Considerations for Returning Individual Genomic Results from Population-Based Surveys: Focus on the National Health and Nutrition Examination Survey: Proceedings of a Workshop (2023)
Chapter: 6 Informed Consent When Considering Returning Genetic Results to Survey Participants (Session 5)
6
Informed Consent When Considering Returning Genetic Results to Survey Participants (Session 5)
This chapter summarizes the presentations and discussion in Session 5, which took place on December 7, 2022. This session focused on informed consent when returning genetic results to research participants. Amy McGuire, director of the Center for Medical Ethics and Health Policy at Baylor College of Medicine, moderated the session. Questions and discussion followed at the end of the session.1
COMMUNITY ENGAGEMENT AND INFORMED CONSENT IN NHANES
Duong (Tony) Nguyen, chief medical officer (CMO) for the National Health and Nutrition Examination Survey (NHANES), kicked off this session by providing more detailed information about the current informed consent and outreach activities for NHANES. Nguyen explained that, as the CMO for NHANES, he is the primary contact for participants and their medical providers if they have any clinical questions about the results. He can provide medical interpretations, medical recommendations, and public health recommendations. In addition, as a member of the NHANES Operations Branch, he participates in NHANES’s outreach activities.
___________________
1 Video recordings of the presentations and discussions, along with copies of the presenters’ slides for Session 5, are available online at https://www.nationalacademies.org/event/12-07-2022/workshop-on-considerations-for-returning-individual-genomic-results-from-population-based-surveys-focus-on-the-national-health-and-nutrition-examination-survey-day-2-virtual
Informed Consent
Nguyen reminded the audience that NHANES consents occur in two phases: first during the household interview and again at the Mobile Examination Center (MEC). During the household interview, field staff provide participants with a printed packet of consent materials, which includes the confidentiality brochure; MEC consent and assent brochures; copies of the consent/assent forms; and NHANES Health Measurements List, which outlines the tests participants may receive depending on their age, as well as an indicator for which health measures will unconditionally get reported back to participants and an indicator for which results will be reported back only when the test indicates a high or abnormal result. Participants must provide verbal consent prior to beginning the home interview.2 Showing copies of each document, Nguyen highlighted some key attributes of the documents, such as where the documents spell out the federal laws in place to protect participants’ privacy and confidentiality and detail the legal ramifications if staff willfully disclosed any information. Particularly relevant to this workshop, Nguyen noted the FAQs section of the Future Research Consent Form, which informs participants that they will not be contacted with any individual results from future studies (see Box 6-1).
Finally, Nguyen explained that the Health Measurements List uses black diamond icons to indicate which results participants can expect to receive and explicitly differentiating those results that will be sent to participants only if the results are abnormal or positive. Listed on page 3 under “Environmental Measurements,” Nguyen highlighted butyrylcholinesterase as an example of a finding that is reported only if a positive or abnormal result is found. He explained to the audience that having butyrylcholinesterase is a biomarker indicative of exposure to organophosphates regularly, and a low level could mean a person may have more difficulty recovering from general anesthesia.3 “We feel that reporting that low level is really important for those who may get general surgery because it’s important for them to know and tell their surgeons and their anesthesiologists so that precautions can be done for them to use a different medication so that that recovery is normal,” said Nguyen.
Reiterating that all of the documents are provided and covered during the in-home interview, Nguyen explained that upon arriving to the MEC participants are presented with the documents again and asked if they have any final questions before providing signatures for consent to participate.
___________________
2 Copies of the NHANES 2021–2022 brochures and consent documents are available at https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/documents.aspx?Cycle=2021-2022
3 Due to a rare medical disorder called pseudocholinesterase deficiency.
Outreach Activities
Nguyen shared that NHANES spends a considerable amount of time trying to encourage participation by underscoring the importance of the study, demonstrating the benefits and relevance of participation, and addressing suspicions and fears of the individual selected for participation. He explained that one of NHANES’s first operational activities is to contact and meet with the local health department(s). In fact, NHANES representatives/staff are securing support and guidance from the local health department(s) on leaders, media contacts, and other important members of the community months before the NHANES study actually arrives to a location. Nguyen explained that these organizations and individuals are contacted in the intervening months to begin building rapport. NHANES outreach activities, frequently conducted by Nguyen himself, can include meeting with elected officials, city councils, and influential community leaders (e.g., religious, university, cultural)—who are invited along with all members of the community to visit and tour the NHANES MEC during each location’s Open House day.
NHANES representatives also give presentations to other community groups, which might include homeowners associations and large apartment complexes, intended to garner support, understanding, and legitimacy for NHANES. “Sometimes a letter of support from the local university goes a long way at the doorstep to show that participant or potential participant
why NHANES is important and what it means to the health of our nation,” said Nguyen. In closing, Nguyen highlighted some of the specific media activities (e.g., TV interviews, radio interviews, newspaper articles, press conferences) that are used in hopes that “by the time we do arrive at their doorstep and knock on their door, they will be familiar with us and be able to participate.”
INFORMED CONSENT: CONTENT FOR RETURN OF RESEARCH RESULTS AND BIOBANKING
Next, David Magnus, director of the Stanford Center for Biomedical Ethics and the vice chair of the Institutional Review Board (IRB) at the All of Us Research Program, spoke about the content of informed consent forms. There is a large body of literature on the return of genomic results. Magnus began by highlighting one article in particular,4 which lays out the concept that there is a “floor,” a “ceiling,” and “the choices in between.” The floor refers to the minimum amount of information that should be returned. For example, most agree that valid, medically important, actionable results should be returned.5 On the other extreme is the ceiling, which Jarvik et al. (2014) describe as the belief that: “Researchers might be ethically and scientifically justified in returning all genomic information … in some format…” (p. 824).6 Finally, Magnus continued, some modern research projects also believe they should return some results that fall “in the space between” to varying degrees. Hence, there are differences in the
___________________
4 Jarvik, G. P., Amendola, L. M., Berg, J. S., Brothers, K., Clayton, E. W., Chung, W., Evans, B. J., Evans, J. P., Fullerton, S. M., Gallego, C. J., Garrison, N. A., Gray, S. W., Holm, I. A., Kullo, I. J., Lehmann, L. S., McCarty, C., Prows, C. A., Rehm, H. L., Sharp, R. R., Salama, J., … Burke, W. (2014). Return of genomic results to research participants: The floor, the ceiling, and the choices in between. American Journal of Human Genetics, 94(6), 818–826. https://doi.org/10.1016/j.ajhg.2014.04.009
5 Magnus explained that preferences for which results are returned vary across stakeholder groups, including participants and researchers, with researchers a bit more cautious than participants. However, in general all groups agree with the “floor” standard of returning valid, medically important, actionable results. Specifically, he cited the following publication: Vears, D. F., Minion, J. T., Roberts, S. J., Cummings, J., Machirori, M., Blell, M., Budin-Ljøsne, I., Cowley, L., Dyke, S. O. M., Gaff, C., Green, R., Hall, A., Johns, A. L., Knoppers, B. M., Mulrine, S., Patch, C., Winkler, E., and Murtagh, M. J. (2021). Return of individual research results from genomic research: A systematic review of stakeholder perspectives. PLoS ONE, 16(11), e0258646. https://doi.org/10.1371/journal.pone.0258646
6 Jarvik, G. P., Amendola, L. M., Berg, J. S., Brothers, K., Clayton, E. W., Chung, W., Evans, B. J., Evans, J. P., Fullerton, S. M., Gallego, C. J., Garrison, N. A., Gray, S. W., Holm, I. A., Kullo, I. J., Lehmann, L. S., McCarty, C., Prows, C. A., Rehm, H. L., Sharp, R. R., Salama, J., … Burke, W. (2014). Return of genomic results to research participants: The floor, the ceiling, and the choices in between. American Journal of Human Genetics, 94(6), 818–826. https://doi.org/10.1016/j.ajhg.2014.04.009
lists that research repositories use, and others still choose not to return any results.
Magnus emphasized at the beginning of his talk that the issue of consent is multifaceted and includes the questions: “What is to be returned?” and “What is to be disclosed about what research is to be conducted?” However, he noted that to the extent possible, he would focus his talk on the question: “What is disclosed about what is returned?”
Consent Strategies: Broad vs. Tiered
Magnus began by describing consent options and noted that guidance from the U.S. Department of Health and Human Services recommends broad consent when possible. He explained that this is partly because it is impossible to apply specific consent to large, scientifically valuable research repositories, such as NHANES and the All of Us Research Program. However, he noted that there is currently a push toward tiered consent. Magnus shared a publication that laid out a possible model for tiered consent,7 which included tiers based on nonmedical tests, limited-versus-high clinical utility medical tests, and subcategories of disease (e.g., severity, age of onset). Magnus noted that when considering which consent structure to use, an important caveat is that no one structure has yet to be proven more effective than the others. For example, a study comparing several consent structural elements (e.g., tiered or broad consent, open or controlled access) found that the consent strategy had almost no impact on participants’ willingness to participate.8
Recommended Content
Next, Magnus advised which elements should be included in consent forms, starting with a few recommendations from a 2018 National Academies report, Returning Individual Research Results to Participants: Guidance for a New Research Paradigm.9 Specifically, Magnus wanted
___________________
7 Bunnik, E. M., Janssens, A. C., and Schermer, M. H. (2013). A tiered-layered-staged model for informed consent in personal genome testing. European Journal of Human Genetics, 21(6), 596–601. https://doi.org/10.1038/ejhg.2012.237
8 Sanderson, S. C., Brothers, K. B., Mercaldo, N. D., Clayton, E. W., Antommaria, A. H. M., Aufox, S. A., Brilliant, M. H., Campos, D., Carrell, D. S., Connolly, J., Conway, P., Fullerton, S. M., Garrison, N. A., Horowitz, C. R., Jarvik, G. P., Kaufman, D., Kitchner, T. E., Li, R., Ludman, E. J., McCarty, C. A., … Holm, I. A. (2017). Public attitudes toward consent and data sharing in biobank research: A large multi-site experimental survey in the US. American Journal of Human Genetics, 100(3), 414–427. https://doi.org/10.1016/j.ajhg.2017.01.021
9 National Academies of Sciences, Engineering, and Medicine. (2018). Returning individual research results to participants: Guidance for a new research paradigm. The National Academies Press. https://doi.org/10.17226/25094
to highlight Recommendations 6 and 9: “Include plans for the return of individual research results in research protocols” (p. 177) and “Ensure transparency regarding return of individual results in the consent process” (p. 208).
In addition to these recommendations from the National Academies report, Magnus highlighted a publication from 2019 that analyzed international laws and policies around the return of individual genomic research results.10 The policies highlighted in the report provide participants with varying degrees of autonomy, including being informed, receiving pretest counseling, providing opt-in or opt-out and tiered consent choices, and allowing participants to change their minds. Among all this variety, a common and critical theme from this report was that protocols for consenting to return individual genomic results need to be in place before the research starts.
Continued Challenges in Achieving Participant Understanding
Magnus addressed the continued efforts and challenges of creating informed consent protocols that lead to adequate participant understanding. In 2015, a Delphi study11 attempted to address this problem by convening an expert panel to establish consensus on what is necessary for participants to understand to provide adequate consent before a biobank study.12 Topics addressed included the return of results and the Genetic Information Nondiscrimination Act of 2008.13 Using these guidelines, researchers carefully designed a simplified consent process to enhance understanding of these critical features specifically. Unfortunately, despite these efforts, researchers found that many people still did not meet their preset criteria for adequate understanding.14 Magnus referenced additional research in this field, for example, using randomized trial designs to compare the level of understanding
___________________
10 Thorogood, A., Dalpé, G., and Knoppers, B. M. (2019). Return of individual genomic research results: Are laws and policies keeping step? European Journal of Human Genetics, 27(4), 535–546. https://doi.org/10.1038/s41431-018-0311-3
11The Delphi technique is a method for answering a research question by identifying a view shared among experts in a given subject matter area (see Barrett, D., and Heale, R. [2020]. What are Delphi studies? Evidence-Based Nursing, 23, 68–69. https://ebn.bmj.com/content/23/3/68).
12 Beskow, L. M., Dombeck, C. B., Thompson, C. P., Watson-Ormond, J. K., and Weinfurt, K. P. (2015). Informed consent for biobanking: Consensus-based guidelines for adequate comprehension. Genetics in Medicine, 17(3), 226–233. https://doi.org/10.1038/gim.2014.102
13 For more information, see https://www.eeoc.gov/statutes/genetic-information-nondiscrimination-act-2008
14 Beskow, L. M., Lin, L., Dombeck, C. B., Gao, E., and Weinfurt, K. P. (2017). Improving biobank consent comprehension: A national randomized survey to assess the effect of a simplified form and review/retest intervention. Genetics in Medicine, 19(5), 505–512. https://doi.org/10.1038/gim.2016.157
when consent information is present through comics, illustrated videos, PowerPoint with voiceovers, and standard written materials. He noted that while these methods can affect levels of understanding, none result in satisfactory comprehension.
Magnus next addressed the response of the 2015 Delphi study expert panel when faced with the fact that even with suitable consent forms, people lack an understanding of the elements they previously deemed necessary. Interestingly, rather than recommending that the majority of participants should be excluded from research studies, the Delphi panel dramatically shifted their opinion and modified their recommendations to say that less information must be understood. Follow-up interviews with panelists indicated significant uncertainty about defining a threshold of understanding and what should happen when prospective participants cannot grasp essential information. Magnus commented on this narrative, saying, “I think this shows actually good judgment in some ways on their part because a lot of our assumptions about informed consent and communication are rested on really problematic understandings about how language and communication works that ignores almost 100 years of work in linguistics, philosophy of language, and linguistic anthropology.” He specifically pointed to an absence of “concepts like the division of linguistic labor” in conversations about informed consent. Overall, Magnus cautioned that many participants will not fully understand the content even with well-developed and well-designed consent forms.
Lessons Learned from Consent Development at the All of Us Research Program
Magnus next shared his experience working to develop the consent process at the All of Us Research Program, which he said he now sees as “both a success story and a precautionary tale.” It is a precautionary tale because the All of Us Research Program, like many other research programs Magnus has worked on, had the problem of “trying to build an airplane while it is in the air.” But on the other hand, Magnus believes that after several years of work, the process that the All of Us Research Program eventually developed is a “rather outstanding modular approach to consent and a plan about what to return.”
Magnus started by elaborating on the difficulties of developing consent processes alongside participant recruitment. For example, he noted that the consent form signed by some of the All of Us Research Program’s earliest participants did not mention genomics in their consents whatsoever. In addition, a second cohort was given some information about the plan to do testing, but it lacked sufficient detail. Magnus noted that this second group of participants led to another major concern: how much information does
one have to give participants to start sequencing their DNA before a plan is in place for the return of genomic results? The All of Us Research Program IRB decided that the program had to have a detailed genetic return-of-results plan, even though the program did not yet have Food and Drug Administration (FDA) approval, and therefore would likely have to implement some changes. Furthermore, the IRB decided that the All of Us Research Program had to reconsent both early cohorts before returning any results. Magnus acknowledged that internal and external factors often push researchers at such programs as the All of Us Research Program and NHANES to get things done as quickly as possible, including beginning to recruit participants. However, Magnus cautioned NHANES against rushing into research. Instead, he recommended that they develop a detailed plan for the return of results before seeking approval from the IRB and beginning their study.
Magnus next shared what he sees as the success of the All of Us Research Program’s final consent and plan to return results. The All of Us Research Program consent process involves primary consent, consent specific to the return of genomic results, and informing loops or “modules” for tiered consent. Consent is tiered around different types of genetic information, such as health-related, pharmacogenetics, ancestry, and recreational results.
The primary consent form introduces some very general information regarding the return of results. For example, it includes an introduction to DNA and the different scientific and analytical methods, including whole-genome sequencing, that scientists might use to study biological samples. In addition, the form explains that data will be stored in a database and that this inherently introduces privacy risks. It explains that there may not be direct benefits to participants, but it might lead to broader societal benefits. Finally, the form emphasizes that participation in the All of Us Research Program is not a replacement for regular medical treatment.
After completing the basic consent form, participants are directed to a consent form specific to return of genomic results. Magnus noted that the All of Us Research Program performed extensive cognitive testing to understand how participants perceived the language in consent forms and how to minimize misunderstandings. To illustrate this, Magnus reiterated the example shared by Anastasia Wise earlier in the day, where the All of Us Research Program found that it should avoid using the term pharmacogenomics because it led participants to assume these results would be related in some way to economics. He provided the following bulleted summary showing each of the questions that are addressed in the All of Us Research Program consent form for return of genomic results:
- How will you check my DNA?
- How long will it take to get results?
- What exactly do you check for?
- What will you tell me?
- Do I need to pay to get my DNA results?
- How could learning my DNA results help me? What are the risks of learning my DNA results?
- What are the risks of sharing my DNA results?
- What are the limits of the All of Us DNA results?
- Are there ways the DNA results can’t be used?
- Will you ever give out my DNA results?
- Do I have to learn my DNA results?
- When will my consent expire?
- Who can answer my questions?
After these questions are addressed in this consent module, the participant decides whether they would not like to receive results, whether they are unsure, or whether they want to learn about some or all of their DNA results. Importantly, participants are reminded that they can change their minds about consent to receive their results, but that based on their primary consent form, researchers will still analyze their samples. Participants who said they would like to receive some or all of their results are directed to informing loops that provide more detail about the results (e.g., ancestry, recreational, health-related) they would like to receive.
Magnus concluded his talk with some general thoughts for NHANES as it begins to think about their consent process for the return of results. First, he encouraged that NHANES have a well-developed plan and consent forms before the protocol is reviewed by IRB and before the launch of its research. Second, Magnus noted that both staged and tiered consent with some broad consent elements can work very well. Specifically, he recommended that NHANES consider a consent process that includes primary consent with basic information, consent more specific to the return of results that covers the range of results that can be returned, and use informing loop modules for each of these different types of results. Finally, Magnus noted that extensive cognitive testing would be required to employ this strategy effectively. Still, he also shared that while he is very impressed by the improvements in understanding that can result from thorough cognitive testing, he still has “some amount of skepticism about whether you can get anything like universal understanding,” which he believes is because of the complex nature of language itself.
THE INFORMED CONSENT PROCESS FOR RETURN OF RESULTS AND BIOBANKING
Michelle Meyer, an associate professor and chair of the Department of Bioethics and Decision Sciences at Geisinger, spoke next about the informed consent process for returning genetic results and biobanking in research studies, focusing primarily on her experiences with electronic consent. Meyer started by placing some biobank programs along a continuum in terms of granularity and timing of choice for the return of results, which she explained impact both the content and the process of consent (see Figure 6-1).
Biobanks on one end of the spectrum offer participants a minimal number of choices, said Meyer. For example, Geisinger’s MyCode biobank bundles the choice about receiving the return of genetic results with the decision to be part of the biobank. There is one decision up front to join MyCode or not, and that entails a decision to consent to be contacted with clinically actionable results. Moving along the spectrum are platforms where people can choose to receive or not receive categories of results but cannot necessarily opt out of receiving individual results within a given category. For example, All of Us participants can choose to receive all their hereditary disease reports, or just pharmacodynamic results, or no results whatsoever. Finally, on the other end of the spectrum are platforms that allow people to pick and choose whether or not to receive each individual result or result category. For example, each of 23andMe’s four results can be individually unlocked such that a person could choose to learn about their BRCA but not their apolipoprotein E gene, while other results are category based, such that unlocking a single carrier result will unlock all carrier results.
Meyer pointed out that a minimal choice might not be concordant with everyone’s preferences and more importantly, because the return of results is bundled with the decision to be in the study, there could be selection biases. On the other hand, she noted that adding or offering granular choices is resource intensive, and there are logistical challenges associated with tracking each choice over time. Another challenge is that participants may forget about their participation in a given study, which creates additional challenges. Additionally, Meyer highlighted ethics or even moral distress as a consideration, particularly where study participants are also patients.
Electronic Consent
As noted by other workshop speakers, Meyer noted that research consent forms are often long, complex, and suboptimally relevant to the
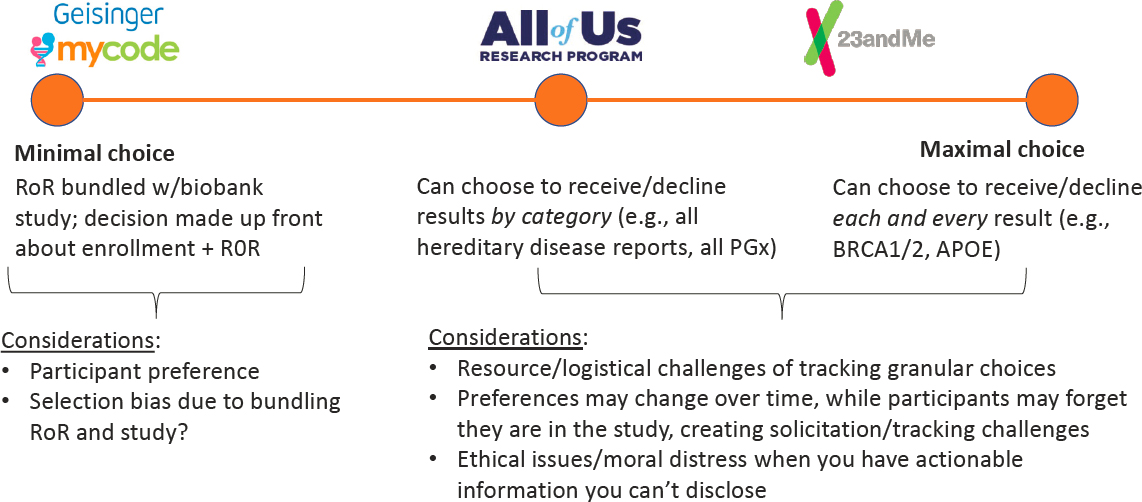
NOTE: APOE = apolipoprotein E; PGx = pharmacogenetics; RoR = return of results.
SOURCES: Workshop presentation by Michelle Meyer December 7, 2022 (slide 3).
participant,15 and postconsent comprehension is generally poor.16 She noted that the studies investigating alternative methods (e.g., use of multimedia, concise forms, extended conversations) for improving consent comprehension have produced mixed results.17 While there has been a fair amount of enthusiasm for electronic consent (eConsent),18 there is a dearth of high-quality evidence from randomized clinical trials supporting it.19
Meyer explained that she would be introducing the audience to an open-source, smartphone-based form of consent developed by Sage Bionetworks that is being used for the Apple ResearchKit and All of Us Research Program. The Safe Bionetworks eConsent has shown to be feasible with generally positive indications of informedness,20 but there is a “dearth of
___________________
15 Kass, N. E., Chaisson, L., Taylor, H. A., and Lohse, J. (2011). Length and complexity of US and international HIV consent forms from federal HIV network trials. Journal of General Internal Medicine, 26, 1324–1328. https://doi.org/10.1007/s11606-011-1778-6
16 Joffe, S., Cook, E. F., Cleary, P. D., Clark, J. W., and Weeks, J. C. (2001). Quality of informed consent in cancer clinical trials: A cross-sectional survey. Lancet, 358(9295), 1772–1777. https://doi.org/10.1016/S0140-6736(01)06805-2; Appelbaum, P. S. (2010). Understanding “understanding”: An important step toward improving informed consent to research. American Journal of Bioethics Primary Research, 1(2), 1–3. https://doi.org/10.1080/21507716.2010.499322
17 Grady, C., Touloumi, G., Walker, A. S., Smolskis, M., Sharma, S., Babiker, A. G., Pantazis, N., Tavel, J., Florence, E., Sanchez, A., Hudson, F., Papadopoulos, A., Emanuel, E., Clewett, M., Munroe, D., and Denning, E. (2017). A randomized trial comparing concise and standard consent forms in the START trial. PLoS ONE, 12(4), e0172607. https://doi.org/10.1371/journal.pone.0172607; Flory, J., and Emanuel, E. (2004). Interventions to improve research participants’ understanding in informed consent for research: A systematic review. Journal of the American Medical Association, 292(13), 1593–601. https://doi.org/10.1001/jama.292.13.1593; Kass, N. E., Taylor, H. A., Ali, J., Hallez, K., and Chaisson L. (2015). A pilot study of simple interventions to improve informed consent in clinical research: Feasibility, approach, and results. Clinical Trials, 12(1), 54–66. https://journals.sagepub.com/doi/full/10.1177/1740774514560831
18 Biesecker, B., Raspa, M., Rupert, D., Moultrie, R., Furberg, R., and McCormack, L. A. (2019). Making clinical trials more patient-centered using digital interactive e-consent tools (RTI Press Occasional Paper No. OP-0063-1910). RTI Press. https://doi.org/10.3768/rtipress.2019.op.0063.1910; Kraft, S. A, Garrison, N. A., and Wilfond, B. S. (2019). Understanding as an ethical aspiration in an era of digital technology-based communication: An analysis of informed consent functions. American Journal of Bioethics, 19(5), 34–36. https://doi.org/10.1080/15265161.2019.1587035
19 De Sutter, E., Zaçe, D., Boccia, S., Di Pietro, M. L., Geerts, D., Borry, P., and Huys, I. (2020). Implementation of electronic informed consent in biomedical research and stakeholders’ perspectives: Systematic review. Journal of Medical Internet Research, 22(10), e19129. https://doi.org/10.2196/19129
20 Doerr, M., Moore, S., Barone, V., Sutherland, S., Bot, B. M., Suver, C. and Wilbanks, J. (2021). Assessment of the All of Us Research Program’s informed consent process. American Journal of Bioethics Empirical Bioethics, 12(2), 72–83. https://doi.org/10.1080/23294515.2020.1847214; Doerr, M., Maguire Truong, A., Bot, B., Wilbanks, J., Suver, C., and Mangravite, L. (2017). Formative evaluation of participant experience with mobile eConsent in the app-mediated Parkinson mPower Study: A mixed methods study. Journal of Medical Internet Research Mobile Health and Ubiquitous Health, 5(2), e14. https://doi.org/10.2196/mhealth.6521
evidence regarding the advantages and disadvantages of electronic methods in terms of understanding of information.”21 Meyer highlighted three important features of the Sage eConsent: iconographic representation of key concepts, tiers of information architecture, and use of teach-back questions which are intended to reinforce the learning of key concepts through the end of the eConsent process.
Trial to Compare eConsent with Standard Consent
Meyer shared some preliminary, unpublished results from a study comparing eConsent to the “standard” consent method of reviewing a written consent form and having a conversation with the consenter. In the trial, MyCode consenters approached Geisinger patients in clinics and asked if they were interested in hearing about MyCode. They randomly assigned the 675 interested patients to receive either the “standard” consent process administered via paper and pencil, or the eConsent process administered on an iPad. In addition to demographic and other survey questions, all participants were measured on comprehension using a ten-question quiz. The recruited participants were mostly female and diverse in age and educational attainment but reflected the very limited racial and ethnic diversity of the central Pennsylvania region. Preliminary results from the trial found that relative to those assigned to the standard mode, participants assigned to the eConsent mode generally scored higher on the objective comprehension measures. However, there was no significant difference between the two groups on the subjective measures of comprehension. The results indicate that the eConsent process objectively took longer than the standard process (average of 1.5 minutes for standard consent versus 3.6 minutes for eConsent) and subjectively felt longer to participants. The study found no significant correlation in either arm between the quiz score and age, sex assigned at birth, gender identity, self-reported health literacy, and race/ethnicity. Meyer shared that, consistent with other studies, this MyCode study found correlations between educational attainment and income in each of the arms and noted “this was not exacerbated in the eConsent arm” for the MyCode study. She also shared that only 14 percent of participants clicked on any of the 13 “learn more” links, with the links on privacy and data sharing being the two that were selected most often.
In closing, Meyer highlighted four concluding considerations. First, the length of the consent process in the eConsent condition takes longer and feels longer, which she explained can be a benefit of sorts because
___________________
21 National Academies of Sciences, Engineering, and Medicine. (2018). Returning individual research results to participants: Guidance for a new research paradigm. The National Academies Press. https://doi.org/10.17226/25094
“consent is one of the few things in life where we actually want to slow people down” in order to “get people thinking a little bit more critically.” Meyer next highlighted that the eConsent requires participants to have some comfort with technology and that, while it is reasonable to expect that comfort to increase over time, she suggested that near-term studies should include a paper-and-pencil alternative available for people who do not want to use a computer or electronic device. Meyer noted that another benefit of eConsent is that it can allow staff who do not have genomics expertise to facilitate the consent process and/or make the consent process self-serve for many participants, which can be really critical for reaching rural populations and having more diverse biobanks. Having eConsent also makes a tiered consent process more cost-effective because it facilitates granular tracking of participant choice over time, Meyer explained. In addition, she noted that eConsent provides a level of standardization that is just not possible with human-mediated consent processes that can introduce biases and unwarranted deviations from study protocols (e.g., presumptions about who might want results or need/not need to hear certain things).
Finally, Meyer offered her perspective that while employing teach-back methods provides an opportunity to set comprehension thresholds, any study enrollment threshold should reflect the risks of enrollment or getting results with poor comprehension and or suboptimal comprehension of particular concepts, including the risks associated with excluding participants from the study or return of results. For example, the Harvard Personal Genome Project required participants to score 100 percent on a genomics quiz for a study that does not have any obvious direct benefits to participants and does include risks associated with publishing a person’s whole genome on the internet, said Meyer. She contrasted this against the All of Us Research Program that asks questions to assess formative comprehension but does not include a comprehension threshold that is required for participation.
QUESTIONS AND REFLECTIONS FOR SESSION 5
McGuire led and moderated the discussion for this session. She started by asking Magnus to weigh in with his thoughts on how the consent process could be managed if NHANES was to ensure that investigators who apply to analyze genetic material collected by NHANES have an IRB plan that is approved. Magnus explained that losing track of people over time is/was a major challenge for All of Us because the program told participants initially that they would only receive certain results if those results were abnormal, which set up an expectation that “no news is good news.” This creates an opportunity for a participant who could not be recontacted for any number of reasons to incorrectly conclude that the reason they did
not receive results was because nothing abnormal was found. He explained that this was one reason the All of Us Research Program said sequencing could be conducted only after participants were reconsented. He advised that study protocols should include thresholds for what sorts of things a study will do and how much effort the study will expend to find a lost participant. In addition, he noted that the consent forms need to set appropriate expectations based on that possibility. Magnus also advised that the recontact protocols be shared up front with researchers applying for access so that they have a complete understanding of all that will be required and can budget accordingly. Finally, he reiterated that communications must avoid creating unrealistic explanations that just because a participant received some recreational genetics results does not necessarily imply anything about what that participant might have to consent to in order to receive more results in the future.
Dana C. Crawford, Case Western Reserve University, clarified that this workshop is intended to focus on the scenario in which the Centers for Disease Control and Prevention (CDC) conducts the genetic testing—not a scenario in which investigators apply to conduct genetic testing on existing specimens stored in the biorepository. She reminded the audience that if the CDC were to add genetic testing to NHANES in the future, those activities would most likely be conducted by a single lab.22
Confirming that this approach would avoid some of the challenges that the All of Us Research Program faced, Magnus distinguished between “secondary uses of data collected for other purposes” and creating a biobank with the intention of doing genomics from the beginning. Jeffrey R. Botkin, University of Utah, reminded the audience that the NHANES biorepository does not accept research proposals for analyses of genetic specimens designed to generate clinically actionable data and in doing so, eliminates the possibility that results would need to be returned to participants. Nguyen confirmed Botkin’s summary and added, “one of the stipulations that we have with our participants is that we will not contact them after their current survey.”
Magnus further distinguished between a program making decisions about what should be returned to all participants versus investigator-driven research projects, which are more likely to return results only if they are abnormal. He shared that the All of Us Research Program allows investigators to analyze the sequenced data, and none of those results are being returned to individuals. “The only things being returned to the individuals are the things that the program decided that they’re going to make sure are analyzed and returned,” said Magnus.
___________________
22 Crawford made this assumption because NHANES intentionally uses a single lab for any given test, as discussed in Session 1.
McGuire next asked if the panelists could speak to how NHANES should handle the issue of participant choice: What are some of the ethical arguments and practical challenges for implementing different approaches (e.g., opt-in, opt-out, tiered consent, tailored consent)? What is the best approach given the NHANES context? Meyer responded first by stressing the importance of acknowledging what kinds of human and program resources are in place. She explained that because of resource constraints, MyCode chose not give participants any opportunities to opt in or out of receiving specific results. Instead, they are not provided explicit information about whether variants were detected, as is done by 23andMe, for example. “That has turned out to be very confusing for participants,” shared Meyer. However, creating and maintaining a secure portal for reporting all findings over time, including those in which no variant is detected, is a resource-intensive endeavor.
Meyer said: “I told you that 99 percent of people in the eConsent arm correctly said, ‘Yes, we’ll tell you about these results.’ In the ten-point quiz, though, the one question out of ten that everybody bombed was about return of results. Why? Because it was a multiple-choice question and one of the decoy wrong answers was, ‘Everybody will get results.’ That’s not true.”
Magnus added: “I worry at a more basic level that this picture that we have of how consent works is so fundamentally at odds with everything that people in linguistics and linguistic anthropology and philosophy of language have been saying for the past 100 years.” He stated, “if we really saw the communications as what they are, which are actions, speech acts, [and] interventions” then the effects of those interventions could be judged beneficial or harmful. This would be preferable to focusing on understanding, which Magnus described as “a dead end.”
McGuire next asked if there is an ethical obligation in a study like NHANES to maximize participant autonomy, even if it could result in a more biased sample if people who do not want results are excluded. Nguyen noted that as a federal health survey, giving participants the choice of what they want is important, but the ability to pick and choose requires more resources than are currently available for NHANES. He said that every year NHANES gets a couple of participants who participate in NHANES but do not want to see their results. Magnus warned against associating autonomy with choice because having a choice means “you don’t know what the right thing to do is based on the right reason” and likened that action to a spasm, which is not necessarily an expression of autonomy. Instead, Magnus suggested that “we should be thinking about what impact does using certain words and engaging in certain communicative rituals, which we call informed consent, have on patient’s trust on their level of participation and the degree to which they feel respected.” He made another point that communication in language is a social activity, not necessarily
an individual one, because everyone does not need to understand a thing so long as other people in the community do understand it.
Relaying a question from the audience, McGuire asked Nguyen if NHANES does any formal assessments of understanding, cognitive impairments, or illiteracy. Nguyen responded that while NHANES does not do this at an individual level, it tries to address these issues in the study protocol by having certain questions posed through a computer-assisted self-interview, which reads the audio aloud and displays the text on the screen (“audio-CASI”). McGuire asked if Meyer or others have looked at using the eConsent process and technology, which has been shown to improve some aspects of understanding, for the return-of-results process. What technologies (e.g., virtual reality) might shape future discussions around informed consent and return of results? What types of technologies could enhance these processes? Meyer answered that she is unaware of any studies looking specifically at nontraditional ways of returning results. She noted that Geisinger did some work with chatbots and that the COVID-19 pandemic identified telehealth as an essential technology. Nguyen underscored that digital communications modalities are somewhat more challenging when considering confidentiality issues.
McGuire next turned to topics of community engagement and outreach, asking Nguyen if NHANES had elicited any community input on the NHANES practices and policies, and the extent to which practices and policies would evolve with public perspectives. Nguyen responded that while NHANES data collection practices and procedures are set, the engagement activities change because “every community is different.”
Magnus noted that those engagement strategies that have proven to be most effective are also more expensive. He reflected that the process that Meyer described that requires participants to learn about the study, go through the informed consent process, and take a quiz may lead to selection bias because “the people who are doing that are the people who have already pretty much decided to enroll in the research.” He added that the return of results can be a potential recruitment incentive.
Meyer commented that informed consent is required for most studies, so it makes sense to try to improve the process. She noted that other reasons to consider eConsent include reaching rural populations, scalability, resources, and standardization. Meyer next offered that community advisory boards (CABs) can be helpful when establishing procedures and policies for a research study. She recommended against selecting people from the community who “look an awful lot like the researchers themselves.” Instead, when establishing a CAB, Meyer suggested that researchers focus on what feedback they are trying to get and work hard to recruit CAB members who “really do look like the people in your community.” She remarked that one challenge of NHANES is that it does not have one single community
but rather 50 communities. Thinking aloud, Meyer offered the idea of randomly selecting a few communities to serve on mini-CABs, who would be rotated out over time to ensure that CABs continue to represent people from the community who are largely unfamiliar with research. Magnus agreed with Meyer and added that having CABs and participant advisory boards can benefit a study.
GENERAL END-OF-DAY DISCUSSIONS FOR SESSIONS 4 AND 5
Botkin opened the general discussion by reflecting that the workshop has shown a gap between the transfer of information to the participant and that participant’s ability to incorporate the findings into their health care effectively. He asked participants to provide their thoughts as to what degree the addition of a genetic component to NHANES would require the program to make operational changes. He offered a specific scenario to consider, in which NHANES returns some items on the findings list from the American College of Medical Genetics and Geonomics (ACMG) to individuals, some of which are quite urgent, some are somewhat less urgent. Would doing so help to address the pipeline issue? Is there any stronger ethical obligation for NHANES to make sure that those results are somehow translated to the care providers and the medical record compared with what is already being translated?
Nguyen responded first, saying that from the NHANES perspective, the ethical obligation of reporting clinically actionable results is the same whether it is a genetic or nongenetic result such as high cholesterol. “If there is something that somebody can do about it right now, whether it be based on seeking further care or getting another test or just follow with their medical provider, we feel like it’s important to provide that information to them right away,” said Nguyen. Then, responding to a follow-up inquiry from Botkin about the ethical obligation to ensure that information is understood and acted upon appropriately, Nguyen explained that for some results, NHANES does provide more information to participants. He offered an example of a high-arsenic result, which would indicate a possible environmental exposure but can also be expected for individuals who recently ate seafood. In this scenario, participants would receive a letter informing them of the potential for a high-arsenic level, what it means for their health, possible reasons for the abnormal result, and what they can do about it.
Magnus stated that it is not straightforward to apply the principles in genomics. He noted that there is not a consensus about which results are relevant to someone’s health. He reflected that looking across genome centers and clinical environments will reveal a lot of variation in where the line is drawn for actionability. “The ACMG ones usually require very high
penetrance, but it’s not obvious that that’s the right place to draw the line. There may be something with lower penetrance, but where it’s really important to know that, and that’s by health importance,” explained Magnus. Magnus added that health-related return of results from genomic sequencing is an FDA-regulated activity, which creates numerous other obligations in the pipeline, such as demonstrating cognitive understanding to ensure people will not make bad decisions when receiving genomic results.
Botkin turned next to the topic of genetic exceptionalism by raising a different question: If a genetic component is included in NHANES, will different types of professionals need to be involved in the consent process, can existing staff be trained on the genetic components? Meyer responded first by noting that because the concepts need to be described to the public in the most basic terms, she was not sure specialized expertise was necessary for a person facilitating the consent process. However, she urged that “there needs to be a lot of expertise involved in developing the process,” and there should be a safety net in the form of a genetic counselor who can be called upon when additional expertise is needed. Meyer reiterated that from her perspective, one of the benefits of eConsent is standardization, which allows experts to focus on “poring over that and really maximizing the content.”
Buchanan added that it also matters how likely an activity is to yield genetic results. He reminded the audience that the vast majority of participants (97%) will not receive genetic results, “and so we’re trying to balance the information that we give such that we don’t typically have that detailed genetics discussion at the time of consent because it won’t be relevant for the vast majority of participants.”
Natasha Bonhomme, planning committee member and founder of Expecting Health, agreed with Meyer. She added that training is not just needed for the genetics component, but also for reaching different communities, which presents an opportunity to map what training is needed at different stages from consent to return of results.
This page intentionally left blank.



















