Effects of Ionizing Radiation: Atomic Bomb Survivors and Their Children (1945-1995) (1998)
Chapter: 6 A Historical Review of Leukemia Risks in Atomic Bomb Survivors
6
A Historical Review of Leukemia Risks in Atomic Bomb Survivors
DALE L. PRESTON
Summary
An excess risk of leukemia was one of the earliest delayed effects of radiation exposure seen in the victims of the atomic bombs dropped on Hiroshima and Nagasaki in August of 1945. Now, more than 50 years after the bombs were dropped, this excess is widely seen as the most apparent long-term effect of radiation. Indeed, death from leukemia is, for many people, a primary symbol of the terrible price paid by the victims of the bombings. Leukemia risks have been a major concern of Atomic Bomb Casualty Commission (ABCC) and Radiation Effects Research Foundation (RERF) researchers. With more than 50 citations in the topical index of the ABCC/RERF Technical Report series (RERF 1992), leukemia is considered in more ABCC/RERF reports than any other single subject. In this paper, I review the history of efforts by scientists of the ABCC and RERF to identify and quantify the excess risks of leukemia in the atomic bomb survivors. The report begins with a discussion of efforts to identify leukemia cases. I then discuss how the description and understanding of the leukemia risks in the survivors has evolved over time. I will conclude with a summary of our current understanding of the nature of these risks. This summary is based upon results in recent reports on leukemia incidence (Preston et al., 1994) and mortality (Pierce et al., 1996). In his recent book Jack Schull (1995) provides additional information on leukemia studies at ABCC and RERF.
Ascertainment of Leukemia Cases
As expected based on the limited knowledge available in 1945, medical observers who examined the victims in the immediate aftermath of the bombs noted severe acute effects on the hematopoietic system of heavily exposed survivors. At that time it was not clear whether or not survivors would experience an increased risk of leukemia, but there was concern that this might be the case. The documents dealing with the establishment of ABCC in 1946 and 1947 recognize, among other things, the need to look for cases of leukemia among the survivors. The first major non-genetic study conducted at ABCC was a clinical survey of the hematological status of survivors and controls carried out in 1947 and 1948. The survey included about 925 exposed persons, primarily children, who reported epilation and a similar number of unexposed controls sampled from the nearby city of Kure. In the report on this survey (Snell et al., 1959) no prevalent cases of leukemia were found among those examined.
However, by the late 1940s Japanese physicians—principally Yamawaki Takuso, a pediatrician at the Hiroshima Red Cross Hospital, and Tomonaga Masanobu, a hematologist at Nagasaki University—were becoming concerned about an apparent excess of leukemia cases among the survivors. They felt that evidence for an elevated risk was especially strong for those who were within 1,000 m of the hypocenter at the time of the bomb. Dr. Yamawaki reported his observations to Wayne Borges. These initial observations led to the commencement of a series of ABCC leukemia surveys. The first of these surveys was carried out under the direction of Drs. Borges and Yamawaki, together with Jarrett Folley, Yamasowa Yamamichi, and William Valentine in Hiroshima and, in Nagasaki by Dr. James Yamazaki with the cooperation of Dr. Tomonaga and others at Nagasaki University. The first ABCC report dealing with the elevated leukemia risks is a memorandum written by Valentine (1951). In addition to the ABCC efforts to record leukemia cases, Dr. Watanabe Susumu of Hiroshima University undertook an independent effort.
The ABCC leukemia surveys continued with varying levels of intensity throughout the 1950s. Published reports (Folley et al., 1952; Moloney and Lange, 1954; and Brill et al., 1962) suggest that major efforts to update the leukemia data were made in 1951, 1953, and 1957. These surveys attempted to ascertain all cases of leukemia and related disorders (including lymphoma, aplastic anemia, and myeloma) among survivors resident in the areas around Hiroshima and Nagasaki. Cases were identified on the basis of diagnoses at or referrals to ABCC, records from local hospitals, examination of Hiroshima and Nagasaki death certificates, autopsy reports, and even, in the early years, newspaper reports of survivor deaths. Until the 1960s there appear to have been no consistent standards for case ascertainment or review. In addition, the surveys were conducted and, in some cases, the reports were presented separately for Hiroshima and Nagasaki. There was no precise definition of the population of interest or even of whom to consider as a
survivor. (These problems were common to virtually all of the epidemiological studies undertaken by ABCC during its first decade.) The poorly defined population from which cases ascertained in the ABCC Leukemia Surveys were drawn is often referred to as the "open-city" population.
From about 1960, Stuart Finch led an effort to improve the quality of the leukemia survey data by standardizing data collection and review procedures. This lead to the formal establishment of the ABCC Leukemia Registry (Finch, 1965a, 1965b; Belsky, 1972). The Leukemia Registry operations manual prescribed that cases be collected for all "survivors of the atomic bombs with Honseki [place of legal family registration] in Hiroshima and Nagasaki regardless of their present place of actual residence" and for all others seeking care for these diseases in either of the cities. An important aspect of the procedures adopted for the Leukemia Registry was the requirement that detailed shielding histories be obtained and doses assigned for all cases among survivors who were within 2,000 m of the bomb. Data collected for the ABCC leukemia surveys were reviewed and incorporated into the Leukemia Registry. In addition, the Hiroshima data collected by Dr. Susumu of Hiroshima University were also reviewed and added to the registry (Finch, personal communication). The Leukemia Registry was quite active from its inception through the late 1980s.
Between 1985 and 1990 a special effort was undertaken to classify cases in the Leukemia Registry using the French-American-British (FAB) system for the detailed characterization of acute leukemia subtypes, and modern classifications for other leukemia subtypes (Matsuo, 1988). At the same time, efforts were made to identify all cases of adult T-cell (ATL) leukemia in the registry. This latter effort was thought to be important because of the fairly recent discovery that the virus (HTLV-1) associated with ATL was relatively common in the Nagasaki area. it was possible to classify about 64% of the cases in the registry using modern criteria.
Since 1958, the Hiroshima and Nagasaki Tumor Registries (Mabuchi et al., 1994) have been collecting data on the incidence of leukemia, lymphoma, myeloma, and other cancers. For various reasons, until recently the Tumor Registry data (especially in Hiroshima) were not considered adequate for analyses of cancer incidence in the survivors. However, over the past decade, the efforts of Dr. Mabuchi and his colleagues have led to improvements in the quality and completeness of the Tumor Registry data (Mabuchi, 1997). At this time, the Tumor Registries are the primary source of data on new cases of leukemia and related diseases among the A-bomb survivors. While the recent incidence analysis (Preston et al., 1994) used data from both the Leukemia and Tumor Registries, there has been no formal merging of the data from the two sources.
Analyses Of Leukemia Risks In The A-Bomb Survivors
As noted above, the first ABCC report on leukemia was the 1951 memo by Valentine (Valentine, 1951). This memo summarized the findings of the first ABCC
TABLE 6.1 Leukemia cases in Atomic Bomb Survivors 1948–50 (based on data from Folley et al., 1952).
|
Distance from hypocenter (m) |
Population (Est.) |
Observed cases |
Expected cases |
Excess cases |
|
0-999 |
2,071 |
4 |
0.1 |
3.9 |
|
1,000-1,499 |
13,823 |
12 |
0.6 |
11.4 |
|
1,500-1,999 |
23,363 |
6 |
1.0 |
5.0 |
|
2,000 + |
155,970 |
7 |
7.0 |
0.0 |
|
Total |
195,227 |
29 |
8.7 |
20.3 |
leukemia survey covering the years from 1948 through 1950. In 1952, Folley et al. published a report on the data presented in the Valentine memo. Table 6.1 shows the distribution of the 29 leukemia cases (19 from Hiroshima, including 4 cases among the 925 people examined during the 1947 hematological survey) considered in this paper, by distance categories. The table also includes estimates of the number of expected and excess (observed minus expected) cases computed by application of the crude rate for survivors in the 2,000 m+ category to survivors in the other distance groups. Despite uncertainties about the completeness of case ascertainment or the accuracy of the population size estimates, evidence for an excess risk of leukemia associated with the atomic bomb exposure is compelling.
Folley et al. (1952) note that the cases were primarily acute leukemias or chronic myelogenous leukemias, and that acute cases seemed most common in the proximal group. While Valentine had concluded that there was some suggestion that the youngest survivors might be at greater risk than those exposed later in life, Folley et al. were careful not to emphasize this possibility.
In 1953 William Moloney, a hematologist, became chief of medicine and organized a series of reports (Lange et al., 1954; Moloney, 1955; Moloney and Lange, 1954; Moloney and Kastenbaum, 1955) describing leukemia incidence through 1952. Based on 75 cases (52 in Hiroshima) that had been found among the survivors, it was concluded that there was clearly an excess risk of leukemia and that this excess appeared to decrease in a manner that was roughly linear in the logarithm of distance. As in the earlier reports, it was noted that the cases were predominately acute types and chronic myelogenous leukemia, while chronic lymphocytic leukemia was extremely rare in the survivors regardless of distance. The authors indicated that age at exposure and sex had no apparent effects on the risks. In a summary of the results that appeared in the New England Journal of
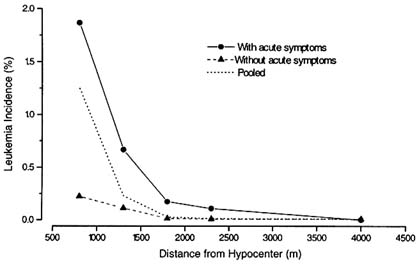
FIGURE 6.1 Leukemia incidence in A-bomb survivors (1948–55) based on Moloney and Kastenbaum (1955).
Medicine, Moloney (1955) emphasized that ''whereas a large single dose of ionizing radiation was required for leukemogenesis in survivors, repeated smaller doses under other circumstances may have a greater leukemogenic effect." Moloney and Kastenbaum (1955) carried out an analysis of leukemia incidence by distance for Hiroshima survivors with and without acute radiation symptoms (epilation, oropharyngeal lesions, or purpura). Figure 6.1 summarizes these data (a similar figure is given by Schull, 1995).
Table 6.2 presents the estimated numbers of survivors with and without acute symptoms, as reported by Moloney and Kastenbaum. The population size estimates in this table are considerably lower, especially for the most proximal and distal groups, than in the initial reports (Table 6.1). These changes reflect the results of ongoing surveys of the survivor populations and the uncertainties inherent in any effort to carry out analyses of the ill-defined "open-city" population from which cases were being drawn.
Rising public concern over the possible health effects of atmospheric nuclear testing led to a paper in Science (Lewis, 1957) that used leukemia data from ABCC and data on the dose-versus-distance estimates from the York air-dose curves, as presented by Neel and Schull (1956), to arrive at an estimate of 2 excess leukemia cases per million person-years. These were the first published quantitative cancer risk estimates based on the ABCC data. In response to the Science article, Wald (1958) published a short updated summary of the Hiroshima leukemia data, stressing the point that uncertainties in dose estimates meant that efforts to quantify the
TABLE 6.2 Estimated numbers of survivors and survivors' acute symptoms by distance from hypocenter (from Moloney and Kastenbaum, 1955).
|
Distance from hypocenter (m) |
Population (Est.) |
Acute Symptoms |
% |
|
0 - 999 |
1,200 |
750 |
63 |
|
1,000-1,499 |
10,500 |
2,250 |
21 |
|
1,500-1,999 |
18,700 |
1,750 |
9 |
|
2,000 + |
50,500 |
850 |
2 |
|
Total |
98,100 |
6,550 |
7 |
leukemia risks were premature. A review of hematological findings, including the leukemia results, during the first decade after the bombs was published by Wald et al. (1958).
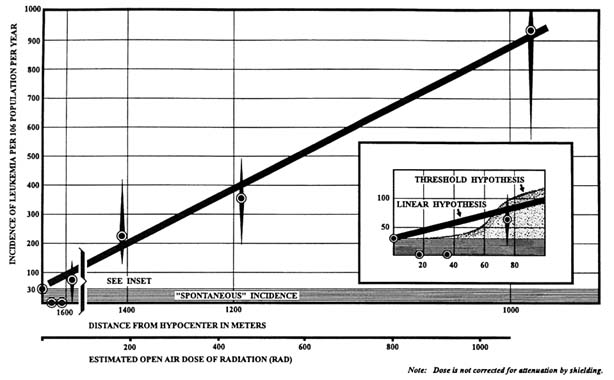
The third ABCC leukemia survey covered the period through 1958. The results were described in a series of papers (Heyssel et al., 1959; Tomonaga et al., 1959; Brill et al., 1962) that appeared in the first year of the ABCC Technical Report series. By this time a total of 209 leukemia cases had been reported in the survivors. However, for their primary summary, the investigators decided to limit attention to those cases that had occurred among members of the newly created Life Span Study (LSS) cohort. (In the papers mentioned above, the LSS is called the Master Sample, a term that is currently used to refer to the larger population from which the LSS was selected.) Limiting the data to cases among LSS cohort members reduced the number of usable cases to 95. These reports also presented some of the first dose-response curves to appear in ABCC publications. Figure 6.2 is a reproduction of the Hiroshima dose-response curve from Heyssel et al. (1959). It was found that the dose response was consistent with linearity in dose.
The reports on the ABCC leukemia survey noted that excess risks were higher among those exposed under the age of 10, and that men had greater excess risks than women. Observed risks were also observed to have been increased from 18 months to two years after exposure. Although risks were still elevated, the excess seemed to have peaked at some time between 5 to 10 years after exposure. Although the papers presented data on the dose response, it was noted that the risks in Nagasaki were higher than those in Hiroshima, suggesting that there were some problems with the York-curve-based T57D dose estimates. Brill et al. (1962) noted that by the late 1950s more leukemia cases had already been seen among proximal survivors than would be expected in their lifetimes and argued that this could serve to refute the notion that the excess could be explained in terms of accelerated aging
(i.e., that the excess cases were simply cases that would have been seen later in life, but exposure had simply hastened their development).
The next comprehensive report on the leukemia data (Ishimaru et al., 1971) considered leukemia cases in the LSS for the 1950 to 1966 period. This was one of the first major ABCC reports to make use of the T65D dosimetry. At this time there were 279 cases in the Leukemia Registry, but only 117 of these people were members of the LSS. It was reported that while the excess risk had peaked in the early 1950s, risks among the survivors were elevated throughout the study period. The results appeared to support earlier observations that the magnitude of the excess depends on age at exposure and sex. Excess risks were higher in Hiroshima than in Nagasaki, and the authors suggest that this difference might be due to neutrons. The deficit of CML cases in Nagasaki was also noted, along with a suggestion that a neutron effect was the "most tenable explanation" for this difference. LSS follow-up was extended to 1971 in a report by Ichimaru et al. (1978). This report presents an extensive analysis of age-and-time patterns in the excess risk and makes the point that excess risks appeared to have peaked earliest and at the highest levels for those exposed early in life, while for those who were older at the time of exposure the peak was less sudden, and the excess seems to have continued over a longer period of time.
A series of reports on leukemia incidence was published in 1981. These reports considered leukemia incidence in the LSS for the period from 1950 through 1978 (Ishimaru et al., 1981a; Ichimaru et al., 1981) and in the "open-city" population for the period from 1946 through 1978 (Ishimaru et al., 1981b). By this time the number of cases among LSS cohort members had increased to 181 (149 in Hiroshima), while there had been 509 cases (297 in Hiroshima) in the "open-city" population. The conclusions reached in these analyses were similar to those of the earlier reports. However, it was emphasized that the dose response for acute leukemias appeared to be non-linear, with a large limiting value for the RBE. The report stated that no excess had been seen in Nagasaki since 1970. It also noted that chronic leukemia cases were twice as likely to be seen in Hiroshima (47 of 149 cases) as in Nagasaki (6 of 40 cases). The nature of the dependence of the excess leukemia risks on age at exposure, time, and city were illustrated by Ichimaru et al. (1981) using the schematic diagram shown in Figure 6.3.
The LSS leukemia incidence data of Ichimaru et al. (1981) were also analyzed by Pierce et al. (1983). They used the data to illustrate how new regression-based methods could be used to make inferences about excess absolute or relative risks in the LSS. The methods described and developed in this paper have become the standard methods for virtually all subsequent analyses of mortality and incidence in the LSS and are widely used by researchers concerned with risk estimation in other populations.
Recently Tomonaga et al. (1991) presented an analysis of the data on the "open-city" population for the period from 1946 through 1980. A total of 766 leukemia cases were used in these analyses. Tomonaga and his colleagues discussed the
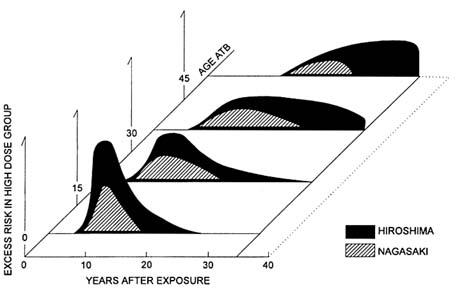
FIGURE 6.3 Summary of the pattern of LSS excess leukemia risks from Ichimaru et al. (1981).
results of the FAB reclassification and used complex statistical methods based on ratios of relative risks to deal with problems caused by the inadequate information about the size of the population covered by the Leukemia Registry. Although the FAB system provides detailed subclassifications for acute myeloid leukemias (AML) and acute lymphocytic leukemias (ALL), the primary analyses were based on the broader classifications of ALL, AML, and chronic myeloid leukemia (CML), supplemented with a group of other leukemias that included adult T-cell leukemia (ATL). The results of this analysis are generally consistent with earlier findings. However, it was suggested that the CML dose response might be relatively more linear at low doses than that for AML.
Current Results
Analyses of the LSS leukemia incidence for the period from 1950 to 1987 were published in 1994 (Preston et al., 1994) as one of a series of reports on cancer incidence in the LSS. In this section I will summarize the results of these analyses. For these analyses, descriptions of the excess risks were given primarily in terms of the excess absolute risk as a function of dose, time since exposure, age at exposure and sex. Preston et al. (1994) present detailed models for the excess
absolute risk for all leukemias as a group and for ALL, AML, CML, ATL, and other leukemias. The analyses focused on leukemia cases among survivors in the LSS cohort who had DS86 shielded kerma estimates less than 4 Gy and who were living in Hiroshima, Nagasaki, or nearby areas at the time of diagnosis. A total of 231 leukemia cases met these criteria. This total includes 32 ALLs, 103 AMLs, 57 CMLs, 23 ATLs, and 16 leukemias of other types. All except one of the ATL cases occurred in Nagasaki survivors.
Table 6.3 presents the number of leukemia cases observed in bone marrow dose categories, by city, for the full follow-up. The table also gives estimates of the number of excess cases for each period in each dose group. These estimates were computed as the difference between the observed and the expected numbers of cases. The expected numbers of cases were computed using the background (zero dose) model for leukemias of all types given by Preston et al. (1994, p. S94). Overall, about one-third of the 231 cases considered here are associated with radiation exposure. There were six additional leukemia cases among the 263 survivors who had DS86 kerma estimates over 4 Gy. It seems likely that all of these cases could be attributed to radiation exposure. There were also 24 leukemia cases among the 7,190 LSS survivors who had an unknown dose. Since most of these survivors were located within 2,000 m of the hypocenter ATB and are likely to have received fairly large doses, it is probable that 50% or more of the leukemia cases can be attributed to the exposure. This would suggest that there were about 100 extra leukemia deaths in the LSS over the 37 years of follow-up covered by this study.
Table 6.4 provides a breakdown of the observed and estimated excess leukemia cases by dose and decade of follow-up. The results indicate that there were appreciable excess risks in all decades except possibly the 1980s. Even in the most recent periods there is a suggestion of a small excess in the highest dose groups.
Figure 6.4 summarizes the temporal pattern of the fitted excess rates by sex for three age-at-exposure groups. This plot is based on the excess absolute risk model in Preston et al. (1994). The pattern of risks is not simple. Generally, risks tended to be largest in the early years of follow-up. Within each age-at-exposure group the peak was higher and subsequent rate of decrease greater for men than for women. The fitted model suggests an increase with time in the EAR for women exposed at age 50. This apparent increase should not be overinterpreted. While the point estimate of the slope is positive, the estimate has a large standard error. Confidence levels for this slope at the 90% level or even lower levels include 0 or even negative values.
Table 6.5 presents observed numbers of cases for five subgroups of leukemia cases in the very low dose (< 0.01 Sv) group and the exposed group, together with the estimated number of excess cases for each type. The excess cases were computed as the difference between the observed cases and the fitted type-specific background models given in Preston et al. (1994). Because these results were based on separate models, the total number of excess cases differed slightly from that in
TABLE 6.3 Observed and excess LSS leukemia cases by dose category and city, 1950–87.
|
|
Hiroshima |
|
|
Nagasaki |
|
|
Total |
|
|
|
Marrow Dose (Sv) |
Subjects |
Obs. |
Excess |
Subjects |
Obs. |
Excess |
Subjects |
Obs. |
Excess |
|
< 0.01 |
26,711 |
59 |
8.2 |
18,481 |
31 |
1.3 |
45,192 |
90 |
9.4 |
|
0.01 - 0.1 |
17,727 |
26 |
-7.9 |
5,589 |
12 |
3.5 |
23,316 |
38 |
-4.4 |
|
0.1 - 0.2 |
4,946 |
7 |
-2.6 |
940 |
1 |
-0.5 |
5,886 |
8 |
-3.1 |
|
0.2 - 0.5 |
5,127 |
26 |
16.3 |
1,265 |
1 |
-1.1 |
6,392 |
27 |
15.2 |
|
0.5 - 1 |
2,309 |
20 |
15.7 |
998 |
4 |
2.4 |
3,307 |
24 |
18.1 |
|
1 - 2 |
1,157 |
20 |
17.8 |
637 |
7 |
5.9 |
1,794 |
27 |
23.7 |
|
2+ |
339 |
15 |
14.5 |
105 |
2 |
1.9 |
444 |
17 |
16.3 |
|
Total |
58,316 |
173 |
61.8 |
28,015 |
58 |
13.4 |
86,331 |
231 |
75.2 |
TABLE 6.4 Observed and excess LSS leukemia cases by dose category and time period, 1950–87.
|
Marrow |
1950–60 |
|
1961–70 |
|
1971–80 |
|
1981–87 |
|
|
Dose (Sv) |
Obs. |
Excess |
Obs. |
Excess |
Obs. |
Excess |
Obs. |
Excess |
|
<0.01 |
21 |
5.3 |
18 |
-1.5 |
30 |
5.4 |
21 |
0.2 |
|
0.01 - 0.1 |
5 |
-3.3 |
8 |
-2.2 |
15 |
2.0 |
10 |
-0.9 |
|
0.1 - 0.2 |
4 |
1.8 |
1 |
-1.7 |
3 |
-0.4 |
0 |
-2.8 |
|
0.2 - 0.5 |
10 |
7.7 |
9 |
6.1 |
6 |
2.4 |
2 |
-1.0 |
|
0.5 - 1 |
14 |
12.9 |
5 |
3.5 |
4 |
2.2 |
1 |
-0.5 |
|
1 - 2 |
13 |
12.4 |
9 |
8.2 |
3 |
2.0 |
2 |
1.2 |
|
2+ |
11 |
10.9 |
1 |
0.8 |
3 |
2.8 |
2 |
1.8 |
|
Total |
78 |
47.7 |
51 |
13.2 |
64 |
16.3 |
38 |
-2.0 |
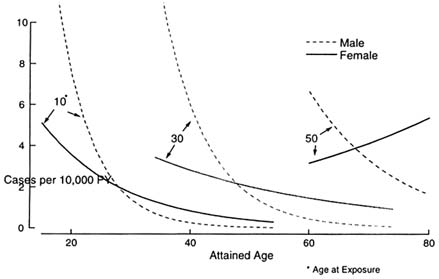
FIGURE 6.4 Temporal patterns of excess leukemia at (ERR1Sv) by sex and age at exposure (Preston et al., 1994).
the earlier tables. The only group for which there is no evidence of an excess risk is the ATL leukemia group. For the other specific types and the "Other" category, radiation appears to account from 50 to 75% of all of the cases among those with significant exposures.
Based on a joint analysis of the ALL, AML, and CML data, Preston et al. (1994) concluded that while the CML dose response seems more linear than that for the other types, the evidence for this is weak, and it is not possible to reject a the hypothesis of a non-linear dose response with the same shape for these three groups. However, they also found that there are significant subtype differences in the sex, age at exposure, and time-dependence of the excess risks.
Conclusions
It has been more than 45 years since it became clear that the Hiroshima and Nagasaki survivors had an increased risk of developing leukemia. During this time the scientists and staff at ABCC and RERF, with the cooperation and support of the survivors and the local medical and medical research communities, have carried out extensive investigations of the nature of this risk. While excess leukemia risks have been seen in other radiation-exposed populations, the ABCC/RERF data provide the most detailed description and serve as the primary source of quantitative
TABLE 6.5 Observed and excess LSS leukemia by exposure category and subtype, 1950–87.
|
|
Observed cases |
|
|
|
Subtype |
<0.01 Sv |
0.01-4 Sv |
Excess |
|
ALL |
9 |
23 |
17 |
|
AML |
43 |
60 |
30 |
|
CML |
17 |
40 |
26 |
|
ATL |
14 |
9 |
-2 |
|
Other |
7 |
9 |
6 |
estimates of these risks. In what follows, I will offer some brief comments and opinions on several issues of ongoing concern regarding leukemia in the A-bomb survivors.
While there is clear evidence of a radiation dose response for leukemia, there are a number of questions about the nature of these risks at low doses. The first of these concerns whether or not there is a threshold exposure below which no excess leukemia risk is seen. With the possible exception of CML (for which the dose response may be somewhat more linear than for other types), the leukemia dose response in the survivors is non-linear, with low doses having a smaller effect than would be predicted by linear extrapolation from high doses. However the LSS data do not offer convincing evidence of a threshold. Indeed these data can rule out thresholds of 0.5 Gy or more, and threshold models do not offer substantial improvements in fit over a simple linear-quadratic model. A related question concerns whether or not low doses, e.g., below 0.1 Sv, have a protective effect. The models developed by Preston et al. (1994) included no explicit constraints for non-negative low dose risks but the dose-response parameter estimates were all positive. Thus, while the LSS data cannot rule out this possibility, they also offer no real evidence of the existence of such an effect. An important question regarding radiation effects on leukemia that cannot be answered by the survivor studies concerns the effects of protracted, low-dose rate exposures. Recent combined analyses of data on nuclear workers in several countries (Cardis et al., 1995a) suggest that there may be elevated risks associated with such exposures, as do preliminary analyses of workers (Koshurnikova et al., 1994) and the general population (Kossenko and Degteva, 1994) with chronic radiation exposures resulting from plutonium production at the Mayak facility in the former Soviet Union.
Another question that arises in most discussion of the LSS leukemia data concerns the nature of differences in the dose response for Hiroshima and Nagasaki. There are important differences in background leukemia rates in the two cities. CML background rates in Nagasaki are about one third of those in Hiroshima, and ATL accounts for about 40% of the Nagasaki cases but almost none of the Hiroshima cases. In addition there are a number of unresolved questions about the accuracy of the Hiroshima neutron dose estimates (Straume et al., 1992). However, despite these issues, current analyses fail to demonstrate significant differences in the excess risks for the two cities for all leukemias as a group. There is however, a significant difference in absolute risks for CML considered by itself, which is proportional to the large difference in CML background rates.
The primary question that arises with respect to temporal patterns is whether or not the excess risk has disappeared. Since about 1970 it has often been stated that the excess is no longer apparent, especially in Nagasaki. The data presented in Table 6.4 suggest that excess risks were apparent at least until the end of the 1970s and, at least for heavily exposed survivors, into the 1980s. The LSS data also suggest that for those exposed as adults, risks have continued throughout their lifetimes. While it is certainly true that risks have fallen dramatically with time, especially for those exposed as children, continued follow-up of this population remains important for our understanding of the complex nature of the leukemia risks. As for the question of whether or not Nagasaki risks have disappeared, as noted above there is no convincing evidence that the temporal patterns or the level of the excess risks (except possibly for CML) in Nagasaki differ from those in Hiroshima.
As data on the experience of the survivors accrue, increasing attention is being focused on radiation effects on cancer incidence and on noncancer effects. However, it will also be important to continue to monitor and analyze leukemia incidence in the LSS, as there is undoubtedly more that can be learned from this population about this important long-term effect of radiation exposure.
| This page in the original is blank. |