Strategies to Enhance NIH-Funded Pediatric Research: Optimizing Child Health (2026)
Chapter: Summary
Summary1
Pediatric health is the cornerstone of the nation’s well-being. to: Increases in the U.S. average lifespan during the 20th century were in great part due to declines in child mortality from increased public health and sanitation and decreased infectious diseases, prematurity, trauma, cancer, and other health issues. These advances would never have happened without the significant and consistent federal investment in pediatric research, supported as a whole or in part by the National Institutes of Health (NIH).
Children today have more opportunities for health and longevity than at any point in history. Yet rising rates of chronic conditions, including obesity, anxiety, and other health challenges, signal that this progress is uneven and fragile. As a leader in supporting pediatric research, NIH has an opportunity to illuminate how rapidly evolving exposures and experiences shape child health trajectories. Through pediatric research investment, NIH can generate actionable knowledge that empowers families, clinicians, and communities to foster resilience, prevent disease, and optimize lifelong health. This report offers recommendations for how NIH, with the support of Congress, can best support research in pediatric health and improve the health of American children and individuals throughout the life course.
Children who grow up without the burden of chronic disease are more likely to thrive academically, socially, and professionally. Improving the health of all our children and adolescents will contribute to the development of the next generation of scientists, engineers, teachers, artists, and
___________________
1 This summary does not include references. Citations to support the text and recommendations herein are provided in the main text.
leaders who will drive the next wave of American progress. A healthy generation of children is the foundation of a resilient, innovative, and secure nation, directly influencing the state of the nation’s future workforce, military readiness, economic productivity, and societal stability.
STUDY TASK AND APPROACH
NIH tasked the National Academies of Sciences, Engineering, and Medicine (the National Academies) with convening an ad hoc consensus committee to examine NIH’s pediatric research portfolio and structure, as was mandated by Congress in 2024, along with examining
- the methods and rationale used in categorizing projects as pediatric research according to NIH’s Research, Condition, and Disease Categorization (RCDC) process;
- how pediatric components have been included or excluded from larger NIH initiatives;
- structural or process impediments to pediatric research applicants;
- how pediatric research priorities are established within and across NIH institutes and centers (ICs);
- how pediatric research activity is coordinated across ICs; and
- ways in which the NIH Clinical Center (CC) could be used to advance innovative pediatric research.2
The health of children is foundational to having a healthy, thriving society composed of healthy individuals across the life course. Health status changes across the life course, molded by biological, psychological, and social transitions; life’s turning points; physical and social exposures; and lived experiences. During the arc of the human life course, health is acquired, developed, optimized, sustained, and ultimately lost. Thus, health is emergent, relational, and ever-changing rather than a fixed state. This perspective is at the core of the life course developmental approach. The committee adopted this approach as a lens to understand child health and pediatric research, to shape the committee’s vision and goals for pediatric health research in the United States, and to develop the recommendations for improving NIH’s support of pediatric research.
___________________
PEDIATRIC HEALTH RESEARCH AT NIH: PAST AND PRESENT
NIH is the world’s largest public funder of biomedical research. Nearly all ICs led by The Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) fund pediatric research. The NIH Intramural Research Program (IRP), which accounts for 11 percent of its budget, also conducts pediatric research.
For nearly 100 years, consistent investment by the federal government has made NIH a global leader in scientific discovery and medical breakthroughs. NIH funding has supported numerous advances, including the development of the polio vaccine and tests for congenital disorders resulting from chromosomal abnormalities and genetic mutations. These breakthroughs created a groundswell of national interest in understanding and improving the health of children and led to the formation of NICHD in 1962. One of NICHD’s early priorities was to understand the impact of health care, the environment, family, and community systems on the healthy development of children, leading to advances in the prevention and treatment of neonatal conditions, novel treatments for childhood cancers, effective vaccines against infectious diseases, and more.
THE CURRENT CRISIS IN CHILD HEALTH
Despite advances in health and medicine, there is broad consensus among scientists, clinicians, and policy makers that child health is in crisis. Children in the United States are experiencing high incidences of chronic diseases and poor mental, emotional, and behavioral health. U.S. children are 80 percent more likely to die than their peers in European nations. The impacts of negative or positive exposures in early life are cumulative, so adults who experience poor health or adversity in childhood have substantially higher rates of a variety of costly chronic health conditions. Social and economic factors such as poverty, food insecurity, and poor access to health care also result in health inequities that imperil the health and future of many American children. A robust and coordinated NIH pediatric research portfolio is needed to address this multifaceted child health crisis.
THE CURRENT PEDIATRIC RESEARCH PORTFOLIO AT NIH
The committee used NIH Office of Budget data from fiscal year (FY) 2015 to FY 2024 to determine recent trends in pediatric research funding. In FY 2024, NIH spent $6.19 billion on pediatric research, of which 10 percent was intramural and 90 percent extramural. From FY 2015 to FY 2024, pediatric research expenditures increased by 70 percent, while NIH-wide total research expenditures increased by 62 percent. However, adjusted for inflation using the Biomedical Research and Development Price Index, growth in pediatric research and NIH-wide research expenditures flattened
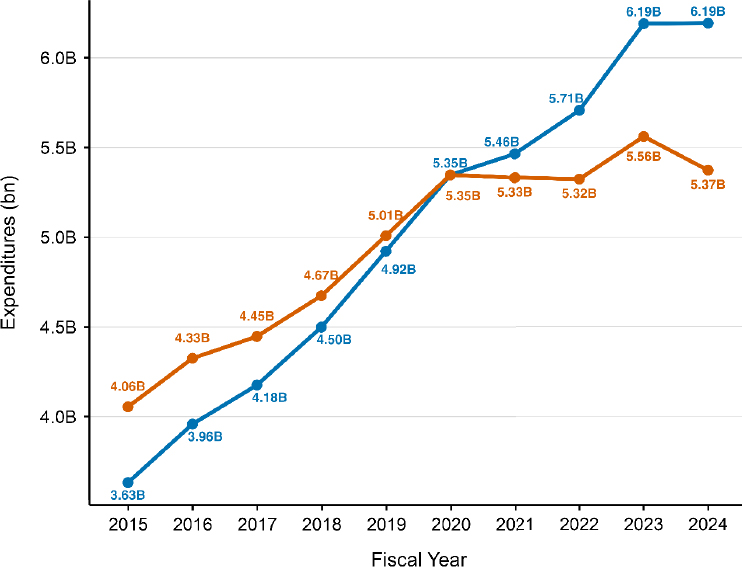
NOTE: FY = fiscal year; RCDC = Research, Condition, and Disease Categorization.
SOURCE: Committee’s analysis of data from the RCDC system, using the Biomedical Research and Development Price Index for inflation adjustment.
from FY 2020 through FY 2024 (see Figure S-1). Pediatric research has consistently accounted for 13 percent of the non-administrative NIH budget over the past decade (see Figure S-2), a smaller share than the 22 percent of the U.S. population represented by children.
All NIH ICs fund some amount of pediatric research, but five ICs—NICHD, National Cancer Institute (NCI), National Heart, Lung, and Blood Institute (NHLBI), National Institute of Mental Health (NIMH), and National Institute of Allergy and Infectious Diseases (NIAID)— account for the majority of those expenditures, with NICHD accounting for 17 percent of total pediatric expenditures across NIH. Across the 10-year period, the five health condition categories with the largest pediatric research expenditures were genetics, neurology, mental health, infectious diseases, and neonatal/perinatal. No broad pediatric health condition category was funded exclusively by a single IC, although a significant majority of research on childhood cancers and craniofacial/oral conditions was funded by NCI and the National Institute of Dental and Craniofacial Research, respectively.
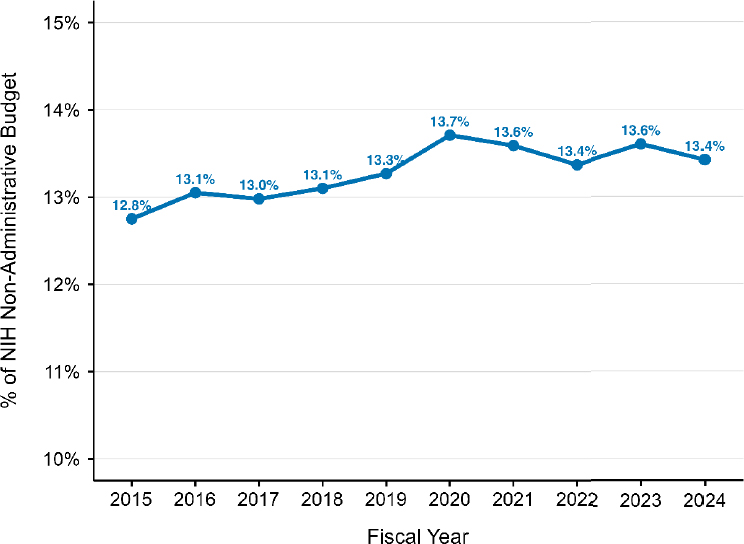
NOTE: FY = fiscal year; NIH = National Institutes of Health; RCDC = Research, Condition, and Disease Categorization.
SOURCE: Committee’s analysis of data from the RCDC system and data from NIH Office of Budget.
Although every IC funded some pediatric research, there was wide variation in the level of funding (see Figure S-3). Aggregating the total pediatric research funding across FY 2015–FY 2024, ICs were categorized into five tiers (bars). Tier 1 included a single institute, NICHD, which funded the plurality of research, accounting for 17 percent of NIH’s pediatric research expenditures. Tier 2 ICs included NCI (11 percent), NHLBI (10 percent), NIMH (10 percent), and NIAID (9 percent). Combined, Tier 1 and Tier 2 ICs accounted for the majority (57 percent) of pediatric research funding. The proportion of each IC’s total research budget spent on pediatric research varied widely, and the diversity of ICs that fund pediatric research suggests a continued need for NICHD leadership, which houses a substantial amount of pediatric expertise that other ICs can use.
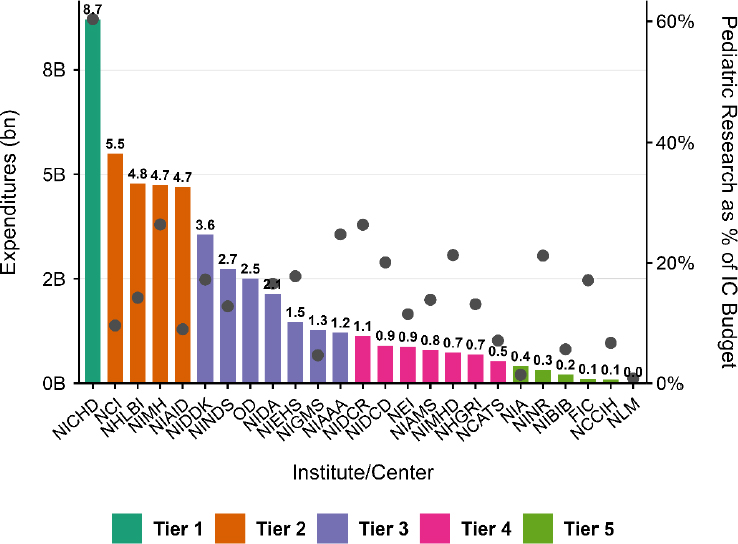
NOTE: FY = fiscal year; IC = institute or center; FIC = Fogarty International Center; MIAMS = National Institute of Arthritis and Musculoskeletal and Skin Diseases; NCATS = National Center for Advancing Translational Sciences; NCCIH = National Center for Complementary and Integrative Health; NCI = National Cancer Institute; NEI = National Eye Institute; NHGRI = National Human Genome Research Institute; NHLBI = National Heart, Lung, and Blood Institute; NIA = National Institute on Aging; NIAAA = National Institute on Alcohol Abuse and Alcoholism; NIAID = National Institute of Allergy and Infectious Diseases; NIBIB = National Institute of Biomedical Imaging and Bioengineering; NICHD = Eunice Kennedy Shriver National Institute of Child Health and Human Development; NIDA = National Institute on Drug Abuse; NIDCD = National Institute on Deafness and Other Communication Disorders; NIDCR = National Institute of Dental and Craniofacial Research; NIDDK = National Institute of Diabetes and Digestive and Kidney Diseases; NIEHS = National Institute of Environmental Health Sciences; NIGMS = National Institute of General Medical Sciences; NIMHD = National Institute on Minority Health and Health Disparities; NINDS = National Institute of Neurological Disorders and Stroke; NINR = National Institute of Nursing Research; NLM = National Library of Medicine; OD = Office of the Director. RCDC = Research, Condition, and Disease Categorization. The bars represent expenditures by the billion corresponding with the left y-axis. The dots represent the proportion of each IC total research budget that went to pediatric research corresponding with the right y-axis.
SOURCE: Committee’s analysis of data from the RCDC system.
The NIH RCDC System for Cataloging Pediatric Research
The RCDC system is used to place NIH-funded projects into spending categories for public reporting and ensures uniform coding of research grants and activities across NIH ICs. The RCDC system defines the “Pediatric” category as research “on health conditions that originate during the embryonic period through age 20.” The committee closely examined the methods and rationale used by the RCDC system in categorizing projects as Pediatric from FY 2015 through FY 2024. In FY 2024 there were 310 spending categories assigned to projects that were also assigned to the Pediatric category.
In a survey of 200 randomly sampled projects (20 projects per year from FY 2015 through FY 2024), the committee found that a small percentage of them were classified by the RCDC system as pediatric research even though the project presented no publicly accessible evidence of being pediatric research. Using the data available through the RCDC system, it was difficult to ascertain with any level of confidence which research studies were basic science and which were translational research.
Recommendation 3-23: The National Institutes of Health (NIH) should improve the Research, Condition, and Disease Categorization (RCDC) system to better assess funding for pediatric research by (a) adding the new spending categories and (b) improving the Categorical Spending webpage in the NIH Research Portfolio Online Reporting Tools (RePORT).
The following new spending categories should be updated:
- Add pediatric developmental stages: during pregnancy; neonate (≤28 days); infant (<1 year old); early childhood, age 1–2 years (1- to 2-year-olds) and age 3–5 years (3- to 5-year-olds); middle childhood (6- to 11-year-olds); adolescence (12- to 17-year-olds); and young adults (18- to 24-year-olds).
- Add a Basic Science spending category and ensure its validity.
- Add new terms for pediatric health conditions to better reflect the breadth of pediatric health conditions. The process to determine these new terms should include child health expertise from each institute and center.
- To improve specificity of diagnostic labeling, consider switching eponyms to indicate diseases—e.g., change Cooley’s Anemia to “Beta Thalassemia Major.”
___________________
3 The recommendations in this summary are numbered based on how they present in the chapters of the report.
To improve the Categorical Spending (RCDC) webpage in RePORT, NIH should
- Publish a reference paper that clearly and comprehensively describes the RCDC classification methodology with sufficient detail that it can be replicated or a similar assessment can be done by the scientific community. Update the methodology report whenever the methodology changes.
- Evaluate the validity of key RCDC terms, such as “pediatric,” and update the classification to improve accuracy and remove possible biases.
- Allow more than one RCDC term to be exported in a specific project. (This functionality currently exists in RePORTER, but not RCDC.)
- Enable download of all projects funded by NIH for a given year.
- Add a flag to clearly identify extramural; intramural; and, specifically, Clinical Center research and ensure that this information is available for all research projects.
- Add a search field that links projects to their respective notice of funding opportunity, program announcement, program announcement with special review, request for application, notice of special interest, or request for proposal.
PEDIATRIC RESEARCH AT THE NIH CC
The CC plays a critical role in supporting pediatric research, particularly for children with rare, complex, or currently untreatable diseases, and makes up most of the IRP’s research budget. The CC hosts clinical trials and natural history studies for many pediatric diseases and offers highly specialized wraparound care tailored for children in research protocols. Pediatric research at the CC includes gene, stem cell, and cellular therapies with an emphasis on deep phenotyping, genotyping, and novel therapeutic strategies. As of the first quarter of 2025, approximately one-third of the 1,500 active research protocols included children under the age of 18, and 80 protocols included children under 2 years old.
Recommendation 3-3: The National Institutes of Health (NIH) Clinical Center (CC) should continue to prioritize the current level of pediatric research, particularly on topics and using methods that are difficult to pursue in extramural environments (e.g., longitudinal studies of rare diseases and early-stage interventional trials) as well as on the long-term outcomes of interventions. Potential mechanisms include
- Increasing capacity while ensuring safety by overcoming operational constraints at the CC. Younger and more acute patient populations should be supported in early-phase interventional and observational protocols.
- Continued, expanded, or new partnerships with children’s hospitals, academic medical centers, schools, public health departments, and other large health centers across the country to best support pediatric populations.
- Offering pediatric education and training opportunities at the CC to continue to develop the specialized workforce needed to support this research.
- Collecting and presenting data in the annual report to the NIH Pediatric Research Consortium (or its equivalent) on the proportion of pediatric research studies, support, and usage by each institute and center at the CC.
PEDIATRIC RESEARCH PRIORITIZATION AND INCLUSION
The committee evaluated efforts to incorporate pediatric research priorities within and across NIH ICs, facilitators to this incorporation, and how challenges can be addressed, mitigated, or eliminated.
Two critical pediatric research facilitators are IC strategic plans and the NIH Pediatric Research Consortium (NPeRC).
NIH IC Strategic Plans
Each IC periodically creates a strategic plan to identify goals and priorities to drive its scientific research, build research capacity, and facilitate effective management of its intramural and extramural research. The committee evaluated current IC strategic plans and found that many research projects discussed in the plans emphasize the importance of treating the condition as early as possible to yield the best return on investment. In addition, most ICs prioritize research on chronic conditions and diseases that arise during childhood and continue into adulthood.
Though all ICs support pediatric research, only about half of IC strategic plans explicitly mentioned “pediatrics” or “children.” Within those plans, there were limited details about the strategic direction for research on child health; more often, pediatric research was embedded within larger strategic priorities, implicitly included in research “across the life course.” Importantly, some strategic plans do include specific pediatric research priorities. For example, NICHD mentions a focus on improving child and adolescent health and the transition to adulthood. Few IC strategic plans articulate exactly how success in achieving their goals is measured or monitored.
Recommendation 4-1: All directors of National Institutes of Health institutes and centers that fund research should explicitly incorporate pediatric health and potential downstream life course impacts into their strategic plans, as childhood chronic conditions, exposures, and experiences may have disproportionate health impacts into adulthood. Include metrics such as those focused on investigators (e.g., funding rates and career advancement), scientific discovery (i.e., publications and innovations), impact on child health (e.g., morbidity, mortality), and downstream life course impacts (e.g., premature cardiovascular disease) to measure success in meeting their goals.
In addition, the committee stresses that adopting a common definition for “pediatric research” will facilitate the integration of pediatric research into IC prioritization and strategic plans.
Recommendation 3-1: The National Institutes of Health should adopt and apply a consistent agency-wide definition of pediatric research. The definition should recognize that pediatric research may include studies that (1) involve data or specimens from or about infants, children, adolescents, or young adults; (2) inform the prevention, diagnosis, or treatment of conditions affecting these populations; (3) advance the health, well-being, or resilience of children, adolescents, or young adults; or (4) investigate childhood origins of adult health conditions.
NIH Pediatric Research Consortium
The NPeRC was created in 2018 to improve child health research collaboration and coordination by harmonizing pediatric research endeavors at NIH, identifying gaps in the pediatric research portfolio, and capitalizing on existing resources, infrastructure, and expertise to facilitate and promote pediatric health research across NIH. All work performed through NPeRC is done without explicit funding or resources. NPeRC members have historically represented 25 ICs, two research programs, and five offices and meet several times a year to develop workshops, review research programs and IC portfolios, discuss scientific opportunities and areas for collaboration, and promote research training for the next generation of pediatric researchers. NPeRC is an invaluable entity within NIH for facilitating and coordinating pediatric research. The committee believes that NPeRC is an excellent model for enhancing NIH-funded pediatric research but that it will benefit from having the financial resources and staff expertise to enable it to grow and have the capacity to continue its important work.
Recommendation 4-2: The National Institutes of Health (NIH) director should
- Elevate the NIH Pediatric Research Consortium (NPeRC) (or its equivalent) to the Office of the Director, with membership including senior leaders within each institute or center (IC) with pediatric health and life course expertise who systematically review all relevant components of strategic plans, including progress and impact made in the past year. Each senior leader should then report back to their IC and to the NIH director.
- Provide appropriate infrastructure funding and adequate resources (including personnel) to enable NPeRC (or its equivalent) to accomplish its goals and for its members to participate in its work, which includes (1) identifying and addressing research gaps, (2) enabling a nimble response to emerging threats to pediatric health, (3) promoting greater efficiency and reach of ongoing initiatives through data harmonization, (4) spearheading novel partnerships, (5) providing consultation to ambitious inter-IC initiatives, and (6) ensuring representation and visibility at national scientific meetings and societies.
- Have NPeRC’s membership (or its equivalent) include expertise in pediatric bioethics. NPeRC should also partner with patient advocacy or community representatives and develop a communications plan to disseminate pediatric research findings to both the scientific community and the general public. NPeRC (or its equivalent) should be prepared to coordinate the NIH-wide response to any emerging pediatric research needs.
FACILITATORS OF SUCCESSFUL INTER-IC INITIATIVES
Inter-IC pediatric health research initiatives are supported by two or more ICs and/or the Common Fund within the Office of the Director. Inter-IC initiatives have had success in addressing several significant pediatric health problems. In some cases, these initiatives have relied on NPeRC for support and expertise. Successful initiatives include adolescent brain development, environmental influences on child health, and pediatric participant-reported outcome measures, among others. Facilitators enabling the success of cross-IC pediatric research initiatives include the following: the originating research questions were developed collaboratively, by multiple ICs; those scientific questions raise issues inherently relevant to pediatric populations (and cannot be answered without inclusion of pediatric populations); processes and procedures were included to establish pediatric-focused scientific infrastructure; children were recruited and seen as integral
to the study from the beginning; and the initiatives received adequate and sustainable funding.
CHALLENGES TO CONDUCTING PEDIATRIC HEALTH RESEARCH
All types of health research routinely encounter challenges, including a finite pool of research funds and lengthy timelines between grant submission and final funding decisions. However, pediatric health researchers also face some unique legal and ethical, methodological, and structural challenges which often require more funding, time, or both to conduct pediatric research.
Legal and Ethical Challenges
Unique regulatory and legal requirements and ethical considerations impact research involving children. Children are considered a vulnerable population, which means that additional ethical and legal safeguards must be in place when conducting pediatric research. One challenge is ambiguity in the interpretation of regulatory requirements associated with different levels of risk to children who participate in a research study. To protect pediatric research participants, federal regulations impose varying requirements based on the research risks and whether those risks are justified by the prospect of direct benefits. However, institutional review boards (IRBs) often use restrictive interpretations of risk and benefit, resulting in study delays, redesign, or cancellation altogether. This occurs despite the existence of NIH’s Inclusion of Children policy and Inclusion Across the Lifespan policy, both of which require children be included in human subjects research unless there are scientific and ethical reasons that would prohibit their participation.
Another challenge is deciding when ethical concerns about pediatric participants are best addressed by incorporating additional safeguards, such as extended safety monitoring, to protect current and future participants and patients, as well as the balance of increased cost and complexity.
To mitigate these challenges, NIH can foster a culture of responsible inclusion of children in research, focused on protecting them through appropriate research rather than from research. NIH can provide the scientific community with clear guidance on ethical protections for children and require explicit articulation of scientific, legal, or ethical reasons for the exclusion of children in its funded research.
Recommendation 4-3: Initiatives within and across the National Institutes of Health (NIH) institutes and centers should coordinate with the NIH Pediatric Research Consortium (NPeRC) (or its equivalent) to include children and/or the downstream life course impact of childhood chronic disease, exposures, and experiences in studies in a strategic and deliberate way. NPeRC (or its equivalent) should support the enforcement of existing policies requiring that studies not exclude children or childhood downstream impacts on the life course without clear and adequate justification.
Recommendation 5-1: The National Institutes of Health (NIH) should work to create a culture of ethical inclusion of children in research, focused on protecting children through research rather than from research. To this end, NIH should develop measurable strategies and mechanisms to better implement and enforce existing policies to ensure inclusion of children at the project and proposal level. Strategies and mechanisms should include
- Updating the simplified review framework by explicitly considering the inclusion of children and its implications for health during the life course as a component of evaluating a proposal (i.e., its significance) during review.
-
Continuing to support the NIH Center for Scientific Review in implementing and monitoring structural changes to support pediatric research.
- Requiring and monitoring that pediatric representation is consistent with the number of applications on all relevant standing study sections.
- Ensuring provision of adequate justification for exclusion of children during grant review: If there is a scientific, legal, or ethical reason for the exclusion of children, this justification should be clearly articulated in the grant application and assessed and documented during the grant review process.
- Elevating prioritization of implications of research on the life course during scientific review: NIH should identify the impact of pediatric research on the life course as an important component of a proposal’s significance section and should do so directly within reviewer guidance. In addition, training for study section reviewers should encourage them to consider whether a proposal adequately addresses the importance of the research for the life course when evaluating the significance or impact of extramural grant applications.
- Improving transparency on inclusion: The Office of the Director of NIH should annually track and report justifications provided for the exclusion of children. This information should be included in the NIH annual report and published on the NIH Pediatric Research Consortium (NPeRC) website, or an NPeRC equivalent website, to track progress on the improved inclusion of children across NIH activities over time.
- Providing clearer institutional guidance about the ethical inclusion of children in research: NPeRC (or NPeRC equivalent), in consultation with the NIH Clinical Center’s Department of Bioethics, should develop a widely accessible toolkit and guidance on ethical issues in pediatric research that have the potential to unduly impede research if misunderstood, such as when to include children in research, provisions for assent, adolescent independent consent, age de-escalation, and payment for research participation.
Scientific Challenges
The physiology and behavior profiles of children, the complexity of diseases that affect children, and the limitations in current research models and scientific approaches for fully unraveling the intricacies of pediatric diseases are also challenges.
Developmental growth and maturation differ between children and adults. Disease and injury risk, progression, and treatment responses may differ due to these developmental stages, making it difficult and sometimes inappropriate to translate adult disease models to pediatric populations. In addition, pediatric models often need to account for age-specific factors such as hormonal changes, brain development, and skeletal maturation, which may not be well represented in animal models or adult human models.
Health outcomes in children are shaped by a complex interplay between environmental exposures and genetics and vary across populations. Pediatric models need to incorporate a wide variety of genetic mutations, which can make the models complex and difficult to study. Environmental factors can influence disease development and response to treatment in children, but these factors are difficult to incorporate into animal or laboratory models. These factors are embedded within broader social and structural contexts that influence children’s development and disease risk.
Disease can also have a significant impact on normative developmental processes. Chronic illness in childhood affects cognitive, emotional, and social development, and these impacts can complicate the study of disease progression and treatment. The psychological burden of disease may affect
children’s ability to participate in clinical trials or models. Furthermore, pediatric disease models often need to consider long-term quality of life outcomes, which can be harder to measure and predict in young patients and require longitudinal study.
Methodological Challenges
Research studies that include human participants include several methodologic considerations which take on an additional complexity when children are a part of the study, including in participant recruitment, the number and diversity of participants, and data collection and measurement. These challenges are more than just considerations for good study design. Left unaddressed, they generate structural barriers to pediatric representation in research.
Recruiting and retaining children in clinical trials is often more difficult than recruiting and retaining adults. Parents or guardians are essential participants in recruitment and study processes, meaning that successful pediatric recruitment requires both building rapport with and educating participants as well as parents or guardians about the study. There is often a lengthier decision-making process among participants in pediatric research than in adult research, and additional time may be needed to obtain a child participant’s assent. Pediatric clinical research is often conducted at urban medical centers, making it difficult for families living in rural and underserved areas to participate. Language barriers may dissuade families from participating in research if adequate interpretation or translation services are not offered. Finally, rare disease studies are a cornerstone of pediatric research, but low prevalence precludes recruitment and enrollment targets on par with adult studies.
Ensuring that the results of pediatric research are generalizable across diverse populations is critical. Many children live in families in which members may have limited English proficiency. Children from rural areas and those living in poverty face distinct health risks and barriers to accessing health care. These children are often underrepresented in clinical trials, so their specific needs and treatment responses are less understood. To increase the participation of rural, underserved, and non-English speaking children and families, flexibility, multilingual resources, and increased collaboration with communities are needed.
Pediatric researchers face several data collection challenges. Longitudinal data collection may be required to be able to observe relevant outcomes across the life course, and data collection mechanisms often need to evolve as participants transition from childhood to adulthood. Many research tools have not been validated across all age groups. Additionally, outcomes in childhood are best understood within the broader context of family and
household factors, where parental health, caregiving practices, and family stressors strongly shape child development and well-being. Capturing these interdependencies requires approaches that extend beyond the individual child to include the larger family unit, but established standards for dyad- or family unit–based data collection are lacking. Studies relevant to child health may have a longer trajectory in reporting groundbreaking findings, something that must be acceptable to many, including Congress. Pediatric research projects and funding should not be shortchanged due to the more expensive nature (infrastructure needs) and a longer timeframe needed to attain fruitful results.
Trust is critical in pediatric research, given that parents or guardians choose to enroll their children, and not themselves, in a study that may pose risk. Entire communities may be deterred from participating in pediatric research if researchers do not practice cultural humility and language justice. Others may mistrust the larger research enterprise because of historical harms done to their communities in the name of science. These concerns and issues of mistrust may be mitigated through meaningful engagement of communities in the research process. The development of lasting trust is increasingly recognized as a component of research that is ethically important and a facilitator of increased participation. Community-based participatory research, the use of patient and family advisory councils, and other robust community-engagement methods could help increase trust, ensure that researchers address actual community concerns, and ultimately ensure the success of pediatric research for all communities.
There are also unique challenges for pediatric health services research. Pediatric health care delivery systems and financing are unique in workforce, geographic distribution, policy, and financing. Financing and policy for children are determined much more at the state level than at the federal level due to the large proportion funded by Medicaid rather than Medicare. Databases commonly used in adult research (Medicare, Veterans Affairs) are not relevant to children, requiring instead that other databases, such as state Medicaid records, be used. These factors require pediatric expertise, data, and funding to answer key questions in child health services research.
Structural, Procedural, and Financial Challenges
Pediatric researchers face an array of unique challenges during the grant application and review processes. While all investigators who seek NIH grant awards grapple with protracted timelines, studies that include children often face an extended period of review due to concerns about additional safeguards for children as a vulnerable population. Pediatric expertise can vary widely among reviewers in a study section, potentially leading to inadequate reviews and lower prioritization of pediatric research.
Funding for pediatric grants may not meet the actual costs required for pediatric trials, which can be more expensive and logistically complex than adult trials. The pediatric population available for study for many diseases is significantly smaller than the available population for adult studies, since most children are healthy. Thus, pediatric research studies, especially for rarer conditions or diseases, often have multiple study and recruitment sites, requiring greater infrastructure costs and time—for example, for multiple IRB reviews or to develop a consortium agreement among the institutions.
Due to the accelerated pace of development in childhood and critical periods which creates the potential for delayed outcomes from interventions, it may require multiple sequential studies to ensure generalizability across pediatric populations.
Researchers should also plan to compensate parents or guardians for missed work time and travel to enrollment sites. Additional research time may be needed if data collection includes parents, siblings, and the children enrolled in the study, which is often the case for pediatric studies.
Recommendation 5-2: National Institutes of Health (NIH) institutes and centers should award pediatric research grants and budgets that support the specific needs of pediatric studies. In addition, to address the mismatch between study timelines and funding cycles, NIH should
- Allow for extended or extendable award timelines and/or renewable grant mechanisms specifically designed for pediatric research, allowing investigators to sustain long-term studies that align with children’s developmental trajectories;
- Provide higher budget maximums to account for the need for representative recruitment and multi-center studies, when scientifically justified;
- Create supplemental funding opportunities specifically designed for longitudinal or follow-up data collection, which would enhance learning across the life course while capitalizing on previously funded and ongoing studies;
- Provide funding supplements to support multilingual research and community engagement to facilitate representation for generalizable results; and
- Increase access and usage of the Clinical and Translational Science Awards as a mechanism for promoting pediatric research.
A VISION FOR THE FUTURE OF PEDIATRIC HEALTH RESEARCH AND CHILD HEALTH
The committee envisions the United States as a global leader in promoting child health, preventing childhood diseases, reversing recent declines in
child health, and applying scientific discoveries through a robust, dynamic, and integrated pediatric research program at NIH.
To actualize that vision, the committee created four goals (see Figure S-4) that served as guideposts for the formulation of its conclusions and recommendations. These goals will ensure that all children are supported, resilient, and thriving across the life course.
The committee sees an opportunity for NIH to lead the United States out of the current crisis in child health to a brighter future. NIH has an opportunity to reaffirm the unique value of pediatric research to the health and well-being of children and, because children are the future, to demonstrate the significant return on investment that the nation gains in health, prosperity, opportunity, innovation, and growth by prioritizing pediatric health research that is comprehensive, equitable, and groundbreaking.
The future of pediatric research will be shaped not only by scientific innovation but by the willingness of leaders to steward public resources wisely, build cross-sector coalitions, and keep children at the center of national health priorities. NIH is uniquely positioned to lead this effort, aligning research to public concerns and demonstrating and communicating impact from the laboratory to the community. A renewed commitment to child health research is not an expansion or a transformation per se—it is a reorientation: toward value, impact, and a future in which every child can thrive. America’s children are worth the investment.
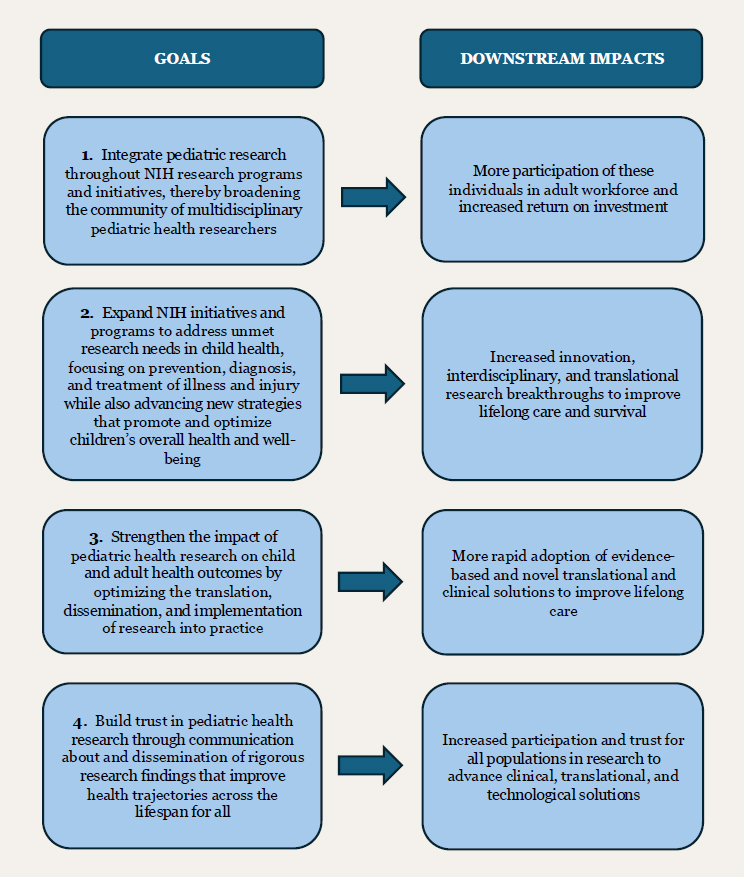
NOTE: NIH = National Institutes of Health.
This page intentionally left blank.



















