer: younger age, a history of pre-existing depression or psychological distress, other serious comorbid conditions, and inadequate social support (Bloom et al., 1987; Ganz et al., 1993, 1992a; Jemal et al., 2002; Leedham and Ganz, 1999; Maunsell et al.,
1992, 1995; Schag et al., 1993; Schover, 1994; Shimozuma et al., 1999; Wenzel et al., 1999). In contrast, the specific type of breast cancer surgery does not influence the level of distress (Ganz et al., 1993, 1992a, 1998a, 1998b; Maunsell et al., 1989; Rowland et al., 2000). What makes each of these patient characteristics a risk factor for psychosocial distress after breast cancer?
Younger Age
Most breast cancer occurs in women older than 50 years (about 75 percent of cases), thus for women in their 30s and 40s who are diagnosed with breast cancer, this is a relatively uncommon event, and certainly one that is not expected. In addition, breast cancer in younger women is often temporally related to a recent pregnancy or may occur during pregnancy, and these women often have small children to care for at the same time they must deal with a life-threatening disease. For younger women who have not already had their children, the diagnosis and treatment of breast cancer leads to the specter of death, the likelihood of infertility as a result of treatments, and the symptomatic burden of premature menopause in addition to the acute toxicities of radiation and chemotherapy treatments. All of these medical factors contribute to the risk, and often the reality, of greater psychological distress in these younger women and greater stress for younger husbands (Bloom and Kessler, 1994; Northouse, 1994). In particular, amenorrhea and premature menopause with attendant hormonal changes associated with breast cancer treatment can be linked to mood disorders and complaints of cognitive impairment (Warga, 2000) which may be managed in part by a selective serotonin reuptake inhibitor such as fluoxetine. These kinds of issues which confront younger women were the subject of an NCI conference and monograph in which Bloom and Kessler analyzed the data by decade of age as to distress and dysphoria in a large cohort of women described earlier and reported that they were at greater risk (Bloom and Kessler, 1994). In addition, for those women who do not have a spouse or intimate partner, there may be heightened concerns about femininity, attractiveness, reproduction, and future potential for such a relationship after a breast cancer diagnosis (see following section on sexual problems), for example, the effects of mastectomy, although for those with reconstruction the adjustment problems are no more likely than for those with breast-conserving surgery (Schover et al., 1995). Finally, for younger women this is often their first encounter with the health-care system (other than childbirth or minor health conditions), and this adds considerable anxiety. In contrast, older women may have had other medical conditions or operations, or may have cared for loved ones with cancer, thus blunting some of the initial distress with having to face a new illness. On the other hand, they are more apt to be facing losses of family members or spouse, and reduced economic status.
Sexual Problems
Questions about sexual difficulties and intimacy have been recommended as part of the initial evaluation of patients with cancer. Sexual dysfunction is often not identified by the cancer care team, and most patients receive little or no assistance in dealing with the effects that cancer and cancer treatment have on sexual intimacy (McKee and Schover, 2001). Sexual counseling has been recommended both early and continuing through treatment and recovery for those who need it, but is not routinely provided. Brief counseling can be provided by one of the professionals on the cancer care team. A minority of patients will need more intense interventions, which may be provided in reproductive health clinics in major centers through referral from smaller settings. Brief interventions might include education on the impact of cancer treatment on sexual functioning, suggestions on resuming sex comfortably, advice on mitigating effects of physical handicaps, self help on overcoming specific sexual problems such as painful intercourse or a loss of desire, and treatment for estrogen deficiency (McKee and Schover, 2001; Schover, 1999).
Pre-Existing Mental Illness or Psychological Morbidity
Although it appears that cancer, in general, does not heighten the risk for serious depression in women with breast cancer (Lansky et al., 1985; Rowland, 1999), a prior history of depression and the presence of pain and physical limitations are associated with a greater likelihood of depression. An early study (Morris et al., 1977) examined a group of women in the United Kingdom who were attending a clinic because of “breast cancer concerns.” They were followed longitudinally and those who had more distress prior to diagnosis tended to be more distressed when studied later after their diagnosis of breast cancer, confirming the importance of psychological and psychiatric comorbidities as a factor in adaptation to breast cancer. In a prospective study of newly diagnosed breast cancer patients, Maunsell and colleagues found that a history of depression and serious life events in the five years preceding the cancer diagnosis were both predictive of higher levels of distress after breast cancer (Maunsell et al., 1992). It is not surprising that the stress associated with a new cancer diagnosis and its treatment would exacerbate preexisting depression or psychological distress. With the prevalence of clinically significant mental disorders among adults estimated at 15 percent (Narrow et al., 2002), it is to be expected that a group of women with breast cancer will be predisposed to more severe cancer-related distress based on psychological morbidity.
Comorbid Physical Conditions
Several studies have indicated that women with comorbid conditions (e.g., cardiac, pulmonary) or impaired performance status report higher levels of psychological distress after a breast cancer diagnosis (Ganz et al., 1993; Lansky et al., 1985). This appears to be independent of age (Ganz et al., 1993), although the likelihood of greater comorbidity at diagnosis is increased with age (Greenfield et al., 1987). Physical recovery after breast cancer surgery may be impaired in women with greater comorbidity (Lash and Silliman, 2000), and this may contribute to greater psychological distress as well.
Social Support
Social support for the woman with breast cancer includes instrumental support, such as transportation to appointments, preparation of meals, help with activities of daily living, and emotional support, meaning the availability of someone to share one’s fears, feelings, and concerns. Inadequate levels of either of these two forms of social support increase the likelihood of heightened distress. This may be particularly important in patients with advanced breast cancer (Bloom, 1982; Bloom and Spiegel, 1984; Koopman et al., 1998).
SUMMARY
“Psychosocial distress varies along a continuum from the “normal” reactions to the stress of coping with cancer and its treatment, to symptoms so intense that the person experiencing them meets the criteria for a psychiatric disorder, a severe social or family problem, or significant spiritual distress” (National Comprehensive Cancer Network, 1999:113). Most of the United States studies upon which available estimates of psychosocial distress are based have been conducted within research-oriented cancer centers and have focused on psychosocial distress or psychiatric illness within the first few years of treatment. It is generally recognized that mental disorders occur relatively frequently among individuals with cancer. Prevalence rates varied from 10 to 25 percent for major depression and depressive symptoms, a rate at least four times higher than in the general population according to one recent review (Agency for Healthcare Research and Quality, 2002). Very little, however, is known from prospective studies of the prevalence of psychosocial distress at the different points along the disease continuum or how levels of distress vary for any particular individual by phase of disease or treatment. Whether women with breast cancer have higher rates of psychosocial distress than others with cancer is also not
known, although there is some evidence that distress is greater in cancers with poorer prognoses (e.g., Zabora et al., 2001a). The prevalence of psychosocial distress among women with cancer ranges from roughly 20 to 40 percent, with the variation likely accounted for by differences in study populations and differences in assessment tools as reviewed here (for example, Curran et al., 1998; Ferrell et al., 1996, 1997a, 1997b; Frost et al., 2000; Fulton, 1998; Ganz et al., 1992, 1996, 1998a, 2000, 2002; Hall et al., 1999; McLachlan et al., 1998; National Comprehensive Cancer Network, 1999; Sprangers et al., 1996; Zabora et al., 2001a, 2002b) leading to a probable mid-range estimate in the area of 30 percent. Specific concerns that women with breast cancer have at various points along the care continuum have been well documented, for example, shock and disbelief at diagnosis, anxiety and distress during treatment, fear of recurrence, intrusive thoughts about illness following treatment, and existential concerns following recurrence. Factors that appear to predispose women for psychosocial distress include younger age, a history of pre-existing depression or psychological distress, other serious comorbid conditions, and inadequate social support.
REFERENCES
Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, Filiberti A, Flechtner H, Fleishman SB, de Haes JC, et al. 1993. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 85(5):365–376.
Agency for Healthcare Research and Quality. 2002. Management of cancer symptoms: Pain, depression, and fatigue: Summary. Evidence Report/Technology Assessment 61:1–9.
Ahles TA, Saykin AJ, Furstenberg CT, Cole B, Mott LA, Skalla K, Whedon MB, Bivens S, Mitchell T, Greenberg ER, Silberfarb PM. 2002. Neuropsychologic impact of standard-dose systemic chemotherapy in long-term survivors of breast cancer and lymphoma. J Clin Oncol 20(2):485–493.
American Psychiatric Association. 1994. Diagnostic and Statistical Manual of Mental Disorders. Fourth edition. Washington, DC: American Psychiatric Association.
Andersen BL, Anderson B, deProsse C. 1989. Controlled prospective longitudinal study of women with cancer. II. Psychological outcomes. J Consult Clin Psychol 57(6):692–697.
Bjelland I, Dahl AA, Haug TT, Neckelmann D. 2002. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res 52(2):69–77.
Bloom JR. 1982. Social support, accommodation to stress and adjustment to breast cancer. Soc Sci Med 16(14):1329–1338.
Bloom JR, Spiegel D. 1984. The relationship of two dimensions of social support to the psychological well-being and social functioning of women with advanced breast cancer. Soc Sci Med 19(8):831–837.
Bloom, JR, Cook, M, Flamer, DP, et al. 1987. Psychological response to mastectomy. Cancer 59(1):189–196.
Bloom JR, Kessler L. 1994. Risk and timing of counseling and support interventions for younger women with breast cancer. J Natl Cancer Inst Monogr 16:199–206.
Bloom, JR, Stewart, SL, Banks, PB, et al. 2000.General and specific measures of quality of life in young women with breast cancer. In Baum A, Andersen B, ed. Psychosocial Interventions for Cancer. Washington, DC: American Psychological Association. Pp. 37–56.
Bondurant S, Ernster V, Herdman R. 1999. Safety of Silicone Breast Implants. Washington, DC: Institute of Medicine, National Academy Press.
Bonomi AE, Cella DF, Hahn EA, Bjordal K, Sperner-Unterweger B, Gangeri L, Bergman B, Willems-Groot J, Hanquet P, Zittoun R. 1996. Multilingual translation of the Functional Assessment of Cancer Therapy (FACT) quality of life measurement system. Qual Life Res 5(3):309–320.
Bradley CJ, Bednarek HL, Neumark D. 2002. Breast cancer and women’s labor supply. Health Serv Res 37(5):1309–1328.
Brady MJ, Cella DF, Mo F, Bonomi AE, Tulsky DS, Lloyd SR, Deasy S, Cobleigh M, Shiomoto G. 1997. Reliability and validity of the Functional Assessment of Cancer Therapy-Breast quality-of-life instrument. J Clin Oncol 15(3):974–986.
Breitbart W, Rosenfeld B, Pessin H, et al. 2000. Depression, hopelessness, and desire for hastened death in terminally ill patients with cancer. JAMA 284(22):2907-2911.
Brennan J. 2001. Adjustment to cancer—coping or personal transition? Psycho-Oncology 10(1):1–18.
Brezden CB, Phillips KA, Abdolell M, Bunston T, Tannock IF. 2000. Cognitive function in breast cancer patients receiving adjuvant chemotherapy. J Clin Oncol 18(14):2695–2701.
Bull AA, Meyerowitz BE, Hart S, Mosconi P, Apolone G, Liberati A. 1999. Quality of life in women with recurrent breast cancer. Breast Cancer Res Treat 54(1):47–57.
Butler LD, Koopman C, Cordova MJ, et al. 2003. Psychological distress and pain significantly increase before death in metastatic breast cancer patients. Psychsom Med 65(3):416–426.
Carroll BT, Kathol RG, Noyes R Jr, Wald TG, Clamon GH. 1993. Screening for depression and anxiety in cancer patients using the Hospital Anxiety and Depression Scale. Gen Hosp Psychiatry 15(2):69–74.
Cella D, Hernandez L, Bonomi AE, Corona M, Vaquero M, Shiomoto G, Baez L. 1998. Spanish language translation and initial validation of the functional assessment of cancer therapy quality-of-life instrument. Med Care 36(9):1407–1418.
Cella DF. 1995. Methods and problems in measuring quality of life. Support Care Cancer 3(1):11–22.
Chou AF. 2002. Shared Decision Making: The Selection Process of Treatment Options and Resulting Quality of Life Implications for Women with Breast Cancer. University of California, Berkeley, July 2002.
Chou AF. 2003. Shared Decision Making: Predictors of Participation in Women with Breast Cancer. Presented at PAM Conference, Cornell College of Human Ecology. [Online]. Available: http://www.human.cornell.edu/pam/seminars/s03sem/ [accessed September 10, 2003].
Clauson J, Hsieh YC, Acharya S, Redemaker AW, Morrow M. 2002. Results of the Lynn Sage Second-Opinion Program for Local Therapy. Patients with breast carcinoma: Changes in management and determinants of where care is delivered. Cancer 94(4):889–894.
Cordova MJ, Cunningham LL, Carlson CR, Andrykowski MA. 2001. Posttraumatic growth following breast cancer: A controlled comparison study. Health Psychol 20(3):176–85.
Cull A, Gould A, House A, Smith A, Strong V, Velikova G, Wright P, Selby P. 2001. Validating automated screening for psychological distress by means of computer touchscreens for use in routine oncology practice. Br J Cancer 85(12):1842–1849.
Curran D, van Dongen JP, Aaronson NK, Kiebert G, Fentiman IS, Mignolet F, Bartelink H. 1998. Quality of life of early-stage breast cancer patients treated with radical mastectomy or breast-conserving procedures: Results of EORTC Trial 10801. The European Organization for Research and Treatment of Cancer (EORTC), Breast Cancer Co-operative Group (BCCG). Eur J Cancer 34(3):307–314.
Dapueto JJ, Francolino C, Gotta I, Levin R, Alonso I, Barrios E, Afonzo Y, Cambiasso S. 2001. Evaluation of the Functional Assessment of Cancer Therapy-General Questionnaire (FACT-G) in a South American Spanish speaking population. Psycho-Oncology 10(1):88–92.
Day R, Ganz PA, Costantino JP. 2001. Tamoxifen and depression: More evidence from the National Surgical Adjuvant Breast and Bowel Project’s Breast Cancer Prevention (P-1) Randomized Study. J Natl Cancer Inst 93(21):1615–1623.
Day R, Ganz PA, Costantino JP, Cronin WM, Wickerham DL, Fisher B. 1999. Health-related quality of life and tamoxifen in breast cancer prevention: A report from the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Clin Oncol 17(9):2659–2669.
Derogatis LR, Morrow GR, Fetting J, Penman D, Piasetsky S, Schmale AM, Henrichs M, Carnicke CL Jr. 1983. The prevalence of psychiatric disorders among cancer patients. JAMA 249(6):751–757.
Detmar SB, Muller MJ, Schornagel JH, Wever LD, Aaronson NK. 2002. Health-related quality-of-life assessments and patient-physician communication: A randomized controlled trial. JAMA 288(23):3027–3034.
Dorval M, Maunsell E, Deschenes L, Brisson J. 1998. Type of mastectomy and quality of life for long term breast carcinoma survivors. Cancer 83(10):2130–2138.
Dow KH, Ferrell BR, Leigh S, Ly J, Gulasekaram P. 1996. An evaluation of the quality of life among long-term survivors of breast cancer. Breast Cancer Res Treat 39(3):261–273.
Evans DL, Staab J, Ward H, Leserman J, Perkins DO, Golden RN, Petitto JM. 1996–1997. Depression in the medically ill: Management considerations. Depress Anxiety 4(4):199–208 .
Fallowfield L, Fleissig A, Edwards R, West A, Powles TJ, Howell A, Cuzick J. 2001. Tamoxifen for the prevention of breast cancer: Psychosocial impact on women participating in two randomized controlled trials. J Clin Oncol 19(7):1885–1892.
Ferrell BR, Grant M, Funk B, Garcia N, Otis-Green S, Schaffner ML. 1996. Quality of life in breast cancer. Cancer Pract 4(6):331–340.
Ferrell BR, Grant M, Funk B, Otis-Green S, Garcia N. 1997a. Quality of life in breast cancer. I. Physical and social well-being. Cancer Nurs 20(6):398–408.
Ferrell BR, Grant M, Funk B, Otis-Green S, Garcia N. 1998a. Quality of life in breast cancer. II. Psychological and spiritual well-being. Cancer Nurs 21(1):1–9.
Ferrell BR, Grant MM, Funk B, Otis-Green S, Garcia N. 1997b. Quality of life in breast cancer survivors as identified by focus groups. Psycho-Oncology 6(1):13–23.
Ferrell BR, Grant MM, Funk BM, Otis-Green SA, Garcia NJ. 1998b. Quality of life in breast cancer survivors: Implications for developing support services. Oncol Nurs Forum 25(5):887–895.
Foley KM. The treatment of cancer pain. 1985. N Engl J Med 313(2):84–95.
Foley KM. Controlling cancer pain. 2000, Hosp Pract 35(4):101–108.
Foundation for Accountability. 1997. FACCT Quality Measures: Breast Cancer Measurement Specifications (Version 1.0). Portland, OR: Foundation for Accountability.
Frost MH, Suman VJ, Rummans TA, Dose AM, Taylor M, Novotny P, Johnson R, Evans R. 2000. Physical, psychological and social well-being of women with breast cancer: The influence of disease phase. Psycho-Oncology 9(3):221–231.
Fulton C. 1998. The prevalence and detection of psychiatric morbidity in patients with metastatic breast cancer. Eur J Cancer Care (Engl) 7(4):232–239.
Fumimoto H, Kobayashi K, Chang CH, Eremenco S, Fujiki Y, Uemura S, Ohashi Y, Kudoh S. 2001. Cross-cultural validation of an international questionnaire, the General Measure of the Functional Assessment of Cancer Therapy scale (FACT-G), for Japanese. Qual Life Res 10(8):701–709.
Ganz PA, Coscarelli A, Fred C, Kahn B, Polinsky ML, Petersen L. 1996. Breast cancer survivors: Psychosocial concerns and quality of life. Breast Cancer Res Treat 38(2):183–199.
Ganz PA, Desmond KA, Belin TR, Meyerowitz BE, Rowland JH. 1999. Predictors of sexual health in women after a breast cancer diagnosis. J Clin Oncol 17(8):2371–2380.
Ganz PA, Desmond KA, Leedham B, Rowland JH, Meyerowitz BE, Belin TR. 2002. Quality of life in long-term, disease-free survivors of breast cancer: A follow-up study. J Natl Cancer Inst 94(1):39–49.
Ganz PA, Greendale GA, Petersen L, Zibecchi L, Kahn B, Belin TR. 2000. Managing menopausal symptoms in breast cancer survivors: Results of a randomized controlled trial. J Natl Cancer Inst 92(13):1054–1064.
Ganz PA, Hirji K, Sim MS, Schag CA, Fred C, Polinsky ML. 1993. Predicting psychosocial risk in patients with breast cancer. Med Care 31(5):419–431.
Ganz PA, Lee JJ, Sim MS, Polinsky ML, Schag CA. 1992a. Exploring the influence of multiple variables on the relationship of age to quality of life in women with breast cancer. J Clin Epidemiol 45(5):473–485.
Ganz PA, Moinpour CM, Cella DF, Fetting JH. 1992b. Quality-of-life assessment in cancer clinical trials: A status report. J Natl Cancer Inst 84(13):994–995.
Ganz PA, Rowland JH, Desmond K, Meyerowitz BE, Wyatt GE. 1998a. Life after breast cancer: Understanding women’s health-related quality of life and sexual functioning. J Clin Oncol 16(2):501–514.
Ganz PA, Rowland JH, Meyerowitz BE, Desmond KA. 1998b. Impact of different adjuvant therapy strategies on quality of life in breast cancer survivors. Recent Results Cancer Res 152:396–411.
Ganz PA, Schag CA, Cheng HL. 1990. Assessing the quality of life: A study in newly-diagnosed breast cancer patients. J Clin Epidemiol 43(1):75–86.
Ganz PA, Schag CA, Lee JJ, Sim MS. 1992. The CARES: A generic measure of health-related quality of life for patients with cancer. Qual Life Res 1(1):19–29.
Gotay CC, Muraoka MY. 1998. Quality of life in long-term survivors of adult-onset cancers. J Natl Cancer Inst 90(9):656–667.
Greenfield S, Blanco DM, Elashoff RM, Ganz PA. 1987. Patterns of care related to age of breast cancer patients. JAMA 257(20):2766–2770.
Greer S, Morris T. 1975. Psychological attributes of women who develop breast cancer: A controlled study. J Psychosom Res 19(2):147–153.
Griff M, Bondurant S, Ernster, V et al. 2000. Information for Women about the Safety of Silicone Breast Implants. Institute of Medicine. Washington, DC: National Academy Press.
Groenvold M, Fayers PM, Sprangers MA, Bjorner JB, Klee MC, Aaronson NK, Bech P, Mouridsen HT. 1999. Anxiety and depression in breast cancer patients at low risk of recurrence compared with the general population: a valid comparison? J Clin Epidemiol 52(6):523–30.
Hall A, A’Hern R, Fallowfield L. 1999. Are we using appropriate self-report questionnaires for detecting anxiety and depression in women with early breast cancer? Eur J Cancer 35(1):79–85.
Hann D, Winter K, Jacobsen P. 1999. Measurement of depressive symptoms in cancer patients: Evaluation of the Center for Epidemiological Studies Depression Scale (CES-D). J Psychosom Res 46(5):437–443.
Heinrich RL, Schag CC, Ganz PA. 1984. Living with cancer: The Cancer Inventory of Problem Situations. J Clin Psychol 40(4):972–980.
Herrmann C. 1997. International experiences with the Hospital Anxiety and Depression Scale: A review of validation data and clinical results. J Psychosom Res 42(1):17–41.
Hewitt M, Rowland JH, Yancik R. 2003. Cancer survivors in the United States: Age, health, and disability. J Gerontol A Biol Sci Med Sci 58(1):82–91.
Holland JC, Rowland JH. 1991. Psychological reactions to breast cancer and its treatment. In: Harris JR, Hellman S, Henderson IC, Kinne DW, eds. Breast Diseases. 2nd ed. Philadelphia: Lippincott. Pp. 849–866.
Hopwood P, Howell A, Maguire P. 1991a. Psychiatric morbidity in patients with advanced cancer of the breast: Prevalence measured by two self-rating questionnaires. Br J Cancer 64(2):349–352.
Hopwood P, Howell A, Maguire P. 1991b. Screening for psychiatric morbidity in patients with advanced breast cancer: Validation of two self-report questionnaires. Br J Cancer 64(2):353–356.
Irvine D, Brown B, Crooks D, Roberts J, Browne G. 1991. Psychosocial adjustment in women with breast cancer. Cancer 67(4):1097–1117.
Jemal A, Thomas A, Murray T, Thun M. Cancer statistics, 2002. CA Cancer J Clin 52(1):23–47.
Justice B. 1999. Why do women treated for breast cancer report good health despite disease or disability? A pilot study. Psychol Rep 84(2):392–394.
Katon W, Ciechanowski P. 2002. Impact of major depression on chronic medical illness. J Psychosom Res 53(4):859–863.
Katon W, Schulberg H. 1992. Epidemiology of depression in primary care. Gen Hosp Psychiatry 14(4):237–247.
Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, Wittchen HU, Kendler KS. 1994. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Arch Gen Psychiatry 51(1):8–19.
Koopman C, Hermanson K, Diamond S, Angell K, Spiegel D. 1998. Social support, life stress, pain and emotional adjustment to advanced breast cancer. Psycho-Oncology 7(2):101–111.
Kornblith AB, Zhang C, Herndon II, JE, Weiss RB, Zuckerman EL, Rosenberg S, Mertz M, Payne D, Massie MJ, Holland JF, Byrd JC, Wingate P, Norton L, Holland JC, for the Cancer and Leukemia Group B (CALGB), Chicago, IL. 2003. Long-term adjustment of survivors of early stage breast cancer 20 years after adjuvant chemotherapy. Cancer 98(4):679–689.
Kornblith AB. 1998. Psychosocial adaptation of cancer survivors. In: Holland JC, ed. Psycho-Oncology. New York: Oxford University Press.
Krishnan KR, Delong M, Kraemer H, Carney R, Spiegel D, Gordon C, McDonald W, Dew M, Alexopoulos G, Buckwalter K, Cohen PD, Evans D, Kaufmann PG, Olin J, Otey E, Wainscott C. 2002. Comorbidity of depression with other medical diseases in the elderly. Biol Psychiatry 52(6):559–588.
Lansky SB, List MA, Herrmann CA, Ets-Hokin EG, DasGupta TK, Wilbanks GD, Hendrickson FR. 1985. Absence of major depressive disorder in female cancer patients. J Clin Oncol 3(11):1553–1560.
Lash TL, Silliman RA. 2000. Patient characteristics and treatments associated with a decline in upper-body function following breast cancer therapy. J Clin Epidemiol 53(6):615–622.
Leedham B, Ganz PA. 1999. Psychosocial concerns and quality of life in breast cancer survivors. Cancer Invest 17(5):342–348.
Love, AW, Kissane DW, Bloch S, Clarke, D. 2002. Diagnostic efficiency of the Hospital Anxiety and Depression Scale in women with early stage breast cancer. Aust N Z J Psychiatry 36(2):246–250.
Mandelblatt JS, Eisenberg JM. 1995. Historical and methodological perspectives on cancer outcomes research. Oncology (Huntingt) 9(11 Suppl):23–32.
Massie MJ, Holland JC. 1989. Overview of Normal Reactions and Prevalence of Psychiatric Disorders. New York: Oxford University Press. Pp. 273–282.
Massie MJ, Holland JC. 1991. Psychological reactions to breast cancer in the pre- and post-surgical period. Semin Surg Oncol 7(5):320–325.
Massie MJ, Holland JC. 1992. The cancer patient with pain: Psychiatric complications and their management. J Pain Symptom Manage 7(2):99–109.
Maunsell E, Brisson J, Deschenes L. 1989. Psychological distress after initial treatment for breast cancer: A comparison of partial and total mastectomy. J Clin Epidemiol 42(8):765–771.
Maunsell E, Brisson J, Deschenes L. 1992. Psychological distress after initial treatment of breast cancer. Assessment of potential risk factors. Cancer 70(1):120–125.
Maunsell E, Brisson J, Deschenes L. 1995. Social support and survival among women with breast cancer. Cancer 76(4):631–637.
Mausner JS, Kramer S, Bahn AK. 1985. Epidemiology: An Introductory Text. 2nd ed. Philadelphia: Saunders.
McEvoy MD, McCorkle R. 1990. Quality of life issues in patients with disseminated breast cancer. Cancer 66(6 Suppl):1416–1421.
McGuire WL, Foley KM, Levy MH, et al. 1989. Pain control in breast cancer: A panel discussion. Breast Canc Res Treat 13(1):5–15.
McHorney CA, Tarlov AR. 1995. Individual-patient monitoring in clinical practice: Are available health status surveys adequate? Qual Life Res 4(4):293–307.
McKee, AL, Schover, LR. 2001. Sexuality rehabilitation. Cancer 92(4 Suppl):1008–1012.
McLachlan SA, Devins GM, Goodwin PJ. 1998. Validation of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (QLQ-C30) as a measure of psychosocial function in breast cancer patients. Eur J Cancer 34(4):510–517.
Meyerowitz BE, Desmond KA, Rowland JH, Wyatt GE, Ganz PA. 1999. Sexuality following breast cancer. J Sex Marital Ther 25(3):237–250.
Montazeri A, Gillis CR, McEwen J. 1996. Measuring quality of life in oncology: Is it worthwhile? I. Meaning, purposes and controversies. Eur J Cancer Care (Engl) 5(3):159–167.
Montazeri A, Jarvandi S, Haghighat S, Vahdani M, Sajadian A, Ebrahimi M, Haji-Mahmoodi M. 2001. Anxiety and depression in breast cancer patients before and after participation in a cancer support group. Patient Educ Couns 45(3):195–198.
Morris T, Greer S, White P. 1977. Psychological and social adjustment to mastectomy. Cancer 40:2381–2387.
Musselman DL, Evans DL, Nemeroff CB. 1998. The relationship of depression to cardiovascular disease: Epidemiology, biology, and treatment. Arch Gen Psychiatry 55(7):580–592.
Narrow WE, Rae DS, Robins LN, Regier DA. 2002. Revised prevalence estimates of mental disorders in the United States: Using a clinical significance criterion to reconcile 2 surveys’ estimates. Arch Gen Psychiatry 59(2):115–123.
National Comprehensive Cancer Network. 1999. NCCN practice guidelines for the management of psychosocial distress. Oncology (Huntingt) 13(5A):113–147.
NCCN, Practice Guidelines for Breast Cancer, Version 2000. 2000. NCCN Proceedings, Oncology 14(11A):33–49.
NCCN. 2002. Clinical Practice Guidelines for Management of Distress. J NCCN 1(3):344–174.
Nemeroff CB, Musselman DL, Evans DL. 1998. Depression and cardiac disease. Depress Anxiety 8(Suppl 1):71–79.
Northouse LL. 1994. Breast cancer in younger women: Effects on interpersonal and family relations. J Natl Cancer Inst Monogr 16:183–190.
Northouse LL, Mood D, Kershaw T, Schafenacker A, Mellon S, Walker J, Galvin E, Decker V. 2002. Quality of life of women with recurrent breast cancer and their family members. J Clin Oncol 20(19):4050–4064.
Osoba D, Rodrigues G, Myles J, Zee B, Pater J. 1998. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol 16(1):139–144.
Petrie KJ, Buick DL, Weinman J, Booth RJ. 1999. Positive effects of illness reported by myocardial infarction and breast cancer patients. J Psychosom Res 47(6):537–543.
Regier DA, Myers JK, Kramer M, Robins LN, Blazer DG, Hough RL, Eaton WW, Locke BZ. 1984. The NIMH Epidemiologic Catchment Area program. Historical context, major objectives, and study population characteristics. Arch Gen Psychiatry 41(10):934–941.
Roth AJ, Kornblith AB, Batel-Copel L, Peabody E, Scher HI, Holland JC. 1998. Rapid screening for psychologic distress in men with prostate carcinoma: A pilot study. Cancer 82(10):1904–1908.
Rowland JH, Desmond KA, Meyerowitz BE, Belin TR, Wyatt GE, Ganz PA. 2000. Role of breast reconstructive surgery in physical and emotional outcomes among breast cancer survivors. J Natl Cancer Inst 92(17):1422–1429.
Rowland, JH, Massie, MJ. 1998. Breast Cancer in Psycho-Oncology. Holland J, ed. New York: Oxford University Press.
Rowland JH. 1999. Anxiety and the blues after breast cancer: How common are they? CNS Spectrums 4(10):40–54.
Santen RJ. 2003. Inhibition of aromatase: Insights from recent studies. Steroids 68(7–8):559–567.
Schag CA, Ganz PA, Heinrich RL. 1991. Cancer Rehabilitation Evaluation System—short form (CARES-SF). A cancer specific rehabilitation and quality of life instrument. Cancer 68(6):1406–1413.
Schag CA, Ganz PA, Polinsky ML, Fred C, Hirji K, Petersen L. 1993. Characteristics of women at risk for psychosocial distress in the year after breast cancer. J Clin Oncol 11(4):783–793.
Schag CA, Heinrich RL. 1990. Development of a comprehensive quality of life measurement tool: CARES. Oncology (Huntingt) 4(5):135–138; discussion 147.
Schag CA, Heinrich RL, Aadland RL, Ganz PA. 1990. Assessing problems of cancer patients: Psychometric properties of the cancer inventory of problem situations. Health Psychol 9(1):83–102.
Schag CC, Heinrich RL, Ganz PA. 1983. Cancer Inventory of Problem Situation: An instrument for assessing cancer patients’ rehabilitation needs. J Psychosoc Oncol 1(4):11–24.
Schagen SB, van Dam FS, Muller MJ, Boogerd W, Lindeboom J, Bruning PF. 1999. Cognitive deficits after postoperative adjuvant chemotherapy for breast carcinoma. Cancer 85(3):640–650.
Schover LR. 1994. Sexuality and body image in younger women with breast cancer. J Natl Cancer Inst Monogr (16):177–182.
Schover LR, Yetman RJ, Tuason LJ, et al. 1995. Partial mastectomy and breast reconstruction: A comparison of their effects on psychosocial adjustment, body image, and sexuality. Cancer 75(1):54–64.
Schover LR, 1999. Counseling cancer patients about changes in sexual function. Oncology 13(11):1585–1591.
Shimozuma K, Ganz PA, Petersen L, Hirji K. 1999. Quality of life in the first year after breast cancer surgery: Rehabilitation needs and patterns of recovery. Breast Cancer Res Treat 56(1):45–57.
Spiegel D, Bloom JR. 1983. Group therapy and hypnosis reduce metastatic breast carcinoma pain. Psychosom Med 45(4):333–339.
Spiegel D, Morrow GR, Classen C, et al. 1999. Group psychotherapy for recently diagnosed breast cancer patients: A multicenter feasibility study. Psycho-Oncology 8(6):482–493.
Sprangers MA, Groenvold M, Arraras JI, Franklin J, te Velde A, Muller M, Franzini L, Williams A, de Haes HC, Hopwood P, Cull A, Aaronson NK. 1996. The European Organization for Research and Treatment of Cancer breast cancer-specific quality-of-life questionnaire module: First results from a three-country field study. J Clin Oncol 14(10):2756–2768.
Stanton AL, Danoff-Burg S, Sworowski LA, et al. 2002. Randomized controlled trial of written emotional expression and benefit finding in breast cancer patients. J Clin Oncol 20(20):4160–4168.
Stewart AL, Greenfield S, Hays RD, Wells K, Rogers WH, Berry SD, McGlynn EA, Ware JE Jr. 1989. Functional status and well-being of patients with chronic conditions. Results from the Medical Outcomes Study. JAMA 262(7):907–913.
Stewart DE, Cheung AM, Duff S, Wong F, McQuestion M, Cheng T, Purdy L, Bunston T. 2001. Attributions of cause and recurrence in long-term breast cancer survivors. Psycho-Oncology 10(2):179–183.
Syrjala K, Chapko J. 1995. Evidence for a biopsychosocial model of cancer treatment-related pain. Pain 61:69–79.
Tchekmedyian NS, Hickman M, Siau J, Greco A, Aisner J. 1990. Treatment of cancer anorexia with megestrol acetate: Impact on quality of life. Oncology (Huntingt) 4(5):185–192.
Tomich PL, Helgeson VS. 2002. Five years later: A cross-sectional comparison of breast cancer survivors with healthy women. Psycho-Oncology 11(2):154–169.
Trimble EL, Rowland J, Varricchio C, Gore-Langton RE. 2001. Clinical trials referral resource. Health related quality of life in cancer clinical trials. Oncology (Huntingt) 15(4):456–458, 461–466.
van Dam FS, Schagen SB, Muller MJ, Boogerd W, vd Wall E, Droogleever Fortuyn ME, Rodenhuis S. 1998. Impairment of cognitive function in women receiving adjuvant treatment for high-risk breast cancer: High-dose versus standard-dose chemotherapy. J Natl Cancer Inst 90(3):210–218.
van’t Spijker A, Trijsburg RW, Duivenvoorden HJ. 1997. Psychological sequelae of cancer diagnosis: A meta-analytical review of 58 studies after 1980. Psychosom Med 59(3):280–293.
Velikova G, Wright EP, Smith AB, Cull A, Gould A, Forman D, Perren T, Stead M, Brown J, Selby PJ. 1999. Automated collection of quality-of-life data: A comparison of paper and computer touch-screen questionnaires. J Clin Oncol 17(3):998–1007.
Ware JE. 1993. Measuring patients’ views: The optimum outcome measure. BMJ 306(6890):1429–1430.
Ware JE Jr, Sherbourne CD. 1992. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 30(6):473–183.
Warga CL. 2000. Menopause and the Mind: The Complete Guide to Coping with the Cognitive Effects of Perimenopause and Menopause, Including Memory Loss, Foggy Thinking, and Verbal Slips. New York: Simon and Schuster.
Wells KB, Stewart A, Hays RD, Burnam MA, Rogers W, Daniels M, Berry S, Greenfield S, Ware J. 1989. The functioning and well-being of depressed patients. Results from the Medical Outcomes Study. JAMA 262(7):914–919.
Wenzel LB, Fairclough DL, Brady MJ, Cella D, Garrett KM, Kluhsman BC, Crane LA, Marcus AC. 1999. Age-related differences in the quality of life of breast carcinoma patients after treatment. Cancer 86(9):1768–1774.
Wickman M. 1995. Breast reconstruction: Past achievements, current status, and future goals. Scand J Reconstr Hand Surg 29:81–100.
Yu CL, Fielding R, Chan CL, Tse VK, Choi PH, Lau WH, Choy DT, O SK, Lee AW, Sham JS. 2000. Measuring quality of life of Chinese cancer patients: A validation of the Chinese version of the Functional Assessment of Cancer Therapy-General (FACT-G) scale. Cancer 88(7):1715–1727.
Zabora J, BrintzenhofeSzoc K, Curbow B, Hooker C, Piantadosi S. 2001a. The prevalence of psychological distress by cancer site. Psycho-Oncology 10(1):19–28.
Zabora J, BrintzenhofeSzoc K, Jacobsen P, Curbow B, Piantados S, Hooker C, Owens A, Derogatis L. 2001b. A new psychosocial screening instrument for use with cancer patients. Psychosomatics 42(3):241–246.
Zabora JR, Smith-Wilson R, Fetting JH, Enterline JP. 1990. An efficient method for psychosocial screening of cancer patients. Psychosomatics 31(2):192–196.
Zigmond AS, Snaith RP. 1983. The hospital anxiety and depression scale. Acta Psychiatr Scand 67(6):361–370.