Strategies to Enhance NIH-Funded Pediatric Research: Optimizing Child Health (2026)
Chapter: 1 Introduction
1
Introduction
The goal of pediatric health research is to understand, prevent, and treat diseases and conditions primarily affecting children, adolescents, and young adults. This research is vital to ensuring healthy development, advancing medical knowledge, and informing evidence-based public health policy. It also illuminates our understanding of the underlying causes of disease and guides the development of treatments and cures. Because children have unique and rapidly evolving physical and socioemotional needs, pediatric health research helps tailor treatments and prevention strategies to be safe and effective for them. It also generates data and evidence that support public policies and programs such as care for children with medical complexity, nutrition guidelines, and injury prevention. Pediatric research addresses health gaps and environmental influences of health such as family environment, socioeconomic status, and chemical exposures by identifying risks and effective interventions. Since many adult health conditions originate in childhood or prenatally, early identification and prevention measures based on pediatric research can improve lifelong health outcomes.
STUDY BACKGROUND AND CONTEXT
The National Institutes of Health (NIH) is the world’s largest medical research agency and public funder of biomedical research (NIH, 2025b). NIH supports scientific discovery through intramural research and extramural grants and contracts to institutions across the United States. NIH’s mission is “to seek fundamental knowledge about the nature and behavior of living systems and the application of that knowledge to enhance health,
lengthen life, and reduce illness and disability” (NIH, 2025d). NIH supports pediatric research across basic, translational, and clinical science, with more than $6.19 billion invested in fiscal year (FY) 2024. Nearly all NIH institutes and centers (ICs) fund pediatric research, led by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), which accounts for about 17 percent of all pediatric research funded by NIH (see Chapter 3). Other key funders of pediatric health research at NIH are the National Cancer Institute; National Heart, Lung, and Blood Institute; National Institute of Allergy and Infectious Diseases; and National Institute of Mental Health. NIH pediatrics research funding increased steadily from FY 2015 to FY 2024, with a cumulative increase of 70.52 percent in real dollars and by 28.72 percent in inflation-adjusted dollars, though the spending power has flattened since 2020 (see Chapter 3 for more detail).
Along with its extensive support for extramural research, NIH also conducts pediatric studies within its Intramural Research Program (IRP), which accounts for 11 percent of the NIH budget (NIH, 2025a). The NIH Clinical Center is the world’s largest research hospital, and, as a major component of the IRP, it hosts around 560 current research studies involving children (NIH Clinical Center, 2023). Approximately half of these are natural history studies of disease; the rest test new therapies, including first-in-human or pediatric-first trials.
To facilitate and improve coordination of pediatric research across NIH, the NIH Pediatric Research Consortium (NPeRC) was launched in 2018 (NICHD, 2025b). Although NPeRC has no direct funding or research authority, it facilitates cross-IC collaboration on the research and development of pediatric devices, clinical trials, pediatric-to-adult health care transitions, and COVID-19, among many other important pediatric research subjects. The NPeRC membership includes representatives from 25 ICs, five offices, and two research programs, All of Us and Environmental Influences on Child Health Outcomes (NICHD, 2025b). NPeRC is currently chaired by the director of NICHD’s Division of Extramural Research. NICHD’s progress has been highlighted in several of NIH’s recent congressional justifications (NICHD, 2023), including NPeRC’s efforts to identify research gaps and opportunities that arise when adolescents with chronic conditions transition to adult health care (2023), efforts to address COVID and long COVID issues among pediatric populations (2024), and efforts to improve the development of pediatric medical devices (2025) (NICHD, 2023, 2024, 2025a).
The mechanism used to track NIH spending, the Research, Condition, and Disease Categorization (RCDC) system, was initiated in 2009 after the National Institutes of Health Reform Act of 2006. The RCDC system categorizes NIH-funded projects into non-mutually exclusive scientific
“spending categories” for public reporting (see Chapter 3 for further detail). The NIH Research Portfolio Online Reporting Tools (RePORT) website provides access to a variety of reporting tools, datasets, and analyses on NIH-funded research as well as research funded by other federal agencies, such as the Administration for Children and Families, the Agency for Healthcare Research and Quality, the Centers for Disease Control and Prevention, the Health Resources and Services Administration, the Food and Drug Administration, and the Department of Veterans Affairs (NIH RePORT, 2025). The RePORT Expenditures and Results module (RePORTER) provides searchable access to NIH-funded projects, publications, and patents (see Chapter 3 for further detail).
PROJECT ORIGIN AND STATEMENT OF TASK
In 2024, NIH requested that the National Academies of Sciences, Engineering, and Medicine (the National Academies) examine NIH’s pediatric research portfolio and structure, as was mandated by Congress in an amendment to the Appropriations Act of 2024.1 In response, the National Academies formed the Committee on Strategies to Enhance Pediatric Health Research Funded by NIH. The sponsor’s charge to the committee is presented in Box 1-1.
SIGNIFICANCE OF PEDIATRIC HEALTH RESEARCH
Children are not just small adults, and they are our future. Children grow, develop, and respond to the world in ways that are completely different than adults, and they are entirely dependent on the adults in their lives to help keep them safe and healthy. We need research that’s specifically focused on them to truly understand what makes them sick but also what helps them thrive.
– Participant in the committee’s call for perspectives
Pediatric health research is vital for advancing our understanding of childhood diseases and developmental processes, leading to more effective, age-appropriate treatments and preventive strategies. Because children represent the future of our country’s economy, its cultural fabric, and its success on the global stage, pediatric health research is also essential for the future vitality of the United States. Child health directly impacts physical and mental health across the entire life course. It lays the foundation for lifelong health by identifying interventions that can improve outcomes from
___________________
1 Further Consolidated Appropriations Act, 2024, Public Law 118-47, 118th Cong., 2nd sess. (March 23, 2024). See also https://www.nationalacademies.org/en/ocga/public-laws/further-consolidated-appropriations-act-2024 (accessed July 10, 2025).
BOX 1-1
Statement of Task
The National Academies of Sciences, Engineering, and Medicine (NASEM) will convene an ad hoc committee to examine pediatric research supported by NIH, as described below. The committee will consider the perspectives of multiple NIH institutes and centers (ICs) in its deliberations, as pediatric research is conducted throughout NIH.
The committee is tasked with examining the current NIH pediatric research portfolio and structure including:
- The methods and rationale involved in categorizing projects as “Pediatrics” research using the Research, Condition, and Disease Categorization Process;
- How pediatric components have been included or excluded from larger NIH initiatives;
- Structural or process impediments to pediatric research applicants;
- How pediatric research priorities are established within and across ICs; and
- How pediatric research activity is coordinated across NIH ICs.
Based on this review, the committee will make recommendations focused on improving NIH’s overall support of child health research. Any recommendations for structural or process changes should include consideration of burden (including financial) on both researchers and NIH staff.
The committee may also consider ways in which the NIH Clinical Center (CC) could be used to advance innovative pediatric research (e.g., whether it would be advantageous to expand the ages eligible for research studies, areas of science uniquely suited to being conducted at the NIH CC, and potential partnerships to expand the research portfolio at the CC).
infancy through adolescence and beyond. Therefore, it is critically important that children receive adequate and appropriate care in childhood that optimizes their health, enabling them to thrive as children and setting them up for optimal health as adults. This kind of care would not be possible without advances in pediatric health research.
In the United States, there is broad consensus among scientists, clinicians, politicians, and public health officials that there is a current crisis in child health (Forrest et al., 2025; HHS, 2025; NASEM, 2024). Children are experiencing high incidences of chronic diseases (obesity, asthma, diabetes,
etc.) as well as poor mental, emotional, and behavioral health (Heffernan and Macy, 2025; NASEM, 2019, 2024). A series of studies conducted in the second half of the 20th century established the importance of in utero and early child health on the trajectory of health over the life course (van den Broek and Fleischmann, 2019). Malnutrition during pregnancy increases the risk of adult coronary artery disease and premature brain aging, as shown by studies of adults born during the Dutch Famine of World War II (Franke et al., 2018). Studies of adverse childhood experiences (ACEs) demonstrate the cumulative effects of these events on the risk of adult depression, substance abuse, obesity, hypertension, and diabetes (NIH RePORT, 2025; Roseboom et al., 2006; van den Broek and Fleischmann, 2019; Webster, 2022). The seminal report From Neurons to Neighborhoods summarized the biological effects on the brain of early life events that affected later cognitive ability and mental health (IOM and NRC, 2000). Most importantly, research has not only uncovered these causal effects but also shown that interventions in utero, infancy, and early childhood will have effects throughout the life course; the impacts of negative or positive exposures in early life are cumulative, and adults who experienced poor health or adversity in childhood have substantially higher rates of a variety of costly chronic health conditions (NASEM, 2019, 2024). However, these outcomes across the life course are not fixed, as research has also demonstrated that individual exposures, choices, and resilience can modulate risk over time (NASEM, 2019).
The health and well-being of too many American children are being imperiled by social influences of health such as poverty, food insecurity, and poor access to health care. According to the American Community Survey, based on family income in 2022, the rate of child poverty in the United States was 16.3 percent, 3.7 percentage points higher than the overall rate of poverty (U.S. Census Bureau, 2023). These rates vary by demographic characteristics, such as geographic location and race/ethnicity. For example, in 2022, “9 of 17 states in the South region had child poverty rates of 18.0 percent or more,” compared with only one state each in the Midwest, Northeast, and West regions (U.S. Census Bureau, 2023). According to a 2023 analysis of data that estimated the overall child poverty rate at 16, child poverty was lower than the overall average among non-Hispanic White and Asian and Pacific Islander children (10 percent among both groups) and higher among American Indian or Alaska Native, Black, and Hispanic or Latino children (27, 29, and 22 percent, respectively) (Annie E. Casey Foundation, 2024). Often associated with factors such as poor living conditions, lack of insurance, and lack of access to healthy food, poverty can give rise to a variety of health problems.
These barriers to health and well-being, as well as gaps in our knowledge of pediatric health, have important consequences. Forrest and
colleagues found that children’s health steadily worsened in the United States between 2007 and 2023 across multiple domains including mortality; chronic physical, mental, and neurodevelopmental conditions; functional status; and physical and emotional symptom domains (Forrest et al., 2025). During the same time period, the study found that infants were 78 percent and 1- to 19-year-olds were 80 percent more likely to die compared with children in comparable high-income countries (see Figure 1-1). Pediatric research is critical to a life course approach to health, offering insights into early-life origins of disease, prevention strategies, and interventions that can reduce chronic illness and improve outcomes well into adulthood (Speer et al., 2023). Poor health and disability affect one’s ability to participate in the workforce, military, and society overall, affecting health care expenditures, the economy, national security, business viability, and public finances (NASEM, 2019). These observations underscore the need to sustain investment in pediatric science as a foundation for improving population health. With declining child health in the United States, the need for pediatric research and innovation has never been more critical (Forrest et al., 2025).
If we don’t take steps now to build a strong, healthy foundation for our young people, then it will not just be our military that pays the price—our nation as a whole will suffer also.
– Richard R. Jeffries, Rear Admiral, U.S. Navy (Retired) and former medical officer of the U.S. Marine Corps
For nearly 100 years, NIH has led the way in biomedical research. The federal government’s interest in improving the health of its citizens, its consistent appropriations, and its recognition that basic and clinical research are essential to life-changing medical advances have made NIH and the U.S. biomedical community global leaders in advancing scientific discovery and medical breakthroughs.
Challenges to Conducting Pediatric Health Research
Pediatric health researchers encounter unique medical, ethical, logistical, and scientific considerations due to the vulnerability and rapid development of children. As a result, in comparison with health research for adult populations, pediatric health research requires the inclusion of age-appropriate methods, additional protection in the informed consent process, and specialized designs of clinical trials (NIH, 2025c; Shah, 2021). These factors shape the pediatric research landscape and contribute to ongoing challenges in conducting pediatric research, such as funding levels that are not commensurate with either disease burden or the timelines needed to conduct pediatric health research. These issues and challenges are explored further throughout the report, especially in Chapter 5.
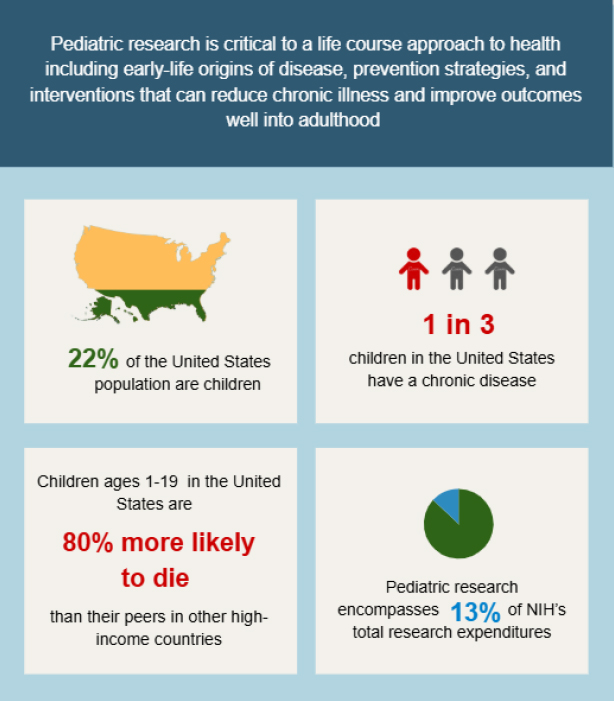
NOTE: NIH = National Institutes of Health.
SOURCES: Data compiled from Forrest et al. (2025) and NASEM (2024).
Several historical cases of ethically problematic research led to the creation of the National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research in 1977 and the passage of regulations intended to ensure the ethical conduct of research for all participants, including children (Shah, 2021). An unintended consequence of this history is that a protectionist mentality has taken hold (Levine, 1988). Described by Carol Levine as “born in scandal and reared in protectionism,” the research oversight system responded to a troubling history by focusing on protecting children from research rather than through research (Levine, 1988). Clinical care guidelines for children are often based on data from adults, resulting in care that is not optimized for children and which may be ineffective or even harmful (Petkova et al., 2023). Furthermore, without research to support
the evidence and approval for the use of many interventions, clinicians caring for children too often are forced to rely on guesswork or to extrapolate from data in adults in ways that can fail to benefit children or even harm them in some cases (Joseph et al., 2015; Klassen et al., 2008; Nardini, 2014; Sinha et al., 2008).
Pediatric health research has led to significant benefits for children and society (see Table 2-1). However, as Chapter 5 of this report discusses in more detail, inadequate communication about these achievements, lingering mistrust due to the historical cases of medical abuse, and a lack of thoughtful community engagement in research have created a gulf between the public and the pediatric health research community. To foster trust and carry out the research needed to fill the gaps in our knowledge of pediatric health, the pediatric health research enterprise needs to bridge this divide. Community engagement, including the engagement of youth, improved dissemination of research, and communication about the benefits of pediatric research to children and the nation at large, is a critical component of successful pediatric research (see Chapter 5 for more on engaging communities in the research process).
STUDY APPROACH
The Committee on Strategies to Enhance Pediatric Research Funded by NIH included 17 members with a range of expertise in basic, clinical, and translational pediatric research; pediatric health services research; biostatistics; pediatric health science policy; bioethics; pediatric health disparities; patient advocacy; and NIH research programs. Biographical information for each member can be found in Appendix A.
The committee held five 2-day hybrid meetings and multiple virtual meetings between December 2024 and September 2025 to gather information, consider findings, and develop recommendations. Several of the committee’s information-gathering sessions featured invited speakers from NIH, who shared valuable insights into the current state of the pediatric health research funding landscape, how NIH prioritizes and impacts pediatric health research, how the various NIH ICs contribute to pediatric health research in their respective health fields, and how the RCDC and RePORTER systems catalog and track pediatric research (see the open session agendas in Appendix B). NIH speakers also discussed some of the challenges they encounter in reviewing, funding, and tracking pediatric research. The committee issued two calls for perspectives (CFPs) through the project webpage: one for input and perspectives from research applicants on the challenges that they face in obtaining funding for pediatric research, how they have approached incorporating pediatric populations into their work, and any real or perceived barriers to conducting such research, and a
second for research participants and families that have participated in NIH research studies. The full list of CFP questions is provided in Appendix C.
The committee reviewed existing literature to inform its analysis. This included peer-reviewed scientific articles as well as publications from public agencies, private organizations, and governmental bodies, with a focus on materials published from 2010 to the present. The review centered on U.S.-based research and covered a wide range of topics relevant to pediatric science, including federal mandates related to pediatric research, trends in funding, notable successes in the field, and barriers that researchers face in entering or remaining in pediatric research, such as difficulties securing funding, limited job opportunities, and attrition from the research workforce. Both extramural and intramural research activities were considered, including studies conducted at the NIH Clinical Center. The committee also reviewed literature referencing the RCDC system, particularly regarding challenges in accurately categorizing pediatric research within this taxonomy. Search terms covered age groups from birth through adolescence, including “child,” “lifespan,” “adolescent,” and “young adult.”
Vision and Goals
This report examines how pediatric research is defined and tracked, its inclusion in NIH-wide initiatives, barriers faced by pediatric investigators, how priorities are set, and coordination mechanisms, culminating in recommendations for strengthening NIH support for child health research. The committee’s vision for the future of NIH pediatric research and the goals to achieve this vision are in Box 1-2.
Life Course Developmental Perspective
The committee used a life course developmental perspective as a lens through which child health and pediatric research are understood. The term “life course” is preferred over “lifespan” (duration of life) or “life cycle” (biological maturation from child to adult form) because it emphasizes the dynamic, developmental, and contextual processes that shape health over time (Alwin, 2012). Health is not static but changes across the life course, molded by biological, psychological, and social transitions; life’s turning points; physical and social exposures; and lived experiences. NIH funds research on individuals at various points in the lifespan. Pediatric research is unique because of the effects of child health over the life course.
Health is acquired, developed, optimized, sustained, and ultimately lost across the human life course. It arises through developmental and relational processes produced by continuous interactions between an individual (I)
BOX 1-2
The Committee’s Vision and Goals
The United States will be the global leader in promoting child health, preventing childhood diseases and morbidity, reversing recent declines in child health, and using scientific discoveries through a robust, dynamic, and integrated pediatric research program at NIH. These goals will ensure that all children are supported, resilient, and thriving across the lifespan. To accomplish this vision NIH would do the following:
GOAL 1: Integrate pediatric research throughout NIH research programs and initiatives, thereby broadening the community of multidisciplinary pediatric health researchers.
GOAL 2: Expand NIH initiatives and programs to address unmet research needs in child health, focusing on prevention, diagnosis, and treatment of illness and injury while also advancing new strategies that promote and optimize children’s overall health and well-being.
GOAL 3: Strengthen the impact of pediatric health research on child and adult health outcomes by optimizing the translation, dissemination, and implementation of research into practice.
GOAL 4: Build trust in pediatric health research through communication about and dissemination of rigorous research findings that improve health trajectories across the lifespan for all.
and the ecosystems (E) in which that person lives, grows, learns, works, and ages. These I⇔E interactions, which span multiple levels—from the inner world of mind–body functioning to families, communities, and the global environment—constitute the dynamic foundation of health development. This perspective positions health as emergent, relational, and ever-changing, rather than as a fixed state, and this perspective is at the core of the life course developmental approach (Halfon et al., 2018).
Life course development recognizes that experiences may have disproportionate effects when they occur during sensitive or critical periods of life, may accumulate incrementally over time, and may occur sequentially in ways that amplify or mitigate earlier exposures. In each case, the timing, duration, and sequencing of exposures interact with individual biobehavioral systems and context to shape outcomes. First, the health effects may manifest within minutes (e.g., a toxin exposure), years (e.g., obesity trajectories), or decades (e.g., ACEs) (Felitti et al., 1998; NASEM, 2019). Second, health emerges from interactions within relational networks that include people, technologies, objects, non-human living beings, and physical and
social settings. These networks create flows of resources, stressors, and supports that channel developmental outcomes. Third, life course development emphasizes the biobehavioral mechanisms and regulatory systems, including epigenetic, neural, physiological, and behavioral processes, through which exposures and experiences are transduced into patterns of mind–body functioning (Aristizabal et al., 2020; NASEM, 2019).
Although development occurs over the full life course, it occurs most rapidly during childhood. These rapid changes set the foundation for adult health. Childhood is a time of both resilience and vulnerability. It is when sensitive periods are most common, a period of life when health can be shaped in both positive and negative ways with short-term and long-term implications. In fact, childhood itself can be considered a sensitive period, which is one of the chief reasons that the United States needs a concentrated focus on research on child health. Therefore, beyond understanding childhood health-related issues, it is critical to understand the downstream life course impacts of childhood chronic diseases, exposures, and experiences on adult populations (see Figure 1-2).
Life course development views health not as a static state but as a set of interrelated trajectories, each reflecting the patterns and trends of specific health attributes (e.g., longevity, diseases, mind–body functioning, and distress). These trajectories are not linear; they are shaped by an individual’s interactions with the physical and social environments, and they can accelerate, plateau, or decline, shaped by resilience and disruption. From this perspective, health development is a continuous, cumulative, and adaptive process, in which childhood provides the foundational structures and capacities that enable—or constrain—human health across the remainder of life.
Previous Work of the National Academies
Over the past decade, the National Academies has published several reports that examine factors influencing pediatric research and child health and recommend ways these can be improved. Because this report focuses specifically on enhancing NIH-funded pediatric research, readers may find these other reports, which focus more on recommendations for broader policies that influence pediatric health, of interest as well. Many previous studies and reports have relevance to this study, and several are referenced in this report. Some recent National Academies’ reports focused on pediatric health and research and NIH’s research portfolio include the following:
- A New Vision for Women’s Health Research: Transformative Change at the National Institutes of Health (2025)
- The Future Pediatric Subspecialty Physician Workforce: Meeting the Needs of Infants, Children, and Adolescents (2023)
- Launching Lifelong Health: Supporting Children, Youth, and Families for a Thriving America (2024)
- Childhood Cancer and Functional Impacts Across the Care Continuum (2021)
- Vibrant and Healthy Kids: Aligning Science, Practice, and Policy to Advance Health Equity (2019)
- The Promise of Adolescence: Realizing Opportunity for All Youth (2019)
Data Limitations and the Changing Research Environment
The committee encountered several challenges in assessing the scope of pediatric research supported by NIH. One involved limitations on available data. Age tagging of grants is not consistent among ICs, and differences in how ICs track and report their work in general make it hard to get a clear picture of the details of pediatric research supported by NIH. A second challenge was tied to new technologies, emerging health issues, and evolving research priorities. These important developments mean that “pediatric research” is a constantly evolving category of work. The committee has attempted in this report to provide a snapshot of current pediatric research in the United States through the lens of NIH. The report also builds on the committee’s vision and goals so that as pediatric research evolves, its North Star remains, ensuring that all children are supported, resilient, and thriving across the life course.
TERMS USED IN THIS REPORT
Pediatric Research
Pediatric research addresses “fundamental knowledge about the nature and behavior of living systems and the application of that knowledge to enhance health, lengthen life, and reduce illness and disability” among individuals who have not yet reached an adult level of biological or socioemotional maturity (NIH, 2025d). There are myriad opportunities at NIH to define or categorize “pediatric research,” many of which are used to suit the needs of different ICs, consortia, or reporting groups. While NIH uses a strict definition of “child” as far as participation in research—that is, a child is any individual younger than 18 years old (NIH Office of Extramural Research, 2015)—it does not strictly define the concept of pediatric research.2 Instead, it offers three categories of research that may be categorized as “pediatric” by the RCDC tool. These include
- a study in which the research participants do not specifically exclude children;
- a study in which the research participants specifically include children; and
- a study in which the research aims, and clinical or public health relevance, focus on conditions or developmental processes that typically originate and manifest in childhood.
Notably, the third category relates to the use of a life course approach when addressing, evaluating, or performing pediatric health research (see the section Life Course Developmental Perspective above). A life course approach requires understanding the distinctions between developmental stages and how they may impact health conditions or diseases. It includes a broad spectrum of ages because parental health preconception can affect a child’s health (NASEM, 2019), and diseases that originate in childhood do not typically disappear once a person turns 18 years old.
Researchers
The committee’s statement of task includes a charge to address impediments faced by pediatric research applicants. These applicants include individuals with a range of degrees including, but not limited to, M.P.H., M.D.,
___________________
2 Presentation by Sarah Glavin to the Committee on Strategies to Enhance Pediatric Health Research Funded by NIH, Meeting 1, December 5, 2024.
D.O., Ph.D., Dr.P.H., Sc.D., D.N.P., and J.D. In many cases, individuals have more than one of these degrees.
This report primarily uses “investigators” to describe this diverse range of individuals and less frequently uses “researcher” or “scientist” in place of “investigator.” Terms such as “clinician–investigator” or “physician–scientist” are used to specifically refer to individuals with both clinical and research duties. Many investigators often possess a clinical degree such as an M.D., D.O., or D.N.P. in addition to a research degree such as a Ph.D., Dr.P.H., Sc.D., or M.S. “Physician” refers specifically to individuals with an M.D. or D.O., while “clinician” encompasses a broader range of individuals with clinical duties, such as nurses, midwives, psychologists, social workers, physical and occupational therapists, and community health workers in addition to physicians (HHS, n.d.; NCI, n.d.-a, n.d.-b).
ORGANIZATION OF THE REPORT
Chapter 2 provides background information on the pediatric research landscape, including NIH’s history within it and the wider funding landscape. Chapter 3 examines the current NIH pediatric research portfolio, including both intramural and extramural research across the ICs. Chapter 4 reviews how pediatric research is prioritized, coordinated, and integrated across and within ICs. Chapter 5 discusses structural and process impediments that pediatric researchers may experience while applying for funding and conducting the research. Finally, Chapter 6 offers a vision for a future robust pediatric health research enterprise.
REFERENCES
Alwin, D. F. 2012. Integrating varieties of life course concepts. Journals of Gerontology, Series B: Psychological Sciences and Social Sciences 67(2):206–220.
Annie E. Casey Foundation. 2024. Children in poverty by race and ethnicity in United States. https://datacenter.aecf.org/data/tables/44-children-in-poverty-by-race-andethnicity#detailed/1/any/false/2545,870,573,869,36/187,11,9,12,1,185,13/324,323 (accessed August 4, 2025).
Aristizabal, M. J., I. Anreiter, T. Halldorsdottir, C. L. Odgers, T. W. McDade, A. Goldenberg, S. Mostafavi, M. S. Kobor, E. B. Binder, M. B. Sokolowski, and K. J. O’Donnell. 2020. Biological embedding of experience: A primer on epigenetics. Proceedings of the National Academy of Sciences 117(38):23261–23269.
Felitti, V. J., R. F. Anda, D. Nordenberg, D. F. Williamson, A. M. Spitz, V. Edwards, M. P. Koss, and J. S. Marks. 1998. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) study. American Journal of Preventive Medicine 14(4):245–258.
Forrest, C. B., L. J. Koenigsberg, F. Eddy Harvey, M. G. Maltenfort, and N. Halfon. 2025. Trends in U.S. children’s mortality, chronic conditions, obesity, functional status, and symptoms. JAMA 334(6):509–516.
Franke, K., C. Gaser, T. J. Roseboom, M. Schwab, and S. R. de Rooij. 2018. Premature brain aging in humans exposed to maternal nutrient restriction during early gestation. Neuro-image 173:460–471.
Halfon, N., C. B. Forrest, R. M. Lerner, and E. M. Faustman (eds.). 2018. Handbook of life course health development. New York: Springer.
Heffernan, M. E., and M. L. Macy. 2025. Trends in mental and physical health among youths. JAMA Pediatrics 179(6):683–685.
HHS (Department of Health and Human Services). n.d. Regulations, policy & guidance. https://www.hhs.gov/ohrp/regulations-and-policy/index.html (accessed August 4, 2025).
HHS. 2025. The MAHA report. https://www.whitehouse.gov/wp-content/uploads/2025/05/WH-The-MAHA-Report-Assessment.pdf (accessed August 4, 2025).
IOM (Institute of Medicine) and NRC (National Research Council). 2000. From neurons to neighborhoods: The science of early childhood development. Washington, DC: The National Academies Press.
Joseph, P. D., J. C. Craig, and P. H. Caldwell. 2015. Clinical trials in children. British Journal of Clinical Pharmacology 79(3):357–369.
Klassen, T. P., L. Hartling, J. C. Craig, and M. Offringa. 2008. Children are not just small adults: The urgent need for high-quality trial evidence in children. PLOS Medicine 5(8):e172.
Levine, C. 1988. Has AIDS changed the ethics of human subjects research? Law, Medicine and Health Care 16(3-4):167–173.
Nardini, C. 2014. The ethics of clinical trials. Ecancermedicalscience 8:387.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2019. Vibrant and healthy kids: Aligning science, practice, and policy to advance health equity. Washington, DC: The National Academies Press.
NASEM. 2024. Launching lifelong health by improving health care for children, youth, and families. Washington, DC: The National Academies Press.
NCI (National Cancer Institute). n.d.-a. Clinician. https://www.cancer.gov/publications/dictionaries/cancer-terms/def/clinician (accessed August 4, 2025).
NCI. n.d.-b. Physician. https://www.cancer.gov/publications/dictionaries/cancer-terms/def/physician (accessed August 4, 2025).
NICHD (Eunice Kennedy Shriver National Institute of Child Health and Human Development). 2023. Congressional justification FY2023. https://www.nichd.nih.gov/sites/default/files/inline-files/CJ_NICHD_FY2023.pdf (accessed December 9, 2025).
NICHD. 2024. Congressional justification FY2024. https://www.nichd.nih.gov/sites/default/files/inline-files/CJ_NICHD_FY2024.pdf (accessed December 9, 2025).
NICHD. 2025a. Congressional justification FY2025. https://www.nichd.nih.gov/sites/default/files/inline-files/CJ_NICHD_FY2025.pdf (accessed December 9, 2025).
NICHD. 2025b. NIH pediatric research consortium (NPeRC). https://www.nichd.nih.gov/research/supported/nperc (accessed April 29, 2025).
NIH (National Institutes of Health). 2025a. Budget. https://www.nih.gov/about-nih/organization/budget (accessed August 5, 2025).
NIH. 2025b. Grants & funding. https://www.nih.gov/grants-funding (accessed September 18, 2025).
NIH. 2025c. Inclusion across the lifespan in human subjects research. https://grants.nih.gov/policy-and-compliance/policy-topics/inclusion/lifespan (accessed April 24, 2025).
NIH. 2025d. Mission and goals. https://www.nih.gov/about-nih/what-we-do/mission-goals (accessed April 4, 2025).
NIH Clinical Center. 2023. Clinical center pediatric research strategic plan. https://www.cc.nih.gov/sites/default/files/assets/home/pdf/CC-Peds-Research-Strategic-Plan.pdf (accessed October 29, 2025).
NIH Office of Extramural Research. 2015. Inclusion of children in clinical research: Change in NIH definition. https://grants.nih.gov/grants/guide/notice-files/not-od-16-010.html (accessed April 30, 2025).
NIH RePORT (Research Portfolio Online Reporting Tools: 2025). RePORTER. https://reporter.nih.gov/ (accessed August 14, 2025).
Petkova, V., D. Georgieva, M. Dimitrov, and I. Nikolova. 2023. Off-label prescribing in pediatric population—Literature review for 2012–2022. Pharmaceutics 15(12):2652.
Roseboom, T., S. de Rooij, and R. Painter. 2006. The Dutch famine and its long-term consequences for adult health. Early Human Development 82(8):485–491.
Shah, S. K. 2021. The ethics of pediatric research. In A. S. Iltis and D. MacKay (eds.), The Oxford handbook of research ethics. New York: Oxford University Press. Pp. 683–698.
Sinha, I., L. Jones, R. L. Smyth, and P. R. Williamson. 2008. A systematic review of studies that aim to determine which outcomes to measure in clinical trials in children. PLOS Medicine 5(4):e96.
Speer, E. M., L. K. Lee, F. T. Bourgeois, D. Gitterman, W. W. Hay, J. M. Davis, and J. R. Javier. 2023. The state and future of pediatric research—An introductory overview. Pediatric Research January 24:1–5 [Epub ahead of print].
U.S. Census Bureau. 2023. Child poverty rate still higher than for older populations but declining. https://www.census.gov/library/stories/2023/12/poverty-rate-varies-by-age-groups.html (accessed August 4, 2025).
Van den Broek, T., and M. Fleischmann. 2019. Prenatal famine exposure and mental health in later midlife. Aging & Mental Health 23(2):166–170.
Webster, E. M. 2022. The impact of adverse childhood experiences on health and development in young children. Global Pediatric Health 9:2333794X221078708.















