Effects of Ionizing Radiation: Atomic Bomb Survivors and Their Children (1945-1995) (1998)
Chapter: 15 The Distinction in Radiobiology Between Medical and Public Health Functions
15
The Distinction in Radiobiology Between Medical and Public Health Functions
VICTOR P. BOND AND LUCIAN WIELOPOLSKI
Summary
Starting with the classical threshold-sigmoid medical-toxicological plot, reasons are advanced for why the coordinates of this function are not appropriate for the analysis of public health–epidemiological data. Misunderstandings with respect to both the level of biological organization and the word ''dose" are pointed out, which explain why public health–epidemiological data, anomalously, yield linear functions on medical-toxicological coordinates. It is then shown why substantially different coordinates must be used to obtain a function that describes properly and completely the cancer data obtained from epidemiological studies on the atomic bomb survivors. Arguments are put forth that contradict the linear, no-threshold hypothesis. Reasons are advanced for why, if the amount of radiation energy is expressed in the proper terms, the numerical value for the cancer "risk coefficient" becomes substantially smaller than it now is.
Introduction
The basic elements of present radiation quantities and units were developed in the era when the dogma was still firmly entrenched that radiation-attributable cancers could be induced only with repeated large exposures, i.e., a threshold was thought to pertain. Thus, most studies at the time were oriented around early effects on, and early responses of organs and organisms to moderate and large exposures.
The model used was that of classical medicine-toxicology, using pharmaceuticals or other chemicals, and characteristic threshold-sigmoid dose-response functions were observed. As will be shown below, such studies with pharmaceuticals require that the mass of biological subjects be used in order to determine the proper amount of chemical to administer.
However, when presumably the same model was employed for the early acute effects of the agent radiation energy, the practice of obtaining the mass, and thus the proper amount of the agent energy, was not followed. Furthermore, the reason for not doing so was neither mentioned nor explained. As a result, when late effects, particularly cancer, became an issue, the crucial step of including the mass and thus the imparted energy, first to both the individual elements and then to the subject population system of interest, was completely ignored.
The two related terms "medical-toxicological" (MT) and "public health–epidemiological" (PH), must be distinguished. With the MT biomedical discipline, the subject of interest is an individual; with the PH discipline, the subject of interest is a well-defined population.
A principal objective of this communication is to explore the reasons for and the severe consequences of not recognizing the proper role of the mass of the subject and thus the total energy imparted. To accomplish this objective, it is highly informative first to examine how the mass of the subject, and thus the total amount of agent transferred, enters into the formulation of classical pharmaceutical dose-response functions.
Classical MT Functions
For Pharmaceuticals
Figure 15.1 shows schematically a classical MT "dose response" function for pharmaceuticals or other chemicals, which typically has a threshold and is sigmoid in shape. The abscissa is here labeled the "prescription dose," DP, in units of the amount of agent per unit mass of biological subject, e.g., mg/kg. It is so labeled because it constitutes an instruction, once a value of DP is selected, to prepare the amount of agent that must actually be administered. This is the product of the prescription dose and the mass of the subject, ms. That product is here termed the true dose, TD, in units of mg. This use of the word dose conforms to actual practice in medicine, and to the definition of the word "dose" in both medical and general dictionaries (DP is not mentioned).
Although neither ms nor TD appear at all in the DP-response curve, it is obvious that, once DP is determined, it is TD and not DP that is actually administered, and that ms is used explicitly when determining the proper value for TD.

FIGURE 15.1 A classical MT dose-response function, used in medicine and toxicology for pharmaceuticals or other chemicals.
For Acute Radiation Responses
Figure 15.2 shows a typical MT curve for acute mortality in mice, which is a frequently used endpoint in radiobiology. The coordinates are identical to those in Figure 15.1, except that the units of DP , mg/kg for the chemical agent, are replaced by Gy (J/kg) for the radiation agent, energy. These quantities express the concentration and not the amount of agent. With radiation only, TD is also termed "imparted energy," with the symbol ![]() (ICRU, 1993). Similarly, DP is
(ICRU, 1993). Similarly, DP is ![]() /m.
/m.
With radiation exposure the animals are immersed in a radiation field and it is assumed that the resulting irradiation is to the whole body and is nominally uniform. Thus agent transfer, rather than indirectly via the bloodstream as with chemicals, is direct, i.e., the radiation field penetrates throughout the body so that energy is uniformly deposited and the agent concentration, ![]() /m, is equivalued throughout.
/m, is equivalued throughout.
However, ![]() /m on the abscissa of Figure 15.2 is an intensive quantity, i.e., it does not depend on the mass of the system, nor is it additive (i.e., DP can be the same throughout a relatively small or large subject). Accordingly, when an animal is uniformly irradiated, the subject perforce receives the value of
/m on the abscissa of Figure 15.2 is an intensive quantity, i.e., it does not depend on the mass of the system, nor is it additive (i.e., DP can be the same throughout a relatively small or large subject). Accordingly, when an animal is uniformly irradiated, the subject perforce receives the value of ![]() appropriate for
appropriate for

FIGURE 15.2 The same plot shown in Figure 15.1, but for
acute mouse mortality in mice exposed to 250 kVp x-rays.
the stated values of ![]() /m and mass, whatever those precise values may be. Thus, there is usually no requirement to weigh or use the mass of the animal (although, of course, the weight and thus
/m and mass, whatever those precise values may be. Thus, there is usually no requirement to weigh or use the mass of the animal (although, of course, the weight and thus ![]() could be obtained easily). Nevertheless, exactly as with chemicals, it is not DP that is transferred. Rather, it is (DP · ms), or
could be obtained easily). Nevertheless, exactly as with chemicals, it is not DP that is transferred. Rather, it is (DP · ms), or ![]() , in units of joules and in an amount sufficient to ensure a constant value of DP throughout the subject, that actually is administered.
, in units of joules and in an amount sufficient to ensure a constant value of DP throughout the subject, that actually is administered.
Moreover, the radiotherapists early coined, and still use the concept of "gram-rad," equal to ![]() , applied to the tumor bed. Every effort is made to minimize this value. However, the lack of a need to obtain the weight of the subject was seriously misinterpreted to mean that with radiation, unlike with the chemical MT model, there is no need even to be aware that the response could not be obtained unless a value of
, applied to the tumor bed. Every effort is made to minimize this value. However, the lack of a need to obtain the weight of the subject was seriously misinterpreted to mean that with radiation, unlike with the chemical MT model, there is no need even to be aware that the response could not be obtained unless a value of ![]() appropriate for the entire subject were delivered. The misunderstanding was reinforced and compounded by the early decision to define absorbed dose purely in terms of a concentration, energy per unit mass (ICRU, 1968). This confusingly gave a new and parochial meaning to a word, dose, that has been used for decades to define a quite different quantity, the amount of agent to an entire subject. As a result of this untenable dual definition of "dose," there is little reason for anyone, including radiobiologists, to be familiar with or appreciate
appropriate for the entire subject were delivered. The misunderstanding was reinforced and compounded by the early decision to define absorbed dose purely in terms of a concentration, energy per unit mass (ICRU, 1968). This confusingly gave a new and parochial meaning to a word, dose, that has been used for decades to define a quite different quantity, the amount of agent to an entire subject. As a result of this untenable dual definition of "dose," there is little reason for anyone, including radiobiologists, to be familiar with or appreciate
the importance of the terms ![]() or TD, at least in this specific context. Of equal significance, this definition enhances the misconception that absorbed dose (i.g., DP) is a measure of the amount of radiation when it is a concentration. The seriousness of these misunderstandings will become even more apparent below.
or TD, at least in this specific context. Of equal significance, this definition enhances the misconception that absorbed dose (i.g., DP) is a measure of the amount of radiation when it is a concentration. The seriousness of these misunderstandings will become even more apparent below.
Linear Functions
Although with MT the focus is always on an individual subject seeking or under medical care, when the emphasis is shifted to public health and epidemiology (PE), the biological subject of interest is a well defined population, NE, of "normal" subjects. These persons are frequently or continuously exposed in a "field" of potentially harmful objects or substances, which results in uncontrolled ("stochastic") interactions (accidents), in which some NE subjects become hit and dosed. The hit and dosed (ND) subjects receive values of TD of varying magnitudes, and thus sustain injury of different degrees of severity.
With this change in biomedical discipline (from MT to PE), different quantities assume importance, and the nature of the graphs changes, i.e., a completely different analysis of the same set of data, which includes all values of TD, DP, ms, NE, ND and Nq, is required. The principal question of interest in PH then becomes, What is the absolute number of quantally responding subjects, Nq, that resulted from individuals in a population being "hit" and dosed? rather than, What are the chances that an individual will respond quantally? Consequently TD , which is an extensive quantity that can be summed over the entire exposed population, is required because the total number responding quantally depends on this total amount of agent.
However, TD or ![]() can also be expressed as
can also be expressed as ![]() = ND • Dp • ms. With ms being a constant, and if DP is assumed to be constant, then
= ND • Dp • ms. With ms being a constant, and if DP is assumed to be constant, then ![]() = kND . Thus
= kND . Thus ![]() is proportional to ND. With uncontrolled delivery of an agent to a population, inevitably one encounters a distribution of values of DP. However, for ease of presentation, the entire distribution is here replaced by a single value (mean) of DP.
is proportional to ND. With uncontrolled delivery of an agent to a population, inevitably one encounters a distribution of values of DP. However, for ease of presentation, the entire distribution is here replaced by a single value (mean) of DP.
With the above simplification, it is easily possible to state succinctly the differences between the classical MT curve and the function for PE. If ND is held constant (e.g., on the ordinate of Figure 15.2) and only the agent concentration, DP, is permitted to vary, one obtains the threshold-sigmoid classical MT curve shown in Figure 15.2. However, if the agent concentration, DP is held constant (e.g., at point A in Figure 15.2) and only ND (or ![]() ) is permitted to vary, one obtains, as is indicated schematically in Figure 15.3, a linear PH function.
) is permitted to vary, one obtains, as is indicated schematically in Figure 15.3, a linear PH function.
With the current interpretation of linear radioepidemiological functions, one might hypothesize from Figure 15.3 that, "any amount of radiation, however small," can cause some acute mortality in an exposed population. However, the linear function in Figure 15.3 represents only an approximation of a step function, each step representing an integer number of subjects (Figure 15.4). Because no fewer

FIGURE 15.3 A PE function. The slope of the line is the value of point A in the linear function obtained when DP is held constant (point A in Figure 15.2), and ND is permitted to vary. The slope of the line equals the value of point A.
than one subject can die, the range of the function can extend only from one to the level at which all subjects are dead. Similarly for the integer ND in the abscissa in Figure 15.3, because no fewer than one subject can be exposed, the lower limit of the domain is one.
When integer steps of the otherwise continuous variable ![]() are used, instead of ND, they represent the mean value of a perhaps normal distribution that is not related to the linear regression line. It is the variance in this distribution that determines, as one moves away from the mean, the probability of a quantal response. In any case, the strict nature of the domain and range of the function precludes linear (or any other kind of) extrapolation of the function to 0,0 coordinates. Thus the linear, no-threshold hypothesis is seriously challenged.
are used, instead of ND, they represent the mean value of a perhaps normal distribution that is not related to the linear regression line. It is the variance in this distribution that determines, as one moves away from the mean, the probability of a quantal response. In any case, the strict nature of the domain and range of the function precludes linear (or any other kind of) extrapolation of the function to 0,0 coordinates. Thus the linear, no-threshold hypothesis is seriously challenged.
Ph Principles Applied To Atomic Bomb Survivors
Selected for this examination is a sample of about 40,000 atomic bomb survivors (NE subjects, all of whom became ND subjects), in which, at the time of the study, a total of 245 radiation-induced lethal solid cancers, Nca, had appeared (Shimizu et al., 1989; Pierce, 1989, as combined by Bond et al., 1991). The survivors were

FIGURE 15.4 The linear function shown in reality represents a continuous approximation to a step function, integer numbers of observed cancers. The number of quantally responding subjects cannot be less than one.
divided into eight dose intervals of arbitrary width, containing widely differing numbers of survivors. It is assumed that all 40,000 survivors received essentially uniform whole body irradiation, from penetrating photons only (i.e., the data are for a standard, "low LET" radiation).
Figure 15.5 shows the linear dose-response function that has been used widely to represent such PH data.1 Although clearly the graph appears to conform to that for a PH function, the coordinates correspond to those of an MT function. Furthermore, no information on the absolute number of cancers induced can be obtained from the plot. Thus, the function alone cannot be of value in PH studies.
In order to obtain a function that is suitable for PH studies, one must go back to the original data for the atomic bomb survivors and plot the absolute number of persons with a lethal cancer, as a function of either ![]() or its equivalent ND. The
or its equivalent ND. The
|
1 |
It is often stated that with Figure 15.5 one needs only to "multiply the 'risk' by the number dosed," to obtain an absolute value of Nca . This is unsatisfactory for PH purposes because this applies only to each DP group separately, when what is needed is the accumulated increments of dose and response for the entire dosed population. Thus, data external to the function are required. |
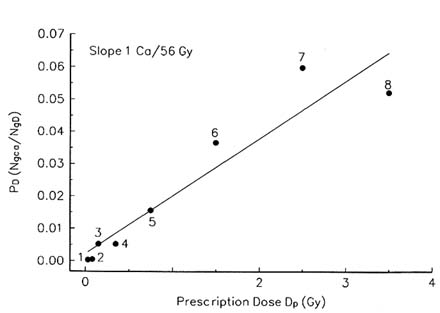
FIGURE 15.5 A plot frequently employed to display cancer data obtained from the atomic bomb survivors. Values for the absolute number of (persons with) an excess cancer are not obtainable from this graph.
result would be Nca alone on the ordinate, and ![]() (or ND) on the abscissa, both proper coordinates for PH functions.
(or ND) on the abscissa, both proper coordinates for PH functions.
However, as shown in Figure 15.6, a first step in this direction has already been taken with the introduction of the hybrid quantity person-Gy, i.e., NDDP. Thus, although this function may be regarded as representing some improvement over Figure 15.1, in that ND now appears on the abscissa, it alone is still inadequate for PH purposes because person-Gy retains the non-additive unit of Gy. Also, the ordinate cannot yield more than about 80 cancers, about one third of the total of 245 induced.
To remedy the problems with Figure 15.6, it is necessary to recognize that each member of the population, a person who has received a determinable amount of energy, is an element of the defined population system of ∼40,000 dosed persons, and that the total amount of imparted energy transferred to the system, on which the total cancer yield depends, is determinable only by summing over all increments of agent delivered to the elements. Such a suitable quantity can be obtained from the person-Gy in Figure 15.6 by multiplying this hybrid quantity by the mass of

FIGURE 15.6 Number of solid cancers in the atomic bomb survivors, plotted as a function of person-Gy. Note that the actual yield, 245 cancers, is not reachable using this plot.
a person (mass of the average atomic bomb survivor, taken to be 55 kg). The resulting quantity, ![]() , being extensive, is additive and dependent on the mass of the system.
, being extensive, is additive and dependent on the mass of the system.
Figure 15.7 shows the results of a conversion, dose group by dose group, of person-Gy to ![]() , but without summation over the groups. Although this does yield coordinates in terms suitable for PE, it still fails to yield the correct number of induced cancers. Figure 15.8 shows the results of summing
, but without summation over the groups. Although this does yield coordinates in terms suitable for PE, it still fails to yield the correct number of induced cancers. Figure 15.8 shows the results of summing ![]() over all groups (this is not extrapolation but rather calculation of the energy imparted to the entire system). It is only this function that can represent the PE data—that is, 245 induced solid cancers—completely and accurately, with no requirement for additional external information.
over all groups (this is not extrapolation but rather calculation of the energy imparted to the entire system). It is only this function that can represent the PE data—that is, 245 induced solid cancers—completely and accurately, with no requirement for additional external information.
The fact that only the summed increments yield the correct number of cancers reinforces the major point made earlier: that is, an additive quantity or number (![]() or ND) that is dependent on the mass of the system must appear as the independent variable. This confirms the fact that the function in Figure 15.5 cannot be appropriate for the PH situation.
or ND) that is dependent on the mass of the system must appear as the independent variable. This confirms the fact that the function in Figure 15.5 cannot be appropriate for the PH situation.
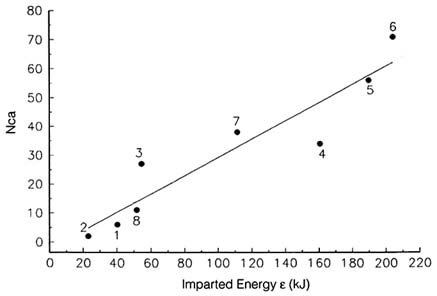
FIGURE 15.7 Absolute solid tumor yield as a function of partial summations of imparted energies in the constituent groups. The total of 245 cancers does not appear on this plot.
It is often claimed, incorrectly, that "doses" (![]() /m) are additive if delivered to the same mass, or different masses of nominally the same value, e.g., the weights of radiation workers. However, additivity in such situations is illusory. The summation performed under these circumstances is not Σi (
/m) are additive if delivered to the same mass, or different masses of nominally the same value, e.g., the weights of radiation workers. However, additivity in such situations is illusory. The summation performed under these circumstances is not Σi (![]() /ms) but rather 1/ms Σi (
/ms) but rather 1/ms Σi (![]() ). Thus it is actually
). Thus it is actually ![]() that is being summed:
that is being summed: ![]() /m is not additive under any circumstances.
/m is not additive under any circumstances.
Cellular Analysis
We return now to the anomaly alluded to above: namely, why, as shown in Figure 15.5, do the cancer data yield a linear function, even though plotted on MT coordinates, are expected to yield a threshold-sigmoid function? The answer begins with the fact that, although overt cancers obviously appear only at the organ-organism level, essentially all human cancers originate at the cell level. Furthermore, there appears to be a one-to-one relationship, that is, one overtly expressed cancer represents one completely transformed cell. This means that the relevant question is not precisely that asked in the first sentence above, but rather,
Why do cell quantal responses yield a linear function when plotted on MT axes that traditionally have yielded a threshold-sigmoid function?
First, the root of the problem is a disparity in the levels of biological organization: the response is at the cellular level, while the physical insult DP applies only at the tissue level. But DP at the higher organizational level cannot provide any information on what happens at the cell level. The solution lies in removing the disparity and recognizing that one can obtain either a linear or a threshold-sigmoid function entirely at the cellular level, just as was done above for the organ-organism level. This places both response and physical insult entirely at the level where the causative interaction between cells and a radiation field transpires. With respect to a threshold and curvilinearity at the cell level, such a function, termed a ''hit size effectiveness function" (HSEF), has been described (Bond et al., 1985; Morstin et al., 1989; Sondhaus et al., 1990). Linear functions associated with the HSEF, with either NH (the number of hits on cells), or ![]() as the independent variable, have been demonstrated (Bond et al., 1995; Sondhaus et al., 1990).
as the independent variable, have been demonstrated (Bond et al., 1995; Sondhaus et al., 1990).
With respect to linear functions at the cellular level, if the radiation quality is held constant at any region of the HSEF, a linear function, Nq as a function of NH (or ![]() ) can be obtained. Therefore, the answer to the original question, or as modified for single cell effects generally, is that, because DP at the organ-organism level is proportional to both NH and
) can be obtained. Therefore, the answer to the original question, or as modified for single cell effects generally, is that, because DP at the organ-organism level is proportional to both NH and ![]() at the cell level, it follows that either a cell response in terms of the number of incipient cancers, or an organ-organism response in terms of Nca, would be linear if plotted against either DP or
at the cell level, it follows that either a cell response in terms of the number of incipient cancers, or an organ-organism response in terms of Nca, would be linear if plotted against either DP or ![]() , with the latter accumulated at either the cell or organ-organism level.
, with the latter accumulated at either the cell or organ-organism level.
Returning now to the linear functions shown in Figure 15.7 and 15.8, and recalling that ND can be used on the abscissa in place of ![]() and that one cancer means one fully transformed cell, it might be attractive to hypothesize that only one hit on (dose to) a susceptible cell may cause a cancer. However, for this to actually happen, and provided that a number of other factors are favorable, the cell single hit dose z1 must be greater than the threshold for the HSEF.
and that one cancer means one fully transformed cell, it might be attractive to hypothesize that only one hit on (dose to) a susceptible cell may cause a cancer. However, for this to actually happen, and provided that a number of other factors are favorable, the cell single hit dose z1 must be greater than the threshold for the HSEF.
The function for mixed solid tumors, obtained from the atomic bomb survivor data, is also unquestionably compatible with linearity (although the data would easily accommodate quadratic, linear-quadratic or other functions) clearly the function is not the threshold-sigmoid type of relationship shown in Figure 15.2. Earlier work with mixed type breast tumors in rats showed a strictly linear dose-response function up to about 4 Gy, where a peaking occurred (Bond et al., 1960). It is tempting to adopt for this phenomenon the same cellular explanation given above, i.e., that, with the microdosimetrically evaluated radiation quality being identical for all values of D, it is only quantity (NH or ![]() ) that could vary.
) that could vary.
However, this explanation for linearity was developed in the context of "low level" radiation, where the microdosimetric cell distribution (z1 spectrum) and its mean, ¯z1, are constant, and the mean number of hits per exposed cell is in the range of 1.0 or smaller. With the linearity continuing to quite high doses, a possible
explanation is that multiple hits on cells, for some endpoints, can act independently, with no interaction up to quite high doses (e.g., 4 Gy).
Another factor that enters with mixed solid tumors is the relatively recent demonstration that, at least for some tumor types, a number of separate mutations, presumably within a stem cell, may be required for the induction and expression of a neoplasm. Supposedly, a large number of environmental agents, including ionizing radiation, can cause any one of these mutations. All such events are presumably independent, and the affected cell does not reveal its carcinogenic potential until the full complement of genetic changes (e.g., five) is attained (Trosko, 1990).
With a short radiation exposure as from the bomb, it is virtually certain that radiation could not have caused more than one of the five or so necessary mutations in any one cell. Also, presumably, that mutation could be number one, five or any number in between. Only in those cells in which the necessary five mutations are induced could the process of expression also be activated; all others would have to await the completion of the five, from other sources of radiation, or other mutagens. Because a simple hit on a cell with (n - 1) hits could be effective, linearity would be expected.
In any event, all excess solid cancers are attributable to a necessary mutation caused by the bomb radiation. Each mutation would have to be regarded as an independent event, especially because the individual mutations are for the most part well separated in time. It is attractive to consider that this independence of event action may play a key role in determining the linearity of response.
Additional Ramifications: Risk Coefficients
In showing that the abscissa of PH functions must be in terms of TD, in units of joules (Figure 15.8) rather than in units of J/kg (Figure 15.6), the numerical value of the risk coefficient (slope of the function) is reduced by a factor equal to the mass of the average person (55 kg for the average atomic bomb survivor). However, because the risk coefficient clearly must be in terms of the amount of the agent energy, the coefficient can be only in terms of TD. Thus, the numerical value of the present risk coefficient (but not the absolute number of tumors) is reduced by the ratio of slopes of the functions in Figure 15.6 and Figure 15.8, i.e., 0.0215/0.00039=55. for the ICRU standard man, the factor would be 70.
The Linear Hypothesis
In Figure 15.8 the PH yield, Nca, as a function of the total amount of the agent energy, has significant consequences with respect to the linear, nonthreshold hypothesis. First, the fact that the abscissa is TD, the actual amount of energy and not its concentration, indicates that this, and not the absorbed dose plot in Figure 15.5, is the appropriate quantity for expressing and evaluating the validity of the hypothesis. Also, as indicated by the inverse of the slope of the function (Bond
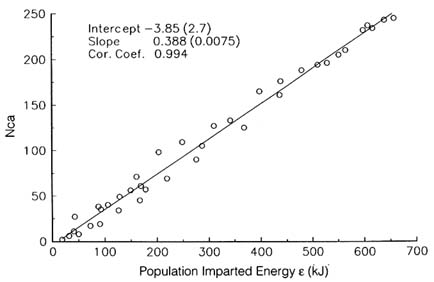
FIGURE 15.8 Absolute solid tumor yield as a function of the total amount of imparted energy. This complete function does show the total of 245 cancers.
et al., 1991), the average amount of radiation energy required to cause a cancer is about 3 kJ (about ten times the acute lethal dose, if delivered to one person). This is not compatible with a conclusion that any amount, however small, may cause a cancer.
To explore the linear hypothesis question further, in Figure 15.9 the group average values of TD required to cause one cancer were plotted as a function of the concentration dose DP (the errors for the first two points are quite large). This makes clear the fact that, however small the energy concentration (absorbed dose) to the average person may be, the quite large (3 kJ) average requirement for one induced cancer remains the same. Also, for this function (Figure 15.9) to be supportive of the linear hypothesis, one would expect the amount of energy required for cancer induction to decrease with decreasing DP. Thus, these findings are incompatible with the linear hypothesis.
A key point is that, with one complete set (table) of relevant data, either type of function can be obtained at will. This shows that it is highly misleading, and the source of enormous confusion, to emphasize that a linear function is "without threshold." Thus, one agent cannot be described simultaneously as being so extremely toxic that there is no threshold for a lethal response, on the basis of one function derived from a given complete set of data, and then described as being

FIGURE 15.9 Average amount of energy required per induced solid tumor (3 kJ), as a function of absorbed dose. This value remains the same, however small the energy concentration (absorbed dose) may be.
so benign as to have a substantial threshold, on the basis of another very different function derived from the identical set of data. Because threshold-sigmoid and linear relationships are completely different functions, it is nonsensical to state or imply that any of the characteristic features of one should also apply to the other.
Lastly, apparently quite convincing to defenders of the linear, nonthreshold hypothesis is the fact that, using cellular systems, a loss of statistical significance of the response as DP is reduced can be overcome by including a suitably larger number of cells. This is done to "improve the statistical significance." However, this argument is fallacious because the independent variable, DP, being intensive and thus not dependent on mass, will remain precisely at the same location, even though the increase in the number of exposed cells may have produced many more quantally responding calls. This gives the impression that one can defy thermodynamic laws and produce more responding cells with no additional expenditure of energy. However, if the extensive, and thus mass-dependent and additive quantity, TD, is used as the independent variable, any addition of mass (e.g., cells) and thus energy at a statistically weak point, will force that point upward on the function (Bond et al., 1995). This fact removes any defensible basis for extrapolation of the
function downward from the region in which statistically reliable actual response data are obtainable.
Discussion And Conclusion
Strong arguments can be made from basic MT considerations that DP (![]() /m) is a measure of agent quality, and TD (
/m) is a measure of agent quality, and TD (![]() ) a measure of radiation quantity (amount). Accordingly, the plots with these two independent variables would be termed quality and quantity functions, respectively. Because substantial space would be required to develop this theme, and because it would further complicate an already difficult subject, it was not included in this paper.
) a measure of radiation quantity (amount). Accordingly, the plots with these two independent variables would be termed quality and quantity functions, respectively. Because substantial space would be required to develop this theme, and because it would further complicate an already difficult subject, it was not included in this paper.
Had the idea of separate quality and quantity functions been developed, a family of linear functions, rather than only one, could have been provided in Figure 15.3. In historic and classical MT functions (Figure 15.1), agent concentration has been used extensively as the most relevant physical measure of agent quality (but always recognizing that the biological response must be the final judge of agent quality). By this measure, the increase in effectiveness with agent concentration (absorbed dose) in Figure 15.1 represents an increase in agent quality.
A strong emphasis on "risk" diverts one from the primary practical responsibility of both the public health officer and the epidemiologist. This is the proper collection of data on the actual number of quantal responses in a given population, for example, the 245 observed excess cancers in a sample of the atomic bomb survivors (a measure of the severity of effect on the dosed population, but not on the individual). Although these data may later be used to formulate probabilities, only observable excess tumors can play a role in determining the primary PH outcome, the absolute number of excess cancers observed. In other words, the overall exercise is clearly a PH problem. Extensive emphasis on average values of "risk" or probability, presumably intended for the individual, projects the incorrect image of the problem being in the MT realm.
The conclusions from the above are: (1) TD or ND, to the total exclusion of DP, are the proper imparted-energy–related independent variables for describing PH data adequately; (2) it is only this approach that can provide the correct total yield of cancers; (3) the PH data do not provide sufficient evidence to even formulate, let alone prove, the linear hypothesis (i.e., linear functions alone cannot provide a basis for it); (4) the numerical value for the risk coefficient for cancers is about 70 times smaller if TD is used, correctly, as the amount of agent energy, than it is when DP is used, incorrectly, as the amount of energy; and (5) the linear, no-threshold hypothesis is flawed.
| This page in the original is blank. |