Protecting Maternal Heart Health: Prevention and Care Before, During, and After Pregnancy (2026)
Chapter: 4 Preventive Services to Address Gaps in Cardiovascular Risk: Screening, Early Detection, and Clinical Management
4
Preventive Services to Address Gaps in Cardiovascular Risk: Screening, Early Detection, and Clinical Management
INTRODUCTION
Effective prevention of cardiovascular disease (CVD) before, during, after, and between pregnancies requires attending to both individual risk factors and the systems that deliver care. Building on the process Chapter 3 described for identifying priority preventive clinical services and evidence gaps, Chapters 4 and 5 examine nine topics with the potential to reduce cardiovascular risk and improve pregnancy and postpartum outcomes among women of reproductive age, including those who are pregnant, postpartum, or in the interpregnancy period. The focus is on preventive services that could feasibly be delivered in clinical settings.
The committee adapted the structured approach used by the U.S. Preventive Services Task Force (USPSTF) to guide its reviews, tailoring it to reflect the specific context of this report. For each service, the committee sought to apply a consistent framework while allowing flexibility to highlight unique features of the intervention, target population, or care setting. As relevant for each question, the reviews include the following:
- Overview of the question and evidence gap;
- Summary of the evidence, including key study characteristics and main findings;
- Timing and frequency of the intervention or service;
- Reproductive stage and risk stratification, including which patients are targeted and how risk is defined;
- Potential benefits, for both cardiovascular and pregnancy-related outcomes;
- Potential harms, including unintended adverse effects or burdens on patients and systems;
- Cost and cost-effectiveness when such evidence is available;
- Population considerations, including access and implications for those at highest risk;
- Implementation considerations, with additional crosscutting issues addressed in Chapter 6; and
- Summary and committee considerations, integrating the evidence, and highlighting remaining research needs.
The nine questions are organized to reflect two broad domains: (1) screening, early detection, and clinical management of cardiovascular risk and conditions in the prepregnancy, pregnancy, postpartum, and interpregnancy periods; and (2) care delivery and supportive services that may enhance access to, coordination of, and adherence with preventive cardiovascular care. Table 4-1 provides the research questions and indicates the reproductive period(s) each service targets.
This chapter focuses on five research questions in the first domain. It includes strategies to identify elevated cardiovascular risk or early manifestations of disease, including structured risk assessment tools and approaches to blood pressure (BP) screening and management. Chapter 5 examines four research questions in the second domain, including models and modalities of care delivery, such as telehealth, integrated cardio-obstetrics care, supportive services, and interventions to promote effective transitions of care.
Throughout Chapters 4 and 5, the committee emphasizes how these preventive services might address known gaps in cardiovascular risk assessment and management in the maternal health continuum. Detailed discussion of crosscutting implementation challenges appears in Chapter 6.
SCREENING AND EARLY DETECTION
Effective prevention of CVD and related complications before, during, and after pregnancy begins with timely recognition of risk. This chapter examines strategies that aim to detect elevated cardiovascular risk or early manifestations of cardiovascular conditions across the prepregnancy, pregnancy, postpartum, and interpregnancy periods. The research questions address several complementary approaches: BP screening and management during pregnancy and postpartum, structured health and lifestyle assessments (Life’s Essential 8 [LE8]), and cardiovascular risk assessment tools. The chapter also considers interventions to increase clinicians’ and patients’ awareness of urgent maternal warning signs (UMWS), with the goal of facilitating earlier recognition of symptoms and prompt care seeking.
TABLE 4-1 Preventive Service Research Questions and Reproductive Periods Covered
| Research Question | Reproductive Period | ||
|---|---|---|---|
| Pre pregnancy | Prenatal | Postpartum/Inter pregnancy | |
| Presented in Chapter 4 | |||
| Prenatal Blood Pressure (BP) Target: Does BP management to a target of <140/90 during pregnancy improve maternal outcomes relative to a higher target? | X | ||
| Enhanced Postpartum Hypertension Management: Does enhanced postpartum hypertension management for patients with hypertensive disorders of pregnancy (including chronic hypertension) improve outcomes? | X | ||
| Urgent Maternal Warning Signs: Does screening for urgent cardiovascular warning signs (or Urgent Maternal Warning Signs), including counseling patients to self-screen for such signs, reduce severe maternal morbidity or mortality? | X | ||
| Structured Cardiovascular Risk Assessment Tools: Does screening with California Maternal Quality Care Collaborative Cardiovascular Disease in Pregnancy toolkit or Malhamé et al.’s cardiovascular disease (CVD) risk assessment tools (2021, 2022) in pregnancy and postpartum improve identification of women with previously unrecognized CVD and improve cardiovascular health outcomes? | X | X | |
| Life’s Essential 8: For women of reproductive age at increased risk of CVD, does comprehensive screening and intervention for risk factors underlying cardiovascular health (specifically, using Life’s Essential 8 screening tool) reduce risk of pregnancy-related cardiovascular morbidity and mortality? | X | X | X |
| Presented in Chapter 5 | |||
| Telehealth: Does the use of telehealth approaches in the prepregnancy, prenatal, or postpartum period improve CVD outcomes? | X | X | X |
| Research Question | Reproductive Period | ||
|---|---|---|---|
| Pre pregnancy | Prenatal | Postpartum/Inter pregnancy | |
| Integrated Cardio-Obstetrics Care Models: Do integrated cardio-obstetrics care models improve cardiovascular and pregnancy outcomes among high-risk pregnant women? | X | ||
| Supportive Services: Do supportive services (e.g., doulas, peer navigation, or other community health workers) improve CVD-related outcomes? | X | X | |
| Postnatal Transition of Care: Do interventions to improve the transition from hospital to outpatient care, or interventions to ensure effective transitions of care to a primary care provider, or actual care by a primary care provider within 12 months postpartum (to improve the transition from outpatient postpartum care to longitudinal preventive care for patients with CVD risk factors) reduce cardiovascular morbidity and morbidity and/or adverse pregnancy outcomes in subsequent pregnancies? | X | ||
NOTES: The items listed in this table represent the research questions reviewed by the committee and do not imply that each service is recommended for implementation. Recommendations are presented separately in Chapter 7 and reflect areas where the committee determined that evidence was sufficient to support implementation guidance. BP = blood pressure; CVD = cardiovascular disease.
PRENATAL BLOOD PRESSURE TARGET
Overview of the Question and Gap
Hypertensive disorders of pregnancy (HDPs) affect nearly 16 percent of U.S. hospital deliveries and are associated with increased cardiovascular maternal morbidity and mortality (Ford et al., 2022). Pregnant women with chronic hypertension (HTN) or gestational HTN are at an increased risk of preeclampsia, stroke, myocardial infarction, heart failure, and death during pregnancy or postpartum (Garovic et al., 2022). Gestational HTN is defined as HTN diagnosed before pregnancy or before 20 weeks’ gestation or HTN that persists ≥ 12 weeks postpartum following a HDP, and the latter is defined as new-onset (de novo) HTN at ≥20 weeks’ gestation; however, HTN first identified at ≥20 weeks can also reflect unrecognized chronic HTN among women who initiate prenatal care later in pregnancy (ACOG, 2020a). A lack of consensus exists in guidelines about the optimal
BP thresholds at which to initiate treatment during pregnancy, due to limitations in high-quality evidence (Sinkey et al., 2020). Table 4-2 outlines the clinical criteria used to define HTN and severe-range HTN in pregnancy.
It is important to recognize that diagnostic definitions and treatment thresholds for HTN in pregnancy differ from those used in nonpregnant adults. Recent American College of Cardiology/American Heart Association (ACC/AHA) guidelines for the general adult population define stage 1 HTN at ≥130/80 mmHg and recommend treatment targets accordingly (Jones et al., 2025). In contrast, obstetric practice has historically defined HTN in pregnancy at ≥140/90 millimeters of mercury (mmHg) and uses different thresholds for treatment initiation and escalation, reflecting pregnancy-specific physiology, fetal considerations, and the available evidence base. Explicit awareness of these distinctions may improve interdisciplinary communication among obstetric, primary care, and cardiology clinicians.
Until 2022, the American College of Obstetricians and Gynecologists (ACOG) recommended initiating antihypertensive therapy in pregnancy only for severe-range chronic HTN or gestational HTN (systolic BP [SBP] ≥160 mmHg or diastolic BP [DBP] ≥110 mmHg) (ACOG, 2019, 2022). For women with chronic HTN, goals were set at 120–159/80–109 mmHg, with earlier treatment considered only for comorbidities (ACOG, 2019, 2020a). These recommendations reflected the absence of definitive data
TABLE 4-2 Hypertension Classification Criteria During Pregnancy
| Term | Definition |
|---|---|
| HTN in Pregnancy | SBP ≥140 mmHg or DBP ≥90 mmHg, or both, on two occasions at least 4 hours apart |
| Severe-Range HTN in Pregnancy | Sustained SBP ≥160 mmHg or DBP ≥110 mmHg, or both, with verification within 15 minutes to prevent treatment delays |
| Chronic HTN | HTN diagnosed or present before pregnancy or before 20 weeks’ gestation, or HTN that persists ≥ 12 weeks postpartum following a HDP |
| Gestational HTN | New-onset (de novo) HTN occurring at ≥20 weeks’ gestation |
| De Novo Postpartum HTN | New-onset (de novo) HTN appearing postdelivery through 6 weeks postpartum after a normotensive pregnancy |
| Preeclampsia | New-onset HTN after 20 weeks’ gestation accompanied by proteinuria or signs of end-organ dysfunction |
| Chronic HTN with Superimposed Preeclampsia | Preeclampsia occurring in a patient with preexisting chronic HTN |
NOTES: DBP = diastolic blood pressure; HDP = hypertensive disorder of pregnancy; HTN = hypertension; SBP = systolic blood pressure; mmHg = millimeters of mercury.
SOURCE: ACOG, 2019, 2020a; Goel et al., 2015.
demonstrating maternal or perinatal benefit with nonsevere-range treatment for either chronic HTN or gestational HTN and concerns that antihypertensive therapy may increase the risk for small for gestational age (SGA) newborns.
However, in the last decade, evidence has been increasing to support a lower BP threshold for initiating antihypertensive therapy in pregnancy, especially for women with chronic HTN. The Chronic Hypertension and Pregnancy (CHAP) randomized trial demonstrated that treating pregnant women with nonsevere-range chronic HTN to reach a BP goal of <140/<90 mmHg led to an 6.8 percentage-point absolute reduction (about an 18 percent relative reduction) in adverse pregnancy outcomes (APOs) compared to no treatment, without evidence of increased risk of fetal growth restriction (Tita et al., 2022). The CHAP trial led to new recommendations from ACOG, Society for Maternal-Fetal Medicine, and ACC/AHA to use a threshold BP of 140/90 mmHg for initiation or titration of medical therapy for chronic HTN in pregnancy (ACOG, 2022; Jones et al., 2025; SMFM, 2022). The recommended BP threshold for treatment of gestational HTN (SBP ≥160 mmHg or DBP ≥110 mmHg) was not changed.
This review evaluates the question “Does BP management to a target of <140/90 mmHg during pregnancy improve maternal outcomes relative to a higher target?” The committee examined evidence from randomized controlled trials (RCTs), cohort studies, meta-analyses, and clinical guidelines to assess whether tighter BP control (for chronic HTN or gestational HTN) improves maternal cardiovascular outcomes and pregnancy outcomes without increasing fetal risk. The research question addressed BP management during pregnancy broadly and included outcomes such as severe-range HTN and preeclampsia when reported in the reviewed studies. Although treatment to a target of <140/90 mmHg was associated with reductions in severe-range HTN and, in some studies, preeclampsia among women with chronic HTN, the strength of evidence varied across hypertensive conditions. The committee did not evaluate interventions designed specifically to prevent preeclampsia (e.g., aspirin prophylaxis), which are addressed in existing clinical guidelines.
Summary of the Evidence
The initial literature search yielded 371 records with publication dates from January 2010 to July 2025, including one duplicate. Of the 370 unique articles screened at the abstract level, the committee identified 43 as potentially relevant and moved to full-text review. Twenty-one articles met inclusion criteria, with the most common reasons for exclusion being wrong intervention, wrong population, or no relevant outcomes. Articles reporting studies conducted in the United States and other very high–income United Nations (UN) countries were eligible for inclusion. The committee
conducted risk-of-bias assessments and data extraction for the 21 empirical studies that remained after full-text review.
The 21 articles were all published in the last decade, including RCTs, cohort and observational studies, and systematic reviews. Quality of evidence was good (13 studies), fair (6 studies), and poor (2 studies). Among the 19 studies with good and fair quality, 12 addressed only chronic HTN, and 7 addressed both chronic HTN and gestational HTN.
Evidence for Chronic Hypertension Target <140/90 mmHg
The evidence that supports lowering the BP threshold for the prenatal management of chronic HTN to 140/90 is substantial, driven by one well-designed, good-quality RCT (CHAP), a good-quality secondary analysis of the Control of Hypertension in Pregnancy Study (CHIPS), and two fair-quality recent meta-analyses (Abe et al., 2025; Attar et al., 2023; Magee et al., 2015, 2016; Tita et al., 2022). Prior studies have consistently shown that BPs of 140–159/90–109 mmHg are associated with APOs, including severe preeclampsia, indicated preterm birth, placental abruption, and perinatal death (Ankumah et al., 2014). Although small randomized trials of antihypertensive therapy during pregnancy showed moderate evidence that it probably halves the risk of developing severe HTN, the effect on other maternal and perinatal outcomes remained unclear, and this evidence did not alter guidelines due to continued concerns about perinatal outcomes (Abalos et al., 2018).
The open-label, multicenter CHAP trial randomized 2,408 pregnant women with nonsevere chronic HTN before 23 weeks’ gestation to receive antihypertensive medications for a BP goal of <140/<90 mmHg (active treatment) or to standard treatment in which antihypertensive therapy was withheld or stopped at randomization unless severe HTN developed (SBP ≥160 mmHg or DBP ≥105 mmHg) (Tita et al., 2022). The active treatment group had lower risk of adverse maternal outcomes, including severe HTN and preeclampsia with severe features, with no significant differences in major adverse cardiovascular events (maternal death, heart failure, heart attack, or stroke), although the composite rates were low. Women who received active treatment also had lower risk of preterm birth, placental abruption, or fetal or neonatal death.
To test the effects of less-tight versus tight control on APOs, the CHIPS randomized trial assigned 987 women (74.6 percent with chronic HTN) with nonsevere HTN1 at 14 weeks’ to 33 weeks and 6 days’ gestation
___________________
1Defined by the authors as nonproteinuric preexisting or gestational HTN, office dBP 90–105 mmHg (or 85–105 mmHg if on antihypertensives). Severe HTN was defined as systolic BP ≥160 mmHg or a dBP ≥110 mmHg, measured twice, 15 minutes apart (Magee et al., 2016).
to less-tight (target DBP <100 mmHg) or tight (target DBP <85 mmHg) control. The trial found no significant differences in either the primary (pregnancy loss or high-level neonatal care) or secondary (serious maternal complications) outcome, although less-tight control was associated with higher rates of severe-range HTN (Magee et al., 2015). A post-hoc analysis of the CHIPS trial used mixed effects logistic regression to determine if clinical outcomes differed by whether patients developed severe HTN, adjusting for treatment arm and baseline factors (Magee et al., 2016). Severe-range HTN was associated with higher rates of preeclampsia and adverse perinatal outcomes in both treatment arms, but it was associated with secondary maternal outcomes (maternal death or serious maternal complications) only in the less-tight control arm. The results led to new recommendations for antihypertensive therapy for lower BP thresholds (SBP ≥135–140 mmHg or DBP ≥85–90 mmHg) in pregnant women with chronic HTN and gestational HTN in international guidelines but not the United States (Brown et al., 2018; Butalia et al., 2018; Webster et al., 2019). Subsequent economic analysis of CHIPS in Canada found that tight control was associated with possibly lower health care system costs related to reducing costs of neonatal care (Ahmed et al., 2016).
Recent meta-analyses of RCTs of good quality (including CHIPS and CHAP) that compared the effects of BP-lowering treatment versus no treatment among pregnant women with nonsevere HTN concluded that targeting a BP of <140/90 mmHg significantly reduced the risks of severe HTN, preeclampsia, preterm birth, and placental abruption for those with chronic HTN (Abe et al., 2025; Attar et al., 2023).
Relative to the international CHIPS trial, which recruited participants from 16 countries, the CHAP trial was conducted in the United States and enrolled a higher proportion of non-Hispanic Black and Hispanic women, more closely mirroring the racial and ethnic diversity of U.S. pregnant women with chronic HTN. The CHAP trial was not powered to assess differences in treatment effects across patient subgroups. However, the overall treatment effect was similar in non-Hispanic White, non-Hispanic Black, Hispanic, and other racial or ethnic groups and participants with and without diabetes. The point estimates for the risk ratio approximated 1.0 for women with newly diagnosed chronic HTN and those with enrollment body mass index (BMI) ≥40 kilograms per square meter (kg/m2), so further evaluation of treatment effect in these subgroups needs to be performed (Tita et al., 2022).
The timing of antihypertensive therapy during the first trimester was not addressed in the CHIPS or CHAP trials. However, observational studies of BP during the first trimester have suggested that women with chronic HTN who need antihypertensives in the first trimester have higher rates of severe-range HTN, preeclampsia, and SGA outcomes (Nzelu et al., 2018).
Aspirin use during pregnancy did not appear to influence the treatment effect in the CHAP or CHIPS trials. In the CHAP trial, approximately 45 percent of the patients took aspirin at baseline, increasing to 77 percent by delivery. Less than one-third of the participants in the CHIPS trial took aspirin at baseline. The relationship between aspirin therapy and BP treatment on outcomes was not evaluated.
Potential Benefits of Targeting a BP Threshold <130/80 for Chronic Hypertension
The ACC/AHA guidelines recommend initiation of antihypertensive therapy in nonpregnant women with stage 1 HTN (SBP 130–139 mmHg or DBP 80–89 mmHg) who have additional cardiovascular risk factors, thus increasing the number of reproductive-age women eligible for treatment (Jones et al., 2025; Topel et al., 2018). In contrast, prior to 2022, ACOG generally recommended antihypertensive therapy in pregnancy only for persistent severe-range BPs (≥160/110 mmHg), with expectant management and closer surveillance for milder elevations (ACOG, 2019). This approach was revised following publication of the CHAP trial, after which ACOG lowered the treatment threshold to 140/90 mmHg for chronic HTN in pregnancy (ACOG, 2022).
The current evidence review identified some limited evidence that using a BP threshold of <130/80 mmHg in pregnancy may reduce adverse maternal cardiovascular outcomes. Observational studies have suggested that both stage 1 HTN and elevated BP category (SBP 120–129 mmHg and DBP <80 mmHg) identifies otherwise “low-risk” women with significant increased risk for preeclampsia compared to a normal BP of <120/80 mmHg (Hauspurg et al., 2019b; Reddy et al., 2020; Sabol et al., 2021; Sisti et al., 2023). Systematic reviews have concluded that a BP of 120–140 mmHg/80–90 mmHg at <20 weeks’ and >20 weeks’ gestation are associated with increased risk of preeclampsia and APOs (Sisti et al., 2023; Slade et al., 2023a,b). However, lowering the diagnostic threshold for HTN in pregnancy from 140/90 mmHg to 130/80 or 120/80 mmHg would not accurately predict women at increased risk for preeclampsia, except possibly for women who are underweight (BMI <18.5 kg/m2) or had previously given birth with no prior history of preeclampsia (Slade et al., 2023a, 2025a,b).
A fair-quality prespecified secondary analysis of the CHAP trial grouped participants by their average postrandomization prenatal clinic BPs to evaluate the association between SBP <130 mmHg and DBP <80 mmHg versus 130–139/80–89 mmHg and pregnancy outcomes (Bailey et al., 2023). The lower average BP was associated with a lower risk of preeclampsia with severe features and indicated preterm birth but not increased risk of SGA
infants. The possibility of using a lower threshold for patients with diabetes has also been discussed, as diabetes is associated with increased risk for preeclampsia and severe cardiac maternal morbidity. A separate secondary analysis of the CHAP trial of 434 pregnant women with both chronic HTN and diabetes found that those who achieved the lower goal of <130/80 mmHg (versus 130–139/80–89 mmHg) had less preeclampsia with severe features and fewer planned (medically indicated) preterm births before 37 weeks for maternal or fetal indications or neonatal intensive care unit (NICU) admissions (Harper et al., 2025). However, several confounders limit its interpretation, and the effect of initiating treatment to achieve a BP of <130/80 mmHg was not evaluated.
Evidence Regarding Treatment of Gestational Hypertension
The evidence for using a lower BP threshold of <140/<90 to initiate or escalate treatment for gestational HTN is moderate but less robust than for chronic HTN. In a meta-analysis of RCTs of BP-lowering treatment among pregnant women with nonsevere HTN, treatment effects did not differ significantly by disorder subtype (gestational HTN versus chronic HTN) for maternal and perinatal outcomes. The one exception was for placental abruption, for which the association appeared more favorable in chronic HTN (Abe et al., 2025). Although the majority of the CHIPS trial participants had chronic HTN, results for the primary and secondary outcomes were similar for gestational HTN and chronic HTN (Magee et al., 2015). A CHIPS subanalysis isolating the 249 gestational HTN participants was not powered to detect differences in the primary or secondary outcomes (Magee et al., 2016); however, the raw data showed a lower rate of the secondary maternal outcome (serious maternal complications) in patients with tight (1.6 percent) compared to less-tight (6.5 percent) control, suggesting benefit for tight control in gestational HTN (Martinez-King et al., 2025).
In retrospective and prospective cohort studies of women without chronic HTN diagnosed before pregnancy, those with new-onset BP 120–129/<80 mmHg (elevated BP) or 130–139/80–89 mmHg (stage 1 HTN) after 20 weeks’ gestation had higher risk of APOs, raising the question of whether a similar lower BP threshold for gestational HTN is warranted (Porcelli et al., 2020; Woolcock et al., 2024). Randomized trials are needed to determine optimal treatment thresholds for gestational HTN for reducing adverse maternal outcomes.
Small for Gestational Age and Blood Pressure Threshold Lower Than 140/90
Across available studies, treatment of HTN during pregnancy to a target of <140/90 mmHg has not been associated with an increased risk of SGA birth. In contrast, uncontrolled high BP (≥140/90 mmHg) has consistently been associated with an elevated risk of SGA, with some studies demonstrating at least twofold increased risk (Ishikuro et al., 2024). Even mildly elevated BP (SBP of 120–139 mmHg or DBP 80–89 mmHg) has been associated with a 59 percent increase in the risk of an SGA birth (Cao et al., 2020).
Observational data suggest a J-shaped relationship between BP and SGA, with potential risk at both very high and very low BP levels. However, BP levels below 140/90 mmHg have not been associated with increased SGA risk (Mitchell et al., 2019). Although maternal low BP (SBP <100 mmHg or DBP <60 mmHg) was associated with SGA among nulliparous women without a history of HTN (de Los Reyes et al., 2021), these thresholds are well below recommended treatment targets and were uncommon in treatment studies. Lower BP thresholds were not studied. Taken together, the available evidence does not indicate that treatment to a <140/90 mmHg target increases the risk of fetal growth restriction.
In a secondary analysis of the CHAP trial, low BP at 28–34 weeks’ gestation (defined as mean SBP <110 mmHg and mean DBP <70 mmHg or mean arterial pressure <80 mmHg) occurred in fewer than 3 percent of participants and was not associated with delivery of an SGA neonate (less than the 5th or 10th percentiles) (Boggess et al., 2022). Lower BP thresholds were not studied. Taken together, the available evidence does not indicate that treatment to a <140/90 mmHg target increases the risk of fetal growth restriction.
Implementation Considerations
Home Blood Pressure Monitoring
HTN management has primarily relied on thresholds from in-office BP measurement. However, in-office BPs of 140/90 and 160/100 mmHg correspond to home monitoring values of 135/85 and 145/90 mmHg, respectively (Jones et al., 2025). Provisional criteria for the diagnosis of HTN in pregnancy have been in-office BPs. The CHAP trial analysis did not incorporate home BP measurements. While the prevalence of white-coat HTN, defined as elevated BP measurements in clinical settings compared with normal BP outside of that environment, is unknown in pregnancy, home BP monitoring may be beneficial. However, not all home BP devices have
been validated for use in pregnancy; thus, it may be useful to ask patients to bring in their monitors to compare with in-office measurements (with a mean difference of ≤5 mmHg between the two) (ACOG, 2019; StrideBP, 2025).
Use of Oral Antihypertensives
Recommended oral antihypertensives in pregnancy include labetalol and extended-release nifedipine; methyldopa and hydrochlorothiazide are less common. In the CHAP trial, the first-line antihypertensive medications were labetalol or extended-release nifedipine, which the trial investigators supplied, and others, such as amlodipine, methyldopa, or hydrochlorothiazide, were based on patient preference. Emerging data suggest that tailoring antihypertensive therapy to each individual’s hemodynamic profile (based on cardiac output and systemic vascular resistance) may reduce severe-range HTN and preeclampsia (di Pasquo et al., 2024; Mulder et al., 2021).
Summary and Committee Conclusions
The committee concludes that BP management to a target of <140/90 mmHg during pregnancy reduces adverse maternal outcomes in women with chronic HTN, supported by consistent findings from randomized trials, meta-analyses, and high-quality observational studies (see Table 4-3). Treatment reduces the occurrence of severe-range HTN, preeclampsia with severe features, and medically indicated preterm birth without increasing the risk of fetal growth restriction. Evidence for using a target of <140/90 mmHg in women with gestational HTN is less robust largely because fewer trials have enrolled these women and subgroup analyses have had limited power to detect differences in key maternal and perinatal outcomes, although available findings suggest potential benefits. Evidence regarding lower targets, such as <130/80 mmHg during pregnancy for either chronic HTN or gestational HTN, remains limited and insufficient to support clinical recommendations. Overall, the committee finds substantial evidence of effectiveness for antihypertensive therapy to achieve a BP of <140/90 mmHg in pregnancy for chronic HTN.
Conclusion 4-1: Evidence is substantial that for women with chronic hypertension that precedes pregnancy, antihypertensive therapy targeting a blood pressure of <140/90 mmHg during pregnancy reduces severe-range hypertension, preeclampsia, indicated preterm birth, and other adverse outcomes, with no evidence of harm to fetal growth. Evidence supporting use of a <140/90 mmHg treatment target for gestational hypertension is moderate.
Research Considerations
Robust randomized trials and comparative effectiveness studies are needed to determine optimal BP thresholds for gestational HTN and evaluate whether lower treatment targets, such as <130/80 mmHg for either chronic HTN or gestational HTN, could confer additional benefit without harm. Future research is needed to assess outcomes among high-risk subgroups, including women with diabetes, severe obesity, or early-pregnancy elevated BP; incorporate validated home BP monitoring strategies; and evaluate long-term maternal cardiovascular outcomes and cost-effectiveness. Because pregnancy-onset or exacerbated HDPs (e.g., de novo gestational HTN or preeclampsia, or worsening chronic HTN/superimposed preeclampsia) can serve as sentinel markers of future cardiovascular risk, studies also need to evaluate long-term maternal cardiovascular outcomes and cost-effectiveness. While not considered to be within the scope of this evidence review, defining optimal BP treatment thresholds for preeclampsia without severe features may be a future research priority.
ENHANCED POSTPARTUM HYPERTENSION MANAGEMENT
Overview of the Question and Gap
HDPs—including chronic HTN; gestational HTN; preeclampsia; chronic HTN with superimposed preeclampsia; and hemolysis, and elevated liver enzymes—are well recognized early-life indicators of future CVD. Women with a history of HDPs have a several-fold higher risk of developing chronic HTN, particularly in the years following pregnancy, and remain at elevated long-term risk for ischemic heart disease, stroke, heart failure, and premature mortality (Behrens et al., 2017; Brown et al., 2013; Levine et al., 2022; Parikh et al., 2021; Wang et al., 2021). For women diagnosed with HDP, the postpartum period represents a critical window for intervention, risk identification, and early secondary prevention of HDP in future pregnancies and mitigating long-term CVD risk.
BP typically peaks 3–7 days postpartum, driven by physiologic changes in intravascular volume and vascular tone changes (Countouris et al., 2025). Even women who were normotensive during pregnancy may experience significant BP elevations during this postpartum period. De novo postpartum gestational HTN occurs in approximately 9 percent of pregnancies and is associated with advanced maternal age, obesity, gestational diabetes, and active smoking (Emeruwa et al., 2025; Parker et al., 2023). SBP peaks around postpartum days 3–5, while DBP peaks around days 5–7 (Countouris et al., 2025). These phenomena coincide with a time of heightened risk for hypertensive crises, eclampsia, severe maternal morbidity,
TABLE 4-3 Summary of Evidence on Prenatal Blood Pressure Targetsa
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Ankumah et al., 2014 Obstetrics and Gynecology | Secondary analysis of RCT cohort (MFMU High-Risk Aspirin Trial); multicenter U.S. network | N = 759 pregnant women with cHTN
Reproductive period: PN (midtrimester pre-enrollment BP at ~13–26 weeks), PP | No intervention—observational comparison across baseline BP categories | Evaluate if BP <140/90 mmHg is associated with lower risk of APOs in women with mild cHTN Secondary: SGA <10%, PE, any PTB | Compared with BP <140/90 mmHg, elevated BPs 140–150/90–99 mmHg and 151–159/100–109 mmHg at pre-enrollment associated with a 2.0- and 3.2-fold increase in the primary composite perinatal outcome | Fair |
| Magee et al., 2016 Hypertension | Post-hoc secondary analysis of CHIPS RCT (international, multicenter) | N = 987 pregnant women with nonsevere preexisting or gHTN, 14–33+6 weeks’ gestation, nonproteinuric |
RCT allocation to
| Severe HTN, PE, SGA <10% | Severe HTN associated with higher rates of each of the CHIPS primary perinatal outcomes; less-tight BP control associated with possible serious maternal complications, maternal readmission within 6 weeks’ PP | Good |
| Reproductive period: PN (midpregnancy onward) | Analysis explores outcomes by development of severe HTN, adjusted for treatment group | |||||
| Nzelu et al., 2018 American Journal of Obstetrics & Gynecology | Prospective cohort King’s College Hospital Antenatal Hypertension Clinic, London, U.K. | N = 586 pregnant women with prepregnancy cHTN
Reproductive period: PN (first trimester through delivery) | Not an intervention study—comparison across three early-pregnancy BP-control strata Clinic policy: maintain BP 130–140/80–90 mmHg during pregnancy; stop meds if BP <130/80 mmHg; escalate if BP rises | Incidence of severe HTN, total PE, preterm PE, birth status | Increase from Group 1 to Group 3 in incidence of severe HTN (10.6%, 22.2%, and 52.1%), preterm PE with onset at <37 weeks’ gestation (7.0%, 15.9%, and 20.4%), and SGA (13.1%, 17.7%, and 21.1%) but not term PE with onset at >37 weeks’ gestation (9.5%, 9.1%, and 6.6%) | Good |
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Hauspurg et al., 2019b American Journal of Obstetrics & Gynecology | Prospective cohort nuMoM2b, 8 U.S. academic centers; nullipara | N = 8,899 nulliparous women (no cHTN, no diabetes) BP categories (first trimester, ~11.6 weeks):
BP trajectory between Visit 1 (11.6 weeks) and Visit 2 (~19 weeks): downward, stable, upward | Observational comparison by BP category Normal BP vs. Elevated BP vs. Stage 1 HTN | Any HDP, gHTN, PE (± severe features), indicated PTB, birth weight/SGA surrogate | Substantially increased risk of HDP, severe PE, indicated PTB, and lower birth weight with Stage 1 HTN and elevated BP in early pregnancy; independently increased HDP risk with an upward BP trajectory even when baseline BP is “normal,” highlighting early-pregnancy BP behavior as a key cardiovascular-relevant risk signal | Good |
| Reproductive period: PN (early pregnancy → delivery) | ||||||
| Mitchell et al., 2019 American Journal of Perinatology | Retrospective cohort (2000–2014), single tertiary center, Alabama, U.S. | N = 600 singleton pregnancies, with cHTN, documented <20 weeks, mean BP <140/90 mmHg during pregnancy
Reproductive period: PN (full pregnancy) | No intervention—observational comparison of outcomes by BP level within the “normal” (<140/90) range Institutional management: goal BP <150/90 mmHg, serial growth scans, weekly testing ≥32–34 weeks | Incidence/odds of PE, SGA, PTB <35 weeks | BP <120/80 mmHg not associated with adverse neonatal outcomes, including SGA, and higher BP even within the normal range associated with increased rates of PE and adverse neonatal outcomes | Good |
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Porcelli et al., 2020 American Journal of Obstetrics & Gynecology | Retrospective cohort Barnes-Jewish Hospital, Washington University (MO, U.S.), 2014–2016 | N = 2,090 pregnant patients who had previously normotensive singleton pregnancies, >1 PN care visit before 20 weeks’ gestation, BP information available in the interval between 20 weeks’ gestation and delivery, and delivery at >23 weeks’ gestation Reproductive period: PN, PP (20 weeks → delivery/PP) | Observational comparison of normotensive women who developed vs. did not develop Stage 1–range BP elevations after 20 weeks | Any HDP, severe-feature PE, PTB, SGA (<10%), maternal morbidity, neonatal morbidity, PP HDP readmission |
| Fair |
| Reddy et al., 2020 American Journal of Obstetrics & Gynecology | Retrospective cohort Monash Health, Melbourne, Australia (2016–2018) | N = 18,243 singleton pregnancies Reproductive period: PN (first trimester → delivery) |
Observational comparison across BP categories and MAP levels at multiple gestational ages Control: Normal (SBP <120 mmHg and DBP <80 mmHg) Comparators: BP categorized using ACC/AHA thresholds:
| PE (overall, early-onset), PTB (overall/spontaneous/indicated), SGA (<10th percentile), composite perinatal morbidity (stillbirth/neonatal death, NICU ≥48 hours, birth weight <3rd percentile) |
| Good |
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Dumitrascu-Biris, 2021 Acta Obstetricia et Gynecologica Scandinavica | Prospective cohort study University hospital, U.K. | Singleton pregnancies with either prepregnancy or newly diagnosed cHTN before 20 weeks’ gestation Reproductive period: PN | Group 1: N = 100 women without history of chronic HTN, presenting in the first trimester with BP >140/90 mmHg Groups 2–4 with prepregnancy cHTN: Group 2, BP <140/90 mmHg without antihypertensives (N = 234); Group 3, BP <140/90 mmHg with antihypertensives (N = 272); Group 4, BP ≥140/90 mmHg despite antihypertensives (N = 192) | FGR; admission to the NNU or NICU for ≥2 days; composite neonatal morbidity; composite serious adverse neonatal outcome | In CH, adverse perinatal outcomes worse in women known to have cHTN and need antihypertensives in the first trimester Women with newly diagnosed cHTN in the first trimester with similar outcomes to those with known cHTN who have antihypertensive treatment discontinued | Fair |
| Sabol et al., 2021 AJOG Maternal-Fetal Medicine | Retrospective cohort Single tertiary center, Washington University/Barnes-Jewish Hospital (MO, U.S.); 2014–2016 | N = 3,000 singleton pregnancies
Reproductive period: PN (early pregnancy → delivery/PP discharge) | Observational comparison across BP groups for time to event and adverse outcomes | Any HDP, PE (± severe features), gHTN, PTB (<37, <34 weeks), SGA <10%, composite maternal morbidity, composite neonatal morbidity | Pregnancies in women with Stage 1 HTN significantly less likely to have composite maternal morbidity and composite neonatal morbidity or require admission to a high-level nursery compared with women with Stage 2 HTN and no significant increased risk of these outcomes compared with normotensive women | Good |
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Tita et al., 2022 New England Journal of Medicine | Large, pragmatic multicenter RCT across 61 U.S. sites; open-label; 2015–2021 | N = 2,408 women with viable singleton pregnancies <23 weeks’ gestation (without PE or gHTN) with either a new or known diagnosis of cHTN during pregnancy
Reproductive period: PN (randomization <23 weeks → delivery → 6 weeks PP) | Intervention: antihypertensives titrated to BP <140/90 mmHg (labetalol or nifedipine as first line) Control: Women with no treatment unless severe HTN developed (SBP ≥160 mmHg or DBP ≥105 mmHg) Comparator: Women who received antihypertensives recommended for use in pregnancy with a BP goal of <140/90 mmHg | Primary composite: severe-feature PE, medically indicated PTB <35 weeks, abruption, fetal/neonatal death Safety: SGA <10th percentile Secondary: overall PE, PTB <37 weeks, severe HTN, maternal/neonatal complications |
Treating to <140/90 mmHg significantly reducing major APOs Primary composite: 30.2% (active) vs. 37.0% (control) → RR 0.82 Key components:
No increased risk of FGR:
Mean PN BP difference ~3/2 mmHg (SBP/DBP); despite small absolute BP difference, substantial risk reductions | Good |
| Reduced severe HTN: 36.1% vs. 44.3% → RR 0.82 Any PE: 24.4% vs. 31.1% → RR 0.79 | ||||||
| Attar et al., 2023 Clinical Cardiology | Systematic review + meta-analysis of 12 RCTs (mixed settings internationally) | N = 4,461 pregnant women with mild cHTN or gHTN (2,395 treated; 2,066 controls) Trials spanning cHTN, gHTN, and mixed populations Reproductive period: PN (treatment during pregnancy → delivery) | Active treatment (labetalol, nifedipine, methyldopa, hydralazine; varying protocols) vs. no treatment/placebo unless severe HTN Varied treatment goals (commonly <140/90 mmHg or DBP <85–90 mmHg) | Severe HTN, PE, placental abruption, renal impairment, pulmonary edema, ECG changes; fetal/neonatal outcomes including SGA, LBW, NICU, neonatal mortality |
Pooled RRs with significant reductions:
No increase in FGR: SGA (<10th%): RR 1.12 | Fair |
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Avalos et al., 2023 Pharmacotherapy | Retrospective cohort with dynamic marginal structural models Three Kaiser Permanente regions (Northern CA, Southern CA, Washington, U.S.); 2005–2014 | N = 11,871 pregnant women with evidence of PN HTN who gave birth (live or still) to a singleton 2005–2014 with gestational age at start of follow-up of at least 20 weeks Reproductive period: PN (from 20 weeks → delivery) | Risks and benefits of treatment of mild-to-moderate-HTN during pregnancy Comparison: 5 antihypertensive initiation protocols: BP ≥140/90 mmHg BP ≥145/95 mmHg BP ≥150/100 mmHg BP ≥155/105 mmHg BP ≥160/110 mmHg | PE, PTB (<37 weeks), SGA (<10th%) | Initiating antihypertensives at mild-to-moderate BP thresholds possibly associated with higher risk of adverse maternal, fetal and neonatal outcomes, specifically PE, PTB, SGA, NICU admission, and stillbirth; risks with a graded pattern (highest for 140/90 mmHg → lowest at 155/105 mmHg); may reflect unmeasured confounding (sicker patients treated earlier) | Poor |
| Bailey et al., 2023 Obstetrics & Gynecology | Secondary analysis of CHAP RCT; 61 U.S. sites; open-label RCT dataset | N = 2,096 pregnant patients before 23 weeks’ gestation with previously or newly diagnosed HTN Reproductive period: PN, PP | Not a treatment-randomization study—compared achieved mean BP levels: <130/80 mmHg vs. 130–139/80–89 mmHg Both arms with women randomized to active treatment or usual care in CHAP | Primary composite: severe-feature PE, indicated PTB <35 weeks, abruption, fetal/neonatal death Secondary: SGA <10%, SGA <5%, any PE, severe HTN, NICU admission, PTB <37 weeks, LBW, respiratory morbidity | Among women with mild cHTN in CHAP, maintaining mean BP <130/80 mmHg (vs. 130–139/80–89 mmHg) associated with a ~55% reduction in major adverse outcomes, including severe PE and indicated PTB, with no increase in SGA; lower BP also associated with improved neonatal outcomes (NICU, LBW, respiratory morbidity); findings supporting that BP targets <130/80 mmHg may offer additional benefit beyond the CHAP treatment threshold of 140/90 mmHg | Fair |
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Gyselaers et al. (2023) Hypertension | Prospective observational cohort (hemodynamic phenotyping) Two clinics at a university hospital, Belgium; 2011–2017 | N = 1,109 first-trimester measurements from normotensive pregnant women with singleton pregnancies
Reproductive period: PN | No intervention; hemodynamic profiles within the same BP threshold compared to predict outcomes Group 1: CO and TPR ≤P75 Group 2: CO >P75 and TPR ≤P75 Group 3: CO ≤P75 and TPR >P75 | CO, TPR, GHD, SGA, LPE |
Physiological spectrum of CO and TPR levels ranging from high to low possible in first trimester normotensive pregnant women; imbalance possibly associated with increased risk of GHD and SGA, irrespective of HTN threshold
| Poor |
| Sisti et al. (2023) European Journal of Obstetrics & Gynecology and Reproductive Biology | Systematic review + meta-analysis; 24 studies; International sample; up to May 2022 | N = 570,150 total pregnancies across studies, including patients ranging from pre-HTN to Stage 1 HTN Reproductive period: PN (pre-20 weeks BP screening → delivery) | Not an intervention study Comparison = BP 120–139/80–89 mmHg vs. BP <120/80 mmHg before 20 weeks | Risk of HDP, PE/eclampsia, gHTN |
| Good |
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Slade et al., 2023a American Journal of Obstetrics & Gynecology | Systematic review + meta-analysis of 23 studies, 734,377 pregnancies (1/3 of studies low-/middle-income countries, half U.S.) | Pregnant women with BP categorized per ACC/AHA at <20 weeks Excluded cHTN in ~50% of studies; most samples low-risk, singleton pregnancies Reproductive period: PN (pre-20 weeks) |
Comparison of outcomes across BP categories:
| PE, serious maternal complications, PTB, perinatal death, stillbirth, NICU admission, SGA | Across 23 studies (>734,000 pregnancies), early-pregnancy BP 120–139/80–89 mmHg associated with higher risk of PE and adverse outcomes, with a clear dose–response pattern; however, only BP ≥140/90 mmHg with clinically meaningful diagnostic value; no improved prediction or safely ruling out risk for lower ACC/AHA thresholds (<130/80 or 120/80 mmHg) | Good |
| Slade et al., 2023b American Journal of Obstetrics & Gynecology | Systematic review + meta-analysis) Systematic review of 12 studies + meta-analysis of 251,172 pregnancies; includes both prospective and retrospective cohorts and secondary RCT analyses across multiple high-, middle-, and low-income countries | Pregnant women with BP measured at ≥20 weeks, categorized per 2017 ACC/AHA thresholds Reproductive period: PN | Comparison of risks across BP categories at any time ≥20 weeks or within gestational strata (20–27, 28–32, 33–36 weeks) Diagnostic test meta-analysis: sensitivity, specificity, likelihood ratios for BP thresholds | PE, serious maternal complications, maternal death, eclampsia, stroke, ICU admission, stillbirth/perinatal death, SGA |
| Good |
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Woolcock et al., 2024 American Journal of Perinatology | Secondary analysis of prospective cohort (8 U.S. academic medical centers) | N = 4,460 of 10,038 in the original nuMoM2b cohort (normotensive nulliparas)
Reproductive period: PN (22–29 weeks → delivery) | Not an intervention; compared BP category at four visits throughout pregnancy (6 weeks to time of birth) (normal vs. elevated vs. Stage 1) Normal BP vs. elevated BP, Stage 1 HTN | HDP, PE, FGR, placental abruption, cesarean delivery, PTB (<37 weeks) | In normotensive nulliparas, developing elevated BP (120–129/<80 mmHg) or Stage 1 HTN (130–139/80–89 mmHg) after 22–29 weeks strongly associated with adverse outcomes; nearly doubled HDP risk and tripled abruption risk with elevated BP; nearly tripled HDP risk and doubled FGR risk with Stage 1 | Good |
| Abe et al., 2025 Hypertension Research | Systematic review + metaanalysis of 40 RCTs. U.S. and international | N = 8,039 pregnant women with nonsevere cHT, gHT, or mixed-type HTN BP ranges:
Excludes severe HTN (≥160/110 mmHg) Reproductive period: PN (treatment during pregnancy → delivery) | Antihypertensive therapy (labetalol, methyldopa, nifedipine, isradipine, pindolol, prazosin, hydralazine, etc.) vs. placebo or no treatment (including expectant management/bed rest) Evaluates treatment effects and whether different targets/achieved levels modify outcomes | Severe HTN, PE, severe-feature PE, HELLP, placental abruption, cesarean section, neonatal death, stillbirth, NICU admission, LBW, PTB (<37 and <34 weeks), SGA (<10th percentile) | Across 40 RCTs (>8,000 patients), significantly reduced severe HTN, PE, and PTB with treatment for nonsevere HTN, with no increase in SGA; subgroup analyses showing no added benefit from achieving lower BP (<130/80 mmHg) compared with <140/90 mmHg, supporting <140/90 mmHg as the optimal target; effects consistent across cHTN, gHTN, and PE phenotypes except for placental abruption, where benefit is limited to cHTN | Fair |
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Harper et al., 2025 American Journal of Obstetrics & Gynecology | Secondary analysis of a multicenter (61 U.S. sites) RCT | N = 434 CHAP study participants with cHTN + diabetes, average PN BP <140/90 mmHg; BP groups: <130/80 mmHg (N = 150) vs. 130–139/80–89 mmHg (N = 284) Reproductive PN (postrandomization <23 weeks → delivery; outcomes included PE through 2 weeks PP | Not a new randomized treatment; comparison by achieved BP level within CHAP study: Lower BP group: average SBP <130 mmHg & DBP <80 mmHg Higher BP group: average SBP 130–139 mmHg and/or DBP 80–89 mmHg | PE with severe features (up to 2 weeks PP); indicated PTB <35 weeks, SGA | Among CHAP participants with cHTN + diabetes and average BP <140/90 mmHg, achieving mean BP <130/80 mmHg (vs. 130–139/80–89 mmHg) associated with substantially lower risk of severe-feature PE, indicated PTB <35 weeks, and NICU admission, and lower SGA <10%, with no increase in perinatal death or cesarean; findings suggesting that, once treatment is initiated (per CHAP), titrating to <130/80 mmHg may confer additional benefit in this high-risk subgroup without growth harm | Good |
| Slade et al., 2025a International Journal of Obesity | Secondary analysis of UPBEAT RCT (diet/lifestyle intervention); U.K. multicenter trial | N = 1,520 pregnant women with obesity (BMI ≥30 kg/m2); BP data available from ≥1 antenatal visit BP groups (highest antenatal BP per ACC/AHA):
| Not an intervention study Compared BP categories and diagnostic thresholds (≥120/80 mmHg, ≥130/80 mmHg, etc.) for predicting adverse outcomes | PTB (<37 weeks), PP hemorrhage (≥1,000 mL), SGA (<10th%), NICU admission | ACC/AHA BP categories <140/90 mmHg (Elevated and Stage 1 HTN) not predictive of PTB, SGA, PPH, or NICU admission; some association only for severe Stage 2 HTN, mostly unadjusted; diagnostic accuracy analyses indicating that no BP threshold <140/90 mmHg improved identification of maternal or neonatal risk | Good |
NOTES: a Studies are listed by publication year (oldest first), then alphabetically by first author within each year. b Quality rating was assessed using the National Heart, Lung, and Blood Institute Quality Assessment Tools. Ratings: Good = low risk of bias; Fair = some concerns; Poor = serious risk of bias. ACC = American College of Cardiology; AHA = American Heart Association; APO = adverse pregnancy outcome; BMI = body mass
index; BP = blood pressure; CHAP = Chronic Hypertension and Pregnancy; CHIPS = Control of Hypertension in Pregnancy Study; cHTN = chronic hypertension; CO = cardiac output; DBP = diastolic blood pressure; ECG = electrocardiogram; FGR = fetal growth restriction; GHD = gestational hypertensive disorder; gHTN = gestational hypertension; HDP = hypertensive disorder of pregnancy; HELLP = hemolysis, elevated liver enzymes, and low platelets; HTN = hypertension; LBW = low birth weight; LPE = late-onset preeclampsia; MAP = mean arterial pressure; mDBP = mean diastolic blood pressure; MFMU = Maternal-Fetal Medicine Network; mmHg = millimeters of mercury; mSBP = mean systolic blood pressure; NICU = neonatal intensive care unit; NNT = number needed to treat; NNU = neonatal unit; NS = not significant; nuMoM2b = Nulliparous Pregnancy Outcomes Study: Monitoring Mothers-to-Be; PE = preeclampsia; PN = prenatal; PP = postpartum; PTB = preterm birth; RCT = randomized controlled trial; RR = relative risk; SBP = systolic blood pressure; SGA = small for gestational age; TPR = total peripheral resistance.
SOURCES: Abe et al., 2025; Ankumah et al., 2014; Attar et al., 2023; Avalos et al., 2023; Bailey et al., 2023; Dumitrascu-Biris et al., 2021; Gyselaers et al., 2023; Harper et al., 2025; Hauspurg et al., 2019b; Magee et al., 2016; Mitchell et al., 2019; Nzelu et al., 2018; Porcelli et al., 2020; Reddy et al., 2020; Sabol et al., 2021; Sisti et al., 2023; Slade et al., 2025a; Slade et al., 2023a,b; Tita et al., 2022; Woolcock et al., 2024.
and readmission. Timely recognition and early, effective treatment during this window may avert severe hypertensive events and complications, reduce emergency department (ED) use and readmissions, and also support improved postpartum quality of life.
Increasingly, professional guidance emphasizes early and structured postpartum BP evaluation, mostly focused on women with HDPs. Recommendations from ACOG (2018) emphasize BP assessment within 72 hours postpartum for women with severe HDPs and 7–10 days postpartum for all women with HDPs (ACOG, 2018). The 2025 AHA/ACC Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults—for the first time—includes tailored BP management guidance for pregnant and postpartum women (Jones et al., 2025). These guidelines define standard care practices, such as recommended time frames for BP assessment, therapeutic thresholds (e.g., initiation of antihypertensive therapy postpartum for persistent BP ≥150/100 mmHg; urgent treatment for BP ≥160/110 mmHg), and lactation-compatible medication options. These guidelines provide important context for interpreting the evidence but should be understood as external expert recommendations rather than conclusions derived from the empirical studies reviewed by the committee.
The 2025 AHA/ACC guideline explicitly recognizes HDP as sentinel markers of elevated long-term cardiovascular risk, thereby aligning postpartum HTN management with broader cardiovascular prevention strategies. Clinical guidelines converge on the principle of early detection and timely intervention in the postpartum period, although treatment thresholds vary slightly between different guidelines.
These professional standards define the basis of standard postpartum HTN care, against which newer enhanced management models can be evaluated (see Box 4-1). These models include remote self-monitored (self-measured) BP and structured follow-up programs. The need for and potential importance of these enhanced models is amplified by the reality that a third or more of women—disproportionately those from racially and socioeconomically underserved communities—do not attend an in-person postpartum visit (ACOG, 2018; Attanasio et al., 2022). This limits opportunities for early BP detection, impedes management of chronic health conditions, and contributes to both short-term risks, such as severe HTN and stroke, and long-term disparities in CVD prevention. Enhanced care models could overcome these gaps and extend high-quality care to populations least likely to access traditional postpartum services.
This review addresses the question “Does enhanced postpartum HTN management for patients with HDP (including chronic HTN) improve outcomes?”
BOX 4-1
Interventions: Standard Versus Enhanced Care for Patients with Hypertensive Disorders of Pregnancy
Standard care includes postpartum blood pressure (BP) checks within guideline windows, clinical assessment, and first-line antihypertensives.
Enhanced care includes multicomponent interventions, such as
- Self-measured BP with active clinical review,
- Telehealth or text-based monitoring,
- Standardized treatment pathways,
- Transitional care models,
- Multidisciplinary postpartum hypertension clinics, and
- Integration with cardiometabolic risk reduction services.
Summary of the Evidence
The initial literature search identified 1,923 records with publication dates from January 2010 to July 2025. Of the 1,922 unique articles screened at the abstract level, 91 were identified as potentially relevant and moved to full-text review, and 43 met inclusion criteria. The most common reasons for exclusion were (1) wrong population (e.g., antenatal only), (2) wrong intervention, or (3) lack of relevant postpartum HTN outcomes. Eligible studies were limited to those conducted in the United States or other very high–income UN countries to ensure alignment with health system structures, practice patterns, and postpartum care delivery models.
Following full-text review, 35 empirical studies underwent quality assessment and data extraction. The committee retained an additional 8 narrative reviews, commentaries, and expert opinion pieces for contextual background. These were not included in the evidence synthesis, but the committee scanned the reference lists to ensure it did not omit any eligible intervention studies.
Across the empirical studies, 7 were good, 23 were fair, and 5 were poor. Several good- and fair-quality investigations—ranging from randomized trials to pragmatic implementation studies—reinforced the overall patterns observed throughout the evidence base. Randomized trials published 2020–2023, including evaluations of self-measured BP with remote monitoring and structured management and follow-up, demonstrated the strongest internal validity (Aderibigbe et al., 2023; Kalafat et al., 2020; Kitt et al., 2021; Triebwasser et al., 2020). These trials observed consistent
improvements in BP ascertainment, BP control, and earlier detection of severe HTN. Complementary implementation-focused and observational studies conducted 2023–2025 also supported the feasibility, acceptability, and clinical utility of self-measured BP-based monitoring, telemedicine-supported follow-up, and standardized postpartum HTN pathways across diverse care settings (Aderibigbe et al., 2023; Kusumaningrum et al., 2025; Macphail et al., 2024; Mai et al., 2025; Rosenfeld et al., 2025). Collectively, these studies—evaluating structured self-measured BP protocols, text-based or app-based monitoring models, and integrated clinical management pathways—strengthened the evidence base despite persistent sources of potential bias, including incomplete follow-up, lack of blinding inherent to BP monitoring interventions, and nonrandomized study designs.
Most outcome measures in these studies were process outcomes (e.g., BP ascertainment, timeliness of treatment) or short-term BP control, which the committee considers intermediate outcomes rather than endpoints that directly reflect improved cardiovascular health. Few studies were powered to detect rare but clinically important outcomes, such as severe maternal morbidity (SMM), stroke, or readmission.
Interventions: Defining Standard Versus Enhanced Care
Standard care for patients with HDPs (including chronic HTN), as described in professional society clinical guidelines, centers on timely postpartum BP evaluation, assessment for symptoms of severe HTN or preeclampsia, and initiation of antihypertensive therapy postpartum for persistent BP ≥150/100 mmHg. The interventions evaluated across the evidence base can be conceptualized on a continuum from standard to enhanced care.
Enhanced care encompasses structured, multicomponent interventions designed to improve detection, treatment, and long-term cardiovascular prevention. These include remote or mobile app–based BP monitoring with active triage and medication titration, standardized clinical management pathways, extended inpatient or transitional monitoring, and comprehensive postpartum HTN programs combining self-measured BP with cardiovascular risk reduction, nutrition counseling, and transition to primary care or cardiology (Arkerson et al., 2023; Bronner et al., 2023; Cairns et al., 2018; Hauspurg et al., 2019b; Hirshberg et al., 2018; Lemon et al., 2024; Nguyen et al., 2022).
Evaluation of Study Quality
The quality of the reviewed studies ranged from good to poor but was most commonly fair, based on the structured assessment of risk of bias, with the following patterns (see Table 4-4 for more details on each study):2
- RCTs showed the highest rigor, with consistent intervention descriptions, validated BP outcomes, and balanced groups, but lacked blinding and sometimes provided incomplete methodologic details. Among eight RCTs reviewed, three were rated good, four fair, and one poor for the outcomes of interest.
- Pre- versus postintervention studies contributed valuable real-world evidence but were susceptible to selection biases, confounding, secular trends, and treatment fidelity variability. Of the three such studies reviewed, all were rated as fair.
- Observational studies broadened understanding of disparities, follow-up patterns, and postpartum trajectories but frequently lacked adequate adjustment for confounding and had incomplete followup reporting. Among 18 studies reviewed, 1 was rated as good, 14 fair, and 3 poor.
- Systematic reviews were generally strong but sometimes included studies of variable quality and heterogenous study designs, limiting certainty in their conclusions. Among five studies reviewed, three were considered good and two fair.
Strength of Evidence
Using standard criteria (consistency, directness, precision, and overall risk of bias), the strength of evidence supporting enhanced postpartum HTN management—particularly self-measured BP programs with structured clinical response—was judged moderate for process measures and BP control and limited for cardiovascular health outcomes. The findings of improvement in process outcomes were directionally consistent across diverse populations and settings, particularly for process outcomes (e.g., attendance at postpartum follow-up visits, early postpartum BP ascertainment, and
___________________
2One study—Hauspurg et al. (2023), which evaluated a combined postpartum home BP monitoring and lifestyle intervention for women with prior HDP—received discrepant risk-of-bias ratings during adjudication. While it was well executed as a feasibility trial, the evidence review identified two limitations relevant to assessing effectiveness: (1) high differential dropout and (2) insufficient power for clinical outcomes. Therefore, it was judged poor quality for determining effectiveness but good quality for feasibility. Its inclusion in the evidence review reflects that feasibility findings are informative for implementation considerations, while appropriately limiting its influence on the overall effectiveness conclusions.
treatment timeliness). Precision was moderate, and risk of bias, while not negligible, did not overturn the consistency of these findings.
Improvements in intermediate and longer-term clinical outcomes had somewhat varied strength of evidence. Across the reviewed studies, most interventions demonstrated consistent improvements in process outcomes (e.g., BP ascertainment, timeliness of treatment, short-term BP control), whereas findings for clinical endpoints, such as readmissions and severe maternal morbidity, were mixed or underpowered. For example, the strength of evidence for self-measured BP programs with structured clinical response improving postpartum BP was judged moderate on the basis of consistent findings from several observational studies and RCTs. These positive effects were limited to interventions that paired self-measured BP with active management, whereas evidence of effectiveness was limited in studies of self-measured BP alone or with coaching or lifestyle modification (Borrowman et al., 2025; Cairns et al., 2018; Kitt et al., 2021, 2023; Rosenfeld et al., 2025). Strength of evidence for other clinical outcomes was generally weaker. For example, several fair-quality observational studies and one good-quality RCT suggested such programs reduce postpartum readmissions, whereas other observational studies and RCTs found no clear evidence of reduction (Arkerson et al., 2023; Cairns et al., 2018; Hirshberg et al., 2018; Kalafat et al., 2020; Kitt et al., 2023; Rosenfeld et al., 2025; Suresh et al., 2021; Zullo et al., 2025). Evidence for these outcomes was generally weaker because many studies of enhanced postpartum interventions were underpowered to detect potentially important effect sizes.
Collectively, the evidence supports cautious conclusions: enhanced postpartum HTN programs reliably improve process outcomes and short-term (<1 year) BP control, but evidence for clinical outcomes remains limited.
Service Specification: Timing, Frequency, and Care Processes
A comprehensive postpartum HTN management program begins before discharge, continues through the first year postpartum, and includes consistent, structured processes.
Before Discharge
ACOG guidance recommends that all women receive counseling on postpartum BP expected trajectory, warning signs of HTN and preeclampsia, and a written follow-up plan before hospital discharge. Programs distributing validated self-measured BP cuffs and providing training on effective use and clear return precautions—as demonstrated in trials such as the Self-Management of Postnatal Hypertension (SNAP-HT) trial and studies on telehealth feasibility—have been shown to improve patient engagement,
enhance early identification of severe BP elevations, and support more reliable early follow-up care across diverse patient groups (Cairns et al., 2018; Hoppe et al., 2019). These steps are aligned with the ACOG Optimizing Postpartum Care guidance, which emphasizes preparation for the vulnerable early postpartum period (ACOG, 2018).
Early Postpartum
RCTs and prospective studies demonstrate that early BP evaluation—particularly within 72 hours for women with severe HTN or discharged on antihypertensives—is associated with improved BP ascertainment and earlier medication adjustments (Arkerson et al., 2023; Hirshberg et al., 2023). Evidence that such evaluation reduces SMM or readmissions is suggestive but limited, as studies were underpowered for these outcomes. ACOG and the 2025 ACC/AHA HTN guidelines specify that all patients with HDP should receive BP assessment within 7–10 days postpartum (ACOG et al., 2018; Jones et al., 2025).
Self-Measured Blood Pressure Monitoring
Multiple studies have found that self-measurement of BP is feasible and reliable. Twice-daily self-measured BP during the first 14 days postpartum is the most common protocol used across studies, such as SNAP-HT, and others via a text-based system or remote monitoring programs (Hirshberg et al., 2018; Lemon et al., 2024). Reduced-frequency monitoring after BP stabilization mirrors step-down titration schedules and other systematic treatment programs that have demonstrated reductions in readmissions and improved BP control (Cairns et al., 2018; Hirshberg et al., 2018; Lemon et al., 2024; Suresh et al., 2021).
Medication Titration Pathways
Across intervention studies—including systematic treatment programs and those using a standardized order set or remote titration methods—therapy was generally initiated or escalated for persistent BPs ≥150/100 mmHg and triggered urgent evaluation at ≥160/110 mmHg during the early postpartum period (≤6 weeks) (Aderibigbe et al., 2023; Nguyen et al., 2022; Sarma et al., 2023). These severe-range thresholds align with ACOG safety guidance and are consistent with the 2025 ACC/AHA guidelines for severe HTN in pregnancy and postpartum (ACOG, 2020a; Jones et al., 2025). Beyond 6 weeks postpartum, women with persistent HTN following an HDP are typically managed according to standard adult HTN targets. Evaluations of specific BP targets unique to the postpartum period remain
limited, with only a single small RCT demonstrating no difference in clinical outcomes between targets of <140/90 and <150/95 mmHg (Aderibigbe et al., 2023).
Risk-Stratified Care
Patients with chronic HTN or high-risk clinical features—including early-onset or severe preeclampsia, renal dysfunction, intensive care unit (ICU) stay, or limited social support—benefit from tailored early follow-up. Studies show they carry the highest risk of postpartum HTN persistence and long-term CVD (Hauspurg et al., 2019a). Risk-stratified care pathways embedded within state and institutional safety initiatives—such as the Ohio Maternal Safety Project—demonstrate that matching surveillance intensity to patient risk is feasible and associated with better adherence to recommended postpartum monitoring (Schneider et al., 2023). However, formal evaluations showing improvement in maternal cardiovascular outcomes have not yet been published.
Summary
The evidence demonstrates that standardized timing of follow-up, validated self-measurement BP protocols, and structured medication titration pathways form the core of effective postpartum HTN care. Programs incorporating these elements consistently support earlier treatment adjustments and improve short-term BP control. Several studies also suggest reductions in HTN-related readmissions, although findings are mixed, and many studies were not powered for this outcome. Emerging evidence indicates that these structured pathways may help mitigate racial and socioeconomic disparities in early postpartum follow-up and BP assessment. Remote monitoring models, in particular, extend high-quality care to patients least likely to access traditional in-person services, addressing a major gap in U.S. maternal health systems.
Risk Stratification
Risk stratification is foundational to postpartum HTN management because it helps identify patients at highest risk for postpartum BP elevation, recurrence, and readmission and guides the intensity and timing of monitoring and follow-up. Many determinants of postpartum risk are present before delivery, often before pregnancy, highlighting the value of prepregnancy and interpregnancy assessment and follow-up (Chen and Chen, 2020; Hauspurg et al., 2019a; Stulberg et al., 2023).
Across the pregnancy continuum, several factors consistently portend more severe postpartum HTN and higher long-term cardiometabolic risk, including chronic HTN, preexisting diabetes, and obesity (Hauspurg et al., 2019a; Khosla et al., 2021). Excess gestational weight gain is common and has been associated with adverse postpartum HTN, cardiovascular, and long-term cardiometabolic outcomes (Deputy et al., 2015; Gregory et al., 2020; Hutchins et al., 2022). Peripartum clinical features, including severe-range BP during labor and delivery, ICU admission, cesarean delivery, and major hemorrhage, further help identify patients at higher risk of early postpartum decompensation (Bernstein et al., 2017; Tao et al., 2024). Postpartum markers—such as persistent BP ≥140/90 mmHg, renal dysfunction, need for antihypertensives at discharge, or limited social support—can signal the need for closer surveillance and proactive medication adjustment. Evidence from structured postpartum HTN programs, standardized treatment pathways, and remote monitoring interventions suggests that higher-risk patients benefit most from intensified early monitoring and proactive medication adjustment, although definitive data on clinical endpoints remain limited (Bisson et al., 2024; Forna et al., 2024; Lemon et al., 2024).
This continuum of risk for higher postpartum BP and need for more intense postpartum BP management can be operationalized using a committee-proposed tiered risk-stratification framework informed by ACOG/Society for Maternal-Fetal Medicine (SMFM) guidance on postpartum BP follow-up timing and supplemented by evidence from published postpartum HTN pathways and remote monitoring programs where formal guideline recommendations are limited (ACOG et al., 2018; Hirshberg et al., 2023; Steele et al., 2023).
- Tier 1 (highest risk): Patients with severe HDP and/or major comorbidity (e.g., chronic kidney disease, diabetes) or those discharged on antihypertensives.
- Consistent with ACOG/SMFM guidance, patients at highest risk undergo early postpartum BP assessment, often within 72 hours of delivery for high-risk patients.
- In many postpartum care models, this early assessment is paired with short-term home BP monitoring and proactive medication adjustment during the first 1–2 weeks. The monitoring frequency and duration reflect programmatic evidence rather than formal ACOG/SMFM specifications (ACOG et al., 2018; Steele et al., 2023).
- Tier 2 (moderate risk): Women with nonsevere HDP discharged without antihypertensives.
- ACOG/SMFM recommend BP evaluation within 7–10 days postpartum (or earlier if symptoms arise) (ACOG et al., 2018).
- Some care models additionally incorporate short-term home BP monitoring during the physiologic BP peak to support early identification of rising BP and timely clinical response. The suggested duration/frequency of monitoring reflects evidence from remote monitoring interventions (Arkerson et al., 2023; Hirshberg et al., 2023).
- Tier 3 (chronic HTN, controlled): Women with well-controlled chronic HTN.
- Early postpartum follow-up commonly emphasizes medication reconciliation and transition planning to primary or specialist care for longer-term BP and CVD risk management. This transition-of-care emphasis reflects emerging models and observational evidence rather than specific ACOG/SMFM tiering (Pihelgas et al., 2025; Reddy et al., 2024).
Overall, a continuum-based risk-stratification framework—beginning before pregnancy, reinforced between pregnancies, and applied through the postpartum period—may help align surveillance intensity with risk and support timely escalation of care and transition to long-term cardiovascular prevention (Hauspurg et al., 2019a; Khosla et al., 2021).
Cost and Cost-Effectiveness
Enhanced postpartum HTN management has important implications for health system efficiency and resource use. However, the committee’s review did not identify any formal cost-effectiveness analyses or economic evaluations of these models. Studies describe potential cost implications—such as reduced admissions, decreased in-person visit burden, and improved triage efficiency—but none formally estimate costs, savings, or cost utility compared with usual care.
Evidence from randomized and observational studies demonstrates that structured self-measured BP programs with timely clinician review can reduce high-cost acute care use by preventing missed severe-range BPs and enabling earlier treatment adjustment. For example, randomized trials of remote postpartum BP monitoring report lower HTN-related readmissions compared with usual care, including 0 versus 3.9 percent in one trial (Hirshberg et al., 2018) and 7 versus 27 percent in another, a meaningful reduction in preventable inpatient care (Kitt et al., 2023). Although health care savings have not yet been formally quantified, this model is relatively low cost and scalable and could reduce unnecessary in-person visits and improve adherence to guideline-recommended surveillance.
Additional postpartum HTN studies also show that remote monitoring models reduce unnecessary in-person encounters, streamline clinical
workflows, and shift evaluations from high-acuity emergency settings to outpatient management (Niu et al., 2022). They also appear to improve system efficiency by reducing provider workload related to follow-up coordination and facilitating earlier medication titration, which may avert progression to hypertensive crises.
Although several studies demonstrate reductions in HTN-related readmissions, evidence regarding ED use is more mixed. Some programs report lower ED use, while others observe an increase—often reflecting earlier identification of elevated BPs through self-measuring and clearer return-precaution guidance. Increased ED use may represent appropriate escalation of care for severe-range values detected sooner than they would have been under usual care. This pattern is consistent with the hypothesis that enhanced surveillance identifies worsening HTN earlier, thereby preventing more severe complications, even if it leads to higher short-term ED use.
Population Considerations
When programs incorporate features that reduce common barriers to postpartum care—such as providing no-cost BP cuffs, multilingual education, lactation-compatible BP medication titration, access to telemonitoring and telehealth, and community health worker support—they can improve engagement among populations that experience the greatest barriers to follow-up and may help improve outcomes and achieve comparable results across all populations for postpartum BP ascertainment and continuity of care (Corlin et al., 2023; Hauspurg et al., 2019a; Lemon et al., 2024; Staff et al., 2024). Telehealth and remote monitoring approaches appear particularly beneficial for women who face barriers to in-person follow-up, including many Black women, rural populations, and those with limited transportation or child care (Hirshberg et al., 2018; Kern-Goldberger and Hirshberg, 2021; Lemon et al., 2024).
These disparities have profound population-level implications. Women comprise more than half of the U.S. population, and uncontrolled postpartum HTN contributes to preventable morbidity, recurrent HDPs, and elevated long-term risks of heart failure, ischemic heart disease, and stroke (Lewey et al., 2024). These downstream sequelae carry substantial personal, familial, and economic consequences, including increased health care use and lost productivity during key years of caregiving, household economic contribution, and workforce participation. Enhanced postpartum HTN pathways—integrating early self-measured BP, standardized medication titration protocols, cardiometabolic risk assessment, and coordinated transition to primary care and/or cardiology—could mitigate these risks by improving early detection and facilitating timely treatment.
Evidence from numerous studies demonstrate that structured postpartum HTN programs improve BP ascertainment and short-term control, particularly among women at higher risk of loss to follow-up (Ditosto et al., 2023; Forna et al., 2024; Lemon et al., 2024; Patel et al., 2025). Across these evaluations, remote or enhanced postpartum monitoring models were associated with reductions in preventable acute care use, including fewer HTN-related ED or triage visits (Ditosto et al., 2023; Lemon et al., 2024) and unplanned HTN-related admissions (Steele et al., 2023). The effects of enhanced postpartum BP management on high-cost hospitalizations and long-term CVD prevention deserve further evaluation, particularly for populations disproportionately affected by maternal morbidity and lack of access to health care.
Implementation Considerations
Effective implementation of enhanced postpartum HTN management requires coordinated infrastructure, interdisciplinary workforce capacity, interoperable data systems, and intentional design to support patients with differing needs and barriers to care. Integrating self-measured BP data directly in electronic health records (EHRs) supports timely clinical action; reduces delays in medication titration; and facilitates clear communication between obstetrics, primary care, and cardiology teams (Forna et al., 2024; Reddy et al., 2024; Sarma et al., 2023). In practice, doing so is possible through several architectures: (1) postpartum women manually enter readings into a patient portal, text-based system, or mobile app; (2) readings are submitted to a remote monitoring platform that transmits structured values into the EHR; or (3) Bluetooth- or cellular-enabled cuffs transmit readings to a platform that interfaces with the EHR.
Effective integration typically means that home BP values populate discrete EHR fields (e.g., flow sheets) and trigger automated flags or inbox tasks for out-of-range values rather than remaining in unstructured messages. A designated clinical team—often nursing staff, pharmacists, care coordinators, or advanced practice clinicians operating under protocol with obstetric and/or cardiology oversight—reviews incoming BP data on a defined cadence, contacts patients when thresholds are exceeded, performs symptom assessment and repeat measurements as needed, adjusts antihypertensive therapy under standing orders when appropriate, and escalates severe-range BP or concerning symptoms to urgent evaluation.
Standardized treatment pathways—such as structured triage algorithms, escalation criteria, and medication titration protocols—promote consistent management across inpatient and outpatient settings. Although most studies were not powered to assess clinical outcomes, several quality-improvement and observational evaluations suggest that these pathways
can improve BP ascertainment, support earlier intervention, and may reduce preventable acute care use.
Successful implementation depends on addressing logistical and system barriers that most strongly affect women at highest risk of adverse outcomes. Programs that distribute validated BP monitors with appropriately sized cuffs, provide multilingual and health literacy–sensitive educational materials, and incorporate community health workers or care navigators have demonstrated higher engagement and more complete postpartum follow-up in implementation studies (Hirshberg et al., 2023; Kern-Goldberger and Hirshberg, 2021; Lewey et al., 2024). Communication-based supports—such as nurse- or pharmacist-led telephone outreach, text- or app-based BP reporting with clinical feedback, telehealth check-ins, and care navigator–facilitated coordination—can mitigate challenges such as transportation barriers, limited digital access, child care needs, and uncertainty about when to seek care, all of which disproportionately affect those at highest risk for adverse outcomes.
Because long-term BP management and cardiovascular risk reduction typically occur in longitudinal primary care settings, effective postpartum HTN programs need to ensure clear transition pathways from obstetric-led monitoring to ongoing primary care follow-up.
The crosscutting factors related to implementation described in Chapter 6 and recommendations in Chapter 7 on integrated data systems, standardized pathways, access-focused supports, and interdisciplinary workforce capacity are also relevant for translating evidence-based postpartum HTN interventions into sustained, and scalable models of care, especially for underserved populations.
Summary and Conclusions
The committee concludes that enhanced postpartum HTN management—including remote or self-measured BP monitoring with timely clinical response, structured medication titration pathways, and coordinated transition to primary or cardiovascular care—has moderate evidence of effectiveness in improving short-term postpartum process outcomes and BP control among women with chronic HTN or HDPs. Across RCTs, controlled intervention studies, and pragmatic implementation programs, enhanced care models consistently increase BP ascertainment, support more rapid medication adjustment, and may reduce BP- and hypertensive-related readmissions during the early postpartum period, when the risk of stroke and SMM is greatest.
Although the evidence base varies in methodological rigor and most studies evaluate outcomes over limited follow-up periods (typically ≤12 weeks), the direction of benefit is consistent across diverse programs,
including those incorporating home BP monitoring with active management, telehealth follow-up, multidisciplinary care pathways, and structured communication protocols. These interventions are low risk, feasible to implement, and particularly valuable for women discharged on antihypertensives, those with severe HDP, and those facing barriers to timely in-person follow-up.
However, evidence supporting multicomponent transitional care models—such as cardiometabolic risk screening, weight and nutrition counseling, mental health assessment, and explicit linkage to long-term primary care or cardiology—remains more limited. Heterogeneity in intervention components, underpowered feasibility studies, and inconsistent reporting of clinical outcomes constrain conclusions regarding the magnitude or durability of benefit beyond the immediate postpartum window.
Conclusion 4-2: Evidence is moderate that enhanced postpartum hypertension management programs—particularly those combining remote or self-measured blood pressure (BP) monitoring with structured clinical response—improve early postpartum BP ascertainment, engagement, and short-term BP control among women with chronic hypertension or hypertensive disorders of pregnancy. Evidence is mixed regarding their effect on hospital readmissions and insufficient to determine whether these interventions reduce severe maternal morbidity, mortality, or long-term cardiovascular outcomes.
Research Considerations
To strengthen the evidence base, larger and adequately powered randomized trials are needed to determine the effectiveness of enhanced postpartum HTN management on clinically meaningful outcomes, including SMM, emergency care use, and readmissions. These trials need to also evaluate the degree to which benefits extend beyond the first 12 weeks postpartum and whether early chronic HTN treatment and surveillance meaningfully alter longer-term outcomes, such as progression to, cardiomyopathy, heart failure, stroke, and ischemic heart disease.
Because many studies evaluated bundled or multicomponent interventions, research needs to clarify which aspects drive the greatest benefit and are feasible to implement at scale. Longitudinal cohort studies following women into the postpartum and interpregnancy periods will be essential to understanding whether enhanced postpartum care influences cardiovascular trajectories across the life course.
Future trials and cohorts could also incorporate biospecimen collection and prespecified biomarker analyses to support risk stratification and clarify mechanisms linking HDP to persistent HTN and later cardiovascular
TABLE 4-4 Summary of Evidence on Enhanced Postpartum Hypertension Managementa
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Cairns et al., 2018 Hypertension | RCT; 5 NHS hospitals, England, U.K. | N = 91 PP women with gHTN or PE requiring antihypertensives (45 intervention; 46 control) Reproductive period: PP (day 10 → 6 months) | Daily home BP monitoring with automated telemonitoring–guided medication down titration vs. usual community midwife/GP care | BP control; proportion of readings in target range; feasibility | Lower BP with self-management (largest at 6 weeks; DBP benefit to 6 months); more readings in target range (93% vs. 62%); high feasibility; no safety issues | Fair |
| Hirshberg et al., 2018 BMJ Quality & Safety | RCT; single academic medical center, U.S. | N = 206 PP women with pregnancy-related HTN (103 text; 103 office) Reproductive period: PP (10 days) | Twice-daily text-based BP monitoring; automated feedback, clinician alerts for severe BPs vs. standard in-office BP check at 4–6 days PP | BP ascertainment; meeting ACOG timing; readmissions | Text monitoring greatly improving BP ascertainment (92 vs. 44 percent) and ACOG-timed checks (84% met both intervals) No HTN-related readmissions in text arm (vs. 3.9%) High satisfaction; similar antihypertensive initiation | Fair |
| Hamza et al., 2019 Archives of Gynecology and Obstetrics | Prospective cohort study, Germany | N = 30 women with PE Reproductive period: PP (2 hours PP and days 6–10) | Within-subject comparisons of pre- and PP biomarker levels and association with PP worsening | Association of PP worsening with biomarker levels | 73% with persistent or worsened PE; 50% with new or worsening complications PP | Poor |
| Hoppe et al., 2019 Pregnancy Hypertension | Prospective single-cohort; Midwestern academic hospital, U.S. | N = 55 PP women with cHTN, gHTN, or PE-spectrum HTN Reproductive period: PP (discharge → 6 weeks) | Daily remote BP transmission + nurse-driven telehealth management | Feasibility; severe HTN (≥160/110 mmHg); BP requiring treatment (≥150/100 mmHg); ED use; readmission | High feasibility (95% retention) Severe HTN 16%; BP requiring treatment 53%; 0 readmissions Telehealth-enabled early identification/intervention; 87% satisfied | Fair |
| Kalafat et al., 2020 Pregnancy Hypertension | Systematic review with meta-analysis Studies included U.K., U.S., France, Belgium | 9 studies included in meta-analysis Pregnant or PP women with HDP, cHTN, GHD, or at high risk of PE; some studies including low-risk pregnancies Reproductive period PN, PP | HBPM with validated or nonvalidated automated BP monitors Conventional care with office-based BP measurement and routine antenatal/PP visits | Induction of labor, PN hospital admissions, PE diagnosis, APOs | Labor induction: OR 0.55 (95% CI 0.36–0.82) PN admissions: OR 0.31 (95% CI 0.19–0.49) Diagnosis of PE: OR 0.50 (95% CI 0.31–0.81) Antenatal visits: SMD −0.49 (95% CI −0.82 to −0.16) | Good |
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Triebwasser et al., 2020 Pregnancy Hypertension | Retrospective cohort study, U.S. | HDP N = 333 (implementation cohort) N = 103 trial cohort Reproductive period: PP | Text-based BP monitoring Women randomized to text-based BP monitoring in a clinical trial compared to an implementation cohort clinically enrolled in text-based BP monitoring | BP ascertainment within first 10 days PP | Severe BP in implementation: 12.9% Of severe BP cases, 65.1% requiring treatment changes No significant difference in treatment initiation/titration vs. trial cohort | Fair |
| Kitt et al., 2021 Hypertension | Individual RCT, U.K. | N = 61 women with PE or gHTN and requiring BP-lowering medication PP (N = 31 control; N = 30 randomized to self-management) Reproductive period: PP | PP BP self-management using home monitoring and teletransmission with clinician feedback Usual PP HTN follow-up (in-person clinic BP checks and standard discharge counseling) | Mean SBP; mean DBP at 3–4 years 6 months PP | Mean SBP at 6 months: Intervention: 126.0 mmHg (SD 10.5) Control: 130.8 mmHg (SD 10.8) Adjusted mean difference: −4.8 mmHg (95% CI, −8.8 to −0.8); p = 0.02 Mean DBP at 6 months: Adjusted mean difference: −3.3 mmHg (95% percent CI, −5.9 to −0.8); p = 0.01. BP control (<140/90 mmHg): 82% in self-management vs. 70% in control; p = 0.04 (95% CI, −10.7 to −4.2) P < 0.001 | Good |
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Riemer et al., 2021 Geburtshilfe Frauenheilkd | RCT, Germany | N = 38 women with severe HDP (PE with or without preexisting HTN and/or HELLP syndrome) and N = 38 without PE or HELLP syndrome Reproductive period: PP (6 weeks) | Lifestyle intervention with physical exercise after delivery (starting 6 weeks PP) Comparison group: PP women without pregnancy complications or known CVR | Feasibility; PWV at the time of delivery | After 6 months, clinically significant difference (d = 0.65) in PWV between the intervention and control groups; PWV of the intervention group corresponding to that of the reference group; control group much higher | Poor |
| Suresh et al., 2021 Obstetrics & Gynecology | Before–after QI initiative, academic tertiary care hospital, U.S. | N = 926 PP with HDP across 4 time periods Reproductive period: PP (delivery → 6 weeks) | Hospital-wide PP STAMPP-HTN bundle (standardized protocols, education, nurse educator, scheduled PP BP checks, BP cuffs) | PP visit adherence; BP levels; severe HTN; readmissions | PP HTN visit adherence ↑ (33.5%→59.4%); immediate PP BP and severe HTN ↓; fewer women with BP ≥140/90 at first PP visit (39%→19%); readmissions unchanged | Fair |
| Nguyen et al., 2022 Pregnancy Hypertension | Before–after QI study; tertiary academic hospital, U.S. | N = 566 with ≥2 severe-range BPs (304 pre; 262 post) Reproductive period: Inpatient PN, PP | Standardized severe HTN pathway + staff education + compliance monitoring vs. preimplementation usual care | Any antihypertensive; consistent treatment; time to medication | Any treatment ↑ (67%→80%); consistent treatment ↑ (29%→47%); time to antihypertensive ↓ (24→10 min); (83%→98%) treated within 60 min; SMM unchanged | Fair |
| Aderibigbe et al., 2023 American Journal of Obstetrics & Gynecology Maternal-Fetal Medicine | Individual RCT, U.S. | N = 256 randomized (128 “tight control,” 128 “liberal control”) Reproductive period: PP | Initiation of antihypertensive therapy at 1 of 2 BP thresholds: 140/90 mmHg (tight control group) or 150/95 mmHg (liberal control) Hg (“liberal control” group). Choice of medication left to the discretion of obstetrical providers or care team | Maternal morbidity (one or more of severe HTN PE with severe features, need for second drug, hospital stay >4 days, or maternal adverse outcome) | No significant difference BP control and need for medication; no reduction for tighter threshold versus traditional threshold | Fair |
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Arkerson et al., 2023 | Multisite RCT; two academic training institutions, U.S. | N = 197 PP women with HDP (96 remote; 101 in office) Reproductive period: PP (0–10 days) | Remote BP monitoring via smartphone platform vs. scheduled in-office BP check | BP ascertainment); antihypertensive initiation; unscheduled visits; readmissions; racial disparities | BP ascertainment ↑ (92% vs. 58%); no differences in med initiation, unscheduled visits, or readmissions; remote monitoring eliminating racial disparity for in-office follow-up | Fair |
| Bronner et al., 2023 American Journal of Obstetrics & Gynecology Maternal-Fetal Medicine | Retrospective cohort study, U.S. | N = 545 patients (245 preintervention; 300 postintervention) Reproductive period: PP (immediate; hospital discharge to 6 weeks PP) | EM Usual care vs. standard monitoring for 36 hours after last BP ≥150/100 mmHg before discharge | Readmission for PE with severe features within 6 weeks PP; LOS; number and timing of readmissions, ICU admissions | 25 of 300 (8.3%) in EM group vs. 10 of 245 (4.1%) preintervention; increased readmission risk after EM implementation | Fair |
| Hauspurg et al., 2023 BJOG | Individual RCT, U.S. | N = 148 PP women with overweight or obesity (BMI ≥25 kg/m2) and history of gHTN or PE Reproductive period: PP | Multicomponent intervention targeting CVR after HDP (remote home BP monitoring, individualized health coaching, iHealth, Wireless Blood Pressure Monitor BP5) | Feasibility; acceptability, BP; weight/BMI | Combined remote BP monitoring and lifestyle coaching PP feasible and well accepted Improvements in BP control, weight, diet, and PA behaviors | Goodb |
| Hirshberg et al., 2023 Obstetrics & Gynecology | Retrospective cohort study, U.S. | N = 1,700 Independence Blue Cross members with HDP Reproductive period: PP (10 days postdelivery) | 10-day text message–based remote BP monitoring following delivery Cohort A (asynchronous control) vs. Cohort C (contemporaneous control) | Stroke, DIC, eclampsia, pulmonary edema, HELLP, renal/liver injury, MI, or cardiomyopathy | Within the first 6 weeks PP, patients enrolled in remote monitoring less likely to have the composite adverse outcome than those in Cohort A (2.9% vs. 4.7%; OR 0.61, 95% CI 0.40–0.98) and with more cardiology visits and fewer PN ED visits and readmissions; no statistically significant difference relative to Cohort C (3.2% vs. 4.5%; OR 0.71, 95% CI 0.47–1.07) | Fair |
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Kitt et al., 2023 JAMA | RCT, U.K. | N = 220 women with PE or gHTN requiring PN antihypertensives when discharged Intervention group (N = 112); control group (N = 108) Reproductive period: PP (day 1 → 9 months) | Self-monitoring with physician-optimized antihypertensive titration vs. usual PN care | 24-hour mean DBP at 9 months PP | 24-hour mean DBP, measured at 249 +16 days PP, 5.8 mmHg lower in the intervention group; 24-hour mean SBP 6.5 mmHg lower in the intervention group than in the control group | Good |
| Mei et al., 2023 Obstetrics & Gynecology | Prospective cohort study, U.S. | N = 780 (390 postintervention; 390 historical control group) Reproductive period: PP | Institution-wide SCAMP for PP HTN with inpatient and outpatient components No comparison group | PP readmission or ED visit for HTN; rates of antihypertensive, compliance with remote BP monitoring, medication adjustments, hypotension and side effects, PP and total LOS | Reduced PP HTN readmissions/ED visits by ~80%; no difference in LOS or hypotension rates; high-risk groups (Black race, chronic HTN, on discharge medication) benefiting most; improved follow-up and early medication titration with remote BP monitoring | Fair |
| Schneider et al., 2023 American Journal of Obstetrics & Gynecology: Maternal-Fetal Medicine | Statewide Quality Improvement Initiative using the AIM Severe Hypertension in Pregnancy patient safety bundle, U.S. | N = 4,678 unique patients (4,948 hypertensive events) from 29 Ohio hospitals (Levels 1–4) Reproductive period: PN, PP (through 6 weeks) | Implementation of multimodal, statewide QI program adapting AIM bundle to improve identification and management of sustained severe HTN Comparison: Baseline data from the same hospitals (July–September 2020) | Feasibility; timely treatment; racial disparities; discharge education; PP follow-up; medication follow-up; BP cuff provision |
| Fair |
| Steele et al., 2023 Obstetrics & Gynecology | Systematic review (with or without metaanalysis), U.K., U.S., India | All comparative studies (N = 13) with participants (N = 3,867) with a diagnosis of HDP Reproductive period: PP | HBPM Comparison: HBPM programs compared with standard in-office BP monitoring or paper logs | BP ascertainment; treatment initiation; maternal morbidity and mortality; racial disparities | Home monitoring not associated with the rate of BP treatment initiation (aRR 1.03, 95% CI 0.74–1.44) but is with reduced unplanned HTN-related hospital admissions (aRR 0.12, 95% CI 0.01–0.96); most (83.3–87.0%) satisfied with management related to home monitoring, associated with reduced racial disparities in ascertainment by approximately 50% compared with office-based follow-up | Good |
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Amro et al., 2024 JAMA Network Open | Pre–post QI; Tertiary care academic medical center, U.S. | N = 1,160 PP patients (595 preintervention, December 2017–December 2018; 565 postintervention, March 2019–December 2019) Reproductive period: PP | BP evaluation and PE screening at well-child visit; management algorithm—with criteria for routine or early PP visits, or prompt referral to the obstetric ED—followed Comparison group: Patients enrolled after implementation of QI program | Readmission due to PE with severe features within 2 months after delivery | Significantly different rates of readmission for PP PE (preintervention, 13 patients [2.1%], vs. postintervention, 29 patients [5.6%]; P = .007) cohorts; postintervention QI cohort with significantly earlier time frame of readmission (median [IQR] 10.0 [10.0–11.0] days PP for preintervention vs. 7.0 [6.0–10.5] days PP for postintervention; P = .001) | Fair |
| Bisson et al., 2024 Pregnancy Hypertension | Retrospective cohort study, U.S. | N = 1,480 No follow-up at 6 weeks to 12 months: 541 Any follow-up: 939 Reproductive period: PP (6 weeks–12 months) |
Provided at delivery discharge:
| Follow-up visits with cardiology and PCPs; BP readings, antihypertensives, EKG performance, diagnosis of stroke or thromboembolic disease; cholesterol values; HbA1c values; number of ED visits; peak BP values | <50% completing PCP or cardiology follow-up by 12 months PP; Black race and public insurance strongly associated with poorer long-term follow-up; BP control worse after 6 weeks and remaining poor at 1 year; patients with cardiology follow-up more medically complex and more likely to be on medication but with worse BP control at 12 months; ED use higher among those with no appropriate follow-up | Fair |
| Sarma et al., 2023 Journal of the American College of Cardiology: Advances | Pilot; Massachusetts General Hospital, U.S. | N = 62 PP patients who delivered February–May 2021 with cHTN, gHTN, or PE Reproductive period: PP | Patients provided with BP cuffs, educated on self-measurement, HTN, and HDP, shown educational videos on BP measurement | PP hospital readmission within 6 weeks; 6-week PP BP; frequency of medication titration; feasibility | Hospital readmission for severe HTN in 7% of patients who completed the intervention, all within the first week; one-third requiring medication initiation and 62% receiving further titration through the study, most frequently in the first PP week among those with gHTN and first 3 PP weeks among those with cHTN and PE | Fair |
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Borrowman at al., 2025 Journal of Medical Internet Research Formative Research | Single-arm quasiexperimental study; U.S. | N = 19 women, 3–6 monthly PP HDP Reproductive period: PP | Remotely delivered 14-week coaching intervention (HDP PP Exercise) (online health coaching sessions, provided with a Fitbit Inspire 2 to track progress) | Feasibility; adaptability; increase average number of steps | No significant changes in steps from pre- to posttesting (mean 138.40, SD 129.40 steps/day; P = .75); significant improvements in PA behavior skills, including planning (mean 5.35, SD 4.97 vs. mean 15.06, SD 3.09; P < .001) and monitoring of PA levels (mean 7.29, SD 3.44 vs. mean 13.00, SD 2.45; P < .001); NS for SBP (mean –1.28, SD 3.59 mmHg; Hedges g = –0.26; P = .16) and DBP (mean –1.80, SD 5.03 mmHg; Hedges g = –0.44; P = .12) | Fair |
| Forna, F. et al., 2024 Pregnancy Hypertension | Matched retrospective cohort, Kaiser Permanente of Georgia, U.S. | N = 1,030 patients enrolled in RPM HTN (517 antepartum; 513 PP) who delivered November 2019–October 2021; 937 matched to historical controls Reproductive period: PN, PP | RPM HTN (Bluetooth-enabled BP monitor and cuff; weekly telehealth visits) Comparison group: matched patients who delivered in the 48-month period before RPM HTN | Mean gestational age at delivery; PTB; Cesarean section; maternal death; mean LOS, PP readmission, ICU admission | Remote HTN monitoring associated with improved BP monitoring, better PP BP control, and improved follow-up after delivery compared to historical controls | Poor |
| Lemon et al., 2024 Obstetrics & Gynecology | Retrospective cohort; Magee-Women’s hospital; University of Pittsburgh, U.S. | N = 12,038 patients with HDPs (6,556 participants, 5,482 controls) Reproductive period: PP | Enrollment in a remote HTN management program (BP cuff, BP management education); text prompt reminders to check BP at various time points Comparison group: usual care | PP care use (including hospital readmission and ED visits); office visit within 6-weeks PP; BP measurement within 10 days; initiation of antihypertensives | Remote monitoring of PP HTN associated with fewer readmissions, increased adherence to national clinical guidelines, and initiation of antihypertensives for patients with HDPs | Fair |
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Macphail et al., 2024 Canadian Journal of Cardiology Open | Systematic review (with or without meta-analysis) Included studies from Canada, Switzerland, Germany, the Netherlands, U.S. | N = 8–151 participants Reproductive period: PP | Structured nutrition intervention Comparison: Standard PP care vs. no structured nutrition intervention | BP, lipids, CVD risk score, weight/BMI, waist circumference, body fat, diet adherence/DASH score, self-efficacy and CVD risk knowledge | Statistically nonsignificant yet clinically important improvements in measures of CVR across a range of nutritional interventions in women after HDPs | Fair |
| Pihelgas et al., 2025 Obstetric Medicine | Case-control study, Canada | Women with history of preterm PE (<34 weeks) N = 470 surveys mailed (cases: 235 mailed, 94 returned; controls: 235 mailed, 63 returned) Reproductive period: PP (1–10 years postpregnancy with PE) | PPPC Multidisciplinary CV risk reduction model Comparison: Women who missed/declined PPPC referral or were seen in obstetric medicine clinic PP but not referred to PPPC | New diagnoses of vascular events or risk factors that occurred after the pregnancy complicated by PE; weight maintenance |
Cardiovascular outcomes
| Poor |
| Reddy et al., 2024 Journal of the American College of Cardiology: Advances | Feasibility study; UPMC Montefiore Hospital, U.S. | N = 3,662 (2,366 in 6-week remote monitoring; 1,318 in extended monitoring) Reproductive period: PP (6 weeks–1 year) | Extension of remote BP management program, including reporting prompts Comparison: 6-week remote monitoring group | Feasibility of a remote BP management program extending through the first year PP | Ongoing BP monitoring beyond the immediate 6 weeks PP in those with persistent HTN after an HDP feasible to optimize BP | Fair |
| Tao et al., 2024 American Journal of Obstetrics & Gynecology: Maternal-Fetal Medicine | Retrospective cohort study, Midwestern academic center, U.S. | N = 413 PP women (267 with PP BP spike) diagnosed with HDP Reproductive period: PP (6 weeks) | Remote BP monitoring program Comparison group: patients with <41 observations but at least 1 observation 3–7 days PP and the group of remaining patients; comparisons of patients’ basic characteristics and different levels of HTN among different risk groups | PP BP spikes, effectiveness of interventions in reducing BP spikes |
| Poor |
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Borders et al., 2025 American Journal of Obstetrics & Gynecology | Prospective cohort study, U.S. | N = 8,783 patients with a first episode of severe HTN during pregnancy or within 6 weeks PP at any participating hospital Reproductive period: PN, PP (6 weeks) | Statewide implementation of the Illinois Perinatal Quality Collaborative Severe Maternal Hypertension Quality Improvement Initiative Comparison: Usual care | Reduction of SMM | SMM decreased significantly (11.5→8.4%); no significant changes in eclampsia, hemorrhage requiring transfusion, or ICU admissions or increase in maternal hypotension | Good |
| Kusumaningrum et al., 2025 Pediomaternal Nursing Journal | Systematic review (with or without meta-analysis) Studies from countries in five continents (Asia, Africa, America, Australia, and Europe) | N = 6,081,090 PP women across reviewed studies Reproductive period: PP | Education, counseling, follow-up, monitoring, exercise Comparison: no treatment, standard treatment | HTN prevention, BP control; adherence to monitoring; medication use; reduced readmissions; disease knowledge; follow-up; long-term risk of metabolic syndrome | Women with a history of PE, especially severe PE, at higher risk of PP HTN; tailored PP care needed to mitigate that risk and reduce rehospitalization | Fair |
| Mai et at., 2025 British Journal of Obstetrics and Gynaecology | Meta-analysis of studies from 7 countries (U.S., England, Australia, Canada, Germany, the Netherlands, and Indonesia) | N = 2,200 women with prior HDP across 16 studies Reproductive period: PP | Self-care, including home BP monitoring, lifestyle change, physical activity, and a neonatal sleep intervention Comparison: usual/standard care, or in-office BP monitoring | Cardiovascular events; cHTN; SBP/DBP; PP HTN readmission; antihypertensive medication use | Meta-analysis (9 RCTs; 952 women) found lower BP with self-care interventions: SBP MD −3.24 mmHg (95% CI −5.42, −1.06; low certainty) and DBP MD −3.07 mmHg (95% CI −4.88, −1.25; low certainty); self-care interventions likely decreased PP HTN readmission (3 RCTs; 605 women): RR 0.35 (95% CI 0.14, 0.89; moderate certainty); insufficient studies to pool cardiovascular events and cHTN outcomes | Fair |
| Patel et al., 2025 Pregnancy Hypertension | Prospective cohort study, U.S. | N = 306 PP patients with HDP Reproductive period: PP | STAMPP-HTN RPM program integrated into PP care Comparison: Usual care with telehealth PP BP check visits | Attendance at first PP BP check visit; 6-week visit attendance | Decrease in HTN rates over the 6-week PP period, with higher rates of HTN among Black compared to non-Black patients; engagement with the RPM program associated with improved BP control | Fair |
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Rosenfeld et al., 2025 Journal of the American College of Cardiology: Advances | Prospective cohort with propensity-matched retrospective control (nonrandomized), U.S. | Interventional (N=392) vs. retrospective (N=1,204); post–propensity score match: N=276 vs. N=429 PP women with hypertensive disorders Reproductive period: PP (6 weeks) | Intervention: treated to maintain BP <130/80 mmHg using remote BP monitoring. Comparison: treated to maintain <150/100 mmHg | ED visit for PP hypertensive disorder; hospital readmission, PP BP, magnesium treatment, medication use, PP visit attendance | ED visits lower in intervention: 3.6% vs. 8.4%; BP lower by ~4/3 mmHg at 6 weeks; reduced ED visits and improved BP control with tight PP BP control <130/80 mmHg with remote monitoring | Fair |
| Zullo et al., 2025 Journal of Perinatal Medicine | Systematic review (with or without metaanalysis), U.S., U.K. | N = 714 (randomized participants diagnosed with HDP across four RCTs): (telemonitoring group: 356; standard care group: 358) Reproductive period: PP | Remote or digital PP BP monitoring Comparison: Standard PP care | Hypertensive-related PP readmission; ED visits, BP assessment; PP visit attendance | No reduction in hypertensive-related readmissions; increased ED visits; no improvement in PP follow-up care completion | Good |
NOTES: a Studies are listed by publication year (oldest first), then alphabetically by first author within each year. b Quality rating was assessed using the National Heart, Lung, and Blood Institute Quality Assessment Tools. Ratings: Good = low risk of bias; Fair = some concerns; Poor = serious risk of bias. b Hauspurg et al., which evaluated a combined PP home BP monitoring and lifestyle intervention for women with prior HDP, received discrepant quality ratings during adjudication. While it was well executed as a feasibility trial, the evidence review identified two limitations relevant to assessing effectiveness: (1) high differential dropout and (2) insufficient power for clinical outcomes. Therefore, it was judged poor quality for determining effectiveness but good quality for feasibility. Its inclusion in the evidence review reflects that feasibility findings are informative for implementation considerations, while appropriately limiting its influence on the overall effectiveness conclusions. ACOG = American College of Obstetricians and Gynecologists; AIM = Alliance for Innovation on Maternal Health; APO = ad-verse pregnancy outcome; aRR = adjusted relative risk; BMI = body mass index; BP = blood pressure; cHTN = chronic hypertension; CI = confidence interval; CI = confidence interval; CV = cardiovascular; CVD = cardiovascular disease; CVR = cardiovascular risk; DASH = disabilities of arm, shoulder, and hand; DBP = diastolic blood pressure; DIC = disseminated intravascular coagulation; ED = emergency department; EM = Extended Inpatient Monitoring; GHD = gestational hypertensive disorder; gHTN = gestational hypertension; GP = general practitioner; HbA1c = hemoglobin A1c; HBPM = home blood pressure monitoring; HDP = hypertensive disorders of pregnancy; HELLP = hemolysis, elevated liver enzymes, and low platelets; HTN = hypertension; ICU = intensive care unit; IQR = interquartile range; LOS = length of stay; MI = myocardial infarction; NHS = National Health System; OR = odds ratio; PA = physical activity; PCP = primary care provider; PE = preeclampsia; PN = prenatal; PP = postpartum; PPPC = postpartum preeclampsia clinic; PTB = preterm birth; PWV = pulse wave velocity; QI = quality improvement; RCT = randomized controlled trial; RPM = remote patient monitoring; SBP = systolic blood pressure; SCAMP = Standardized Clinical Assessment and Management Plan; SD = standard deviation; SMM = severe maternal morbidity; STAMPP = Systematic Treatment and Management of Postpartum Hypertension; UPMC = University of Pittsburgh Medical Center.
SOURCES: Aderibigbe et al., 2023; Amro et al., 2024; Arkerson et al., 2023; Bisson et al., 2024; Borders et al., 2025; Borrowman et al., 2025; Bronner et al., 2023; Cairns et al., 2018; Forna et al., 2024; Hamza et al., 2019; Hauspurg et al., 2023; Hirshberg et al., 2018; 2023; Hoppe et al., 2019; Kalafat et al., 2020; Kitt et al., 2021, 2023; Kusumaningrum et al., 2025; Lemon et al., 2024; Macphail et al., 2024; Mai et al., 2025; Mei et al., 2023; Nguyen et al., 2022; Patel et al., 2025; Pihelgas et al., 2025; Reddy et al., 2024; Riemer et al., 2021; Rosenfeld et al., 2025; Sarma et al., 2023; Schneider et al., 2023; Steele et al., 2023; Suresh et al., 2021; Tao et al., 2024; Triebwasser et al., 2020; Zullo et al., 2025.
disease. Studies could evaluate biomarker trajectories, as opposed to single time points; establish postpartum reference ranges and clinically meaningful thresholds; and test whether biomarkers improve prediction beyond readily available clinical variables, socioeconomic variables, and self-measured BP data. This research could assess whether biomarker-informed strategies can safely tailor the intensity and duration of postpartum monitoring and treatment (e.g., identifying women who benefit from prolonged monitoring versus those appropriate for earlier step-down and primary care transition).
Implementation science is needed to define how technology platforms, workforce models, reimbursement structures, and cross-sector partnerships can support sustainable deployment of enhanced postpartum hypertension (HTN) programs and reduce gaps in access, follow-up, and treatment. Particular attention should be paid to populations disproportionately affected by maternal morbidity and mortality, ensuring that enhanced models reduce rather than widen disparities. Finally, evaluating how enhanced postpartum management can be integrated into broader cardiovascular prevention frameworks remains a key national research priority, including opportunities to align postpartum care with HTN control efforts, primary care transition initiatives, and long-term cardiometabolic risk reduction strategies.
URGENT MATERNAL WARNING SIGNS
Overview of the Question and Gap
UMWS are signs and symptoms during or after pregnancy that can indicate a potential dangerous or fatal complication. Interventions to increase earlier recognition and assessment of UMWS have been promoted as a strategy to reduce maternal morbidity and mortality from multiple causes (AWHONN, 2025; CDC, 2024a). Many of these early warning signs are related directly to cardiovascular morbidity and mortality, including vital sign abnormalities (e.g., HTN, tachycardia, tachypnea, oxygen desaturation) and symptoms such as chest pain, shortness of breath, and syncope. UMWS are important for patients, communities, and clinicians to take notice of and not dismiss because they can be early signals of life-threatening conditions, such as severe HTN, stroke, cardiomyopathy, pulmonary embolism, sepsis, or hemorrhage.
Delayed recognition or response to these warning signs is frequently identified by committees who review maternal deaths in states and jurisdictions (Maternal Mortality Review Committees [MMRCs]).3 These issues are
___________________
3Maternal Mortality Review, the core function performed by MMRCs, is a formal review process adopted by many states that follows structured guidelines established by CDC.
crucial quality-improvement opportunities to prevent maternal morbidity and mortality (Umar et al., 2019).
For this review, the committee defined screening for early maternal warning signs to include any screening for one or more UMWS signs or symptoms in clinical (e.g., vital sign-based triggers in hospitals) or community (e.g., patients monitor for symptoms such as headaches or chest pain) settings during pregnancy, postpartum, or both. The committee undertook a review to evaluate the evidence on whether screening for urgent cardiovascular warning signs (or UMWS), including counseling patients to self-screen or having health care teams initiate appropriate clinical protocols when such signs are detected, reduces SMM or mortality.
Summary of the Evidence
The initial literature search yielded 1,356 records (390 duplicates) with publication dates from January 2015 to August 2025; 966 were screened at the abstract level. Eighty-four articles were eligible for full-text review because they were conducted in the United States and other very high–income UN countries and reported outcomes relevant to the research question. Only three met all inclusion criteria; the most common reasons for exclusion were wrong intervention and no relevant outcome. Risk-of-bias assessments and data extraction were conducted for these three studies (see Table 4-5). The committee also noted several studies focused on assessing the predictive accuracy of early warning scores rather than whether implementing these tools improved maternal outcomes and several studies indicating that educating patients about UMWS improved knowledge and readiness. The committee identified 17 narrative and scoping reviews and expert opinion pieces and used them to provide background and context and screened the reference lists to ensure it did not miss relevant intervention studies.
All three included studies (1 fair, 2 poor) evaluated inpatient use of electronic early warning systems for health care teams on maternal morbidity outcomes among pregnant and newly postpartum patients in hospital settings. None examined outpatient or self-screening interventions for UMWS with maternal morbidity or mortality outcomes.
Inpatient Maternal Early Warning Systems
One study (poor quality) evaluated implementation of a Maternal Early Warning Trigger (MEWT) tool with clinical response pathways in six hospitals within a California health system, using 23 hospitals in the same system as contemporaneous comparators (N = 36,832 deliveries at pilot sites [24,221 pre-MEWT; 12,611 post-MEWT] and N = 146,359 at comparison
TABLE 4-5 Summary of Evidence on Urgent Maternal Warning Systemsa
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Shields et al., 2016 American Journal of Obstetrics & Gynecology | Prospective implementation; six hospitals within a large health system, U.S. | N = 36,832 deliveries at pilot sites (24,221 pre-MEWT; 12,611 post-MEWT) and N = 146,359 at comparison sites Reproductive period: Delivery hospitalization | MEWT tool vs. baseline usual care; nonpilot sites as contemporaneous comparison | CDC-SMM; composite morbidity; ICU admission | At pilot sites, CDC-SMM 2.0% → 1.6% and composite morbidity 5.9% → 5.1%; no change at nonpilot sites Screening >93%; trigger-positive 2.3% MEWT sensitivity for ICU cases 96.9%; ICU admissions unchanged | Poor |
| Blumenthal et al., 2021 American Journal of Perinatology | Prospective pre–and postimplementation study; three hospitals (one tertiary + two community sites), U.S. | N = 20,000 encounters screened (pre-MEWT N = 9,971; post-MEWT N = 9,949) Reproductive period: Delivery hospitalization + PP inpatient stay | Electronic MEWT (EPIC-integrated triggers + order sets) vs. prior nonelectronic system | Composite morbidity (ICD-10 + PPLOS + ICU), MEWT category-specific metrics, process measures | Slightly increased overall morbidity (1.6% → 2.06%) due to unusually low baseline year Improved time to antibiotics in sepsis (1.87 h → 0.75 h) and antihypertensives ≤60 min (62% → 83%) Trigger rate 2.1% MEWT sensitivity for morbidity 50% (higher for HTN, sepsis, cardiopulmonary; lower for hemorrhage) | Fair |
| Drake et al., 2021 Anaesthesia | Before–after implementation study; large tertiary maternity center, Aotearoa New Zealand | Emergency response and arrest call data for maternity inpatients before (January 2017–May 2018) and after (March 2019–December 2020) NZMEWS. Reproductive period: Inpatient PN, PP (up to discharge) | NZMEWS vs. prior vital signs chart | Emergency response calls; cardiorespiratory arrest calls (per 100 births) | Emergency response calls 0.8 → 0.6 per 100 births. Cardiorespiratory arrest calls 0.14 → 0.09 per 100 births (NS) Findings support earlier recognition/response; multiple contextual factors may contribute | Poor |
NOTES: a Studies are listed by publication year (oldest first), then alphabetically by first author within each year. b Quality rating was assessed using the National Heart, Lung, and Blood Institute Quality Assessment Tools. Ratings: Good = low risk of bias; Fair = some concerns; Poor = serious risk of bias. CDC = Centers for Disease Control and Prevention; HTN = hypertension; ICD-10 = International Classification of Diseases, 10th revision; ICU = intensive care unit; MEWT = Maternal Early Warning Trigger; NS = not significant; NZMEWS = New Zealand Maternity Early Warning System; PN = prenatal; PP = postpartum; PPLOS = prolonged postpartum length of stay; SMM = severe maternal morbidity.
SOURCES: Blumenthal et al., 2021; Drake et al., 2021; Shields et al., 2016.
sites) (Shields et al., 2016). The key finding was that SMM decreased in the intervention hospitals (2.0 to 1.6 percent), while remaining unchanged in comparison hospitals (2.4 percent to 2.4 percent), but the analytic limitations reduce confidence in a causal effect. MEWT was designed to identify early signs of sepsis, cardiovascular dysfunction, severe hypertensive disorders, and severe hemorrhage and prompt standardized management (e.g., ordering brain natriuretic peptide and cardiac enzyme blood tests) (Shields et al., 2016). All deliveries in the six intervention hospitals were compared preimplementation (January 2012–December 2013; N = 9,971) versus postimplementation (October 2014–October 2015; N = 9,949). Baseline SMM, according to the CDC definition, was higher in the nonintervention hospitals (2.4 versus 2.0 percent). The intervention hospitals experienced an 18.6 percent relative reduction in SMM (2.0 to 1.6 percent), with no change in the nonintervention hospitals (2.4 to 2.4 percent). However, no adjustment was made for baseline differences, statistical methods were minimally reported, and the baseline imbalance between groups was not discussed. Screening timing (triage, antepartum, labor, or postpartum) was not described explicitly, and patients who did not deliver during an admission (e.g., triage or antepartum admissions) were not accounted for clearly. Alerts were triggered in 2.3 percent of births; sensitivity for ICU admission was 96.9 percent with specificity of 99.9 percent. In more than 80 percent of trigger events, physician assessment and intervention occurred within 60 minutes, and clinicians followed the clinical pathway about 80 percent of the time (Shields et al., 2016).
A second study (fair quality) was a pre- versus postimplementation evaluation of a modified, EPIC-integrated MEWT system across three hospitals in a different California health system (pre-MEWT N = 9,971; post-MEWT N = 9,949) (Blumenthal et al., 2021). It found that overall composite morbidity increased after implementation, but treatment within 60 minutes improved for severe HTN triggers (62 percent preimplementation versus 83 percent postimplementation) (Blumenthal et al., 2021). The tool was applied to labor and delivery patients through the end of the postpartum stay (excluding ICU and operating room time). The primary outcome was a validated composite maternal morbidity (SMM codes, prolonged hospitalization, unanticipated ICU admission, or any combination of the three). Most MEWT triggers were cardiovascular, including HTN (51 percent) and cardiopulmonary issues (23 percent). Composite morbidity increased from 1.60 percent preimplementation to 2.06 percent postimplementation, driven largely by increased HTN-related codes, while unanticipated ICU admission did not change. The authors noted that secular variation limited causal interpretation, including an unusually low morbidity rate in the baseline year; the specific study years were not reported. Alerts occurred in 2.1 percent of encounters; MEWT sensitivity for detecting morbidity
was 50 percent with specificity of 96 percent (higher sensitivity for HTN, sepsis, and cardiopulmonary issues and lower sensitivity for hemorrhage) (Blumenthal et al., 2021).
A third study (poor quality) evaluated implementation of the New Zealand Maternity Early Warning Score (NZMEWS) in a single tertiary hospital, accompanied by staff education and audit/feedback (Drake et al., 2021). NZMEWS is a pregnancy-specific adaptation of a nationally implemented early warning score originally developed for nonpregnant populations. All births in the preimplementation period (January 2017–June 2018) were compared with those in the postimplementation period (March 2019–December 2020). It was implied but unclear that the immediate postpartum period was included. Emergency response calls fell from 0.8 to 0.6 per 100 births. Calls specifically for cardiorespiratory arrest were not significantly different (0.14 to 0.09 per 100 births). The number of alerts and alert performance characteristics were not reported, and confounding from concurrent safety initiatives could not be excluded.
Across three pre- and postimplementation studies, maternal early warning systems generated alerts in a small share of encounters (about 2 percent when reported) and were associated with improvements in response processes (e.g., timely treatment of severe HTN), but effects on maternal morbidity endpoints were inconsistent and difficult to interpret, given substantial risk of confounding and variation in outcome definitions and reporting.
Potential Benefits and Harms
Potential benefits of inpatient maternal early warning systems include earlier recognition of clinical deterioration, more consistent escalation of care, and more timely treatment for conditions such as severe HTN, sepsis, and cardiopulmonary compromise. Across the available implementation studies, these tools were associated with improved process measures, including higher proportions of patients with severe HTN treated within 60 minutes and modest reductions in emergency response calls. One study found a small reduction in SMM, although causal attribution remains uncertain, with a second study showing a potential increase in SMM.
Potential harms of these interventions include inaccurate or unnecessary alerts leading to alert fatigue for clinicians, overtreatment for patients, or both and false reassurance when concerning symptoms or vital sign abnormalities do not meet trigger thresholds. In all three studies, alert volumes were low (approximately 2 percent of encounters), and specificity for the outcomes examined was high (>95 percent), which would likely mitigate some provider overload. Other patient-related harms could include
worsened psychosocial stress, worsened trust with the health system, or both, especially for false positive alerts.
Additional Evidence on Tool Performance and Education
Although not part of the committee’s formal inclusion set (because they focus on predictive performance, perinatal outcomes, or intermediate outcomes rather than maternal cardiovascular morbidity or mortality), several additional studies were noted that further contextualize both inpatient early warning systems and patient-facing educational interventions.
Validation and Performance of Obstetric Early Warning Scores
The sensitivity and specificity of obstetric early warning systems (e.g., Modified Early Obstetric Warning System [MEOWS] and Maternal Early Warning System [MEWS] derivatives) vary widely depending on the outcome studied (e.g., specific morbidities, such as severe HTN, or composite morbidities). The positive and negative predictive values also vary depending on the population studied (higher versus lower probability of the outcome). In general, these systems show moderate to high specificity and low sensitivity. In a prospective cohort of high-risk postpartum women in Finland, a system based on MEOWS criteria demonstrated its highest sensitivity and positive predictive value for PE, with SBP and DBP and heart rate being the strongest predictors of morbidity (Hannola et al., 2021).
A Spanish single-center cohort study evaluating a MEWS system during the first 2 hours after delivery found that it triggered in 6.4 percent of women, with sensitivity of 0.28 and specificity of 0.94 for a potentially fatal disorder (ICU admission, early surgery, or prolonged stay) (Ibáñez-Lorente et al., 2021). A large U.S. cohort study compared several published criteria (MEOWS, MEWS, and MEWT) and concluded that commonly used thresholds have poor sensitivity for major morbidities (hemorrhage, infection, and acute cardiovascular and pulmonary disease), though this can be improved at the expense of specificity (Kern-Goldberger et al., 2023).
Finally, a quality-improvement initiative that combined MEWS with severe HTN safety bundles demonstrated substantial improvements in timely treatment of hypertensive emergencies and elimination of racial disparities in treatment delays. Although the downstream effects on severe morbidity and mortality remained incompletely characterized, the results showed that standardized response pathways can improve important process outcomes (Sims et al., 2025).
These validation studies reinforce the committee’s interpretation that obstetric early warning tools are best conceptualized as high-specificity trigger systems for escalation of care rather than screening tools for a
general population of pregnant women, newly postpartum women, or both. They also highlight that hypertensive and cardiovascular parameters—especially BP and pulse—tend to be among the most informative physiologic indicators.
Patient and Community Education on Urgent Maternal Warning Signs
Beyond the evidence within the formal specifications of this review, a small but growing literature exists on patient-facing education about pregnancy warning signs. The following section provides a few examples, with Figure 4-1 offering a sample UMWS intervention graphic.
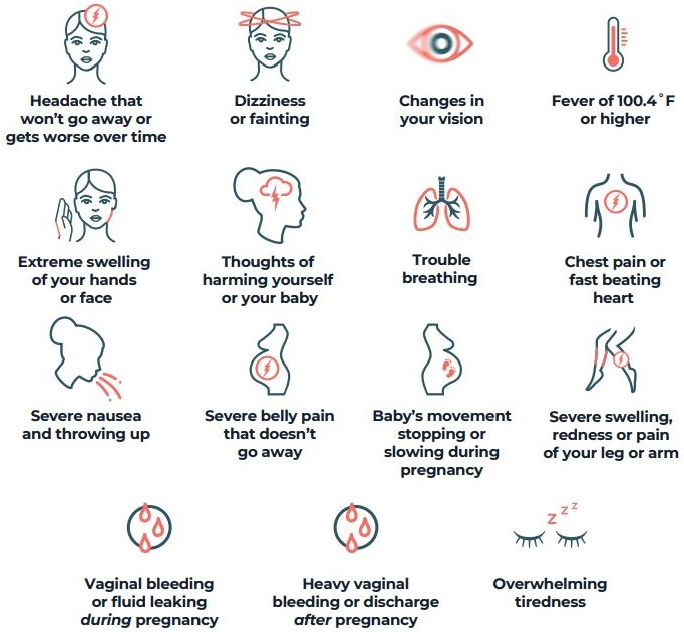
NOTE: The Centers for Disease Control and Prevention’s Hear Her® campaign advises “Be aware of urgent maternal warning signs and symptoms during pregnancy and in the year after delivery; seek medical care immediately if you experience any signs or symptoms that are listed; the symptoms can be a sign of a life-threatening condition.”
SOURCE: CDC, 2024b.
The MAMAACT intervention in Denmark was a cluster randomized effectiveness trial that evaluated a multicomponent intervention that included training midwives in intercultural communication and providing multilingual patient educational materials on pregnancy complications, with the goal of reducing ethnic and social disparities in stillbirth and infant health. It improved aspects of pregnant women’s health literacy and midwives’ health literacy responsiveness; effects on maternal morbidity and mortality were not measured (Rasmussen et al., 2023a). In another study, the intervention was associated with a nonsignificant increase in a neonatal composite outcome, mostly driven by increases in NICU admissions (Rasmussen et al., 2023b).
Several recent interventions have focused explicitly on UMWS. A mixed-methods pilot involving Maryland home visiting programs evaluated an education toolkit comprising a 3-minute video, an illustrated handout listing 15 UMWS, a magnet, and a discussion guide, combined with 1.5 hours of staff training. Home visiting staff reported that the materials were highly acceptable, understandable across diverse client populations, and feasible to use in both in-person and remote visits, though use of individual toolkit components was inconsistent. The study primarily assessed acceptability, feasibility, and perceived impact, and it did not measure maternal morbidity or mortality outcomes (Stierman et al., 2025).
A single-center randomized trial tested a postpartum educational video on maternal mortality warning signs (infection, hemorrhage, HTN disorders, and postpartum depression) versus routine discharge education (White et al., 2023). Both groups improved their knowledge from baseline to post education. The proportion of participants with improved scores did not differ significantly between groups (64.5 versus 50.0 percent), but the video group had slightly higher median posteducation scores and reported higher satisfaction with education. The trial did not assess downstream clinical outcomes.
Evaluations of broader communication initiatives, such as the Centers for Disease Control and Prevention’s Hear Her campaign, suggest that national messaging can increase awareness of UMWS and may influence intentions to seek timely care, but effects on SMM or mortality have not been established (Spencer et al., 2025).
Cost and Cost-Effectiveness
None of the identified studies of MEWS or UMWS interventions reported intervention costs, resource use, or formal cost-effectiveness analyses. Thus, the economic impact of these approaches could not be evaluated.
Implementation Considerations
Implementing inpatient MEWS requires aligning several elements: reliable vital sign acquisition, clear escalation pathways, integration with EHR workflows, and workforce preparation. Programs described in the literature embedded triggers directly into EHR flowsheets, paired them with standardized order sets and response algorithms, and specified who should respond, how quickly, and with what initial evaluation and treatment. Ongoing audit and feedback were central to refining thresholds, minimizing missed events, and maintaining staff engagement.
National resources, such as the Alliance for Innovation on Maternal Health (AIM) MEWS Implementation Resource Kit and Obstetric In Situ Drill Program Manual, emphasize that unit-based simulation and drills—bringing together nurses, obstetric clinicians, anesthesia, and other team members—are key to practicing activation criteria, bedside communication, and role clarity in real clinical environments (AIM, 2022, n.d.-b). State-level initiatives, including those led by perinatal quality collaboratives, such as Texas AIM and California Maternal Quality Care Collaborative (CMQCC), also recommend that multidisciplinary hospital teams implement patient safety bundles for severe HTN, hemorrhage, and sepsis, with technical assistance and collaborative learning that often include simulation-based training (CMQCC, 2026; Texas DSHS, 2025, n.d.). These experiences reinforce that early warning tools and UMWS protocols need to be paired with training, drills, and adequate staffing. Without clear escalation processes and mechanisms to receive needed clinical support in an urgent situation, even accurate alerts may not translate into timely treatment.
For patient-facing UMWS efforts outside of hospital settings, effective implementation will first require additional research to identify strategies that are effective at improving maternal health outcomes. These strategies will likely need to be multicomponent and multidisciplinary, similar to those employed in inpatient settings. Thus, they will need to include effective strategies for diverse forms of community, patient, and clinician education and engagement and built-in methods to quickly escalate care when abnormalities are identified. Involving community members from populations most affected by maternal morbidity and mortality and delays in care for UMWS will likely be important.
Summary and Conclusions
Overall, the strength of evidence is limited regarding the effect of inpatient electronic MEWS, coupled with associated clinical care pathways, on maternal morbidity and mortality. The few available studies, their poor to fair quality, and inconsistent effects on SMM limit conclusions about the
direct effects of MEWS on health outcomes. Across studies, early warning systems appeared to improve some process measures—particularly timeliness of treatment for HTN and sepsis—and, in one setting, were associated with reduced emergency response calls. However, effects on composite morbidity and ICU admissions were variable and difficult to interpret given baseline differences, secular trends, and limited adjustment for confounding.
With respect to outpatient education and patient-facing tools and education, the committee did not identify evidence that interventions reduced maternal cardiovascular morbidity, SMM, or mortality. Existing interventions, such as MAMAACT, home-visiting–based UMWS education toolkits, postpartum educational videos, and the Hear Her campaign, have focused mostly on improving health literacy, knowledge of warning signs, and patient communication with clinicians. These studies provide important proof of concept that UMWS education is acceptable, feasible, and able to improve knowledge and self-reported certainty about how to respond to warning signs, but they do not yet establish causal links to reduced maternal cardiovascular events or deaths.
This gap is notable because state MMRCs repeatedly identify delayed recognition of UMWS by both patients and clinicians as a common, preventable contributor to pregnancy-related deaths and often recommend patient and community education as a prevention strategy. However, these recommendations are supported largely by expert consensus and care review rather than intervention trials. Rigorous evaluations of outpatient and community-based interventions are clearly needed that can reduce delays in seeking care when UMWS are present.
Conclusion 4-3: Evidence is limited that inpatient maternal early warning systems using electronic trigger tools modestly improve process measures such as timely treatment of hypertension and sepsis and may reduce need for emergency on maternity units. Evidence is insufficient to determine whether these systems reduce severe maternal morbidity or mortality. There is no direct evidence that outpatient education, patient self-screening, or improved community awareness of UMWS reduce maternal cardiovascular morbidity, severe maternal morbidity, or mortality.
Research Considerations
Research is needed to evaluate the effectiveness of UMWS screening—in both clinical and community settings—on maternal cardiovascular outcomes, SMM, and mortality. Studies could do the following:
- Strengthen evidence on the effects of MEWS in inpatient settings on health outcomes. Use robust designs (e.g., cluster randomized, stepped wedge, or well-controlled quasiexperimental studies) to assess the effect on cardiovascular morbidity (e.g., hypertensive emergencies, cardiomyopathy, pulmonary embolism), ICU admission, and cardiovascular mortality, while accounting for secular trends and concurrent safety initiatives.
- Develop and evaluate UMWS screening in outpatient, community settings, or both. Design and evaluate patient and family education programs, self-screening checklists, home visiting toolkits, and digital symptom reporting tools that operationalize screening during pregnancy and postpartum, with outcomes that include timely care seeking, use of emergency services, and maternal cardiovascular morbidity and mortality.
- Build on interventions such as MAMAACT and home visiting programs to test whether culturally and linguistically tailored UMWS education can reduce racial, ethnic, and social disparities in delays to care and in maternal outcomes.
- Measure unintended consequences. Evaluate potential harms, such as alert fatigue, overtriage, increased unnecessary ED visits, unnecessary patient anxiety, and barriers to appropriate escalation, for both inpatient warning systems and patient-facing self-screening tools.
STRUCTURED CARDIOVASCULAR RISK ASSESSMENT TOOLS
Overview of the Question and Gap
Cardiovascular screening during pregnancy and the postpartum period has been proposed as a strategy to improve early identification of unrecognized disease. Several structured tools have been developed, including the CMQCC Screening Tool, which has demonstrated promising diagnostic yield in early implementation studies (Blumenthal et al., 2020). In clinical workflows, it is typically implemented as a brief checklist/algorithm of symptoms, signs, or risk factors, with certain responses triggering evaluation (e.g., tests such as electrocardiogram [EKG] and cardiology consults), for CVD. In most published implementations, this screening has been applied universally to pregnant and postpartum patients rather than limited to those with known CVD, with the goal of identifying previously unrecognized conditions. In one EHR-integrated implementation, for example, it was operationalized as about 18 discrete data elements and could be completed in about 30 seconds because most fields autopopulated from routine history and vital signs (Blumenthal et al., 2020; Hameed, 2022).
The algorithm begins with a screen for severely abnormal symptoms requiring urgent evaluation (e.g., dyspnea/reduced exercise tolerance [New York Heart Association class >II], orthopnea, palpitations, dizziness/syncope, or chest pain), paired with standardized vital sign thresholds (e.g., resting heart rate ≥110 beats per minute, SBP ≥140 mmHg, respiratory rate ≥24, oxygen saturation ≤96 percent) and clinical risk factors (e.g., age ≥40, African American race, prepregnancy BMI ≥35, preexisting diabetes, chronic HTN, substance use, or prior chemotherapy). Use of established cardiology terminology—such as New York Heart Association functional classification—may facilitate communication across obstetric and cardiology teams by providing a shared clinical framework. Patients are considered screen positive when at least one symptom occurs with at least one abnormal vital sign and at least one risk factor (or the cumulative score reaches four or greater), which triggers predefined pathways for diagnostic testing (e.g., EKG and B-type natriuretic peptide, or echocardiography) and specialty evaluation (Blumenthal et al., 2020; Hameed, 2022).
Additional screening tools include cardiovascular SMM prediction models (Malhamé et al., 2022), which are multivariable calculators rather than bedside questionnaires. The SMM delivery model incorporates 11 predictor variables (plus interaction terms), and the postpartum model has eight variables, using routinely available clinical/demographic inputs (e.g., HDP, multiple gestation, maternal age ≥40, cardiac lesions/valvular disease, and race and ethnicity) to identify women at elevated risk for acute cardiovascular complications (Malhamé et al., 2021).
Despite growing interest and supportive feasibility data, CVD screening is not widely implemented across U.S. perinatal systems (Hameed et al., 2024, 2025b). Barriers include challenges integrating screening into EHRs, varying institutional workflows, and the need for increased personnel to manage follow-up evaluation.
Therefore, the committee reviewed the question “Does screening with CMQCC Cardiovascular Disease in Pregnancy toolkit or Malhamé et al.’s CVD risk assessment tools in pregnancy and postpartum improve identification of women with previously unrecognized CVD and improve cardiovascular health outcomes?”
Summary of the Evidence
The initial literature search yielded 72 records with publication dates from January 2010 to October 2025 that were screened at the abstract level. Articles deemed eligible for full-text review included those describing studies conducted in the United States and other very high–income UN countries and an outcome relevant to the committee question. The committee identified 24 as potentially relevant and moved to full-text review.
Six articles met all inclusion criteria, with the most common reasons for exclusion being wrong intervention. The committee conducted risk-of-bias assessments and data extraction. It identified two additional narrative reviews and expert opinion pieces and used them to provide background and context. It also screened the reference lists to ensure it did not miss any relevant intervention studies.
The evidence base supporting screening includes (see Table 4-6)
- A prospective implementation study (fair quality) (Blumenthal et al., 2020),
- Large cohort analyses of universal risk assessment (fair quality) (Hameed et al., 2023b, 2025b), and
- Validated risk prediction models for cardiovascular SMM (fair quality) (Malhamé et al., 2021, 2022).
The committee also reviewed clinical rationales and expert recommendations (Chambers et al., 2022) and a study examining predictive performance of multiple tools (Thakkar et al., 2023). Collectively, these studies provide consistent evidence of feasibility, diagnostic yield, and effective identification of high-risk women, but none evaluate whether screening reduces maternal cardiovascular morbidity or mortality.
Key Findings from Implementation Studies
In one study (fair quality), CMQCC screening at two medical centers identified cardiovascular risk in 8 percent of pregnant and postpartum women (N = 846 screened, N = 69 positive). Of the screen-positive patients who completed sufficient follow-up, 30 percent (N = 12) were diagnosed with confirmed CVD (Blumenthal et al., 2020). Predictors of positive screening included elevated systolic BP, oxygen saturation ≤96 percent, dyspnea, chronic HTN, diabetes, and African American race. Completion of follow-up among screen-positive women varied by site, raising questions about real-world diagnostic yield.
Evidence from Large Network Cohorts
A large network cohort study (fair quality) evaluated EHR-embedded CMQCC screening across 23 sites (N = 14,958) (Hameed et al., 2023b). Key findings include risk assessment completion rates of 57–99 percent, with 100 percent in systems with EHR hard stops; higher completion correlated with increased detection of cardiovascular conditions; and clinicians reporting workflow barriers but perceiving overall value in detection. In an analysis of 31,232 patients (Hameed et al., 2025b), standardized CMQCC
TABLE 4-6 Summary of Evidence on Cardiovascular Disease Screening in Pregnancy and Postpartuma
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Blumenthal et al., 2020 American Journal of Perinatology Reports | Prospective implementation; CMQCC CVD screening algorithm in two academic medical centers, U.S. | N = 846 screened (CA: 648; NY: 198) screen-positive N = 69 Reproductive period: PN, PP | CMQCC CV disease screening algorithm | Screen-positive rate; confirmed CVD; predictors; follow-up completion | Screen-positive 8% (5% in CA; 19% in NY); among those with follow-up, 30% with confirmed CVD Predictors: O2 saturation ≤96%, SBP ≥140, dyspnea, African American race, chronic HTN, diabetes; screening able to identify unrecognized CVD | Fair |
| Malhamé et al., 2020 BJOG | Retrospective cohort; obstetric teaching hospital, U.S. | N = 89,681 delivery hospitalizations (2007–2017) Reproductive period: Delivery → 6 weeks PP | Development and internal validation of two prediction models (delivery CSMM and postpartum CSMM) | CSMM | CSMM 5/1,000 deliveries (delivery 4/1,000; PP 1/1,000), driven by severe HTN and pulmonary edema/acute HF Models with excellent discrimination (AUC 0.87 delivery; 0.85 PP) Strongest predictors: gHTN, cHTN, multiple gestation, cardiac lesions, age ≥40; for PP model: severe PE, non-Hispanic Black race, cHTN/gHTN, age ≥40 | Fair |
| Malhamé et al., 2022b Canadian Journal of Cardiology | Retrospective cohort; academic obstetrics hospital, U.S. | N = 4,171 with PE; N = 334 with acute CV morbidity Reproductive period: Delivery → 6 weeks PP | Development and internal validation of a risk prediction model | Acute CV morbidity (pulmonary edema/acute HF, difficult-to-control HTN, arrhythmia, cerebrovascular events) | Acute CV morbidity 8%; predominantly severe HTN and pulmonary edema Prediction model AUC 0.72; earlier GA and older age strongest predictors; model internally validated | Fair |
| Hameed et al., 2023b JACC: Advances | Prospective implementation across 3 large hospital networks (23 sites), CA & TN, U.S. | N = 14,958 PN/PP patients with ≥1 OB visit; prior CVD excluded Reproductive period: PN, PP | EHR-embedded (Epic/Cerner systems) CMQCC CVD risk assessment tool | Completion of risk assessment; follow-up of screen-positive patients | Risk assessment completion 57–99% across networks; follow-up 56–73% Sites with EHR hard stops with 100% completion Higher screening correlating with CVD detection Clinicians reporting workflow barriers but overall positive impact | Fair |
| Author/Year/Journal | Study Type/Setting | Population Description | Intervention/Comparison | Key Outcomes | Main Findings | Quality Ratingb |
|---|---|---|---|---|---|---|
| Hameed et al., 2025a,b American Journal of Obstetrics & Gynecology Maternal-Fetal Medicine | Retrospective analysis of prospectively implemented CMQCC algorithm across 3 large hospital networks, U.S. | N = 31,232 PN or PP Reproductive period: PN→ 6 weeks PP | Standardized CMQCC CVD risk assessment vs. clinician judgment–based testing | Abnormal cardiac test yield (BNP, EKG, echo); odds of abnormal testing | Screened women ↑ abnormal testing (6.9% vs. 4.2%); risk-positive women 23.4 percent abnormal tests vs. 6.6 percent risk negative Among risk-positive patients: 27% abnormal-test → CVD diagnosis vs. 14% normal test | Fair |
NOTES: a Studies are listed by publication year (oldest first), then alphabetically by first author within each year. b Quality rating was assessed using the National Heart, Lung, and Blood Institute Quality Assessment Tools. Ratings: Good = low risk of bias; Fair = some concerns; Poor = serious risk of bias. AUC = area under the curve; BNP = brain natriuretic peptide; cHTN = chronic hypertension; CMQCC = California Maternal Quality Care Collaborative; CSMM = cardiovascular severe maternal morbidity; CV = cardiovascular; CVD = cardiovascular disease; ECG/EKG = electrocardiogram; EHR = electronic health record; GA = gestational age; gHTN = gestational hypertension; HF = heart failure; HTN = hypertension; OB = obstetric/obstetric care; PE = preeclampsia; PN = prenatal; PP = postpartum; SBP = systolic blood pressure.
SOURCES: Blumenthal et al., 2020; Hameed et al., 2023b, 2025a,b; Malhamé et al., 2021, 2022.
screening found increased detection of abnormal cardiac testing compared with clinician judgment–based testing (6.9 versus. 4.2 percent; OR 1.69), yielding particularly high diagnostic rates among screen-positive patients (abnormal tests in 23.4 versus 6.6 percent). However, neither study assessed whether screening improved clinical outcomes, such as improving timely diagnosis of management of cardiomyopathy, hypertensive crises, or SMM.
Prediction Models
One group developed and internally validated cardiovascular severe maternal morbidity prediction models, reporting AUCs ranging from 0.72 to 0.87 across delivery, postpartum, and preeclampsia-specific models (Malhamé et al., 2021, 2022). These help identify women at high risk for acute cardiovascular events but do not directly evaluate CMQCC’s screening workflow or assess whether screening reduces adverse outcomes.
Strengths and Limitations
The evidence supporting the CMQCC CVD screening tool has several notable strengths. Findings across multiple large and diverse cohorts consistently demonstrate that screening in pregnancy and postpartum is feasible to implement and successfully identifies women with unrecognized cardiovascular risk or disease. The predictive models developed in complementary work show good discrimination, reinforcing the potential of structured tools to identify women at highest risk of SMM (Malhamé et al., 2021; Malhamé et al., 2022). Studies also indicate that integrating screening tools into EHR systems improves completion rates, and clinicians generally report that screening enhances awareness of cardiovascular risk.
However, important limitations temper the conclusions that can be drawn from this evidence base. No RCTs have evaluated CMQCC screening, and, crucially, no studies have examined whether it improves maternal cardiovascular outcomes or morbidity or prevents severe cardiac events. The studies focus largely on diagnostic yield and process outcomes, leaving substantial gaps regarding clinical effectiveness. Implementation strategies vary widely across sites, with differences in screening thresholds, follow-up procedures, and resource availability, making it difficult to determine which components are most effective. Follow-up of screen-positive patients is inconsistent across studies, potentially limiting the true diagnostic yield and raising concerns that some women may not receive timely further evaluation. Finally, evidence on patient experience, cost-effectiveness, and the potential to lessen or widen gaps in health outcomes is limited, underscoring the need for more rigorous and comprehensive evaluation.
Timing and Frequency
Several expert commentaries recommend incorporating cardiovascular risk assessment early in pregnancy to facilitate timely identification of underlying disease (Chambers et al., 2022). Screening during the postpartum period has also been proposed, given the elevated risk of cardiomyopathy and hypertensive events that are most prevalent in the first 6 weeks, but risk may persist up to 1 year (Hameed et al., 2025b). Interpregnancy screening has been suggested to support long-term cardiovascular prevention and risk reduction, although evidence is based primarily on expert opinion rather than empirical data.
Potential Benefits and Harms
Screening consistently identifies women with previously unrecognized structural heart disease (e.g., cardiomyopathy, valvular disease), arrhythmias, chronic HTN, or concerning cardiopulmonary symptoms warranting further evaluation. Early identification may allow timely evaluation, referral, and treatment, with the goal of decreasing maternal morbidity and mortality. It may also empower patients by increasing knowledge regarding long-term cardiovascular prevention. If paired with effective interventions, screening could reduce maternal and infant morbidity through timely disease recognition.
Large cohort studies report diagnostic yields of 6–30 percent among screen-positive women, depending on the population and completion of follow-up (Blumenthal et al., 2020; Hameed et al., 2025b; Malhamé et al., 2021). This demonstrates significant detection of actionable cardiovascular findings (Hameed et al., 2024, 2025a,b).
Potential harms include false positive screens leading to unnecessary testing, increased patient anxiety, variable follow-up quality (a positive screen may not lead to further care), and resource strain on cardiology services. Because screening is typically universal, even modest false positive rates may result in increased diagnostic testing and specialist referral, with implications for cost, capacity, and equitable access to follow-up. The burden required to participate in screening may be disproportionately high among underserved women with limited transportation, child care, or access to digital tools used in telehealth-enabled workflows.
Cost and Cost-Effectiveness
Formal cost-effectiveness analyses are lacking. CVD screening introduces diagnostic and provider costs. However, preventing SMM and emergencies may substantially offset these costs (Hameed et al., 2024, 2025b).
Telehealth-enabled screening may further improve efficiency, depending on payer coverage and patient access.
Population Considerations
CVD–related SMM disproportionately affects Black and Native American and Alaska Native populations (Hameed et al., 2024). Universal screening may reduce disparities by standardizing risk assessment rather than relying on clinician judgment alone, whereas inconsistent or selective implementation may worsen them. However, no studies directly assess whether screening reduces differences in outcomes, and follow-up barriers may be greater for underserved populations. Screening should recognize that race is a social construct and that non-Hispanic Black women often serve as a proxy for marginalized populations in clinical risk models (NASEM, 2019, 2022).
Implementation Considerations
Statewide implementation in California is both feasible and well received by clinicians when structured CVD screening tools are used (Blumenthal et al., 2020). Implementation requires clinician training, interdisciplinary workflow integration, and alignment with quality measures (Hameed et al., 2023a). Challenges include resource constraints, variable infrastructure, limitations in digital access for telehealth, and coordination gaps.
Standardized cardiovascular risk assessment during pregnancy and the postpartum period has also been incorporated into emerging national quality measurement efforts, including Centers for Medicare & Medicaid Services Merit-based Incentive Payment System Measure #496 and the Partnership for Quality Measurement endorsed CVD Risk Assessment measure (CBD #4715) (AIM, n.d.-a; Partnership for Quality Measurement, 2025). In addition, cardiac condition screening is included in the Alliance for Innovation on Maternal Health (AIM)/ACOG Consensus Bundle on Cardiac Conditions in Obstetric Care (AIM, n.d.-a). These endorsements reflect growing national recognition of the importance of systematic CVD risk assessment, even as evidence on clinical outcome impact continues to evolve.
Summary and Conclusions
The committee finds that structured cardiovascular screening tools, such as the CMQCC algorithm, offer a promising approach to identifying pregnant and postpartum women at risk for cardiovascular morbidity, with consistent evidence demonstrating feasibility, diagnostic yield,
and improved detection of unrecognized disease. However, the committee also recognizes that the evidence base is limited to observational and implementation studies and does not establish whether screening improves maternal cardiovascular outcomes, reduces SMM, or prevents mortality. No studies directly evaluate clinical effectiveness, and follow-up after positive screens varies widely across settings, raising concerns about equitable care pathways.
Given the compelling clinical rationale, consistent diagnostic yield, and alignment with national maternal safety priorities, structured cardiovascular screening may represent a valuable preventive strategy if implemented with standardized protocols and clear follow-up pathways. However, additional evaluation is needed to determine whether screening leads to reductions in cardiovascular morbidity, mortality, and disparities.
In weighing the evidence, the committee considered several factors: consistent diagnostic yield across diverse settings, the serious and potentially life-threatening nature of unrecognized cardiovascular conditions during pregnancy and postpartum, feasibility of integration into existing workflows, and alignment with national maternal safety initiatives. At the same time, it recognized important uncertainties, including the absence of demonstrated reductions in maternal morbidity or mortality, the potential for false positives, resource strain, and uneven follow-up. Given these tradeoffs, the committee characterizes structured cardiovascular screening as a promising preventive strategy that warrants ongoing evaluation of clinical outcomes; any implementation would need careful attention to follow-up and resource capacity, rather than unqualified universal adoption.
Conclusion 4-4: Evidence is moderate that cardiovascular disease screening tools—such as the California Maternal Quality Care Collaborative algorithm—identify pregnant and postpartum women with previously unrecognized cardiovascular disease or elevated cardiovascular risk. However, evidence is insufficient on whether screening improves maternal cardiovascular outcomes.
Research Considerations
Rigorous research is needed to evaluate the clinical effectiveness of universal CVD screening during pregnancy and postpartum. Future studies need to include adequately powered prospective controlled trials or nonrandomized studies of interventions with appropriate control groups that (1) assess whether screening improves maternal cardiovascular outcomes, including cardiomyopathy, hypertensive complications, and SMM; (2) identify optimal screening thresholds, components, and follow-up pathways;
and (3) examine implementation across diverse care settings, including the effect of workflow integration, clinician training, and follow-up capacity. Research that evaluates the effectiveness of such screening in different populations is also needed, especially for groups disproportionately affected by cardiovascular morbidity. Formal cost-effectiveness analyses are needed to elucidate the feasibility and sustainability of systemwide screening initiatives.
LIFE’S ESSENTIAL 8
Overview of the Question and Gap
The committee posed the following question: “For women of reproductive age at increased risk of CVD, does comprehensive screening and intervention for risk factors underlying cardiovascular health, specifically, using the Life’s Essential 8 screening tool (LE8), reduce the risk of pregnancy-related cardiovascular morbidity and mortality?” The committee designed this question broadly to address the outcomes related to comprehensive cardiometabolic health screening across the prepregnancy, pregnancy, postpartum, and interpregnancy periods.
Comprehensive screening and the resulting interventions might hold promise for addressing clinical service gaps that underlie pregnancy-related cardiovascular morbidity and mortality. The committee viewed LE8 as a potential unifying framework to address the fragmented nature of cardiovascular risk screening in a single tool. However, research has not yet established its clinical utility in pregnancy-related care. LE8, as defined by the AHA, comprises eight domains—four behavioral (diet, physical activity, nicotine exposure, and sleep health) and four health (healthy weight, blood lipids, blood glucose, and BP) factors. Each component is measured on a scale of 0–100 based on a questionnaire (for behaviors), laboratory test, or biometric measurement. Clinicians can calculate an overall cardiovascular health score by averaging the component scores. Higher scores on the LE8 indicate better cardiovascular health, as defined by the AHA.
Although seven of these eight factors (except sleep health) are addressed separately in recommendations by USPSTF, the Women’s Preventive Services Initiative (WPSI), or Bright Futures, the committee was specifically interested in whether routine use of a comprehensive screening tool before, during, or after pregnancy could reduce pregnancy-related cardiovascular mortality and morbidity. LE8 is a cardiovascular health assessment framework rather than a specific behavioral intervention; consistent with the committee’s focus on clinical preventive services, this review did not evaluate screening, treatment, or individual lifestyle or weight-loss interventions already recommended by USPSTF and WPSI but instead examined whether
use of a comprehensive assessment framework could improve identification, coordination, and follow-up of cardiovascular risk factors across the reproductive continuum. In formulating this question, the committee assumed implicitly that if screening identified problems in one or more factors, effective intervention would be initiated.
Summary of the Evidence
The preliminary literature search on LE8 yielded 40 records with publication dates from January 2010 to August 2025. Of the articles screened at the abstract level, none were identified as potentially relevant and moved to full-text review (reasons for exclusion included wrong population or wrong intervention). The committee then initiated another literature search with a specific focus on sleep health as a component, since it does not have a clinical preventive service in place as the other seven components do. This search yielded 39 results, 21 of which were identified as potentially relevant and moved to full-text review; 4 articles met inclusion criteria, with the most common reasons for exclusion being wrong population, wrong intervention, or no relevant outcomes. These articles were all narrative reviews and expert opinion pieces, so the committee did not conduct an evidence synthesis. Rather, it used these articles to provide background and context and screened the reference lists to ensure it did not miss any relevant intervention studies. The committee conducted an additional search to identify articles that reviewed LE8 and cardiovascular outcomes in general to inform the discussion in the following section.
One article published after the initial search found that among women with APOs, higher LE8 scores were associated with lower incidence of CVD events over a median of 13.5 years of follow-up (Chen et al., 2025). In addition, for women with better LE8 scores, having had a prior APO was not associated with long-term CVD risk, suggesting that better status on LE8 factors may attenuate the excess risk associated with APOs.
Overall, the committee concluded that direct evidence is lacking regarding the effectiveness of cardiovascular health assessment using LE8 among women of reproductive age to assess for and prevent pregnancy-related cardiovascular morbidity and mortality. Despite this, robust data demonstrate associations between cardiometabolic risk factors that LE8 screens for, APOs, and elevated long-term cardiovascular risk. For some women, this increased risk may manifest in the perinatal period, so it is important to emphasize this relationship and acknowledge that recommendations from USPSTF and WPSI regarding appropriate intervention for seven of the eight factors in LE8 (except sleep health) apply to many women in the prepregnancy, prenatal, postpartum, and interpregnancy periods.
Substantial, consistent evidence demonstrates that women with APOs experience elevated long-term risk of CVD events. APOs can include HDP, gestational diabetes mellitus (GDM), placental abruption, stillbirth, preterm delivery, and delivering an SGA infant. A 2019 systematic review that included 83 studies found that CVD risk was elevated in women with gestational HTN, preeclampsia, placental abruption, preterm birth, GDM, and stillbirth (Grandi et al., 2019). A 2021 AHA scientific statement characterized the body of evidence linking APOs and later CVD risk as strong (strength of evidence A) (Parikh et al., 2021).
For example, a long-term cohort study found that women with recurrent HDP had markedly increased risk of mortality from all causes (hazard ratio [HR] 2.04), ischemic heart disease (HR 3.3), and stroke (HR 5.1) (Theilen et al., 2018). APOs are also associated with increased risk of adverse cardiovascular outcomes, including early myocardial infarction and coronary artery disease (Vaughan et al., 2024), stroke (Canoy et al., 2016; Grandi et al., 2019; Riise et al., 2018), peripheral vascular disease, and heart failure (Canoy et al., 2016; Grandi et al., 2019; Riise et al., 2018).
Women with a history of APOs also tend to have elevated rates of cardiovascular risk factors, such as HTN, dyslipidemia, hyperglycemia, and overweight or obesity—risk factors encompassed within LE8. Some experts have posited that APOs are risk enhancers that potentiate the risks posed by traditional cardiovascular risk factors (Chen et al., 2025). Because APOs share many underlying risk pathways with LE8 components, the LE8 framework may provide a structured approach for identifying and modifying these shared factors during the reproductive years.
USPSTF and WPSI recommend specific interventions related to LE8 factors for adults with CVD risk factors. Table 4-7 shows which aspects of AHAs LE8 are covered by the USPSTF and WPSI recommendations (all WPSI and Grade A and B USPSTF services are covered under the Affordable Care Act).
Most recommendations related to LE8 factors apply to either all women or to those with APOs because they have elevated cardiovascular risk. Tobacco use cessation and HTN screening are recommended for all adults. Regarding nicotine replacement therapy (NRT) for pregnant women, USPSTF in 2021 stated that evidence is insufficient to assess the balance of benefits and harms (USPSTF, 2021d). This is largely due to mixed evidence of efficacy in trials of NRT, mostly attributable to poor adherence and potentially increased nicotine metabolism in pregnancy rather than evidence of harm (ACOG, 2020b). In a motivated patient with a clear plan to quit, pharmacotherapy remains an option with potential benefits (ACOG, 2020b).
Although direct evidence of the safety of NRT in pregnancy is lacking, observational data provide some reassurance regarding low risk of harm, with several meta-analyses demonstrating no evidence of association with
TABLE 4-7 Aspects of AHAs Life’s Essential 8 Covered by USPSTF and WPSI Recommendations
| LE8 Category | Relevant USPSTF Recommendation(s)a | Relevant WPSI Recommendation(s) |
|---|---|---|
| Diet | Behavioral counseling to promote a healthy diet and physical activity for adults with CVD risk factorsc—Grade B. Adults without risk factors—Grade C. Applies across the lifespan (USPSTF, 2020a, 2022a). | Counseling to promote a healthy diet and physical activity for women and girls with overweight/obesity and additional CVD risk factors (e.g., HTN, dyslipidemia, abnormal glucose). Applies across the lifespan (WPSI, 2025). |
| Physical Activity | Same counseling recommendations as for diet (with CVD risk factorsb—Grade B; without—Grade C) (USPSTF, 2020a, 2022a). | Same as diet: Counseling to promote physical activity for women and girls with overweight/obesity and other CVD risk factors (WPSI, 2025). |
| Nicotine Exposure | Tobacco use cessation interventions (adults, including pregnant women)—Grade A. Pharmacotherapy (nonpregnant adults)—Grade A. E-cigarettes for cessation—I statement. Youth prevention—Grade B (USPSTF, 2020b, 2021d). | Tobacco use screening and counseling for all women and girls, including pregnant women (WPSI, 2025). |
| Sleep Health | Obstructive Sleep Apnea screening in asymptomatic adults—I statement (USPSTF, 2022b). | Not addressed as a separate preventive service by WPSI. |
| Healthy Weight (BMI) | Adults with BMI ≥30—intensive, multicomponent behavioral interventions (Grade B). Children and adolescents with high BMI—behavioral interventions (Grade B). Note: adult screening statement has an update in process (USPSTF, 2018, 2024). | Screening for obesity and counseling for behavioral interventions for all women and girls aged 13+ (WPSI, 2025). |
| Blood Lipids | Statin use for primary prevention—adults 40–75 with ≥1 risk factor (e.g., dyslipidemia, diabetes, HTN, or smoking) and 10-year CVD risk ≥10 percent (Grade B); selectively offer at 7.5–<10 percent (Grade C); insufficient evidence for adults ≥76 y (I). The most recent USPSTF recommendation to screen adults for lipid disorders was in 2016; this received an A or B recommendation depending on age and risk factors and has been archived because it is being re-evaluated (USPSTF, 2022c). | Lipid screening for women and girls aged 13–17 with familial dyslipidemia, risk factors, or high-risk conditions; adults as indicated (WPSI, 2025). |
| LE8 Category | Relevant USPSTF Recommendation(s)a | Relevant WPSI Recommendation(s) |
|---|---|---|
| Blood Glucose | Prediabetes & type 2 diabetes screening—adults 35–70 with overweight/obesity (Grade B). GDM screening—B at ≥24 weeks; I before 24 weeks (USPSTF, 2021a,c). | Screening for diabetes after pregnancy for those with prior GDM; screening for women with overweight/obesity and additional risk factors (WPSI, 2025). |
| Blood Pressure | HTN screening in adults—Grade A. HDPs screening—Grade B (USPSTF, 2021b, 2023). | Screening for HDPs; general BP screening for all adults (WPSI, 2025). |
NOTES: a Grades indicate the strength of recommendation (A, B, C, or I); see Chapter 1 section on the USPSTF for more information. b For diet and physical activity counseling, UPSPTF defines CVD risk factors as having one or more of the following: (1) HTN or elevated BP; (2) dyslipidemia; (3) mixed or multiple risk factors, such as metabolic syndrome or estimated 10-year CVD risk of >7.5 percent. AHA = American Heart Association; BMI = body mass index; CVD = cardiovascular disease; GDM = gestational diabetes mellitus; HDP = hypertensive disorder of pregnancy; HTN = hypertension; USPSTF = U.S. Preventive Services Task Force; WPSI = Women’s Preventive Services Initiative.
congenital anomalies, preterm birth, stillbirth, early-pregnancy loss, low birth weight, NICU admission, or neonatal death (Claire et al., 2020; Taylor et al., 2021; Tran et al., 2025). Smaller trials suggest pregnant women who successfully quit smoking while using nicotine replacements have a decrease in overall cotinine exposure and a small increase in birth weight (Pesola et al., 2024).
USPSTF recommends statins for primary prevention of CVD (assumes lipid screening is conducted) in adults aged 40–75 with one or more CVD risk factors and 10-year risk of cardiovascular event of 10 percent or greater (grade B) or 7.5–<10 percent (grade C). Screening for lipid disorders in children and adolescents received an I statement (insufficient evidence). USPSTF does not directly address lipid screening in adults younger than 40 or adults 40+ without any CVD risk factors. Behavioral counseling to promote a healthy diet and physical activity is recommended for adults with cardiovascular risk factors.
USPSTF recommends blood glucose screening for GDM at 24 weeks or after. Nonpregnant adults aged 35–70 with BMI ≥30 (overweight) are recommended to screen for diabetes or prediabetes. USPSTF recommends behavior counseling interventions for optimal weight and preventing excess weight gain in pregnancy. All adults with BMI ≥30 should be offered intensive, multicomponent behavioral interventions. Thus, these two recommendations apply to women with high BMI, with some but not all women with APOs falling in this group. As context, anecdotal information suggests that
some institutions now screen for preexisting diabetes at the first prenatal visit with hemoglobin A1c either universally or for anyone with risk factors (e.g., a history of APOs or GDM).
Sleep health remains an underaddressed domain. USPSTF stated that evidence is insufficient to recommend for or against screening asymptomatic adults for obstructive sleep apnea, and WPSI does not comment on this topic. However, a reasonable body of evidence demonstrates that sleep-disordered breathing has an independent association with HDP and GDM (Facco et al., 2017; Lu et al., 2021; Rice et al., 2023; Stajić et al., 2022; Tantrakul et al., 2023). The committee’s literature search for studies of screening or interventions to promote sleep health as a means to specifically prevent adverse cardiovascular outcomes in women identified four relevant articles, which were narrative review and expert opinion, and the committee used them as background and context. A broader search for studies of interventions to promote sleep health and reduce APOs yielded several studies, including an RCT of 193 pregnant women at high risk of obstructive sleep apnea (Kalkhoff et al., 2022). This trial evaluated sleep study surveillance, with autoregulated positive airway therapy given to those with sleep apnea. The intervention did not decrease composite APOs or hospital costs, although the small sample size and poor adherence precluded a definitive conclusion. Among women already diagnosed with obstructive sleep apnea, one systematic review and meta-analysis of continuous positive airway pressure treatment in pregnancy found a 30–35 percent risk reduction in HDP, across all age and BMI categories (Lee et al., 2024). The committee found that evidence on this topic was insufficient to support a finding or conclusion. However, it finds that sleep is an underresearched but potentially valuable screening opportunity.
Summary and Conclusions
Women with APOs are at elevated cardiovascular risk, yet evidence directly evaluating comprehensive screening and intervention of cardiovascular risk factors using LE8 to prevent pregnancy-related cardiovascular morbidity and mortality is lacking. The data are limited to observational studies showing that higher LE8 scores are associated with lower long-term CVD risk among women with prior APOs and that LE8 factors and APOs share common cardiometabolic pathways. The committee did not identify any studies that evaluated LE8-guided screening or interventions during the prepregnancy, pregnancy, postpartum, or interpregnancy periods.
USPSTF and WPSI recommend that adults with elevated cardiovascular risk, which would include many women with APOs, receive appropriate intervention to promote healthy diet and physical activity. USPSTF also
recommends that all adults, which would include women of reproductive age, receive screening for HTN, lipid disorders, and, when appropriate, tobacco use cessation interventions.
The committee concludes that continued effort should focus on ensuring that women with APOs receive recommended screenings and interventions for the LE8 risk factors. Although LE8 itself has not been validated as a clinical screening tool in reproductive-age or postpartum populations, it may offer a promising integrative framework to promote consistent, comprehensive assessment and coordination of cardiovascular risk management across reproductive care settings. In particular, the utility of screening for sleep health and sleep-disordered breathing in pregnancy is understudied. Identifying women who could benefit from treatment of the latter might reduce HDP and their downstream morbidity and mortality. More research is needed.
Conclusion 4-5: Evidence is insufficient on whether using the Life’s Essential 8 as a comprehensive clinical screening and management framework for women of reproductive age reduces pregnancy-related cardiovascular morbidity or mortality. Nevertheless, strong evidence supports screening and treatment for many of its specific components (e.g., hypertension, dyslipidemia, diabetes, tobacco use, and obesity) in adults with elevated cardiovascular risk, including many women with adverse pregnancy outcomes, consistent with current U.S. Preventive Services Task Force and Women’s Preventive Services Initiative recommendations.
Research Considerations
Priority areas for research related to LE8 include domains where the evidence is underdeveloped, such as whether interventions to address sleep-disordered breathing in pregnancy improve health or intermediate outcomes. Research would be useful to determine whether using LE8 or any other tool for comprehensive cardiovascular risk assessment improves outcomes beyond the current approach of using screening and management recommendations separately for each risk factor. Additional research is also needed to develop and test lifestyle interventions tailored to women with pregnancy-related HTN or other APOs, including strategies to reduce BP and long-term cardiovascular risk in the postpartum period. Studies could include (1) validation of LE8 scoring and thresholds in reproductive-age and postpartum populations, including those with APOs; and (2) pragmatic or stepped-wedge trials comparing LE8-based comprehensive risk assessment plus structured follow-up against usual care, with outcomes such as risk-factor control, recurrent APOs, and intermediate cardiovascular
endpoints. Implementation-focused research could evaluate how LE8 can be integrated into EHRs and care workflows and whether its use helps close gaps in cardiovascular risk identification and management for populations at highest risk.
EVIDENCE REVIEW, PART 2
Chapter 5 contains the second portion of the committee’s evidence review on Care Delivery and Supportive Services and a summary of its review from both Chapters 4 and 5.
REFERENCES
Abalos, E., L. Duley, D. W. Steyn, and C. Gialdini. 2018. Antihypertensive drug therapy for mild to moderate hypertension during pregnancy. Cochrane Database of Systematic Reviews 10(10):CD002252. https://doi.org/10.1002/14651858.CD002252.pub4.
Abe, M., Y. Shinohara, N. Arata, H. Metoki, A. Fukami, H. Arima, and A. Mito. 2025. Blood pressure-lowering treatment for pregnant women with non-severe hypertension: A systematic review and meta-analysis. Hypertension Research 48(8):2152–2162. https://doi.org/10.1038/s41440-025-02239-3.
ACOG (American College of Obstetricians and Gynecologists). 2018. ACOG committee opinion no. 736: Optimizing postpartum care. Obstetrics & Gynecology 131(5):e140–e150. https://doi.org/131(5)10.1097/AOG.0000000000002633.
ACOG. 2019. ACOG practice bulletin no. 203: Chronic hypertension in pregnancy. Obstetrics & Gynecology 133(1):e26–e50. https://doi.org/10.1097/AOG.0000000000003020.
ACOG. 2020a. ACOG practice bulletin no. 222: Gestational hypertension and preeclampsia. Obstetrics & Gynecology 135(6):e237–e260. https://doi.org/10.1097/AOG.0000000000003891
ACOG. 2020b. Tobacco and nicotine cessation during pregnancy. Committee opinion no. 807. 135:e221–229. https://doi.org/10.1097/AOG.0000000000003822.
ACOG, A. J. Kaimal, M. Gandhi, C. M. Pettker, and H. Simhan. 2025. Clinical guidance for the integration of the findings of the Chronic Hypertension and Pregnancy (CHAP) study. https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2022/04/clinical-guidance-for-the-integration-of-the-findings-of-the-chronic-hypertension-and-pregnancy-chap-study (accessed December 26, 2025).
ACOG, A. Stuebe, T. Auguste, and M. Gulati. 2018. ACOG committee opinion no. 736: Optimizing postpartum care. Obstetrics & Gynecology 131(5):e140–e150. https://doi.org/10.1097/AOG.0000000000002633.
Aderibigbe, O. A., D. N. Hackney, A. C. Ranzini, and J. R. Lappen. 2023. Tight vs. liberal control of mild postpartum hypertension: A randomized controlled trial. American Journal of Obstetrics & Gynecology MFM 5(2):100818. https://doi.org/10.1016/j.ajogmf.2022.100818.
Ahmed, R. J., A. Gafni, E. K. Hutton, Z. J. Hu, E. Pullenayegum, P. von Dadelszen, E. Rey, S. Ross, E. Asztalos, K. E. Murphy, J. Menzies, J. J. Sanchez, W. Ganzevoort, M. Helewa, S. K. Lee, T. Lee, A. G. Logan, J.-M. Moutquin, J. Singer, J. G. Thornton, R. Welch, and L. A. Magee, for the CHIPS Trial Collaborative Group. 2016. The cost implications of less tight versus tight control of hypertension in pregnancy (CHIPS trial). Hypertension 68(4):1049–1055. https://doi.org/10.1161/HYPERTENSIONAHA.116.07466.
AIM (Alliance for Innovation on Maternal Health). 2022. Obstetric in-Situ Drill Program Manual. https://saferbirth.org/wp-content/uploads/FINAL_AIM_ObstetricInSituDrill-ProgramManual.pdf (accessed December 31, 2025).
AIM. n.d.-a. Cardiac Conditions in Obstetric Care. https://saferbirth.org/psbs/cardiac-conditions-in-obstetric-care/ (accessed February 17, 2026).
AIM. n.d.-b. Maternal Early Warning System Implementation Resource Kit. https://saferbirth.org/wp-content/uploads/FINAL_AIM_MEWSIRK.pdf?utm (accessed December 31, 2025).
Amro, F. H., K. C. Smith, S. S. Hashmi, M. S. Barratt, R. Carlson, K. M. Sankey, M. F. Bartal, S. C. Blackwell, S. P. Chauhan, and B. M. Sibai. 2024. Well-child visits for early detection and management of maternal postpartum hypertensive disorders. JAMA Network Open 7(6):e2416844. https://doi.org/10.1001/jamanetworkopen.2024.16844.
Ankumah, N.-A., J. Cantu, V. Jauk, J. Biggio, J. Hauth, W. Andrews, and A. T. N. Tita. 2014. Risk of adverse pregnancy outcomes in women with mild chronic hypertension before 20 weeks of gestation. Obstetrics & Gynecology 123(5):966–972. https://doi.org/10.1097/AOG.0000000000000205.
Arkerson, B. J., M. M. Finneran, S. R. Harris, J. Schnorr, E. R. McElwee, L. Demosthenes, and R. Sawyer. 2023. Remote monitoring compared with in-office surveillance of blood pressure in patients with pregnancy-related hypertension: A randomized controlled trial. Obstetrics & Gynecology 142(4):855–861. https://doi.org/10.1097/AOG.0000000000005327.
Attanasio, L. B., B. L. Ranchoff, M. I. Cooper, and K. H. Geissler. 2022. Postpartum visit attendance in the United States: A systematic review. Women’s Health Issues 32(4):369–375. https://doi.org/10.1016/j.whi.2022.02.002.
Attar, A., A. Hosseinpour, and M. Moghadami. 2023. The impact of antihypertensive treatment of mild to moderate hypertension during pregnancy on maternal and neonatal outcomes: An updated meta-analysis of randomized controlled trials. Clinical Cardiology 46(5):467–476. https://doi.org/10.1002/clc.24013.
Avalos, L. A., R. S. Neugebauer, N. Nance, S. E. Badon, T. C. Cheetham, T. R. Easterling, K. Reynolds, A. Idu, Z. Bider-Canfield, V. L. Holt, and S. Dublin. 2023. Maternal and neonatal outcomes associated with treating hypertension in pregnancy at different thresholds. Pharmacotherapy 43(5):381–390. https://doi.org/10.1002/phar.2778.
AWHONN (Association of Women’s Health, Obstetric and Neonatal Nurses). 2025. Why Is Postpartum Discharge Training Essential for Nurses and Clinicians? https://www.awhonn.org/education/post-birth-warning-signs-education-program/ (accessed December 31, 2025).
Bailey, E. J., A. T. N. Tita, J. Leach, K. Boggess, L. Dugoff, B. Sibai, K. Lawrence, B. L. Hughes, J. Bell, K. Aagaard, R. K. Edwards, K. Gibson, D. M. Haas, L. Plante, T. D. Metz, B. M. Casey, S. Esplin, S. Longo, M. Hoffman, G. R. Saade, J. Foroutan, M. G. Tuuli, M. Y. Owens, H. N. Simhan, H. A. Frey, T. Rosen, A. Palatnik, S. Baker, P. August, U. M. Reddy, W. Kinzler, E. J. Su, I. Krishna, N. Nguyen, M. E. Norton, D. Skupski, Y. Y. El-Sayed, D. Ogunyemi, Z. S. Galis, L. Harper, N. Ambalavanan, S. Oparil, H. C. Kuo, J. M. Szychowski, and K. Hoppe. 2023. Perinatal outcomes associated with management of stage 1 hypertension. Obstetrics & Gynecology 142(6):1395–1404. https://doi.org/10.1097/AOG.0000000000005410.
Behrens, I., S. Basit, M. Melbye, J. A. Lykke, J. Wohlfahrt, H. Bundgaard, B. Thilaganathan, and H. A. Boyd. 2017. Risk of post-pregnancy hypertension in women with a history of hypertensive disorders of pregnancy: Nationwide cohort study. BMJ 358:j3078. https://doi.org/10.1136/bmj.j3078.
Bernstein, P. S., J. N. Martin, Jr., J. R. Barton, L. E. Shields, M. L. Druzin, B. M. Scavone, J. Frost, C. H. Morton, C. Ruhl, J. Slager, E. Z. Tsigas, S. Jaffer, and M. K. Menard. 2017. National Partnership for Maternal Safety: Consensus bundle on severe hypertension during pregnancy and the postpartum period. Obstetrics & Gynecology 130(2):347–357. https://doi.org/10.1097/AOG.0000000000002115.
Bisson, C., E. Patel, A. Mueller, S. Suresh, C. Duncan, A. Premkumar, S. Shahul, and S. Rana. 2024. Extended postpartum outcomes with systematic treatment of and management of postpartum hypertension program. Pregnancy Hypertension 37:101138. https://doi.org/10.1016/j.preghy.2024.101138.
Blumenthal, E. A., B. A. Crosland, D. Senderoff, K. Santurino, N. Garg, M. Bernstein, D. Wolfe, and A. Hameed. 2020. California cardiovascular screening tool: Findings from initial implementation. AJP Reports 10(4):e362–e368. https://doi.org/10.1055/s-0040-1718382.
Blumenthal, E. A., N. Hooshvar, V. Tancioco, R. Newman, D. Senderoff, and J. McNulty. 2021. Implementation and evaluation of an electronic maternal early warning trigger tool to reduce maternal morbidity. American Journal of Perinatology 38(09):869–879. https://doi.org/10.1055/s-0040-1721715.
Boggess, K., J. Leach, L. Dugoff, B. Sibai, B. L. Hughes, J. Bell, K. Aagaard, R. Edwards, K. Gibson, D. M. Haas, L. Plante, T. Metz, B. Casey, S. Longo, M. K. Hoffman, G. R. Saade, K. K. Hoppe, J. Foroutan, M. Owens, H. N. Simhan, H. Frey, T. Rosen, A. Palatnik, S. Baker, W. Kinzler, E. Su, I. Krishna, M. E. Norton, D. Skupski, Y. Y. El-Sayed, R. Librizzi, L. Pereira, M. Habli, S. Williams, G. Pridijan, D. S. McKenna, E. Chang, S. Osmundson, Z. Galis, L. Harper, N. Ambalavanan, J. Szychowski, and A. Tita. 2022. Relationship between third-trimester low maternal blood pressure and small-for-gestational-age birth weight in pregnant individuals with mild chronic hypertension. Obstetrics & Gynecology 146(3):405–412. https://doi.org/10.1097/AOG.0000000000006008.
Borders, A., L. Keenan-Devlin, E. H. Oh, D. Young, W. Grobman, and P. L. King. 2025. Reducing severe maternal morbidity for birthing persons with severe hypertension through a statewide quality improvement initiative. American Journal of Obstetrics and Gynecology 232(1):128.e1–128.e9. https://doi.org/10.1016/j.ajog.2024.04.026.
Borrowman, J. D., L. J. Carr, G. L. Pierce, W. T. Story, B. B. Gibbs, and K. M. Whitaker. 2025. Postpartum remote health coaching intervention for individuals with a hypertensive disorder of pregnancy: Proof-of-concept study. JMIR Formative Research 9(1):e65611. https://doi.org/10.2196/65611.
Bronner, B. A., P. L. Trowbridge, A. C. Perry, A. C. McCormick, T. P. Waters, and S. de Los Reyes. 2023. Effectiveness of extended postpartum inpatient monitoring for hypertensive disorders of pregnancy to reduce the risk of readmission for preeclampsia with severe features. American Journal of Obstetrics & Gynecology MFM 5(7):100956. https://doi.org/10.1016/j.ajogmf.2023.100956.
Brown, M. A., L. A. Magee, L. C. Kenny, S. A. Karumanchi, F. P. McCarthy, S. Saito, D. R. Hall, C. E. Warren, G. Adoyi, and S. Ishaku. 2018. Hypertensive disorders of pregnancy: ISSHP classification, diagnosis, and management recommendations for international practice. Hypertension 72(1):24–43. https://doi.org/10.1016/j.preghy.2018.05.004.
Brown, M. C., K. E. Best, M. S. Pearce, J. Waugh, S. C. Robson, and R. Bell. 2013. Cardiovascular disease risk in women with pre-eclampsia: Systematic review and meta-analysis. European Journal of Epidemiology 28(1):1–19. https://doi.org/10.1007/s10654-013-9762-6
Butalia, S., F. Audibert, A.-M. Côté, T. Firoz, A. G. Logan, L. A. Magee, W. Mundle, E. Rey, D. M. Rabi, S. S. Daskalopoulou, and K. A. Nerenberg. 2018. Hypertension Canada’s 2018 guidelines for the management of hypertension in pregnancy. Canadian Journal of Cardiology 34(5):526–531. https://doi.org/10.1016/j.cjca.2018.02.021.
Cairns, A. E., K. L. Tucker, P. Leeson, L. H. Mackillop, M. Santos, C. Velardo, D. Salvi, S. Mort, J. Mollison, L. Tarassenko, and R. J. McManus. 2018. Self-management of postnatal hypertension: The SNAP-HT trial. Hypertension 72(2):425–432. https://doi.org/10.1161/HYPERTENSIONAHA.118.10911.
Canoy, D., B. J. Cairns, A. Balkwill, F. L. Wright, A. Khalil, V. Beral, J. Green, and G. Reeves. 2016. Hypertension in pregnancy and risk of coronary heart disease and stroke: A prospective study in a large UK cohort. International Journal of Cardiology 222:1012–1018. https://doi.org/1018.10.1016/j.ijcard.2016.07.170.
Cao, C., W. Cai, X. Niu, J. Fu, J. Ni, Q. Lei, J. Niu, X. Zhou, and Y. Li. 2020. Prehypertension during pregnancy and risk of small for gestational age: A systematic review and metaanalysis. Journal of Maternal-Fetal and Neonatal Medicine 33(8):1447–1454. https://doi.org/10.1080/14767058.2018.1519015.
CDC (Centers for Disease Control and Prevention). 2024a. Hear Her Campaign: An Overview. https://www.cdc.gov/hearher/about/index.html (accessed December 31, 2025).
CDC. 2024b. Signs and Symptoms of Urgent Maternal Warnings Signs. https://www.cdc.gov/hearher/maternal-warning-signs/index.html (accessed December 31, 2025).
Chambers, M. E., M. Y. De Zoysa, and A. B. Hameed. 2022. Screening for cardiovascular disease in pregnancy: Is there a need? Journal of Cardiovascular Development and Disease 9(3):89. https://doi.org/10.3390/jcdd9030089.
Chen, H., R. Li, S. Liu, S. Zhao, T. Guo, S. Tian, J. Zhong, Z. Tang, Z. Ge, J. Xia, T. Geng, X. Pan, A. Pan, F. Qian, and G. Liu. 2025. Life’s Essential 8 and cardiovascular disease in women with a history of adverse pregnancy outcomes. European Journal of Preventive Cardiology 32(10):833–842. https://doi.org/10.1093/eurjpc/zwaf021.
Chen, K.-H., and L.-R. Chen. 2020. Provoking factors for postpartum chronic hypertension in women with preceding gestational hypertension/preeclampsia: A longitudinal cohort study of 22,798 pregnancies. International Journal of Medical Sciences 17(4):543. https://doi.org/10.7150/ijms.39432.
Claire, R., C. Chamberlain, M. A. Davey, S. E. Cooper, I. Berlin, J. Leonardi-Bee, and T. Coleman. 2020. Pharmacological interventions for promoting smoking cessation during pregnancy. Cochrane Database of Systematic Reviews 3(3):Cd010078. https://doi.org/10.1002/14651858.CD010078.pub3.
CMQCC (California Maternal Quality Care Collaborative). 2026. All Toolkits. https://www.cmqcc.org/toolkits-quality-improvement/all-toolkits (accessed January 6, 2026).
Corlin, T., N. Raghuraman, R. M. Rampersad, and B. A. Sabol. 2023. Postpartum remote home blood pressure monitoring: The new frontier. AJOG Global Reports 3(3):100251. https://doi.org/10.1016/j.xagr.2023.100251.
Countouris, M., Z. Mahmoud, J. B. Cohen, D. Crousillat, A. B. Hameed, C. M. Harrington, A. Hauspurg, M. C. Honigberg, J. Lewey, K. Lindley, M. M. McLaughlin, N. Sachdev, A. Sarma, K. Shapero, R. Sinkey, A. Tita, K. E. Wong, E. Yang, L. Cho, and N. A. Bello. 2025. Hypertension in pregnancy and postpartum: Current standards and opportunities to improve care. Circulation 151(7):490–507. https://doi.org/10.1161/CIRCULATIONAHA.124.073302.
de Los Reyes, S., B. A. Plunkett, and A. Dude. 2021. The association between persistent maternal hypotension and small for gestational age neonates. American Journal of Obstetrics & Gynecology MFM 3(6):100449. https://doi.org/10.1016/j.ajogmf.2021.100449.
Deputy, N. P., A. J. Sharma, and S. Y. Kim. 2015. Gestational weight gain—United States, 2012 and 2013. Morbidity and Mortality Weekly Report 64(43):1215–1220. https://doi.org/10.15585/mmwr.mm6443a3.
di Pasquo, E., S. R. Giannubilo, B. Valentini, S. Salvi, R. Rullo, S. Fruci, E. Filippi, S. Ornaghi, S. Zullino, F. Rossi, D. Farsetti, D. D. Di Martino, B. Vasapollo, A. Locatelli, M. De Santis, A. Ciavattini, A. Lanzone, F. Mecacci, E. Ferrazzi, H. Valensise, and T. Ghi. 2024. The “Preeclampsia and Hypertension Target Treatment” study: A multicenter prospective study to evaluate the effectiveness of the antihypertensive therapy based on maternal hemodynamic findings. American Journal of Obstetrics & Gynecology MFM 6(5):101368. https://doi.org/10.1016/j.ajogmf.2024.101368.
Ditosto, J. D., M. V. Roytman, B. M. Dolan, S. S. Khan, C. M. Niznik, and L. M. Yee. 2023. Improving postpartum and long-term health after an adverse pregnancy outcome: Examining interventions from a health equity perspective. Clinical Obstetrics and Gynecology 66(1):132–149. https://doi.org/10.1097/GRF.0000000000000759.
Drake, M., G. Austin, L. Dann, Y. Li, C. Shuker, and A. Psirides. 2021. Introduction of a standardised maternity early warning system: Indicative data from a before-and-after study at a large pilot site before national rollout in Aotearoa New Zealand. Anaesthesia 76(12):1600–1606. https://doi.org/10.1111/anae.15557.
Dumitrascu-Biris, D., D. Nzelu, T. Dassios, K. Nicolaides, and N. A. Kametas. 2021. Chronic hypertension in pregnancy stratified by first-trimester blood pressure control and adverse perinatal outcomes: A prospective observational study. Acta Obstetricia et Gynecologica Scandinavica 100(7):1297–1304. https://doi.org/10.1111/aogs.14132.
Emeruwa, U. N., A. Çapi, M. B. Jacobs, L. C. Laurent, N. A. Bello, and C. Gyamfi-Bannerman. 2025. Incidence and risk factors of de novo postpartum hypertension: Understanding links to long-term cardiovascular risk. JACC: Advances 4(6_Part_1):101756. https://doi.org/10.1016/j.jacadv.2025.101756.
Facco, F. L., C. B. Parker, U. M. Reddy, R. M. Silver, M. A. Koch, J. M. Louis, R. C. Basner, J. H. Chung, C.-L. Nhan-Chang, G. W. Pien, S. Redline, W. A. Grobman, D. A. Wing, H. N. Simhan, D. M. Haas, B. M. Mercer, S. Parry, D. Mobley, S. Hunter, G. R. Saade, F. P. Schubert, and P. C. Zee. 2017. Association between sleep-disordered breathing and hypertensive disorders of pregnancy and gestational diabetes mellitus. Obstetrics & Gynecology 129(1):31–41. https://doi.org/10.1097/AOG.0000000000001805.
Ford, N. D., S. Cox, J. Y. Ko, L. Ouyang, L. Romero, T. Colarusso, C. D. Ferre, C. D. Kroelinger, D. K. Hayes, and W. D. Barfield. 2022. Hypertensive disorders in pregnancy and mortality at delivery hospitalization—United States, 2017–2019. Morbidity and Mortality Weekly Report 71(17):585–591. https://doi.org/10.15585/mmwr.mm7117a1.
Forna, F., E. Gibson, A. Miles, P. Seda, F. Lobelo, A. Mbanya, B. Pimentel, G. Sobers, S. Leung, and K. Koplan. 2024. Improving obstetric and perinatal outcomes with a remote patient monitoring program for hypertension in a large integrated care system. Pregnancy Hypertension 35:37–42. https://doi.org/10.1016/j.preghy.2023.12.007.
Garovic, V. D., R. Dechend, T. Easterling, S. A. Karumanchi, S. McMurtry Baird, L. A. Magee, S. Rana, J. V. Vermunt, and P. August. 2022. Hypertension in pregnancy: Diagnosis, blood pressure goals, and pharmacotherapy: A scientific statement from the American Heart Association. Hypertension 79(2):e21–e41. https://doi.org/10.1161/HYP.0000000000000208.
Goel, A., M. R. Maski, S. Bajracharya, J. B. Wenger, D. Zhang, S. Salahuddin, S. S. Shahul, R. Thadhani, E. W. Seely, and S. A. Karumanchi. 2015. Epidemiology and mechanisms of de novo and persistent hypertension in the postpartum period. Circulation 132(18):1726–1733. https://doi.org/10.1161/CIRCULATIONAHA.115.015721.
Grandi, S. M., K. B. Filion, S. Yoon, H. T. Ayele, C. M. Doyle, J. A. Hutcheon, G. N. Smith, G. C. Gore, J. G. Ray, K. Nerenberg, and R. W. Platt. 2019. Cardiovascular disease–related morbidity and mortality in women with a history of pregnancy complications. Circulation 139(8):1069–1079. https://doi.org/10.1161/CIRCULATIONAHA.118.036748.
Gregory, E. F., K. K. Upadhya, T. L. Cheng, K. J. Psoter, and K. B. Mistry. 2020. Enabling factors associated with receipt of interconception health care. Maternal and Child Health Journal 24(3):275–282. https://doi.org/10.1007/s10995-019-02850-0.
Gyselaers, W., P. Dreesen, A. S. Staelens, K. Tomsin, L. Bruckers, and S. Vonck. 2023. First-trimester normotension is a weak indicator of normal maternal cardiovascular function. Hypertension 80(2):343–351. https://doi.org/10.1161/HYPERTENSIONAHA.122.19346.
Hameed, A. 2022. CVD Risk Assessment Implementation Guide. https://bpb-us-e2.wpmucdn.com/sites.uci.edu/dist/4/4953/files/2024/04/CVD-Implementation-Guide-282a9a062f-92baea.pdf (accessed December 31, 2025).
Hameed, A. B., A. Haddock, D. S. Wolfe, K. Florio, N. Drummond, C. Allen, I. Taylor, S. Kendig, G. Presumey-Leblanc, and E. Greenwood. 2023a. Alliance for Innovation on Maternal Health: Consensus bundle on cardiac conditions in obstetric care. Obstetrics & Gynecology 141(2):253–263. https://doi.org/10.1097/AOG.0000000000005048.
Hameed, A. B., M. Tarsa, C. R. Graves, J. Chang, M. Billah, T. Hatfield, and H. Thiel de Bocanegra. 2023b. Cardiovascular risk assessment as a quality measure in the pregnancy and postpartum period. JACC: Advances 2(1):100176. https://doi.org/10.1016/j.jacadv.2022.100176.
Hameed, A. B., M. Tarsa, C. R. Graves, A. Grodzinsky, H. Thiel De Bocanegra, and D. S. Wolfe. 2024. Universal cardiovascular disease risk assessment in pregnancy: Call to action JACC: Advances expert panel. JACC: Advances 3(8):101055. https://doi.org/10.1016/j.jacadv.2024.101055.
Hameed, A. B., M. Tarsa, and A. Waks. 2025a. Response to letter to the editor: Standardized cardiovascular risk assessment in pregnancy and postpartum. American Journal of Obstetrics & Gynecology MFM 7(9):101736. https://doi.org/10.1016/j.ajogmf.2025.101736.
Hameed, A. B., M. Tarsa, A. Waks, A. Grodzinsky, K. L. Florio, J. Chang, M. B. Jacobs, O. I. Balogun, and H. T. De Bocanegra. 2025b. Results of cardiovascular testing among pregnant and postpartum persons undergoing standardized cardiovascular risk assessment. American Journal of Obstetrics & Gynecology MFM 7(5):101656. https://doi.org/10.1016/j.ajogmf.2025.101656.
Hamza, A., C. Gerlinger, J. Radosa, E. Solomayer, J. Hagmann, U. Sester, R. Bohle, R. Stroeder, Z. Takacs, G. Meyberg-Solomayer, I. Juhasz-Boess, and M. Kasoha. 2019. Pilot study: Placental biomarker predictive capability (sFlt-1, PlGF and their ratio) of postpartum maternal outcome. Archives of Gynecology and Obstetrics 299(6):1557–1566. https://doi.org/10.1007/s00404-019-05128-6.
Hannola, K., S. Hoppu, S. Mennander, H. Huhtala, H. Laivuori, and K. Tihtonen. 2021. Obstetric early warning system to predict maternal morbidity of pre-eclampsia, postpartum hemorrhage and infection after birth in high-risk women: A prospective cohort study. Midwifery 99:103015. https://doi.org/10.1016/j.midw.2021.103015.
Harper, L. M., H.-C. Kuo, K. Boggess, L. Dugoff, B. Sibai, K. Lawrence, B. L. Hughes, J. Bell, K. Aagaard, and R. K. Edwards. 2025. Blood pressure control in pregnant patients with chronic hypertension and diabetes: Should <130/80 be the target? American Journal of Obstetrics and Gynecology 232(5):482.e481–482.e488. https://doi.org/10.1016/j.ajog.2024.09.006.
Hauspurg, A., M. E. Countouris, and J. M. Catov. 2019a. Hypertensive disorders of pregnancy and future maternal health: How can the evidence guide postpartum management? Current Hypertension Reports 21(12):96. https://doi.org/10.1007/s11906-019-0999-7.
Hauspurg, A., S. Parry, B. M. Mercer, W. Grobman, T. Hatfield, R. M. Silver, C. B. Parker, D. M. Haas, J. D. Iams, G. R. Saade, R. J. Wapner, U. M. Reddy, and H. Simhan. 2019b. Blood pressure trajectory and category and risk of hypertensive disorders of pregnancy in nulliparous women. American Journal of Obstetrics and Gynecology 221(3):277e271–277e278. https://doi.org/10.1016/j.ajog.2019.06.031.
Hauspurg, A., E. W. Seely, J. Rich-Edwards, C. Hayduchok, S. Bryan, A. T. Roche, A. Jeyabalan, E. M. Davis, R. Hart, J. Shirriel, and J. Catov. 2023. Postpartum home blood pressure monitoring and lifestyle intervention in overweight and obese individuals the first year after gestational hypertension or pre-eclampsia: A pilot feasibility trial. BJOG 130(7):715–726. https://doi.org/10.1111/1471-0528.17381.
Hirshberg, A., K. Downes, and S. Srinivas. 2018. Comparing standard office-based followup with text-based remote monitoring in the management of postpartum hypertension: A randomised clinical trial. BMJ Quality & Safety 27(11):871–877. https://doi.org/10.1136/bmjqs-2018-007837.
Hirshberg, A., Y. Zhu, A. Smith-McLallen, and S. K. Srinivas. 2023. Association of a remote blood pressure monitoring program with postpartum adverse outcomes. Obstetrics & Gynecology 141(6):1163–1170. https://doi.org/10.1097/AOG.0000000000005197.
Hoppe, K. K., M. Williams, N. Thomas, J. B. Zella, A. Drewry, K. Kim, T. Havighurst, and H. M. Johnson. 2019. Telehealth with remote blood pressure monitoring for postpartum hypertension: A prospective single-cohort feasibility study. Pregnancy Hypertension 15:171–176. https://doi.org/10.1016/j.preghy.2018.12.007.
Hutchins, F., S. R. El Khoudary, J. Catov, R. Krafty, A. Colvin, E. Barinas-Mitchell, and M. M. Brooks. 2022. Excessive gestational weight gain and long-term maternal cardiovascular risk profile: The Study of Women’s Health Across the Nation. Journal of Women’s Health 31(6):808–818. https://doi.org/10.1089/jwh.2021.0449.
Ibáñez-Lorente, C., R. Casans-Francés, S. Bellas-Cotán, and L. E. Muñoz-Alameda. 2021. Implementation of a maternal early warning system during early postpartum. A prospective observational study. PloS One 16(6):e0252446. https://doi.org/10.1371/journal.pone.0252446.
Ishikuro, M., T. Obara, K. Murakami, F. Ueno, A. Noda, T. Onuma, M. Kikuya, H. Metoki, and S. Kuriyama. 2024. The association between blood pressure control in women during pregnancy and adverse perinatal outcomes: The TMM BirThree cohort study. Hypertension Research 47(5):1216–1222. https://doi.org/10.1038/s41440-023-01570-x.
Jones, D. W., K. C. Ferdinand, S. J. Taler, H. M. Johnson, D. Shimbo, M. Abdalla, M. M. Altieri, N. Bansal, N. A. Bello, A. P. Bress, J. Carter, J. B. Cohen, K. J. Collins, Y. Commodore-Mensah, L. L. Davis, B. Egan, S. S. Khan, D. M. Lloyd-Jones, B. M. Melnyk, E. A. Mistry, M. O. Ogunniyi, S. L. Schott, S. C. Smith, A. W. Talbot, W. Vongpatanasin, K. E. Watson, P. K. Whelton, and J. D. Williamson. 2025. 2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM guideline for the prevention, detection, evaluation and management of high blood pressure in adults: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 152(11):e114–e218. https://doi.org/10.1161/CIR.0000000000001356.
Kalafat, E., C. Benlioglu, B. Thilaganathan, and A. Khalil. 2020. Home blood pressure monitoring in the antenatal and postpartum period: A systematic review meta-analysis. Pregnancy Hypertension 19:44–51. https://doi.org/10.1016/j.preghy.2019.12.001.
Kalkhoff, S. M., M. A. Lutgendorf, T. C. Morrison, T. Han, and D. L. Spence. 2022. A randomized controlled trial of sleep study surveillance with targeted autoregulated positive airway pressure therapy for obstructive sleep apnea in pregnancy. American Journal of Obstetrics & Gynecology MFM 4(3):100571. https://doi.org/10.1016/j.ajogmf.2022.100571.
Kern-Goldberger, A., and A. Hirshberg. 2021. Reducing disparities using telehealth approaches for postdelivery preeclampsia care. Clinical Obstetrics and Gynecology 64(2):375–383. https://doi.org/10.1097/GRF.0000000000000605.
Kern-Goldberger, A. R., J. Ewing, M. Polin, M. D’Alton, A. M. Friedman, and D. Goffman. 2023. The predictive value of vital signs for morbidity in pregnancy: Evaluating and optimizing maternal early warning systems. American Journal of Perinatology 40(14):1590–1601. https://doi.org/10.1055/s-0041-1739432.
Khosla, K., S. Heimberger, K. M. Nieman, A. Tung, S. Shahul, A. C. Staff, and S. Rana. 2021. Long-term cardiovascular disease risk in women after hypertensive disorders of pregnancy: Recent advances in hypertension. Hypertension 78(4):927–935. https://doi.org/10.1161/HYPERTENSIONAHA.121.16506.
Kitt, J. A., R. L. Fox, A. E. Cairns, J. Mollison, H. H. Burchert, Y. Kenworthy, A. McCourt, K. Suriano, A. J. Lewandowski, L. Mackillop, K. L. Tucker, R. J. McManus, and P. Leeson. 2021. Short-term postpartum blood pressure self-management and long-term blood pressure control: A randomized controlled trial. Hypertension 78(2):469–479. https://doi.org/10.1161/HYPERTENSIONAHA.120.17101.
Kitt, J., R. Fox, A. Frost, M. Shanyinde, K. Tucker, P. A. Bateman, K. Suriano, Y. Kenworthy, A. McCourt, and W. Woodward. 2023. Long-term blood pressure control after hypertensive pregnancy following physician-optimized self-management: The POP-HT randomized clinical trial. JAMA 330(20):1991–1999. https://doi.org/10.1001/jama.2023.21523.
Kusumaningrum, T., Nursalam, M. Triharini, and D. Soares. 2025. Postpartum care for hypertension prevention in women with a history of preeclampsia: A systematic review. Pediomaternal Nursing Journal 11(1):63–75. https://doi.org/10.20473/pmnj.v11i1.69365.
Lee, Y.-C., Y.-C. Chang, L.-W. Tseng, W.-N. Lin, C.-T. Lu, L.-A. Lee, T.-J. Fang, W.-N. Cheng, and H.-Y. Li. 2024. Continuous positive airway pressure treatment and hypertensive adverse outcomes in pregnancy: A systematic review and meta-analysis. JAMA Network Open 7(8):e2427557. https://doi.org/10.1001/jamanetworkopen.2024.27557.
Lemon, L. S., B. Quinn, A. Binstock, J. C. Larkin, H. N. Simhan, and A. Hauspurg. 2024. Clinical outcomes associated with a remote postpartum hypertension monitoring program. Obstetrics & Gynecology 144(3):377–385. https://doi.org/10.1097/aog.0000000000005665.
Levine, L. D., B. Ky, J. A. Chirinos, J. Koshinksi, Z. Arany, V. Riis, M. A. Elovitz, N. Koelper, and J. Lewey. 2022. Prospective evaluation of cardiovascular risk 10 years after a hypertensive disorder of pregnancy. Journal of the American College of Cardiology 79(24):2401–2411. https://doi.org/10.1016/j.jacc.2022.03.383.
Lewey, J., T. M. Beckie, H. L. Brown, S. D. Brown, V. D. Garovic, S. S. Khan, E. C. Miller, G. Sharma, and L. S. Mehta. 2024. Opportunities in the postpartum period to reduce cardiovascular disease risk after adverse pregnancy outcomes: A scientific statement from the American Heart Association. Circulation 149(7):e330–e346. https://doi.org/10.1161/CIR.0000000000001212.
Lu, Q., X. Zhang, Y. Wang, J. Li, Y. Xu, X. Song, S. Su, X. Zhu, M. V. Vitiello, J. Shi, Y. Bao, and L. Lu. 2021. Sleep disturbances during pregnancy and adverse maternal and fetal outcomes: A systematic review and meta-analysis. Sleep Medicine Reviews 58:101436. https://doi.org/10.1016/j.smrv.2021.101436.
Macphail, M. G., S. Juul, K. Wollny, J. Y. Negre, A. Metcalfe, K. H. Chaput, S. Butalia, and K. A. Nerenberg. 2024. Nutrition interventions for lowering cardiovascular risk after hypertensive disorders of pregnancy: A systematic review. CJC Open 6(2):195–204. https://doi.org/10.1016/j.cjco.2023.10.018.
Magee, L. A., P. Von Dadelszen, E. Rey, S. Ross, E. Asztalos, K. E. Murphy, J. Menzies, J. Sanchez, J. Singer, A. Gafni, A. Gruslin, M. Helewa, E. Hutton, S. K. Lee, T. Lee, A. G. Logan, W. Ganzevoort, R. Welch, J. G. Thornton, and J.-M. Moutquin. 2015. Less-tight versus tight control of hypertension in pregnancy. New England Journal of Medicine 372(5):407–417. https://doi.org/10.1111/1471-0528.13568.
Magee, L. A., P. von Dadelszen, J. Singer, T. Lee, E. Rey, S. Ross, E. Asztalos, K. E. Murphy, J. Menzies, J. Sanchez, A. Gafni, M. Helewa, E. Hutton, G. Koren, S. K. Lee, A. G. Logan, W. Ganzevoort, R. Welch, J. G. Thornton, and J.-M. Moutquin, for the CHIPS Study Group. 2016. The CHIPS randomized controlled trial (Control of Hypertension in Pregnancy study) is severe hypertension just an elevated blood pressure? Hypertension 68(5):1153–1159. https://doi.org/10.1161/HYPERTENSIONAHA.116.07862.
Mai, T. D., S. Katsuragawa, A. McDougall, P. Y. Nguyen, L. Romero, J. Vogel, and M. Makama. 2025. Self-care interventions for preventing cardiovascular diseases after hypertensive pregnancy disorders: A systematic review and meta-analysis. BJOG 132(10):1350–1361. https://doi.org/10.1111/1471-0528.18152.
Malhamé, I., V. Danilack, C. Raker, E. Hardy, H. Spalding, B. Bouvier, H. Hurlburt, R. Vrees, D. Savitz, and N. Mehta. 2021. Cardiovascular severe maternal morbidity in pregnant and postpartum women: Development and internal validation of risk prediction models. BJOG 128(5):922–932. https://doi.org/10.1111/1471-0528.16512.
Malhamé, I., C. A. Raker, E. J. Hardy, H. Spalding, B. A. Bouvier, H. Hurlburt, R. Vrees, S. S. Daskalopoulou, K. Nerenberg, D. A. Savitz, N. Mehta, and V. A. Danilack. 2022. Development and internal validation of a risk prediction model for acute cardiovascular morbidity in preeclampsia. Canadian Journal of Cardiology 38(10):1591–1599. https://doi.org/10.1016/j.cjca.2022.05.007.
Martinez-King, L. C., L. M. Savitsky, S. Rose, and C. Albright. 2025. Nonsevere hypertensive disorders of pregnancy and oral antihypertensive medications: An argument in favor of use. American Journal of Obstetrics & Gynecology MFM 7(1):101561. https://doi.org/10.1016/j.ajogmf.2024.101561.
Mei, J. Y., K. Corry-Saavedra, T. A. Nguyen, and A. Murphy. 2023. Standardized clinical assessment and management plan to reduce readmissions for postpartum hypertension. Obstetrics & Gynecology 142(2):384–392. https://doi.org/10.1097/AOG.0000000000005248.
Mitchell, C. J., A. Tita, S. B. Anderson, D. N. Pasko, and L. M. Harper. 2019. Adverse outcomes with maternal blood pressure less than 140/90 in pregnancy complicated by hypertension. American Journal of Perinatology 36(13):1394–1400. https://doi.org/10.1055/s-0038-1677474.
Mulder, E. G., C. Ghossein-Doha, E. Cauffman, V. A. Lopes van Balen, V. M.M.M. Schiffer, R.-J. Alers, J. Oben, L. Smits, S. M. van Kuijk, and M. E.A. Spaanderman. 2021. Preventing recurrent preeclampsia by tailored treatment of nonphysiologic hemodynamic adjustments to pregnancy. Hypertension 77(6):2045–2053. https://doi.org/10.1161/HYPERTENSIONAHA.120.16502.
NASEM (National Academies of Sciences, Engineering, and Medicine). 2019. Integrating social care into the delivery of health care: Moving upstream to improve the nation’s health. Washington, DC: The National Academies Press. https://doi.org/10.17226/25467.
NASEM. 2022. Improving representation in clinical trials and research: Building research equity for women and underrepresented groups. Washington, DC: The National Academies Press. https://doi.org/10.17226/26479.
Nguyen, N. T. T., K. Kurtovic, C. Mitchell, M. Evangelista, R. Del Valle, S. M. Boling, and B. L. Hughes. 2022. Improving treatment of severe hypertension in pregnancy and postpartum using a hypertensive pathway. Pregnancy Hypertension 30:1–6. https://doi.org/10.1016/j.preghy.2022.07.007.
Niu, B., N. Mukhtarova, O. Alagoz, and K. Hoppe. 2022. Cost-effectiveness of telehealth with remote patient monitoring for postpartum hypertension. Journal of Maternal-Fetal and Neonatal Medicine 35(25):7555–7561. https://doi.org/10.1080/14767058.2021.1956456.
Nzelu, D., D. Dumitrascu-Biris, K. H. Nicolaides, and N. A. Kametas. 2018. Chronic hypertension: First-trimester blood pressure control and likelihood of severe hypertension, preeclampsia, and small for gestational age. American Journal of Obstetrics and Gynecology 218(3):337.e331–337.e7. https://doi.org/10.1016/j.ajog.2017.12.235.
Parikh, N. I., J. M. Gonzalez, C. A. M. Anderson, S. E. Judd, K. M. Rexrode, M. A. Hlatky, E. P. Gunderson, J. J. Stuart, D. Vaidya, American Heart Association, Council on Epidemiology and Prevention, Council on Arteriosclerosis Thrombosis and Vascular Biology, Council on Cardiovascular and Stroke Nursing, and Stroke Council. 2021. Adverse pregnancy outcomes and cardiovascular disease risk: Unique opportunities for cardiovascular disease prevention in women: A scientific statement from the American Heart Association. Circulation 143(18):e902–e916. https://doi.org/10.1161/CIR.0000000000000961.
Parker, S. E., A. Ajayi, and C. D. Yarrington. 2023. De novo postpartum hypertension: Incidence and risk factors at a safety-net hospital. Hypertension 80(2):279–287. https://doi.org/10.1161/HYPERTENSIONAHA.122.19275.
Partnership for Quality Measurement. 2025. CVD Risk Assessment Measure—Proportion of Pregnant/Postpartum Patients Who Receive CVD Risk Assessment with a Standardized Tool. https://p4qm.org/measures/4715 (accessed February 17, 2026).
Patel, E., C. Bisson, S. Suresh, A. Mueller, C. Duncan, S. Shahul, E. Lengyel, and S. Rana. 2025. Systematic treatment and management of postpartum hypertension using remote patient monitoring. Pregnancy Hypertension 39:101180. https://doi.org/10.1016/j.preghy.2024.101180.
Pesola, F., K. M. Smith, A. Phillips-Waller, D. Przulj, C. Griffiths, R. Walton, H. McRobbie, T. Coleman, S. Lewis, R. Whitemore, M. Clark, M. Ussher, L. Sinclair, E. Seager, S. Cooper, L. Bauld, F. Naughton, P. Sasieni, I. Manyonda, and P. Hajek. 2024. Safety of e-cigarettes and nicotine patches as stop-smoking aids in pregnancy: Secondary analysis of the Pregnancy Trial of e-Cigarettes and Patches (PREP) randomized controlled trial. Addiction 119(5):875–884. https://doi.org/10.1111/add.16422.
Pihelgas, A., L. Sevick, G. Pelinska, and W. W. Sia. 2025. Effectiveness of a postpartum vascular risk reduction clinic on behavioral change and long-term cardiovascular outcomes in women who had preeclampsia: A case-control study. Obstetric Medicine 18(3):150–156. https://doi.org/10.1177/1753495X241260792.
Porcelli, B. A., E. Diveley, K. Meyenburg, C. Woolfolk, J. I. Rosenbloom, N. Raghuraman, M. J. Stout, and B. A. Sabol. 2020. A new definition of gestational hypertension? New-onset blood pressures of 130 to 139/80 to 89 mm Hg after 20 weeks of gestation. American Journal of Obstetrics and Gynecology 223(3):442. e441–442.e7. https://doi.org/10.1016/j.ajog.2020.06.019.
Rasmussen, T. D., A.-M. N. Andersen, C. T. Ekstrøm, S. S. Jervelund, and S. F. Villadsen. 2023a. Improving health literacy responsiveness to reduce ethnic and social disparity in stillbirth and infant health: A cluster randomized controlled effectiveness trial of the MAMAACT intervention. International Journal of Nursing Studies 144:104505. https://doi.org/10.1016/j.ijnurstu.2023.104505.
Rasmussen, T. D., S. F. Villadsen, A. V. Hansen, L. H. Mortensen, C. T. Ekstrøm, S. S. Jervelund, and A. M. Nybo Andersen. 2023b. Effectiveness evaluation of an antenatal care intervention addressing disparities to improve perinatal outcomes in Denmark: A nationwide register-based analysis of a cluster randomised controlled trial (MAMAACT). BJOG 130(7):759–769. https://doi.org/10.1111/1471-0528.17404.
Reddy, A., A. Hauspurg, K. Venkatakrishnan, D. Pippi, L. Lemon, K. Berlacher, A. Jeyabalan, and M. Countouris. 2024. Establishing a remote blood pressure monitoring program through the first year postpartum after pregnancy-induced hypertension. JACC Advances 3(9):101189. https://doi.org/10.1016/j.jacadv.2024.101189.
Reddy, M., D. L. Rolnik, K. Harris, W. Li, B. W. Mol, F. Da Silva Costa, E. M. Wallace, and K. Palmer. 2020. Challenging the definition of hypertension in pregnancy: A retrospective cohort study. American Journal of Obstetrics and Gynecology 222(6):606 606.e1–606. e21. https://doi.org/10.1016/j.ajog.2019.12.272.
Rice, A. L., S. Bajaj, A. M. Wiedmer, N. Jacobson, A. K. Stanic, K. M. Antony, and M. H. Bazalakova. 2023. Continuous positive airway pressure treatment of obstructive sleep apnea and hypertensive complications in high-risk pregnancy. Sleep and Breathing 27(2):621–629. https://doi.org/10.1007/s11325-022-02669-0.
Riemer, M., S. Schulze, L. Wagner, M. Richter, G. Ayerle, A. Simm, S. Seeger, R. Schwesig, M. Tchirikov, and G. Seliger. 2021. Cardiovascular risk reduction in women following hypertensive disorders of pregnancy—a prospective, randomised, controlled interventional study. Geburtshilfe und Frauenheilkunde 81(08):966–978. https://doi.org/10.1055/a-1345-8733.
Riise, H. K. R., G. Sulo, G. S. Tell, J. Igland, O. Nygård, A. C. Iversen, and A. K. Daltveit. 2018. Association between gestational hypertension and risk of cardiovascular disease among 617,589 Norwegian women. Journal of the American Heart Association 7(10):e008337. https://doi.org/10.1161/jaha.117.008337.
Rosenfeld, E. B., D. Sagaram, R. Lee, E. Sadural, R. C. Miller, R. Lin, D. Jenkins, K. Black-ledge, I. Nikodijevic, A. Rizzo, V. Martinez, E. E. Daggett, O. McGeough, C. V. Ananth, and T. Rosen. 2025. Management of postpartum preeclampsia and hypertensive disorders (MOPP) postpartum tight vs. standard blood pressure control. JACC: Advances 4(3):101617. https://doi.org/10.1016/j.jacadv.2025.101617.
Sabol, B. A., B. Porcelli, E. Diveley, K. Meyenburg, C. Woolfolk, J. I. Rosenbloom, N. Raghuraman, and M. J. Stout. 2021. Defining the risk profile of women with stage 1 hypertension: A time to event analysis. American Journal of Obstetrics & Gynecology MFM 3(4):100376. https://doi.org/10.1016/j.ajogmf.2021.100376.
Sarma, A. A., D. R. Crousillat, P. Del Cueto, N. S. Scott, J. S. Tangren, A. Bryant Mantha, and I. T. Goldfarb. 2023. Feasibility of virtual blood pressure monitoring titrated to ACC/AHA thresholds among outpatients with postpartum hypertension. JACC: Advances 2(5):100390. https://doi.org/10.1016/j.jacadv.2023.100390.
Schneider, P., A. Lorenz, M. C. Menegay, S. Afflitto, E. Lamb, N. Cossler, K. Dixon, K. S. Gibson, C. Lannon, S. Fuller, S. Ford, R. Oza-Frank, R. Everett, and J. R. Lappen. 2023. The Ohio Maternal Safety Quality Improvement Project: Initial results of a statewide perinatal hypertension quality improvement initiative implemented during the COVID-19 pandemic. American Journal of Obstetrics & Gynecology MFM 5(6):100912. https://doi.org/10.1016/j.ajogmf.2023.100912.
Shields, L. E., S. Wiesner, C. Klein, B. Pelletreau, and H. L. Hedriana. 2016. Use of maternal early warning trigger tool reduces maternal morbidity. American Journal of Obstetrics and Gynecology 214(4):1.e1–1.e6. https://doi.org/10.1016/j.ajog.2016.01.154.
Sims, T. D., L. Shubert, S. Denning, L. Shay, C. Green, and C. Davidson. 2025. Impact of a maternal early warning system and severe hypertension safety bundle on timely treatment of hypertensive emergencies: A quality improvement and health equity initiative. BJOG 132(13):2160–2167. https://doi.org/10.1111/1471-0528.18273.
Sinkey, R. G., A. N. Battarbee, N. A. Bello, C. W. Ives, S. Oparil, and A. T. Tita. 2020. Prevention, diagnosis, and management of hypertensive disorders of pregnancy: A comparison of international guidelines. Current Hypertension Reports 22(9):66. https://doi.org/10.1007/s11906-020-01082-w.
Sisti, G., C. Fochesato, D. Elkafrawi, B. Marcus, and A. Schiattarella. 2023. Is blood pressure 120–139/80–89 mmhg before 20 weeks a risk factor for hypertensive disorders of pregnancy? A meta-analysis. European Journal of Obstetrics & Gynecology and Reproductive Biology 284:66–75. https://doi.org/10.1016/j.ejogrb.2023.03.011.
Slade, L. J., H. D. Mistry, J. N. Bone, M. Wilson, M. Blackman, N. Syeda, P. von Dadelszen, and L. A. Magee. 2023a. American College of Cardiology and American Heart Association blood pressure categories—a systematic review of the relationship with adverse pregnancy outcomes in the first half of pregnancy. American Journal of Obstetrics and Gynecology 228(4):418–429e434. https://doi.org/10.1016/j.ajog.2022.10.004.
Slade, L. J., M. Wilson, H. D. Mistry, J. N. Bone, N. A. Bello, M. Blackman, N. Syeda, P. von Dadelszen, and L. A. Magee. 2023b. The 2017 American College of Cardiology and American Heart Association blood pressure categories in the second half of pregnancy—a systematic review of their association with adverse pregnancy outcomes. American Journal of Obstetrics and Gynecology 229(2):101–117. https://doi.org/10.1016/j.ajog.2023.01.013.
Slade, L., N. Syeda, H. D. Mistry, J. N. Bone, M. Wilson, M. Blackman, L. Poston, K. M. Godfrey, P. von Dadelszen, L. A. Magee, and UPBEAT Consortium. 2025a. Do lower antenatal blood pressure cut-offs in pregnant women with obesity identify those at greater risk of adverse maternal and perinatal outcomes? A secondary analysis of data from the UK Pregnancies Better Eating and Activity Trial (UPBEAT). International Journal of Obesity 49(8):1523–1531. https://doi.org/10.1038/s41366-025-01803-8.
Slade, L. J., A. Syngelaki, M. Wilson, H. D. Mistry, R. Akolekar, P. von Dadelszen, K. H. Nicolaides, and L. A. Magee. 2025b. Blood pressure cutoffs at 11–13 weeks of gestation and risk of preeclampsia. American Journal of Obstetrics and Gynecology 232(2):214. e21–214.e210. https://doi.org/10.1016/j.ajog.2024.04.032.
SMFM (Society for Maternal-Fetal Medicine). 2022. Society for Maternal-Fetal Medicine statement: Antihypertensive therapy for mild chronic hypertension in pregnancy—the Chronic Hypertension and Pregnancy trial. American Journal of Obstetrics and Gynecology 227(2):B24–B27. https://doi.org/10.1016/j.ajog.2022.04.011.
Spencer, P., L. Ouyang, S. Cox, H. Tevendale, S. Carrigan, B. Behm, J. Rosenthal, A. E. Thompson, M. Lakusta, E. Strunz, and W. D. Barfield. 2025. Assessing early impact of the Hear Her® communication campaign. Health Promotion Practice:15248399251354966. https://doi.org/10.1177/15248399251354966.
Staff, A. C., M. L. Costa, R. Dechend, D. P. Jacobsen, and M. Sugulle. 2024. Hypertensive disorders of pregnancy and long-term maternal cardiovascular risk: Bridging epidemiological knowledge into personalized postpartum care and follow-up. Pregnancy Hypertension 36:101127. https://doi.org/10.1016/j.preghy.2024.101127.
Stajić, D., D. Ilić, J. Vuković, B. Baturan, A. Ilić, and A. Milovančev. 2022. The effect of continuous positive airway pressure treatment on hypertensive disorder in pregnant women with obstructive sleep apnea. Sleep and Breathing 26(1):297–305. https://doi.org/10.1007/s11325-021-02397-x.
Steele, D. W., G. P. Adam, I. J. Saldanha, G. Kanaan, M. L. Zahradnik, V. A. Danilack-Fekete, A. M. Stuebe, A. F. Peahl, K. K. Chen, and E. M. Balk. 2023. Postpartum home blood pressure monitoring: A systematic review. Obstetrics & Gynecology 142(2):285–295. https://doi.org/10.1097/AOG.0000000000005270.
Stierman, E. K., T. Watts, S. M. Lawson, T. M. Bruce, M. Reed-Vance, K. M. Bower, A. A. Creanga, and J. A. Callaghan-Koru. 2025. Educating families on urgent maternal warning signs: Learning from a pilot to improve training and tools for maternal and child home visiting programs. Health Promotion Practice 26(4):772–784. https://doi.org/10.1177/15248399241256691.
StrideBP. 2025. Validated Devices for Blood Pressure Measurement in Pregnancy/Preeclampsia. https://www.stridebp.org/pregnancy-pdf/ (accessed December 26, 2025).
Stulberg, D. B., L. P. Schumm, K. Schueler, M. Giurcanu, and M. E. Peek. 2023. Preconception care utilization: Self-report versus claims-based measures among women with Medicaid. PLOS Global Public Health 3(11):e0002592. https://doi.org/10.1371/journal.pgph.0002592.
Suresh, S. C., C. Duncan, H. Kaur, A. Mueller, A. Tung, J. L. Perdigao, K. Khosla, R. Dhir, K. Stewart, K. Wallace, R. Ahn, and S. Rana. 2021. Postpartum outcomes with systematic treatment and management of postpartum hypertension. Obstetrics & Gynecology 138(5):777–787. https://doi.org/10.1097/AOG.0000000000004574.
Tantrakul, V., A. Ingsathit, S. Liamsombut, S. Rattanasiri, P. Kittivoravitkul, N. Imsom-Somboon, S. Lertpongpiroon, S. Jantarasaengaram, W. Somchit, W. Suwansathit, J. Pengjam, S. Siriyotha, P. Panburana, C. Guilleminault, A. Preutthipan, J. Attia, and A. Thakkinstian. 2023. Treatment of obstructive sleep apnea in high risk pregnancy: A multicenter randomized controlled trial. Respiratory Research 24(1):171. https://doi.org/10.1186/s12931-023-02445-y.
Tao, J., S. Infusino, Y. Mintz, and K. K. Hoppe. 2024. Predictive modeling of postpartum blood pressure spikes. American Journal of Obstetrics & Gynecology MFM 6(7):101301. https://doi.org/10.1016/j.ajogmf.2024.101301.
Taylor, L., R. Claire, K. Campbell, T. Coleman-Haynes, J. Leonardi-Bee, C. Chamberlain, I. Berlin, M. A. Davey, S. Cooper, and T. Coleman. 2021. Fetal safety of nicotine replacement therapy in pregnancy: Systematic review and meta-analysis. Addiction 116(2):239–277. https://doi.org/10.1111/add.15185.
Texas DSHS (Department of State Health Services). n.d. Texas Health Data: Texas AIM. https://healthdata.dshs.texas.gov/dashboard/maternal-and-child-health/maternal-health/texas-aim (accessed December 31, 2025).
Texas DSHS. 2025. TexasAIM. https://www.dshs.texas.gov/maternal-child-health/programs-activities-maternal-child-health/texasaim (accessed December 31, 2025).
Thakkar, A., A. B. Hameed, M. Makshood, B. Gudenkauf, A. A. Creanga, I. Malhame, S. M. Grandi, S. A. Thorne, R. D’Souza, and G. Sharma. 2023. Assessment and prediction of cardiovascular contributions to severe maternal morbidity. JACC: Advances 2(2). https://doi.org/10.1016/j.jacadv.2023.100275.
Theilen, L. H., H. Meeks, A. Fraser, M. S. Esplin, K. R. Smith, and M. W. Varner. 2018. Long-term mortality risk and life expectancy following recurrent hypertensive disease of pregnancy. American Journal of Obstetrics and Gynecology 219(1):107.e101–107.e106. https://doi.org/10.1016/j.ajog.2018.04.002.
Tita, A. T., J. M. Szychowski, K. Boggess, L. Dugoff, B. Sibai, K. Lawrence, B. L. Hughes, J. Bell, K. Aagaard, R. K. Edwards, K. Gibson, D. M. Haas, L. Plante, T. Metz, B. Casey, S. Esplin, S. Longo, M. Hoffman, G. R. Saade, K. K. Hoppe, J. Foroutan, M. Tuuli, M. Y. Owens, H. N. Simhan, H. Frey, T. Rosen, A. Palatnik, S. Baker, P. August, U. M. Reddy, W. Kinzler, E. Su, I. Krishna, N. Nguyen, M. E. Norton, D. Skupski, Y. Y. El-Sayed, D. Ogunyemi, Z. S. Galis, L. Harper, N. Ambalavanan, N. L. Geller, S. Oparil, G. R. Cutter, and W. W. Andrews, for the CHAP Consortium. 2022. Treatment for mild chronic hypertension during pregnancy. New England Journal of Medicine 386(19):1781–1792. https://doi.org/10.1056/NEJMoa2201295.
Topel, M. L., E. M. Duncan, I. Krishna, M. L. Badell, V. Vaccarino, and A. A. Quyyumi. 2018. Estimated impact of the 2017 American College of Cardiology/American Heart Association blood pressure guidelines on reproductive-aged women. Hypertension 72(4):e39–e42. https://doi.org/10.1161/HYPERTENSIONAHA.118.11660.
Tran, D. T., J. M. Cohen, S. Donald, C. E. Cesta, K. Furu, L. Parkin, S.-A. Pearson, J. Reutfors, A. L. Robijn, H. Zoega, N. Zwar, and A. Havard. 2025. Risk of major congenital malformations following prenatal exposure to smoking cessation medicines. JAMA Internal Medicine 185(6):656–667. https://doi.org/10.1001/jamainternmed.2025.0290.
Triebwasser, J. E., M. K. Janssen, A. Hirshberg, and S. K. Srinivas. 2020. Successful implementation of text-based blood pressure monitoring for postpartum hypertension. Pregnancy Hypertension 22:156–159. https://doi.org/10.1016/j.preghy.2020.09.001.
Umar, A., C. A. Ameh, F. Muriithi, and M. Mathai. 2019. Early warning systems in obstetrics: A systematic literature review. PloS One 14(5):e0217864. https://doi.org/10.1371/journal.pone.0217864.
USPSTF (U.S. Preventive Services Task Force). 2018. Weight Loss to Prevent Obesity-Related Morbidity and Mortality in Adults: Behavioral Interventions. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/obesity-in-adults-interventions (accessed January 7, 2026).
USPSTF. 2020a. Healthy Diet and Physical Activity for Cardiovascular Disease Prevention in Adults with Cardiovascular Risk Factors: Behavioral Counseling Interventions. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/healthy-diet-and-physical-activity-counseling-adults-with-high-risk-of-cvd (accessed January 7, 2026).
USPSTF. 2020b. Tobacco Use in Children and Adolescents: Primary Care Interventions. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/tobacco-and-nicotine-use-prevention-in-children-and-adolescents-primary-care-interventions (accessed January 7, 2026).
USPSTF. 2021a. Gestational Diabetes: Screening. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/gestational-diabetes-screening (accessed January 8, 2026).
USPSTF. 2021b. Hypertension in Adults: Screening. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/hypertension-in-adults-screening (accessed January 7, 2026).
USPSTF. 2021c. Prediabetes and Type 2 Diabetes: Screening. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/screening-for-prediabetes-and-type-2-diabetes (accessed January 8, 2026).
USPSTF. 2021d. Tobacco Smoking Cessation in Adults, Including Pregnant Persons: Interventions. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/tobacco-use-in-adults-and-pregnant-women-counseling-and-interventions (accessed January 7, 2026).
USPSTF. 2022a. Healthy Diet and Physical Activity for Cardiovascular Disease Prevention in Adults Without Cardiovascular Disease Risk Factors: Behavioral Counseling Interventions. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/healthy-lifestyle-and-physical-activity-for-cvd-prevention-adults-without-known-risk-factors-behavioral-counseling (accessed January 7, 2026)
USPSTF. 2022b. Obstructive Sleep Apnea in Adults: Screening. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/obstructive-sleep-apnea-in-adults-screening (accessed January 7, 2022).
USPSTF. 2022c. Statin Use for the Primary Prevention of Cardiovascular Disease in Adults: Preventive Medication. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/statin-use-in-adults-preventive-medication (accessed January 7, 2026).
USPSTF. 2023. Hypertensive Disorders of Pregnancy: Screening. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/hypertensive-disorders-pregnancy-screening (accessed January 7, 2026).
USPSTF. 2024. High Body Mass Index in Children and Adolescents: Interventions. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/obesity-in-children-and-adolescents-screening (accessed January 7, 2026).
Vaughan, L. E., Y. Kanaji, S. Suvakov, S. Parashuram, Y. S. Butler Tobah, A. M. Chamberlain, S. J. Bielinski, N. Milic, R. Gulati, K. A. Nath, A. Lerman, and V. D. Garovic. 2024. Hypertensive disorders of pregnancy increase the risk for myocardial infarction: A population-based study. Journal of the American College of Cardiology 84(23):2264–2274. https://doi.org/10.1016/j.jacc.2024.06.049.
Wang, Y.-X., M. Arvizu, J. W. Rich-Edwards, L. Wang, B. Rosner, J. J. Stuart, K. M. Rexrode, and J. E. Chavarro. 2021. Hypertensive disorders of pregnancy and subsequent risk of premature mortality. Journal of the American College of Cardiology 77(10):1302–1312. https://doi.org/10.1016/j.jacc.2021.01.018.
Webster, K., S. Fishburn, M. Maresh, S. C. Findlay, and L. C. Chappell. 2019. Diagnosis and management of hypertension in pregnancy: Summary of updated NICE guidance. BMJ 366. https://doi.org/10.1136/bmj.l5119.
White, K. J., D. Tortal, K. Callahan, K. Eng, M. Hyland, E. Underwood, L. Senter, D. León-Martínez, M. Son, and H. Lipkind. 2023. Using a patient educational video to improve knowledge of maternal mortality warning signs: A randomized controlled trial. Obstetrics & Gynecology 142(5):1139–1147. https://doi.org/10.1097/AOG.0000000000005368.
Woolcock, H., N. Parra, Y. Zhang, U. M. Reddy, N. A. Bello, E. Miller, and W. A. Booker. 2024. Pregnancy outcomes in women who developed elevated blood pressure and stage I hypertension after 20 weeks, gestation. American Journal of Perinatology 41(15):2135–2143. https://doi.org/10.1055/a-2298-5347.
WPSI (Women’s Preventive Services Initiative). 2025. Well-Woman Chart. https://www.womenspreventivehealth.org/wp-content/uploads/WPSI-Well-Woman-Chart-2025_FINAL.pdf (accessed December 24, 2025).
Zullo, F., D. Di Mascio, F. H. Amro, S. Sorrenti, E. D’Alberti, A. Giancotti, G. Rizzo, and S. P. Chauhan. 2025. Postpartum remote blood pressure monitoring and risk of hypertensive-related readmission: Systematic review and meta-analysis of randomized controlled trials. Journal of Perinatal Medicine 53(4):439–448. https://doi.org/10.1515/jpm-2024-0515.
This page intentionally left blank.













































































































