Effects of Ionizing Radiation: Atomic Bomb Survivors and Their Children (1945-1995) (1998)
Chapter: 3 Medical Radiation Exposures of Atomic Bomb Survivors
3
Medical Radiation Exposures of Atomic Bomb Survivors
KAZUO KATO, WALTER J. RUSSELL, AND KAZUNORI KODAMA
Summary
The medical dosimetry program of the Radiation Effects Research Foundation (RERF), formerly the Atomic Bomb Casualty Commission (ABCC), in Hiroshima and Nagasaki has been conducted since 1961. Information concerning the medical radiation exposures of the Adult Health Study (AHS) participants was obtained continually through interviews by specially trained personnel at ABCC/RERF. A series of hospital and clinic surveys in the two cities have revealed the activity of the medical radiation exposures among the atomic bomb survivors. Repeated phantom dosimetry has been conducted to determine the radiation doses to the subjects. Preliminary calculations revealed that 39% of the members of the AHS population received cumulative active bone marrow doses exceeding 1 cGy by the end of 1982. This means that the doses from diagnostic x-ray examinations had already become significantly great contaminates of the radiation doses from the atomic bombs. The radiation therapy received by the atomic bomb survivors is also studied in this dosimetry program. Radiation treatments of 1,670 members of the Life Span Study population were detected in surveys through 1984, and the studies are focused on the primary cancers that have developed after radiation therapy.
Introduction
Risk evaluation in the low-dose region using the atomic bomb data is indispensable for estimating the risk of ionizing radiation exposures in catastrophes such
as nuclear reactor accidents and nuclear warfare. However, the atomic bomb data have relatively large uncertainties in the low-dose region, as introduced by Kato et al. (1987). The atomic bomb survivors have not only received ionizing radiation from the A-bombs but also from medical procedures. Such medical radiation exposures have probably contributed to some increases in cancer incidence among the A-bomb survivors, and this is one of the reasons why the atomic bomb data have large uncertainties in the low-dose region. Quantitative assessments of such contributions have been continuing at the Atomic Bomb Casualty Commission (ABCC)/Radiation Effects Research Foundation (RERF) since 1961. The assessments included several series of surveys of medical radiation exposures, which revealed the trends of medical radiation exposures at the institutions in Hiroshima and Nagasaki. These surveys were performed mainly in order to estimate the individual cumulative medical doses received by the members of the Adult Health Study (AHS) who routinely visited the ABCC/RERF. The number of medical radiation exposures by body site and by type of radiation source were documented from the interviews of the AHS participants during such routine visits. Every radiological examination conducted on the AHS participants at RERF has been documented in detail. The doses incurred by medical radiation exposures were estimated by phantom dosimetry experiments and measurements of outputs of radiological units at the hospitals and clinics in both cities. The results of the interview data and phantom dosimetry enable us to evaluate the individual doses to the AHS participants from the diagnostic x-ray examinations.
During radiation therapy, patients receive relatively large doses which are important for evaluating the radiation risks using epidemiological data of the atomic bomb survivors. In our studies, a large-scale survey was performed and devoted to investigating radiation therapy among the members of the Life Span Study (LSS) at RERF. During this survey, records of members who received radiation treatments were transcribed and later reproduced using human phantoms to estimate the organ doses. This study is now in progress.
Hospital And Clinic Surveys
Practices of Hospitals and Clinics
Ihno et al. (1963) conducted a hospital-clinic survey in 1962 and 1963 in Hiroshima and Nagasaki. They obtained information concerning the number of exposures by site, type of radiological equipment, and exposure conditions of examinations taken at the hospitals and clinics. The total number of diagnostic x-ray apparatuses surveyed was 50 in hospitals and 54 in clinics. In order to obtain more precise information, Sawada et al. (1971a) carried out a large-scale survey in 1964. The facilities for this survey were all large institutions and 40% of small institutions in both cities. Here, a large institution was a hospital or clinic using more than 10,000 films per year. The number of large institutions was 14 in Hiroshima and 11 in Nagasaki, in 1963. The number of small institutions was 487 in Hiroshima
and 334 in Nagasaki. The survey produced records of yearly totals for films, radiographic, fluoroscopic and photofluorographic examinations, and number of treatments by x-ray and telecobalt from 1945 to 1963. Subsequently, trends in radiological practice in Hiroshima and Nagasaki from 1964 to 1970 were surveyed by Sawada et al. (1979). The survey covered 17 large and 153 randomly sampled small institutions in Hiroshima, and 13 large and 108 randomly sampled small Nagasaki institutions.
A large-scale survey of hospitals and clinics was conducted in 1974 (Sawada et al., 1979; Antoku et al., 1986). During two-week periods in that year, all records of medical x-ray examinations conducted in Hiroshima and Nagasaki large institutions and a 40% random sample of small institutions were collected to confirm exposures and estimate doses by type, frequency, and exposure conditions. The members of the RERF population involved were identified among the examinees. The technical factors used in Hiroshima and Nagasaki medical institutions were also analyzed.
Use of radiation therapy for A-bomb survivors has also been assessed during these surveys mentioned. However, the information lacked sufficient detail, and three additional surveys were conducted only on radiation therapy among the atomic bomb survivors. The first survey was conducted in 1970 by Russell and Antoku (1976). The second survey was performed in 1980 by Pinkston et al. (1981). These two surveys confirmed that 187 members of the AHS population received radiation therapy exposures. After these two surveys of radiation therapy and two pilot studies, a third survey was conducted in 1985, which provided the information necessary concerning radiation therapy received by the LSS population. During the third survey, a survey team visited the responsible hospitals and all radiation therapy records in each hospital were examined. The radiation therapy data were transcribed from the medical records. The number of hospitals surveyed were 8 large hospitals in Hiroshima (one of which was actually located in the city of Kure) and 3 large hospitals in Nagasaki. Other smaller hospitals had ceased administering radiation therapy by the time this survey was conducted. During the three radiation therapy surveys, the radiation therapy data were obtained from the medical records of 22 institutions in Hiroshima and 8 institutions in Nagasaki, and the data on the radiation therapy provided to a total 1,670 members were obtained.
No survey has been conducted since 1985. During this period, modern diagnostic x-ray equipment such as computed tomography and computed radiography have been installed in many institutions. The quality of films has also been improved, and the technical exposure factors seem to have changed. It is not certain whether the medical records of the radiation therapy have been kept for more than 10 years. Only hospital and clinic surveys enable us to obtain the information about the technical exposure factors used in the diagnostic x-ray examinations, and about how radiation treatments were conducted for the atomic bomb survivors.
Trends in radiological practice in the early days were assessed in the two surveys that were performed by Sawada et al. (1971a, 1975). The result of these surveys
is shown in Figure 3.1. The numbers of radiographic examinations in the early days may be uncertain due to the long time lapse before the first survey was undertaken. The figure shows that the number of radiographic examinations steadily increased until 1950 in Hiroshima and until 1953 in Nagasaki. This increase seems to have been caused by more diseases among the atomic bomb survivors in both cities. Takeshita et al. (1978) reported that the number of radiographs taken in Japan rapidly increased from 1960 through 1970. The increases in Hiroshima and Nagasaki in those days were more moderate than those in all Japan as shown in Figure 3.1. This implies that the physicians and patients minimized the use of medical x-ray in both cities. The trends of fluoroscopic examinations in the early days were different from those of radiography. Fluoroscopy was frequently used in Hiroshima. No steady increase in the numbers of fluoroscopy was seen in Nagasaki and in the whole of Japan. The difference between Hiroshima and Nagasaki probably can be explained by the difference in the number of large institutions in the two cities.
The number of examinations by population, sex, and city in 1974 was examined by Sawada et al. (1979). Figure 3.2 shows that the numbers of radiographs per capita in Nagasaki became greater than in Hiroshima. The frequency of fluoroscopy in Nagasaki was still less than in Hiroshima, and both were nearly the same as those in 1970. The number of radiographic and fluoroscopic examinations for the Nagasaki non-AHS male population was significantly larger than those for the other non-AHS populations and for the general population. The reason for this is not clear. The relatively high frequency of x-ray examinations in the AHS population is due mainly to the RERF AHS ''routine" x-ray examinations they received. If the examination at RERF were excluded from analysis, the mean annual x-ray examination frequency for the AHS population would be nearly the same as for those of non-AHS participants.
The radiological examinations detected in the surveys and interviews of the AHS participants mentioned below were tallied by body sites and by city (Ihno et al., 1963; Sawada et al., 1979; Russell et al., 1963). The number of chest examinations far exceeded all others. The number of exposures per examination was examined by Sawada et al. (1979) and was 12-16 in gastrointestinal series and less than 5 in most other examinations. The fewest exposures were made during chest examinations. Thus, more than half the radiographic exposures were from upper GI series due to the many spot films made during fluoroscopy.
Trends in Radiation Therapy
The number of radiation treatments in Hiroshima and Nagasaki found in the hospital and clinic surveys (Sawada et al., 1971a; Sawada et al., 1975) is shown in Figure 3.3. All relatively large hospitals and clinics were selected for these surveys. The number of radiation treatments steadily increased until 1962, but the increase suddenly ceased around 1964 in both cities. The reason for the declines in radiation therapy in those days is now in question.


In the 1964-65 interviews, a total of 150 treatments by radiation were reported by Hiroshima AHS participants, where 102 (68%) were for ailments thought by the subjects to have been benign (Sawada et al., 1967). Of the remaining 48 (32%) of the exposures, only 15 (10%) were thought by the participants to have been for malignant disease. Only two exposures to radiation therapy were reported by Nagasaki AHS participants, both for unknown diseases.
The number of the AHS participants who reported receiving radiation therapy before 1979 was 525 in Hiroshima and 135 in Nagasaki (Pinkston et al., 1981). The first and second radiation therapy surveys confirmed treatment for 143 patients in Hiroshima and 47 in Nagasaki. The confirmation rate was 38% in both cities. The major reasons for this low confirmation rate were unavailability of hospital records, confusion of therapeutic exposures with diagnostic ones, and no hospital or clinic reported. This low confirmation rate was one of the reasons why the third hospital clinic survey for radiation therapy was performed between 1981 and 1984.
By means of the three radiation therapy surveys (Russell et al., 1976; Pinkston et al., 1981; Kato et al., 1996), a total of 1,670 members of the LSS population were confirmed to have received radiation therapy. Among them, 364 patients were neither in Hiroshima nor in Nagasaki at the times of the atomic bombs. The treatments were conducted not only for malignant neoplasms, but also for benign diseases. Among the malignant lesions, carcinoma of the cervix was most frequent, followed by carcinoma of the breast and lung carcinoma. Among the benign lesions treated by radiation were many skin diseases and tuberculosis.
Interviews of the Atomic Bomb Survivors
Ishimaru and Russell (1962) conducted a three-month survey, from April to June, 1961. This was the first survey of medical x-ray exposures of the atomic bomb survivors. It involved a medical questionnaire designed to determine the frequency, location, date, kind of medical x-ray, and part of the body exposed during the past year. The results of the questionnaires aided in determining the numbers of radiographic and photofluorographic units, their location by type of institution and by city in 1961. The total number of subjects who responded to this survey was 1,862:1,303 in Hiroshima and 559 in Nagasaki. For the 1,303 Hiroshima participants included in this study, their ABCC/RERF medical records were compared with answers shown on the questionnaires. The reporting rate was 40%, where the reporting rate was defined as the percentage of reported and confirmed exposures to those documented in ABCC/RERF charts.
Sawada et al. (1967) analyzed the responses to interviews with 5,293 AHS participants in Hiroshima and with 2,221 in Nagasaki in 1964 and 1965. From their responses, the frequency of exposures was 0.34 among the Hiroshima males, 0.25 among Hiroshima females, 0.13 among the Nagasaki males, and 0.09 among Nagasaki females.
Sawada et al. (1971b) conducted two pilot studies on the responses of the AHS participants regarding radiological examinations. The first study was performed
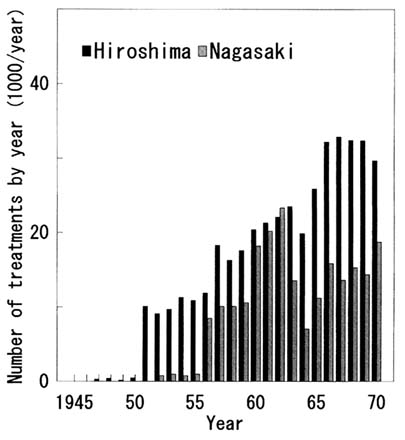
FIGURE 3.3 Radiation treatments by year in Hiroshima and Nagasaki (Sawada et al., 1971; Sawada et al., 1975).
in 1966, where a self-administered questionnaire was completed by 100 AHS participants. Eighteen participants either reported fluoroscopic examination at ABCC/RERF, or were recorded as having had at least one. Among them, 7 participants did not report any fluoroscopic examinations at ABCC/RERF. The reports by the remaining 11 participants were not confirmed by the records, or had some errors as to number, date, body site, or type of examination. This showed that an appropriate interview is necessary to obtain correct responses from AHS participants. The second pilot study was performed in 1966 and 1967. In this study,
one primary specially trained member of the clerical staff and one alternate interviewed 454 AHS participants. Agreement of responses and records was markedly improved over the first pilot study. For example, 101 participants had records of fluoroscopy at ABCC/RERF, and 86 participants correctly reported that they had received fluoroscopy examinations at ABCC/RERF.
Yamamoto and Fujita (1977) analyzed the data from the medical history questionnaires completed by the AHS participants from 1 April 1965 to 31 December 1967. For diagnostic x-ray, 50% of the total from both cities reportedly experienced exposure since their last ABCC/RERF examination, 20% within the three months prior to interview. The affirmative response rates for radiation therapy exposure were 2.6% in Hiroshima and 1.6% in Nagasaki; and for occupational exposure, 0.5% and 0.2%, respectively. Neither radiation therapy nor occupational exposure rates differed significantly by A-bomb dose or age.
The dates of GI examinations reported by 240 AHS participants in 1982 were compared with those of the medical records at the hospitals involved (Yamamoto et al., 1988). Positive responses were regarded as correct when they agreed completely with hospital records, and within three months before or after of the examination date. In this study, there was 81% agreement of responses.
From December 1967 in Hiroshima and January 1968 in Nagasaki, data on medical radiation exposures of AHS participants were continuously obtained by interviews. The routine interviews were conducted mainly by clerks who had special knowledge of radiology.
Dosimetry
Dosimetry of Diagnostic X-Ray Exposures
In 1963, Ihno and Russell (1963) estimated the doses to gonads and active bone marrow by diagnostic x-ray examinations. This work consisted of the application of experimental data by Epp et al. (1961, 1963) to the records of radiographic examinations at the ABCC/RERF. For example, the mean bone marrow dose for a chest projection using a tube voltage of 100 kVp, current multiplied by exposure time of 7.5 mAs, and source-to-film distance of 72 in was estimated to be 28 µGy,
In order to determine the active bone marrow doses from measurements of absorbed doses, Russell et al. (1966) measured the active bone marrow distribution in the human body. A phantom comprised of a human skeleton was used whose size and body weight were approximately 156 cm and 53.5 kg, which were those of the average Japanese adult in 1964. The results were used in the dosimetry work at RERF.
Bone marrow and gonadal doses from diagnostic x-ray exposure were determined in a previous series of dosimetry studies (Antoku et al., 1965, 1971, 1972, 1973, 1980; Takeshita et al., 1972). The phantom used was a Mix-D phantom containing a human skeleton and beeswax impregnated cellulose to represent lung tissue. The absorbed doses were measured using Memorial polystyrene condenser
ionization chambers made in the Department of Medical Physics of the Sloan-Kettering Institute, New York. Surface doses and x-ray outputs were measured using an Electronic Instruments Limited dose meter, model 37A, equipped with a 35-cc polystyrene ionization chamber. Several examples of the doses incurred from the diagnostic x-ray examinations at ABCC/RERF are shown in Table 3.1. The outputs of the x-ray equipment at ABCC/RERF were measured and the doses were determined for the actual examination conditions. The outputs of the diagnostic x-ray equipment at the institutions in Hiroshima are shown in Figure 3.4. As shown in this figure, the outputs varied. This means large errors might have resulted in estimating doses without correction for output. To minimize the discrepancies in radiation output and quality between the units in the hospitals and clinics and the experimental units, 218 radiography units and 49 photofluorography units in both cities were assessed for radiation output and quality. Together with the exposure factors obtained in the hospital and clinic surveys, the doses to patients from x-ray examinations conducted in Hiroshima and Nagasaki were determined. A part of the results is shown in Table 3.2.
Kato et al. (1991a, 1991b, 1991c) continued phantom-based dosimetry research to estimate doses to the salivary glands, thyroid gland, lung, breast, stomach, and colon incurred by radiological examinations. In these studies, an adult female human phantom made by Alderson Research Laboratories was used. Radiological examinations were reproduced and the organ doses were measured by Mg2SiO4(Tb) thermoluminescent detectors (Kasei Optonix, MSO-S).
Each detector was calibrated using an ionization chamber (Exradin A2 Shonka-Wycoff chamber). Experiments were performed using the radiological equipment at RERF and also those at several institutions in Hiroshima. Organ doses from typical radiography and fluoroscopy at RERF are shown in Table 3.3. The doses from upper gastrointestinal series were adjusted so that the maximum skin dose was the same as that determined in the prior study of dosimetry. The critical organ doses were determined for the other types of examinations. For example, doses from computed tomography (CT) were determined as shown in Table 3.4. In this text, active bone marrow dose is absorbed dose averaged over the whole active bone marrow in the human body. Active bone marrow exposed to the CT direct beam receives relatively high doses. For example, a rib dose of 5 cGy/examination was observed during a chest CT.
The first record of a CT examination of an AHS participant appeared in 1977, and the numbers of records rapidly increased. The AHS participants reported approximately 200 examinations in 1983, as shown in Figure 3.5. They resulted in large increases of doses to the AHS participants. Recently, computerized radiography such as digital subtraction angiography, which reduces dose to a patient, has become more popular. The dosimetry for these radiographs was also conducted in our study, and the results are useful for evaluating individual cumulative doses.
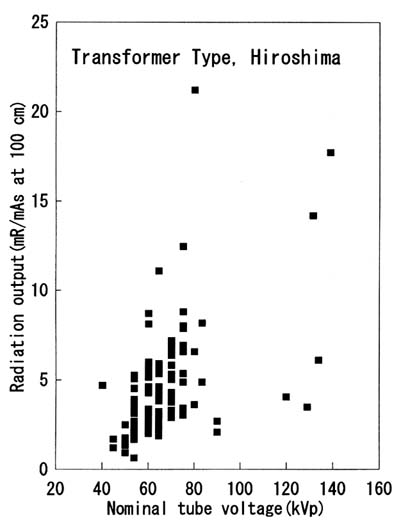
TABLE 3.1 Radiation doses from radiography and fluoroscopy at ABCC/RERF (Antoku et al., 1971).a
|
Projection / site |
Film size (inch) |
Tube voltage (kVp) |
Current × exposure time (mAs) |
Mean bone marrow dose (µGy/exp) |
Gonadal dose (µGy/exp) |
Skin dose (µGy/exp) |
|
|
|
|
|
|
|
Male |
Female |
|
|
PA chest |
14 × 17 |
100 |
5 |
16.5 |
0.2 |
0.4 |
92.1 |
|
Lat. chest |
14 × 17 |
110 |
15 |
31.5 |
0.3 |
0.8 |
370.0 |
|
AP abdomen |
14 × 17 |
100 |
20 |
169.2 |
116.0 |
511.0 |
1,590.0 |
|
AP C-spine |
8 × 10 |
90 |
20 |
27.4 |
0.2 |
0.2 |
981.0 |
|
AP T-spine |
11 × 14 |
100 |
30 |
174.0 |
1.9 |
2.6 |
2,490.0 |
|
AP L-spine |
11 × 14 |
100 |
30 |
245.7 |
147.0 |
704.0 |
2,210.0 |
|
Flx-A upper GIb |
- |
90 |
|
325.0/min |
124.0/min |
811.0/min |
12,200.0/min |
|
Flx-B upper GIc |
- |
90 |
|
68.9/min |
3.5/min |
128.0/min |
3,280.0/min |
|
Upper GI spot |
8 × 10 |
90 |
PHT |
PHT |
0.7 |
26.8 |
1010.0 |
|
a All projections have added filtration of 2.5 mm Al, except for Flx-B upper GI Spot, which are equal to 3.0 mm Al. b Flx-A: Conventional fluoroscopy. c Flx-B: Image-intensifier fluoroscopy. Source-to-film distance for chest films is 72 in; abdomen, C-spine, T-spine and L-spine are 40 in. |
|||||||
TABLE 3.2 Mean dose from radiography and fluoroscopy at institutions in Hiroshima and Nagasaki (Antoku et al., 1972, 1980).
|
Site of examination |
Mean bone marrow dose (µGy/exam) |
Gonadal dose (µGy/exam) |
Surface dose (µGy/exam) |
|
|
|
|
Male |
Female |
|
|
Chest |
48 |
1.6 |
6.1 |
382 |
|
Abdomen |
375 |
119.0 |
1,500.0 |
7,850 |
|
C-spine |
289 |
<0.1 |
<0.1 |
18,900 |
|
T-spine |
510 |
4.6 |
21.3 |
17,000 |
|
L-spine |
1,281 |
259.0 |
2,340.0 |
53,500 |
|
Upper GI |
1,000 |
66.0 |
2,000.0 |
55,000 |
|
Mass chest |
390 |
2.9 |
16.2 |
6,460 |
|
Mass GI |
2,310 |
210.0 |
1,400.0 |
57,300 |
Dosimetry of Radiation Therapy Exposures
Kato et al. (1994) proceeded to simulate radiation therapy, in which the Alderson Rando adult human female phantom mentioned above was exposed to various kinds of therapeutic radiation. This facilitated measurement of the doses to the salivary and thyroid glands, the lungs, breasts, stomach, colon, ovary, and active bone marrow. Each radiation therapy exposure was studied using its own characteristics and technical conditions. It was therefore necessary to perform various simulated treatments. The radiation sources used were 60Co needles, 3000 Ci 60Co gamma-ray therapy apparatus, and x-ray equipment for radiation therapy at the Research Institute for Nuclear Medicine and Biology, Hiroshima University, and the 4 MeV and 10 MeV linear electron accelerators at Hiroshima University Hospital. Doses were measured using thermoluminescence dosimeters which were used in the study of diagnostic x-ray dosimetry. Ionization chambers (JARP HU5 and Capintec PM-30) were also used for determining the sensitivities of thermoluminescence dosimeters. Radiation therapy for cervical cancer was the most frequent among the treatments found in the surveys. Most of the treatment doses to the cervix were larger than 50 Gy; hence, organs outside the exposure field were also exposed to intense scattered radiation. The method for teletherapy for cervical cancer is relatively uniform, and our results can be compared with those obtained by other studies. Preliminary results are nearly identical to those reported by Stovall (1983) except for the lower and middle energy range of x-ray exposure.
TABLE 3.3 Radiation doses from radiography and fluoroscopy at RERF, Hiroshima, in units of µGy/exposure (Kato et al., 1991b).
|
Projection/ site |
Surface |
Salivary |
Thyroid |
Breast |
Lung |
Stomach |
Colon |
|
PA chest |
140.0 |
9.4 |
12.0 |
20.0 |
66.0 |
23.0 |
2.5 |
|
Lat. chest |
330.0 |
61.0 |
80.0 |
110.0 |
120.0 |
21.0 |
3.5 |
|
AP abdomen |
2,940.0 |
8.8 |
13.0 |
55.0 |
56.0 |
800.0 |
960.0 |
|
AP C-spine |
1,940.0 |
890.0 |
1,710.0 |
31.0 |
220.0 |
2.5 |
1.3 |
|
AP T-spine |
3,160.0 |
91.0 |
170.0 |
2,030.0 |
710.0 |
630.0 |
87.0 |
|
AP L-spine |
3,000.0 |
9.9 |
13.0 |
54.0 |
53.0 |
1,710.0 |
1,350.0 |
|
Flx upper GI* |
3,280.0 |
8.3 |
12.0 |
340.0 |
180.0 |
2,340.0 |
770.0 |
|
Spot upper GI |
1,010.0 |
2.5 |
3.6 |
110.0 |
56.0 |
720.0 |
240.0 |
|
* Flx denotes fluoroscopy, dose in units of µGy/min. |
|||||||
TABLE 3.4 Radiation doses during CT (unit: mGy/examination) (Kato et al., 1991c).
|
|
CT examination |
||||
|
Tissue |
Head |
Chest |
Upper abdomen |
Lower abdomen |
Whole abdomen |
|
Surface |
42.00 |
48.00 |
45.00 |
37.00 |
47.00 |
|
Salivary |
3.16 |
4.60 |
0.34 |
0.07 |
0.31 |
|
Thyroid |
1.65 |
6.67 |
0.47 |
0.07 |
0.40 |
|
Breast |
0.20 |
48.10 |
3.00 |
0.60 |
3.00 |
|
Lung |
0.50 |
43.00 |
7.00 |
0.40 |
6.70 |
|
Stomach |
ND |
5.30 |
35.30 |
2.70 |
42.10 |
|
Colon |
ND |
0.80 |
5.40 |
17.00 |
38.10 |
|
Female gonads |
ND |
0.20 |
0.40 |
24.20 |
25.40 |
|
Active bone marrow |
4.10 |
7.30 |
5.60 |
4.60 |
10.30 |
|
ND: Not detected. |
|||||

FIGURE 3.5 Preliminary tally of computed tomography examinations reported by the AHS participants. The more precise data by irradiation site, by city, and by year will be reported with organ doses in the future.
Medical Radiation Dose And Its Significance
Cumulative Dose from Diagnostic X-Ray Exposures
Kato et al. (1991b) calculated the cumulative doses by organ and by age for a female AHS participant, as shown in Figure 3.6. The integration was done only for the examinations at RERF until 1982. She received many upper gastrointestinal series, and her stomach doses were relatively high. Doses received by each AHS participant were incurred during examinations at RERF and at the other institutions. Figure 3.7 shows cumulative bone marrow doses received by 25 AHS participants. Cumulative doses indicated in this figure were calculated for examinations reported before the end of 1986. The participant who received the highest dose among these 25 participants received 18 fluoroscopic examinations. Her cumulative skin dose was 264.5 cGy. Figure 3.8 shows the distribution of cumulative bone marrow doses from diagnostic x-ray examinations that were conducted for the total 15,111 AHS participants before the end of 1982 (Yamamoto et al., 1988). The average bone marrow dose was 1.2 cGy for the A-bomb exposed group, and 0.89 cGy for the control group (those not in the cities at the time of bombing). At the same
evaluations, the mean cumulative gonadal dose was 1.7 cGy for the female A-bomb exposed group, and 1.3 cGy for the female control group. The percentage of members whose bone marrow doses were larger than 1 cGy was 40.4% in Hiroshima and 32.8% in Nagasaki. The bone marrow doses from the atomic bombs calculated by Shimizu et al. (1989) are also shown in Figure 3.8. This figure suggests that numerous atomic bomb survivors have received medical radiation doses which are comparable with their atomic bomb radiation doses.
Radiation Therapy Doses in the Double Primary Cancer Cases
An analysis using the radiation therapy survey data and the data for cancer incidence before the end of 1983 showed that 134 patients developed malignant neoplasms after their radiation treatments. A precise analysis is in progress. In several cases, the mean therapy dose and the mean atomic bomb dose received in each target organ are compared. Average target organ doses from therapy were much larger than those from the atomic bombs.
Radiation therapy for cervical cancer was typically conducted using high radiation doses on the order 5,000 cGy and typical time-integrated activity of intracavitary therapy by Ra-needle of 3200 mghr. As suggested by Boice et al. (1985), such a large treatment dose might destroy the marrow in the pelvis. However, the doses outside the pelvis were also large. Previous investigations by Russell et al. (1976) and Pinkston et al. (1981) and a preliminary study of the second cancers show that 134 cases of second primary cancers included 9 leukemia cases. Among them, two acute myelocytic leukemias were diagnosed after radiation therapy for cancer of the cervix. A case of sarcoma 11 years after external beam radiation therapy for cervical cancer was also reported by Pinkston and Sekine (1982).
Dose Response to Chromosome Aberrations
It is well known that an increased frequency of radiation-induced chromosomal aberrations has been observed among atomic bomb survivors (Preston et al., 1988). It is also known that diagnostic x-ray exposures may be associated with chromosomal aberrations. The results of a study by Awa and Sawada (1990) seem to confirm this, as shown in Figure 3.9.
However, the frequency of stable cells with aberrations caused by diagnostic x-ray examinations seems to have been higher than that estimated from the linear dose-response model for the atomic bomb doses. Possible reasons for this are as follows:
- Partial active bone marrow is exposed to x-rays in radiography. For example, the maximum bone marrow dose from a CT examination is approximately ten times the bone marrow dose averaged over total bone marrow. This is in contrast to the bone marrow dose from atomic bomb radiation exposure, and the dose responses might be different from one another.


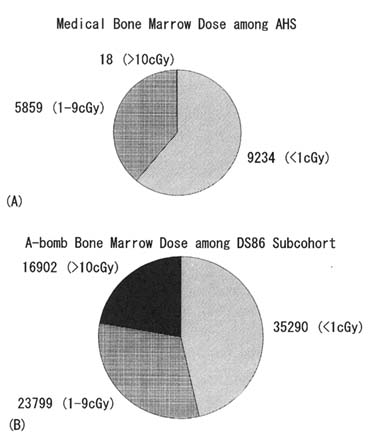
FIGURE 3.8 Distribution of cumulative individual bone marrow doses incurred by diagnostic x-ray examinations (A) and by the atomic bombs (B). The active bone marrow doses from diagnostic x-ray examinations were evaluated for 15,111 Adult Health Study participants until the end of 1982 (Yamamoto et al., 1988). The doses from the atomic bombs were evaluated for 76,000 members in the LSS population (Shimizu et al., 1989).
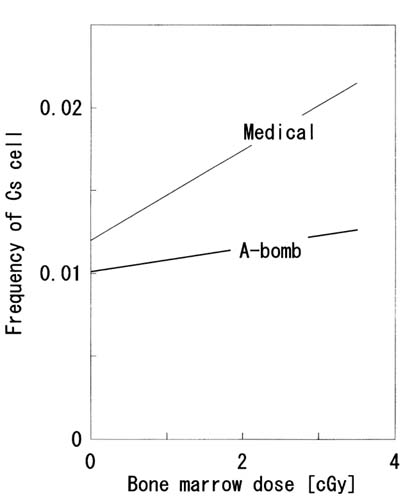
FIGURE 3.9 Dose-response relationships for stable chromosome aberrations. The line indicated by ''Medical" was for bone marrow doses from diagnostic x-ray examinations in Hiroshima (Awa and Sawada, 1990). The line labeled "A-bomb" was for the bone marrow doses from the Hiroshima A-bomb (Preston et al., 1988).
- In the early stages of the present studies, the reporting rate by the AHS participants was 40%. The individual bone marrow doses might have been underestimated due to lack of information about examinations conducted in the early stages. The data from the hospital and clinic surveys during the early years will be useful in supplementing them.
- As shown in cell survival data by Spadinger and Palcic (1992), the biological effects of low-energy photons used in radiological examinations may be greater than those of high-energy photons such as the A-bomb gamma rays.
The relationship between radiation therapy and chromosome aberrations is also under study. The results will be reported in the future.
The present study of medical dosimetry has shown that the doses from the radiological examinations have increased the radiation dose levels of the atomic bomb survivors. The study of radiation therapy showed that many patients treated by radiation received large doses to critical organs near the treatment sites. These medical radiation exposures have been performed since 1945. Relatively long follow-up studies (50 years at maximum) have already become possible. Without the atomic bomb radiations, it may be sufficient to determine the effects of medical radiation exposure, as suggested by the study of the fluoroscopy to the thorax (Boice et al., 1978). Since the quality of medical radiation exposure is different from that of the atomic bomb exposures, it is difficult to assume that they both have the same effects in carcinogenesis. We therefore suspect that the A-bomb zero-dose members in the AHS population will play an important role in solving this equation. The size of the AHS population is relatively small; hence, we must carefully evaluate the subjects' medical radiation doses.
Acknowledgments
The authors are grateful to Drs. Shigetoshi Antoku, Shozo Sawada, Osamu Yamamoto, John S. Laughlin, and Lowell Anderson for their helpful comments and suggestions. The assistance of Mrs. Grace Masumoto in preparing the manuscript is deeply appreciated.