Launching Lifelong Health by Improving Health Care for Children, Youth, and Families (2024)
Chapter: 7 Investing in Child Health through Population- and Community-Level Primary Prevention
7
Investing in Child Health through Population- and Community-Level Primary Prevention
Finding resources is an ongoing struggle for our families. It is impossible for parents to focus on the [health] struggles that their children are having if they are first unable to meet their basic needs. Mental health care, access to enough food, and transportation are all huge factors which can affect follow-through and compliance.
—Comment to committee from registered nurse in Iowa
The previous chapter discussed the role of health insurance and financing for clinical services. This chapter examines noninsurance financing toward public health and its influences on children’s health and wellbeing. “Public health” has been variously defined but is commonly thought of as the science and pursuit of promoting and protecting the health of all people and their communities. This definition makes clear two important dimensions of public health—its focus on (primary) prevention and its focus on the health of a population (Wiley, 2016). As described in Chapter 6, primary prevention can be clinically based, occur through the traditional health care system, and be delivered to patients one-on-one; but more often, primary prevention efforts are community or population based (Institute of Medicine [IOM], 2010) and thus fall under the public health umbrella. Importantly, although some associate the term “public health” with a narrow focus on governmental efforts, public health encompasses a diverse group of public and private collaborators and includes the health care delivery system (IOM, 2012b). Diez Roux (2016) emphasized that the relevant definition of “public” in the term “public health” is “of or concerning the people as a whole” (p. 620).
Across the spectrum of health care, primary prevention is especially salient for children. By definition, disease prevention must occur before its onset, and childhood represents a time before the onset of most chronic conditions. Moreover, and as emphasized in previous chapters, health can be viewed as a cumulative process in which outcomes in one period affect outcomes in future periods. As such, childhood presents a critical window for influencing health outcomes over an individual’s entire life course, and primary prevention during childhood offers a unique opportunity for minimizing the future burden of disease. Expanding on the notion of primary prevention as a form of insurance (Newhouse, 2021), new spending on public health efforts for children can be seen as a form of insurance for the nation against high future health care and non–health care costs attributable to preventable conditions.
What is more, primary prevention plays an important role in connecting people with community resources (e.g., social services, nutrition assistance programs) and is recognized as a prominent lever for reducing health disparities and achieving health equity. Thus, primary prevention activities represent an important element of the full spectrum of health care that children receive, and they are critical to children’s health care system transformation (see Figure 7-1).
The committee’s aim in this chapter is to describe the contours of public health spending relevant to children. While social determinants of health are

SOURCE: José Luis Bayer, Chile; © Peace Child International, used with permission.
part of the public health perspective (such as spending to reduce poverty or improve housing), this discussion is limited to public health spending that is primarily health care related, in alignment with this report’s focus.
PUBLIC HEALTH
As in earlier reports (IOM, 1998, 2003a, 2012a,b,c), the committee’s conception of public health is broad, involving organized community efforts aimed at preventing poor health and disease at the population level. Providing essential public health services, such as those in Box 7-1, requires interaction among government health agencies, the health care system, the private sector, community organizations, and other public–private partnerships. The work of public health has evolved to address changing societal needs. Traditionally, public health has engaged systems and policy to mitigate infectious disease and unsafe conditions (IOM, 2012c). Among others, important programs for children, youth, and families have increased the availability of vaccines, developed standards for safer foods and water, prevented childhood lead poisoning, and lessened tobacco use. Given the complex nature of health challenges in the United States today, public
BOX 7-1
Essential Public Health Services
- Assess and monitor population health status, factors that influence health, and community needs and assets
- Investigate, diagnose, and address health problems and hazards affecting the population
- Communicate effectively to inform and educate people about health, factors that influence it, and how to improve it
- Strengthen, support, and mobilize communities and partnerships to improve health
- Create, champion, and implement policies, plans, and laws that impact health
- Utilize legal and regulatory actions designed to improve and protect the public’s health
- Enable equitable access to the individual services and care needed to be healthy
- Build and support a diverse and skilled public health workforce
- Improve and innovate public health functions through ongoing evaluation, research, and continuous quality improvement
- Build and maintain a strong organizational infrastructure for public health
SOURCE: de Beaumont Foundation and Public Health National Center for Innovations, 2024. https://debeaumont.org/10-essential-services/

SOURCE: Adapted from Rechel (2020) and Community Preventive Services Task Force.
health is core to fighting chronic conditions and health disparities that often have roots in childhood experiences.
Public health and health care each bring significant assets to partnerships that may improve child health outcomes. Figure 7-2 illustrates the integration of services and settings as public health and health care collaborate on primary prevention. Early experiences in several cities suggest public health–health care collaborations enhance chronic disease care, preventive service delivery, and maternal–child health. Reviews of such collaborations indicate that delineating shared goals, data structure and sharing rules, and resource constraints, as well as asset mapping, are important steps (Martin-Misener et al., 2012; McVicar et al., 2019). The goals of public health–health care collaborations require articulation and careful measurement (see Chapter 9).
A variety of models of collaboration have been developed and have evolved over time. Beginning with individual partnership models used by specific practices or groups of health care practices and public health staff, some models1 evolved into regional networks around topic areas or disease conditions. A desired final phase of such models is an ecosystem model, whereby all the partners in both public health and health care share integrated communications, data, and performance evaluation. Since many networks studied were still in early phases of development, few networks have been observed to reach the most mature stages. Developing these models and spreading them to new sites with a greater focus on children
___________________
1See Derr (2023) for a history of public health community collaboration.
will require more resources (see further discussion at end of the chapter). Given that child health and primary prevention efforts include significant community components, without public health partnerships, they are not likely to improve significantly.
Important Public Health Programs for Children
This section highlights effective public health strategies, interventions, and policies that have historically and continuously benefited young people across the nation. From preventive measures to community-based programs and nationwide policies, these initiatives have had a tangible, positive impact on the lives of millions of American children and families. The selected issues below focus on improved outcomes for children across the United States. It is important to note that public policies (such as decisions that affect community environment and housing options) can have indirect negative consequences on children’s health. It was beyond the scope of the committee’s work to examine these.
Maternal and Infant Health
Increased attention to maternal and infant health has led to heightened efforts and resources aimed at enhancing health outcomes and reducing disparities (Hill, Artiga, & Ranji, 2022; Koppaka, 2011a; Lassi, Kumar, & Bhutta, 2016). Programs administered through the Health Resources and Services Administration (HRSA), discussed in greater depth below, provide public health leadership and financial support for maternal and child health programs nationwide. These programs focus on improving access to prenatal care and promoting healthy behaviors during pregnancy. Additional efforts—such as the Pregnancy Risk Assessment Monitoring System and the Collaborative Improvement and Innovation Network, breastfeeding support programs, and safe sleep campaigns—are meaningful strategies for identifying and combatting infant mortality risks (Centers for Disease Control and Prevention [CDC], 2013; Mehta et al., 2021).
Vaccine-Preventable Diseases
Childhood immunizations, and vaccines generally, are a notable public health success (Amanna & Slifka, 2020; CDC, 1999; Koppaka, 2011a,b). Instances of individuals suffering from preventable infectious diseases, such as measles, diphtheria, and whooping cough, have reached historic lows (CDC, n.d.a, 2020b, 2024i,n). From 2000 to 2010 alone, an estimated 2.5 million deaths were prevented yearly among children under age 5 years using measles, polio, and diphtheria-tetanus-pertussis vaccines (Koppaka, 2011a).
Several public health initiatives have contributed to increased rates of childhood immunization, helping to protect children from vaccine-preventable diseases. The Vaccines for Children (VFC) program, discussed further below, is supported through CDC’s (2024a,j,q) National Center for Respiratory Diseases. National immunization awareness campaigns and community outreach efforts at the national, state, and local levels educate parents, caregivers, and health care providers about the importance of childhood vaccinations and provide information on vaccine safety and efficacy, recommended immunization schedules, and the benefits of vaccination in preventing serious illness (CDC, 2019a, 2024a; Kaufman et al., 2018; National Vaccine Advisory Committee, 2013).
While childhood vaccines have saved lives and money, vaccine hesitancy remains a persistent concern for population health (Nuwarda et al., 2022). School immunization requirements, which are implemented at the state level, mandate that children receive certain vaccines before enrolling in schools and child care facilities (Seither et al., 2023a,b). These requirements help ensure high vaccination coverage rates among school-aged children. However, a recent CDC report that used data from the 2021–2022 school year revealed that while rates of unvaccinated and undervaccinated children remain low, the share of U.S. kindergartners receiving state-required vaccines continues to decrease (Seither et al., 2023a,b). As discussed in Chapter 3, it is important to underscore the value of trust in information about vaccines from public health officials and health care providers (Funk et al., 2023).
Fluoridation of Water
Community water fluoridation programs have been implemented across the United States since the mid-20th century (Armfield, 2010; Department of Health and Human Services Federal Panel on Community Water Fluoridation, 2015). Fluoride is added to public water supplies at optimal levels to prevent tooth decay. This public health measure has been shown to benefit children and families by reducing the prevalence of dental caries (also known as cavities), promoting oral health, and improving overall wellbeing (Boehmer et al., 2023).
Tobacco Control
Tobacco use affects child health in various ways, including prenatal exposure to smoke, secondhand smoke, and smokeless tobacco products (Gould et al., 2020; Jenssen et al., 2023). Prenatal exposure can result in birth defects, preterm birth, growth restriction, and stillbirth. Postnatally, secondhand smoke exposure increases the risk of neonatal and infant death, respiratory infections, meningococcal disease, and asthma attacks (Been & Sheikh, 2018). Children and adolescents who use various tobacco products face an elevated risk of nicotine dependence and are more prone to
continued tobacco use into adulthood. Since the release of the first Surgeon General’s Report on tobacco in 1964, evidence-based policies and interventions at federal, state, and local levels have reduced tobacco use substantially for people of all ages (Been & Sheikh, 2018; Koppaka, 2011a). Some key initiatives include the regulation of tobacco sales to people under a certain age; tobacco taxes, which are particularly effective for reducing tobacco use among youth; tobacco advertising restrictions, which reduce children’s exposure to pro-tobacco messages; and smoke-free policies, which protect nonsmokers from secondhand smoke exposure and contribute to social norms around smoking (Cruz et al., 2019; Jenssen et al., 2023).
Youth tobacco prevention programs and educational campaigns targeted at children and adolescents often use school-based interventions, community outreach, and media campaigns to deliver anti-tobacco messages and promote healthy behaviors (Flay, 2009; Jenssen et al., 2023). However, continued efforts and vigilance are necessary to address remaining challenges and prevent tobacco use initiation among youth. Youth use of e-cigarettes, vapes, and other electronic devices that contain nicotine has increased significantly over the past decade (Birdsey et al., 2023; Jones & Salzman, 2020). While regulations and flavor bans by the Food and Drug Administration have helped to restrict the sale of flavored vaping products (Li et al., 2022a), the evolving landscape of electronic smoking products and marketing tactics necessitates continued vigilance and adaptation of strategies for protecting children and adolescents from the harms of vaping.
Motor-Vehicle Safety
Like tobacco reduction, improved motor-vehicle safety is another public health effort that began in the 1960s and has resulted in significant improvements for children (CDC, 1999). Government and community recognition of the need for motor-vehicle safety prompted the initiation of programs by federal and state governments, academic institutions, community-based organizations, and private organizations. Public health initiatives aimed at improving motor-vehicle safety for children in the United States are driven by a multifaceted approach.
First, child-passenger safety laws have been established in most states (Insurance Institute for Highway Safety [IIHS], 2024). These laws mandate the use of appropriate child safety seats, booster seats, or seat belts (based on age, weight, and height), thereby increasing compliance and reducing the risk of injuries or fatalities in crashes (Bae et al., 2014; Eichelberger, Chouinard, & Jermakian, 2012; Mannix et al., 2012; Zaza et al., 2001). Currently, 49 states and the District of Columbia have implemented seat belt laws for adults, while all 50 states and the District of Columbia have enacted legislation safeguarding children in vehicles (IIHS, 2024; Koppaka, 2011a). Moreover, public health agencies advocate for legislation and improved
safety standards, working alongside policy makers and industry stakeholders to promote advancements in technology and vehicle design (Fleetwood, 2017; Pollack Porter, Rutkow, & McGinty, 2018).
Education and outreach programs further raise awareness among parents and caregivers about the importance of proper restraint usage, providing guidance on installation and highlighting potential consequences of misuse (Britton et al., 2023; Penmetsa, Wang, & Nambisan, 2017; Sartin et al., 2019). Child safety seat inspection stations and other related programs, often established through public–private collaborations, offer hands-on assistance to ensure correct installation and enhance the effectiveness of restraints (O’Neil et al., 2013; Ostergaard & Guzzetta, 2021; Tessier, 2010).
Additionally, graduated driver licensing policies for teen drivers have contributed to a decrease in the number of teenage crash fatalities (Baker, Chen, & Li, 2007).
Finally, community partnerships and collaborations facilitate the dissemination of information and implementation of targeted interventions, leveraging existing networks to reach a broader audience and enhance motor-vehicle safety for children (Buttazzoni et al., 2024; Ehiri et al., 2006; Turner et al., 2005).
Government Public Health Departments
State and local health departments are critical nodes in the funding of public health programs for children, drawing not only on federal resources but also, to a variable extent across states, on revenue generated by user fines and fees as well as state government funds (including, e.g., from state cigarette taxes; IOM, 2012b,c). To provide services to communities, local health departments also rely on contributions and collaborations with businesses, media, schools, policy makers, and health care systems in the community.
Funding for public health has declined significantly across all federal, state, and local levels in the past two to three decades, compared with spending on direct health care services. While estimates of national public health spending vary, they consistently reveal underinvestment (IOM, 2012b,c). Available estimates put spending on public health activities at less than 5% of the nation’s health-related spending (Farberman & Kelley, 2020; Himmelstein & Woolhandler, 2016). DeSalvo and colleagues (2019) estimate that the national investment in public health is $19/person, which leaves a $13/person gap in annual spending necessary to achieve core public health capabilities associated with the Foundational Public Health Services model.2 As such, activities to promote population health
___________________
2The Foundational Public Health Services model defines a minimum set of public health capabilities and programs for communities (see https://phaboard.org/center-for-innovation/public-health-frameworks/the-foundational-public-health-services).
NOTE: Expenditures are shown by fiscal year, which is defined in the Profile Survey as July through June (e.g., Fiscal Year 2021 was from July 1, 2020 – June 30, 2021).
SOURCE: ASTHO, 2023.
and prepare for and prevent emergencies that impact the wellbeing of communities have been challenged by a shrinking workforce and insufficient funding to fulfill mission (Association of State and Tribal Health Officials [ASTHO], 2023).
States provide about 28% of overall state health department revenues and 21% of local health department revenues on average. Federal funds cover the rest of state and local health department activities (McKillop, Farberman, & Lieberman, 2023; see Figure 7-3). In fiscal year (FY) 2021, federal sources predominantly funded state health agency WIC services,3 chronic and infectious disease initiatives, and hazard preparedness and response. The expenditure categories of injury prevention, environmental health, administrative functions, and quality of services were largely funded by state sources (ASTHO, 2023).
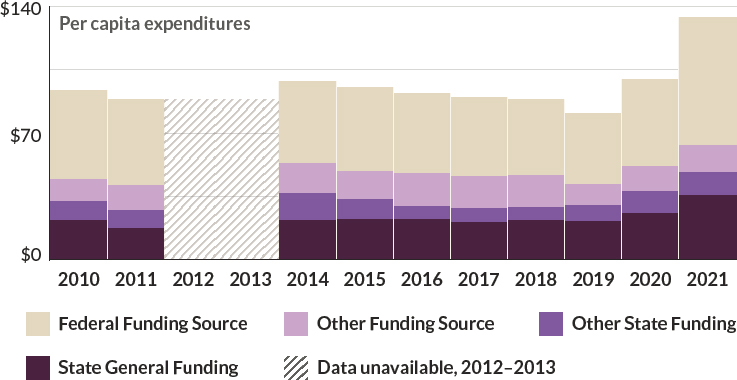
Over the past 10 years, the average and per capita expenditures for public health agencies have varied; most are relatively stable, although considerable variations exist across states and communities. In FY 2021, public health spending increased significantly to respond directly to the COVID-19 pandemic. Spending to address the emergency represented approximately one-third of 2021 total state public health agency expenditures (ASTHO, 2023; see Figure 7-4). Of those expenditures not related to COVID-19, about 15% went toward clinical services and consumer care and 11% supported
___________________
3WIC stands for Special Supplemental Nutrition Program for Women, Infants, and Children.

NOTES: The number of reporting agencies varies each year and by funding source. Expenditures are shown by fiscal year, which is defined in the Profile Survey as July through June (e.g., Fiscal Year 2021 was from July 1, 2020–June 30, 2021).
SOURCE: ASTHO, 2023.
WIC programs. The extra investment during the emergency has not been sustained despite the importance of prevention to child health (Martin et al., 2021, 2023; Trust for America’s Health, 2023). One ongoing challenge is that federal funding for state and local public health efforts is often allocated by disease category and is thus compartmentalized, leaving little flexibility for responsiveness to local priorities or for cross-cutting capabilities (IOM, 2012b). It is noteworthy, however, that efforts to convert categorical grants into more flexible funding have been found to result in decreased funding (based on theoretical program administration cost savings and flexible funds that risk being diverted to unrelated priorities (Leider et al., 2018).
FEDERAL PROGRAMS FOR MEETING COMMUNITY NEEDS
Federal spending on children includes tax provisions and other income supports, as well as funding for direct provision of health care services and spending on social services such as nutrition, education, child care, and housing (see Figure 7-5). About half of this spending is universal, and the other half targets families with lower incomes and historically marginalized populations (Lou et al., 2023). The bulk of federal spending on children is directed to tax provisions, which are not covered in this study, but do reduce child poverty (National Academies of Sciences, Engineering, and Medicine

NOTES: Programs that spend less than $10 billion are not shown separately but are included as part of “Other” and in the totals by category. CCDF = Child Care and Development Fund; CHIP = Children’s Health Insurance Program; CTC = child tax credit; EIP = economic impact payments (pandemic response stimulus checks administered through the tax code); EITC = earned income tax credit; ESI = employer-sponsored health insurance; SNAP = Supplemental Nutrition Assistance Program; SSI = Supplemental Security Income; TANF = Temporary Assistance for Needy Families.
SOURCE: Lou et al., 2023. Authors’ estimates based primarily on Office of Management and Budget, Budget of the United States Government, Fiscal Year 2023.
[National Academies], 2019a, 2023g) and have an indirect influence on health. Another significant portion of funding is for direct health care services (discussed in Chapter 6).
This section reviews federal expenditures on social services with impact on population health. Many programs are administered through the U.S. Department of Health and Human Services (HHS). Key HHS operating divisions and offices that support children’s health care financially include HRSA, CDC, the Indian Health Service, the Substance Abuse and Mental Health Services Administration (SAMHSA), and the Administration for Children and Families (ACF). Other government agencies with programs aimed at improving the health, wellbeing, and future productivity of children and youth
include the U.S. Department of Agriculture (USDA) and U.S. Department of Education. This review does not include all relevant current and former programs that support preventive services, and some important services and contexts are not discussed here (First Focus on Children, 2023). For example, research shows that variations in stable housing, transportation, and access to parks and green space all shape inequities for children and families that affect health and wellbeing. These areas of programs, policies, and systems are not the focus of the solutions discussed in this report and are well documented in other reports (National Academies, 2017a, 2019a,d, 2023g).
This section focuses on the programs, policies, and systems that more directly serve primary preventive care needs, aim to reduce health disparities, and improve population health. It is organized around funding for services through grants to the states for providing preventive services in community settings and promoting maternal and early child health; nutritious meals; substance use disorder prevention and treatment; and mental and behavioral health services.
The agencies discussed provide funding in various forms—including block, programmatic, and competitive grants—to state and local health departments, nongovernmental organizations, state and local education agencies, tribal nations, territory administrators, faith-based institutions, and other partners to provide health care to children. A common feature of such services is that they are often, although not exclusively, community based, allowing the interventions to be adapted to local characteristics and priorities. They can take on different forms; be universal or targeted to at-risk individuals; be delivered to individuals or to groups; or be delivered by health care systems, workplaces, the military, schools, child care centers, and state or local health departments (Community Preventive Services Task Force, 2022).
Preventive Services
Head Start and Early Head Start
ACF funds local partners to provide health and wellbeing services to children under age 5 years through the Head Start and Early Head Start programs. In addition to early learning services, Head Start supports health by engaging children in physical activity, serving nutritious meals and snacks, ensuring that children receive developmental screenings, promoting oral hygiene, promoting resilience, and providing parenting support (ACF, 2023a,b).
Created as part of President Lyndon Johnson’s War on Poverty, Head Start provides comprehensive early childhood education, health, nutrition, and parent support services to low-income, preschool-age (ages 3–5 years) children and their families. Early Head Start was created in 1995 to aid pregnant women and children from birth to age 3 years (Office of Head Start, 2023a,b). Families receive services in their homes and/or Head Start
centers, which are locally operated and funded directly by ACF (Office of Head Start, 2023b,c). In addition to Head Start and Early Head Start, the American Indian and Alaska Native Head Start program began in 1965 and provides grants to federally recognized American Indian and Alaska Native tribes; the Migrant and Seasonal Head Start program (started in 1969) provides services to migrant farm workers and their families.
Head Start and Early Head Start have notable direct impacts on children’s health outcomes. Compared with children who are not receiving these services, children enrolled in Early Head Start are more likely to be immunized and have access to services for their disabilities (Love et al., 2002). Those in Head Start are more likely to receive dental checkups (Lee & Gortmaker, 2013) and have improved oral health knowledge, behaviors, and activities (Joufi, Claiborne, & Shuman, 2021). Children with obesity, overweight, or underweight are more likely to have a healthier body mass index by kindergarten (Lumeng et al., 2015). In addition, Head Start has been shown to improve mental health outcomes (D’Onise, Lynch, & McDermott, 2010).
Parent involvement in Head Start has indirect impacts on health outcomes, with children demonstrating significantly better socioemotional, language, and cognitive development (Love et al., 2002) when their parents are involved. Head Start graduates are less likely to be in poor health as adults and more likely to report positive parenting behaviors. The children of Head Start graduates have significantly lower odds of becoming teen parents (Barr & Gibbs, 2017; Bauer & Schanzenbach, 2016; Deming, 2009; Johnson, 2010).
The reach and impact of the Head Start program differs across states (National Academies, 2019d) and varies by community and family cultural background. Black children are shown to experience greater gains in self-esteem and socioemotional development, and Hispanic children demonstrate notable gains in educational outcomes (Bauer & Schazenbach, 2016). Although 33% of Black children living in poverty are enrolled in Head Start, compared with 23% of Asian and 27% of Hispanic children, funding per child is lower in states that enroll higher percentages of Black children. The average funding per child across the five areas with the highest percentage of Black children (Washington, DC; Georgia; Louisiana; Maryland; Mississippi) was $9,450, compared with $12,654 in the five states with the lowest percentage (Idaho, Montana, Utah, Vermont, and Wyoming), adjusting for differences in cost of living by state (Friedman-Krauss, Barnett, & Duer, 2022).
Because of insufficient funding, Head Start serves less than half of all 3- and 4-year-olds living in poverty (Barnett & Friedman-Krauss, 2016); this varies widely across states, with an estimated 56% in North Dakota and an estimated 9% in Nevada (Friedman-Krauss, Barnett, & Duer, 2022). Early Head Start reaches about 9% of all eligible children and families. Nationally, around 13% of children enrolled in Head Start and 12% in Early Head Start qualify for special education services under the Individuals with Disabilities Education Act (Friedman-Krauss, Barnett, & Duer, 2022).
The COVID-19 pandemic negatively impacted enrollment in Head Start, as nationally 287,000 fewer children attended in 2020–2021 than in 2018–2019 (the enrollment rate dropped from 41% to 30%), in spite of increased funding for COVID-19 relief. In FY 2022, Head Start and Early Head Start were appropriated $11,036,820,000, an increase of $289 million over FY 2021 (ACF, 2023b).
Centers for Disease Control and Prevention
CDC invests in health surveillance and research as well as prevention activities, which fall variably along the spectrum of direct to indirect children’s health care services. Most directly relevant to primary preventive care is the funding CDC provides through the Prevention and Public Health Fund, which makes up 10% of CDC’s budget, totaling $903 million in FY 2023 (McKillop & Lieberman, 2023; this fund also supports SAMHSA and ACF). By statute, the Prevention and Public Health Fund supports a range of programs, spanning disease prevention; early detection; chronic disease management; mental health and injury prevention programs; and promotion of healthy lifestyles, including increasing nutrition and physical activity and reducing tobacco use. The fund provides financial support to states and communities directly so they can address their most pressing health challenges and community needs (Trust for America’s Health, 2023).
Within the Fund, programs that target the health and wellbeing of children and families most directly include the immunization program, Preventive Health and Health Services Block Grants for state-specific needs, childhood lead poisoning surveillance, maternity and breastfeeding care through hospitals, early care and education collaboratives, and suicide prevention.
The immunization program improves access to vaccination by covering the cost for uninsured children and adults, those on Medicaid, and American Indians and Alaska Natives. It also supports critical infrastructure for collecting and tracking data related to immunization, supporting safety and quality improvement. Passed into law in 1993 in response to a measles outbreak in the United States, the Vaccines for Children (VFC) program provides vaccines to children at no cost, providing critical access to those families who might not be able to pay otherwise. All vaccines recommended by CDC’s Advisory Committee on Immunization Practices are eligible for coverage through VFC. An earlier study estimates that, during the first 20 years of the program, the increase in vaccination rates for children born between 1994 and 2013 has helped prevent 21 million hospitalizations and 732,000 deaths, and has resulted in an estimated net savings of $1.38 trillion in total societal costs, which includes an estimated net $295 billion in direct costs (Whitney et al., 2014). The VFC program has been cited as one of the reasons measles has not been endemic since 2000 (Orenstein, 2023).
VFC has also contributed to the narrowing of racial/ethnic and socioeconomic inequities in access to vaccination, leading to a decreased disparity in vaccination rates. An estimated 50% of children are eligible for the VFC program in the United States, with younger children more likely to be eligible and adolescents less likely (Kang et al., 2023; Lindley, Smith, & Rodewald, 2011). A majority of children served by VFC identify with a racially marginalized community (Walker et al., 2014). In FY 2022, VFC was appropriated $5.54 billion (CDC, 2024a).
From the Prevention and Public Health Fund, CDC also administers the Preventive Health and Health Services (PHHS) Block Grant to states, tribes, local health departments, and territories. In FY 2020, this totaled $149,098,135, and of that, 2.9% ($3,882,662) was allocated explicitly to maternal, infant, and child health care (CDC, 2023f). Evaluation of the impact of the PHHS Block Grants has not identified any specific child or maternal health outcomes but rather support for the broader public health infrastructure (CDC, 2023f).
In 2023, the Fund also administered $17 million to prevent childhood lead poisoning, $9.75 million for hospitals to promote breastfeeding, and $12 million for Garrett Lee Smith grants through SAMHSA for prevention and early intervention of youth suicide in a variety of settings (Trust for America’s Health, 2023).
Since 1999, CDC has also funded the Racial and Ethnic Approaches to Community Health (REACH) program, focused on reducing health disparities among specific racial/ethnic groups by funding state and local health departments, tribes, universities, and community-based organizations. Grantees are instructed to use funds to build partnerships in communities with the highest burden of health inequity. While there are no child-specific requirements for use of the funding, REACH grantees have demonstrated positive impacts on child health outcomes, such as increased breastfeeding (Witt et al., 2021) and increased access to and consumption of fruits and vegetables through food prescriptions (Jones, VanWassenhove-Paetzol et al., 2020). In FY 2022, the REACH program received $43.45 million (Trust for America’s Health, 2022).
The Good Health and Wellness in Indian Country (GHWIC) program is CDC’s largest investment to improve health for American Indians and Alaska Natives. Similar to REACH, GHWIC aims to reinforce work already under way in communities and support culturally appropriate approaches to health. Apart from a goal to increase breastfeeding, none of GHWIC’s goals are child specific. In FY 2022, the program received $22.5 million (Trust for America’s Health, 2022).
Despite efforts to create a separate fund for prevention services and activities, federal priorities have diverted funding from the Prevention and Public Health Fund away from prevention activities toward direct health care services (Harkin, 2013). Even more concerning are expected cuts to
programs such as VFC that deliver a significant amount of preventive care to children (Miller, 2023).
CDC also administers the National Center on Birth Defects and Developmental Disabilities (NCBDDD), which provides resources for research, awareness, public health practice, and surveillance, with a focus on child health and disability. NCBDDD’s efforts have included evaluating the impact of folic acid supplementation; promoting standards of preconception care; providing resources for attention deficit and hyperactivity disorder and autism spectrum disorder, including the “Learn the Signs. Act Early” campaign for facilitating earlier diagnosis for these conditions; and creating surveillance systems for sickle cell disease and thalassemia (Boyle, Cordero, & Trevathan, 2012). NCBDDD funds the Early Hearing Detection and Intervention program, which promotes hearing screening, diagnosis, and early intervention, ensuring that infants are screened for hearing loss, that those who need it receive a full evaluation, and that those with hearing loss receive intervention services (CDC, 2024l). NCBDDD also provides resources for developing treatments for hemophilia and funds comprehensive hemophilia treatment centers. CDC studies have shown that people with hemophilia who receive care from a hemophilia treatment center are 40% less likely to be hospitalized and less likely to die because of bleeding complications (CDC, n.d.c), compared with those who do not receive this care. In FY 2022, NCBDDD (2023) received $177 million in appropriations.
Maternal and Early Child Health
HRSA Title V Maternal and Child Health Block Grant
Through the Maternal and Child Health Bureau (MCHB), HRSA (2023j) administers block grants to states for improving access to health care—including prenatal–postnatal services, preventive and primary care for children, and community-based services—focused on low-income individuals and children and youth with special health care needs. Through legislative and administrative decisions, the MCHB has evolved since its founding in 1912 as the Children’s Bureau to better respond to the needs of children and families. Title V was established as part of the Social Security Act (1935 § 501) to provide “grants to states for maternal and child welfare.” States are required to provide a level of matching for funds they receive in federal Title V block grant support. With the establishment of Medicaid in 1965, Title V funds have been increasingly used to fill gaps in the system of care for children and mothers (Warren & Kavanaugh, 2023).
[For] three decades, state Title V programs have played an important role in increasing access to and use of timely prenatal care and other family health care services through outreach and coordination by (1) facilitating
partnerships among agencies that provide direct services to pregnant women; (2) helping to ensure that maternal and child health professionals in WIC, Head Start, and other public programs provide pregnant women with accurate and current information on coverage in their state; (3) increasing access to presumptive Medicaid eligibility, which provides pregnant women with access to immediate prenatal care; and (4) increasing continuity of coverage for low-income women who become pregnant. (National Academies, 2019d, p. 333)
Title V programs have a significant history of supporting very young children, stemming back to the Children’s Bureau, which among its first activities published an “Infant Care” pamphlet in 1914 and had a series of “Baby Week Campaigns” in 1917. Subsequent investments and priorities included children with special health care needs (“children who are crippled or who are suffering from conditions which lead to crippling”) as part of the Social Security Act (1935 § 501) and children from low-income neighborhoods as part of Medicaid (Warren & Kavanaugh, 2023). Currently, at least 30% of federal support for state programs has been allocated for well-child programs, and at least 30% goes to programs for children with special health care needs (formerly the Crippled Children’s Service; HRSA, 2019). As with women’s health, state programs have helped to facilitate partnerships across key agencies; improve knowledge of the health status of children and youth in the state; and link households with other agencies, especially Medicaid and the U.S. Social Security Administration (for Supplemental Security Income coverage; National Academies, 2019d). In FY 2022, Title V maternal and child health block grants were appropriated $736 million (Black Maternal Health Caucus, 2023; HRSA, 2023g).
Maternal, Infant, and Early Childhood Home Visiting
HRSA, in partnership with ACF, administers the Maternal, Infant, and Early Childhood Home Visiting (MIECHV) program to fund states and jurisdictions. The program provides for voluntary home visits during early pregnancy and childhood to families in at-risk communities to provide parenting support and child-centered services in the home (e.g., developmental screenings; HRSA, 2023f). By law, state and territory awardees are required to implement evidence-based home visiting models. ACF created the Home Visiting Evidence of Effectiveness (HomVEE) project to conduct thorough and transparent reviews of early childhood home visiting models (HHS, n.d.).
In FY 2018, the MIECHV program provided nearly 1 million home visits and served approximately 150,000 parents and children in 76,000 families across all 50 states; Washington, DC; 5 territories; and 23 tribal and urban
American Indian and Alaska Native communities (HRSA, n.d.c). It has been reported that 40% of U.S. counties provide home visiting services, with 13 states offering home visiting in 75% of counties and 10 states providing it in 10 or fewer counties (NHVRC, 2018). The National Home Visiting Resource Center (2023) estimates that more than 22 million additional families could benefit but were not being reached. The MIECHV program was reauthorized in 2018 at a funding level of $400 million annually through 2022 (Sandstrom, 2019). The 2022 reauthorization increased funding and established new procedures through 2027 (CRS, 2023a,b).
Positive health impacts of the MIECHV program in some settings have included fewer preterm and low birth weight babies, more children adequately immunized and completing well-child visits, greater achievement of developmental milestones, fewer child emergency department visits, and better maternal physical and mental health (Sandstrom, 2019). While nurse home visiting can provide important health care services for children, mother wellbeing, and family functioning (Goldfeld et al., 2022), the evidence for their effectiveness at a population level is currently mixed. Studies reviewed by HomVEE have noted lower rates of newborn death, preterm and low-weight birth, and need for emergency or hospital care in the first year of life (Sandstrom, 2019).4 Other studies have found that such programs do not improve birth outcomes, even for non-Hispanic Black mothers (McConnell et al., 2022; Robling et al., 2016). Findings may differ because of the implementation of different home visiting models in different settings and variation of use across the United States (see Figure 7-6).
Some of the variability shown in Figure 7-6 is due to different state decisions to support home visiting programs through a mix of funding sources, including funding from MIECHV, as well as from Medicaid, Title V, Temporary Assistance for Needy Families, Child Welfare, and Head Start. Additionally, under a recent reauthorization, MIECHV opted for a new model for distributing funds to states. In addition to investing in evidence-based interventions from a list created by HomVEE, the newer model authorizes states to use up to 25% of their grant funds to enter into public–private partnerships called pay-for-success agreements (see further discussion of this model below).
___________________
4HomVEE has also looked specifically at models with potential relevance for American Indian and Alaska Native families and children. Family Spirit is an example of a model designed for American Indian pregnant women and families with children younger than age 3 years; it utilizes paraprofessional home visitors from the community to support mothers’ and caregivers’ parenting skills. Studies have found favorable impacts on maternal health, child development, and positive parenting practices (HHS, 2022).

NOTES: Estimated percentage of eligible children is calculated as the percent of children under age 3 years served by home visiting programs out of all children under age 3 in families with incomes below 150% of the federal poverty level. Vermont’s home visiting participation numbers were impacted by model changes during 2019 and likely not reflective of accurate participation rates. NR = not reported.
SOURCE: National Home Visiting Resource Center Yearbook (2020) and American Community Survey 1-year Public Use Microdata Sample (Census Bureau, 2018, 2019).
Nutritious Meals
USDA provides health care to children by distributing funds through programs such as WIC, the Supplemental Nutrition Assistance Program (SNAP), and the Summer Food Service Program (discussed below), as well as the National School Lunch and School Breakfast programs (discussed in Chapter 8, see also USDA, 2023a).
Special Supplemental Nutrition Program for Women, Infants, and Children
In WIC, USDA provides federal grants to states for “supplemental foods, health care referrals, and nutrition education for low-income pregnant, breastfeeding, and non-breastfeeding postpartum women, and to infants and children up to age 5 who are found to be at nutritional risk” (USDA, 2023c, para. 1). Families with incomes below 100% or 185% of the federal poverty level (depending on the state) are eligible for WIC, and the program serves half of all infants in the United States.
WIC provides assistance through breastfeeding support and education, healthy foods, nutrition education and counseling, screening referrals to other services, and vouchers to purchase fruits and vegetables from authorized farmers’ markets (USDA, 2024a). WIC services are provided in many settings, including county health departments, hospitals, mobile clinics, community centers, schools, public housing sites, migrant health centers and camps, and Indian Health Service facilities (USDA, 2024a).
To be eligible to receive benefits, WIC participants need to meet four categories of requirements: categorical, residential, income, and nutrition risk (USDA, 2024a). Infants younger than age 1 year; children younger than age 5 years; and women who are pregnant, postpartum (up to 6 months), or breastfeeding meet the WIC categorical requirement. To meet the residential requirement, participants need to reside in the state or local service area in which they apply but are not required to have lived in that area for a minimum amount of time. Participants also have to earn incomes at or below income standards that are set by state agencies and fall within 100% and 185% of the federal poverty guidelines issued annually by HHS. Additionally, participants need to be determined by a health professional to have at least one medical (e.g., anemia, underweight) or dietary (e.g., poor diet) condition from a list of conditions indicating nutrition risk that is set by states (USDA, 2018).
Participation rates among eligible children decline significantly after infancy. Over 98% of eligible infants participate; however, participation rates decline among children ages 1, 2, 3, and 4 years—65%, 49%, 44%, 25%, respectively—and only 52% of eligible pregnant individuals participate (Trippe et al., 2019; USDA, 2024b). Factors contributing to decreased participation rates have been reported as concerns regarding immigration
status, lack of transportation to attend in-person appointments, and administrative barriers that made it more difficult for families to enroll or stay enrolled in WIC (National Academies, 2017a; Vargas & Pirog, 2016). Participation increased during the pandemic because of the multiple waivers that existed (e.g., remote benefits issuance, physical presence, allowance of uploading electronic certification documents) that streamlined certification and increased the fruit and vegetable benefit (National Academies, 2023c).
In FY 2018, WIC served approximately 6.9 million people and cost the federal government about $5.3 billion (USDA, 2019). Numerous studies using varied methods have found evidence of improved birth outcomes for participating women (see, e.g., Figlio, Hamersma, & Roth, 2009; Fingar et al., 2017; Foster, Jiang, & Gibson-Davis, 2010; Hoynes, Page, & Stevens, 2011). These studies found reductions in the likelihood of low birth weight (Figlio, Hamersma, & Roth, 2009; Hoynes, Page, & Stevens, 2011) and reductions in infant mortality (Khanani et al., 2010). Studies generally have found that the effects of WIC on birth outcomes are stronger for women with lower education levels, those living in areas of high poverty, and those who are African American (Hoynes, Page, & Stevens, 2011; Khanani et al., 2010). The Center on Budget and Policy Priorities concluded that WIC is a “cost-effective investment that improves the nutrition and health of low-income families—leading to healthier infants, more nutritious diets, and better health care for children, and subsequently to higher academic achievement for students” (Carlson & Neuberger, 2021, p. 1). Other studies—particularly in regard to 2009 improvements in the program that promoted consumption of fruits, vegetables, whole grains, and low-fat dairy products—have found improved dietary intake, perinatal outcomes, and early children development (Guan et al., 2021; Hamad et al., 2019a,b; Schultz, Byker Shanks, & Houghtaling, 2015; Tester, Leung, & Crawford, 2016).
Supplemental Nutrition Assistance Program
SNAP “provides food benefits to low-income families to supplement their grocery budget so they can afford the nutritious food essential to health and well-being” (USDA, 2023d, para. 1). The program targets those whose incomes are less than 130% of the federal poverty level. The maximum monthly benefit for a family of four in 2023 was $939, to be used for purchasing food at participating stores. The program expects that participating households will spend about 30% of their own financial resources purchasing food.
In 2017, an estimated 42 million people benefited from SNAP (Nchako & Cai, 2018). Children represented 44% of SNAP participants and received 43% of the benefits. One in five children in the United States received SNAP benefits in 2017. Participation in SNAP is generally high for those that are eligible (82% nationally, but as low as 55% in some states).
The main barrier to SNAP utilization among children is the ineligibility of many immigrant groups. Among immigrants, only those with permanent residency and those who are refugees can access SNAP benefits. Those who are undocumented and those awaiting permanent residency are not eligible. Having parents or siblings in the latter categories affects the benefit levels of eligible children who are U.S. citizens. Of the total number of SNAP participants, 8% were children with U.S. citizen status living with noncitizen adults (Cronquist & Lauffer, 2019). Undocumented noncitizens of the United States are not eligible for SNAP, but noncitizens who have lived in the United States for at least 5 years, receive disability-related assistance, or are less than 18 years of age are eligible (if they also meet the general eligibility requirements; USDA, 2023e).
SNAP has been linked to improvements in newborn health, improved child outcomes, reduced poverty, and improved economic and health outcomes in adulthood (Almond, Hoynes, & Schanzenbach, 2011; Bailey et al., 2020; Carlson & Keith-Jennings, 2018; Hoynes & Schanzenbach, 2015; Hoynes, Miller, & Simon, 2015; Hoynes, Page, & Stevens, 2011; Hoynes, Schanzenbach, & Almond, 2016). However, SNAP does not eliminate food insecurity. SNAP benefits per meal are estimated to be 25% less than the average cost of a low-income meal and do not cover the cost of a low-income meal in 99% of U.S. counties (Waxman, Gundersen, & Thompson, 2018). Evidence supports the importance of expanding SNAP benefits during the summer months, when children lack access to free and reduced-price lunches through school (Carlson & Keith-Jennings, 2018). A report by the National Academies on reducing child poverty found that expanding SNAP benefits, accounting for the needs of adolescents, and increasing benefits during the summer months could decrease child poverty rates by as much as 2.3%, depending on how large the expansion is (National Academies, 2019a).
Summer Food Service Program
Other programs, such as the Summer Food Service Program, also extends the availability of free meals for low-income populations into the summer months when children are not in school. Several demonstrations have shown that expanding meal programs can minimize the observed spike in food insecurity during the summer (Collins & Klerman, 2017; Gundersen & Ziliak, 2015).
Before 2020, many children lacked access to a food site during the summer. According to one study, in 2018, only 43% of children lived in a census tract with a meal site; this resulted in one child participating in the summer program for every seven participating in school lunch programs (Bauer & Parsons, 2020). During the COVID-19 pandemic, Congress authorized
electronic benefit transfer (EBT) payments, providing vouchers for grocery purchases instead of prepared meals during the summer. The summer EBT program was made permanent in December 2022. Thirty-five states, 5 territories, and 4 tribal governments have opted into the EBT program as of January 1, 2024. This new approach to tackling food insecurity and promoting nutrition has added flexibility and has helped address community challenges to accessing to this free service for those eligible.
Mental and Behavioral Health Services
Linking Actions for Unmet Needs in Children’s Health
SAMHSA’s (2023b) Linking Actions for Unmet Needs in Children’s Health (Project LAUNCH; and its sister program Indigenous-Project LAUNCH, focused on American Indian and Alaska Native communities and U.S. territories and Pacific jurisdictions), provides grants to partner organizations to screen children and caregivers for mental health needs, improve the capacities of adult caregivers of young children to help support their healthy socioemotional development, prevent behavioral disorders, identify and address behavioral concerns before they develop into serious emotional disturbances, and integrate behavioral health into primary care. The goal of Project LAUNCH has been to improve outcomes along multiple dimensions through cross-sector engagement to mitigate risk factors contributing to poor child outcomes and to promote protective factors that support resilience and healthy development (see Figure 7-7). One study in Massachusetts found indicators of program success, demonstrating longitudinal improvement in social, emotional, and behavioral outcomes of children and decreased symptoms of stress and depression in caregivers. This has led the way to expanding and improving sustainability of the model (Molnár et al., 2018). Current LAUNCH models aim, for example, to expand a team-based pediatric primary care approach—partnering an early childhood mental health clinician with a family or lived experience representative—to reach additional cities (Massachusetts); add mental health consultation to existing home visiting and parent engagement initiatives (California); support cross-sector engagement among departments of public health and mental health, university child development resources, and existing public–private partnerships for children (Alabama); and strengthen a family-focused network of culturally connected health and wellness services (Confederated Salish and Kootenai Tribes, n.d.).5 In FY 2022, $23.5 million was appropriated for Project LAUNCH (SAMHSA, 2022c).
___________________
5For more information and additional grantees, see https://healthysafechildren.org/project-launch-grantees

SOURCE: American Institutes for Research, n.d.
Other Funding and Programs for Supporting Mental Health in Particular Populations
SAMHSA funds numerous prevention and treatment programs for supporting positive mental and behavioral health. The rise in the number of programs reflects a robust response to growing concern nationally and in communities on the state of mental health for children and youth, as well as growing recognition of populations most in need. Many have criticized the lack of a comprehensive mental health care system for children and families (Bringewatt & Gershoff, 2010; Cummings, Wen, & Druss, 2011). As discussed in Chapter 5, mental health services have been notably fragmented from primary preventive care, but emergent efforts are focused on integration with primary care and community settings most accessible to individuals. Access to mental health programs is particularly valuable to marginalized populations that have experienced years of disadvantage
and discrimination. There is evidence that children and families from low-income and historically marginalized communities have a lower likelihood of engagement in high-quality mental health services (Hodgkinson et al., 2017; Rodgers et al., 2022) than those from other communities. As noted earlier, programs presented here do not capture all efforts in this area.
SAMHSA’s Infant and Early Childhood Mental Health (IECMH) grants provide services to children from birth to age 12 years and their parents/caregivers at risk for serious emotional disturbance through multigenerational therapy and evidence-based mental health promotion, prevention, and treatment interventions (SAMHSA, 2023a). IECMH services foster socioemotional functioning, the development of positive relationships with adults and peers, and the creation of a solid sense of identity and autonomy. A strong foundation of socioemotional processes is likely to prevent the emergence of mental health problems in infancy and early childhood, as well as later in the life course (National Academies, 2023g). In addition to individual grants to provide mental health services, the program supports a consultation center. The Center of Excellence for IECMH Consultation provides technical assistance to programs, classroom staff, and families (Ash, Mackrain, & Johnston, 2013; Brinamen, Taranta, & Johnston, 2012; Duran et al., 2009). A number of studies have documented the effectiveness of the Center for reducing child behavior problems, improving teacher–child relationships and classroom climate, and lowering suspension and expulsion rates and teacher turnover (Brennan et al., 2008; Center of Excellence for IECMH Consultation, 2021; Hepburn et al., 2013; Perry et al., 2010; SAMHSA, 2014; Shivers, Faragó, & Gal-Szabo, 2022). In FY 2022, IECMH grants were appropriated $9.98 million through SAMHSA (2022a).
SAMHSA’s National Child Traumatic Stress Initiative improves treatment and services for children, adolescents, and families that have experienced traumatic events. Authorized by Congress as part of the Children’s Health Act (2000), the initiative created a National Child Traumatic Stress Network (NCTSN) to increase access to effective trauma- and grief-focused treatment and services and support the development of trauma-informed child-serving systems (SAMHSA, 2024). NCTSN recognizes that certain populations are at increased risk for exposure to trauma, including children dealing with substance abuse or experiencing homelessness, those with caregivers in the active military or returned home as veterans, those who identify as LGBTQ+, those who have intellectual and developmental disabilities, and those whose family is experiencing economic stress. In FY 2022, NCTSN grantees provided screening to more than 84,000 individuals and evidence-based treatment to more than 42,000 children, adolescents, and family members, with thousands more benefiting indirectly through the training and consultation provided by NCTSN grantees. In FY 2022, the initiative was appropriated $81.88 million through SAMHSA (2022c).
SAMHSA’s Tribal Behavioral Health Grants provide support for mental health care for tribes and tribal organizations and are intended to prevent and reduce suicidal behavior and substance abuse and to promote positive mental health among American Indian and Alaska Native young people ages 24 years and younger. Goals for these grants include developing and implementing an array of integrated services and supports for improving outcomes by working with tribes to support strategies that have been shown to be effective or promising in Native communities. In FY 2022, the Tribal Behavioral Health Grants program was appropriated $20.73 million through SAMHSA (2022c).
EXPANDING RESOURCES TO ADVANCE COMMUNITY-LEVEL HEALTH PROMOTION AND DISEASE PREVENTION
As discussed above, the federal government provides a great deal of funding and support for direct and indirect health care through state, tribal, and local agencies. Many federal programs serve important needs in local communities, and many programs have provided assistance for decades and have evolved to address a changing society. However, the needs are great, and many programs fail to reach all eligible children, youth, and families. Furthermore, several barriers hamper efforts to achieve positive population health outcomes and health equity. Promising models need to be expanded so they can benefit more children and families in local communities. There is opportunity to further integrate programs with health care systems to identify children, youth, and families in need and monitor progress together. Important as well is adapting these models to meet the specific cultural and community needs of participant children and families. Several funding sources could become more available and widely used to address some of these needs.
Community Benefit and Reinvestment Activities
Nonprofit Hospitals
Nonprofit hospitals benefit financially from tax exemptions at the federal, state, and local levels when they invest in community benefit activities (i.e., initiatives, activities, and investments undertaken to improve health in the communities they serve; Government Accountability Office, 2023e; Hilltop Institute, n.d.). Of approximately 6,000 hospitals in the United States, about half are identified as nongovernment, nonprofit community hospitals and thus qualify for tax-exempt status (American Hospital Association [AHA], 2024). AHA (2024) estimates the total forgone federal revenue from the hospital tax exemption at $12.4 billion in 2019.
In exchange for tax exemption, hospitals engage in a variety of community benefits that they must document. Significant opportunities exist for government institutions to address gaps in coordination and oversight of these investments (Riley, Clary, & Higgins, 2019). Although these funds originate from health care systems via tax exemption, they need not be directed toward clinical care. Community benefits from nonprofit hospitals, and potentially health plans, represent potential sources of funding that can be directed toward a wide variety of activities, including community-based primary preventive health care for children and adolescents. Input from a broad set of stakeholders, including those engaged in other federal planning activities around maternal and child health, can also ensure that the investments align with other local initiatives. With local stakeholder input, hospitals can tailor their programs and practices flexibly to address their communities’ specific needs and concerns (Hut, 2023).
The federal government has implemented policies for quantifying community benefits of hospitals and conducting community health needs assessments in order to increase transparency and accountability. However, community health needs assessments are not required explicitly to examine any particular priority area, such as community-based prevention, or any population, such as children. Thus, there is a disconnect between services that could benefit child health, in both the short and long terms, and the investments that are actually made under community benefit, particularly investments that go beyond direct patient care in the facility. Planning for child health promotion and prevention services through community needs assessment is promoted through many disparate channels. To illustrate, states are required by federal law to conduct comprehensive needs assessments as a condition of Title V MCHB Grant support every 5 years. At the same time, tax-exempt hospitals must report their community health needs assessments every 3 years.
A major step toward increased transparency came in 2009, when the Internal Revenue Service (IRS) published an updated version of its Form 990, including Schedule H, a special tax form for hospitals on which community benefit activities are catalogued (Evashwick & Jackson, 2020). The IRS also began requiring hospital facilities to track their community benefits spending in relation to costs incurred by, for example, bad debt or the cost of Medicare participation. Hospitals record, for example, charity care and Medicaid payment shortfalls as community benefit, along with activities that are not tied to patient care but might involve community health improvement services (Kanter et al., 2020). Following the implementation of Schedule H, the Patient Protection and Affordable Care Act (ACA, 2012 § 9007) instituted triennial community health needs assessments for nonprofit hospitals beginning in 2012 (Evashwick & Jackson, 2020; IRS, 2023). As part of these assessments, hospitals are required to solicit
and consider input from health experts and may also consider input from consumer groups, community organizations, academics, local governments, and other community stakeholders (National Academy for State Health Policy, 2019). Hospital organizations with multiple facilities must conduct a community health needs assessment for each facility. Additionally, hospitals must promulgate implementation strategies for addressing their identified community health needs. However, there is no legal definition of “community benefits” and little guidance on how to integrate community experts into assessments, which leaves hospitals with considerable flexibility in implementing strategies and interventions in their communities (Riley, Morrison, & McEvoy, 2019; Santos, 2020).
In addition to calls for greater transparency and planning around community investments by hospitals, there has been considerable, ongoing policy debate around the level of community benefit investment, particularly whether hospitals are generating total benefits commensurate with the financial relief they receive through tax exemption (Congressional Research Service, 2010). One comparison of the value of community benefits and tax exemptions in nonprofit hospitals found that the amount of community benefits and charity care provided by nonprofits varied substantially across organizations and that 86% of nonprofit hospitals provided less charity work than the value of their tax exemptions (Zare, Eisenberg, & Anderson, 2022). A separate analysis found that nationally this gap amounted to a total fair-share deficit of $25.7 billion (Lown Institute, 2024).
Other studies have found that despite lower uninsured rates since the passage of the ACA, community benefits among nonprofit hospitals have not increased over time (Kanter et al., 2020), as might be expected with greater resources available to hospitals. Medicaid expansion under the ACA had a significant impact on hospital financing, reducing uncompensated care from 4.1 percentage points to 3.1 percentage points of hospital operating costs based on short-run estimates (Dranove, Garthwaite, & Ody, 2016). These reductions in uncompensated care occurred almost exclusively in states with Medicaid expansions and were larger in hospitals that had higher pre-ACA uncompensated care burdens and nonprofit hospitals. Despite the reduction in uncompensated care, there appears to be little evidence that community benefits among nonprofit hospitals increased. A separate news report revealed that seven of the ten most profitable hospitals in the country are nonprofits and found that since passage of the ACA, revenues of the most profitable hospitals have increased by 15%, while charity care has dropped by 35% (Ofri, 2020). The Medicaid expansion has had a somewhat complex impact on the accounting of community benefits, decreasing charity care, but increasing the amount counted as “unreimbursed” Medicaid expenditures, meaning aggregate payments declined relative to aggregate charges (Kanter et al., 2020). Ultimately, research does
not support that insurance expansion under Medicaid increased nonprofit hospitals’ spending on community-directed, preventive services.
Nonprofit hospitals are exempt not only from federal taxes, but also from state income tax, state and local sales tax, and state and local property tax. In some states, there have been more deliberate steps to direct community benefit spending than at the federal level. Eleven states have their own reporting requirements (Hilltop Institute, n.d.), while Massachusetts has established elaborate guidelines for community-benefit priority areas, reporting, and evaluation as part of its determination-of-need process for hospitals (Office of the Attorney General, 2018). Five states extend beyond reporting and explicitly require a minimum spending amount on community benefits for nonprofit hospitals. In Illinois and Utah, for example, these amounts are tied to the amount of the hospitals’ property tax exemption (Atkeson & Higgins, 2021).
Tax-Exempt Health Plans
Despite policy movement around greater accountability among tax-exempt hospitals, in most cases there are no analogous community benefit requirements or reporting for tax-exempt health insurance plans. Recently, a national analysis identified 92 federally tax-exempt health plans (60 plans excluding dental plans) and examined the “profits” (i.e., total revenues less total expenses) generated by health insurance plans that are tax exempt under federal law as 501(c)(4) “social welfare organizations” (Plummer et al., 2023). This represents a missed opportunity to engage an important health stakeholder in community health planning and promotion. These tax-exempt health plans do not face similar transparency requirements to tax-exempt hospitals. One exception is Massachusetts, which established community benefits guidelines for health maintenance organizations that parallel the guidelines for nonprofit hospitals. These guidelines apply only to health maintenance organizations, not other types of insurers, such as preferred provider organizations.
Community Reinvestment Approaches
Changing community benefit requirements would target only tax-exempt hospitals and health plans. For-profit entities, on the other hand, contribute tax dollars to federal, state, and local governments, which may or may not be invested in primary preventive services for children. Reinvestment approaches could span health care entities regardless of their tax status.
A somewhat related example exists in the banking realm. Under the Community Reinvestment Act (CRA, 1977), banks are encouraged to help meet the credit needs of communities in which they do business, with a
particular focus on low- and moderate-income communities. Such investments are not required but are viewed favorably in merger and other business reviews. Under the CRA, banks report performance metrics in a standardized fashion, depending on their size, and ratings are made public and searchable. There is evidence that the CRA induced small increases in bank activity in low- and middle-income areas (Brevoort, 2022).
While implementation in the health care context may be more complex, the basic principle of a reporting requirement with particular focus and benefit for disadvantaged communities has precedence in other sectors. A strict approach in the health care context might serve to tie reporting and evaluation more stringently to certificate-of-need standards where they exist, or to accreditation more broadly.
Financing Mechanisms for Supporting Community Partnerships
Increased investment in child health through population- and community-level primary prevention can be gained from cross-sector work among public health, health care, and other child-serving sectors and will require repurposing of some funds and additional resources. Several financing strategies are articulated here.
Repurposing Funds for Multisector, Child Health–Related Outcomes
Major social service programs in housing, employment, and transportation invest billions of dollars in U.S. cities and states annually. Very few of these programs are directed, advised, or evaluated in terms of child outcomes, even though they are strongly connected to child health. Large child health care systems have increasingly engaged with public agencies and private partners in focusing major projects on aspects of child health or community development in areas with child health concerns.
The Center for Community Investment6 underscores the important role in many communities of large health care systems’ political, operational, and fiscal strength in facilitating the pipeline of community development. Levels of collaboration across sectors vary, but they are similar to the collaborative activities described previously between public health and health care. Steps include (1) shared goals and accountability (easiest) in investments, (2) shared governance and collaboration on improvement (harder), (3) shared data (harder yet), and (4) shared savings (hardest). Often, these steps take advantage of the relative strengths of various partners in the activities. For example, when appropriate, public officials can make available with right of first refusals any properties with
___________________
tax delinquency or abandonment. Private developers bring construction and application experience to efforts such as the Low-Income Housing Tax Credit competition. Hospitals often have expertise in subcontracting construction, legal aspects of property acquisition, and project management. Together, these teams can be highly competitive for contested tax credit deals.
Reclassification of Community Prevention as Part of Medical Loss Ratio
The medical loss ratio (MLR) is the proportion of medical premiums paid to insurers that reimbursed provider claims in a given period (Centers for Medicare & Medicaid Services [CMS], 2010). In 2010, the ACA required that the National Association of Insurance Commissioners develop standardized regulations that provided minimum MLRs (i.e., limiting administrative costs and profit) in public-sector plans and required transparency in reporting. The MLR is critical to managed care and accountable care organizations caring for children, in that care investments that are covered in the MLR will gradually be reflected in the capitation rate they are paid. Care investments that are not counted as part of the MLR will count only as additional overhead without revenue.
Currently, community prevention is not counted in CMS guidance on actuarial calculations of the MLR, so any prevention investments made count against managed care or accountable care organizations that take the initiative with community prevention. For example, evidence-based community programs such as the Good Behavior Game for young children (Kellam et al., 2011) or Earned Income Tax Credit assistance, both of which improve long-term outcomes, are added costs when used by managed care or accountable care organizations. If they were counted as part of the MLR rules by CMS, these expenses would allow improved capitation rates for value-based purchasing contracts caring for children and adolescents.
Pay-for-Success Models
Pay-for-success models, including the program supported by the U.S. Treasury Department, offer the enticing concept of using private-sector investments to support public goods or outcomes. This model creates an avenue for private-sector partners to fund preventive health interventions and requires states to pay only if the private partner delivers improved outcomes. First trialed for prison recidivism in the United Kingdom, pay-for-success models encourage investors to bid on supporting investments that generate public savings and return the savings to investors. Pay-for-success models have generated investments in teen pregnancy prevention in South Carolina and early school intervention in Utah.
The goal of the model is clear: to monitor and improve outcomes on average; however, a number of downsides, including two main concerns, have been noted.
First, pay-for-success models have been most attractive as returns for investors when an expensive event (e.g., return to prison) is avoided and the savings are generated to a single public agency (such as the justice system). To identify such opportunities, a feasibility study is required before projects begin—these studies call for significant collaboration and buy-in. Kennedy-Moulton and colleagues (2022) noted that barriers identified by feasibility studies include legal and administrative complexity, community-based organization capacity, and agreeable outcome tracking. As a result, although feasibility studies have been conducted in more than 65 communities nationwide, few projects have been fully funded (Karaca-Mandic et al., 2023).
Second, pay-for-success programs that are funded have an increased incentive to engage in “risk-score gaming”—that is, to target those most likely to succeed, which has the potential to widen disparities if based on proxies for advantage or disadvantage, such as neighborhood or race (Chomilo, 2023). Prevention programs for children tend to have very long-term yields with no single event dominating savings and no single agency garnering most of the savings. As a result, pay-for-success models for children have not attracted a great deal of private investment. Instead, they have received very modest investments from mission-driven foundations and investors, which limits their scope.
Mandated Investment by Health Plans
Another option for increasing resources for child-focused prevention and health promotion involves mandated investment by health plans and possibly provider organizations. Mandated investment can come in any one of several ways:
- Health plans are taxed directly, with funds set aside by the taxing authority for prevention investments—California is currently undertaking this approach (Durham, 2023). Massachusetts had a similar plan from 2012 to 2020. As of 2023, 18 states tax their health plans, with varied uses for those funds.7
- Health plans are subject to a minimum investment requirement specified by state or federal regulatory authorities, as in the CRA (1977) for the banking industry.
- Health plans have incentives or capitation withheld until specific outcomes are achieved. Oregon and Ohio have instituted initiatives that do not require specific health plan investments but withhold dollars until outcome goals are met.
___________________
7See https://www.kff.org/other/state-indicator/states-with-an-mco-provider-tax-in-place
To date, no studies examine the effectiveness of these strategies for generating resources to invest in prevention and child health. Moreover, when funds are generated, considerable questions remain about how best to expend them to enable flexibility, rapid cycle improvement, and community-focused services. Mann and Ferguson (2020) argue that developing flexible community wellness funds provides the most opportunity to improve child health in a way that is respectful to community wishes and allows local strengths to be brought to the fore.
CONCLUSION
Primary preventive care is critical for child populations and dictates the assurance of conditions in which families and communities can be healthy and well. Many communities in the United States are challenged to provide children and families with the environments and services they need to be healthy; in these contexts, the role of public health needs to be intensified. State and local health departments, however, are woefully underfunded. Many public health efforts lack coherence and coordination. Moreover, no minimum package of public health services is ensured in each locality.
The federal government provides significant funding for preventive programs around maternal health, early child development, and nutrition. There is less funding available for mental and behavioral health services, but these programs are starting to expand. Despite the commitment to support populations in need, significant variations remain in the extent of support among states, and investments are insufficient to reach all who would be eligible for the programs. Another consideration is whether program requirements are appropriately flexible to accommodate specific community needs. This chapter presented several strategies for increasing resources and reinvestment in preventive activities aimed at improving child and community health.
Public health defined broadly goes beyond government public health departments and requires collaboration across sectors. Substantial and lasting improvements in population health can be achieved only through collaborative efforts with shared goals between the health care systems and public health efforts. Nonprofit hospitals and health care systems can focus their community benefit dollars to pursue long-term strategies for building healthier neighborhoods and advancing upstream initiatives aimed at mitigating the root causes of poor health and wellbeing, especially in low-income communities. Health care systems and government health agencies can be anchors and advocates for the equitable expansion of high-quality care and services, responsive to health-related social needs in the communities they serve.
This page intentionally left blank.

































