Effects of Ionizing Radiation: Atomic Bomb Survivors and Their Children (1945-1995) (1998)
Chapter: 1 Development of A-Bomb Survivor Dosimetry
1
Development of A-Bomb Survivor Dosimetry
GEORGE D. KERR
Summary
An all-important datum in risk assessment is the radiation dose to individual survivors of the bombings in Hiroshima and Nagasaki. The first set of dose estimates for survivors was based on a dosimetry system developed in 1957 by the Oak Ridge National Laboratory (ORNL). These Tentative 1957 Doses (T57D) were later replaced by a more extensive and refined set of Tentative 1965 Doses (T65D). The T65D system of dose estimation for survivors was also developed at ORNL and served as a basis for risk assessment throughout the 1970s.
In the late 1970s, it was suggested that there were serious inadequacies with the T65D system, and these inadequacies were the topic of discussion at two symposia held in 1981. In early 1983, joint US-Japan research programs were established to conduct a thorough review of all aspects of the radiation dosimetry for the Hiroshima and Nagasaki A-bomb survivors. A number of important contributions to this review were made by ORNL staff members. The review was completed in 1986 and a new Dosimetry System 1986 (DS86) was adopted for use.
This paper discusses the development of the various systems of A-bomb survivor dosimetry, and the status of the current DS86 system as it is being applied in the medical follow-up studies of the A-bomb survivors and their offspring.1

FIGURE 1.1(a) Example of a shielding history for a survivor exposed inside a one-story Japanese-type house in Hiroshima.
Introduction
Some individuals survived close to the bombs because they were protected by buildings (Noble, 1967). The amount of protection provided by buildings and other nearby structures is commonly referred to as shielding (see Figure 1.1). Other individuals survived because they were located at very great distances from the hypocenters of the bombs. Thus, an individual's distance from the hypocenter or ground range was one of the important criteria used in the selection of the major study populations of the Radiation Effects Research Foundation (RERF) and its predecessor, the Atomic Bomb Casualty Commission (ABCC) (Beebe and Usagawa, 1968).
A summary of the major study populations is provided in Table 1.1. Originally the Life Span Study (LSS) consisted of 100,000 survivors and control subjects, but additional members were added to this mortality study in 1967 and 1985 so that the LSS extended sample (designated more appropriately as the LSS-E85 sample)
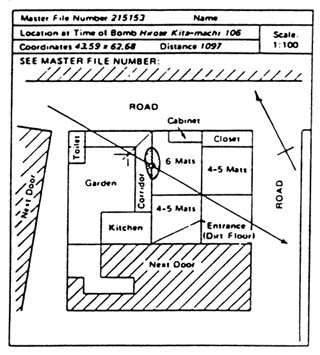
FIGURE 1.1(b) Example of a shielding history for a survivor exposed inside a one-story Japanese-type house in Hiroshima.
now consists of 120,000 survivors and control subjects (Preston et al., 1987). The Adult Health Study (AHS) originally consisted of 20,000 members, all of whom were part of the LSS sample. Attrition by death and migration reduced this clinical study sample to about 50% of its original size by 1984. Thus, the current AHS sample was also enlarged to include more of the highly exposed survivors in the LSS sample, the in utero clinical sample, which is part of the larger in utero sample, and appropriate control subjects.
The survivors (and offspring of survivors) who were located at ground ranges of less than 2,500 m are the core group of the major study samples and are often referred to as the proximal exposed group. Other groups used as controls are the distal exposed group of survivors who were located at ground ranges between 2,500 and 10,000 m, and the non-exposed group of survivors who were located at more than 10,000 m. The non-exposed group is referred to commonly as the not-in-city (NIC) group because it contains a large number of individuals who were not in

FIGURE 1.1(c) Example of a shielding history for a survivor exposed inside a one-story Japanese-type house in Hiroshima.
the cities at the time of bombing (ATB) but took up residency in Hiroshima or Nagasaki prior to 1950 (Ishida and Beebe, 1959).
Shielding histories were compiled for proximal exposed survivors starting in 1951 in Nagasaki and 1954 in Hiroshima (Noble, 1967; Beebe and Usagawa, 1968). The strategies used in the two cites were somewhat different because there were more proximal exposed survivors in Hiroshima than in Nagasaki (see Table 1.2). In Nagasaki, shielding histories were compiled on all survivors who were located at ground ranges of less than 2,000 m. However, the approach in Hiroshima was to take shielding histories out to 2,000 m for only those survivors included in smaller study samples (e.g., the AHS and in utero samples). It was decided initially that shielding histories would only be taken on the LSS subjects who were located at less than 1,200 m. After shielding histories were compiled on the LSS subjects under 1,200 m, however, the 100 percent criteria was extended
TABLE 1.1 Major study populations.
|
Study |
Approximate number of subjects |
Year base populations established |
Year studies initiated |
|
Survivors: |
|||
|
Life Span Study (LSS) |
120,000 |
1950a |
1958 |
|
Adult Health Study (AHS) |
23,500 |
1950a |
1958 |
|
In utero sample |
2,800 |
1945–46b |
1960 |
|
Offspring of survivors: |
|||
|
First generation (F1) mortality |
75,000 |
1946–85c |
1960 |
|
Chromosome aberrations |
33,000 |
1946–85c |
1967 |
|
Biochemical Genetics Study (BGS) |
45,000 |
1946–85c |
1975 |
|
aSpecial supplement to the 1950 National Census in Japan. bBirth records from August 1945 through May 1946. cBirth records from June 1946 through December 1985. |
|||
to those LSS subjects under 1,300 m, and so on, ending at 1,600 m (Milton and Shohoji, 1968).
When the T65D system became available (Auxier et al., 1966), it appeared that the radiation doses were approximately equal at 1,600 m in Hiroshima and 2,000 m in Nagasaki. At that time, shielding histories were available for most of the Nagasaki survivors who were located at ground ranges of less than 2,000 m. In Hiroshima, shielding histories were available for most of the LSS subjects under 1,600 m, 30% of the LSS subjects between 1,600 and 2,000 m, and most other sample subjects under 2,000 m. In both cities, there were a number of cases in which shielding histories were either incomplete or unavailable because of the migration or death of survivors before 1965. For some cases, however, information such as ''exposed inside a Japanese house" or "exposed outside unshielded" was available from earlier studies and surveys (Ishida and Beebe, 1959).
In the late 1970s, the T65D estimates for Nagasaki survivors were recalculated using a different hypocenter and burst height for the bomb (Kato and Schull, 1982), and the dose estimates for survivors in both cities were redesignated as T65D Revised (T65DR). There were no changes in the dose estimates for Hiroshima survivors, and the changes for the Nagasaki survivors were small (less than 10%). Hence, it needs to be noted that sometimes the T65DR estimates for survivors may
TABLE 1.2 Inventory of shielding histories for proximal exposed survivors by shielding category.
|
City |
Shielding category |
Number |
Percent |
|
Hiroshima |
Outside–unshielded |
2,490 |
12.2 |
|
|
Outside–partially shielded |
547 |
2.7 |
|
|
Outside–shielded by terrain |
46 |
0.2 |
|
|
Outside–shielded by a house |
2,463 |
12.1 |
|
|
Inside–Japanese house |
14,130 |
69.4 |
|
|
Inside–concrete building |
329 |
1.6 |
|
|
Inside–factory building |
33 |
0.2 |
|
|
Inside–air raid shelter |
46 |
0.2 |
|
|
Miscellaneous shielding |
275 |
1.4 |
|
|
Total all categories |
20,359 |
100.0 |
|
Nagasaki |
Outside-unshielded |
513 |
6.1 |
|
|
Outside-partially shielded |
625 |
7.5 |
|
|
Outside-shielded by terrain |
392 |
4.7 |
|
|
Outside-shielded by a house |
1,125 |
13.5 |
|
|
Inside-Japanese house |
3,660 |
43.8 |
|
|
Inside-concrete building |
616 |
7.4 |
|
|
Inside-factory building |
1,047 |
12.5 |
|
|
Inside-air raid shelter |
336 |
4.0 |
|
|
Miscellaneous shielding |
41 |
0.5 |
|
|
Total all categories |
8,355 |
100.0 |
be referred to simply as T65D estimates (Kerr, 1989). The hypocenters and burst heights used in the various dosimetry studies are discussed by Milton and Shohoji (1968), Kato and Schull (1982), and Kerr et al. (1987).
Tentative 1957 Doses (T57D)
During Operation Teapot at the Nevada Test Site (NTS) in 1955, ORNL, in cooperation with the Los Alamos National Laboratory (LANL), conducted a series of experiments which provided a much better understanding of weapon radiation fields. The results of these Operation Teapot experiments indicated the possibility of a definitive description of radiation fields from the Hiroshima and Nagasaki bombs (Kerr et al., 1992).
Consequently, in early 1956, a survey team visited ABCC in Hiroshima and Nagasaki to determine the feasibility of a dosimetry study. This survey team included Sam Hurst and Rufus Ritchie of ORNL, Payne Harris of LANL, Bill Ham of the Medical College of Virginia, and Bob Corsbie of the US Atomic Energy Commission (AEC). Several ABCC studies had already reported an elevated incidence of cataracts and leukemia in the surviving populations, especially in Hiroshima.
After reviewing records and examining shielding configurations for survivors, the survey team recommended that a dosimetry program be initiated. Emphasis was to be placed on the shielding provided by Japanese-type houses because of the high structural uniformity of the houses and the large number of survivors who were inside such structures when exposed. As a result of the survey team's findings, an AEC-funded program was established at ORNL and designated as Ichiban—a Japanese word meaning first or number one—because it was considered to be one of the top-priority programs at ORNL during the late fifties and early sixties.
After completion of the analysis of data from Plumbbob, a summary of all dosimetry information applicable to the survivors was prepared and transmitted to the shielding group at ABCC. Designated as T57D, this tentative dosimetry served as a guide for determining dose values from the shielding histories of the exposed individuals. With the assignment of Ed Arakawa to Hiroshima from 1958 to 1960, the shielding results from the nuclear weapons test at NTS were applied in medical follow-up studies of the survivors by ABCC (Arakawa, 1960). These studies, together with the equations for the weapon radiation fields by E.N. York of the Air Force Special Weapons Center (York, 1957), led to the assignment of gamma-ray and neutron doses to individual medical records of survivors instead of the previously used broad dose-value categories based on distance from the hypocenter of the bombs. The T57D system of dose estimation was first used in 1959 to derive dose response curves for leukemia among lightly shielded survivors of the two cities (Heyssel et al., 1959; Tomonaga et al., 1959).
The procedure for estimating radiation doses to survivors exposed in houses that were either unshielded or lightly shielded by neighboring houses was as follows. From Figure 1.1(a), the distance from the hypocenter or ground range in Hiroshima was computed (i.e., 1,097 m) and the radiation levels in the open at the given ground range in Hiroshima were then determined from the equations defining the dose curves shown in Figure 1.4. With the help of Figure 1.1(c), the house penetration distance was measured (i.e., the dashed line from the roof to the survivor), and the house transmission factors were then determined from Figure 1.3. The computations of in-air tissue kerma within the house were performed separately for each radiation component (i.e., neutrons and gamma rays) and for each exposed individual in Hiroshima or Nagasaki.
York's dose curves in Figure 1.4 were in general agreement with the results of an earlier 1951 study by R.R. Wilson (1956). In this earlier study, Wilson concluded that the ratio of neutrons to gamma rays was quite different at Hiroshima and Nagasaki, and one might hope to separate the radiological effects due to gamma


rays and neutrons by a comparative study of the effects in the two cities. At Hiroshima, neutron effects might predominate, whereas at Nagasaki, the situation was reversed and nearly all the radiation dose was due to gamma rays. To improve the radiation dose estimates for atomic bomb survivors, Ritchie and Hurst (1959) suggested that it would be necessary to (1) establish more accurate source terms for neutrons and gamma rays from the Hiroshima and Nagasaki bombs and (2) obtain information on radiation shielding by more general house configurations.
Tentative 1965 Doses (T65D)
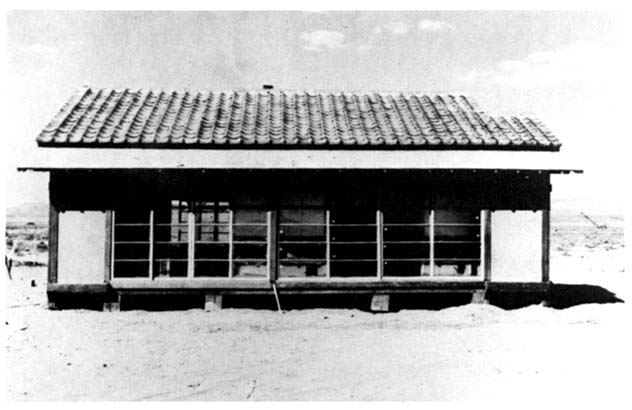
Following Operation Plumbbob, laboratory studies of the shielding coefficients of Japanese and American building materials were conducted by John Auxier, Fred Sanders, and Wendell Ogg. Cement-asbestos board, commercially available in large sheets, was found to be suitable as a substitute for the mixture of clay, oyster shells, and seaweed wall plaster and for the embedding clay and tile roofs of Japanese houses for both neutrons and gamma rays. The wood framing used in Japan fitted well with the substitution of cement-asbestos board, and domestic materials were used to construct Japanese house replicas for shielding studies during later weapon tests at NTS (see Figure 1.5).
During Operation Hardtack II in 1958, a large number of collimators were used for measuring the angular distributions of the neutrons and gamma rays from a nuclear weapon, and seven replicas of Japanese houses were constructed for the shielding studies. Three different floor plans which represented about 90% of all single family dwellings in Hiroshima and Nagasaki were used to construct the seven house replicas (i.e., three small one-story tenement houses, two medium-size one-story houses, and two large two-story houses). Emphasis was placed on evaluating the shielding as functions of house size, orientation, and position relative to other nearby houses. Because of the durability of the wall board, six of the seven houses were repaired and used three times and the seventh was used twice. The measurements at weapon test sites ended with the Limited Test Ban Treaty of 1962.
Consequently, it was decided to do a definitive study of the radiation fields at large distances from a small unmoderated and unshielded reactor. Designated as Operation BREN (Bare Reactor Experiment Nevada), the experiments were conducted under the leadership of John Auxier and Fred Sanders during the spring and early summer of 1962. The reactor was mounted on a hoist car, which was in turn mounted on a 465-m tower at NTS and operated at various heights above ground to simulate the prompt neutron and gamma-ray fields from a nuclear weapon. At 465 m (1,527 ft.), the BREN tower was taller than the Washington Monument at 169 m (555 ft.), the Eiffel Tower at 300 m (984 ft.), and the Empire State Building at 448 m (1,472 ft.). A 60Co source of about 1,200 curies was to simulate the delayed gamma-ray field from the fireball of a nuclear weapon following the completion of the reactor studies.
During Operation BREN in 1962, extensive measurements were made of the radiation fields in the open, in Japanese houses, and in clusters of Japanese houses. By the use of data from Operation BREN and earlier weapon tests, Cheka et al. (1965) developed a set of nine-parameter linear regression equations that could be used to calculate the transmission factors for survivors exposed inside houses in either city. The nine-parameter equations allowed these factors to be calculated as functions of such things as house size and orientation, location of a survivor inside the house, house penetration distance, location of the house with respect to nearby structures, and proximity of a survivor to an unshielded window facing toward the bomb.
The primary techniques for obtaining transmission factors in the T65D system of dose estimation for A-bomb survivors were as follows:
- The nine-parameter formulas for survivors exposed inside either one- or two-story Japanese houses or smaller tenement houses (Milton and Shohoji, 1968, pp. 42–43).
- The globe technique of determining transmission factors by a combination experimental and calculational approach, using measured angular distributions as input data (Noble, 1967, pp. 28–29 and 79–80).
- The ad hoc assignment of transmission factors based on a review of shielding histories or groups of similar shielding histories (Milton and Shohoji, 1968, pp. 8–9).
The globe technique was used for survivors who were outside but shielded by houses or terrain and for some survivors who were inside concrete buildings. Several important examples of ad hoc assignments within the T65D system were as follows:
- The use of averaged transmission factors for survivors who were known to be inside Japanese houses but for whom shielding histories were either incomplete or unavailable.
- The assignment of transmission factors of 0.9 or 1.0 for survivors inside factory buildings at Nagasaki and either shielded or unshielded by heavy equipment and machine tools, respectively.
- The assignment of transmission factors of 1.0 for all survivors who lacked shielding histories and were located at ground ranges of more than 1,600 m in Hiroshima and 2,000 m in Nagasaki.
Transmission factors and radiation doses were neither calculated nor assigned for 3,017 proximal exposed survivors because their shielding conditions were either extremely complex or unknown.
Following Operation BREN in 1962, Auxier et al. (1966) also developed a new set of dose curves for the weapon radiation fields in the open that were designated


as T65D (see Figure 1.6). Ideally, these dose curves would have been established from test firings of exact duplicates of the Japanese weapons. Some information was available from early tests of several Nagasaki-type weapons, but the Hiroshima bomb was the only one of its type that was ever fired, and the weapon radiation fields in Hiroshima had to be constructed using indirect evidence from calculations and experiments with nuclear reactors. However, the dose curves generated by the T65D equations were found to agree closely with results of independent studies by Hashizume et al. (1967) at the Japanese National Institute of Radiological Sciences (NIRS) and by Ichikawa, Higashimura, and Sidei (1966) at the University of Kyoto (see Figure 1.6).
The gamma-ray doses of Ichikawa and co-workers were derived using thermoluminescence of quartz crystals from roof tiles. Some rather large uncertainties were involved in the estimated ground ranges. Since roof tiles were used only on Japanese houses and all houses close to the hypocenter were destroyed, the exact location of each roof tile ATB was in doubt. The gamma-ray and neutron doses in the NIRS study were derived using the gamma-ray-induced thermoluminescence of quartz crystals in decorative tiles and bricks and the neutron-induced 60Co radioactivity in steel reinforcing bars (rebars) taken from commercial buildings that had been repaired and used for a number of years after the bombings. The exact location of each sample ATB was well known, and the uncertainties in the estimated ground ranges were minimized. The NIRS study seemed to confirm the T65D results, and the T65D dose curves for the weapon radiation fields in both cities were used with a great deal of confidence in risk assessment throughout the 1970s.
Finally, the transport of radiation in the body of the survivors was calculated by Troyce Jones and co-workers in the 1970s (Jones et al., 1975), and the results were provided to the RERF as sets of organ dose factors which allowed one to account for the self-shielding of internal organs by overlying tissues of the body (Kerr, 1979). For leukemia, the organ of interest was the active bone marrow, and for other cancers, the specific organs of interest were the female breast tissue, lungs, stomach, etc. For studies of survivors exposed in utero, the radiation dose to the fetus was needed, and for studies of first generation (F1) offspring of survivors, the radiation doses to the testes and ovaries of the F1 parents were important. The absorbed doses to the deeply seated internal organs and fetus were significantly less than the T65D estimates of in-air tissue kerma for survivors, which served only as an approximation to the maximum absorbed dose at the surface (skin) of the body (see, for example, Committee on the Biological Effects of Ionizing Radiations, 1972, p. 101).
In the late 1970s, it was suggested that there were serious inadequacies with the T65D system, and these inadequacies were discussed at two symposia held in 1981 (Sinclair and Failla, 1981; Bond and Thiessen, 1982). The starting point for these discussions was the source term calculations for the Hiroshima and Nagasaki bombs by W.E. Preeg of LANL (Bond and Thiessen, 1982, pp. 125–130). In early

FIGURE 1.7 Illustration of the overlap among members and parents of offspring in the major study samples.
1983, joint US-Japan research programs were established to conduct a thorough review of all aspects of the radiation dosimetry for the Hiroshima and Nagasaki A-bomb survivors (RERF, 1983a; RERF, 1983b). The review was completed in 1986 and the new DS86 system of dose estimation was adopted for use (RERF, 1987; Shimizu et al., 1989).
Two conditions were set on the cohort selected for dose estimation using the DS86 methods: (1) each individual must have a T65D (or T65DR) estimate, and (2) each individual must be a member or parent of an offspring in a major study sample (see Figure 1.7). The total cohort due to overlap among the populations of the various samples is approximately 141,600 individuals (i.e., the 120,000 survivors of the LSS sample plus the 1,600 survivors of the in utero clinical sample and the 20,000 F1 parents who are not part of the LSS sample).
To facilitate the application of the DS86 methods of dose estimation for individual survivors, a modular computer code system was developed (RERF, 1987, Vol. 1, pp. 405–431). The DS86 methods were embodied in this code system as follows:
- A database for the weapon radiation fields in the open, which specifies the differential energy and angular fluences of neutron and gamma rays at four different heights above ground and at 25-m intervals from 100 to 2,500 m of ground range in both cities (Kerr et al., 1987).
- A database for house-shielding cases, which describes how the differential neutron and gamma-ray fluences were modified at over 50 locations inside a Japanese house (or house cluster) and at a similar number of locations in which a survivor was outside and either partially shielded or totally shielded by a Japanese house (Woolson et al., 1987).
- A database for organ dosimetry, which describes how the differential neutron and gamma-ray fluences were further modified at 15 internal organ sites as functions of a survivor's orientation and posture ATB (RERF, 1987, Vol. 1, pp. 306–404). Age-dependent organ tissue doses can be made for infants (less than 3 years old ATB), children (3 to 12 years old ATB), and adults (more than 12 years old ATB).
Since the DS86 Final Report was published, two additional shielding databases have been added to the modular computer code. One of these databases was developed for application to terrain-shielded survivors at Nagasaki (the database for terrain shielding in the DS86 Final Report was never used and it was later replaced by a more refined database for terrain shielding), and the other database was developed for application to factory-shielded survivors at several sites in Nagasaki (the Ordnance Plant at Oshashi, Steel Works at Mori-machi, and Dockyards at Saiwai-cho).
Suppose a survivor was exposed inside a small one-story Japanese-type house as illustrated in Figure 1.8. First, the house was positioned about the survivor to simulate his or her actual shielding configuration ATB, and both the house and individual were positioned at the correct ground range from either the Hiroshima or Nagasaki bomb. Next, the differential particle fluences from the database for the radiation fields in the open for the appropriate city were coupled with the adjoint particle fluences from the database for house shielding to obtain the radiation fields inside the house. Finally, t he adjoint particle fluences from the database for organ doses were coupled with the radiation fields inside the house to provide organ tissue doses (as functions of age, posture, and orientation of the individual ATB) and in-air tissue kermas (inside and outside the house). This same procedure was used with the databases for other shielding situations (i.e., outside shielded by a house, inside a factory building, etc.).
Because of the expense of a re-examination of the shielding histories, the DS86 database for house shielding was constructed to use computerized shielding data

FIGURE 1.8 Illustration of the overall DS86 coupling procedure for dose estimation for individual A-bomb survivors with shielding histories.
that had been coded for T65D. Unlike T65D, however, DS86 does not make use of transmission factors or organ-dose factors per se, and organ tissue doses and in-air tissue kermas were calculated directly for survivors with shielding histories if the survivors' location ATB fit one of the following categories:
- Inside a Japanese-type house or tenement for which nine-parameter data were coded (18,315 individuals).
- In the open but shielded by a Japanese-type house or tenement for which globe data were coded (3,806 individuals).
- In the open but shielded by terrain features for which globe data were coded (361 individuals).
- In the open and unshielded with thermal flash burns reported on exposed portions of the face, neck, or arms (1,297 individuals).
- Inside a steel frame factory building of light construction in Nagasaki without any additional shielding by heavy equipment or machine tools (815 individuals).
For survivors without shielding histories, it was necessary to develop supplemental techniques for indirect computation of the in-air tissue kerma and organ tissue doses. The various supplemental techniques for dose estimation are as follows:
- The use of an in-air tissue kerma of zero at ground distances of more than 2,560 m in Hiroshima and 2,760 m in Nagasaki, where the in-air kermas to shielded survivors were less than 0.005 Gy (45,405 individuals).
- The use of averaged transmission factors and organ doses for survivors with limited shielding data which identified them as being exposed inside Japanese-type houses or tenements ATB (25,962 individuals).
- The use of averaged transmission factors and organ doses for survivors with limited shielding data which identified them as being exposed outside with or without shielding by houses or terrain ATB (10,034 individuals).
For this latter group, the in-air tissue kermas and organ tissue doses are less than 0.2 Gy in Hiroshima and less than 0.1 Gy in Nagasaki. Most of these survivors have been used traditionally as control subjects, and their addition to the LSS sample offers little in the assessment of somatic risks. The primary reason for this extension of DS86 was to meet the special needs of the genetic studies. An offspring of two exposed parents may not be part of the control group for the assessment of genetic risks, and the offspring may be classified as a DS86 unknown-dose case if the radiation doses are not available for both parents. Thus, the use of this extension of DS86 is considered optional in the analyses of data from the different study populations (see Table 1.1).
Currently, DS86 estimates using either direct or indirect methods are available for 105,995 individuals or 92% of the total of 115,019 survivors who are members of the LSS and in utero samples, or parents of offspring in the F1 mortality sample (see Table 1.3). However, there are now 9,024 survivors without DS86 estimates (DS86 unknown) compared to only 3,017 survivors without T65D estimates (T65D unknown). Most of the DS86 unknown-dose cases are proximal exposed survivors who reported being in the open without reporting flash burns, inside very heavily shielding structures (e.g., concrete buildings or air-raid shelters), or in very complex shielding situations (e.g., inside street cars, etc.).
Figure 1.9 presents a comparison of the DS86 and T65D curves for the radiation fields in the open at Hiroshima and Nagasaki, and Table 1.4 presents a comparison of DS86 and T65D values of the radiation doses for an adult A-bomb survivors exposed inside a Japanese-type house at 1,200 m of ground range in both cities. The latter DS86 and T65D values can be compared directly because they were derived in a consistent manner (i.e., the DS86 values are based on house transmission factors and organ dose factors derived as averages from direct DS86 estimates for all survivors who were exposed inside Japanese-type houses or tenements). The principal differences between these two dosimetry systems can be summarized as follows:
TABLE 1.3 Inventory of DS86 estimates for individual survivors.
|
Estimation method |
Number of individuals |
|
Direct DS86 estimates |
24,594 |
|
Indirect DS86 estimates |
81,401 |
|
Total DS86 estimates |
105,995 |
|
Unknown DS86 |
9,024 |
|
Total DS86 cohort |
115,019 |
|
Not-in-city (NIC) |
26,616 |
|
Sample totals |
141,635 |
- In Hiroshima, the gamma-ray kerma is larger than before, due in part to a change in estimate of bomb yield from the T65D value of 12.5 kiloton to the DS86 value of 15 kiloton, whereas in Nagasaki, values of bomb yield and gamma-ray kerma were similar to previous values (see Figure 1.9).
- In both Hiroshima and Nagasaki, the neutron kermas are significantly less than before for a couple of reasons (see Figure 1.9). One reason is that the newer source terms suggest that the prompt neutrons coming from the Hiroshima bomb are more degraded in energy than thought previously (RERF, 1983a, pp. 13–39), and the other reason is that the high humidity in Hiroshima and Nagasaki was not adequately taken into account before (i.e., modern weapon calculations indicate a reduction by a factor of two in neutron kerma because of the higher humidities, all other things being equal). The DS86 values suggest that neutrons are no longer considered a significant contributor to the radiation doses for Hiroshima survivors, and survivors in both cities were exposed mainly to gamma rays (see Table 1.4).
- The newer DS86 values for the transmission of gamma rays by houses are about half of the T65D values [i.e., the average transmission factors are 0.90 (T65D) versus 0.46 (DS86) in Hiroshima and 0.81 (T65D) versus 0.48 (DS86) in Nagasaki]. Thus, the T65D system seriously overestimated the transmission of gamma rays by houses (see Table 1.4). The newer DS86 values for the transmission of neutrons by houses have remained about the same as the T65D values [i.e., the average factors for the two systems are 0.36 (T65D) versus 0.46 (DS86) in Hiroshima and 0.35 (T65D) versus 0.41 (DS86) in Nagasaki].
- Organ dosimetry was not included as part of the original T65D system, but techniques for the estimation of organ tissue doses were added later. These techniques have now been found to seriously underestimate the tissue transmission of gamma rays by a factor of as much as two in the case of the deeply seated internal organs (Kerr, 1989). However, the increased tissue transmission for gamma rays in the DS86 system is largely or wholly offset by the changes in the house transmission factors, except in the case of a few superficial organs such as the female breast (see Table 1.4).
Discussion
One major task of the recent dose reassessment studies was to test the DS86 calculations to the maximum extent feasible. For example, considerable effort was made to extend the thermoluminescent (TL) measurements of the 1960s to longer ground ranges in both cities (RERF, 1987, Vol. 1, pp. 143–184). These TL measurements as well as the newer TL measurements of the DS86 study, are shown in Figure 1.10 as functions of the slant range, which is the distance from the weapon's burst point in air to a point of interest at or near the ground. The slant range is used here to account for differences in the heights of the various TL samples above the ground. It should be noted that the DS86 calculations for the gamma-ray fields in the open are in close agreement with the TL measurements at the longer ranges where there are considerable differences between the DS86 and T65D values (see Figure 1.9). The TL measurements are discussed in reports by Ichikawa and colleagues (Ichikawa et al., 1966; Ichikawa et al., 1987; Hoshi et al., 1987) and the staff of the NIRS in Japan (Hashizume et al., 1967; Maruyama et al., 1987).
A major disappointment of the DS86 study was the poor agreement between calculations and measurements of cobalt activation by slow neutrons at both Hiroshima and Nagasaki (Loewe, 1985; Kerr et al., 1990; Kimura and Hamada, 1993). Recently, it has been found that the DS86 neutron calculations were in close agreement with a newer and more extensive set of measurements at Nagasaki for chlorine activation by slow neutrons (Straume et al., 1994). However, the new chlorine-activation data have also confirmed the previously noted discrepancy in the cobalt activation at Hiroshima (see Figure 1.11). At Hiroshima, the calculated-to-measured ratios for cobalt activation are always greater than one at shorter ranges (i.e., less than 600 m of ground range or 840 m of slant range) and always less than one at longer ranges. Thus, the DS86 neutron calculations for Hiroshima appear to be too low by factors ranging from 2 to 10 at the ranges of most interest in the A-bomb survivor studies (i.e., 1,000 to 2,000 m of ground range or 1,160 to 2,080 m of slant range).


TABLE 1.4 Comparison of radiation doses for an adult A-bomb survivor exposed inside a Japanese-type house at 1,200 m of ground range.
|
City |
Dosimetric quantity |
Dose system |
Average radiation dose (Gy) |
|
|
|
|
|
|
Total |
Gamma rays |
Neutrons |
|
Hiroshima |
In-air tissue kerma |
DS86 T65D |
0.783 1.041 |
0.762 0.855 |
0.021 0.186 |
|
|
Female breast tissue |
DS86 T65D |
0.663 0.794 |
0.650 0.692 |
0.013 0.102 |
|
|
Active bone marrow |
DS86 T65D |
0.634 0.543 |
0.626 0.491 |
0.008 0.052 |
|
|
Lung |
DS86 T65D |
0.619 0.482 |
0.612 0.441 |
0.007 0.041 |
|
|
Stomach |
DS86 T65D |
0.584 0.450 |
0.578 0.415 |
0.006 0.035 |
|
|
Large intestine |
DS86 T65D |
0.573 0.382 |
0.569 0.356 |
0.004 0.026 |
|
Nagasaki |
In-air tissue kerma |
DS86 T65D |
1.556 3.219 |
1.544 3.186 |
0.016 0.037 |
|
|
Female breast tissue |
DS86 T65D |
1.311 2.570 |
1.301 2.550 |
0.010 0.020 |
|
|
Active bone marrow |
DS86 T65D |
1.274 1.797 |
1.267 1.787 |
0.007 0.010 |
|
|
Lung |
DS86 T65D |
1.236 1.604 |
1.230 1.596 |
0.006 0.008 |
|
|
Stomach |
DS86 T65D |
1.175 1.507 |
1.170 1.500 |
0.005 0.007 |
|
|
Large intestine |
DS86 T65D |
1.160 1.282 |
1.156 1.277 |
0.004 0.005 |
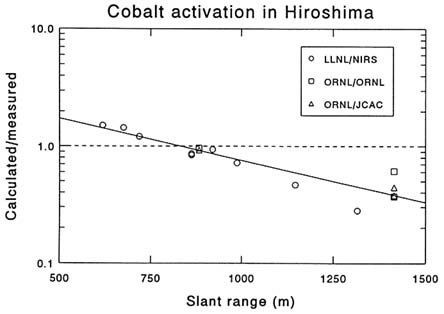
FIGURE 1.11 Calculated-to-measured ratios for cobalt activation in Hiroshima. The ratios shown in the figure are derived from studies at the Lawrence Livermore National Laboratory (LLNL), Japanese National Institute for Radiological Sciences (NIRS), Japan Chemical Analysis Center (JCAC), and Oak Ridge National Laboratory (ORNL).
A new set of ORNL calculations has been made recently by Rhoades et al. (1994) to obtain neutron kermas that were consistent with the various neutron activation data at Hiroshima (see Figure 1.12). Once a neutron source term was found that reproduced the neutron activation by fast neutrons in sulfur and by slow neutrons in cobalt, chlorine, and europium to within approximately 20% at all ranges, it was used to calculate the in-air tissue kerma from neutrons and from neutron-produced gamma rays in air and ground, which were then added to the other gamma-ray components of the weapon radiation fields in the open. Good agreement is maintained with the DS86 gamma-ray values (and the TL measurements shown in Figure 1.10), even though the new ORNL calculations are a factor of five greater than the DS86 neutron values and only a factor of two less than the T65D neutron values over the ranges of most interest in the A-bomb survivors studies (i.e., 1,000 to 2,000 m of ground range or 1,160 to 2,080 m of slant range). Based on these new ORNL calculations, it seems particularly important to give a top priority to a more complete resolution of the causes for
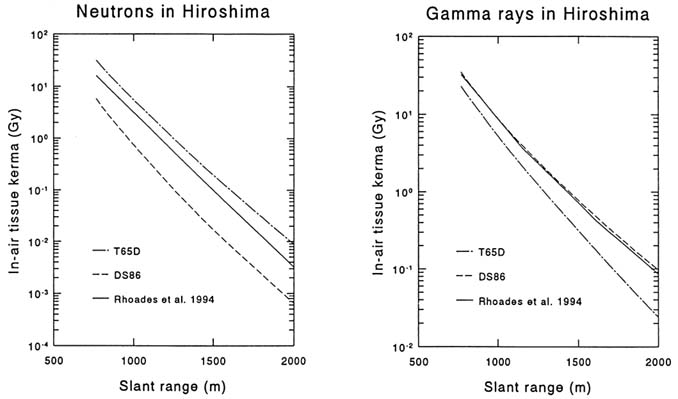
FIGURE 1.12 Comparison of the weapon radiation fields in the open in Hiroshima from T65D, DS86, and ORNL calculations by Rhoades et al. (1994). A source term was selected in these 1994 ORAL calculations which reproduced the correct neutron activation by fast neutrons in sulfur and by slow neutrons in cobalt, chlorine, and europium.
the DS86 neutron discrepancy and to incorporate the revised neutron doses at Hiroshima into an updated DS86 system (see Figure 1.12). This should enable neutron quality factors to be derived directly from human data rather than using the more exaggerated values sometimes seen in animal or cell studies (Grimwood and Charles, 1994).
Acknowledgments
The author has served as a consultant to the RERF since 1975, and many individuals at the RERF and elsewhere have contributed to the work summarized in this report. Those who deserve special acknowledgments for their contributions are Dale Preston (RERF), Shoichiro Fujita (RERF), Jill Ohara (RERF), Dean Kaul (SAIC), Bill Woolson (SAIC), and the many ORNL staff members who have contributed to the development of the radiation dosimetry for the A-bomb survivors.
| This page in the original is blank. |